

Abstract
Background: Experiences of sexual trauma are associated with adverse patient and health system outcomes, but are not systematically documented in electronic health records (EHR). Objective: To describe variations in how sexual trauma is documented in the Veterans Health Adminstration’s EHR. Methods: Sexual trauma concepts were extracted from from 362,559 clinical notes using a natural language processing pipeline. Results: We observed variations in the presence of sexual trauma in notes across five United States regions: Pacific, Continental, Midwest, North Atlantic, Southeast. We also observed variations in the types of notes used to document sexual trauma (e.g., mental health, primary care) and sources of sexual trauma (e.g., adult, childhood, military) mentioned in the EHR. Our findings illustrate potential differences in cultural norms related to patient disclosure of sensitive information, and provider documentation. Standardized protocol for eliciting and documenting sexual trauma histories are needed to ensure Veteran access to high quality, trauma-informed care.
Introduction
Experiences of sexual trauma are associated with adverse patient and health system outcomes and are important to elicit during patient-provider interactions. These experiences are, however, not routinely disclosed by trauma survivors in civilian1, 2 and military settings3-5. Moreover, these adverse experiences are not systematically documented in patient medical records due a variety of reasons, including provider norms and patient preferences. Sexual trauma, which includes both experiences of assault and harassment, has been described as part of adverse childhood experiences, as well as in adulthood on college campuses, in the workplace, and in intimate partner relationships. We are increasingly aware of the detrimental clinical outcomes associated with sexual trauma. These include psychiatric comorbidities such as depression, anxiety, post-traumatic stress disorder, and alcohol and drug use disorders6,7. The initial psychiatric sequelae of sexual trauma, in the absence of intervention, may accumulate to affect a broad range of health and psychosocial domains, with symptoms often persisting for several years following the incident. Indeed, long-term consequences of sexual trauma include chronic medical conditions (e.g., chronic pulmonary disease, liver disease, and hypertension)8, legal involvement9, homelessness10, and suicide11.
Disclosure of a history of sexual trauma is an essential first step to receiving counseling or trauma-informed treatment that may address the long-term sequelae of these traumatic experiences12. However, little is known about the circumstances of sexual trauma disclosure in health care settings, or how patient histories of sexual trauma are documented in electronic health record (EHR) notes. Most health care systems lack routine screening for patient histories of sexual trauma. Even when screenings occur, sexual trauma experiences are under-reported due to stigma, shame, and privacy concerns13. For example, a recent study of documentation of sexual trauma in the Veterans Health Administration found that male and racial/ethnic minorities with a history of military sexual trauma were less likely than female and non-Hispanic Whites, respectively, to disclose information regarding sexual trauma on an initial clinical screen14. Some patients only volunteer sexual trauma information in a therapeutic context, or when rapport has been established with their routine provider. In other cases, sexual trauma is documented when a patient presents to the emergency department for treatment of acute symptoms. An examination of the free text of EHR notes may shed light on the circumstances of patient disclosures of sexual trauma and provider practices of documentation in medical records.
Health care providers document a patient’s medical status, psychosocial circumstances, and historical information through clinical narratives in the EHR, and the presence and availability of this information in clinical documents informs patient care. In the case of sexual trauma, the availability of patient history information facilitates the delivery of trauma-informed care across the health care system15. However, there is reason to think that sexual trauma history information may not be captured in a standardized way. Use of International Classication of Disease (ICD) codes to record sexual trauma histories is limited, and research in other clinical domains has identified substantial variations in documentation practices16. To optimize health care efficiency, and to maximize the utility of the EHR, it is important to identify major variations in clinical documentation of sexual trauma histories and to understand the nature of those variations16.
This paper aims to characterize regional geographic variations in documentation of sexual trauma histories in the Veterans Health Adminstration (VHA). We chose United States geographic regions as a potential source of variation because these may serve as proxies for sociocultural norms in patient reporting and provider documentation of sexual trauma information18. To accomplish the study aim, mentions of sexual trauma concepts in the EHR were extracted via a natural language processing (NLP) pipeline. Prior studies have demonstrated the feasibility of using NLP techniques to identify mentions of sexual trauma in the EHR17, and have examined racial/ethnic and sex differences in patterns of sexual trauma disclosure14. To our knowledge, this is a first study to explore regional variations in sexual trauma documentation.
The VHA is an optimum setting to explore geographic variations in sexual trauma documentation because of the size of the healthcare system, and because patient histories of sexual trauma have been prioritized for documentation. Indeed, VHA is the largest integrated healthcare system in the United States, serving nearly 6 million unique patients every year through 152 medical centers and nearly 1000 outpatient clinics. Since 2004, VHA has implemented universal screening of all Veterans seeking care in its medical facilities for exposure to sexual trauma during military service (military sexual trauma, MST). Under this model, many patients with a history of sexual trauma have received access to specialized care designed to mitigate adverse outcomes associated with sexual harassment and assault. Eligible Veterans also receive treatment for experiences of sexual trauma occurring outside of military service (during childhood or adulthood). Information learned through an examination of regional variations in VHA medical records may apply to other healthcare systems in the United States, and to international health care settings where sexual trauma is prevalent19.
Methods
Setting and Study Population
This study examined documentation of sexual trauma concepts from a national, random sample of Veterans who served in recent conflicts as part of Operations Enduring Freedom/Iraqi Freedom/New Dawn (OEF/OIF/OND) and who received care in VHA medical facilities. We selected a random sample of 10,000 male and 10,000 female OEF/OIF/OND Veterans by linking a Department of Defense (DoD) roster of service members who served in the recent conflicts with administrative data stored in the VHA corporate data warehouse. Data were accessed through the VHA Informatics Computing Infrastructure (VINCI), a secure research portal20. Veterans were included in this study if they received care in VHA medical facilities, and had a valid MST screen result between October 2009 and October 2014. For each patient, we analyzed 12 months of electronic medical notes that are available in the VHA corporate data warehouse for use in research10. All study procedures were approved by the University of Utah Institutional Review Board and the Research Review Committee of the VA Salt Lake City Health Care System.
Procedures
We downloaded all electronic medical notes associated with outpatient visits for the study cohort in the 12 months following an initial MST screen result. We processed the 12-month set of electronic medical notes using an NLP pipeline, V3NP, that was developed to extract all sexual trauma concepts such as adverse childhood experiences and mentions of sexual trauma in adulthood (including trauma that occurred during military service) from VHA electronic medical records17. The pipeline was built on the APACHE-Unstructured Information Management applications (UIMA) framework21. In brief, the pipeline parses the electronic medical note into its component parts such as sections, content headings, lists, sentences, lines, and finally individual concepts (tokens). The individual tokens were then compared to a look-up dictionary of sexual trauma terms. The dictionary was developed for this pipeline using terms from standard vocabularies and supplemented with expert opinion after review of a set of VHA electronic medical records as there was lack of complete coverage of sexual trauma concepts in the UMLS Metathesaurus and SNOMED-CT. An important feature of the pipeline was to include lexical variants of terms and to exclude concepts that were negated such as “no evidence of sexual trauma”. Thus, the goal of the pipeline was to extract “positively asserted” concepts. All concepts related to sexual trauma extracted by the NLP pipeline as positively asserted (with clinical text surrounding the extracted concept to provide context, “snippets”) were reviewed by a set of trained human reviewers for true positive mentions. As reported elsewhere, the overall positive predictive value for identifying sexual trauma at the individual concept level was 0.9017. The trained reviewers also determined the type of sexual trauma described in each mention: 1) childhood sexual trauma, 2) adult sexual trauma, 3) military sexual trauma (MST), 4) unspecified sexual trauma, or 5) no sexual trauma (i.e., false positive).
At the document level, we created a binary variable noting any evidence of sexual trauma (yes/no), and a categorical variable with specific type(s) of sexual trauma recorded: adult only, childhood only, MST only, unpsecified only, or multiple types of trauma. Documents that only included false positive mentions of sexual trauma, and those documents lacking true positive mentions were coded as having no evidence of sexual trauma.
Geographic Variables
All clinical notes were affiliated with a VHA medical center or outpatient clinic where the patient received care. We extracted geocoded attributes of each facility from VHA administrative records. Facilities are coded as urban, rural, highly rural, or insular, based on rural-urban commuting area (RUCA) definitions using the standard VHA classification that has been validated for Veteran research22, 23. We coded clinical notes as urban or non-urban, based on the RUCA classification (RUCA <=1.1 is urban, all other values are non-urban) of the facility where the note was written.
VHA facilities are also categorized into one of five geographic regions of the United States, based on aggregated Veterans Affairs Integrated Service Network (VISN) catchment areas: Pacific, Continental, Midwest, Southeast, and North Atlantic regions (Figure 1). We assigned clinical notes to one of the five geographic regions, based on the faclity where the note was written.
Figure 1:
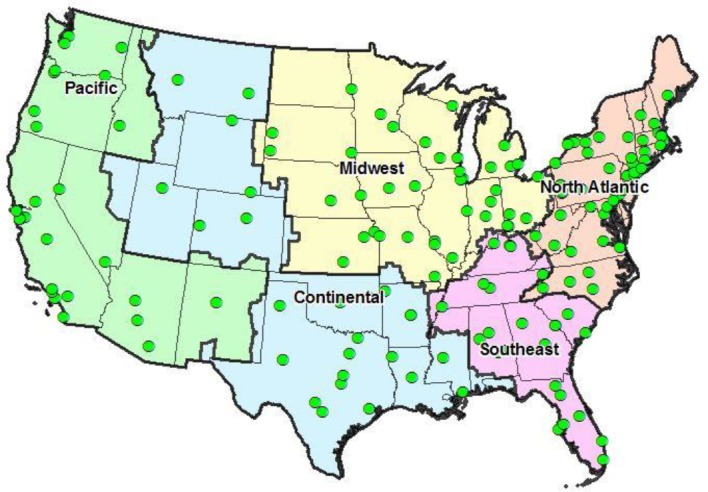
Five United States geographic regions. Region boundaries correspond to Veterans Affairs Integrated Service Network (VISN) catchment areas. Green circles indicate Veterans Affairs medical center locations.
Statistical Analyses
We used cross-tabulations to characterize regional variations in notes containing sexual trauma documentation (yes/no), the type of notes mentioning sexual trauma, and types of sexual trauma mentions (e.g., military, adult, childhood, etc). We used logistic regressions to estimate regional differences in sexual trauma documentation (yes/no) and multinomial logistic regressions to estimate regional differences in the types of notes mentioning sexual trauma. All models controlled for patient sex, and used a robust standard error specification to account for the clustering of notes within VHA patients. Wald joint tests of significance were used to simultaneously test region coefficents.
Results
Of 20,000 male and female VHA outpatients, 14,831 had at least one medical note during the study period. A total of 362,559 notes were processed from the study cohort using the NLP pipeline; and 4,178 of 4,937 (84.6%) notes contained true positive mentions of sexual trauma concepts. The NLP precision was slightly better in the Midwest region (note level positive predictive value [PPV]=88.4%), compared to the other United States regions: Pacific PPV=84.4%, Continental PPV=84.7%, Southeast PPV=82.8%, and North Atlantic PPV=83.0%. Regardless of sexual trauma mentions, the majority of all notes were observed in urban versus rural VHA facilities (n=324,053, 91.8%).
As shown in Table 1, there were regional variations in the documentation of sexual trauma (Wald X2 = 59.94, p=<0.001). The Southeast region had the largest average number of notes per patient, but a relatively low frequency of notes containing sexual trauma mentions. Only 15.6% of notes continaining sexual trauma were in the Southeast region, compared to 20.4% of notes lacking sexual trauma mentions.
Table 1:
Regional variation in number of notes, by presence of sexual trauma concept
| Notes sexual mention | lacking trauma | Notes sexual mentions | containing trauma | Number of notes per patient | ||
| Geographic region | N | % | N | % | Mean | SD |
| Pacific | 58,775 | 16.4 | 745 | 17.8 | 22.0 | 55.5 |
| Continental | 73,045 | 20.4 | 1,005 | 24.1 | 24.5 | 50.1 |
| Midwest | 68,731 | 19.2 | 810 | 19.4 | 23.4 | 50.7 |
| Southeast | 72,933 | 20.4 | 651 | 15.6 | 27.8 | 57.3 |
| North Atlantic | 84,886 | 23.7 | 967 | 23.2 | 24.8 | 50.9 |
Notes Containing Sexual Trauma Concepts
Notes lacking sexual trauma concepts included 1,995 unique note titles, whereas notes containing sexual trauma concepts only included 365 unique titles. As shown in Table 2, notes lacking sexual trauma concepts were often addendums and administrative in nature; nursing, primary care, and mental health disciplines were also represented. In contrast to other notes, most of the notes containing sexual trauma mentions were mental health in nature. Smaller numbers of notes with sexual trauma mentions related to primary care or to VHA compensation and pension (C&P) examinations.
Table 2:
Top 10 most frequent note titles, by presence of sexual trauma concept
| Titles of notes lacking sexual trauma concepts | N | % | Titles of notes containing sexual trauma concepts | N | % |
| Addendum | 69,941 | 19.5 | Mental health note | 417 | 10.0 |
| Administrative note | 10,652 | 3.0 | Psychology note | 254 | 6.1 |
| Nursing note | 10,111 | 2.8 | Psychiatry note | 234 | 5.6 |
| Mental health note | 8,764 | 2.5 | Addendum | 144 | 3.5 |
| Primary care note | 8,316 | 2.3 | Mental health outpatient note | 137 | 3.3 |
| Telephone encounter note | 7,985 | 2.2 | Mental health medication mgmt. | 122 | 2.9 |
| No show note | 5,363 | 1.5 | Group counseling note | 118 | 2.8 |
| Primary care nursing note | 5,074 | 1.4 | C & P examination note | 117 | 2.8 |
| Primary care telephone note | 4,637 | 1.3 | Social work note | 112 | 2.7 |
| Medication management note | 4,441 | 1.2 | Primary care note | 75 | 1.8 |
Classification of Note Titles
We reviewed the 365 unique note titles names, and combined note titles with similar names into groups. The note titles broadly fell into six main categories: primary care, mental health, social services, medical or surgical services, emergency or inpatient services, C&P exams, and other. The other category included labs, radiology, person-specific notes (e.g., physician, attending), addendums, and miscellaneous (e.g., no-show note, administrative note).
In notes lacking sexual trauma concepts (Figure 2a), the proportion of primary care and mental health notes were similar across regions of the United States. Of all geographic regions, facilities located in the Pacific states had a higher percentage of mental health notes than the other U.S. regions (15.1% vs. 12.1%-13.8% in other regions), and a smaller percentage of primary care notes (17.4% versus 19.2%-20.8% in other regions).
Figure 2a:
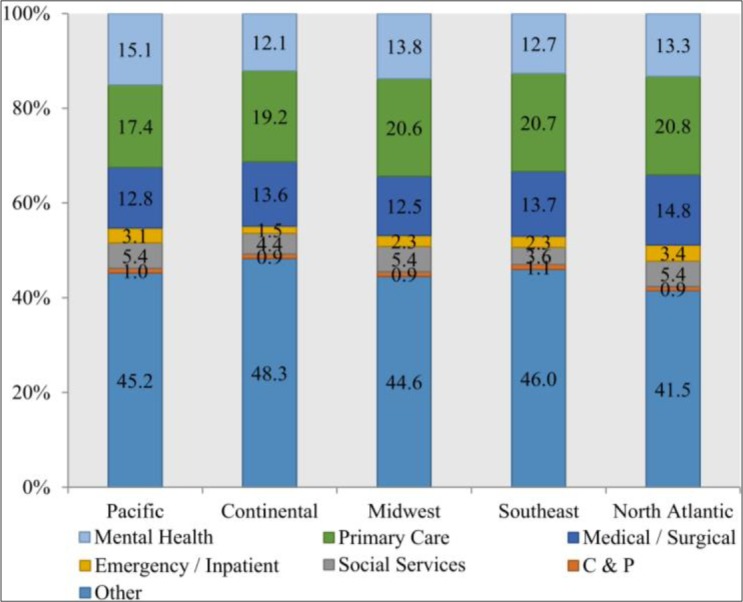
Types of notes lacking sexual trauma mentions, by geographic region
In contrast to notes lacking sexual trauma mentions, we observed greater regional variation in notes containing sexual trauma concepts (Figure 2b; Wald X2 = 176.99, p=<0.001). VHA facilities located in Pacific states had a greater percentage of primary care notes (28.3%), compared to facilities in the Southeast (13.1%) and other regions (17.3%-20.0%). Facilities in the North Atlantic had a higher percentage of emergency or inpatient service notes, compared to facilities in other regions (4.5% vs. 1.8%-3.7% in other regions).
Figure 2b:
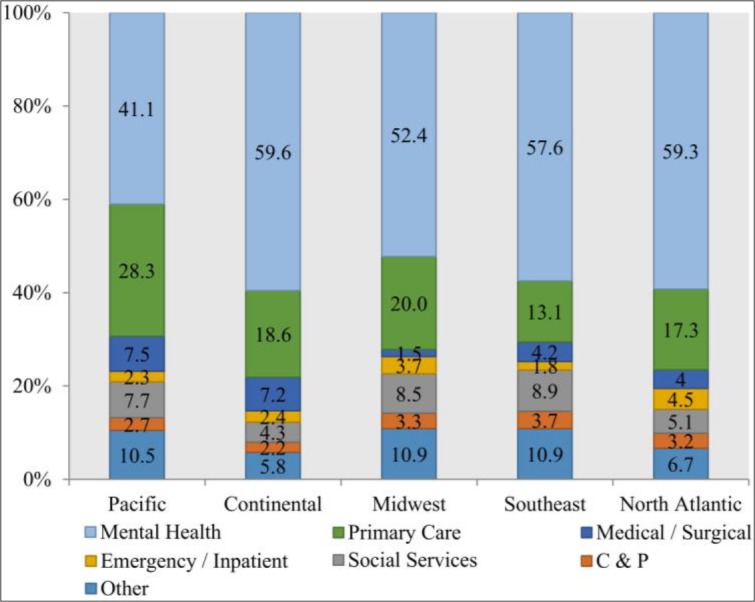
Types of notes containing sexual trauma concepts, by geographic region
Region and Sex Variations in Sexual Trauma Mentions
We explored whether the patterns of regional differences in notes with sexual trauma concepts were related to patient sex. Most (94%) of all notes containing sexual trauma concepts belonged to female patients. Thus, the regional distribution of note titles among female Veterans was similar to the total distribution (males and females combined) presented in Figure 2b above. Among female patients, for instance, VHA facilities located in Pacific states were more likely than facilities in other regions to document sexual trauma in primary care (23.8%). VHA facilities in the Southeast were less likely than facilities in other United States regions to document sexual trauma in primary care (10.1%; data not shown). VHA facilities in Pacific states had lower percentages of sexual trauma notes from mental health (39.9%) compared to facilities in other regions (50.3%-60.3%; data not shown).
A different pattern was observed in the notes of male patients (n=248) than in notes of females. As shown in Figure 3, VHA facilities in the Continental U.S. region were more likely to document sexual trauma for male patients in primary care (19.6%), compared to facilities in other U.S. regions (7.7%-9.8%). VHA facilities in the Midwest and Atlantic regions were more likely than facilities in other regions to document sexual trauma concepts for male patients in mental health note types (75.4% and 70.7% versus 38.3%-59.1%). More than in other geographic regions, sexual trauma concepts in Southeast facilities were documented in social service (14.9%), medical/specialty (12.8%), and other (14.9%) notes. Tests of regional variation in the types of notes mentioning sexual trauma were statistically significant in the models for females and males (both Wald test p- values <0.001).
Figure 3:
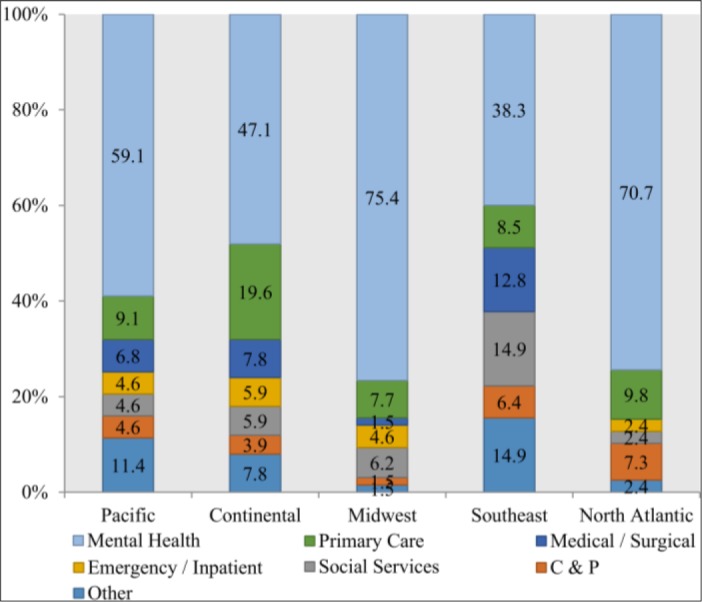
Types of notes containing sexual trauma concepts for male patients, by geographic region
Types of Sexual Trauma Concepts: Geographic Variations by Sex
We also explored the types of sexual trauma concepts picked up by the NLP pipeline: military sexual trauma, sexual trauma occurring in adulthood (outside of the military), childhood sexual trauma, and other sexual trauma incidents where circumstances were not specified. The overall test of regional variations in type of sexual trauma recorded was statistically signficant (Wald X2 = 99.95, p<0.001), with distinct regional patterns in the type of sexual trauma documented for female versus male patients.
As shown in Figure 4a, sexual trauma notes for female patients in the Pacific states often referenced adult sexual trauma (43.2%), with relatively smaller percentages of sexual trauma concepts related to military service (34.1) or childhood (11.4%); 9.1% of sexual trauma notes in Pacific states referenced more than one type of trauma. For female patients, sexual trauma notes in the Continental and Midwest regions had the greatest percentage of childhood trauma references (27.5% and 27.7%, respectively); while sexual trauma notes in the Southeast and North Atlantic regions primarily related to military sexual trauma only (71.7% and 63.4%, respectively).
Figure 4a:
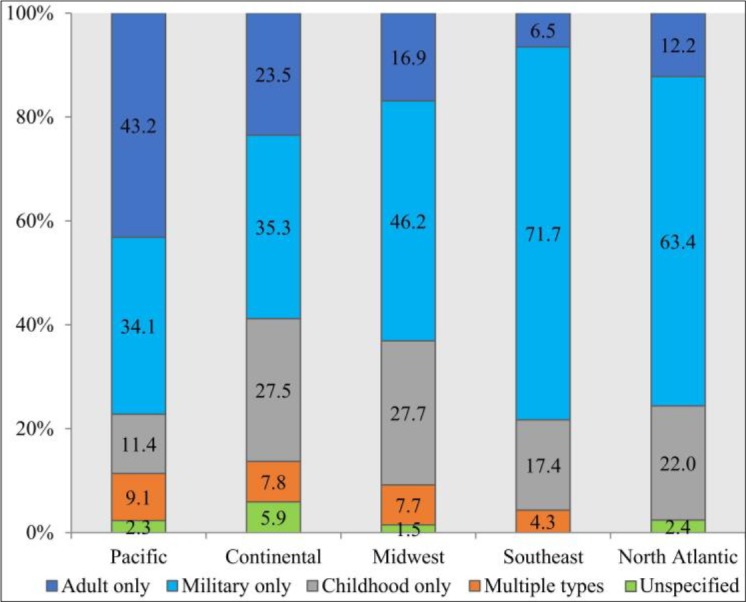
Types of sexual trauma concept documented in notes of female patients, by geographic region
For male patients, the majority of sexual trauma notes referenced military sexual trauma only (56.0%-70.2% across regions; Figure 4b) or multiple types of trauma (9.6%-21.6% across domains). Regardless of region, male patients’ sexual trauma notes rarely referenced non-military sexual trauma.
Figure 4b:
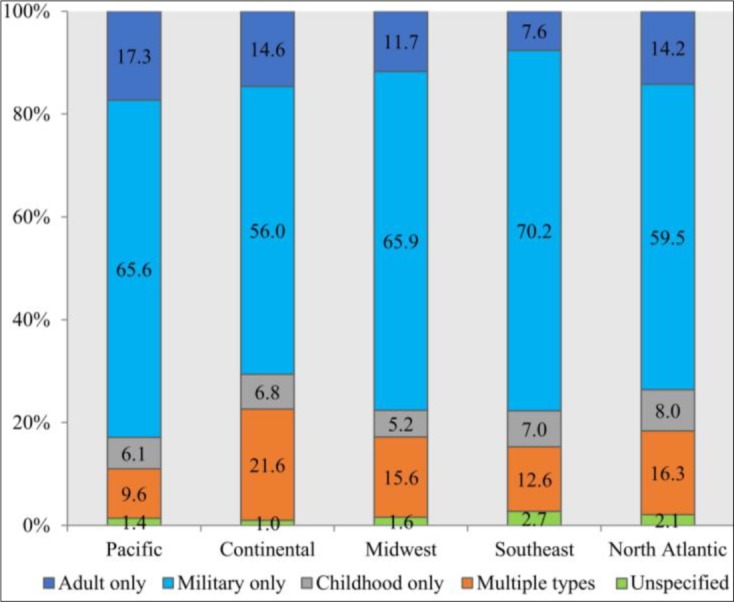
Types of sexual trauma concept documented in notes of female patients,by geographic region
Discussion
Patient histories of sexual trauma have important implications for patient and health system outcomes, but documentation of this sensitive and personal information lacks standardization. If sexual trauma information is not recorded at all, sexual trauma survivors may have more difficulty accessing high quality, trauma-informed care. In addition, lack of provider awareness of trauma histories could inadvertently lead to poor care delivery and re-traumatization of patients.
We sought to examine regional variations in the extent and nature of documentation of sexual trauma experiences in the VHA’s EHR. While there was relatively small geographic variation in the types of notes used to document non-sexual trauma phenomena, documentation of sexual trauma histories varied across the major United States regions. In the Pacific states, we observed relatively greater proportions of primary care notes and relatively smaller percentages of mental health notes, compared to the other geographic regions. We also found more variation in the types of sexual trauma documented in Pacifc states, compared to other United States regions, particularly for female patients. It may be the case that primary care providers in Pacific states have received more training in eliciting sexual trauma histories, or experience less hesitation in recording this information in the EHR.
Our finding of unique patterns of results in male versus female patients highlights some areas where sexual trauma may not be reported due to fear of stigma. Our finding of relatively few mental health notes for male patients in the Southeast region, compared to other United States regions, suggests there may be increased barriers to seeking mental health care or to disclosing sexual trauma in the course of mental health treatment for men in the Southeast. In the Southeast region, we also observed relatively small percentages of sexual trauma notes in primary care and relatively small percentages of non-military types of sexual trauma documented, compared to other United States regions. Importantly, the performance of the NLP pipleline was similar across geographic regions. While the current study was not designed to explain reasons for lack of documentation, our results suggest that cultural factors may be at play. For example, the Southeast is thought to be more culturally conservative than other United States regions, and this could explain relatively low rates of disclosure and documentation of sexual trauma in the clinical setting. Future research is warranted to elucidate how patients and providers navigate discussions of sexual trauma in diverse clincial settings in the Southeast and in other United States regions.
We note study limitations. First, this study did not systematically evaluate false negative captures of military sexual trauma. Additonal work is evaluate to determine the performance of the NLP pipeline overall, and across diverse cultural contexts. Second, the study sample included small numbers of notes for male patients in each geographic region, which precluded multivariable analyses that might help to explain regional patterns. Specifically, the study did not examine patient, provider, or health system factors that may contribute to variations in sexual trauma documentation. It is possible that some of the regional variations observed in the current study could be due to patient differences in sexual trauma exposure and help-seeking or to patients requesting that their trauma not be documented. Despite limitations, this descriptive analysis illustrates the utility of NLP methods to detect systematic differences in the documentation of sensitive and personal information in the EHR. Our future work will consider provider characteristics (e.g. age, gender) in combination with patient factors to better understand the variations in sexual trauma documentation observed here.
Conclusions
While there is increasing public health attention on sexual harassment and assault, little is known about how sexual trauma histories are documented and managed in integrated health care systems. To fill this knowledge gap, this study examined the clinical context of sexual trauma documentation, and the nature of traumas reported. We found variations in documentation that are unlikely to be explained by differential exposures alone. Standardized mechanisms of collecting and documenting sexual trauma histories are needed to ensure Veterans’ access to high quality, trauma-informed care. Provider training designed to increase awareness of the cultural barriers and challenges of eliciting and documenting sexual trauma in clinical notes may be an important first step.
Acknowledgements
Funding for this project was provided by grant IIR 12-084 (PI: A.V.G.), and VA Center of Innovation Award #I50HX001240 from the Health Services Research and Development of the Office of Research and Development of the US Department of Veterans Affairs. Dr. Jones is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR002538 and KL2TR002539, and the VA Office of Academic Affiliations Post-Doctoral Fellowship in Medical Informatics. The views expressed in this article are those of the authors and do not necessarily represent the position or policy of the U.S. Department of Veterans Affairs, the National Institutes of Health, or the U.S. government.
Figures & Table
References
- 1.Tjaden PG, Thoennes N. Washington, D.C.: U.S. Department of Justice, Office of Justice Programs, National Insitute of Justice; 2000. National Institute of Justice (U.S.), Centers for Disease Control and Prevention (U.S.). Full report of the prevalence, incidence, and consequences of violence against female: Findings from the national violence against female survey. [Google Scholar]
- 2.Ahrens CE, Stansell J, Jennings A. To tell or not to tell: The impact of disclosure on sexual assault survivors’ recovery. Violence Vict. 2010;25:631–48. doi: 10.1891/0886-6708.25.5.631. [DOI] [PubMed] [Google Scholar]
- 3.Hoyt T, Klosterman Rielage J, Williams LF. Military sexual trauma in male: A review of reported rates. J Trauma Dissociation. 2011;12:244–60. doi: 10.1080/15299732.2011.542612. [DOI] [PubMed] [Google Scholar]
- 4.Burns B, Grindlay K, Holt K, Manski R, Grossman D. Military sexual trauma among us servicewomen during deployment: A qualitative study. Am J Public Health. 2014;104:345–9. doi: 10.2105/AJPH.2013.301576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Department of Defense. In: Department of Defense. Washington DC: 2016. Department of defense annual report on sexual assault in the military fiscal year 2016. [Google Scholar]
- 6.Gilmore AK, Brignone E, Painter JM, Lehavot K, Fargo J, Suo Y, et al. Military sexual trauma and co- occurring posttraumatic stress disorder, depressive disorders, and substance use disorders among returning afghanistan and iraq veterans. Womens Health Issues 2016. 26:546–54. doi: 10.1016/j.whi.2016.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pavao J, Turchik JA, Hyun JK, Karpenko J, Saweikis M, McCutcheon S, et al. Military sexual trauma among homeless veterans. J Gen Intern Med 2013. (28 Suppl 2):S536–41. doi: 10.1007/s11606-013-2341-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Suris A, Lind L Military sexual trauma. A review of prevalence and associated health consequences in veterans. Trauma Violence Abuse 2008. 9:250–69. doi: 10.1177/1524838008324419. [DOI] [PubMed] [Google Scholar]
- 9.Backhaus A, Gholizadeh S, Godfrey KM, Pittman J, Afari N The many wounds of war. The association of service-related and clinical characteristics with problems with the law in iraq and afghanistan veterans. Int J Law Psychiatry 2016. 49:205–213. doi: 10.1016/j.ijlp.2016.10.007. [DOI] [PubMed] [Google Scholar]
- 10.Brignone E, Gundlapalli AV, Blais RK, Carter ME, Suo Y, Samore MH, et al. Differential risk for homelessness among us male and female veterans with a positive screen for military sexual trauma. JAMA Psychiatry 2016. 73:582–9. doi: 10.1001/jamapsychiatry.2016.0101. [DOI] [PubMed] [Google Scholar]
- 11.Kimerling R, Makin-Byrd K, Louzon S, Ignacio RV, McCarthy JF. Military sexual trauma and suicide mortality. Am J Prev Med 2016. 50:684–91. doi: 10.1016/j.amepre.2015.10.019. [DOI] [PubMed] [Google Scholar]
- 12.Clark C, Classen C, Fourt A, Shetty M Treating the trauma survivor. New York, NY: Routledge: Taylor & Francis Group; 2015. An essential guide to trauma- informed care. [Google Scholar]
- 13.Blais RK, Brignone E, Fargo JD, Galbreath NW, Gundlapalli AV. Assailant identity and self-reported nondisclosure of military sexual trauma in partnered female veterans. Psychol Trauma 2018. 10:470–474. doi: 10.1037/tra0000320. [DOI] [PubMed] [Google Scholar]
- 14.Gundlapalli AV, Jones AL, Redd A, Divita G, Brignone E, Pettey WB, et al. Med Care In Press; Combining natural language processing of electronic medical notes with administrative data to determine racial/ethnic differences in disclosure and documentation of military sexual trauma in veterans. [DOI] [PubMed] [Google Scholar]
- 15.Reeves E. A synthesis of the literature on trauma-informed care. Issues Ment Health Nurs 2015. 36:698–709. doi: 10.3109/01612840.2015.1025319. [DOI] [PubMed] [Google Scholar]
- 16.Sohn S, Wi CI, Juhn YJ, Liu H. Analysis of clinical variations in asthma care documented in electronic health records between staff and resident physicians. Stud Health Technol Inform 2017. 245:1170–1174. [PMC free article] [PubMed] [Google Scholar]
- 17.Divita G, Brignone E, Carter ME, Suo Y, Blais RK, Samore MH, et al. Extracting sexual trauma mentions from electronic medical notes using natural language processing. Stud Health Technol Inform. 2017;245:351–355. [PubMed] [Google Scholar]
- 18.George LK, Winfield I, Blazer DG. Sociocultural factors in sexual assault: Comparison of two representative samples of female. J Soc Issues. 2002;48:105–125. [Google Scholar]
- 19.Stoltenborgh M, van IJzendoorn MH, Euser EM, Bakermans-Kranenburg MJ. A global perspective on child sexual abuse: Meta-analysis of prevalence around the world. Child Maltreatment. 2011;16((2)):79–101. doi: 10.1177/1077559511403920. [DOI] [PubMed] [Google Scholar]
- 20.US Department of Veterans Affairs. Washington DC: US Department of Veterans Affairs; 2016. In VA Informatics and Computing Infrastructure (VINCI) [Google Scholar]
- 21.Divita G, Carter ME, Tran LT, Redd D, Zeng QT, Duvall S, et al. Vol. 4. EGEMS (Wash DC): 2016. V3nlp framework: Tools to build applications for extracting concepts from clinical text; p. 1228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.West AN, Lee RE, Shambaugh-Miller MD, Bair BD, Mueller KJ, Lilly RS, et al. Defining “rural” for veterans’ health care planning. J Rural Health. 2010;26:301–9. doi: 10.1111/j.1748-0361.2010.00298.x. [DOI] [PubMed] [Google Scholar]
- 23.West AN, Weeks WB, Charlton ME. Differences among states in rural veterans’ use of VHA and non-VHA hospitals. J Rural Health. 2017;33((1)):32–40. doi: 10.1111/jrh.12152. [DOI] [PubMed] [Google Scholar]