

Abstract
Background
Endocrine therapy removes the influence of oestrogen on breast cancer cells and so hormonal treatments such as tamoxifen, megestrol acetate and medroxyprogesterone acetate have been in use for many years for advanced breast cancer. Aromatase inhibitors (AIs) inhibit oestrogen synthesis in the peripheral tissues and have a similar tumour‐regressing effect to other endocrine treatments. Aminoglutethimide was the first AI in clinical use and now the third generation AIs, anastrozole, exemestane and letrozole, are in current use. Randomised trial evidence on response rates and side effects of these drugs is still limited.
Objectives
To compare AIs to other endocrine therapy in the treatment of advanced breast cancer in postmenopausal women.
Search methods
For this update, the Cochrane Breast Cancer Group Specialised Register and the Cochrane Central Register of Controlled Trials (CENTRAL) and relevant conference proceedings were searched (to 30 June 2008).
Selection criteria
Randomised controlled trials in postmenopausal women comparing the effects of any AI versus other endocrine therapy, no endocrine therapy, or a different AI in the treatment of advanced (metastatic) breast cancer. Non‐English language publications, comparisons of the same AI at different doses, AIs used as neoadjuvant treatment, or outcomes not related to tumour response were excluded.
Data collection and analysis
Data from published trials were extracted independently by two review authors and cross‐checked by a third. Hazard ratios (HR) were derived for analysis of time‐to‐event outcomes (overall and progression‐free survival). Odds ratios (OR) were derived for objective response, clinical benefit, and toxicity.
Main results
Thirty‐seven trials were identified, 31 of which were included in the main analysis of any AI versus any other treatment (11,403 women). No trials were excluded due to inadequate allocation concealment. The pooled estimate showed a significant survival benefit for treatment with an AI over other endocrine therapies (HR 0.90, 95% CI 0.84 to 0.97). A subgroup analysis of the three commonly prescribed AIs (anastrozole, exemestane, letrozole) also showed a similar survival benefit (HR 0.88, 95% CI 0.80 to 0.96). There were very limited data to compare one AI with a different AI, but these suggested an advantage for letrozole over anastrozole.
AIs have a different toxicity profile to other endocrine therapies. For those currently prescribed, and for all AIs combined, they had similar levels of hot flushes and arthralgia; increased risks of rash, nausea, diarrhoea and vomiting; but a 71% decreased risk of vaginal bleeding and 47% decrease in thromboembolic events compared with other endocrine therapies.
Authors' conclusions
In women with advanced (metastatic) breast cancer, aromatase inhibitors including those in current clinical use show a survival benefit when compared to other endocrine therapy.
Plain language summary
Aromatase inhibitors for treatment of advanced breast cancer in postmenopausal women
Advanced (or metastatic) breast cancer is cancer that has spread beyond the breast and regional lymph node areas. Breast cancer can progress to metastatic disease despite the person undergoing a range of therapies given after initial treatment, such as surgery, chemotherapy or radiation therapy. Metastatic breast cancer is treatable but it is not curable. Most breast cancer is sensitive to the female hormone oestrogen. Sensitive cancer cells need oestrogen to stay alive and removal of oestrogen from the body, or stopping any circulating oestrogen getting to the cancer cells, is very effective treatment for hormone‐sensitive breast cancers. Endocrine (hormonal) therapy removes the influence of oestrogen on breast cancer cells. Hormonal treatments for advanced breast cancer include tamoxifen, the progestins megestrol acetate and medroxyprogesterone acetate, and aromatase inhibitors (AIs). AIs reduce the body's ability to make (synthesise) oestrogen and have tumour‐regressing effects. The AIs in current clinical use include anastrozole, exemestane, and letrozole.
The aim of this systematic review was to compare AIs to other endocrine therapy in the treatment of advanced (metastatic) breast cancer. A systematic search was conducted which identified 37 controlled trials in which over 14,000 women were randomised to treatment groups. Treatment with an AI improved survival for women with metastatic disease by 10%. The overall benefits on disease‐free survival and response of the tumour were however unclear based on the studies included in this review. Trials using AIs as first‐line and second‐line therapy reported benefits of therapy that varied with the different AIs and measures of effectiveness. We were unable to identify specific subgroups of women who may benefit from AI use.
Toxicity (negative side effects) was not well reported in the trials. Where it was reported, there was variation as to the method used for reporting, the type of toxicities reported, as well as the criteria used to assess toxicity. Nevertheless, toxicity data were available for 26 of the 32 trials where an AI was compared with a non‐AI. AIs had similar levels of arthritic pain (arthralgia) and hot flushes (especially when compared to tamoxifen); increased risks of rash, diarrhoea, nausea and vomiting; but decreased risk of vaginal bleeding and blood clotting (thromboembolic) events compared with other endocrine therapies. Limited quality of life (QOL) data were provided and, as such, no conclusions can be drawn by this review as to the effect on QOL related to an AI versus a non‐AI. This is due to the differences between participants and the side‐effect profiles of the agents used, different methods of drug application (injection versus tablets), and use of four different QOL instruments at several different timepoints, some which provided results of responders versus non‐responders rather than by treatment group. Some QOL measures were based on clinician‐reported rather than patient‐reported symptoms.
Background
Description of the condition
Breast cancer is the most common cause of cancer and cancer mortality in women worldwide (Ferlay 2000). Metastatic breast cancer occurs when the cancer has spread beyond the breast and regional node areas. Breast cancer can progress to metastatic disease despite a range of adjuvant systemic therapies. Once breast cancer is metastatic it is no longer curable, but it is treatable. The aim of any further treatment is to improve the individual's quality and length of life.
Description of the intervention
Endocrine (hormonal) therapy removes the influence of oestrogen on breast cancer cells, preventing the cancer cells from growing and spreading. It has been shown to improve survival in early breast cancer EBCTCG 2005. Hormone dependency of breast cancer was first demonstrated in the 19th century by a Glasgow surgeon, Thomas Beatson, who achieved temporary regression of metastatic disease by oophorectomy (Beatson 1896). Other early methods of therapy consisted of adrenalectomy and hypophysectomy. These procedures have largely been superseded by effective hormonal treatments. Most endocrine therapies either block the binding of oestrogen to its receptor, for example tamoxifen, or reduce serum and tumour concentrations of oestrogen, for example aromatase inhibitors (AIs). A positive initial response to endocrine treatment is a good indication for use of second and even third‐line endocrine therapy, until the disease becomes hormone resistant (Roseman 1997). The most important predictor of response to hormone therapy is the oestrogen receptor (ER) status of the original tumour.
How the intervention might work
Currently, the most widely‐used endocrine therapy for treatment of hormone‐sensitive metastatic disease is tamoxifen (Howell 1997). Tamoxifen is an oral, non‐steroidal competitive ER antagonist. Tamoxifen, however, also has an agonist effect and although patients may relapse and develop acquired resistance to tamoxifen, this does not mean that they will not respond to other endocrine therapy.
Other endocrine therapies used in this setting are fulvestrant, megestrol acetate (MA), and medroxyprogesterone acetate (MPA). Fulvestrant is an ER antagonist that both downregulates and degrades the ER and reduces progesterone receptor content but, unlike tamoxifen, does not have an agonist effect. It can be used as a treatment for tamoxifen‐resistant advanced disease or after failure of treatment with an AI, so is an alternative second choice to an AI. MPA and MA are oral progestogens which have been shown to have significant antitumour activity after failure of other endocrine therapies in postmenopausal patients.
In postmenopausal women, oestrogen is no longer produced in the ovaries but androgens (mainly from the adrenal glands) are converted to oestrogens in peripheral tissue by the enzyme aromatase (Miller 1996a). Aromatase inhibitors (AIs) are a class of compounds that act systemically to inhibit oestrogen synthesis in tissues. AIs are of two types, reversible and irreversible; both types of inhibitors compete with normal substrates for binding on the enzyme. The non‐competitive inhibitors (which are steroidal) leave the enzyme permanently inactivated (Ibrahim 1995). AIs are classified as either first, second or third generation (Table 1). Aminoglutethimide (AG) was the first AI and although effective it was poorly tolerated. This was supplanted by 4‐hydroxy androstenedione (formestane), which was better tolerated. Third generation AIs fall into two principal categories of (a) non‐steroidal, reversible triazole derivatives (anastrozole, fadrozole, letrozole, vorozole) and (b) steroidal, irreversible inhibitors (exemestane). The most widely used AIs are currently anastrozole, exemestane, and letrozole.
1. Aromatase inhibitors ‐ description.
| Generic Name | Trade Name | Generation | Doses used |
| aminoglutethimide | First | 125 mg, 250 mg, 500 mg, 750 mg, 1000 mg | |
| anastrozole | Arimidex | Third, non‐steroidal | 1 mg, 10 mg |
| atamestane | Third, steroidal | 500mg | |
| exemestane | Aromasin | Third, steroidal | 25 mg |
| fadrozole | CGS16949A | Third, non‐steroidal | 2 mg |
| formestane | Lentaron | Second | 250 mg im |
| letrozole | Femara | Third, non‐steroidal | 0.5 mg, 2 mg, 2.5 mg, 10 mg |
| vorozole | Third, non‐steroidal | 2.5 mg |
Why it is important to do this review
AIs have a different toxicity profile to other endocrine therapies, although some side effects that mimic menopausal symptoms due to depletion of oestrogen are the same, such as hot flushes and sweating. Adverse events particular to AIs include stomach upsets (nausea, vomiting, diarrhoea), rash, and arthralgia. In particular, AG is poorly tolerated and can cause drowsiness, fever, and inhibition of cortisol synthesis. Formestane, although generally well tolerated as a treatment, results in a local reaction around the injection site. Of the other endocrine therapies, tamoxifen can cause endometrial changes including vaginal bleeding and increased risk of thromboembolic events. Side effects with progestogens are usually mild but may include hot flushes, night sweats, nausea and indigestion, fluid retention, weight gain, and headaches as well as an increased risk of thromboembolism. Fulvestrant can have similar oestrogen deprivation side effects, injection site reactions, vomiting and diarrhoea.
AIs are now increasingly being used in the treatment of early breast cancer, which may have an impact on their use in advanced (metastatic) disease.
Objectives
This systematic review aimed to compare AIs to other endocrine therapy in the treatment of advanced (metastatic) breast cancer in postmenopausal women.
Methods
Criteria for considering studies for this review
Types of studies
Only randomised controlled trials in the following populations were included.
Types of participants
a) Included:
postmenopausal women with advanced (stage 3) or metastatic (stage 4) breast cancer either at diagnosis or upon relapse;
oestrogen receptor (ER) positive or status unknown.
b) Excluded:
local recurrence only;
with no restrictions on metastatic site or age of the women;
inclusion not limited to use of an AI as first‐line therapy.
Types of interventions
Any AI versus any other endocrine treatment
Any AI versus no endocrine treatment
Any AI plus other endocrine treatment versus other endocrine treatment alone
Direct comparison between different AIs
Types of outcome measures
Outcome measures were defined a priori as follows.
Primary outcomes
Overall survival (defined as time from date of randomisation to date of death from any cause)
Secondary outcomes
Progression‐free survival (defined as time from date of randomisation to disease progression), also known as time to progression
Clinical response rate, comprising objective response (those women with either complete or partial shrinkage of the tumour) and clinical benefit (objective response plus stable disease for more than 24 weeks)*
Treatment toxicity (particularly AI related)
Quality of life (QOL), where available and comparable
Dropout rate
Time to treatment end (stopped or changed due to toxicity)
* International Union Against Cancer (UICC) guidelines were used for evaluation of these criteria (Hayward 1977).
Subgroup analyses The following subgroup analyses were considered:
first‐line therapy (where the AI was given as initial therapy for advanced disease);
second‐line therapy (where the advanced disease had already been treated with a different AI or another endocrine therapy);
ER positive versus ER unknown;
according to site of distant metastases and differential treatment effect.
Search methods for identification of studies
Only English language publications were included.
Electronic searches
1. The Cochrane Breast Cancer Group Specialised Register.
For the first published version of this review (Gibson 2007), the Cochrane Breast Cancer Group Specialised Register was searched (December 2004, 30 September 2005). For this update, additional searches were conducted (30 June 2008). Details of the search strategy used by the group for the identification of studies and the procedure used to code references are outlined in the group's module (www.mrw.interscience.wiley.com/cochrane/clabout/articles/BREASTCA/frame.html). Studies coded as "advanced" and "endocrine therapy" were extracted for consideration.
2. The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2008, Issue 2). See Appendix 1.
Searching other resources
Reference sections of each published paper were searched for additional studies. Conference proceedings were also searched but abstracts, apart from one, were not included. The one that was included (Schmid 2001) had no corresponding publication but there was adequate information in the abstract for the trial to be included.
Data collection and analysis
Selection of studies
Two authors (CLD, LJG) assessed all trials identified through the search strategy and independently decided on eligibility; any differences were resolved by discussion and confirmed by a third author (DJL). Final confirmation of inclusion was made by two authors (LJG, DJL). Any exclusions have been justified and documented in the table Characteristics of excluded studies.
Data from unpublished trials are not included in the review but these are included in the table of ongoing trials. For these, information was obtained from the trial protocol or other available source. Authors were approached for missing or additional information however only two replies were received out of six contacted.
Data extraction and management
Two review authors (CLD, LJG) extracted data independently using data extraction forms designed for this purpose. Data extracted included details of treatment arms and patient numbers, baseline patient characteristics, tumour response rates, time to progression, median survival, and median follow up. Data on toxicity and quality of life were extracted at a later date. The authors were not blinded to the source of the document for article selection or data extraction. A third author (DJL) assessed the data collected to ensure consistency and accuracy. Any differences were resolved by discussion. Data on study quality were extracted as described in 'Assessment of the methodological quality'. Hazard ratios and their associated variances were extracted for all measures available. If a hazard ratio and confidence interval were not reported, these values were calculated (Parmar 1995). Of the report authors (n = 8) who were contacted for supplementary information on the primary endpoints, only two replied (and the data were not available). For the updated review, data extraction was performed independently by two of the review authors (CLD, DJL).
Assessment of risk of bias in included studies
Two review authors (LJG, CLD) independently assessed the quality of all trials deemed eligible and discrepancies were resolved by discussion. The quality of each trial was assessed based on reports in the publication regarding:
quality of allocation concealment;
comparability between the baseline characteristics of the treatment arms;
inclusion of all randomised participants in the analysis;
details of dropouts.
Randomisation was assessed by grading the allocation concealment (for example blinded, stratified) as: A = adequate, B = unclear, C = inadequate (see Characteristics of included studies). It was not possible to accurately assess the quality of randomisation in all trials due to lack of information in the published articles. Any imbalance between treatment arms, both in numbers and characteristics, was taken into account in the grading.
Intention‐to‐treat statements: analyses that were stated to be by intention to treat and included all randomised patients for the primary endpoint. However, it is common practice to report response variables, that is clinical benefit and objective response, only on 'assessable' patients. We have reported these outcomes on both assessable and randomised patients.
Description of the eligibility and exclusion criteria: all trials described in detail the patient characteristics of those patients eligible for the trial. The table 'Characteristics of included studies' includes information on the balance of baseline characteristics, details of patients excluded after randomisation, definitions of the outcome measures, duration of follow up, and median length of follow up.
Measures of treatment effect
The most complete dataset feasible was assembled. Data were, however, only available for the following endpoints: overall survival, progression‐free survival, clinical benefit, objective response, and toxicity.
Overall and progression‐free survival were analysed using time‐to‐event methods and for this the hazard ratio (HR) is the most appropriate statistic. If a HR and corresponding confidence intervals (CI) were not reported, these values were calculated indirectly using median time to event (progression or survival) and the number of events extracted from the published Kaplan‐Meier curves, following the method of Parmar 1995. A weighted average of survival duration across trials was then calculated. Ratios of treatment effects for time to event were reported so that HRs less than 1.0 favoured the AI regimen.
Response rates were obtained from the tables of best response presented for each trial. Response has been analysed based on assessable (not randomised) patients as most of the trials included in this review only reported responses in this way. As a sensitivity analysis, we also analysed results by intention to treat (ITT); there was no difference. Response rates were analysed as dichotomous variables (for example objective response compared complete or partial response versus stable disease or no response). An odds ratio (OR) and its associated 95% CI were calculated for each trial and a pooled OR derived. Ratios of treatment effects on response were reported so that ORs less than 1.0 favoured the AI regimen. In this case, the 'event' is in effect 'not getting an objective reponse' or 'not getting a clinical benefit'.
Results are presented graphically and all figures follow the same format. Each trial is presented as a single line within each category. The point estimate of the treatment effect is represented by a square, the size of which is proportional to the size of the trial. The associated 95% CI is included as a horizontal line. The summary in each category is represented by a diamond, the north‐south axis is the pooled estimate and the east‐west axis is the 95% CI.
Unit of analysis issues
There were no unit of analysis issues in this review.
Dealing with missing data
The number of actual dropouts was very difficult to quantify as the quantity and quality of reporting varied greatly. Only 10 trials gave full details by treatment arm. Three trials quoted the number of patients withdrawn due to toxicity as "a small number" (Buzdar 1996b; Buzdar 1996c; Kaufmann 2000). Thus the patients that could be confidently identified as lost to follow up, refusals, or withdrawals totalled 62.
Toxicity
Not all toxicities (also known as side effects or adverse events) were reported in this review. We selected eight predefined toxicities from expert experience, reflecting side effects specific to AIs (nausea, vomiting, diarrhoea, rash, arthralgia) and other hormonal treatments (hot flushes, vaginal bleeding, thromboembolic events). Each side effect was analysed as a dichotomous variable (yes or no) with the effect of the AI considered separately to that of the comparator. This was deemed the most informative method of presentation as the different comparators have different toxicity profiles, whereas AIs have similar toxicity profiles. An OR and its associated 95% CI were calculated for each trial and a pooled OR derived. Ratios of treatment effects for toxicity were reported so that ORs less than 1.0 favoured the AI regimen.
Assessment of heterogeneity
Statistical heterogeneity between trials was assessed using the Chi2 statistic. However, there were cases where the value for the I2 statistic was high but the Chi2 test was not statistically significant; we advise caution in interpreting these results. Evidence of heterogeneity between trials was identified for tumour response rates and progression‐free survival though not overall survival, which seems less susceptible to heterogeneity. The reasons for this are unknown but this statistical heterogeneity may be explained by clinical heterogeneity. It is possible that outcomes involving subjective endpoints, that is tumour response, may be subject to variation whereas the hard endpoint used in the survival analysis is unequivocal. With progression‐free survival, the trials were undertaken in populations that varied considerably. For example, some trials were using the AI as first‐line treatment, some as second‐line treatment, and in other trials as mixed first‐ and second‐line. Other contributory factors may be the difference in dosage of some AIs and significant differences in the proportion of patients who were truly hormone receptor positive. We stress that as this review describes a very mixed range of studies of mixed patient populations, carried out over 30 years, the relative effect between treatment arms would still be consistent even with this mix of different patient groups.
Assessment of reporting biases
There is a lack of reporting of overall survival information compared to tumour response. Many of the trials were carried out over 10 years ago but there have been no subsequent publications with updated (or any) survival information.
Data synthesis
The Cochrane Review Manager Software (RevMan5) was used to analyse the data.
A Mantel‐Haenszel fixed‐effect model was used for the primary analyses (see the Cochrane Handbook for Systematic Reviews of Interventions) unless there was significant heterogeneity, in which case a random effects model was used (Higgins 2003). A fixed‐effect model was used for all overall survival analyses, and all analyses for any AI versus a different AI. For any AI versus a non‐AI, and current AIs versus non‐AIs, a random‐effects model was used for progression‐free survival, clinical benefit, and objective response. When an AI was used as first‐line therapy, a random‐effects model was used for the clinical response variables but not for progression‐free survival; whereas a fixed‐effect model was used for the clinical response variables for second‐line therapy.
A pooled analysis was performed in each group, but the results from each AI were considered separately within the same group, where possible. Trials were pooled by type of AI for survival, progression‐free survival, clinical benefit, and objective response outcomes. For toxicity, the data were pooled by type of comparator, that is tamoxifen, MA, MPA, or fulvestrant, as the toxicities of different AIs are similar due to their mode of action. This approach was considered to be more informative due to differences between the AIs (first versus second or third generation; steroidal versus non‐steroidal). Post hoc, it was also decided to separately present the pooled results for the AIs that are in current clinical use (by definition the newer, third generation AIs) as this is more relevant to the clinical situation today. The AIs included were: aminoglutethimide (first generation); formestane (second generation); and anastrozole, exemestane, fadrozole, letrozole and vorozole (third generation). The non‐AIs included were: megestrol acetate (MA), tamoxifen, fulvestrant, medroxyprogesterone acetate (MPA), and hydrocortisone (HC).
Subgroup analysis and investigation of heterogeneity
In all cases, tests for heterogeneity have been performed across all trials and in each of the treatment groupings outlined above. Some of the trials that were pooled used different doses of AI, which may have contributed to some of the heterogeneity. Instances of statistically significant heterogeneity are discussed in the results section.
Sensitivity analysis
All analyses were based on the intention‐to‐treat (ITT) principle as far as was possible, that is comparing all women allocated to one treatment versus all those allocated to the other irrespective of compliance. Thus the results may slightly underestimate any treatment effects. However, analysis of response used the number of assessable women as the denominator as this is the accepted method. As a sensitivity analysis, both denominators were used (see Figures) and there was no major difference for response when comparing assessable to ITT. For statistical tests a P value of less than 0.05 was considered to denote statistical significance.
Results
Description of studies
Some references were excluded because they were either non‐English language papers, reviews, non‐randomised studies, or conference proceedings without the addition of published data. The exception to this was the conference abstract by Schmid 2001 which was included as it presented several of the endpoints relevant to this review in abstract form; there is no published paper for this trial. Where a trial compared two doses of an AI with a comparator, the trial was included using the arm with the standard or most commonly used dose of that particular AI versus the comparator. For anastrozole this was 1 mg; and for fadrozole it was 2.5 mg, or 2 mg if 2.5 mg was not used.
Results of the search
The original search (Gibson 2007) yielded 152 English language references, of which 133 were possibly eligible. Twenty‐five of the 133 references, relating to 22 trials, were excluded as they compared the same AI at different doses. Fifty relevant references were identified relating to 25 randomised trials which fulfilled the eligibility criteria. An additional five references for five trials were identified by the authors from reference lists in papers and reviews. The updated search (June 2008) yielded a further 54 references of which 17 were possible inclusions. This resulted in a further seven trials being assessed as eligible for inclusion.
Included studies
We included 37 trials which randomised 14,060 women. There was a great deal of variation across the trials. Trials ranged in size from 60 (Kleeberg 1997) to 1021 women (Bonneterre 2001). Fourteen trials randomised patients from multiple countries; of the remaining 23 trials, three were limited to the UK, two were from Spain, two from South Africa, two from Switzerland, six from the US, and one each from North America (US and Canada), Denmark, France, Germany, Greece, Japan, Norway, and Switzerland. The country was not formally reported in 14 trials but surmised from the addresses of the authors.
In 32 trials comparing AIs with non‐AIs,11,710 women were randomised; 2350 women were randomised in five trials of one AI versus a different AI. It should be noted that seven trials included two different doses of an AI compared with a third comparison. Data for 12,883 women were included in this review.
Of the 32 trials comparing AIs with non‐AIs, 11 used the first generation AI aminogluthetimide, three used the second generation AI formestane, and 18 used a third generation AI (anastrozole: four trials; exemestane: three trials; fadrozole: six trials; letrozole: four trials; vorozole: one trial). In these, tamoxifen was the comparator in 12 trials, MA in 13 trials, MPA in four trials, hydrocortisone (HC) in one trial, and fulvestrant in two trials.
The five trials of AIs versus a different AI compared letrozole versus anastrozole, aminoglutethimide, atamestane, or fadrozole; and anastrozole versus formestane.
The AI arm in some of the older trials (Alonso‐Munoz 1988; Canney 1988; Ingle 1986; Powles 1984; Rose 1986; Russell 1997) did not compare an AI by itself but in combination with another treatment. One very recent trial (Goss 2007) compared an AI versus a new AI (atamestane) in conjunction with a selective oestrogen receptor modulator (SERM).
In 11 of the 37 trials (randomising 3876 women) in which any AI was used as first‐line treatment versus any other comparator, tamoxifen was compared in all trials. In 19 of 37 trials (7413 randomised women) any AI was compared with any comparator as second‐line therapy. In four trials the AIs were used as both first‐ and second‐line treatments within the trials, but as the data were not split by this variable they were not included in these comparisons.
Data for all endpoints were not available in the published reports. Where data were unavailable, authors were approached for supplementary data. Five principal endpoints with sufficient data were identified: overall survival, progression‐free survival, response (either based on clinical benefit or objective response), and treatment toxicity. Likewise, data were not available in the published reports for all subgroups proposed in the review protocol. The AI versus any non‐AI comparison had enough data for all five endpoints as well as a subgroup consisting of data from the three most commonly prescribed AIs (anastrozole, exemestane, and letrozole). In addition, the results of four of the five endpoints (not toxicity) outlined above are presented in three separate groups based on: individual AIs versus different AIs, AIs used as first‐line treatment only, AIs used as second‐line therapy only.
Time to treatment end
No trial had a fixed treatment period. However, all but two of the trials (Leitzel 1995; Samonis 1994) reported on at least one of the following: time to progression, time to failure or time to death, or both of the latter.
Excluded studies
Non‐randomised studies, trials in premenopausal women, and non‐English language publications were criteria for exclusion from the review. Trials which compared two different doses of the same AI were also excluded (see the table 'Characteristics of excluded studies').
Risk of bias in included studies
Thirty‐seven randomised trials were included in this review. One of the included trials did not have data on the primary or secondary endpoints so could not be included in any analysis (Leitzel 1995). It should be noted that trials by the author of one of the included trials (Bezwoda 1998), relating to high dose chemotherapy, have been found to include falsified data. However, no such findings have been reported for trials included in this review. There was therefore no reason to exclude the trial. Analysis was performed with and without this trial and there was no difference in the pooled results, although for clinical benefit the result became just significant.
It was not possible to accurately assess the quality of all trials due to lack of information in the published articles. Allocation concealment was rated as adequate in 23 trials but there were insufficient details of the allocation concealment in the remaining 14 and so they were labelled as unclear. Of these, no randomisation method was given in eight trials and four were reported to have parallel groups. No trials were deemed to have inadequate allocation concealment, from the information given in the published papers, and none were excluded for this reason. Six trials were double‐blind, double‐dummy; seven were double‐blind; one was double‐blind in one arm but open in the other (Buzdar 1996a); and one (which consisted of two trials analysed together) was double‐blind in one and open in the other trial (Mauriac 2003).
Baseline characteristics were not commented upon in 12 trials, five trials commented on a slight imbalance. One trial (Buzdar 1996a) had an imbalance in the treatment arm but this was believed to be an artefact. Another trial (Lundgren 1989) reported that "the two groups were well balanced with regard to the most important prognostic variables, with the exception of main metastatic site". All other trials reported balanced baseline characteristics in all arms.
Summary of numbers of women used in the analysis
Women randomised, all arms: 14,060 Women randomised, included arms: 12,883 Women randomised, assessable (for response): 11,111
Effects of interventions
Over 12,000 women were randomised to the included arms of 37 trials but time‐to‐event data were only available for about half of them. The results of the meta‐analysis should be interpreted bearing this in mind.
Aromatase inhibitors (AIs) versus any non‐aromatase inhibitor Of the 32 trials comparing an AI versus a non‐AI, one had no data on response or survival by treatment arm although these were included as endpoints (Leitzel 1995). Of the remaining 31 trials, data were available on overall tumour response rates in all 31, clinical benefit in 26, progression‐free survival in 11 and overall survival in 13 trials. For overall survival, the reported figures were available from the publications for six trials (Bonneterre 2001; Buzdar 1996a; Buzdar 2001; Ingle 1986; Dombernowsky 1998; Thuerlimann 1996) and were calculated for seven trials (Bezwoda 1998; Gale 1994; Goss 1999; Kaufmann 2000; Milla‐Santos 2003; Rose 1986; Russell 1997). In terms of progression‐free survival, HRs were reported in the publications of five trials (Bonneterre 2001; Buzdar 2001; Chia 2008; Ingle 1986; Mourisden 2001). The remaining six trials (Dombernowsky 1998; Goss 1999; Kaufmann 2000; Mauriac 2003; Russell 1997; Thuerlimann 1997) had sufficient data for calculation of the HRs.
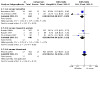
1. Overall survival Data on survival were available in 13 trials reporting an estimated 2776 events in 4789 women. No data were available for formestane. The pooled HR of 0.90 (95% CI 0.84 to 0.97) showed a statistically significant 10% benefit of treatment (P = 0.007) with an AI, with a consistent effect across all subgroups. Data on individual AIs were sparse and no conclusions could be drawn.
2. Progression‐free survival Data on progression‐free survival (PFS) were available in 11 trials reporting an estimated 4391 events in 5890 women. PFS was not statistically significantly associated with the use of an AI (HR 0.98, 95% CI 0.84 to 1.13). This overall effect is virtually uninterpretable due to the significant heterogeneity (P < 0.00001) by type of AI and also within specific AIs.
3. Proportion of women with clinical benefit (8789 assessable women) Data were available for seven AIs (aminoglutethimide, formestane, anastrozole, exemestane, fadrozole, letrozole, vorozole) from 27 trials. Approximately one third of the data came from three trials (Bonneterre 2001; Mauriac 2003; Mourisden 2001). The AIs were shown to be superior to the non‐AIs (OR 0.87, 94% CI 0.77 to 0.99) and there was statistically significant heterogeneity (P = 0.008) across trials.
4. Proportion of women with an objective response (9595 assessable women) Thirty‐one trials reported objective response. Data were available for seven AIs (aminoglutethimide, formestane, anastrozole, exemestane, fadrozole, letrozole, vorozole). The pooled OR suggested no statistically significant effect of treatment with an AI (OR 0.88, 95% CI 0.77 to 1.01) and again there was statistically significant heterogeneity (P = 0.02). Of the individual AIs, only letrozole was associated with a statistically significant benefit over the non‐AI (OR 0.65, 95% CI 0.51 to 0.82) in the 1637 women randomised (Buzdar 2001; Dombernowsky 1998; Mourisden 2001; Schmid 2001).
5. Toxicity Not all trials provided data on toxicity and there were inconsistencies among trials where it was reported. Toxicity data were available for only 26 of the trials comparing an AI with a non‐AI. Within trials, the reported toxicities varied both in the number or range and types of toxicities reported as well as the criteria used for reporting. Some trials reported predefined or selected toxicities (Bonneterre 2001; Kaufmann 2000; Mauriac 2003), some chose to report toxicities occurring in a certain minimum percentage of participants (Bezwoda 1998; Buzdar 2001; Chia 2008; Dombernowsky 1998; Goss 1999; Mauriac 2003; Mourisden 2001), some used worst toxicity grades (Falkson 1996; Thuerlimann 1996; Thuerlimann 1997) or major toxicity (Canney 1988); one reported toxicity grades 1 to 4 separately (Paridaens 2003), one used common toxicities (Buzdar 1996a) though what this meant was not defined, two reported adverse experiences (Buzdar 1996b; Buzdar 1996c), and two reported all toxicities (Freue 2000; Rose 1986). Eight trials did not state which reporting criteria they used. In addition, one trial (Perez Carrion 1994) only reported on the toxicities considered to be treatment related and has not been included. For the trial of an AI against fulvestrant (Mauriac 2003), data on toxicity were obtained from different sources. The combined analysis of the two trials 0020 and 0021 reported predefined events and data on hot flushes and thromboembolic events were available. The separate publications of the results of 0020 and 0021 detailed toxicities occurring in 10% or more of the participants. Trial 0020 reported data on both nausea and vomiting so these were combined with these data from 0021. In addition, trial 0021 had data on the frequency of diarrhoea and rash.
Despite the different reporting criteria the data were pooled. This must be borne in mind when looking at the absolute numbers. The analyses are reported according to the comparator due to the different toxicity profiles of each. An overall pooled result for AI versus non AI is not provided.
Hot flushes Hot flushes were the specific toxicity that was most widely reported. Data on hot flushes were available from 20 of the 32 trials with 8306 women. Of these, seven compared an AI with tamoxifen, 10 with MA, two with fulvestrant, and one with MPA. The use of an AI had a very similar risk of hot flushes to tamoxifen and fulvestrant. The AI was associated with statistically signficantly more reports of hot flushes than with MA (OR 1.73, 95% CI 1.40 to 2.14) but less than with MPA (OR 0.20, 95% CI 0.06 to 0.73), which had data from only one very small trial.
Nausea Data on nausea were available from 18 trials with 7895 women. Another two trials reported data on nausea and vomiting combined. Of the 18, six compared an AI with tamoxifen, nine with MA, two with fulvestrant, and one with MPA. AIs were associated with a statistically significant increase in risk of nausea compared to MA (OR 1.77, 95% CI 1.33 to 2.35) but there was no statistically significant difference between AIs and tamoxifen (P = 0.32) or fulvestrant (P = 0.96).
Vomiting Two trials had data on nausea and vomiting combined and so were not included. Data on vomiting were available from two trials comparing AIs with tamoxifen, five versus MA, and one versus fulvestrant for a total of 4404 women. The AI was statistically significantly worse when compared to MA (OR 2.03, 95% CI 1.42 to 2.90). The comparisons with tamoxifen and fulvestrant suggested no statistically significant differences.
Diarrhoea Ten trials with 5200 women had data on diarrhoea toxicity. Of these, three compared an AI with tamoxifen, five with MA, and two with fulvestrant. AIs were associated with a statistically significant higher rate of diarrhoea than either tamoxifen (OR 1.64, 95% CI 1.06 to 2.55) or MA (OR 1.48, 95% CI 1.02 to 2.13) but not fulvestrant (P = 0.36). Rash Fifteen trials with 4598 women had data on rash toxicity. Of these, four compared an AI with tamoxifen, eight with MA, two with MPA, and one with fulvestrant. AIs were associated with a statistically significant increased risk of rash when compared with tamoxifen (OR 33.61, 95% CI 4.71 to 239.97) and for the two trials versus MPA (OR 36.80, 95% CI 3.35 to 404.73) but not against MA or fulvestrant. Within the comparison with MA there was statistically significant heterogeneity (P = 0.0003) and moderate heterogeneity with tamoxifen. Vaginal bleeding Data on vaginal bleeding were reported in six trials of 2750 women: one compared an AI with tamoxifen, three with MA, and two with MPA. Compared with MA, there was a statistically significant benefit of 78% for treatment with the AI (OR 0.22, 95% CI 0.10 to 0.45). The two trials versus MPA also found a statistically significant difference with an OR of 0.13 (95% CI 0.02 to 0.71). In one of the larger trials (Bonneterre 2001) that compared an AI with tamoxifen, there was no statistically significant difference (P = 0.15).
Thromboembolic events Thromboembolic event data were available from six trials with 2937 women. Two compared an AI with tamoxifen, three with MA, and one with fulvestrant. The AI had a statistically significant advantage only over tamoxifen (OR 0.48, 95% CI 0.27 to 0.85). Arthralgia Data on arthralgia were available for 2470 women in two trials versus tamoxifen (1031 women) and four trials versus MA (1439 women). There was no statistically significant difference between the AIs and either tamoxifen or MA. Subgroup analysis: aromatase inhibitors (AIs) in current clinical use versus any non‐aromatase inhibitor
Eleven of the 32 trials comparing an AI with a non‐AI were on the three AIs in current clinical use, namely anastrozole, exemestane and letrozole. The pooled results for these are reported. Data on overall survival and time to progression were available from only six and seven trials respectively, but response rates and clinical benefit were available from all 11 trials. In terms of survival, HRs were reported in the publications of four trials: anastrozole (Bonneterre 2001; Buzdar 1996a) and letrozole (Buzdar 2001; Dombernowsky 1998). Another two trials (Kaufmann 2000; Milla‐Santos 2003) had sufficient data for calculation of the HRs. For time to progression, the corresponding numbers of trials were four (Bonneterre 2001; Buzdar 2001; Chia 2008; Mourisden 2001) and three (Dombernowsky 1998; Kaufmann 2000; Mauriac 2003), respectively.
1. Overall survival Data on survival were available from six trials (Bonneterre 2001; Buzdar 1996a; Buzdar 2001; Dombernowsky 1998; Kaufmann 2000; Milla‐Santos 2003). The AI was statistically significantly superior to the non‐AI with a HR of 0.88 (95% CI 0.80 to 0.96), equivalent to a 12% benefit of treatment with an AI. This effect was consistent across all subgroups.
2. Progression‐free survival Data on progression were available from seven trials (Bonneterre 2001; Buzdar 2001; Chia 2008; Dombernowsky 1998; Kaufmann 2000; Mauriac 2003; Mourisden 2001) reporting an estimated 3660 events in 5004 women. Use of an AI was not statistically significantly associated with a change in the hazard of progression (HR 0.93, 95% CI 0.78 to 1.12). The results did not vary by type of AI. There was significant heterogeneity in the pooled result (P < 0.00001) within the anastrozole trials (P < 0.00001) and the letrozole trials (P = 0.01).
3. Proportion of women with clinical benefit (5619 assessable women) Data were available from 11 trials. The pooled OR suggested a statistically significant advantage of 20% for the AI (OR 0.80, 95% CI 0.66 to 0.97). There was statistically significant heterogeneity among the trials (P = 0.002).
4. Proportion of women with an objective response (5619 assessable women) All 11 trials reported objective response. The pooled OR of 0.79 (95% CI 0.65 to 0.97) showed a statistically significant advantage to the AI but there was statistically significant heterogeneity (P = 0.03) across the trial results. There was also significant heterogeneity within the exemestane trials. 5. Toxicity One of the suggested benefits of the third generation AIs is a reduced toxicity profile. The results were presented by comparator as the comparators have different toxicity profiles whereas the AIs have similar toxicity profiles. The denominators for the comparison of anastrozole with fulvestrant varied depending on whether the combined trial results were available (hot flushes, nausea, vomiting, thromboembolic events) or not (diarrhoea, rash). Hot flushes Hot flushes were the specific toxicity that was reported most widely. Data on hot flushes were available from nine of the 11 trials, with 5623 women. Three trials compared the AI with tamoxifen, four with MA, and two with fulvestrant. The use of an AI had a very similar risk of hot flushes to tamoxifen and fulvestrant but was associated with statistically significant more reports of hot flushes than with MA (OR 1.69, 95% CI 1.24 to 2.30). Nausea Data on nausea were available from nine of the 11 trials, involving 5623 women. Of the nine trials, three compared an AI with tamoxifen, four with MA and two with fulvestrant. The AIs had statistically signicantly more reports of nausea than MA (OR 1.45, 95% CI 1.09 to 1.95) but there was no statistically significant difference when the AIs were compared to tamoxifen or fulvestrant.
Vomiting Five trials with 3499 women had data on vomiting alone and only MA as the comparator had more than one trial. There was no statistically significant differences between the AI and either tamoxifen or fulvestrant. Compared with MA, the AIs had a statistically significantly increased risk of vomiting (OR 1.77, 95% CI 1.11 to 2.83).
Diarrhoea Seven trials with 4295 women had data on diarrhoea toxicity. Two compared an AI with tamoxifen, three with MA, and two with fulvestrant. There was a statistically significant increased risk of diarrhoea with the AIs against MA (OR 2.40, 95% CI 1.34 to 4.29).
Rash Four trials with 2033 women that compared AIs with MA or fulvestrant (one trial only) had data on rash. AIs were not associated with a statistically significant increased risk of rash and there was statistically significant heterogeneity among the three trials with MA as the comparator (P = 0.04). Vaginal bleeding Data on vaginal bleeding were reported in three trials with 1932 women, one compared an AI with tamoxifen and two with MA. There was a statistically significant benefit to treatment with the AIs in comparison with MA (OR 0.29, 95% CI 0.13 to 0.65).
Thromboembolic events Thromboembolic event data were available for 2378 women in three trials but there was only one trial per comparator (tamoxifen, MA, or fulvestrant). AIs were associated with a statistically significant lower incidence of thromboembolic events than tamoxifen (OR 0.53, 95% CI 0.30 to 0.96) but not compared with MA or fulvestrant.
Arthralgia Data on arthralgia as a specific side effect were only available for 1394 women in three trials, two versus tamoxifen and one versus MA. Against both comparators, the AI was not statistically significantly associated with a difference in the incidence of arthralgia.
Other analyses Aromatase inhibitors (AIs) versus any different aromatase inhibitor
A total of 2346 women in five trials were randomised to one AI versus a different AI. Of these, all five had data on response but only two had results on overall survival and progression‐free survival (Gershanovich 1998; Goss 2007). Letrozole was compared with a different AI in all the trials (Gershanovich 1998; Rose 2003; Tominaga 2003) except that of Kleeberg 1997 which compared anastrozole with formestane. The trial by Rose and colleagues (Rose 2003) compared letrozole to anastrozole and in this section has been included in both the letrozole and anastrozole groups. 1. Overall survival The Gershanovich 1998 and Goss 2007 trials were the only ones that had data on overall survival and the results were driven by Goss 2007 as 70% data came from this trial. Letrozole had a reduced HR of 0.91 (95% CI 0.82 to 1.02) but this was not statistically significant and there was signficant trial heterogeneity (P = 0.006).
2.Progression‐free survival Two trials had data on progression from 1416 women (Gershanovich 1998; Goss 2007) and, again, the results were driven by the Goss 2007 trial. In these trials, letrozole was associated with a slightly reduced hazard in terms of progression‐free survival compared to aminoglutethimide, but this was not statistically significant and there was heterogeneity (P = 0.01) between the trials.
3. Proportion of women with clinical benefit (1747 assessable patients) Letrozole was associated with a statistically significant clinical benefit compared with a different AI (OR 0.77, 95% CI 0.62 to 0.95). There was no significant trial heterogeneity (P = 0.63).
4. Proportion of women with an objective response (1747 assessable patients) The pooled overall result was not presented as Rose 2003 was included in both individual AI comparisons and so would be counted twice. Letrozole was statistically significantly different from any other AI (OR 0.62, 95% CI 0.50 to 0.78). Results of all letrozole trials were consistent (test for heterogeneity P = 0.32). Anastrozole appeared to be significantly inferior to a different AI (OR 1.59, 95% CI 1.07 to 2.37). Aromatase inhibition as first‐line therapy versus any non‐AI therapy (tamoxifen)
Twelve trials that randomised 3746 women used AIs exclusively as first‐line therapy for advanced (metastatic) disease and all comparisons were against tamoxifen. We did not include any trials that were mixed first‐ and second‐line. Data from three trials with 1483 women (anastrozole, fadrozole, AG) were available for overall survival and four trials with 2390 women (one trial each on formestane, anastrozole, and letrozole) for progression‐free survival. Eleven trials reported results for objective response and nine trials for clinical benefit.
1. Overall survival There was no statistically significant difference in the effect of treatment with an AI compared to tamoxifen.
2. Progression‐free survival The first‐line AI regimen was statistically significantly superior to tamoxifen with a decreased hazard of 0.78 (95% CI 0.71 to 0.86). Anastrozole (Bonneterre 2001) and letrozole (Mourisden 2001) were statistically significantly different from tamoxifen (reduced hazard of 18% and 30%, respectively).
3. Proportion of women with clinical benefit (3252 assessable women) As results for individual AIs, except for aminoglutethimide and anastrozole, were based on only a single trial the pooled result is emphasised. The AIs were better than tamoxifen as first‐line therapy (OR 0.69, 95% CI 0.51 to 0.92) although there was significant heterogeneity across the AIs (P = 0.002). 4. Proportion of women with objective response (3503 assessable women) Aminoglutethimide was the only AI with more than two trials published. The AIs were better than tamoxifen as first‐line therapy (OR 0.77, 95% CI 0.59 to 1.00) although this was of borderline statistical signficance. There was considerable heterogeneity (P = 0.003) by type of AI. Exemestane and letrozole were the only AIs that were statistically significantly better than tamoxifen but in both cases the results were only based on one trial. Aromatase inhibition as second‐line therapy versus any non‐AI therapy Women who had previously been treated with endocrine therapy, either a different AI or non‐AI, for advanced (metastatic) disease and received the trial AI as second‐line therapy were included in 19 trials. The trial by Leitzel 1995 was of second‐line therapy but does not contribute to the results here, thus giving 18 trials. Aminoglutethimide was used as second‐line in five trials, formestane in two, anastrozole in two, exemestane in two, fadrozole in three, letrozole in three, and vorozole in one trial. The majority of the comparisons (12) were against MA. We did not include trials where there was a mixture of first‐ and second‐line therapy.
Data on objective response were available from all of the trials; clinical benefit from 16 trials; HRs for progression‐free survival from eight trials; and HRs for overall survival from two trials.
1. Overall survival Data on overall survival were limited with data from two trials of different AIs, anastrozole and letrozole. Second‐line treatment with an AI was statistically significantly associated with a decreased hazard of death (HR 0.80, 95% CI 0.66 to 0.96). This effect was consistent for both AIs (heterogeneity P = 0.79).
2. Progression‐free survival AI use was not associated with a statistically significant difference in the risk of progression. There was significant heterogeneity (P = 0.001) across trials, with use of either anastrozole or vorozole associated with a significantly increased risk of progression.
3. Proportion of women with clinical benefit (5410 assessable women) There did not appear to be any effect in terms of a statistically significant clinical benefit when an AI was used as second‐line therapy (OR 0.99, 95% CI 0.88 to 1.11). This lack of effect was consistent across AI subgroups (heterogeneity P = 0.88).
4. Proportion of women with objective response (5937 assessable women) Overall there was no statistically significant difference between the use of an AI as second‐line therapy and any other therapy (OR 0.98, 95% CI 0.86 to 1.13). When looking at individual AIs, none showed any evidence of a benefit but this was based on small numbers. There was no statistical heterogeneity (P = 0.52).
Other subgroup analysis
We were not able to perform subgroup analyses on the following groups of patients as these data were not systematically reported:
ER positive versus ER unknown;
according to site of distant metastases and differential treatment effect.
Quality of Life
Nine trials (Bezwoda 1998; Buzdar 1996b; Buzdar 1996c; Buzdar 2001; Chia 2008; Goss 1999; Kaufmann 2000; Mauriac 2003; Thuerlimann 1997) quoted quality of life (QOL) as a secondary endpoint. Three of the trials (Bezwoda 1998; Buzdar 1996b; Buzdar 1996c) did not report any QOL data. Only one (Thuerlimann 1997) has published two papers on the QOL data in detail. One trial (Dombernowsky 1998) mentioned that a QOL instrument was used, at baseline and at each visit whilst on treatment, but it was not mentioned as an endpoint nor were any data included. Chia 2008 reported that the difference in QOL between the treatment arms was not statistically significant; however the graph was shown on the online publication only.
There are several reasons why the limited QOL data are not included in this review: heterogeneous changes among patients, that is different symptoms and side effect profiles; different methods of drug application, that is injection versus tablets; use of four different QOL instruments at several different timepoints; some results given as responders versus non‐responders rather than by treatment groups; some QOL measures based on clinician‐reported rather than patient‐reported symptoms.
Discussion
Summary of main results
This review demonstrates a survival benefit of 10% with the use of AIs for the treatment of advanced (metastatic) breast cancer. This finding is not consistent across all AIs, with the greatest benefit (a survival benefit of 12%) associated with the AIs in current clinical use, namely anastrozole, exemestane and letrozole. However, data on survival were only available for about half the women and one of the trials (Buzdar 1996a) was not designed or powered to detect significant differences in survival.
The positive effects of AIs in terms of tumour response were statistically significant for first‐line therapy where the comparator was tamoxifen. There were no data available for other comparators. When comparing the effect of the AI as second‐line therapy there was no statistically significant difference on tumour response. In terms of progression‐free survival, there was a statistically significant decrease in hazard of progression for treatment with the AIs as first‐line therapy only. The paucity of data makes it difficult to make any firm conclusions in terms of overall survival.
In terms of toxicity, AIs are known to be associated with a higher incidence of nausea, diarrhoea, rash and arthralgia but a lower risk of vaginal bleeding and thromboembolic events. However, combining data across trials was difficult as both the toxicities reported and the criteria for reporting toxicities, if reported at all, varied greatly. We therefore did not have data on all predetermined toxicities with all comparators. Despite the inadequacies of the data, our review corroborated the direction of the known side effects. There was a higher incidence of hot flushes when compared to MA but not to tamoxifen; nausea compared to MA but not tamoxifen or fulvestrant; vomiting compared to MA but not tamoxifen or fulvestrant; diarrhoea compared to tamoxifen and MA but not fulvestrant; and rash compared to tamoxifen and MPA but not MA or fulvestrant. The risk of vaginal bleeding was about 80% lower with AI treatment and the incidence of thromboembolic events halved. For arthralgia, there was no statistically significant difference between the AIs and either tamoxifen or MA.
Overall completeness and applicability of evidence
A lack of standardised reporting of clinical endpoints impacted upon the analysis of all AIs, not just aminoglutethimide. Therefore, it was not possible to include all trials in each section. This reduced the power of certain analyses, especially overall and progression‐free survival. In addition, many of the data required to carry out analyses of prospectively identified subgroups, as set out in the review protocol, were not available. We could not, therefore, identify specific subgroups of women who may benefit from AI use.
There are very limited data on quality of life reported in this setting. The limited quality of life data which was reported did not show any significant differences between the AI and comparator groups; however, some differences were found with some subscales in favour of the AI (Goss 1999; Kaufmann 2000). The patient's perspective in advanced disease treatment is an important endpoint and should be included in trials as it would aid interpretation in this mainly palliative setting.
Quality of the evidence
This review has combined data from a wide variety of trials that were carried out over 20 years. Some of the trials did not use an AI as a single agent but in combination with another endocrine therapy. There was heterogeneity both across types of AI and within each AI. The results of trials of three generations of AIs have been combined as well as results from trials of steroidal and non‐steroidal therapy. This has been forced, to some extent, by the lack of data on individual AIs.
Within each AI, trials varied in terms of sample size, dose of AI, comparison regimen, outcomes, length of follow up and quality of reporting. For example, the 11 trials of aminoglutethimide consisted of between 62 and 313 patients; four of the trials were of first‐line therapy, five second‐line, and two mixed. Doses of aminoglutethimide used were 125 mg in one trial, 250 mg* in three, 500 mg* in four, 750 mg in one, and 1000 mg in two (* dose doubled after a specific period of treatment). The comparator was tamoxifen in five trials (20 mg in three, 30 mg in one, 40 mg in one), MA 160 mg in three trials, MPA 500 mg in one trial, MPA 1000 mg in four trials, and HC 20 mg in one trial. Not all endpoints were available in each trial and four reported overall survival, three progression‐free survival, eight clinical benefit, and 10 objective response.
Potential biases in the review process
If the description of randomisation is used as a barometer of reporting trial quality, it appears that this has improved over time. For example, in the trials of the first generation AI aminoglutethimide six of 11 randomisations were categorised as unclear whereas only two of the nine trials of third generation AI letrozole were considered as such.
Evidence of heterogeneity between trials was identified for tumour response rates and progression‐free survival though not overall survival. The reasons for this are unknown but this statistical heterogeneity might be explained by clinical heterogeneity. It may be that outcomes involving the subjective endpoint, that is tumour response, are subject to variation whereas the hard endpoint used in the survival analysis is unequivocal. Other contributory factors may be the difference in dosage of some AIs and significant differences in the proportion of patients who were truly hormone receptor positive.
Agreements and disagreements with other studies or reviews
In September 2006, Mauri and colleagues published a paper entitled, "Survival with aromatase inhibitors and inactivators versus standard hormonal therapy in advanced breast cancer: meta‐analysis" Mauri 2006 which came to the same conclusion; that is, "Inhibition of the AI system, in particular with third generation AIs, appears to be associated with statistically significant improved survival of patients with advance breast cancer compared with standard hormonal treatments".
Authors' conclusions
Implications for practice.
Historically, the treatment for advanced (metastatic) breast cancer has been with hormonal treatments such as tamoxifen or the progestins MA or MPA. This review confirms a survival benefit of treating advanced (metastatic) breast cancer with the third generation aromatase inhibitors (anastrozole, exemestane, and letrozole) that are being used clinically today.
Implications for research.
This review would benefit from additional publications with greater survival details, that is median survival and number of events, for those trials that did not publish them originally. Further data from exemestane trials are required to evaluate this AI more completely. Efforts should be made to standardise reporting of toxicity and a quality of life component should also be included.
What's new
| Date | Event | Description |
|---|---|---|
| 7 February 2018 | Review declared as stable | Although many trials have been published since the last review version, the review contains sufficient evidence on the efficacy of Aromatase inhibitors (AIs) such that AIs are standard therapy. Therefore we do not expect to update this review. |
History
Protocol first published: Issue 4, 2001 Review first published: Issue 1, 2007
| Date | Event | Description |
|---|---|---|
| 6 August 2009 | New search has been performed | New search and addition of 7 trials |
| 6 August 2009 | New citation required but conclusions have not changed | Update for Issue 4, 2009 |
| 5 August 2009 | Amended | reference added |
| 8 July 2009 | Amended | edited to address additional reviewers' comments |
| 29 June 2009 | Amended | edited to address reviewers' comments |
| 3 February 2009 | Amended | Feedback from group incorporated |
| 27 November 2008 | New search has been performed | Search run by BCG on 2 November 2007. Authors updated search to 30 June 2008. Additional studies identified and data updated |
| 5 September 2008 | Amended | Converted to new review format. |
| 13 August 2008 | New citation required and conclusions have changed | Substantive amendment |
Notes
This updated review includes the following additional seven trials to the 30 in the original publication: Chia 2008; Gale 1994; Garcia‐Giralt 1992; Goss 2007; Lundgren 1989; Samonis 1994. There were also two papers by Mourisden and colleagues (Mourisden 2004; Mourisden 2007) which contributed follow‐up information.
The update demonstrated a survival benefit of 10% with the use of AIs for the treatment of advanced (metastatic) breast cancer, compared to 11% in the original review.
Acknowledgements
The authors were funded by Cancer Research UK. Lorna Gibson would like to thank Julian Peto and Isabel dos Santos Silva for their support. The authors would like to thank the Cochrane Breast Cancer Group for their support and are indebted to Olivia Fletcher for critical reading of the manuscript.
Appendices
Appendix 1. The Cochrane Central Register of Controlled Trials (CENTRAL) Issue 2, 2008
Search terms "aromatase inhibitor" AND "randomised trial" AND "breast cancer " AND (advanced OR metastatic)
Data and analyses
Comparison 1. AI versus non‐AI.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Overall survival (reported or calculated) | 13 | HR (IV, Fixed, 95% CI) | 0.90 [0.84, 0.97] | |
| 1.1.1 aminoglutethimide (any dose) | 4 | HR (IV, Fixed, 95% CI) | 0.94 [0.80, 1.12] | |
| 1.1.2 anastrozole 1 mg | 3 | HR (IV, Fixed, 95% CI) | 0.90 [0.79, 1.03] | |
| 1.1.3 exemestane 25 mg | 1 | HR (IV, Fixed, 95% CI) | 0.85 [0.72, 0.99] | |
| 1.1.4 fadrozole 2 mg | 2 | HR (IV, Fixed, 95% CI) | 1.04 [0.77, 1.40] | |
| 1.1.5 letrozole 2.5 mg | 2 | HR (IV, Fixed, 95% CI) | 0.88 [0.73, 1.05] | |
| 1.1.6 vorozole 2.5 mg | 1 | HR (IV, Fixed, 95% CI) | 1.10 [0.49, 2.47] | |
| 1.2 Progression‐free survival (reported or calculated) | 11 | HR (IV, Random, 95% CI) | 0.98 [0.84, 1.13] | |
| 1.2.1 aminoglutethimide (any dose) | 2 | HR (IV, Random, 95% CI) | 1.07 [0.73, 1.55] | |
| 1.2.2 formestane 250 mg | 1 | HR (IV, Random, 95% CI) | 0.93 [0.68, 1.28] | |
| 1.2.3 anastrozole 1 mg | 2 | HR (IV, Random, 95% CI) | 1.05 [0.65, 1.70] | |
| 1.2.4 exemestane 25 mg | 2 | HR (IV, Random, 95% CI) | 0.91 [0.72, 1.14] | |
| 1.2.5 letrozole 2.5 mg | 3 | HR (IV, Random, 95% CI) | 0.87 [0.68, 1.11] | |
| 1.2.6 vorozole 2.5 mg | 1 | HR (IV, Random, 95% CI) | 1.27 [1.04, 1.56] | |
| 1.3 Clinical benefit (assessable) | 27 | 8789 | Odds Ratio (M‐H, Random, 95% CI) | 0.87 [0.77, 0.99] |
| 1.3.1 aminoglutethimide (any dose) | 9 | 1292 | Odds Ratio (M‐H, Random, 95% CI) | 0.79 [0.63, 1.00] |
| 1.3.2 formestane 250 mg | 2 | 521 | Odds Ratio (M‐H, Random, 95% CI) | 1.05 [0.59, 1.86] |
| 1.3.3 anastrozole 1 mg | 4 | 2626 | Odds Ratio (M‐H, Random, 95% CI) | 0.74 [0.48, 1.12] |
| 1.3.4 exemestane 25 mg | 3 | 1356 | Odds Ratio (M‐H, Random, 95% CI) | 0.86 [0.63, 1.19] |
| 1.3.5 fadrozole 2 mg | 4 | 982 | Odds Ratio (M‐H, Random, 95% CI) | 1.05 [0.80, 1.38] |
| 1.3.6 letrozole 2.5 mg | 4 | 1637 | Odds Ratio (M‐H, Random, 95% CI) | 0.77 [0.60, 1.00] |
| 1.3.7 vorozole 2.5 mg | 1 | 375 | Odds Ratio (M‐H, Random, 95% CI) | 1.35 [0.88, 2.07] |
| 1.4 Objective response (assessable) | 31 | 9595 | Odds Ratio (M‐H, Random, 95% CI) | 0.88 [0.77, 1.01] |
| 1.4.1 aminoglutethimide (any dose) | 11 | 1545 | Odds Ratio (M‐H, Random, 95% CI) | 0.83 [0.63, 1.09] |
| 1.4.2 formestane 250 mg | 3 | 1000 | Odds Ratio (M‐H, Random, 95% CI) | 1.23 [0.92, 1.64] |
| 1.4.3 anastrozole 1 mg | 4 | 2626 | Odds Ratio (M‐H, Random, 95% CI) | 0.95 [0.77, 1.17] |
| 1.4.4 exemestane 25 mg | 3 | 1356 | Odds Ratio (M‐H, Random, 95% CI) | 0.67 [0.33, 1.33] |
| 1.4.5 fadrozole 2 mg | 5 | 1056 | Odds Ratio (M‐H, Random, 95% CI) | 1.18 [0.85, 1.65] |
| 1.4.6 letrozole 2.5 mg | 4 | 1637 | Odds Ratio (M‐H, Random, 95% CI) | 0.65 [0.51, 0.82] |
| 1.4.7 vorozole 2.5 mg | 1 | 375 | Odds Ratio (M‐H, Random, 95% CI) | 0.70 [0.34, 1.42] |
| 1.5 Clinical benefit (randomised) | 27 | 9425 | Odds Ratio (M‐H, Random, 95% CI) | 0.88 [0.78, 0.99] |
| 1.5.1 aminoglutethimide (any dose) | 9 | 1395 | Odds Ratio (M‐H, Random, 95% CI) | 0.81 [0.65, 1.01] |
| 1.5.2 formestane 250 mg | 2 | 586 | Odds Ratio (M‐H, Random, 95% CI) | 1.00 [0.58, 1.70] |
| 1.5.3 anastrozole 1 mg | 4 | 2626 | Odds Ratio (M‐H, Random, 95% CI) | 0.74 [0.48, 1.12] |
| 1.5.4 exemestane 25 mg | 3 | 1584 | Odds Ratio (M‐H, Random, 95% CI) | 0.88 [0.71, 1.11] |
| 1.5.5 fadrozole 2 mg | 4 | 1000 | Odds Ratio (M‐H, Random, 95% CI) | 1.08 [0.82, 1.41] |
| 1.5.6 letrozole 2.5 mg | 4 | 1782 | Odds Ratio (M‐H, Random, 95% CI) | 0.77 [0.61, 0.96] |
| 1.5.7 vorozole 2.5 mg | 1 | 452 | Odds Ratio (M‐H, Random, 95% CI) | 1.25 [0.83, 1.88] |
| 1.6 Objective response (randomised) | 31 | 10422 | Odds Ratio (M‐H, Random, 95% CI) | 0.90 [0.78, 1.03] |
| 1.6.1 aminoglutethimide (any dose) | 11 | 1765 | Odds Ratio (M‐H, Random, 95% CI) | 0.89 [0.66, 1.20] |
| 1.6.2 formestane 250 mg | 3 | 1133 | Odds Ratio (M‐H, Random, 95% CI) | 1.20 [0.91, 1.60] |
| 1.6.3 anastrozole 1 mg | 4 | 2626 | Odds Ratio (M‐H, Random, 95% CI) | 0.95 [0.77, 1.17] |
| 1.6.4 exemestane 25 mg | 3 | 1584 | Odds Ratio (M‐H, Random, 95% CI) | 0.68 [0.37, 1.27] |
| 1.6.5 fadrozole 2 mg | 5 | 1080 | Odds Ratio (M‐H, Random, 95% CI) | 1.21 [0.87, 1.69] |
| 1.6.6 letrozole 2.5 mg | 4 | 1782 | Odds Ratio (M‐H, Random, 95% CI) | 0.65 [0.52, 0.82] |
| 1.6.7 vorozole 2.5 mg | 1 | 452 | Odds Ratio (M‐H, Random, 95% CI) | 0.67 [0.33, 1.37] |
1.1. Analysis.

Comparison 1: AI versus non‐AI, Outcome 1: Overall survival (reported or calculated)
1.2. Analysis.

Comparison 1: AI versus non‐AI, Outcome 2: Progression‐free survival (reported or calculated)
1.3. Analysis.

Comparison 1: AI versus non‐AI, Outcome 3: Clinical benefit (assessable)
1.4. Analysis.

Comparison 1: AI versus non‐AI, Outcome 4: Objective response (assessable)
1.5. Analysis.

Comparison 1: AI versus non‐AI, Outcome 5: Clinical benefit (randomised)
1.6. Analysis.

Comparison 1: AI versus non‐AI, Outcome 6: Objective response (randomised)
Comparison 2. AI versus non‐AI: Toxicity.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 hot flushes | 20 | 8306 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.24 [1.10, 1.41] |
| 2.1.1 AI versus tamoxifen | 7 | 2616 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.88, 1.29] |
| 2.1.2 AI versus megestrol acetate | 10 | 3926 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.73 [1.40, 2.14] |
| 2.1.3 AI versus fulvestrant | 2 | 1546 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.82, 1.42] |
| 2.1.4 AI versus medroxyprogesterone acetate | 1 | 218 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.20 [0.06, 0.73] |
| 2.2 nausea | 18 | Odds Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.2.1 AI versus tamoxifen | 6 | 2548 | Odds Ratio (M‐H, Random, 95% CI) | 1.29 [0.78, 2.13] |
| 2.2.2 AI versus megestrol acetate | 9 | 3755 | Odds Ratio (M‐H, Random, 95% CI) | 1.77 [1.33, 2.35] |
| 2.2.3 AI versus medroxyprogesterone acetate | 1 | 53 | Odds Ratio (M‐H, Random, 95% CI) | 8.19 [0.40, 166.83] |
| 2.2.4 AI versus fulvestrant | 2 | 1539 | Odds Ratio (M‐H, Random, 95% CI) | 1.01 [0.77, 1.32] |
| 2.3 vomiting | 8 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.3.1 AI versus tamoxifen | 2 | 1239 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.79, 1.90] |
| 2.3.2 AI versus megestrol acetate | 5 | 2319 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.03 [1.42, 2.90] |
| 2.3.3 AI versus fulvestrant | 1 | 846 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.60, 1.35] |
| 2.4 diarrhoea | 10 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.4.1 AI versus tamoxifen | 3 | 2149 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.64 [1.06, 2.55] |
| 2.4.2 AI versus megestrol acetate | 5 | 1961 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.48 [1.02, 2.13] |
| 2.4.3 AI versus fulvestrant | 2 | 1090 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.79, 1.90] |
| 2.5 rash | 15 | Odds Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.5.1 AI versus tamoxifen | 4 | 711 | Odds Ratio (M‐H, Random, 95% CI) | 33.61 [4.71, 239.97] |
| 2.5.2 AI versus megestrol acetate | 8 | 3219 | Odds Ratio (M‐H, Random, 95% CI) | 2.06 [0.92, 4.62] |
| 2.5.3 AI versus medroxyprogesterone acetate | 2 | 271 | Odds Ratio (M‐H, Random, 95% CI) | 36.80 [3.35, 404.73] |
| 2.5.4 AI versus fulvestrant | 1 | 397 | Odds Ratio (M‐H, Random, 95% CI) | 1.39 [0.77, 2.50] |
| 2.6 vaginal bleeding | 6 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.6.1 AI versus tamoxifen | 1 | 1017 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.45 [0.16, 1.32] |
| 2.6.2 AI versus megestrol acetate | 3 | 1462 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.22 [0.10, 0.45] |
| 2.6.3 AI versus medroxyprogesterone acetate | 2 | 271 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.13 [0.02, 0.71] |
| 2.7 thromboembolic | 6 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.7.1 AI versus tamoxifen | 2 | 1228 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.27, 0.85] |
| 2.7.2 AI versus megestrol acetate | 3 | 863 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.54 [0.26, 1.10] |
| 2.7.3 AI versus fulvestrant | 1 | 846 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.56, 2.31] |
| 2.8 arthralgia | 6 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.8.1 AI versus tamoxifen | 2 | 1031 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.81, 1.60] |
| 2.8.2 AI versus megestrol acetate | 4 | 1439 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.40 [0.98, 2.00] |
2.1. Analysis.

Comparison 2: AI versus non‐AI: Toxicity, Outcome 1: hot flushes
2.2. Analysis.

Comparison 2: AI versus non‐AI: Toxicity, Outcome 2: nausea
2.3. Analysis.

Comparison 2: AI versus non‐AI: Toxicity, Outcome 3: vomiting
2.4. Analysis.

Comparison 2: AI versus non‐AI: Toxicity, Outcome 4: diarrhoea
2.5. Analysis.

Comparison 2: AI versus non‐AI: Toxicity, Outcome 5: rash
2.6. Analysis.

Comparison 2: AI versus non‐AI: Toxicity, Outcome 6: vaginal bleeding
2.7. Analysis.
Comparison 2: AI versus non‐AI: Toxicity, Outcome 7: thromboembolic
2.8. Analysis.

Comparison 2: AI versus non‐AI: Toxicity, Outcome 8: arthralgia
Comparison 3. Current AIs versus non‐AI.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 3.1 Overall survival (reported or calculated) | 6 | HR (IV, Fixed, 95% CI) | 0.88 [0.80, 0.96] | |
| 3.1.1 anastrozole 1 mg | 3 | HR (IV, Fixed, 95% CI) | 0.90 [0.79, 1.03] | |
| 3.1.2 exemestane 25 mg | 1 | HR (IV, Fixed, 95% CI) | 0.85 [0.72, 0.99] | |
| 3.1.3 letrozole 2.5 mg | 2 | HR (IV, Fixed, 95% CI) | 0.88 [0.73, 1.05] | |
| 3.2 Progression‐free survival (reported or calculated) | 7 | HR (IV, Random, 95% CI) | 0.93 [0.78, 1.12] | |
| 3.2.1 anastrozole 1 mg | 2 | HR (IV, Random, 95% CI) | 1.05 [0.65, 1.70] | |
| 3.2.2 exemestane 25 mg | 2 | HR (IV, Random, 95% CI) | 0.91 [0.72, 1.14] | |
| 3.2.3 letrozole 2.5 mg | 3 | HR (IV, Random, 95% CI) | 0.87 [0.68, 1.11] | |
| 3.3 Clinical benefit (assessable) | 11 | 5619 | Odds Ratio (M‐H, Random, 95% CI) | 0.80 [0.66, 0.97] |
| 3.3.1 anastrozole 1 mg | 4 | 2626 | Odds Ratio (M‐H, Random, 95% CI) | 0.74 [0.48, 1.12] |
| 3.3.2 exemestane 25 mg | 3 | 1356 | Odds Ratio (M‐H, Random, 95% CI) | 0.86 [0.63, 1.19] |
| 3.3.3 letrozole 2.5 mg | 4 | 1637 | Odds Ratio (M‐H, Random, 95% CI) | 0.77 [0.60, 1.00] |
| 3.4 Objective response (assessable) | 11 | 5619 | Odds Ratio (M‐H, Random, 95% CI) | 0.79 [0.65, 0.97] |
| 3.4.1 anastrozole 1 mg | 4 | 2626 | Odds Ratio (M‐H, Random, 95% CI) | 0.95 [0.77, 1.17] |
| 3.4.2 exemestane 25 mg | 3 | 1356 | Odds Ratio (M‐H, Random, 95% CI) | 0.67 [0.33, 1.33] |
| 3.4.3 letrozole 2.5 mg | 4 | 1637 | Odds Ratio (M‐H, Random, 95% CI) | 0.65 [0.51, 0.82] |
| 3.5 Clinical benefit (randomised) | 11 | 5992 | Odds Ratio (M‐H, Random, 95% CI) | 0.81 [0.67, 0.97] |
| 3.5.1 anastrozole 1 mg | 4 | 2626 | Odds Ratio (M‐H, Random, 95% CI) | 0.74 [0.48, 1.12] |
| 3.5.2 exemestane 25 mg | 3 | 1584 | Odds Ratio (M‐H, Random, 95% CI) | 0.88 [0.71, 1.11] |
| 3.5.3 letrozole 2.5 mg | 4 | 1782 | Odds Ratio (M‐H, Random, 95% CI) | 0.77 [0.61, 0.96] |
| 3.6 Objective response (randomised) | 11 | 5992 | Odds Ratio (M‐H, Random, 95% CI) | 0.80 [0.66, 0.96] |
| 3.6.1 anastrozole 1 mg | 4 | 2626 | Odds Ratio (M‐H, Random, 95% CI) | 0.95 [0.77, 1.17] |
| 3.6.2 exemestane 25 mg | 3 | 1584 | Odds Ratio (M‐H, Random, 95% CI) | 0.68 [0.37, 1.27] |
| 3.6.3 letrozole 2.5 mg | 4 | 1782 | Odds Ratio (M‐H, Random, 95% CI) | 0.65 [0.52, 0.82] |
3.1. Analysis.

Comparison 3: Current AIs versus non‐AI, Outcome 1: Overall survival (reported or calculated)
3.2. Analysis.

Comparison 3: Current AIs versus non‐AI, Outcome 2: Progression‐free survival (reported or calculated)
3.3. Analysis.

Comparison 3: Current AIs versus non‐AI, Outcome 3: Clinical benefit (assessable)
3.4. Analysis.

Comparison 3: Current AIs versus non‐AI, Outcome 4: Objective response (assessable)
3.5. Analysis.

Comparison 3: Current AIs versus non‐AI, Outcome 5: Clinical benefit (randomised)
3.6. Analysis.

Comparison 3: Current AIs versus non‐AI, Outcome 6: Objective response (randomised)
Comparison 4. Current AIs versus non‐AI: Toxicity.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 4.1 hot flushes | 9 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.1.1 AI versus tamoxifen | 3 | 2048 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.13 [0.91, 1.39] |
| 4.1.2 AI versus megestrol acetate | 4 | 2036 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.69 [1.24, 2.30] |
| 4.1.3 AI versus fulvestrant | 2 | 1539 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.81, 1.41] |
| 4.2 nausea | 9 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.2.1 AI versus tamoxifen | 3 | 2048 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.72, 1.11] |
| 4.2.2 AI versus megestrol acetate | 4 | 2036 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.45 [1.09, 1.95] |
| 4.2.3 AI versus fulvestrant | 2 | 1539 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.77, 1.32] |
| 4.3 vomiting | 5 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.3.1 AI versus tamoxifen | 1 | 1017 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.67, 1.72] |
| 4.3.2 AI versus megestrol acetate | 3 | 1636 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.77 [1.11, 2.83] |
| 4.3.3 AI versus fulvestrant | 1 | 846 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.60, 1.35] |
| 4.4 diarrhoea | 7 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.4.1 AI versus tamoxifen | 2 | 1927 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.49 [0.95, 2.35] |
| 4.4.2 AI versus megestrol acetate | 3 | 1278 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.40 [1.34, 4.29] |
| 4.4.3 AI versus fulvestrant | 2 | 1090 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.79, 1.90] |
| 4.5 rash | 4 | Odds Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 4.5.1 AI versus megestrol acetate | 3 | 1636 | Odds Ratio (M‐H, Random, 95% CI) | 1.63 [0.47, 5.70] |
| 4.5.2 AI versus fulvestrant | 1 | 397 | Odds Ratio (M‐H, Random, 95% CI) | 1.39 [0.77, 2.50] |
| 4.6 vaginal bleeding | 3 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.6.1 AI versus tamoxifen | 1 | 1017 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.45 [0.16, 1.32] |
| 4.6.2 AI versus megestrol acetate | 2 | 915 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.29 [0.13, 0.65] |
| 4.7 thromboembolic | 3 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.7.1 AI versus tamoxifen | 1 | 1017 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.53 [0.30, 0.96] |
| 4.7.2 AI versus megestrol acetate | 1 | 515 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.30, 1.73] |
| 4.7.3 AI versus fulvestrant | 1 | 846 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.56, 2.31] |
| 4.8 arthralgia | 3 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.8.1 AI versus tamoxifen | 2 | 1031 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.81, 1.60] |
| 4.8.2 AI versus megestrol acetate | 1 | 363 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.77 [0.89, 3.51] |
4.1. Analysis.

Comparison 4: Current AIs versus non‐AI: Toxicity, Outcome 1: hot flushes
4.2. Analysis.

Comparison 4: Current AIs versus non‐AI: Toxicity, Outcome 2: nausea
4.3. Analysis.

Comparison 4: Current AIs versus non‐AI: Toxicity, Outcome 3: vomiting
4.4. Analysis.
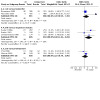
Comparison 4: Current AIs versus non‐AI: Toxicity, Outcome 4: diarrhoea
4.5. Analysis.

Comparison 4: Current AIs versus non‐AI: Toxicity, Outcome 5: rash
4.6. Analysis.

Comparison 4: Current AIs versus non‐AI: Toxicity, Outcome 6: vaginal bleeding
4.7. Analysis.

Comparison 4: Current AIs versus non‐AI: Toxicity, Outcome 7: thromboembolic
4.8. Analysis.

Comparison 4: Current AIs versus non‐AI: Toxicity, Outcome 8: arthralgia
Comparison 5. AI versus different AI.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 5.1 Overall survival (reported) | 2 | HR (IV, Fixed, 95% CI) | Subtotals only | |
| 5.1.1 letrozole | 2 | HR (IV, Fixed, 95% CI) | 0.91 [0.82, 1.02] | |
| 5.2 Progession‐free survival (reported or calculated) | 2 | HR (IV, Fixed, 95% CI) | Subtotals only | |
| 5.2.1 letrozole | 2 | HR (IV, Fixed, 95% CI) | 0.97 [0.90, 1.04] | |
| 5.3 Clinical benefit (assessable) | 5 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.3.1 letrozole | 4 | 1687 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.62, 0.95] |
| 5.3.2 anastrozole | 2 | 663 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.92, 1.79] |
| 5.4 Objective response (assessable) | 5 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.4.1 letrozole | 4 | 1687 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.62 [0.50, 0.78] |
| 5.4.2 anastrozole | 2 | 663 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.59 [1.07, 2.37] |
| 5.5 Clinical benefit (randomised) | 5 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.5.1 letrozole | 4 | 2098 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.68, 0.98] |
| 5.5.2 anastrozole | 2 | 773 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.90, 1.72] |
| 5.6 Objective response (randomised) | 5 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.6.1 letrozole | 4 | 2098 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.54, 0.82] |
| 5.6.2 anastrozole | 2 | 782 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.50 [1.01, 2.23] |
5.1. Analysis.

Comparison 5: AI versus different AI, Outcome 1: Overall survival (reported)
5.2. Analysis.

Comparison 5: AI versus different AI, Outcome 2: Progession‐free survival (reported or calculated)
5.3. Analysis.

Comparison 5: AI versus different AI, Outcome 3: Clinical benefit (assessable)
5.4. Analysis.

Comparison 5: AI versus different AI, Outcome 4: Objective response (assessable)
5.5. Analysis.

Comparison 5: AI versus different AI, Outcome 5: Clinical benefit (randomised)
5.6. Analysis.

Comparison 5: AI versus different AI, Outcome 6: Objective response (randomised)
Comparison 6. AI as first‐line therapy versus any other therapy (tamoxifen).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 6.1 Overall survival (reported or calculated) | 3 | HR (IV, Fixed, 95% CI) | 0.99 [0.86, 1.14] | |
| 6.1.1 aminoglutethimide as first‐line therapy | 1 | HR (IV, Fixed, 95% CI) | 1.12 [0.82, 1.53] | |
| 6.1.2 anastrozole as first‐line therapy | 1 | HR (IV, Fixed, 95% CI) | 0.97 [0.81, 1.16] | |
| 6.1.3 fadrozole as first‐line therapy | 1 | HR (IV, Fixed, 95% CI) | 0.91 [0.63, 1.32] | |
| 6.2 Progression‐free survival (reported or calculated) | 4 | HR (IV, Fixed, 95% CI) | 0.78 [0.71, 0.86] | |
| 6.2.1 aminoglutethimide | 1 | HR (IV, Fixed, 95% CI) | 0.84 [0.65, 1.08] | |
| 6.2.2 formestane as first‐line therapy | 1 | HR (IV, Fixed, 95% CI) | 0.93 [0.68, 1.28] | |
| 6.2.3 anastrozole as first‐line therapy | 1 | HR (IV, Fixed, 95% CI) | 0.82 [0.71, 0.95] | |
| 6.2.4 letrozole as first‐line therapy | 1 | HR (IV, Fixed, 95% CI) | 0.70 [0.60, 0.82] | |
| 6.3 Clinical benefit (assessable) | 9 | 3252 | Odds Ratio (M‐H, Random, 95% CI) | 0.69 [0.51, 0.92] |
| 6.3.1 aminoglutethimide (any dose) | 3 | 479 | Odds Ratio (M‐H, Random, 95% CI) | 0.63 [0.42, 0.93] |
| 6.3.2 formestane 250 mg | 1 | 348 | Odds Ratio (M‐H, Random, 95% CI) | 1.36 [0.87, 2.13] |
| 6.3.3 anastrozole 1 mg | 2 | 1259 | Odds Ratio (M‐H, Random, 95% CI) | 0.48 [0.16, 1.44] |
| 6.3.4 exemestane 25 mg | 1 | 113 | Odds Ratio (M‐H, Random, 95% CI) | 0.47 [0.22, 0.99] |
| 6.3.5 fadrozole 2 mg | 1 | 209 | Odds Ratio (M‐H, Random, 95% CI) | 1.09 [0.58, 2.06] |
| 6.3.6 letrozole 2.5 mg | 1 | 844 | Odds Ratio (M‐H, Random, 95% CI) | 0.63 [0.48, 0.82] |
| 6.4 Objective response (assessable) | 11 | 3503 | Odds Ratio (M‐H, Random, 95% CI) | 0.77 [0.59, 1.00] |
| 6.4.1 aminoglutethimide (any dose) | 4 | 656 | Odds Ratio (M‐H, Random, 95% CI) | 0.75 [0.45, 1.25] |
| 6.4.2 formestane 250 mg | 1 | 348 | Odds Ratio (M‐H, Random, 95% CI) | 1.20 [0.77, 1.87] |
| 6.4.3 anastrozole 1 mg | 2 | 1259 | Odds Ratio (M‐H, Random, 95% CI) | 0.85 [0.65, 1.11] |
| 6.4.4 exemestane 25 mg | 1 | 113 | Odds Ratio (M‐H, Random, 95% CI) | 0.26 [0.11, 0.62] |
| 6.4.5 fadrozole 2 mg | 2 | 283 | Odds Ratio (M‐H, Random, 95% CI) | 1.20 [0.69, 2.09] |
| 6.4.6 letrozole 2.5 mg | 1 | 844 | Odds Ratio (M‐H, Random, 95% CI) | 0.58 [0.42, 0.78] |
| 6.5 Clinical benefit (randomised) | 9 | 3451 | Odds Ratio (M‐H, Random, 95% CI) | 0.74 [0.56, 0.98] |
| 6.5.1 aminoglutethimide (any dose) | 3 | 533 | Odds Ratio (M‐H, Random, 95% CI) | 0.74 [0.51, 1.08] |
| 6.5.2 formestane 250 mg | 1 | 409 | Odds Ratio (M‐H, Random, 95% CI) | 1.25 [0.85, 1.86] |
| 6.5.3 anastrozole 1 mg | 2 | 1259 | Odds Ratio (M‐H, Random, 95% CI) | 0.48 [0.16, 1.44] |
| 6.5.4 exemestane 25 mg | 1 | 122 | Odds Ratio (M‐H, Random, 95% CI) | 0.55 [0.27, 1.13] |
| 6.5.5 fadrozole 2 mg | 1 | 221 | Odds Ratio (M‐H, Random, 95% CI) | 1.23 [0.69, 2.21] |
| 6.5.6 letrozole 2.5 mg | 1 | 907 | Odds Ratio (M‐H, Random, 95% CI) | 0.65 [0.50, 0.84] |
| 6.6 Objective response (randomised) | 11 | 3746 | Odds Ratio (M‐H, Random, 95% CI) | 0.81 [0.62, 1.05] |
| 6.6.1 aminoglutethimide (any dose) | 4 | 748 | Odds Ratio (M‐H, Random, 95% CI) | 0.83 [0.48, 1.45] |
| 6.6.2 formestane 250 mg | 1 | 409 | Odds Ratio (M‐H, Random, 95% CI) | 1.18 [0.77, 1.80] |
| 6.6.3 anastrozole 1 mg | 2 | 1259 | Odds Ratio (M‐H, Random, 95% CI) | 0.85 [0.65, 1.11] |
| 6.6.4 exemestane 25 mg | 1 | 122 | Odds Ratio (M‐H, Random, 95% CI) | 0.30 [0.13, 0.69] |
| 6.6.5 fadrozole 2 mg | 2 | 301 | Odds Ratio (M‐H, Random, 95% CI) | 1.28 [0.76, 2.15] |
| 6.6.6 letrozole 2.5 mg | 1 | 907 | Odds Ratio (M‐H, Random, 95% CI) | 0.59 [0.43, 0.79] |
6.1. Analysis.

Comparison 6: AI as first‐line therapy versus any other therapy (tamoxifen), Outcome 1: Overall survival (reported or calculated)
6.2. Analysis.

Comparison 6: AI as first‐line therapy versus any other therapy (tamoxifen), Outcome 2: Progression‐free survival (reported or calculated)
6.3. Analysis.

Comparison 6: AI as first‐line therapy versus any other therapy (tamoxifen), Outcome 3: Clinical benefit (assessable)
6.4. Analysis.

Comparison 6: AI as first‐line therapy versus any other therapy (tamoxifen), Outcome 4: Objective response (assessable)
6.5. Analysis.

Comparison 6: AI as first‐line therapy versus any other therapy (tamoxifen), Outcome 5: Clinical benefit (randomised)
6.6. Analysis.

Comparison 6: AI as first‐line therapy versus any other therapy (tamoxifen), Outcome 6: Objective response (randomised)
Comparison 7. AI as second‐line therapy versus any other therapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 7.1 Overall survival (reported or calculated) | 2 | HR (IV, Fixed, 95% CI) | 0.80 [0.66, 0.96] | |
| 7.1.1 anastrozole as second‐line therapy | 1 | HR (IV, Fixed, 95% CI) | 0.78 [0.61, 1.00] | |
| 7.1.2 letrozole as second‐line therapy | 1 | HR (IV, Fixed, 95% CI) | 0.82 [0.63, 1.07] | |
| 7.2 Progression‐free survival (reported or calculated) | 8 | HR (IV, Random, 95% CI) | 1.08 [0.94, 1.23] | |
| 7.2.1 aminoglutethimide (any dose) | 1 | HR (IV, Random, 95% CI) | 1.25 [0.91, 1.72] | |
| 7.2.2 formestane 250 mg biweekly | 2 | HR (IV, Random, 95% CI) | 1.03 [0.90, 1.19] | |
| 7.2.3 anastrozole 1 mg | 1 | HR (IV, Random, 95% CI) | 1.34 [1.16, 1.55] | |
| 7.2.4 exemestane 25 mg | 2 | HR (IV, Random, 95% CI) | 0.91 [0.72, 1.14] | |
| 7.2.5 letrozole 2.5 mg | 1 | HR (IV, Random, 95% CI) | 0.98 [0.77, 1.25] | |
| 7.2.6 vorozole 2.5 mg | 1 | HR (IV, Random, 95% CI) | 1.27 [1.04, 1.56] | |
| 7.3 Clinical benefit (assessable) | 16 | 5410 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.88, 1.11] |
| 7.3.1 aminoglutethimide (any dose) | 4 | 686 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.66, 1.23] |
| 7.3.2 formestane 250 mg biweekly | 1 | 173 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.41, 1.39] |
| 7.3.3 anastrozole 1mg | 2 | 1367 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.84, 1.29] |
| 7.3.4 exemestane 25 mg | 2 | 1243 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.75, 1.20] |
| 7.3.5 fadrozole 2 mg | 3 | 773 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.77, 1.41] |
| 7.3.6 letrozole 2.5 mg | 3 | 793 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.68, 1.23] |
| 7.3.7 vorozole 2.5mg | 1 | 375 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.35 [0.88, 2.07] |
| 7.4 Objective response (assessable) | 18 | 5937 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.86, 1.13] |
| 7.4.1 aminoglutethimide (any dose) | 5 | 734 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.68, 1.30] |
| 7.4.2 formestane 250 mg biweekly | 2 | 652 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.24 [0.84, 1.83] |
| 7.4.3 anastrozole 1 mg | 2 | 1367 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.84, 1.50] |
| 7.4.4 exemestane 25 mg | 2 | 1243 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.63, 1.26] |
| 7.4.5 fadrozole 2 mg | 3 | 773 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.17 [0.76, 1.80] |
| 7.4.6 letrozole 2.5 mg | 3 | 793 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.53, 1.08] |
| 7.4.7 vorozole 2.5 mg | 1 | 375 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.70 [0.34, 1.42] |
| 7.5 Clinical benefit (randomised) | 16 | 6432 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.90, 1.11] |
| 7.5.1 aminoglutethimide (any dose) | 4 | 1320 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.85, 1.31] |
| 7.5.2 formestane 250 mg biweekly | 1 | 177 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.40, 1.31] |
| 7.5.3 anastrozole 1 mg | 2 | 1367 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.84, 1.29] |
| 7.5.4 exemestane 25 mg | 2 | 1462 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.74, 1.16] |
| 7.5.5 fadrozole 2 mg | 3 | 779 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.77, 1.41] |
| 7.5.6 letrozole 2.5 mg | 3 | 875 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.68, 1.21] |
| 7.5.7 vorozole 2.5mg | 1 | 452 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.83, 1.88] |
| 7.6 Objective response (randomised) | 18 | 7113 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.92, 1.18] |
| 7.6.1 aminoglutethimide (any dose) | 5 | 1475 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.15 [0.91, 1.45] |
| 7.6.2 formestane 250 mg biweekly | 2 | 724 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.84, 1.79] |
| 7.6.3 anastrozole 1 mg | 2 | 1367 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.84, 1.50] |
| 7.6.4 exemestane 25 mg | 2 | 1462 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.62, 1.24] |
| 7.6.5 fadrozole 2 mg | 3 | 779 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.17 [0.76, 1.80] |
| 7.6.6 letrozole 2.5 mg | 3 | 854 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.56, 1.13] |
| 7.6.7 vorozole 2.5 mg | 1 | 452 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.33, 1.37] |
7.1. Analysis.

Comparison 7: AI as second‐line therapy versus any other therapy, Outcome 1: Overall survival (reported or calculated)
7.2. Analysis.

Comparison 7: AI as second‐line therapy versus any other therapy, Outcome 2: Progression‐free survival (reported or calculated)
7.3. Analysis.

Comparison 7: AI as second‐line therapy versus any other therapy, Outcome 3: Clinical benefit (assessable)
7.4. Analysis.

Comparison 7: AI as second‐line therapy versus any other therapy, Outcome 4: Objective response (assessable)
7.5. Analysis.

Comparison 7: AI as second‐line therapy versus any other therapy, Outcome 5: Clinical benefit (randomised)
7.6. Analysis.

Comparison 7: AI as second‐line therapy versus any other therapy, Outcome 6: Objective response (randomised)
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Alonso‐Munoz 1988.
| Study characteristics | ||
| Methods | Spain, multicentre, N = 105, Dec 1982 ‐ Dec 1985 Three arm trial (only two arms included in review N = 70) Randomisation method not given Baseline characteristics balanced | |
| Participants | Age range 37 ‐ 75y Proven metastatic breast cancer, measurable disease sites No previous endocrine therapy | |
| Interventions | AG (500mg for 2w, then 100mg) versus TAM 40mg versus AG + TAM 40mg Numbers in each treatment arm: 35 versus 35 versus 35 (AG+TAM arm data excluded from review N = 35) Assessable patients (two included arms): 31 versus 34 Patients evaluable for toxicity (two included arms): 33 versus 34 | |
| Outcomes | Toxicity, TTP, response rate Not survival | |
| Notes | 11 not evaluable (4 AG, 6 TAM + AG, 1 TAM) due to: 4 died within 6w, 1 discontinued treatment, 5 toxicity, 1 lost to FU FU duration not given TTP not given by treatment arm | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Blinding (performance bias and detection bias) All outcomes | High risk | |
Bezwoda 1998.
| Study characteristics | ||
| Methods | South Africa, multicentre, N = 96 Double‐blind, double‐dummy Balanced block stratification by centre Baseline slight imbalance in ER status: 28% versus 20% ER+ | |
| Participants | Age range 44 ‐ 82y Measurable or evaluable metastatic breast cancer Prior TAM treatment No previous treatment with AI ECOG perf status < 3 | |
| Interventions | Fadrozole 2mg versus MA 160mg Numbers in each treatment arm: 46 versus 50 Assessable patients: 46 versus 50 Patients evaluable for toxicity: 46 versus 50 Treatment until progression or for 1y; median duration 20w | |
| Outcomes | Primary ‐ response rate, TTP, TTF, survival Secondary ‐ QOL, performance status, pain assessment | |
| Notes | FU to relapse or death Median FU not stated Intention‐to‐treat analysis Subsidiary analysis on a per protocol basis (41 versus 43) 7 major protocol violations, 2 refusals, 1 early death, 1 lost to FU (numbers not consistent) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | balanced block stratification by centre |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind, double‐dummy |
Bonneterre 2001.
| Study characteristics | ||
| Methods | International, multicentre trial, combined results of two trials Feb 1996 ‐ July 1998 97 sites in US and Canada, N = 353 83 sites in Europe, Australia, New Zealand, South Africa, South Amercia, N = 668 Total randomised = 1021 Double‐blind, double‐dummy Baseline characteristics well‐balanced | |
| Participants | Age range 30 ‐ 92y Advanced or metastatic breast cancer | |
| Interventions | Anastrozole 1mg versus TAM 20mg Numbers in each treatment arm: 171 versus 182 (N America) and 340 versus 328 (rest of world) Assessable patients: 511 versus 510 Patients evaluable for toxicity: 506 versus 511 Treatment continued until disease progression | |
| Outcomes | Primary ‐ objective response, TTP, tolerability Secondary ‐ TTF, survival | |
| Notes | FU to progression and death Median FU not known Number of dropouts not given | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind, double‐dummy |
Buzdar 1996a.
| Study characteristics | ||
| Methods | International, multicentre. 122 centres: 49 in North America, 73 in Europe, Australia, South Africa, Double‐blind anastrozole, open megestrol acetate Randomisation method ‐ blocks of 6 (Europe), blocks of 3 (N America), parallel groups Two trials combined (N = 764): North America (N = 346) and Europe, Australia, South Africa (N = 378) Three‐arm trial (only two arms included in review N = 516) Baseline: apparent imbalance in one treatment group (believed to be artefact) | |
| Participants | Age range 29 ‐ 97y Advanced breast cancer Progressed on anti‐oestrogen for advanced disease or progressed on or during adjuvant TAM WHO perf status < 3 | |
| Interventions | anastrozole 1mg versus anastrozole 10mg versus MA 160mg Numbers in each treatment arm: 263 versus 248 versus 253 (anastrozole 10mg arm excluded from review N = 248) Assessable patients (two included arms): 263 versus 253 Patients evaluable for toxicity (two included arms): 262 versus 253 Treatment continued until disease progression or withdrawal from treatment for other reasons | |
| Outcomes | Primary ‐ TTP, tumour response, tolerability Secondary ‐ TTF, response duration, survival Clinical assessment every 4w until week 24, every 12w until week 48, then every 3m until progression | |
| Notes | FU median duration 6m 3 no treatment, 1 wrong treatment, 8 lost to FU Intention‐to‐treat analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | blocks of 6 (Europe), blocks of 3 (N America), parallel groups |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind anastrozole, open megestrol acetate |
Buzdar 1996b.
| Study characteristics | ||
| Methods | Protocol 03 Multicentre, 47 sites, N = 380 Feb 1989 ‐ Dec 1991 Double‐blind, parallel, controlled equivalence Randomisation method not specified | |
| Participants | Age range 35 ‐ 92y Metastatic breast cancer At least one prior hormonal treatment for metastic disease more than 3m previously Prior AI use an exclusion Performance status < 3 | |
| Interventions | Fadrozole 2mg versus MA 160mg Numbers in each treatment arm: 196 versus 184 Drug code broken 18m after end of enrolment Assessable patients: 195 versus 184 Patients evaluable for toxicity: 196 versus 184 Treatment continued until disease progression | |
| Outcomes | Objective response rate, TTP, survival, toxicity, duration of response, survival, QOL | |
| Notes | Published together with protocol 06 (Buzdar 1996c) FU until progression Intention‐to‐treat analysis N = 379 1 patient excluded but included in safety and tolerability | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | randomisation method not specified |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind, parallel, controlled equivalence |
Buzdar 1996c.
| Study characteristics | ||
| Methods | Protocol 06 Multicentre, 55 sites, N = 303 Oct 1989 ‐ Aug 1992 Double‐blind, parallel, controlled equivalence Randomisation method not specified | |
| Participants | Age range 36 ‐ 92y Metastatic breast cancer At least one prior hormonal treatment for metastic disease more than 3m previously Prior AI use an exclusion Performance status<3 | |
| Interventions | Fadrozole 2mg versus MA 160mg Numbers in each treatment arm: 152 versus 151 Assessable patients: 150 versus 148 Patients evaluable for toxicity:152 versus 151 Drug code broken 18m after end of enrolment Treatment continued until disease progression | |
| Outcomes | Primary ‐ overall tumour response (TTP, TTF, survival) Other ‐ earliest diagnosis of PD, tolerability, safety, QOL | |
| Notes | Published together with protocol 03 (Buzdar 1996b) FU: 33m for tumour response/safety (median 5.5m) 45m for survival (median 18 to 20m) Intention‐to‐treat analysis N = 298 Not designed or powered to detect differences in survival | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | randomisation method not specified |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind, parallel, controlled equivalence |
Buzdar 2001.
| Study characteristics | ||
| Methods | International, multicentre, 120 sites in US, Canada, Europe, N = 602 Three‐arm trial (only two arms included in review N = 400) Double‐blind, double dummy, phase III Randomisation by country w/o stratification by centre Enrolment over 30 months Baseline characteristics no imbalance | |
| Participants | Age range not given Locally advanced/locoregionally recurrent/metastatic breast cancer At least one measurable/assessable lesion Relapsed or progressed while on anti‐oestrogen or relapsed within 12m of stopping antioestrogen Chemotherapy for advanced disease allowed KPF >=50% | |
| Interventions | Letrozole 2mg versus letrozole 10mg versus MA 160mg Numbers in each treatment arm: 202 versus 199 versus 201 (letrozole 2mg arm excluded from review N = 202) Assessable patients: 182 versus 180 Patients evaluable for toxicity: 199 versus 201 Treatment continued until disease progression or withdrawal for other reason | |
| Outcomes | Primary ‐ tumour response Secondary ‐ TTF, TTP, survival, QOL | |
| Notes | FU period 48m after the first visit of the last patient randomised Intention‐to‐treat analysis 23 ineligible and excluded from tumour analyses | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | randomisation by country w/o stratification by centre |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind, double‐dummy |
Canney 1988.
| Study characteristics | ||
| Methods | UK, number of centres not given, N = 218 Randomised without stratification, performed centrally by phone over 24m | |
| Participants | Median age 64y Actively progressive disease Received hormonal therapy with tamoxifen Received no anticancer therapy within preceding 4w | |
| Interventions | AG (250mg for 2w, increased to 500mg if not toxic effect plus 40mg HC) versus high dose MPA 1000mg Numbers in each treatment arm: 106 versus 112 Patients evaluable for toxicity: 106 versus 112 | |
| Outcomes | Duration of response, survival, time to response | |
| Notes | FU duration: minumum 9m, median 55w for AG, 57w MPA 7 patients either violated protocol or did not meet entry criteria but included in analyses Crossover on failure No variation between groups in known prognostic variables | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | performed centrally by phone |
Chia 2008.
| Study characteristics | ||
| Methods | International, multicentre, 138 centres, N = 693 Aug 2003 ‐ Nov 2005 Double‐blind, double‐dummy, phase III Trial acronym = EFECT Randomisation method not given Baseline characteristics well balanced except for ER+/PR+ ( 56.4% versus 67.5%) | |
| Participants | Age range 32 ‐91y Locally advanced or metastatic disease Disease progression after prior non‐steroidal AI treatment At least one measurable or assessable lesion ER+/PR+ WHO perf status < 3 | |
| Interventions | Exemestane 25mg versus fulvestrant 500mg on day 0, 250mg on days 14 and 28, followed by 250mg every four weeks Numbers in each treatment arm: 342 versus 351 Assessable patients: 270 versus 270 Treatment continued until disease progression | |
| Outcomes | Primary ‐ TTP Secondary ‐ objective response, CB, response duration, TTF, overall survival, tolerability, QOL | |
| Notes | FU until death Intention‐to‐treat analysis 90% power to detect HR≥1.31 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind, double‐dummy |
Dombernowsky 1998.
| Study characteristics | ||
| Methods | International, multicentre, Mar 1993 ‐ Sep 1994 10 countries, 91 sites, N = 551 Three‐arm trial (only two arms included in review N=363) Double‐blind, randomisation stratified by country; computer‐generated permuted blocks of size 6 or 3, 1:1:1 allocation Baseline characteristics balanced | |
| Participants | Advanced/locoregionally recurrent/metastatic breast cancer Measurable/assessable disease Failure to respond to previous antioestrogen WHO perf status < 3 | |
| Interventions | Letrozole 0.5mg versus letrozole 2.5mg versus MA 160mg Numbers in each treatment arm: 188 versus 174 versus 189 (letrozole 0.5mg arm excluded from review N = 188) Assessable patients: 153 versus 166 Patients evaluable for toxicity: 174 versus 189 | |
| Outcomes | Primary ‐ overall tumour response (TTP, TTF, survival) Other ‐ earliest diagnosis of PD, tolerability, safety | |
| Notes | FU: 33m for tumour response/safety (median 5.5m) 45m for survival (median 18 to 20m) Intention‐to‐treat analysis Not designed or powered to detect differences in survival as significant | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | stratified by country; computer‐generated permuted blocks of size 6 or 3, 1:1:1 allocation |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind |
Falkson 1996.
| Study characteristics | ||
| Methods | South Africa, single centre, N = 80 Sep 1991 ‐ Dec 1994 Randomisation method not given Baseline: difference of 10y in median age of patients in arm 1 versus arm 2 | |
| Participants | Age range 43 ‐ 90y Progressive, inoperable, recurrent or metastatic breast cancer No prior treatment for advanced disease ECOG perf status < 3 | |
| Interventions | Fadrozole 2mg versus TAM 20mg Numbers in each treatment arm: 40 versus 40 Assessable patients: 36 versus 38 Patients evaluable for toxicity: 40 versus 40 Minimum treatment 8w | |
| Outcomes | Survival, TTF, duration of overall response, toxicity, objective response rates | |
| Notes | FU 14 to 1122d, median FU 153d Intention‐to‐treat analysis 2 ineligible, 1 lost to FU 74 patients evaluable | |
Freue 2000.
| Study characteristics | ||
| Methods | International, multicentre, 9 countries, 78 centres, N = 547
Aug 1991 ‐ Mar 1995
Computer‐generated random allocation w/o stratification Open study No difference in baseline characteristics |
|
| Participants | Age range not given Advanced disease Measurable disease ER/PR positive or unknown WHO perf status < 3 Only TAM as 1st line endocrine therapy | |
| Interventions | Formestane 250mg im every 2w versus MA 160mg Numbers in each treatment arm: 276 versus 271 Assessable patients: 242 versus 237 Numbers for safety analysis: 276 versus 271 Treatment duration 12m | |
| Outcomes | TTF, TTP, overall survival, overall response | |
| Notes | FU until death Median FU not given 90% power to detect 33% difference in median TTF Intention‐to‐treat analysis Ineligible/non‐evaluable: 34 versus 34 Non‐cancer deaths: 2 versus 4 Discontinued for AE: 3 versus 13 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | computer‐generated random allocation without stratification |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | High risk | open |
Gale 1994.
| Study characteristics | ||
| Methods | ECOG trial, multicentre, US, N = 249 1977 ‐ 1983 Stratified randomly permuted blocks of four Baseline characteristics relatively evenly balanced One institution had 60% versus 4% response rates | |
| Participants | Age range not given Progressive, recurrent, metastatic breast cancer Measurable disease ECOG perf status < 4 No previous treatment with AG or TAM | |
| Interventions | AG 250mg qid versus TAM 20mg Numbers in each treatment arm: 122 versus 119 Assessable patients: 108 versus 108 | |
| Outcomes | Tumour response, TTF, overall survival | |
| Notes | Initial trial design changed in May 1979 (adrenalectomy treatment arm discontinued) Crossover on progression Crossover results not included Intention‐to‐treat analysis Adrenalectomy patients (N = 8) were excluded | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | stratified randomly permuted blocks of four |
| Allocation concealment (selection bias) | Low risk | adequate |
Garcia‐Giralt 1992.
| Study characteristics | ||
| Methods | France, multicentre, N = 257 No randomisation details | |
| Participants | Age range 36 ‐ 91y Histologically confirmed metastatic breast cancer ER+/PR+ Initial response to TAM before relapse | |
| Interventions | AG 500mg + HC versus MPA 1000mg Numbers in each treatment arm: 131 versus 119 Assessable patients: 124 versus 112 Second‐line therapy after TAM | |
| Outcomes | Tumour response, TTP, new metastases, AEs | |
| Notes | Median FU not known Treatment until progression Crossover on progression 6 lost to FU, 1 man | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | not used |
Gershanovich 1998.
| Study characteristics | ||
| Methods | International, multicentre, 11 countries, 86 sites N = 555 Three‐arm trial (only two arms included in review N = 363) Open‐label 1:1:1 Baseline no major differences | |
| Participants | Median age letrozole 2.5mg 66y, letrozole 0.5 mg 64y, AG 65y Advanced or metastatic breast cancer Measurable/evaluable advanced disease WHO perf status < 3 | |
| Interventions | Letrozole 2.5mg versus letrozole 0.5mg versus AG 500 mg Numbers in each treatment arm: 185 versus 192 versus 178 (letrozole 2.5mg arm excluded from review N = 192) Assessable patients: 173 versus 162 | |
| Outcomes | Response, TTP, TTF, survival, tolerability and safety, overall survival | |
| Notes | FU duration median > 20m 44 not assessable, counted as non‐responders in the analysis Median duration of treatment 5m Modified intention‐to‐treat population ie enrolled and received trial medication | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Blinding (performance bias and detection bias) All outcomes | High risk | |
Goss 1999.
| Study characteristics | ||
| Methods | Nov 1991 ‐ Dec 1995 Multicentre, 29 sites in Canada and 38 in US, N = 452 Open‐label, stratified by disease status Baseline characteristics comparable | |
| Participants | Age range 39 ‐ 90y Advanced breast cancer, histologically confirmed Progressed after tamoxifen treatment | |
| Interventions | Vorozole 2.5mg versus MA 160mg Numbers in each treatment arm: 225 versus 227 Assessable patients: 190 versus 185 Patients evaluable for toxicity: 195 versus 198 2nd line treatment after tamoxifen | |
| Outcomes | Primary ‐ response rate Secondary ‐ TTP, survival, duration of response, safety subjective symptoms, QOL | |
| Notes | Median FU 11.6m (vorozole), 9.9m (MA) 1 withdrawn before treatment 4 ineligible, 18 adverse events, 1 lost to FU, 18 other | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | stratified by disease status |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | High risk | open‐label |
Goss 2007.
| Study characteristics | ||
| Methods | Multinational, multicentre, 60 centres in US, Canada, Russia, Ukraine, N = 865 Randomised, double‐blind, active control, phase III Randomisation in blocks of four, stratified by centre. Performed centrally, site notified by fax Treatment code unblinded after database lock Baseline characteristics well balanced | |
| Participants | Median age letrozole 63y atamestane 65y Locally recurrent/advanced/ metastatic disease Measurable disease No AI or antioestrogen/SERM treatment in previous 12m ECOG perf status < 3 | |
| Interventions | Letrozole 2.5mg versus atamestane 500mg + toremifene 60mg Numbers in each treatment arm: 431 versus 434 Assessable patients: 297 versus 298 | |
| Outcomes | Primary ‐ TTP Secondary ‐ overall survival, TTF, tumour response, toxicity | |
| Notes | FU to death Intention‐to‐treat analysis Treatment continued until disease progression or withdrawal for other reasons 80% power to detect a 24% increase in TTP | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | blocks of four, stratified by centre |
| Allocation concealment (selection bias) | Low risk | performed centrally, site notified by fax |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind |
Ingle 1986.
| Study characteristics | ||
| Methods | US, number of centres not known, N = 102 Randomised using Pocock‐Simon approach to adaptive randomisation, stratified | |
| Participants | Age range 38 ‐ 83y Progressive metastatic disease Measurable or evaluable lesion ECOG perf status < 4 No prior therapy with either AG or TAM | |
| Interventions | TAM 20mg versus TAM (20mg) + AG (500mg for 2 weeks then 1000mg) + HC (100mg daily for 2 weeks then 40mg) Numbers in each treatment arm: 49 versus 51 Assessable patients:49 versus 51 Patients evaluable for toxicity: 48 versus 46 | |
| Outcomes | Objective response, TTP, survival, toxicity | |
| Notes | No data on duration of FU Target accrual = 160 but terminated early due to excess toxicity on the TAM + AG + HC arm 2 patients ineligible | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | used Pocock‐Simon approach to adaptive randomisation, stratified |
Kaufmann 2000.
| Study characteristics | ||
| Methods | International, multicentre, Oct 1995 ‐ May 1998 19 countries, 144 centres N = 769 Double‐blind, parallel‐group, phase III Baseline characteristics comparable | |
| Participants | Age range 30 ‐ 91y Advanced breast cancer Progressed or relapsed during tamoxifen treatment | |
| Interventions | Exemestane 25mg versus MA 160mg Numbers in each treatment arm: 366 versus 403 Assessable patients: 337 versus 366 Patients evaluable for toxicity: 358 versus 400 | |
| Outcomes | Objective response, TTP, TTF, survival, tumour response, duration of tumour control, tumour related signs and symptoms, QOL, tolerability | |
| Notes | FU median duration 48.9w 6 randomised but not treated 66 not evaluable for tumour response Intention‐to‐treat analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind |
Kleeberg 1997.
| Study characteristics | ||
| Methods | International, multicentre, 27 Jun ‐ 1 Dec 1995 18 centres, Europe and South Africa, N = 60 open‐label, parallel‐group, comparative Baseline good balance re age, weight, prior tamoxifen treatment | |
| Participants | Age range 40 ‐ 84y Advanced breast cancer Measurable or evaluable disease | |
| Interventions | Anastrozole 1mg oral per day versus formestane 250mg im every 2w Numbers in each treatment arm: 29 versus 31 Assessable patients: 29 versus 31 Treatment until disease progression | |
| Outcomes | Primary ‐ oestradiol suppression and tolerability Secondary ‐ response rates, TTP, adverse events, blood oestrone sulphate, patient and doctor perception of treatment | |
| Notes | No details re randomisation exclusions or FU Not powered to detect clinically significant difference in oestrogen suppression between the two arms | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Blinding (performance bias and detection bias) All outcomes | High risk | open‐label |
Leitzel 1995.
| Study characteristics | ||
| Methods | Location and date of trial not given Multicentre, N = 300 Double‐blind, double‐dummy, parallel Randomisation method not given | |
| Participants | Age range 18 ‐ 85y Metastatic breast cancer ECOG < 3 | |
| Interventions | Fadrozole 2mg versus MA 160mg Numbers in each treatment arm not given Duration of intervention not given Second‐line treatment | |
| Outcomes | Tumour response, progression, c‐erbB‐2 antigen in serum | |
| Notes | FU until death Results not given by treatment group Survival was not given by treatment group although it was measured | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind, double‐dummy |
Lundgren 1989.
| Study characteristics | ||
| Methods | Norway, multicentre, N = 176 Randomisation without stratification, details not given Baseline characteristics well balanced for most important prognostic variables, except main metastatic site | |
| Participants | Mean age 62.0y versus 62.7y Advanced breast cancer Evaluable disease Previous treatment with TAM KPS >50 | |
| Interventions | AG 250mg bid for 2w then 250mg qid versus MA 160mg Numbers in each treatment arm: 86 versus 90 Assessable patients: 76 versus 74 Second‐line treatment | |
| Outcomes | Response rate, reponse duration, survival, toxicity | |
| Notes | Intention‐to‐treat analysis Excluded patients: 10 protocol violations/patient refusal; 12 early deaths; 4 adverse events | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | randomisation without stratification, details not given |
| Allocation concealment (selection bias) | Unclear risk | not used |
Mauriac 2003.
| Study characteristics | ||
| Methods | Data were combined and published from two trials 0020 and 0021 (May 1997 ‐ September 1999) Trial 0020: multicentre, phase III, open, parallel group Europe, Australia and South Africa, 83 centres, N = 451 Trial 0021: multicentre, phase III, double‐blind, double‐dummy, parallel group North America, N = 400 Combined data from both trials included in review N = 851 | |
| Participants | Age range 33 ‐ 89y Locally advanced or metastatic breast cancer Progressed during adjuvant endocrine therapy or first‐line therapy for advanced disease WHO performance status < 3 | |
| Interventions | Anastrozole 1mg versus fulvestrant 250mg/month im Trial 0020: numbers in each treatment arm: 222 versus 229 Trial 0021: numbers in each treatment arm: 206 versus 194 Combined trials (included in review): numbers in each treatment arm: 423 versus 428 Assessable patients: 423 versus 428 Patients evaluable for toxicity: 423 versus 423 Continued until objective disease progression or other events required withdrawal | |
| Outcomes | TTP, objective response, tolerability, QOL | |
| Notes | Median FU 15.1m (combined data) Intention‐to‐treat analysis Additional to protocol: non‐inferiority of fulvestrant with anastrozole was carried out retrospectively | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Trial 0020 open Trial 0021 double‐blind |
Mercer 1993.
| Study characteristics | ||
| Methods | UK, query single‐centre, Jan 1987 ‐ Dec 1990, N = 61 No information regarding randomisation Groups well matched but after exclusions numbers small | |
| Participants | Eligibility >50y Age range 45 ‐ 86y Advanced breast cancer Progressive disease on tamoxifen (adjuvant or treatment) | |
| Interventions | Low dose AG 125mg versus HC 20mg Number in each treatment arm: 28 versus 33 Assessable patients: 27 versus 29 | |
| Outcomes | Tumour response, TTF, side‐effects, overall survival | |
| Notes | FU details not given 5 patients excluded | |
Milla‐Santos 2003.
| Study characteristics | ||
| Methods | Spain, single‐centre, N = 238, May 1997 ‐ Dec 1999 Randomisation following Meinert's methodology. Baseline characteristics comparable | |
| Participants | Age range 55 ‐ 77y Histologically confirmed advanced breast cancer, measurable disease sites No previous endocrine therapy ECOG<3 | |
| Interventions | Anastrozole 1mg versus TAM 40mg Numbers in each treatment arm: 121 versus 117 Assessable patients: 121 versus 117 | |
| Outcomes | Primary ‐ response rates, clinical benefit, TTP in patients achieving a CB, overall survival, toxicity | |
| Notes | FU to 35m intention‐to‐treat analysis All patients evaluable Analysis cutoff 1 April 2001 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | randomisation following Meinert's methodology |
Mourisden 2001.
| Study characteristics | ||
| Methods | International, multicentre, Nov 1996 ‐ Jan 1999 29 countries, 201 sites, N = 939 Double‐blind, double‐dummy, parallel group Baseline characteristics well balanced | |
| Participants | Age range 31 ‐ 96y Locally advanced/locoregionally recurrent/metastatic breast cancer which is measurable/assessable Previous chemotherapy allowed for advanced disease WHO perf status < 3 | |
| Interventions | Letrozole 2.5mg versus TAM 20mg Numbers in each treatment arm: 453 versus 454 Assessable patients: 421 versus 423 Patients evaluable for toxicity: 455 versus 455 Treatment continued until disease progression | |
| Outcomes | Primary ‐ TTP Secondary ‐ tumour response rate, TTF, ORR, survival, tolerability, KPS | |
| Notes | FU median 32m Intention‐to‐treat analysis 907 analysed, 32 excluded Analysis cutoff March 2000 Survival not reported 729 discontinued treatment of which 391 'crossed over' | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind, double‐dummy |
Paridaens 2003.
| Study characteristics | ||
| Methods | International, multicentre, October 96 ‐ May 99 13 centres in 6 countries, N = 122 Open‐label phase II, randomised centrally using minimisation by EORTC, stratified by centre, adjuvant TAM, CT for metastatic disease, dominant disease site The trial was designed as a randomised phase II trial not to enable comparison of the efficacy of the two drugs but to establish a 'go, no‐go' rule for exemestane activity and safety before a formal randomised phase III trial. Patients randomised into the phase II trial will be incorporated into the phase III trial | |
| Participants | Age range 37 ‐ 87y Measurable metastatic or locally recurrent inoperable breast cancer No prior hormone therapy for metastatic disease ECOG perf status < 3 | |
| Interventions | Exemestane 25mg versus TAM 20mg Numbers in each treatment arm: 62 versus 60 Intention‐to‐treat analysis: 61 versus 59 Toxicity data: 62 versus 59 Assessable patients: 56 versus 57 Patients evaluable for toxicity: 62 versus 59 Treatment continued until disease progression | |
| Outcomes | Response rates Stop‐go for phase III Phase II therefore inadequate power, no statistical comparison of efficacy of endpoints between the two treatments were planned or performed | |
| Notes | FU details 2 patients (1 exemestane, 1 TAM) ineligible as not having metastatic breast cancer, 7 additional (5 exemestane, 2 TAM) not evaluable for response, 1 lost to FU Phase II patients to be included in phase III trial Intention‐to‐treat analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | stratified by centre, randomised centrally by EORTC using minimisation |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | High risk | open‐label |
Perez Carrion 1994.
| Study characteristics | ||
| Methods | International, multicentre, May 1988 ‐ December 1990, N = 409 Open study, equivalence trial Baseline characteristics well matched | |
| Participants | Age range 38 ‐ 87y WHO perf status < 3 | |
| Interventions | Formestane 250mg im versus TAM 30mg Numbers in each treatment arm: 203 versus 206 Assessable patients: 173 versus 175 | |
| Outcomes | Response, survival, TTP, TTF, tolerability | |
| Notes | FU details not reported 61 patients not evaluable, 10 lost to FU, 3 refusals Intention‐to‐treat analysis Trial closed early due to changes in clinical practice, ie increasing use of TAM in the adjuvant setting | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Blinding (performance bias and detection bias) All outcomes | High risk | open |
Powles 1984.
| Study characteristics | ||
| Methods | Sept 1979 ‐ June 1983 UK, single‐centre, N = 222 Previously determined allocation list unknown to clinician. Baseline characteristics mean age marginally greater for TAM patients | |
| Participants | Patients with disseminated breast cancer who had not previously received TAM, AG, or danazol No endocrine or chemotherapy within 6w | |
| Interventions | TAM 20mg versus TAM 20mg + AG 750mg + danazol 300mg + HC 40mg Number on each treatment arm: 111 versus 111 Assessable patients: 99 versus 99 Patients evaluable for toxicity: 111 versus 111 Treatment continued until 3m assessment (unless rapid development of tumour in meantime) otherwise stopped when evidence of tumour progression arose either through failure to respond or because of relapse after response or stabilisation of disease | |
| Outcomes | Tumour response | |
| Notes | FU duration not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | previously determined allocation list unknown to clinician |
Rose 1986.
| Study characteristics | ||
| Methods | Denmark, multicentre, June 1979 ‐ Sept 1988, 4 centres N = 313 Three‐arm trial (only two arms included in review N = 215) Randomised by centre, non‐stratified, stochastic array of numbers, closed envelope system Baseline characteristics well balanced | |
| Participants | Age > 65y, age range 66 ‐ 84y First recurrence of metastatic breast cancer Progressive disease with measurable and/or evaluable lesions Performance status < 4 | |
| Interventions | TAM 30mg versus TAM 30mg + AG 250mg qid + HC 60mg v TAM 30mg + fluoxymesterone 20mg Numbers in each treatment arm: 108 versus 107 versus 98 (TAM + fluoxymesterone excluded from review N = 98) Assessable patients: 83 versus 94 Patients evaluable for toxicity: 87 versus 97 Treatment until progression (minimum 12 weeks) | |
| Outcomes | TTF, TTP, survival, toxicity | |
| Notes | FU duration not reported 34 ineligible 21 not evaluable 9 lost to FU 258 fully evaluable | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | randomised by centre, non‐stratified, stochastic array of numbers |
| Allocation concealment (selection bias) | Low risk | closed envelope system |
Rose 2003.
| Study characteristics | ||
| Methods | International phase IIIb/IV, 19 countries, multicentre, 112 sites, N = 713 Dec 1997 ‐ Nov 1999 Open, random assignation stratified by centre via predetermined randomisation list Baseline characteristics well balanced | |
| Participants | Age range 27 ‐ 92y Advanced or metastatic breast cancer with measurable and/or evaluable disease Histologically/cytologically confirmed Previous treatment with antioestrogen WHO performance status 0‐2 | |
| Interventions | Letrozole 2.5mg versus anastrozole 1mg Numbers in each treatment arm: 356 versus 357 Assessable patients: 299 versus 304 | |
| Outcomes | Primary ‐ TTP Secondary‐ objective response, duration of response, rate and duration of overall clinical benefit, overall survival, general safety | |
| Notes | FU duration not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | random assignation stratified by centre |
| Allocation concealment (selection bias) | Low risk | predetermined randomisation list |
| Blinding (performance bias and detection bias) All outcomes | High risk | open‐label |
Russell 1997.
| Study characteristics | ||
| Methods | May 1984 ‐ November 1990, Phase III, N = 288 Three‐arm trial (only two arms included in review N = 155) No stratification Treatment arms reasonably well balanced | |
| Participants | Age range 33 ‐ 92y Progressive metastatic disease Measurable or evaluable lesion Patients had received TAM in advanced setting No prior MA or AG | |
| Interventions | MA 160mg versus AG (500mg for 2w then 1000mg) + HC (100mg for 2w then 40mg) versus MA 160mg + AG (500mg for 2w then 1000mg) + hydrocortisone Numbers in each treatment arm: 75 versus 80 versus 80 (MA 160mg + AG (500mg for 2w then 1000mg) + hydrocortisone arm data excluded from review N = 80) Assessable patients: 42 versus 32 Patients evaluable for toxicity: 88 versus 89 | |
| Outcomes | Response, TTF, survival, toxicity | |
| Notes | FU median duration amongst those still alive = 5.2y (213 had died) 53 ineligible (38 re misunderstanding re prior TAM use,7 due to life threatening visceral involvement, 3 with less than 6 months of TAM, 2 ER ‐, 1 prior hormonal therapy other than TAM, 1 no confirmed disease sites) Patients on MA or AG alone were crossed over after progression | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | no stratification |
Samonis 1994.
| Study characteristics | ||
| Methods | Greece, single‐centre, N = 85 trial duration 2.5y Three‐arm trial (only two arms included in the review N = 57) Stratified randomisation ‐ statified into four groups by previous adjuvant treatment Table of baseline characteristics | |
| Participants | Age range 50 ‐ 73y Metastatic breast cancer Measurable disease No previous treatment with AG or MPA KPS > 70% | |
| Interventions | AG (250mg for 3d, then to 1000mg) versus MPA (500mg for 1m then twice weekly) versus AG + MPA Numbers in each treatment arm:28 versus 29 versus 28 (AG + MPA data excluded from review) Assessable patients (two included arms): 26 versus 27 | |
| Outcomes | Response to treatment, toxicity | |
| Notes | FU duration not given Excluded patients: 1 accidental death, 4 lost to FU | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | statified into four groups by previous adjuvant treatment |
Schmid 2001.
| Study characteristics | ||
| Methods | International, multicentre, N = 171 Three‐arm trial (only two arms included in review N = 112) Double‐blind | |
| Participants | Mean age 64.5 Advanced breast cancer with bone metastases | |
| Interventions | Letrozole 2.5mg versus letrozole 0.5mg versus MA 160mg Number in each treatment arm: 52 versus 59 versus 60 (letrozole 0.5mg arm excluded from review N = 59) Assessable patients: 48 versus 53 | |
| Outcomes | Objective response, clinical benefit, TTP, survival | |
| Notes | Publication only available as abstract but sufficient data to include | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind |
Thuerlimann 1996.
| Study characteristics | ||
| Methods | Switzerland, Phase III multicentre, 7 sites, N = 221 June 1988 ‐ Dec 1994 Phone randomisation, stratified, minimisation not double blind Baseline: prognostic factors well balanced apart from metastatic site | |
| Participants | Age range 39 ‐ 87y Measurable/evaluable advanced breast cancer Indication for hormone treatment ECOG < 2 | |
| Interventions | Fadrozole 2mg versus TAM 20mg Numbers in each treatment arm: 111 versus 110 Eligible patients: 105 versus 107 Assessable patients: 103 versus 106 Patients evaluable for toxicity: 104 versus 107 First‐line treatment Treatment until progression | |
| Outcomes | TTF, response rate, toxicity, overall survival, TTP, subjective benefit (not reported), duration of response | |
| Notes | FU 7½ y Eligible patients: 212 9 ineligible(6 fadrozole, 3 TAM) 12 withdrawals Crossover only after failure so not analysed Analysis on data to Dec 1995, median FU of survivors 3y | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | minimisation, stratified |
| Allocation concealment (selection bias) | Low risk | phone randomisation |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | not double blind |
Thuerlimann 1997.
| Study characteristics | ||
| Methods | Feb 1991 ‐ Jun 1995, N = 179 Stratified, central randomisation Baseline characteristics well balanced (only difference in weight) | |
| Participants | Age range 43 ‐ 87y Advanced breast cancer Histologically and/or cytologically proven with measurable/evaluable disease Failed prior adjuvant and/or palliative tamoxifen treatment ie second‐line treatment Prior chemotherapy allowed ECOG perf status < 3 | |
| Interventions | Formestane 250mg im (biweekly) versus MA 160mg Numbers in each treatment arm: 91 versus 86 Assessable patients: 90 versus 83 Patients evaluable for toxicity: 90 versus 81 | |
| Outcomes | TTF, toxicity | |
| Notes | FU duration not reported 2 ineligible, 4 dropouts 173 fully evaluable After failure of randomised treatment 75 patients 'crossed over' | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | stratified |
| Allocation concealment (selection bias) | Low risk | central randomisation |
Tominaga 2003.
| Study characteristics | ||
| Methods | Japan, multicentre, 62 sites, N = 157 Double‐blind, double‐dummy, parallel groups Adaptive dynamic balancing method | |
| Participants | Mean age 59.7y (letrozole) and 61.0y (fadrozole) Advanced disease Measurable or assessable pathological lesions | |
| Interventions | Letrozole 1mg versus fadrozole 2mg Numbers in each treatment arm: 79 versus 78 Assessable patients: 77 versus 77 Minimum 8w treatment Treatment until disease progressed or patient experienced toxicity resulting in discontinuation | |
| Outcomes | ORR, safety of letrozole compared to fadrozole | |
| Notes | FU median 13.3m | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | adaptive dynamic balancing method |
| Allocation concealment (selection bias) | Low risk | adequate |
| Blinding (performance bias and detection bias) All outcomes | Low risk | double‐blind |
KPS ‐ Karnofsky Performance Status AG ‐ aminoglutethimide AI ‐ aromatase inhibitor CB ‐ clinical benefit ECOG ‐ Eastern Cooperative Oncology Group EORTC ‐ European Organization for the Research and Treatment of Cancer ER ‐ oestrogen receptor FU ‐ follow up im ‐ intramuscular mg ‐ milligram TAM ‐ tamoxifen MA ‐ megestrol acetate MPA ‐ medroxy progesterone acetate HC ‐ hydrocortisone N ‐ number of patients ORR ‐ objective response rate PD ‐ progressive disease perf status ‐ performance status qid ‐ four times daily QOL ‐ quality of life TTF ‐ time to failure TTP ‐ time to progression d ‐ days w ‐ weeks m ‐ months y ‐ years WHO ‐ World Health Organisation w/o ‐ without
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abe 2002 | dose comparison of same AI (letrozole) |
| Bajetta 1994 | dose comparison of same AI (formestane) |
| Bajetta 1997 | dose comparison of same AI (exemestane) |
| Bajetta 1997a | dose comparison of same AI (letrozole) |
| Bajetta 1999 | dose comparison of same AI (letrozole) |
| Beretta 1990 | dose comparison of same AI (letrozole) |
| Bruning 1989 | dose comparison of same AI (aminoglutethimide) |
| Bruning 1990 | dose comparison of same AI (aminoglutethimide) |
| Castelazo 2004 | non‐English (Spanish) paper |
| Cataliotti 2006 | comparison of anastrozole versus tamoxifen as neoadjuvant treatment |
| Dixon 2000 | dose‐comparison of same AI (anastrozole) |
| Dowsett 1989 | dose‐comparison of same AI (formestane) |
| Dowsett 1990 | dose‐comparison of same AI (fadrozole) |
| Dowsett 1994 | dose‐comparison of same AI (fadrozole) |
| Dowsett 1995 | dose‐comparison of same AI (letrozole) |
| Eiermann 2001 | comparison of letrozole versus tamoxifen as pre‐operative treatment |
| Geisler 1996 | outcome: aromatase levels and plasma oestrogen levels |
| Geisler 2002 | outcome: aromatase levels and plasma oestrogen levels |
| Ingle 1997 | dose comparison of same AI (letrozole) |
| Johnston 1994 | dose comparison of same AI (vorozole) |
| Miller 1996b | dose comparison of same AI (fadrozole) |
| Pronzato 1993 | AI (aminoglutethimide) versus same AI plus tamoxifen |
| Raats 1992 | dose comparison of same AI (fadrozole) |
| Smith 2005 | comparison of anastrozole versus tamoxifen as neoadjuvant treatment |
| Svenstrup 1994 | dose comparison of same AI (fadrozole) |
| Wang 2003 | non‐English (Chinese) paper |
Characteristics of ongoing studies [ordered by study ID]
CAAN.
| Study name | CAAN |
| Methods | |
| Participants | Target accrual = 90 postmenopausal women with histologically proven advanced breast cancer |
| Interventions | Exemestane + celecoxib versus exemestane versus letrozole |
| Outcomes | Levels of serum lipids and cholesterol |
| Starting date | February 2002 |
| Contact information | LWC Chow lwcchow@hkucc.hku.hk |
| Notes | initial report published in 2005 |
ECOG E4101.
| Study name | ECOG E4101 |
| Methods | |
| Participants | Target accrual = 148 postmenopausal women with HR+ metastatic breast cancer previously treated with up to two chemotherapy regimens and/or one prior endocrine therapy |
| Interventions | Faslodex + gefitinib versus arimidex + gefitinib |
| Outcomes | |
| Starting date | |
| Contact information | Dr RW Carlson or AstroZeneca |
| Notes | currently recruiting in the USA |
ICR‐CTSU Sofea.
| Study name | Sofea Phase III |
| Methods | |
| Participants | Target accrual = 750 women with metastatic disease who have failed after non‐steroidal AI |
| Interventions | Faslodes versus faslodex + anastrozole versus exemestane |
| Outcomes | |
| Starting date | March 2004 |
| Contact information | Dr SRD Johnston, Royal Marsden Hospital email: sofea‐icrctsu@icr.ac.uk |
| Notes | Open to recruitment in UK |
Paridaens 2003.
| Study name | Phase III EORTC‐10951 |
| Methods | |
| Participants | Postmenopausal women with metastatic and progressive disease or locally recurrent and inoperable |
| Interventions | exemestane versus tamoxifen |
| Outcomes | |
| Starting date | |
| Contact information | robert.paridaens@uz.kuleven.ac.be |
| Notes | phase II to phase III study |
HR+ HER positive
Differences between protocol and review
Many of the data required to carry out analyses of prospectively identified subgroups, as set out in the review protocol, were not available. We could not, therefore, identify specific subgroups of women who may benefit from AI use.
Contributions of authors
Judith Bliss wrote the original protocol, initiated the review with Lorna Gibson and reviewed the review.
Lorna Gibson worked with the Cochrane Breast Group to identify the initial list of references; she then worked through the list to identify eligible trials. Lorna carried out the first independent data extraction from the eligible trials and was a main contributor to the review and analysis, and the update.
Claire Dawson carried out a second independent extraction of data from the eligible trials and contributed to the original review.
David Lawrence carried out an independent check of the data extraction for accuracy and consistency and was a main contributor to the original review analysis, and the update.
Sources of support
Internal sources
Cancer Research UK, UK
External sources
No sources of support supplied
Declarations of interest
One of the authors (JMB) is a member of the management group and grant holder for the Intergroup Exemestane Study. This is funded by Pfizer, the producers of the aromatase inhibitor exemestane.
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
Alonso‐Munoz 1988 {published data only}
- Alonso-Munzo MC, Ojeda-Gonzalez M, Beltran-Fabregat M, Dorca-Ribugent J, Lopez-Lopez L, Borras-Balada J et al. Randomized trial of tamoxifen versus aminoglutethimide and versus combined tamoxifen and aminoglutethimide in advanced postmenopausal breast cancer. Oncology 1988;45:350-3. [DOI] [PubMed] [Google Scholar]
Bezwoda 1998 {published data only}
- Bezwoda WR, Gudgeon A, Falkson G, Jordaan JP, Goedhals L. Fadrozole versus megestrol acetate: a double-blind randomised trial in advanced breast cancer. Oncology 1998;55:416-20. [DOI] [PubMed] [Google Scholar]
Bonneterre 2001 {published data only}
- Bonneterre J, Buzdar A, Nabholtz JA, Robertson JFR, Thuerlimann B, von Euler M et al. Anastrozole is superior to tamoxifen as first-line therapy in hormone receptor positive advanced breast carcinoma. Cancer 2001;92(9):2247-58. [DOI] [PubMed] [Google Scholar]
- Bonneterre J, Thuerlimann B, Robertson JFR, Krzakowski M, Mauriac L, Koralewski P, et al. Anastrozole versus tamoxifen as first-line therapy for advanced breast cancer in 668 postmenopausal women: results of the tamoxifen or arimidex randomized group efficacy and tolerability study. Journal of Clinical Oncology 2000;18(22):3748-57. [DOI] [PubMed] [Google Scholar]
- Nabholtz JM, Bonneterre J, Buzdar A, Robertson JFR, Thuerlimann B. Anastrozole (Arimidex) versus tamoxifen as first-line therapy for advanced breast cancer in postmenopausal women: survival analysis and updated safety results. European Journal of Cancer 2003;39:1684-9. [DOI] [PubMed] [Google Scholar]
- Nabholtz JM, Buzdar A, Pollak M, Harwin W, Burton G, Mangalik A et al. Anastrozole is superior to tamoxifen as first-line therapy for advanced breast cancer in postmenopausal women: results of a North American multicenter randomized trial. Journal of Clinical Oncology 2000;18(22):3758-67. [DOI] [PubMed] [Google Scholar]
- Nabholtz JM. Advanced breast cancer updates on anastrozole versus tamoxifen. Journal of Steroid Biochemistry and Molecular Biology 2003;86:321-5. [DOI] [PubMed] [Google Scholar]
- Thuerlimann B, Robertson JFR, Nabholtz JM, Buzdar A, Bonneterre J. Efficacy of tamoxifen following anastrozole ('Arimidex') compared with anastrozole following tamoxifen as first-line treatment for advanced breast cancer in postmenopausal women. European Journal of Cancer 2003;39:2310-17. [DOI] [PubMed] [Google Scholar]
- Vergote I, Bonneterre J, Thuerlimann B, Robertson J, MKrzakowski M, Mauriac L et al. Randomised study of anastrozole versus tamoxifen as first-line therapy for advanced breast cancer in postmenopausal women. European Journal of Cancer 2000;36(Suppl:):81-91. [DOI] [PubMed] [Google Scholar]
Buzdar 1996a {published data only}
- Budzar A, Jonat W, Howell A, Jones SE, Blomqvist C, Vogel CL et al. Anastrozole, a potent and selective aromatase inhibitor, versus megestrol acetate in postmenopausal women with advanced breast cancer: results of overview analysis of two phase III trials. Journal of Clinical Oncology 1996;14:2000-11. [DOI] [PubMed] [Google Scholar]
- Buzdar AU, Jonat W, Howell A, Jones SE, Blomqvist CP, Vogel CL et al. Anastrozole versus megestrol acetate in the treatment of postmenopausal women with advanced breast carcinoma. Cancer 1998;83(6):1142-52. [PubMed] [Google Scholar]
- Buzdar AU, Jonat W, Howell A, Plourde PV. Arimidex: a potent and selective aromatase inhibitor for the treatment of advanced breast cancer. Journal Steroid Biochemistry Molecular Biology 1997;61(3-6):145-9. [PubMed] [Google Scholar]
- Drummond M, Thompton E, Howell A, Jonat W, Buzdar A, Brown J. Cost-effectiveness implications of increased survival with anastrozole in the treatment of advanced breast cancer. Journal of Medical Economics 1999;2:33-43. [Google Scholar]
- Jonat W, Howell A, Blomqvist C, Eiermann W, Winblad G, TyrrellC et al. A randomized trial comparing two doses of the new selective aromatase inhibitor anastrozole (Arimidex) with megestrol acetate in postmenopausal women with advanced breast cancer. European Journal of Cancer 1996;32A(3):404-12. [DOI] [PubMed] [Google Scholar]
- Robertson JFR, Howell A, Buzdar A, Euler M, Lee D. Static disease on anastrozole provides similar benefit as objective response in patients with advanced breast cancer. Breast Cancer Research and Treatment 1999;58:157-62. [DOI] [PubMed] [Google Scholar]
Buzdar 1996b {published data only}
- Buzdar A, Smith R, Vogel C, Bonomi P, Keller AM, Favis G et al. Fadrazole HCl (CGS-16949A) versus megestrol acetate in postmenopausal patients with metastatic breast carcinoma: results of two randomized, double-blind, controlled multi-institutional trials. Cancer 1996;77(12):2503-13. [DOI] [PubMed] [Google Scholar]
Buzdar 1996c {published data only}
- Buzdar A, Smith R, Vogel C, Bonomi P, Keller AM, Favis G et al. Fadrazole HCl (CGS-16949A) versus megestrol acetate in postmenopausal patients with metastatic breast carcinoma: results of two randomized, double-blind, controlled multi-institutional trials. Cancer 1996;77(12):2503-13. [DOI] [PubMed] [Google Scholar]
Buzdar 2001 {published data only}
- Buzdar A, Douma J, Davidson N, Elledge R, Morgan M, Smith R et al. Phase III, multicenter, double-blind, randomized study of letrozole, an aromatase inhibitor, for advanced breast cancer versus megestrol acetate. Journal of Clinical Oncology 2001;19(14):3357-66. [DOI] [PubMed] [Google Scholar]
Canney 1988 {published data only}
- Canney PA, Priestman TJ, Griffiths T, Latief TN, Mould JJ, Spooner D. Randomized trial comparing aminoglutethimide with high-dose medroxyprogesterone acetate in therapy for advanced breast carcinoma. Journal of the National Cancer Institute 1988;80(14):1147-51. [DOI] [PubMed] [Google Scholar]
Chia 2008 {published data only}
- Chia S, Gradishar W, Mauriac L, Bines J, Amant F, Federico M et al. Double-blind, randomized placebo controlled trial of fulvestrant compared with exemestane after prior nonsteroidal aromatase inhibitor therapy in postmenopausal women with hormone receptor-positive, advanced breast cancer: results from EFECT. Journal of Clinical Oncology 2008;26(10):1664-70. [DOI] [PubMed] [Google Scholar]
Dombernowsky 1998 {published data only}
- Dombernowsky P, Smith I, Falkson G, Leonard R, Panasci L, Bellmunt J et al. Letrozole, a new oral aromatase inhibitor for advanced breast cancer: double-blind randomized trial showing a dose effect and improved efficacy and tolerability compared with megestrol acetate. Journal of Clinical Oncology 1998;16(2):453-61. [DOI] [PubMed] [Google Scholar]
Falkson 1996 {published data only}
- Falkson CI, Falkson HC. A randomised study of CGS 16949A (fadrozole) versus tamoxifen in previously untreated postmenopausal patients with metastatic breast cancer. Annals of Oncology 1996;7:465-9. [DOI] [PubMed] [Google Scholar]
Freue 2000 {published data only}
- Freue M, Kjaer C, Boni J, Joliver F, Jaenicke F, Willemse PhHB et al. Open comparative trial of formestane versus megestrol acetate in postmenopausal patients with advanced breast cancer previously treated with tamoxifen. The Breast 2000;9:9-16. [DOI] [PubMed] [Google Scholar]
Gale 1994 {published data only}
- Gale KE, Andersen JW, Tormey DC, Mansour EG, David TE, Horton J et al. Hormonal treatment for metastatic breast cancer. An Eastern Cooperative Oncology Group Phase III trial comparing aminoglutethimide to tamoxifen. Cancer 1994;73(2):354-361. [DOI] [PubMed] [Google Scholar]
Garcia‐Giralt 1992 {published data only}
- Garcia-Giralt E, Ayme Y, Carton M, Daban A, Delozier T, Fargeot P et al. Second and third line hormonotherapy in advanced post-menopausal breast cancer: a multicenter randomized trial comparing medroxyprogesterone acetate with aminoglutethimide in patients who have become resistant to tamoxifen. Breast Cancer Research and Treatment 1992;24:139-45. [DOI] [PubMed] [Google Scholar]
Gershanovich 1998 {published data only}
- Gershanovich M, Chaudri HA, Campos D, Lurie H, Bonaventura A, Jeffrey M et al. Letrozole, a new oral aromatase inhibitor: randomised trial comparing 2.5mg daily, 0.5 mg daily and aminoglutethimide in postmenopausal women with advanced breast cancer. Annals of Oncology 1998;9:639-45. [DOI] [PubMed] [Google Scholar]
- Gershanovitch M. Letrozole, a new aromatase for advanced breast cancer. Voprosy Onkolgii 45;4:361-8. [PubMed] [Google Scholar]
Goss 1999 {published data only}
- Goss PE, Winer EP, Tannock IF, Schwarz LH. Randomized phase III trial comparing the new potent and selective third generation aromatase inhibitor vorozole with megestrol acetate in postmenopausal advanced breast cancer patients. Journal of Clinical Oncology 1999;17(1):52-63. [DOI] [PubMed] [Google Scholar]
Goss 2007 {published data only}
- Goss P, Bondarenko IN, Mankhas GN, Pendergrass KB, Miller WH, Langecker P et al. Phase III, double-blind, controlled trial of atamastane plus toremifene compared with letrozole in postmenopausal women with advanced receptor-positive breast cancer. Journal of Clinical Oncology 2007;25(31):4961-6. [DOI] [PubMed] [Google Scholar]
Ingle 1986 {published data only}
- Ingle JN, Green SJ, Ahmann DL, Long HJ, Edmonson JH, Rubbin J et al. Randomized trial of tamoxifen alone or combined with aminoglutethimide and hydrocortisone in women with metastatic breast cancer. Journal of Clinical Oncology 1986;4(6):958-64. [DOI] [PubMed] [Google Scholar]
Kaufmann 2000 {published data only}
- Hillner BE, Radice D. Cost-effectiveness analysis of exemestane compared with megestrol in patients with advanced breast carcinoma. Cancer 2001;91(3):484-9. [DOI] [PubMed] [Google Scholar]
- Kaufmann M, Bajetta E, Dirix LY, Fein LE, Jones SE, Cervek J et al. Exemestane improves survival compared with megestrol acetate in postmenopausal patients with advanced breast cancer who have failed on tamoxifen: results of a double-blind randomised phase III trial. European Journal of Cancer 2000;36 Suppl:81-91. [DOI] [PubMed] [Google Scholar]
- Kaufmann M, Bajetta E, Dirix LY, Fein LE, Jones SE, Zilembo N et al. Exemestane is superior to megestrol acetate after tamoxifen failure in postmenopausal women with advanced breast cancer: results of a phase III randomised double-blind trial. Journal of Clinical Oncology 2000;18(7):1399-411. [DOI] [PubMed] [Google Scholar]
Kleeberg 1997 {published data only}
- Kleeberg UR, Dowsett M, Carrion RP, Dodwell DJ, Vorobiof DA, Aparicio LA, Robertson JFR. A randomised comparison of oestrogen suppression with anastrozole and formestane in postmenopausal patients with advanced breast cancer. Oncology 1997;54 Suppl 2:19-22. [DOI] [PubMed] [Google Scholar]
- Vorobiof DA, Kleeberg UR, Perez-Carrion R, Dodwell DJ, Robertson JFR, Calvo L et al. A randomized, open, parallel-group trial to compare the endocrine effects of oral anastrozole (Arimidex) with intramuscular formestane in postmenopausal women with advanced breast cancer. Annals of Oncology 1999;10:1219-25. [DOI] [PubMed] [Google Scholar]
Leitzel 1995 {published data only}
- Leitzel K, Teramoto Y, Konrad K, Chinchilli VM, Volas G, Grossberg H et al. Elevated Serum c-erb B-2 Antigen levels and decreased response to hormone therapy of breast cancer. Journal of Clinical Oncology 1995;13(5):1129-35. [DOI] [PubMed] [Google Scholar]
Lundgren 1989 {published data only}
- Lundgren S, Gundersen S, Klepp R, Lonning PE, Lund E, Kvinnsland S. Megestrol acetate versus aminoglutethimide for metastatic breast cancer. Breast Cancer Research and Treatment 1989;14:201-6. [DOI] [PubMed] [Google Scholar]
Mauriac 2003 {published data only}
- Howell A, Robertson JFR, Quaresma Albano J, Ascgermannova A, Mauriac L, Kleeberg UR et al. Fulvestrant, formerly ICI 182, 780, is as effective as anastrozole in postmenopausal women with advanced breast cancer progressing after prior endocrine treatment. Journal of Clinical Oncology 2002;20(16):3396-403. [DOI] [PubMed] [Google Scholar]
- Mauriac L, Pippen JE, Quaresma Albano J, Gertler SZ Osborne CK. Fulvestrant (Faslodex) versus anastrozole for the second-line treatment of advanced breast cancer in subgroups of postmenopausal women with visceral and non-visceral metasteses: combined results from two multicentre trials. European Journal of Cancer 2003;39(9):1228-33. [DOI] [PubMed] [Google Scholar]
- Osborne CK, Pippen J, Jones, SE, Parker LM, Ellis M, Come S et al. Double-blind, randomized trial comparing the efficacy and tolerability of the fulvestrant versus anastrozole in postmenopausal women with advanced breast cancer progressing on prior endocrine therapy: results of a North American Trial. Journal of Clinical Oncology 2002;20(16):3386-95. [DOI] [PubMed] [Google Scholar]
- Robertson JFR, Osborne CK, Howell A, Jones SE, Mauriac L, Ellis M et al. Fulvestrant versus anastrozole for the treatment of advanced breast carcinoma in postmenopausal women. Cancer 2003;98(2):229-38. [DOI] [PubMed] [Google Scholar]
- Vergote I. Fulvestrant versus anastrozole as second-line treatment of advanced breast cancer in postmenopausal women. European Journal of Cancer 2002;38 Suppl(6):57-8. [DOI] [PubMed]
Mercer 1993 {published data only}
- Mercer PM, Ebbs SR, Fraser SCA, Coltart RS, Bates T. Trial of aminoglutethimide vs hydrocortisone as second-line hormone treatment of advanced breast cancer. European Journal of Surgical Oncology 1993;19:254-8. [PubMed] [Google Scholar]
Milla‐Santos 2003 {published data only}
- Milla-Santos A, Milla L, Portella J, Rallo L, Pons M, Rodes E et al. Anastrozole versus tamoxifen as first-line therapy in postmenopausal patients with hormone-dependent advanced breast cancer. American Journal of Clinical Oncology 2003;26(3):317-22. [DOI] [PubMed] [Google Scholar]
Mourisden 2001 {published data only}
- Irish W, Sherrill B, Cole B, Gard C, Glendenning GA, Mourisden H. Quality-adjusted survival in a crossover trial of letrozole versus tamoxifen in postmenopausal women with advance breast cancer. Annals of Oncology 2005;16:1458-62. [DOI] [PubMed] [Google Scholar]
- Lipton A, Ali SM, Leitzel K, Demers L, Harvey HA, Chaudri-Ross HA et al. Serum HER-2/neu and response to the aromatase inhibitor letrozole versus tamoxifen. Journal of Clinical Oncology 2003;21(10):1967-72. [DOI] [PubMed] [Google Scholar]
- Mourisden H, Chaudri-Ross HA. Efficacy of First-Line letrozole versus tamoxifen as a function of age in postmenopausal women with advanced breast cancer. The Oncologist 2004;9:497-506. [DOI] [PubMed] [Google Scholar]
- Mourisden H, Gershanovich M, Sun Y, Perez-Carrion R, Boni C, Monnier A et al. Phase III study of letrozole versus tamoxifen as first-line therapy of advanced breast cancer in postmenopausal women: analysis of survival and update of efficacy from the International Letrozole Breast Cancer Group. Journal of Clinical Oncology 2003;21(11):2101-9. [DOI] [PubMed] [Google Scholar]
- Mourisden H, Gershanovich M, Sun Y, Perez-Carrion R, Boni C, Monnier A et al. Superior efficacy of letrozole versus tamoxifen as first-line therapy for postmenopausal women with advanced brreast cancer: results of a phase III study of the international letrozole breast cancer group. Journal of Clinical Oncology 2001;19(10):2596-606. [DOI] [PubMed] [Google Scholar]
- Mourisden H, Sun Y, Gershanovich M, Perez-Carrion R, Becquart D, Chaudri-Ross HA, Lang R. Superiority of letrozole to tamoxifen in the first-line treatment of advanced breast cancer: evidence from metastatic subgroups and a test of functional ability. The Oncologist 2004;9:489-96. [DOI] [PubMed] [Google Scholar]
- Mourisden HT. Letrozole in advanced breast cancer: the PO25 trial. Breast Cancer Research and Treatment 2007;105:19-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
Paridaens 2003 {published data only}
- Atalay G, Dirix L, Biganzoli L, Beex L, Nooji M, Cameron D et al. The effect of exemestane on serum lipid profile in postmenopausal women with metastatic breast cancer: a comparison study to EORTC Trial 10951, 'Randomized phase II study in first line hormonal treatment for metastatic breast cancer with exemestane or tamoxifen in postmenopausal patients'. Annals of Oncology 2004;15(2):211-7. [DOI] [PubMed] [Google Scholar]
- Paridaens R, Dirix L, Lohrisch C, Beex L, Nooji M, Cameron D et al. Mature results of a randomized phase II multicenter study of exemextane versus tamoxifen as first-line hormone therapy for postmenopausal women with metastatic breast cancer. Annals of Oncology 2003;14:1391-8. [DOI] [PubMed] [Google Scholar]
Perez Carrion 1994 {published data only}
- Perez Carrion R, Alberola Candel V, Calabresi F, Michel RT, Santos R, Delozier T et al. Comparison of the selective aromatase inhibitor formestane with tamoxifen as first-line therapy in postmenopausal women with advanced breast cancer. Annals of Oncology 1994;5 Suppl 7:19-24. [PubMed] [Google Scholar]
Powles 1984 {published data only}
- Powles TJ, Ashley S, Ford HT, Gazet JC, Nash AG, Neville AM, Coombes RC. Treatment of disseminated breast cancer with tamoxifen, aminoglutethimide, hydrocortisone, and danazol, used in combination or sequentially. The Lancet 1984;1(8391):1369-72. [DOI] [PubMed] [Google Scholar]
Rose 1986 {published data only}
- Rose C, Kamby C, Mouridsen HT, Andersson M, Bastholt L, Moller KA et al. Combined endocrine treatment of elderly postmenopausal patients with metastatic breast cancer. Breast Cancer Research and Treatment 2000;61(2):103-10. [DOI] [PubMed] [Google Scholar]
- Rose C, Kamby C, Mouridsen HT, Bastholt L, Brincker H, Skovaard-Poulsen H et al. Combined endocrine treatment of postmenopausal patients with advanced breast cancer. A randomised trial of tamoxifen vs. tamoxifen plus aminoglutethimide and hydrocortisone. Breast Cancer Research and Treatment 1986;7 Suppl:45-50. [PubMed] [Google Scholar]
Rose 2003 {published data only}
- Rose C, Vtoraya O, Pluzanska A, Davidson N, Gershanovich M, Thomas R et al. An open randomised trial of second-line endocrine therapy in advanced breast cancer. European Journal of Cancer 2003;39(16):2318-27. [DOI] [PubMed] [Google Scholar]
- Tobias JS, Howell A. An open randomised trial of second-line endocrine therapy in advanced breast cancer: comparison of the aromatase inhibitors letrozole and anastrozole. European Journal of Cancer 2004;40(12):1913. [DOI] [PubMed] [Google Scholar]
Russell 1997 {published data only}
- Russell C, Green SJ, O'Sullivan J, Hynes HE, Budd T, Congdon JE et al. Megestrol acetate and aminoglutethimide/hydrocortisone in sequence or in combination as second-line endocrine therapy of estrogen receptor-positive metastatic breast cancer: a southwest oncology group phase III trial. Journal of Clinical Oncology 1997;15(7):2494-501. [DOI] [PubMed] [Google Scholar]
Samonis 1994 {published data only}
- Samonis G, Margioris AN, Bafaloukos D, Razis DV. Prospective randomized study of aminoglutethimide (AG) versus medroxyprogesterone acetate (MPA) versus AG+MPA in generalized breast cancer. Oncology 1994;51(5):411-5. [DOI] [PubMed] [Google Scholar]
Schmid 2001 {published data only}
- Schmid P, Wischnewsky MB, Possinger K. Self organizing maps and prognosis of advanced breast cancer patients with bone metastases receiving letrozole or MA. Breast Cancer Research and Treament 2001;64:77. [Google Scholar]
Thuerlimann 1996 {published data only}
- Thuerlimann B, Beretta K, Bacchi M, Castiglione-Gertsch M, Goldhirsch A, Jungi WF et al. First-line fadrozole HCI (CGS 16949A) versus tamoxifen in postmenopausal women with advanced breast cancer. Annals of Oncology 1996;7:471-9. [DOI] [PubMed] [Google Scholar]
Thuerlimann 1997 {published data only}
- Bernhard J, Casiglione-Gertsch M, Hsu Schmitz S-F, Thuerlimann B, Cavalli F, Morant R et al. Quality of life in postmenopausal patients with breast cancer after failure of tamoxifen: formestane versus megestrol acetate as second-line hormonal treatment. European Journal of Cancer 1999;35(6):913-20. [DOI] [PubMed] [Google Scholar]
- Bernhard J, Thuerlimann B, Hsu Schmitz S-F, Castiglione-Gertsch M, Cavalli F, Morant R et al. Defining clinical benefit in postmenopausal patients with breast cancer under second-line endocrine treatment: does quality of life matter. Journal of Clinical Oncology 1999;17(6):1672-9. [DOI] [PubMed] [Google Scholar]
- Thuerlimann B, Castiglione M, Hsu-Scmitz SF, Cavalli F, Bonnefoi H, Fey MF et al. Formestane versus megestrol acetate in postmenopausal breast cancer patients after failure of tamoxifen: a phase III prospective randomised cross over trial of second-line hormonal treatment (SAKK 20/90). European Journal of Cancer 1997;33(7):1017-24. [DOI] [PubMed] [Google Scholar]
Tominaga 2003 {published data only}
- Tominaga T, Adachi I, Sasaki Y, Tabei T, Ikeda T, Takatsuka Y et al. Double-blind randomised trial comparing the non-steroidal aromatase inhibitors letrozole and fadrozole in postmenopausal women with advanced breast cancer. Annals of Oncology 2003;14:62-70. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Abe 2002 {published data only}
- Abe R, Tominaga T, Nomizu T, Nomura Y, Takashima S, Koyama H et al. CGS20267 (letrozole), a new aromatase inhibitor: late phase II study for postmenopausal women with advanced or recurrent breast cancer (no. 1) - investigation of recommended clinical dose CGS20267 Study Group. Gan To Kaguku Ryoho 2002;29(5):729-40. [PubMed] [Google Scholar]
Bajetta 1994 {published data only}
- Bajetta E, Zilembo N, Buzzoni R, Noberasco C, Di Leo A, Bartoli C et al. Endocrinological and clinical evaluation of two doses of formestane in advanced breast cancer. British Journal of Cancer 1994;70:145-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferrari L, Zilembo N, Bajetta, Buzzoni R, Noberasco C, Martinetti A et al. Effect of two 4-hydroxyandrostenedione doses on serum insulin-like growth factor I levels in advanced breast cancer. Breast Cancer Research and Treatment 1994;30:127-32. [DOI] [PubMed] [Google Scholar]
Bajetta 1997 {published data only}
- Bajetta E, Zilembo N, Noberasco C, Martinetti A, Mariani L, Ferrari L et al. The minimal effective exemestane dose for endocrine activity in advanced breast cancer. European Journal of Cancer 1997;33(4):587-91. [DOI] [PubMed] [Google Scholar]
Bajetta 1997a {published data only}
- Bajetta E, Ferrari L, Celio L, Mariana L, Miceli R, Di Leo A et al. The aromatase inhibitor letrozole in advanced breast cancer: effects on serum insulin-like growth factor (IGF)-I and IGF-binding protein-3 levels. Journal of Steroid Biochemistry 1997;63(4-6):261-7. [DOI] [PubMed] [Google Scholar]
Bajetta 1999 {published data only}
- Bajetta E, Zilembo N, Dowsett M, Guillevin L, Di Leo A, Celio L et al. Double-blind, randomised, multicentre endocrine trial comparing two letrozole doses in postmenopausal breast cancer patients. European Journal of Cancer 1999;35(2):208-13. [DOI] [PubMed] [Google Scholar]
Beretta 1990 {published data only}
- Beretta KR, Hoeffken K, Kvinnsland S, Trunet P, Chaudri HA, Bhatnagar AS et al. CGS 16949A, a new aromatase inhibitor in the treatment of breast cancer - a phase I study. Annals of Oncology 1990;1(6):421-6. [DOI] [PubMed] [Google Scholar]
Bruning 1989 {published data only}
- Bruning PF, Bonfer JMG, Hart AAM, Linden E, Jong-Bakker M, Moolenaar AJ, Nooijen WJ. Low dose aminoglutethimide without hydrocortisone for the treatment of advanced postmenopausal breast cancer. European Journal of Clinical Oncology 1989;25(2):369-76. [DOI] [PubMed] [Google Scholar]
Bruning 1990 {published data only}
- Bruning PF, Bonfrer JMG, Wildiers J, Jassem J, Beex LVAM, Schorangel J, Nooijen WJ. Second-line endocrine treatment of postmenopausal advanced breast cancer preliminary endocrine results of a 5-arm randomized phase II trial of medium vs low dose aminoglutethimide, with or without hydrocortisone vs hydrocortisone alone (EORTC 10861). Journal of Steroid Biochemistry 1990;37(6):1013-9. [DOI] [PubMed] [Google Scholar]
Castelazo 2004 {published data only}
- Castelazo RG, Molotia Xolalpa D, Basavilvazo Rodriguez MA, Angeles Victoria L, Zarate A, Hernandez-Valencia M. Survival of breast cancer patients treated with inhibitors of the aromatase vs tamoxifen. Ginecologia y Obstetricia de Mexico 2004;72:493-9. [PubMed] [Google Scholar]
Cataliotti 2006 {published data only}
- Cataliotti L, Buzdar AU, Noguchi S, Bines J, Takatsuka Y, Petrakova K. Comparison of anastrozole versus tamoxifen as preoperative therapy in postmenopausal women with hormone receptor-positive breast cancer. Cancer 2006;106(10):2095-103. [DOI] [PubMed] [Google Scholar]
Dixon 2000 {published data only}
- Dixon JM, Renshaw L, Bellamy C, Stuart M, Hoctin-Boes G, Miller WR. The effects of neoadjuvant anastrozole (Arimidex) on tumor volume in postmenopausal women with breast cancer: a randomized, double-blind, single-center study. Clinical Cancer Research 2000;6(6):2229-35. [PubMed] [Google Scholar]
Dowsett 1989 {published data only}
- Dowsett M, Cunningham DC, Stein RC, Evans S, Dehennin L, Hedley A, Coombes RC. Dose-related endocrine effects and pharmokinetics of oral and intramuscular 4-hydroxyandrostenedione in postmenopausal breast cancer patients. Cancer Research 1989;49:1306-12. [PubMed] [Google Scholar]
Dowsett 1990 {published data only}
- Dowsett M, Stein RC, Mehta A, Coombes RC. Potency and selectivity of the non-steroidal aromatase inhibitor CGS 16949A in postmenopausal breast cancer patients. Clinical Endocrinology 1990;32:623-34. [DOI] [PubMed] [Google Scholar]
Dowsett 1994 {published data only}
- Bonnefoi HR, Smith IE, Dowsett M, Trunet, Houston SJ, da Luz RJ et al. Therapeutic effects of the aromatase inhibitor fadrozole hydrochloride in advanced breast cancer. British Journal of Cancer 1996;73:539-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dowsett M, Smithers D, Moore J, Trunet PF, Coombes RC, Powles TJ et al. Endocrine changes with the aromatase inhibitor fadrozole hydrochloride in breast cancer. European Journal of Cancer 1994;30A(10):1453-8. [DOI] [PubMed] [Google Scholar]
Dowsett 1995 {published data only}
- Dowsett M, Jones A, Johnston SRD, Jacobs S, Trunet P, Smith IE. In vivo measturement of aromatase inhibition by letrozole (CGS 20267) in postmenopausal patients with breast cancer. Clinical Cancer Research 1995;1:1511-5. [PubMed] [Google Scholar]
Eiermann 2001 {published data only}
- Eiermann W, Paepke S, Appfelstaedt J, Llombart-Cussac A, Eremin J, Vinholes J et al. Preoperative treatment of postmenopausal breast cancer patients with letrozole: a randomized double-blind multicenter study. Annals of Oncology 2001;12:1527-32. [DOI] [PubMed] [Google Scholar]
Geisler 1996 {published data only}
- Geisler J, King N, Dowsett M, Ottestad L, Lundgren S, Walton P et al. Influence of anastrozole (Arimidex), a selective, non-steroidal aromatase inhibitor, on in vivo aromatisation and plasma oestrogen levels in post menopausal women with breast cancer. British Journal of Cancer 1996;74:1286-91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Geisler 2002 {published data only}
- Geisler J, Haynes B, Anker G, Dowsett M, Loenning PE. Influence of letrozole and anastrozole on totla body aromatization and plasma estrogen levels in postmenopausal breast cancer patients evaluated in a randomised, cross-over study. Journal of Clinical Oncology 2002;20(3):751-7. [DOI] [PubMed] [Google Scholar]
Ingle 1997 {published data only}
- Ingle JN, Johnson PA, Suman VJ, Gerstner JB, Mailliard JA, Camoriano JK et al. A randomized phase II trial of two dosage levels of letrozole as third-line hormonal therapay for women with metastatic breast carcinoma. Cancer 1997;80:218-24. [DOI] [PubMed] [Google Scholar]
Johnston 1994 {published data only}
- Johnston SRD, Smith IE, Doody D, Jacobs S, Robertshaw H, Dowsett M. Clinical and endocrine effects of the oral aromatase inhibitor vorozole in postmenopausal patients with advanced breast cancer. Cancer Research 1994;54:5875-81. [PubMed] [Google Scholar]
Miller 1996b {published data only}
- Miller AA, Lipton A, Henderson IC, Navari R, Mulagha MT, Cooper J. Fadrozole hydrochloride in postmenopausal patients with metastatic breast carcinoma. Cancer 1996;78:789-93. [DOI] [PubMed] [Google Scholar]
Pronzato 1993 {published data only}
- Pronzato P, Rubagotti A, Amoroso D, Bertelli G, Queirolo P, Sertoli MR, Rosso M et al. Second-line hormone therapy for breast cancer. Uselessness of first-line continuation. American Journal of Clinical Oncology 1993;16(6):522-5. [DOI] [PubMed] [Google Scholar]
Raats 1992 {published data only}
- Falkson G, Raats JI, Falkson H. Fadrozole hydrochloride, a new nontoxic aromatase inhibitor for the treatment of patients with metastatic breast cancer. Journal of Steroid and Biochemistry and Molecular Biology 1992;43(1-3):161-5. [DOI] [PubMed] [Google Scholar]
- Raats JI, Falkson G, Falkson H. A study of fadrozole, a new aromatase inhibitor, in postmenopasual women with advanced metastatic breast cancer. Journal of Clinical Oncology 1992;10(1):111-6. [DOI] [PubMed] [Google Scholar]
Smith 2005 {published data only}
- Smith IE, Dowsett M, Ebbs SR, Dixon MJ, Skene A, Blohmer JU et al. Neoadjuvant treatment of postmenopausal breast cancer with anastrozole, tamoxifen, or both in combination: the IMPACT multicenter double-blind randomized trial. Journal of Clinical Oncology 2005;23(22):5108-16. [DOI] [PubMed] [Google Scholar]
Svenstrup 1994 {published data only}
- Svenstrup B, Herrstedt J, Bruenner N, Bennet P, Wachmann H, Dombernowsky P. Sex hormone levels in postmenopausal women with advanced metastatic breast cancer treated with CGS 169 49A. European Journal of Cancer 1994;30A(9):1254-8. [DOI] [PubMed] [Google Scholar]
Wang 2003 {published data only}
- Wang HQ, Ren CC, Feng WJ, Lin MB, Xiong YQ, Huang P et al. Treatment of advanced metastatic breast cancer with exemestane, a multicenter randomized controlled study of 195 cases. Zhonghua Yi Xue Za Zhi 2003;83(3):188-90. [PubMed] [Google Scholar]
References to ongoing studies
CAAN {published data only}
- CAAN. Ongoing study. February 2002. Contact author for more information.
ECOG E4101 {published data only}
- ECOG E4101. Ongoing study. Starting date of trial not provided. Contact author for more information.
ICR‐CTSU Sofea {published data only}
- SofeaPhase III. Ongoing study. March 2004. Contact author for more information.
Paridaens 2003 {published data only}
- Phase III EORTC-10951. Ongoing study. Starting date of trial not provided. Contact author for more information.
Additional references
Beatson 1896
- Beatson GT. On the treatment of inoperable cases of carcinoma of the mamma. Suggestions for a new method of treatment with illustrative cases. Lancet 1896;2:104-7. [PMC free article] [PubMed] [Google Scholar]
EBCTCG 2005
- Early Breast Cancer Trialists' Cooperative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005;365:1687-1717. [DOI] [PubMed] [Google Scholar]
Ferlay 2000 [Computer program]
- Globocan 2000: Cancer Incidence, Mortality and Prevalence Worldwide. Ferlay J, Bray F, Pisani P and Parkin DM, Version 1. Lyon: IARC Press, 2001.
Gibson 2007
- Gibson LJ, Dawson CL, Lawrence DJ, Bliss JM. Aromatase inhibitors for treatment of advanced breast cancer in postmenopausal women. Cochrane Database of Systematic Reviews 2007, Issue 1. [DOI: 10.1002/14651858] [DOI] [PubMed] [Google Scholar]
Hayward 1977
- Hayward JL, Carbone PP, Heuson JC, Kumaoka S, Segaloff A, Rubens RD. Assessment of response to therapy in advanced breast cancer: a project of the Programme on Clinical Oncology of the International Union Against Cancer, Geneva, Switzerland. Cancer 1977;39(3):1289-94. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327(7414):557-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Howell 1997
- Howell A, Dowsett M. Recent advances in endocrine therapy of breast cancer. BMJ 1997;315:863-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ibrahim 1995
- Ibrahim NK, Buzdar AU. Aromatase inhibitors: current status. American Journal of Clinical Oncology 1995;18(5):407-17. [DOI] [PubMed] [Google Scholar]
Mauri 2006
- Mauri D, Pavlidis N, Polyzos NP, Ioannidis JP. Survival with aromatase inhibitors and inactivators versus standard hormonal therapy in advanced breast cancer: meta-analysis. Journal of the National Cancer Institute 2006;98(18):1285-91. [DOI] [PubMed] [Google Scholar]
Miller 1996a
- Miller WR. Aromatase inhibitors. Endocrine-related Cancer 1996;3:65-79. [Google Scholar]
Parmar 1995
- Parmar MKB, Machin D. Survival analysis: A Practical Approach. John Wiley, 1995. [Google Scholar]
Roseman 1997
- Roseman BJ, Buzdar AU, Singletary SE. Use of aromatase inhibitors in postmenopausal women with advanced breast cancer. Journal of Surgical Oncology 1997;66:215-20. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Cochrane 2007
- Gibson LJ, Dawson CK, Lawrence DH, Bliss JM. Aromatase inhibitors for treatment of advanced breast cancer in postmenopausal women. Cochrane Database of Systematic Reviews 2007, Issue 1. [DOI] [PubMed] [Google Scholar]