

Abstract
Ibrutinib has shown to have better efficacy than standard chemoimmunotherapy in del17 positive chronic lymphocytic leukemia (CLL) patients; however its role in del17 negative patients is less clear. We aim to evaluate the efficacy of ibrutinib-based regimens in CLL. Seven databases were searched in accordance with PRISMA statement guidelines using the following keywords: chronic lymphocytic leukemia, CLL, Bruton tyrosine kinase inhibitor, BTK inhibitor, ibrutinib, and PCI-32765. Data from only prospective clinical trials was included. In a phase 3 trial (n = 136), the overall response rate (ORR) with ibrutinib was 92% whereas 18% patients had a complete response (CR). Progression free survival (PFS) and overall survival (OS) at 2 years were 89% and 95% respectively. Phase 3 trial (n = 195) with single agent ibrutinib showed ORR of 63%. PFS at 6 months and OS at 12 months were 88% and 90% respectively. In a phase 2 trial of relapsed and/or refractory (R/R) or high risk treatment naive (TN) patients, combination of ibrutinib and rituximab (n = 104) achieved an ORR of 100% (CR 28%) as compared to ORR 98% (CR 21%) with ibrutinib monotherapy (n = 102) with no significant difference in PFS. Combination of ibrutinib and ublituximab (n = 64) had an ORR of 78% (CR 7%) in a phase 3 study. In del17p negative R/R patients, combination of bendamustine/rituximab (BR) and ibrutinib (n = 289) achieved an ORR of 83% (CR/CRi 10%) and the 18 month PFS was 79%. In a phase 2 trial treated with ibrutinib (n = 145), patients with del17p R/R disease achieved an ORR of 64% and the 24 month PFS and OS was 63% and 75% respectively. In TN del17p patients (n = 35), ORR was 97% (CR-0) and the 24 month PFS and OS were 82% and 84% respectively with single agent ibrutinib. Ibrutinib is the treatment of choice for patients with del17p mutation and has good efficacy in RR/TN patients without del17p mutation. Ibrutinib is being evaluated in combination with rituximab for del17p mutations. Future prospects include combination of ibrutinib with frontline chemotherapy and other novel agents for TN and RR del17p negative patients.
Keywords: Chronic lymphocytic leukemia, Bruton tyrosine kinase inhibitor, BTK inhibitor, Ibrutinib, PCI-32765, Efficacy, Relapse
Introduction
Chronic lymphocytic leukemia (CLL) is the most common leukemia in western hemisphere with an age adjusted incidence of 5 per 100,000. Most patients are diagnosed at a median age of 70 years [1, 2]. It has an indolent course and usually presents with signs and symptoms of fatigue, weight loss, low grade fever, night sweats and lymphadenopathy. Its diagnosis requires ≥ 5,000/µL monoclonal B lymphocytes for at least 3 months and confirmation of mono-clonality of B lymphocytes by flow cytometry. Leukemic cells in CLL co-express both, B cell and T cell antigens (CD19, CD20, CD23 and CD5).
According to the updated guidelines (2018) from the International Workshop for Chronic Lymphocytic Leukemia (iwCLL), most patients with early stage asymptomatic disease can be monitored without treatment. Indications to initiate chemotherapy includes anemia, thrombocytopenia, massive (> 6 cm) symptomatic splenomegaly, lymphadenopathy (10 cm in the longest dimension), lymphocyte doubling time of less than 6 months or persistent symptoms associated with CLL (unintentional weight loss, night sweats) [3, 4]. The choice of therapy depends upon age, functional status, creatinine clearance, cytogenetics and associated comorbidities. Current standard of care for patients younger than 65 years of age is a combination of fludarabine, cyclophosphamide and rituximab (FCR); whereas patients having kidney dysfunction or who are older than 65 years of age are best treated with a combination of bendamustine and rituximab [5]. With currently available treatment its prognosis is very promising having a 5-year survival rate of 84% [6]. Patients harboring del17p/TP53 aberrations exhibit poor response and survival with the frontline chemoimmunotherapy [7, 8].
With advent of novel agents, such as ibrutinib, idelalisib, dasatinib, venetoclax, ofatumumab, obinutuzumab, the landscape of treatment of CLL is changing [9]. Ibrutinib is an orally administered drug that acts on Bruton tyrosine kinase (BTK) pathway which is aberrantly activated in CLL [10, 11]. In a phase 1 study by Advani et al (2013), ibrutinib was well tolerated and shown to have substantial activity across various B cell malignancies including follicular lymphoma, CLL/SLL (small lymphocytic leukemia), diffuse large B cell lymphoma and mantle cell lymphoma. Out of 16 patients with relapsed and/or refractory (R/R) CLL, 11 patients had an overall response (OR) i.e. complete response (CR) in two patients whereas partial response (PR) in nine patients [12]. Subsequently, on the basis of improvement in the overall response rate (ORR) in the RESONATE trial and phase 1/2b trial of ibrutinib in relapsed/refractory patients (Byrd JC et al), ibrutinib was given an expedited approval by Food and Drug Administration (FDA) for treatment of patients with R/R disease and patients with del17p mutation [13, 14].
The standard of care for patients with del17p mutation is ibrutinib, but it is less clear if the combination regimen of anti CD20 monoclonal antibodies like rituximab, or ublituximab and ibrutinib would improve survival with an acceptable side effect profile. Ibrutinib was initially approved for only del17p mutation and patients with R/R disease. More recently in addition to other novel agents its use has been evaluated in many ongoing phase clinical trials of treatment naive (TN) CLL patients. Unlike del17p mutation, treatment implications for other prognostic factors such as del11q mutation, immunoglobulin heavy chain variable (IGHV) mutation, RAI stage etc. are less clear.
Literature Search
A literature review was performed using methods specified in the PRISMA statement for reporting systematic reviews. Controlled vocabulary search terms (MeSH and Emtree), as well as keywords, were used to search the following seven databases for clinical trials that examined the efficacy of ibrutinib-based regimen in CLL: Pub Med/Medline, Elsevier/Embase, Elsevier/Scopus, Wiley/Cochrane Library, Thomas Reuters/Web of Science, EBSCO/CINAHL, and ClinicalTrials.gov. All databases were searched from the date of their inception to the date literature searches were completed on May 5, 2018. Reference lists of, and citations to the articles eventually selected from the database searches, were also screened. Two independent reviewers (SM, MS) initially screened all retrieved titles and abstracts for relevance. The same protocol was used to screen the full text of articles initially selected. Disagreements were resolved by consensus. Inclusion criteria for our review were prospective clinical trials including CLL/SLL patients who received ibrutinib either as monotherapy or as combination therapy. Single arm clinical trials containing ibrutinib either as monotherapy or part of combination therapy were also included in addition to the randomized controlled trials. Ongoing trials with preliminary data available as well as unpublished trials presented at the national oncology and hematology conferences like American Society of Hematology (ASH) and American Society of Clinical Oncology (ASCO) were also included. We included phase 1 studies with data available for efficacy for at least 10 patients in addition to the phase 2 and 3 studies. Case studies, letters, opinions, reviews, including systematic reviews and meta-analyses were excluded as were articles not in English. To assess for risk of bias and quality, we used Newcastle-Ottawa scale for non-randomized studies. One author (MS) independently extracted the data, which was subsequently examined by a second author (SM).
The following variables were analyzed: author, year, study design, number of subjects, regimen used (ibrutinib and comparing regimen), dosage, age and patient characteristics, high risk cytogenetic features, median follow-up response rate, progression free survival and overall survival. The primary outcome for our review was quantitative assessment of response measurement in ORR, progression free survival (PFS) and overall survival (OS). Adverse events and side effects were not the focus of our analysis.
Literature Review
We identified 3,809 medical records after initial database search, and 2,365 medical records were further screened after removing duplicates. We assessed 38 full length articles for eligibility, and 16 prospective clinical trials were included in the final analysis (Fig. 1). An aggregate of 1,528 CLL patients was part of our analysis including 308 patients who were TN and 1,014 patients who were R/R. Table 1 ([10, 13, 15-25]) and Supplementary Table 1 (www.thejh.org) show the summary of all included prospective clinical trials evaluating response rate, progression free survival and overall survival of ibrutinib-based regimen in CLL.
Figure 1.
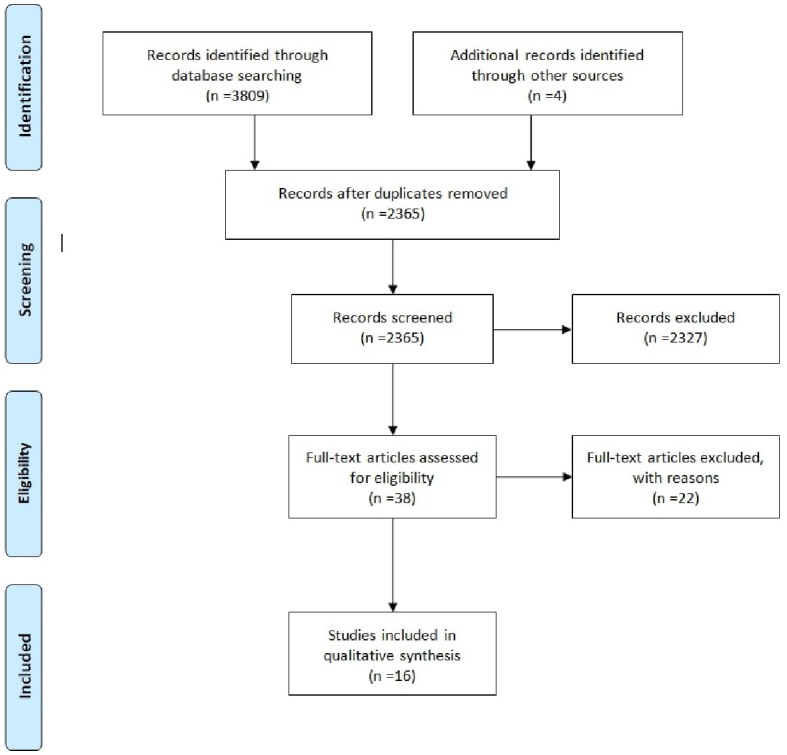
PRSIMA Statement guidelines were followed for identification, screening, eligibility and inclusion of articles.
Table 1. Summary of Prospective Clinical Trials Evaluating Role of Ibrutinib-Based Regimen in CLL.
| Trial | Regimen | Pts. (n) | Age (med) | Prior therapies (med) | Med f/u (M) | High risk factors n (%) | ORR (%) | CR (%) | PR (%) | PFS % (M) | OS % (M) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| O’Brien et al [15] 2018 (5 year f/u) (1b/2) | Ibr | 31 | 71 | TN | 61.5 | Del17p | 6 | 87 | 29 | 92 (61) | 92 (61) | |
| Del11q | 3 | |||||||||||
| 67 | 64 | 4 | 61.5 | Del17p | 34 | 89 | 44 (61) | 60 (61) | ||||
| Del11q | 35 | |||||||||||
| Burger JA et al [21] 2014 (phase 2) | Ibr+ R | 40 | 63.2 | 2 | 16.8 | Del17p | 50 | 95 | 8 | 87 | 78 (18) | 84 (18) |
| Del11q | 32.5 | |||||||||||
| Byrd JC et al [13] 2014 (phase 3) | Ibr | 195 | 67 | 3 | 9.4 | Del17p | 32 | 63 | 0 | 63 | 88 (6) | 90 (12) |
| Del11q | 32 | |||||||||||
| Farooqui et al [16] 2014 (phase 2) | Ibr | 35 | 62 | TN | 15 | Del17p | 100 | 97 | 0 | 97 | 82 (24) | 84 (24) |
| Del11q | - | |||||||||||
| 16 | 62 | R/R | 26 | Del17p | 100 | 80 | 0 | 80 | 82 (24) | 74 (24) | ||
| Del11q | - | |||||||||||
| Burger JA et al [10] 2015 (phase 3) | Ibr | 136 | 73 | TN | 28.6 | Del17p | 0 | 92 | 18 | - | 89(24) | 95 (24) |
| Del11q | 21 | |||||||||||
| Brown, JR et al [23] 2015 (phase 1b) | Ibr + BR | 30 | 62 | 2 | 15.8 | Del17p | 23.3 | 96.7 | 40 | 56.7 | 86(12) | - |
| Del11q | 33.3 | |||||||||||
| Chanan-Khan et al [22] 2016 (phase 3) | Ibr + BR | 289 | 64 | 2 | 17 | Del17p | 0 | 83 | 10 | 73 | 79 (18) | - |
| Del11q | 30 | |||||||||||
| Susan O’brien et al [24] 2016 (phase 2) | Ibr | 145 | 64 | 2 | 11.5 | Del17p | 100 | 64 | 0 | 64 | 63 (24) | 75 (24) |
| Del11q | 16 | |||||||||||
| JP Sharman et al 2017 [25] (phase 3) | Ibr + Ubl | 64 | 67 | 3 | 12 | Del17p | 64 | 78 | 7 | 71 | - | - |
| Del11q | 36 | |||||||||||
| Ibr | 62 | Del17p | 66 | 45 | 0 | 45 | ||||||
| Del11q | 34 | |||||||||||
| Burger JA et al [20] 2017(phase 2) | Ibr | 102 | 65 | NR | 25.2 | Del17p | 37 | 98 | 21 | 77 | 91.2 (24) | - |
| Ibr + R | 104 | 65 | NR | 22.7 | Del11q | - | 100 | 28 | 72 | 90.4 (24) | - | |
| Jain N et al [17] 2017 (phase 2) | Ibr +FCG | 32 | NR | TN | 5.5 | Del17 | 0 | 100 | 46 | - | - | - |
| Davids MS et al [18] 2017 (phase 2) | Ibr + FCR | 49 | <65 | TN | 21 | Del17p | 9 | 100 | 63 | - | - | |
| Del11q | 26 | - | ||||||||||
| Rogers KA et al [19] 2017 (phase 1b2) | G + Ibr + V | 25 | NR | TN | NR | Del17p | 12 | 96 | 52 | - | - | - |
| Del11q | 20 | |||||||||||
Pts: patients; Ibr: ibrutinib; R: rituximab; BR: bendamustine + rituximab; Ubl: ublituximab; FCG: fludarabine + cyclophosphamide + obinutuzumab; FCR: fludarabine + cyclophosphamide + rituximab; G: obinutuzumab; V: venetoclax; TN: treatment naive; ORR: overall response rate; CR: complete response rate; PR: partial response rate; PFS: progression free survival; OS: overall survival; M: months; med: median.
Role of ibrutinib in TN patients
Ibrutinib in patients over 65
The extended 5-year follow-up of the phase 1/2b study by O’Brien et al (2018) was recently published. The study included 31 TN patients over the age of 65 who were treated at a dose of 420 mg daily. The frequency of high risk cytogenetic abnormalities was as follows: del17p (6%), 11q (3%), unmutated IGHV (48%). Over one-half (55%) patients belonged to either RAI stage 3 or 4 and whereas 19% had bulky disease i.e. > 5 cm lymph nodes. The ORR at the end of 5-year follow-up was 87% with a CR of 29%. Patients had been followed for a median of 61.5 months (0.7 - 72.5). The median PFS was not reached whereas the 5-year PFS was 92%. Three percent of the patients had progressive disease. Median OS was not reached however the 5-year OS was reported to be 92%. When compared to the 3-year follow-up reported for the same study, the CR rate had improved (29% vs. 26%) [15].
Ibrutinib in patients with del17p/TP53 aberrations
In a phase 2 study by Farooqui et al (2014), ibrutinib was evaluated in a trial of 51 patients with del17p and/or TP 53 aberrations (35 TN; 16 R/R). Among the patients who were previously untreated, 97% achieved an OR at a median follow-up time of 26 weeks. Twenty-four-month OS and PFS were 84% and 82% respectively [16].
Ibrutinib vs. chlorambucil in del17p negative patients over the age of 65 (RESONATE 2)
In a phase 3 trial by Burger et al (2015), ibrutinib at 420 mg daily was found superior to chlorambucil (0.5 - 0.8 mg/kg on days 1 and 15 of each cycle, maximum cycles: 12) as a first line regimen. The median age of the 136 patients in the ibrutinib arm was 73 years (65 - 89). Patients with del17p mutation were excluded; however 21% patients had 11q23 mutations and 43% of the patients had unmutated IGHV. Updated results after a prolonged follow-up were reported at the American Society of Hematology (ASH) 2016 annual meeting. Investigator assessed ORR at 28.6 months was 92% (CR 18%). The median PFS/OS were not reached, however the 24-month PFS and OS were 89% and 95% respectively. In comparison, patients treated with chlorambucil achieved an ORR of 34%. Twenty-four-month PFS and OS were 34% and 84% respectively. Of note, 41% of the patients crossed over to ibrutinib arm from chlorambucil but the results were calculated on intention to treat analysis. The hazard ratio for PFS in patients with del11q mutation (n = 54) was 0.03 as compared to 0.23 in patients with negative del11q mutation (n = 197) showing a better response of ibrutinib which was more pronounced in del11q positive patients (lower hazard ratio) [10, 26].
Ibrutinib, fludarabine, cyclophosphamide, obinutuzumab (iFCG) in mutated IGHV
Preliminary results from phase 2 single arm trial by Jain N et al [17] were presented at ASH 2017. Thirty-two TN IGHV patients were treated with ibrutinib, fludarabine, cyclophosphamide, obinutuzumab (IFCG) from cycle 1 to cycle 3. Primary endpoint was considered achieving CR or CR with incomplete blood count recovery (CRi) but minimal residual disease (MRD) negative status.
For patients who had achieved primary end point by the end of cycle 3, only ibrutinib and obinutuzumab were continued from cycle 4 to cycle 6. In the absence of any disease after the cycle 6, only ibrutinib was continued until the cycle 12. If there was evidence of disease at the end of cycle 3 or 6, both ibrutinib and obinutumab were continued until cycle 12. After cycle 3, the response rate was 100% whereas 87% had achieved bone marrow (MRD) negative remission and 44% patients had achieved CR/CRi with undetectable MRD. At the end of cycle 12, out of 19 patients with MRD negative disease, 84% had CR/CRi. All patients remain MRD negative after a median follow-up of 5.5 months after stopping ibrutinib [17].
Ibrutinib, fludarabine, cyclophosphamide, rituximab (iFCR) in patients less than 65 years of age
The phase 2 trial by David et al (2017) included 49 TN patients with adequate organ function and age less than 65 years (median: 55) , who received ibrutinib, fludarabine, cyclophosphamide and rituximab (iFCR). The median follow-up was 12.1 months. Ibrutinib at 420 mg daily was given for 7 days followed by iFCR which was continued for up to six cycles. Patients were continued on ibrutinib for 2 years unless limited by disease progression or toxicity. High risk features included del17p (9%), del11q (26%), unmutated IGHV (57%), ZAP 70 positivity (59%), and TP53 without del17p (6%). Among the 28 patients that underwent re-staging after completing iFCR, the ORR was 100% (CR/CRi 39%, PR 61%). Similarly, among the patients evaluated for bone marrow minimal residual disease, 39% were negative [18].
Obinutuzumab, ibrutinib, venetoclax regimen
In a phase 1b/2 study by Rogers KA et al 2017, 25 patients were treated with a regimen consisting of obinutuzumab, ibrutinib (added during the second cycle) and venetoclax (added during the third cycle) up to 14 cycles. Preliminary results were presented at ASH 2017. Baseline characteristics of these patients included unmutated IGHV (71%), del17p (12%), del11q (20%), del13q (20%). Patients were evaluated after cycle 8 for response which showed an ORR was 96% (CR/CRi 52%, PR 46%). More than half of the patients (58%) had MRD negative disease in both blood and bone marrow [19].
Role of ibrutinib in relapsed/refractory CLL (n = 1,014)
Ibrutinib as a single agent
The phase 1b/2 study by O’Brien et al included 67 R/R CLL patients. The median age was 64 years (37 - 82) and the median prior number of therapies was 4 (1 - 12). Del17p and del11q were present in over one-third of the patients i.e. 34% and 35% respectively. Bulky disease (> 5 cm lymph nodes) and RAI stage 3 or 4 stage was present in 54% and 57% of the patients respectively. Single agent ibrutinib at 420 mg daily achieved an ORR of 89% in patients with R/R disease. The median PFS was 51 months and the estimated 5-year PFS was 44%. Median OS was not reached whereas the 5-year OS was reported to be 60%. In the subgroup analysis, patients with del17p mutation achieved an ORR of 79% whereas the median PFS and OS were 26 months and 57 months respectively. Patients with unmutated IGHV had a higher ORR (90% vs. 81%) but a shorter median PFS (42 months vs. 63 months) and 5-year PFS (39% vs. 53%) [15].
Ibrutinib vs. ofatumumab (RESONATE trial)
In the phase 3 randomized trial by Byrd et al (2014) [13], ibrutinib (420 mg daily) was compared with ofatumumab (300 mg intravenous (IV) on the first week, then 2,000 mg IV every week for 7 weeks, then every fourth week for 16 weeks). The prior median number of treatments in the ibrutinib arm (n = 195) was 3 (range 1 - 12) and in the ofatumumab arm (n = 196) it was 2 (range 1 - 13). Patients were followed for a median of 9.4 months. Median age was 67 years in both treatment arms.
High risk features were comparable between ibrutinib arm vs. ofatumumab (del17p 32% vs. 33%; del11q 32% vs. 30%; B2 macroglobulin > 3.5 mg/L 78% vs. 74%; baseline cytopenia 64% vs. 63%, bulky disease i.e. > 5cm lymph nodes 64% vs. 52% respectively) respectively.
ORR in patients treated with ibrutinib (independent assessment) was 63% (PR 43%, partial response with lymphocytosis 20%). Progressive disease (PD) was present in 3% whereas 32% of the patients had stable disease (SD). The investigator assessed that ORR in the ibrutinib arm was 85% (CR 2%; PR 83%), SD in 11% and PD in 1%. The investigator assessed that ORR in the ofatumumab arm was 24% (CR 1%, PR 23%), SD was 54%, and PD was 14%. At the median follow-up of 9.4 months, median PFS for ibrutinib had not reached, whereas it was 8.1 for ofatumumab. PFS at 6 months was 88% as compared to 65% with ofatumumab. OS at 12 months was 90% in ibrutinib arm, ofatumumab 81%. In patients with del17p, ibrutinib had a higher PFS than ofatumumab at 6 months (83% vs. 49%).
In a subgroup analysis comparing PFS in del11q positive patients (n = 122) vs. del11q negative patients (n = 259), the hazard ratio was 0.14 in del11q patients and 0.26 in del11q negative patients. The hazard ratio favored ibrutinib in both groups but showed a better efficacy in del11q positive patients given lower hazard ratio [13].
Ibrutinib vs. ibrutinib + rituximab (I + R) in R/R and high risk TN patients
Randomized single center study by Burger et al (2017) included 206 patients who either had R/R disease or high-risk TN patients. Median age was 65. Del17p, unmutated IGHV and RAI stage 3-4 disease were present in 37%, 72% and 38% respectively. Patients received ibrutinib 420 mg daily either alone (n = 102) or in combination with rituximab (n = 104) for six cycles (375 mg/m2 weekly during cycle 1 and then every fourth week from cycle 2 through 6). At a median follow-up time of 25.2 months, ORR was 98% (CR 21%, PR 77%) in the arm with ibrutinib monotherapy whereas in the combination regimen at a median follow-up of 22.7 months the ORR was 100% (CR 28%, PR 72%). Although there was no significant difference in PFS between the two groups in the 2 years of follow-up, patients in the (I + R) combination group had significantly shorter median time to normalization of absolute lymphocyte count (3 vs. 8.9 months) and median time to achieve CR (11.5 vs. 21 months). Moreover, the number of patients who achieved MRD negative status was higher in the combination group (5 vs. 1) [20].
Ibrutinib + rituximab in R/R and TN patients
A single arm study by Burger et al (2014) evaluating ibrutinib at dose of 420 mg daily in addition to weekly rituximab injection (375 mg/m2) for cycle 1 and then one dose every 4 weeks for cycle 2 - 6 was evaluated in 40 patients with a median age of 63.2 (range 35 - 82). One-half of the patients had del17p mutation/TP53 (40% R/R and 10% TN), del11q mutation was present in 32.5%, del13q mutation in 12.5% and IGHV was unmutated in 80% of the patients. At a median follow-up of 16.8 months, ORR was 95% (PR 87% CR 8%). PFS and OS at 18 months were 78% and 84% respectively. In patients with del17P /TP53 mutation, the ORR was 90% (CR 10%, PR 80%), PFS and OS at 18 months were 72% and 78% respectively [21].
Ibrutinib vs. rituximab
In the recently published randomized trial in patients from Asia Pacific region, patients were randomly assigned in a 2:1 ratio to either receive ibrutinib 420 mg (n = 106) daily or rituximab (n = 54) for 3 - 6 cycles (cycle 1: 375 mg/m2 on day 1, 500 mg/m2 on day 15; cycle 2: 500 mg/m2 on day 1 and day 15; cycle 3 - 6: 500 mg/m2 on day 1). The median age in ibrutinib arm was 65 (39 - 87) as compared to 67 (21 - 86) in the rituximab arm. Baseline high risk features were comparable in ibrutinib vs. rituximab arm such as del17p (21.7% vs. 24.1%), unmutated IGHV (59.4% vs. 64.8%), baseline cytopenia (77.4% vs. 79.6%), 11q deletion (20.8% vs. 22.2%) except presence of bulky disease i.e. > 5cm lymph nodes which was much higher in the group that received rituximab (39.6% vs. 51.9%). The ORR was much higher in the ibrutinib arm 68 % (CR 3.8%; PR 64.2%) vs. 7.4% (CR 0; PR 7.4%) in the rituximab. PFS was significantly improved in patients who received ibrutinib (hazard ratio: 0.180 (95% CI 0.105 - 0.308, P < 0.0001)). Median PFS was not reached with ibrutinib as compared to 8.3 months (range: 0 - 22.6) with rituximab whereas 18 - month PFS was 74% and 11.9% respectively. The 24-month OS was higher in the ibrutinib arm (79.8% vs. 57.6%) with a HR of 0.446 (95% CI 0.221 - 0.900). Patients with del11q mutation had a lower HR for PFS in ibrutinib as compared rituximab (0.123 (0.032 - 0.463) vs. 0.204 (0.114 - 0.364)) respectively [27].
Bendamustine/rituximab + ibrutinib (BRi) vs. bendamustine/rituximab (BR): HELIOS trial
Phase 3 trial by Chanan-khan et al (2016) compared combination of BR with either ibrutinib (n = 289) or placebo (n = 289) in RR CLL/SLL. The median prior number of treatments in each group was 2. Patients in the ibrutinib arm had a median age of 64 (31 - 86) as compared to 63 (36 - 83) in placebo arm. Baseline characteristics and high-risk features were comparable. Patients with del17p were excluded. Percentage of high-risk feature in BRi arm vs. BR included RAI stage 3 or 4 (39% vs. 46%), bulky disease i.e. lymph nodes > 5cm (58% vs. 54%), del11q (30% vs. 22%), unmutated IGHV (81% vs. 80%), raised ZAP 70 expression (75% vs. 69%), purine analog refractory (26% vs. 26%) respectively. Both groups had 289 patients initially; however 90 patients in the placebo group with disease progression crossed over to the group who got ibrutinib. At median follow-up of 18 months, median PFS for ibrutinib arm was not reached. The median PFS was 13.9 by independent assessment for placebo arm. The PFS at 18 months was 79% vs. 24% respectively. ORR in BRi arm was 83% (CR/CRi 10%, PR 72.3%) as compared to 68% (CR/CR 3%, PR 65%) in the placebo arm. Thirty-one percent of the patients in the placebo group crossed over to ibrutinib and when adjusted for cross over, OS was significantly better in the ibrutinib group (HR 0.577, 95% CI: 0.348 - 0.957, P value: 0.033). The percentage of patients with MRD negative status was higher in the ibrutinib group (13% vs. 5%, P = 0.0011). Overall hazard ratio for PFS was 0.203 (95% CI: 0.150 - 0.276). In a subgroup analysis of PFS in terms of del11q status, the hazard ratio was 0.083 in del11q patients and 0.274 in del11q negative patients. The efficacy of ibrutinib was more pronounced in patients with positive del11q mutation [22].
Bendamustine/rituximab + ibrutinib (BRi) vs. fludarabine/cyclophosphamide/rituximab + ibrutinib (FCRi)
A phase 1b clinical trial by Brown et al (2015) compared the addition of ibrutinib to either FCR (n = 3) or BR (n = 30) in R/R patients. The number of patients who received FCR + ibrutinib was only 3 because of limited number of R/R patients who were purine analog naive and eligible for FCR regimen. Patients who got ibrutinib with BR had a median age of 62 and achieved an ORR of 96.6% (CR 40%, CRi 0, nodular PR 6.7%, PR 46.7%, PR-L 3.3%) and progression of disease in 3.3% patients. PFS at 6 months was 93.1% and at 12 months was 85.9%. The frequency of del17p13 and del11q were 23.3% and 33.3% respectively [23].
Ibrutinib in patients with del17p/TP53 aberrations
The phase 2 trial by Farooqui et al (2014) included 16 R/R with TP53 aberrations. The ORR was 80%. Median follow-up period was 15 weeks. Two-year OS was 74%. Two-year PFS in IGHV mutated patients was 94% compared to 71% in IGHV unmutated patients. To determine if del17p confers resistance to ibrutinib treatment, proportion of del17p mutations was measured before and 24 weeks post treatment initiation. Among 47 patients evaluated, 47% had a decrease in the proportion of del17p cells, 47% had an increase whereas for 6% of the patient it was unchanged. Among the four patients who had progressive disease on ibrutinib, two had decrease in the proportion of del17p cells whereas the other two were not a part of the analysis [16].
Ibrutinib in patients with del17p: RESONATE 17 trial
RESONATE 17 is a phase 2 clinical trial by O’Brien et al which included 145 patients with del17p mutation and relapsed/refractory disease. The median number of prior therapies was 2 (range 1 - 3). The median age of the patients was 64 (range 57 - 72). The median proportion of cells with del17p was 66%. Besides del17p, other high-risk features included 13q deletion (74%), 11q deletion (16%) and unmutated IGHV (67%). Sixty-three percent of the patients belonged to either RAI stage 3 or 4 whereas bulky disease i.e. > 5cm lymph nodes was present in 49%. ORR at a median follow-up of 11.5 months was 64% (CR-O, PR 64%) as per independent assessment. The extended investigator analysis at 27.6 months showed an ORR of 83% (PR 64%, PR-L 7% nodular PR 2%, CR 8%, and CR with incomplete bone marrow recovery 2%).
PFS at 24 months was 63 % whereas median PFS at 27.6 months was not reached. Twenty-seven percent of the patients developed (PD) and 11.7% had progressed to Ritchers’ transformation (RT). OS at 24 months was 75% whereas median OS at 27.6 months was not reached. Subgroup analysis showed that proportion of cells with del17p did not predict overall response (83.1 (73.3 - 90.5) in patients with del17p greater than median vs. 83.6 (71.9 - 91.8) in patients with percentage of cells having the mutation less than the median) [24].
Ibrutinib + ublituximab vs. ibrutinib in high risk R/R patients: GENUINE trial
In an ongoing phase 3 trial by Sharman et al , a combination of ibrutinib with ublituximab (900 mg dosed on days 1, 8, and 15 of cycle 1 and day 1 of cycles 2 to 6) was compared with ibrutinib alone in relapsed patients with at least one high risk cytogenetic abnormality( del17p 66%, del11q 34%). Median age was 67 and median number of prior therapies was 3 (range1 - 8). At a median follow-up of 12 months, patients who received the combination of ibrutinib and ublituximab had an ORR of 78% (CR: 7% and MRD negative disease 19%). Patients in the ibrutinib arm had an ORR of 45% (CR: 0%, MRD negative disease 12%), P value < 0.001 [25].
Discussion
Patients with del17p mutation have poor outcomes with chemoimmunotherapy (FCR, BR) which was the standard of care in such patients in the pre-ibrutinib era [28, 29]. In a study by Fischer et al (2015), of the 22 patients with del17p mutation in (FCR) arm, only 5% CR (ORR 68%) was seen in TN patients with CLL. The median PFS was 11.3 months [7]. In the trial evaluating BR for CLL in the first line setting, eight patients had del17p mutation but none of them achieved CR while three patients (37.5%) were able to achieve partial response [8]. In comparison, ibrutinib in patients with del17p mutation had superior efficacy resulting in an expedited approval by FDA in February 2014. In the phase 2 trial by Farooqui et al [16], the ORR in TN and R/R del17p13 positive patients treated with ibrutinib was 97% and 80% respectively.
In the last two decades, the addition of rituximab to standard chemotherapy (FCR, BR) has revolutionized the treatment of CLL [30]. Similarly, the addition of anti-CD20 monoclonal antibodies to ibrutinib can potentially lead to even better results in patient with del17p mutations. Such agents under evaluation in clinical trials are rituximab, ofatumumab and ublituximab. The combination regimen, ibrutinib plus rituximab, achieved an ORR of 90% in patients with del17p mutation/TP53 aberration which was higher than ORR achieved with ibrutinib seen in the RESONATE 17 trial (83% investigator assessed). The better efficacy with the combination regimen was seen in spite of higher frequency of the poor prognostic features present (RAI stage 3 or 4: 72.5% vs. 63%; del11q 32.5% vs. 16%; unmutated IGHV 80% vs. 67%). Interestingly, ibrutinib associated lymphocytosis, although not proven to be a poor prognostic indicator, was much shorter with ibrutinib plus rituximab regimen as compared to ibrutinib alone in the RESONATE 17 trial (8% after 6 months and absent after 12 months vs. 20% after 12 months respectively). Ibrutinib plus rituximab regimen was well tolerated with reported improvement in the global health status post 6 months initiating the treatment. Compared to single agent ibrutinib in RESONATE 17 trial, patients who received the combination regimen (ibrutinib plus rituximab) had higher incidence of lung infections (grade 1/2: 36%, grade 3/4: 5% vs. grade 1/2: 21%, grade 3/4: 4%), but lower incidence of atrial fibrillation (grade 1/2: 6% vs. grade3/4: 7%) [21, 24]. Head to head randomized control trials are needed to determine if addition of anti-CD20 monoclonal antibodies to ibrutinib improves long-term outcomes in patients with del17p mutation. A randomized clinical trial of ibrutinib plus rituximab vs. ibrutinib is currently underway which contains over one-third (37%) of the patients with del17p mutation. Preliminary results showed slightly better response rate with the combination regimen vs. ibrutinib alone (ORR 100% vs. 98% and CR 28% vs. 21%). GENUINE trial which included 64% of patients with del17p.13 mutation, showed combination of ibrutinib and ublituximab was associated with better ORR(78% vs. 45%) and CR (7% vs. 0), and higher percentage of patients who were able to achieve MRD negative status as compared to ibrutinib alone. Although these results are encouraging, it is still premature to make any conclusions until long-term follow-up data are available
In the pre-ibrutinib era, various other regimens have been evaluated in patients with del17p/TP53 aberrations. In a trial by Pileckyte et al, 13 patients with del17p mutations were treated with a combination regimen of high dose methylprednisone and rituximab achieving an ORR of 69%. Patients were followed for a median period of 22 months with a median PFS and OS of 12 months and 31 months respectively [31]. Combination of high dose methyl prednisone and alemtuzumab achieved decent response rate (ORR 85%, CR 36%), but the adverse effect profile was concerning having grade 3 and/or 4 hepatotoxicity and infections in more than 50% of the patients [32]. Direct comparison cannot be drawn but the results from these trials show an inferior response rate compared to ibrutinib.
In addition to ibrutinib, the two other promising novel agents are venetoclax and idelalisib. Venetoclax, a selective BCL-2 inhibitor, was evaluated in a phase 1 study of del17p positive R/R CLL patients. In 106 patients with the mutation, ORR was 79.4% (CR/CRi 7.5%) which was higher than the ORR (64%) seen with ibrutinib in a similar patient population in the RESONATE 17 trial [12]. Twelve-month PFS and OS were 72% and 86.7% respectively [33]. In a phase 2 study by O’Brien, combination of idelalisib (P13Kδ inhibitor working on BCR pathway) and rituximab achieved a 100% ORR (CR 33.3%, PR 66.7%) in the nine TN patients with del17p mutations [34]. In comparison, the 20 del17p positive patients (predominantly R/R) treated with ibrutinib and rituximab in the trial by Burger et al, the ORR was 90% (CR 80%, PR 10%) [21]. The data for venetoclax and idelalisib in patients with del17p are still limited, but like ibrutinib has shown promising results thus far.
Subgroup analysis of the RESONATE 2, HELIOS and RESONATE trial showed that patients with positive del11q22.3 had lower hazard ratio for PFS as compared to the patients who were negative for this mutation. We propose that the efficacy of ibrutinib may be more pronounced in patients who are positive for del11q mutation. A multivariate analysis of the pooled data from the three trials mentioned above, showed that the presence of del11q22.3 mutation was associated with a longer PFS and OS in patients treated with ibrutinib as compared to patients treated with the comparing regimen ( i.e. chlorambucil; ofatumumab; bendamustine, rituximab and placebo) [35]. As mentioned in the results section, other high risk factors such as unmutated IGHV, presence of bulky disease i.e. > 5 cm lymph node, and elevated ZAP 70 expression had lower hazard ratio for PFS in patients treated with ibrutinib as compared to the non-ibrutinib regimen.
The treatment of del17p negative patients in TN as well as relapsed and refractory cases depends upon patient’s age, comorbidities, kidney function (creatinine clearance) and functional status. Chemoimmunotherapy consisting of FCR is still considered first-line treatment in younger, low risk TN patients with low comorbidity load. In the trial by Burger et al (2015) single agent ibrutinib achieved an ORR of 92% (CR 18%) in TN del17p negative patients. Median follow-up was 28.6 whereas median PFS and OS were not reached [10]. In comparison, in a trial by Eichhorst et al (2016), FCR in TN del17p negative patients achieved an ORR of 95% (CR 40%) and median PFS of 55.2 months at a median follow-up of 37.1 months. Although the complete response rate was higher in the trial treated with FCR as compared to ibrutinib (40% vs. 18%) but the patients in the FCR trial were younger (median age 62 vs. 73) [5]. Based on better PFS and CR rates with FCR, it is the regimen of choice in TN del17p negative patients with good functional status.
Treatment choice in relapsed patient with negative del17p is more complicated [36]. FCR/BR regimen can be repeated in patients who are physically fit with limited prior therapies and longer remissions with prior therapies [37]. Ibrutinib in combination with BR has shown an ORR of 83% and an 18-month PFS of 79% in del17p negative R/R patients [22]. Ibrutinib used as monotherapy in R/R patients had an ORR of 63% having a 6-month PFS of 88% [13]. Among other novel agents, venetoclax and idelalisib have shown similar results in R/R patients in various phase 1 and 2 clinical trials [38, 39].
Conclusions
Ibrutinib is the treatment of choice for patients with high risk, but prognosis remains poor. Combining ibrutinib with immunotherapy (rituximab, ofatumumab or ublituximab) has shown promising preliminary results in high-risk del17p positive CLL. We await long-term follow-up from these studies to further shed light on the best regimen in high-risk del17p CLL patients. In patients with del17p negative disease, and who are intensive CIT ineligible, ibrutinib is still a very effective chemotherapeutic agent. Future prospects include combination regimen consisting of ibrutinib and chemo immunotherapy (FCR/ BR) as well as combination of ibrutinib with other novel agents (venetoclax, idelalisib) in TN and R/R del17p negative CLL patients. Limitations of our review include the heterogeneity of patient population and incomplete results from ongoing clinical trials. Our subgroup analysis shows that the efficacy in terms of PFS of ibrutinib may be more pronounced in patients with del11q mutation independent of del17p mutation.
Acknowledgments
None to declare.
Financial Disclosure or Funding
Authors declare no financial disclosure or funding.
Conflict Of Interest
Authors declare no conflict of interest exists.
Author Contributions
All authors were involved in literature search, data extraction and contributed towards writing the manuscript.
References
- 1.Shanafelt TD, Rabe KG, Kay NE, Zent CS, Jelinek DF, Reinalda MS, Schwager SM. et al. Age at diagnosis and the utility of prognostic testing in patients with chronic lymphocytic leukemia. Cancer. 2010;116(20):4777–4787. doi: 10.1002/cncr.25292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Cancer stat facts: Chronic lymphocytic leukemia (CLL). In: 2008-2014.
- 3.Hallek M, Cheson BD, Catovsky D, Caligaris-Cappio F, Dighiero G, Dohner H, Hillmen P. et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood. 2008;111(12):5446–5456. doi: 10.1182/blood-2007-06-093906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hallek M. Chronic lymphocytic leukemia: 2017 update on diagnosis, risk stratification, and treatment. Am J Hematol. 2017;92(9):946–965. doi: 10.1002/ajh.24826. [DOI] [PubMed] [Google Scholar]
- 5.Eichhorst B, Fink AM, Bahlo J, Busch R, Kovacs G, Maurer C, Lange E. et al. First-line chemoimmunotherapy with bendamustine and rituximab versus fludarabine, cyclophosphamide, and rituximab in patients with advanced chronic lymphocytic leukaemia (CLL10): an international, open-label, randomised, phase 3, non-inferiority trial. Lancet Oncol. 2016;17(7):928–942. doi: 10.1016/S1470-2045(16)30051-1. [DOI] [PubMed] [Google Scholar]
- 6.Jain N, O'Brien S. Initial treatment of CLL: integrating biology and functional status. Blood. 2015;126(4):463–470. doi: 10.1182/blood-2015-04-585067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hallek M, Fischer K, Fingerle-Rowson G, Fink AM, Busch R, Mayer J, Hensel M. et al. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet. 2010;376(9747):1164–1174. doi: 10.1016/S0140-6736(10)61381-5. [DOI] [PubMed] [Google Scholar]
- 8.Fischer K, Cramer P, Busch R, Bottcher S, Bahlo J, Schubert J, Pfluger KH. et al. Bendamustine in combination with rituximab for previously untreated patients with chronic lymphocytic leukemia: a multicenter phase II trial of the German Chronic Lymphocytic Leukemia Study Group. J Clin Oncol. 2012;30(26):3209–3216. doi: 10.1200/JCO.2011.39.2688. [DOI] [PubMed] [Google Scholar]
- 9.Lamanna N, O'Brien S. Novel agents in chronic lymphocytic leukemia. Hematology Am Soc Hematol Educ Program. 2016;2016(1):137–145. doi: 10.1182/asheducation-2016.1.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Burger JA, Tedeschi A, Barr PM, Robak T, Owen C, Ghia P, Bairey O. et al. Ibrutinib as Initial Therapy for Patients with Chronic Lymphocytic Leukemia. N Engl J Med. 2015;373(25):2425–2437. doi: 10.1056/NEJMoa1509388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Parmar S, Patel K, Pinilla-Ibarz J. Ibrutinib (imbruvica): a novel targeted therapy for chronic lymphocytic leukemia. P T. 2014;39(7):483–519. [PMC free article] [PubMed] [Google Scholar]
- 12.Advani RH, Buggy JJ, Sharman JP, Smith SM, Boyd TE, Grant B, Kolibaba KS. et al. Bruton tyrosine kinase inhibitor ibrutinib (PCI-32765) has significant activity in patients with relapsed/refractory B-cell malignancies. J Clin Oncol. 2013;31(1):88–94. doi: 10.1200/JCO.2012.42.7906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Byrd JC, Brown JR, O'Brien S, Barrientos JC, Kay NE, Reddy NM, Coutre S. et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N Engl J Med. 2014;371(3):213–223. doi: 10.1056/NEJMoa1400376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Byrd JC, Furman RR, Coutre SE, Flinn IW, Burger JA, Blum KA, Grant B. et al. Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med. 2013;369(1):32–42. doi: 10.1056/NEJMoa1215637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.O'Brien S, Furman RR, Coutre S, Flinn IW, Burger JA, Blum K, Sharman J. et al. Single-agent ibrutinib in treatment-naive and relapsed/refractory chronic lymphocytic leukemia: a 5-year experience. Blood. 2018;131(17):1910–1919. doi: 10.1182/blood-2017-10-810044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Farooqui MZ, Valdez J, Martyr S, Aue G, Saba N, Niemann CU, Herman SE. et al. Ibrutinib for previously untreated and relapsed or refractory chronic lymphocytic leukaemia with TP53 aberrations: a phase 2, single-arm trial. Lancet Oncol. 2015;16(2):169–176. doi: 10.1016/S1470-2045(14)71182-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jain N. Ibrutinib, Fludarabine, cyclophosphamide, and obinutuzumab (GA101)(iFCG) for first-line treatment of patients with CLL with mutated IGHV and without TP53 aberrations. 2017. [DOI] [PubMed]
- 18.David MS. A Multicenter, phase 2 study of Ibrutinib plus FCR as frontline therapy for younger patients with CLL. 2017.
- 19.Rogers KA HY, Stark A, Initial results of the phase 2 treatment naiive cohort in a phase 1b/2 study of Obinutuzumab, Ibrutinib, and Venetoclax in CLL. ASH2017.
- 20.Burger JA SM, Ferrajoli A, Randomized trial of ibrutinib versus ibrutinib plus rituximab (Ib+R) in patients with chronic lymphocytic leukemia. In: American Society of Hematology annual meeting. Abstract # 4272017.
- 21.Burger JA, Keating MJ, Wierda WG, Hartmann E, Hoellenriegel J, Rosin NY, de Weerdt I. et al. Safety and activity of ibrutinib plus rituximab for patients with high-risk chronic lymphocytic leukaemia: a single-arm, phase 2 study. Lancet Oncol. 2014;15(10):1090–1099. doi: 10.1016/S1470-2045(14)70335-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chanan-Khan A, Cramer P, Demirkan F, Fraser G, Silva RS, Grosicki S, Pristupa A. et al. Ibrutinib combined with bendamustine and rituximab compared with placebo, bendamustine, and rituximab for previously treated chronic lymphocytic leukaemia or small lymphocytic lymphoma (HELIOS): a randomised, double-blind, phase 3 study. Lancet Oncol. 2016;17(2):200–211. doi: 10.1016/S1470-2045(15)00465-9. [DOI] [PubMed] [Google Scholar]
- 23.Brown JR, Barrientos JC, Barr PM, Flinn IW, Burger JA, Tran A, Clow F. et al. The Bruton tyrosine kinase inhibitor ibrutinib with chemoimmunotherapy in patients with chronic lymphocytic leukemia. Blood. 2015;125(19):2915–2922. doi: 10.1182/blood-2014-09-585869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.O'Brien S, Jones JA, Coutre SE, Mato AR, Hillmen P, Tam C, Osterborg A. et al. Ibrutinib for patients with relapsed or refractory chronic lymphocytic leukaemia with 17p deletion (RESONATE-17): a phase 2, open-label, multicentre study. Lancet Oncol. 2016;17(10):1409–1418. doi: 10.1016/S1470-2045(16)30212-1. [DOI] [PubMed] [Google Scholar]
- 25.Jeff Sharman, A phase 3, randomized, study to assess the efficacy and safety of ublituximab in combination with ibrutinib compared to ibrutinib alone, in patients with previously treated high-risk chronic lymphocytic leukemia. ASCO Post 2017.
- 26.Paul Barr TR. Updated Efficacy and Safety from the phase 3 Resonate-2 Study: Ibrutinib as first-line treatment option in patients 65 years and older with chronic lymphocytic leukemia/small lymphocytic leukemia. 2016.
- 27.Huang X, Qiu L, Jin J, Zhou D, Chen X, Hou M, Hu J. et al. Ibrutinib versus rituximab in relapsed or refractory chronic lymphocytic leukemia or small lymphocytic lymphoma: a randomized, open-label phase 3 study. Cancer Med. 2018;7(4):1043–1055. doi: 10.1002/cam4.1337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Strati P, Keating MJ, O'Brien SM, Ferrajoli A, Burger J, Faderl S, Tambaro FP. et al. Outcomes of first-line treatment for chronic lymphocytic leukemia with 17p deletion. Haematologica. 2014;99(8):1350–1355. doi: 10.3324/haematol.2014.104661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Dohner H, Stilgenbauer S, Dohner K, Bentz M, Lichter P. Chromosome aberrations in B-cell chronic lymphocytic leukemia: reassessment based on molecular cytogenetic analysis. J Mol Med (Berl) 1999;77(2):266–281. doi: 10.1007/s001090050350. [DOI] [PubMed] [Google Scholar]
- 30.Lee LJ, Toze CL, Huang SJT, Gillan TL, Connors JM, Sehn LH, Bruyere H. et al. Improved survival outcomes with the addition of rituximab to initial therapy for chronic lymphocytic leukemia: a comparative effectiveness analysis in the province of British Columbia, Canada. Leuk Lymphoma. 2018;59(6):1356–1363. doi: 10.1080/10428194.2017.1387904. [DOI] [PubMed] [Google Scholar]
- 31.Pileckyte R, Jurgutis M, Valceckiene V, Stoskus M, Gineikiene E, Sejoniene J, Degulys A. et al. Dose-dense high-dose methylprednisolone and rituximab in the treatment of relapsed or refractory high-risk chronic lymphocytic leukemia. Leuk Lymphoma. 2011;52(6):1055–1065. doi: 10.3109/10428194.2011.562572. [DOI] [PubMed] [Google Scholar]
- 32.Pettitt AR, Jackson R, Carruthers S, Dodd J, Dodd S, Oates M, Johnson GG. et al. Alemtuzumab in combination with methylprednisolone is a highly effective induction regimen for patients with chronic lymphocytic leukemia and deletion of TP53: final results of the national cancer research institute CLL206 trial. J Clin Oncol. 2012;30(14):1647–1655. doi: 10.1200/JCO.2011.35.9695. [DOI] [PubMed] [Google Scholar]
- 33. Stephen Stilgenbauer BFE, Johannes Schetelig. Venetoclax monotherapy induces deep remissions, including complete remission and undetectable MRD, in ultra-high risk relapsed/refractory chronic lymphocytic leukemia with 17p deletion: results of the pivotal international phase 2 study. 2015.
- 34.O'Brien SM, Lamanna N, Kipps TJ, Flinn I, Zelenetz AD, Burger JA, Keating M. et al. A phase 2 study of idelalisib plus rituximab in treatment-naive older patients with chronic lymphocytic leukemia. Blood. 2015;126(25):2686–2694. doi: 10.1182/blood-2015-03-630947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. al KTe. 11q Deletion (del11q) is not a prognostic factor for adverse outcomes for patients with Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (CLL/SLL) treated with ibrutinib: pooled data from 3 randomized phase 3 studies. In: ASH 2016. Abstract # 20422016.
- 36.Shustik C, Bence-Bruckler I, Delage R, Owen CJ, Toze CL, Coutre S. Advances in the treatment of relapsed/refractory chronic lymphocytic leukemia. Ann Hematol. 2017;96(7):1185–1196. doi: 10.1007/s00277-017-2982-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Robak T, Dmoszynska A, Solal-Celigny P, Warzocha K, Loscertales J, Catalano J, Afanasiev BV. et al. Rituximab plus fludarabine and cyclophosphamide prolongs progression-free survival compared with fludarabine and cyclophosphamide alone in previously treated chronic lymphocytic leukemia. J Clin Oncol. 2010;28(10):1756–1765. doi: 10.1200/JCO.2009.26.4556. [DOI] [PubMed] [Google Scholar]
- 38.Roberts AW, Davids MS, Pagel JM, Kahl BS, Puvvada SD, Gerecitano JF, Kipps TJ. et al. Targeting BCL2 with Venetoclax in Relapsed Chronic Lymphocytic Leukemia. N Engl J Med. 2016;374(4):311–322. doi: 10.1056/NEJMoa1513257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Furman RR, Sharman JP, Coutre SE, Cheson BD, Pagel JM, Hillmen P, Barrientos JC. et al. Idelalisib and rituximab in relapsed chronic lymphocytic leukemia. N Engl J Med. 2014;370(11):997–1007. doi: 10.1056/NEJMoa1315226. [DOI] [PMC free article] [PubMed] [Google Scholar]