

Abstract
Aim
We aimed to develop up‐to‐date references with standard deviation scores (SDS) for prepubertal and total height.
Methods
Longitudinal length/height measures from 1572 healthy children (51.5% boys) born at term in 1989‐1991 to non‐smoking mothers and Nordic parents were obtained from the GrowUp 1990 Gothenburg cohort. A total height SDS reference from birth to adult height was constructed from Quadratic‐Exponential‐Pubertal‐Stop (QEPS) function estimated heights based on individual growth curves. A prepubertal height SDS reference, showing growth trajectory in the absence of puberty, was constructed using the QE functions.
Results
The total height reference showed taller prepubertal mean heights (for boys 1‐2 cm; for girls 0.5‐1.0 cm) with a narrower normal within ± 2SDS range vs the GrowUp 1974 Gothenburg reference. Adult height was increased by + 0.9 cm for women (168.6 cm) and by + 1.6 cm for men (182.0 cm). Height in children growing at −2SDS (the cut‐off used for referrals) differed up to 2 cm vs the GrowUp 1974 Gothenburg reference, 3 cm vs Swedish 1981 references and World Health Organisation (WHO) 0‐5 years standard, and 6‐8 cm vs the WHO 5‐19 years reference.
Conclusion
Up‐to‐date total and prepubertal height references offer promise of improved growth monitoring compared with the references used in Sweden today.

Abbreviations
- AgeP5
age at which 5% of the P‐function growth is reached
- CI
confidence interval
- E
negative exponential growth function of age E (age) in cm
- GA
gestational age
- LMS
In the LMS method, the age‐related data distribution is summarised by three smooth age‐dependent parameters L, M and S: the Box‐Cox power Lambda (L), the median (M) and the coefficient of variation Sigma (S)
- P
quadratic logistic function describing the pubertal growth P (age) in cm
- Q
quadratic growth function of age Q (age) in cm
- QE
sum of Q & E‐function giving non‐pubertal growth QE (age) in cm,) equal to total prepubertal height in cm as a function of age
- QEPS
quadratic‐exponential‐pubertal‐stop growth model
- S
stop function S (age) in cm, stopping the Q function at the end of growth
- SDS
standard deviation score
- T
total height function in cm; T (age) = QEPS (age) = Q (age) + E (age) + P (age) – S (age)
Key notes.
Up‐to‐date height references with standard deviation scores allowing more accurate monitoring of growth in children are needed.
Total and prepubertal height references were generated based on longitudinal height measurements from a homogeneous subgroup of healthy children of the GrowUp 1990 Gothenburg cohort.
New references show that prepubertal children are taller (+0.5‐3 cm in girls; +1‐3 cm in boys), and the normal range is narrower, when compared to the current Swedish growth charts.
1. BACKGROUND
It is well established that growth during infancy, childhood and adolescence provides a good indication of the well‐being of the individual, with poor growth often reflecting underlying psychosocial problems, medical diseases or syndromes. Repeated accurate measurement and assessment of height in comparison with that expected in healthy individuals is therefore of great importance throughout the entire growth period.1, 2 Such evaluations are made possible by the existence of height references depicting growth in healthy infants, children and adolescents.3 In Sweden, growth has been assessed relative to references since the 19th century.4, 5, 6 Today, three references with accompanying growth charts are approved for use within the Swedish healthcare system.7, 8, 9, 10
To be most useful for healthcare systems, height references should be generated based on longitudinal data obtained from a relatively homogeneous, healthily growing population.7, 8, 11, 12 Individuals who are unhealthy due to chronic diseases, with syndromes or born preterm are typically omitted. Consideration must also be made of environmental and socioeconomic factors during and after birth when selecting individuals. Smoking during pregnancy is known to influence growth in utero and after birth.13 It is also important to select a reference population that is born in a time period close to that being studied. This is owing to the continuing secular trend for height to increase in each successive generation in most western countries, including the Nordics.11, 12, 14 Furthermore, there is considerable variation between populations in terms of the precise pattern of growth over time, as well as adult height.8, 15, 16 As a result, populations grow at different paces, with some populations being notably shorter or taller than others.12 Owing to these differences, it is still useful to have national growth references. When selecting the population to use to generate a new height reference, it is important to take all of these factors into consideration.
Growth models have primarily been generated to test hypotheses about the regulation and mechanisms responsible for growth in humans.17, 18 However, individual growth curves constructed by such models from attained heights can also be used to develop growth references. Such references provide details of the various functions thought to underlie the different phases of human growth. In 2000, this method was used by our group to develop a graphical reference for prepubertal height in Sweden, based on the childhood component of the infancy‐childhood‐puberty (ICP) model.7, 18 A similar approach was used by Rikken and Wit in the development of their reference for childhood growth.19 Being able to adjust the reference based on the onset of pubertal growth is particularly important when assessing individuals in whom puberty is delayed. Growth in these individuals will typically follow the prepubertal height trajectory at a time point when growth in their peers has already started to accelerate owing to the pubertal growth spurt.
The primary aim of this study was to develop an up‐to‐date reference for total length/height from birth to adult height serving as a tool for monitoring growth. As part of this, we aimed to produce a prepubertal height reference depicting the growth expected in individuals continuing to follow a prepubertal growth trajectory. These two height references were developed using the Quadratic‐Exponential‐Pubertal‐Stop (QEPS) model and were based on longitudinal length/height data from a homogeneous cohort selected from the GrowUp 1990 Gothenburg cohort born in Sweden.20 The population was selected to include healthy children born at term to Nordic parents; children with known chronic diseases and syndromes, and children born to mothers who smoked during pregnancy having been excluded.
Secondary aims of the study were to assess the impact of including vs excluding mothers who smoked during pregnancy on the reference and to compare the new reference with those currently used in Sweden: the GrowUp 1974 Gothenburg,7 Swedish 1981,9 World Health Organisation (WHO) 0‐5 years standard8 and WHO 5‐19 years10 references.
2. MATERIAL AND METHODS
2.1. Ethical approval
Ethical approval was obtained from the Regional Ethics Review Board in Gothenburg (Ad 444‐08 T062‐09). Informed consent was given by participants for examination at school and use of growth data from previous sources. Legal guardians gave informed consent for individuals less than 18 years of age.
2.2. Reference population
The population used to construct the reference, Table 1, was selected from the entire cohort of GrowUp 1990 Gothenburg, Table S1.20 This included 1572 healthy children (763 girls, see Table 1a; 809 boys, see Table 1b) born to Nordic parents in Sweden between 1989 and 1991, for whom information on longitudinal growth until adult height was available. All children selected were born at full term, gestational age (GA), 37‐43 weeks21 and had non‐smoking mothers. Height and weight were measured at obstetric clinics, well‐baby clinics, child healthcare centres and schools; a mean of 24 measurements were obtained per child.
Table 1.
(A) Reference population for girls; (B) Reference population for boys
| Variable | N | Mean | 95% | SD | Skewnes | P‐value |
|---|---|---|---|---|---|---|
| (A) | ||||||
| Gestational age, days | 763 | 281.1 | 280.4‐281.7 | 9.16 | 0.31 | 0.4369 |
| Birth weight, gram | 763 | 3563 | 3528‐3598 | 495 | 0.25 | <.0001 |
| Birth length, cm | 763 | 50.23 | 50.09‐50.38 | 2.00 | 0.09 | <.0001 |
| Emax, cm | 763 | 62.82 | 62.62‐63.02 | 2.84 | 0.23 | .6877 |
| Etimescale | 763 | 0.99 | 0.98‐1.00 | 0.09 | 0.19 | <.0001 |
| Qmax, cm | 763 | 98.66 | 98.10‐99.22 | 7.85 | 0.12 | .0453 |
| AgeTPHV, years | 759 | 11.80 | 11.73‐11.87 | 1.00 | ‐0.04 | .0141 |
| Menarche, years | 720 | 12.88 | 12.79‐12.98 | 1.29 | 0.04 | .1676 |
| AgeP5, years | 763 | 9.82 | 9.75‐9.89 | 1.00 | ‐0.01 | .0130 |
| AgeP50, years | 763 | 12.04 | 11.97‐12.11 | 0.99 | ‐0.02 | .0136 |
| Pmax, cm | 763 | 12.96 | 12.71‐13.22 | 3.55 | 0.15 | .6885 |
| Tmax, cm | 763 | 168.21 | 167.75‐168.66 | 6.38 | 0.11 | .0016 |
| Adult height, cm | 763 | 168.56 | 168.11‐169.02 | 6.40 | 0.14 | .0020 |
| Height of mother, cm | 748 | 167.20 | 166.79‐167.60 | 5.68 | 0.17 | .8279 |
| Height of father, cm | 717 | 181.68 | 181.20‐182.16 | 6.54 | ‐0.03 | .0285 |
| (B) | ||||||
| Gestational age, days | 809 | 281.0 | 280.3‐281.6 | 9.31 | ‐0.36 | .6804 |
| Birth weight, gm | 809 | 3691 | 3655‐3725 | 500 | 0.16 | <.0001 |
| Birth length, cm | 809 | 51.0 | 50.9‐51.2 | 2.10 | 0.18 | <.0001 |
| Emax, cm | 809 | 65.1 | 64.9‐65.3 | 2.70 | 0.03 | .8376 |
| Etimescale | 809 | 0.98 | 0.98‐0.99 | 0.09 | 0.03 | <.0007 |
| Qmax, cm | 809 | 105.6 | 105.1‐106.1 | 7.59 | 0.16 | .0491 |
| AgeTPHV, years | 809 | 13.67 | 13.60‐13.74 | 0.96 | 0.01 | .0028 |
| AgeP5, years | 809 | 11.80 | 11.73‐11.87 | 0.97 | ‐0.02 | .0028 |
| AgeP50, years | 809 | 13.81 | 13.75‐13.88 | 0.96 | 0.02 | .0027 |
| Pmax, cm | 809 | 17.3 | 17.0‐17.5 | 3.71 | ‐0.17 | .4059 |
| Tmax, cm | 809 | 181.8 | 181.3‐182.2 | 6.41 | 0.09 | .0003 |
| Adult height, cm | 809 | 182.0 | 181.6‐182.5 | 6.42 | 0.10 | .0004 |
| Height of mother, cm | 745 | 167.4 | 167.0‐167.8 | 5.89 | ‐0.05 | .1373 |
| Height of father, cm | 709 | 181.2 | 180.7‐181.71 | 6.77 | 0.16 | .0941 |
(A) Healthy girls and (B) healthy boys born in around 1990 to non‐smoking mothers for whom good quality longitudinal data were available. Descriptive data and statistical comparison with Tables S2a and S2b (smoking mothers during pregnancy). No variable was statistically different to Tables S3a and S2b (all mothers, independent of smoking, respectively).
Abbreviations: Adult height, Team‐measured adult height, and if Tmax was higher, the difference was added; AgeP5(50), age at which 5 (50)% of the P‐function is reached; CI, confidence interval; E (Q,P,T) max, maximum of E (Q,P,T) function; SD, standard deviation; TPHV, from Total curve estimated Peak Height Velocity.
Adult height: a trained team‐measured individuals in their twelfth school year. Height was measured to the nearest 0.1 cm using a calibrated Harpenden stadiometer (Holtain Ltd).20 Adult height was defined based on an increase in height of <0.5 cm during the previous 12 months; individuals who were still growing underwent additional measurements until adult height was attained. Health status and ethnicity were obtained via questionnaire given to students at the time of growth measurement.20
Maternal health: information on maternal smoking habits during pregnancy was obtained from the Medical Birth Registry, and 335 children (155 girls) were omitted from the reference population due to maternal smoking, see Tables S1 and S2.
Data on breastfeeding were not available for the study cohort; however, Swedish breastfeeding statistics for 1990 show that 97% of infants were breastfed during the first week of life, falling to 88% at 2 months, 70% at 4 months and 54% at 6 months.22
Visual growth curve analysis and use of a mathematical selection tool (MathSelect < 0.975) ensured that growth data for the individuals selected was of high quality; an additional selection criterion was used to restrict the sample to individuals with serial height measurements covering all the growth phases.23 For more information, see Table 1 for healthy girls/boys born to non‐smoking mothers in 1990, Table S2 for healthy boys/girls born in 1990 to smoking mothers and Table S3 for all healthy girls/boys born in 1990, regardless of maternal smoking habits.
2.3. QEPS method
References for age were constructed for both total height and prepubertal height and were computed in two steps. Firstly, the observed individual data were fitted using the QEPS model, Supplemental information and Figure S1, left.17 In the next step, a set of age points was defined for the entire growth period. At each age point, distributions were fitted with maximum likelihood estimation onto the corresponding values of the individual QEPS functions using the Box‐Cox power exponential transformation.24 This transformation is designed to reduce non‐normality of errors in a linear model and it can be used to describe various data distributions, from the normally distributed to the skewed or kurtotic. All function values of T (age) were used to construct a reference for total height, that is including Q, E, P and S functions; function values of Q (age) and E (age) from the total height function (QE (age) were used to construct the prepubertal height reference, that is summing Q and E functions. Age at onset of the pubertal growth spurt for each individual was defined as AgeP5, the age at which 5% of P‐function‐related growth was attained (Figure S1, right). The computation of prepubertal height reference is shown in Figure S2: attained height values between 4 years of age until AgeP5 (left), individual prepubertal (QE) height curves obtained from prepubertal heights until AgeP5 in Figure S2A, and until 16yrs of age in Figure S2B (centre), and the resulting prepubertal QE function based reference, mean and SDS (right).
2.4. Comparison between total height 1990 references obtained using QEPS or LMS method
LMS‐derived growth references, introduced by Cole and Green,25 are commonly used to model total height and are widely regarded to be reliable.3 The LMS method summarises the age‐related data distribution using a three parameter Box‐Cox power distribution, corresponding to age‐dependent skewness (L), median (M) and coefficient of variation (S). We compared the total height references obtained using the QEPS and LMS methods to ascertain whether both were similar. As seen in Figure S3, the total height references generated by QEPS and LMS methods did not differ systematically. See Supplement for LMS method used.
2.5. Materials used in present Swedish references for comparisons
Comparisons were made between the new growth references and the references currently used within the healthcare system in Sweden; these include the GrowUp 1974 Gothenburg,7, 21 Sweden 1981,8 WHO 0‐5 years9 and WHO 5‐19 years10 references. See Supplement for information on materials and methods used.
2.6. Statistical evaluations
Data analysis was performed with Matlab software (version R2015b; The Mathworks). The Matlab Curve Fitting Toolbox was used for nonlinear curve fitting and customised for penalised nonlinear fitting of individual curves.17 For the individual parameters, 95% confidence intervals (CIs) were estimated. To simplify general mathematical formulae, age was assumed to be equal to age corrected for GA. For comparisons between groups, t‐tests were used if data were normally distributed; otherwise, non‐parametric tests were used. Normality was tested using the SAS Univariate procedure (Shapiro‐Wilk) and nonparametric tests using the SAS NPAR1WAY procedure (Mann‐Whitney). The figures were prepared with SAS software, version 9.3. Cubic spline interpolation was used in order to make smooth curves in the figures and to compare the different methods.
3. RESULTS
3.1. Total height reference based on the 1990 cohort
The new references for total height (mean ± 2SDS) are shown in Figure 1 (left, 0‐2 years; middle, 2 − 20 years). For each of the 1572 individuals in the reference population, a QEPS function derived growth curve from birth to adult height was obtained. Mean adult height was 168.6 cm for girls and 182.0 cm for boys; the sex‐difference in height was 13.4 cm. The onset of the pubertal growth spurt occurred 1.9 years earlier in girls than in boys (Table 1). Table S4 presents the numerical values for mean and SD at selected ages from birth to 20 years and at adult height for the total height references for boys and girls.
Figure 1.
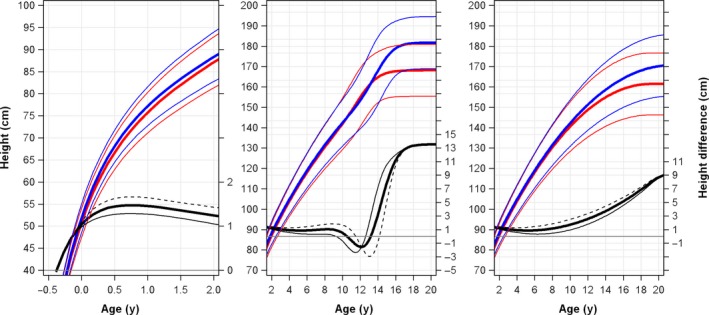
New 1990 references for total height and prepubertal height in girls and boys. References for total height generated based on the Q, E, P and S functions (left and middle panels) and for prepubertal height based on the Q and E functions of the QEPS model (right panel). Values shown are mean ± 2SDS for girls (red) and boys (blue) of different ages. The difference in mean height gained (thick solid black line), +2SDS (thin solid black line) and −2SDS (dotted black line) for boys relative to girls is shown at the bottom of each graph. The 1990‐born population used to generate the reference is described in Table 1. For numerical values, for total height reference see Table S4 and for prepubertal height reference see Table S5
3.2. Prepubertal height reference based on the 1990 cohort
Figure 1 (right) shows growth for boys and girls as a result of the Q and E functions of the QEPS model; the P and S functions are zero before puberty. On average, boys gained 9.2 cm more than girls as a result of growth related to the Q and E functions (Table 1). In Figure 2, the difference in height between the total and the prepubertal height references is shown in the bottom of the figure and numerical values are given in the legend. Table S5 presents the numerical values for mean and SD at selected ages from 4‐16 years for the prepubertal reference values for girls and boys.
Figure 2.
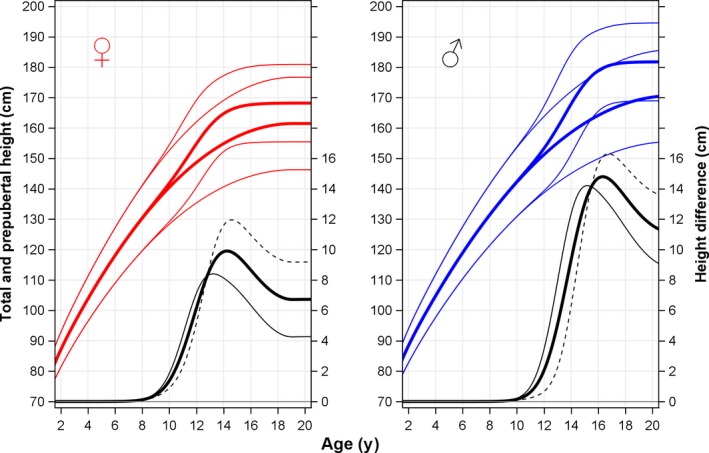
Difference between total and prepubertal height references in girls and boys. References for total height generated based on the Q, E, P and S functions (upper curves) and for prepubertal height based on the Q and E functions of the QEPS model (lower curves). Total height values shown are mean ± 2SDS for girls (in red, left) and boys (in blue, right). The difference in height between the total and the prepubertal reference values for children growing along the mean (thick solid black line), along +2SDS (thin solid black line) and along −2SDS (dotted black line), is shown at the bottom of each graph. The population used to generate the references is described in Table 1. For girls (Figure 2, left), the maximum difference in height between the two references was found at 14.2 y of age for those growing along the mean (difference of 9.9cm), at 13.3 y for girls growing along + 2SDS (difference of 8.4cm), and at 14.6 y for girls growing along −2SDS (difference of 12 cm). The corresponding maximum height differences for boys (Figure 2, right) were found at 16.4 y of age for those growing along the mean (difference to be of 14.8 cm), at 15.3 y of age for those growing at + 2SDS (difference of 14.2 cm), and at 16.8 y of age for those growing at −2SDS (difference of 16.3 cm)
In Figure 3, the new prepubertal QE function estimated reference based on the 1990 cohort is compared with the prepubertal reference used in current growth charts that are based on the prepubertal childhood component (of the ICP model) of the total height reference of the GrowUp 1974 cohort. However, when the 1974 prepubertal reference was estimated by QE functions, it became almost superimposed on the 1990 prepubertal QE‐estimated reference (data not shown).
Figure 3.
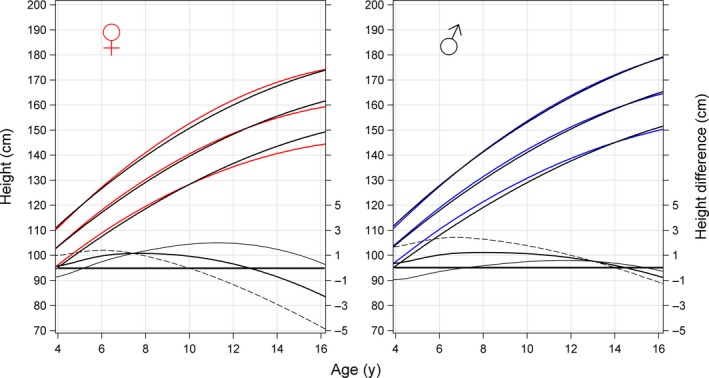
Comparison between the new 1990 prepubertal reference and the 1974 prepubertal reference. Comparison between the new 1990 prepubertal height reference population for girls (red, to the left) and boys (blue, to the right) for mean and ± 2SDS and the 1974 prepubertal reference population (black) in relation to chronological age (y). The right Y‐axis display the corresponding differences between 1990 and 1974 (mean = bold black lines, −2SDS = thin black lines and + 2SDS = broken black lines); zero lines for difference are indicated with a black horizontal line)
3.3. Population selected for 1990 total height reference: influence of smoking during pregnancy
Adult heights attained by healthy girls and boys born to non‐smoking mothers were greater than those attained by children born to smoking mothers; the cumulative proportion of adult heights attained was right‐shifted for children with non‐smoking compared with smoking mothers (P < .001; Figure S4). Both boys and girls born to smoking mothers were approximately 2 cm shorter at adult height compared to children of non‐smoking mothers. When references obtained from healthy children born to non‐smoking mothers in 1990 were compared with those born to all mothers, as seen in Figure S5, the difference at mean height was 0.3SDS in favour of children born to non‐smoking mothers. Of note, the ±2SDS range was narrower at all prepubertal ages for both boys and girls born to non‐smoking mothers. The difference in adult height at –2SDS was 0.6 cm for boys and 0.3 cm for girls, with those born to non‐smoking mothers being of taller stature.
3.4. Comparison of the new total height reference and the GrowUp 1974 Gothenburg reference
The new 1990 reference population of healthy individuals born to non‐smoking mothers was compared to the growth charts used in Sweden since 2000 from the healthy subgroup of the GrowUp 1974 Gothenburg cohort. Figure 4 shows the difference for the means, −2SDS and +2SDS between the two references. The mean and −2SDS of the prebubertal children were 0.5‐1 cm greater for girls and 1‐2 cm greater for boys, whereas the two +2SDS lines were almost superimposed resulting in a narrower normal range for the new reference. Also at adult height, 1990 born were greater than those born 1974:0.9 cm for women and 1.6 cm for men.
Figure 4.
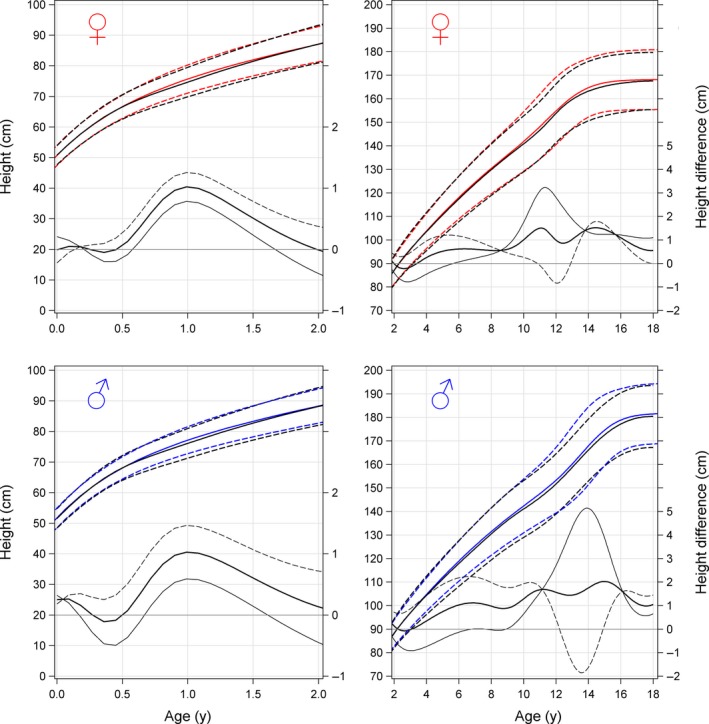
Comparison between the new 1990 reference and the 1974 reference. Comparison between the new 1990 population reference (red/blue) and the 1974 reference used for the growth charts (black).7, 21 Total height is shown in the top panel for girls and in the bottom panel for boys; references for children aged 0‐2 y and 2‐18 y are shown on the left and right panel, respectively. The difference between the total heights obtained using the two references is shown in the bottom panel of each figure. Differences in mean (thick solid black line), in +2SDS (thin solid black line) and in −2SDS (dotted black line) are shown. Visual inspection of data before puberty shows a maximal difference in attained height at −2SDS of 2 cm for boys and 1cm for girls; the corresponding values for the means are 0.5 cm and 1 cm, respectively. For interpretation of difference in normal range (within ± 2SDS): if the dotted thin line for the −2SDS difference is above the thin solid line for the +2SDS difference, the range for ± 2SDS is narrower for the new 1990 reference than for the 1974 all healthy population; as seen, this is the case for both boys and girls at most ages
3.5. Comparison of the new total height reference and the Swedish 1981 reference
As seen in Figure S6, differences between the new 1990 reference and the Swedish 1981 reference were found for both sexes: a difference in height of up to 3 cm in favour of the new height reference was observed for boys growing at −2SDS, and up to 1.5 cm for girls growing at +2SDS. Mean adult height was 1.3 cm greater for boys and 0.7 cm greater for girls in the 1990 reference compared with the Swedish 1981 reference.
3.6. Comparison of the new total height reference and the WHO references
As seen in the left‐hand panels of Figure S7, height was greater at all age points in the new 1990 reference compared to the WHO standard for infants/children aged 0‐5 years. The normal range of height values in the new reference was also narrower than that of the WHO 0‐5‐years standard: between 1‐1.6 cm up to 2 years, and at 5 years it was 2.6 cm and 2.8 cm for girls and boys, respectively. Regarding attained length/height during infancy, there was a difference between the new 1990 reference and the WHO, both the longitudinal 0‐2 years and the cross‐sectional 2‐5 years standards in terms of growth at −2SDS across the entire age periods. For both sexes, height at 5 years of age was over 3 cm greater in the new 1990 reference compared to the cross‐sectional WHO standard.
Overall height was greater on average in the new 1990 reference compared with the WHO reference for children aged 5‐19 years (Figure S7, right). The range associated with ±2SDS was narrower in the new reference compared with the WHO reference. At −2SDS, height based on the new 1990 reference was up to 6 cm greater for girls and 8cm greater for boys than in the WHO reference.
4. DISCUSSION
One of the main reasons for using a height reference in healthcare settings, whether it be in well‐baby clinics, child healthcare clinics or schools, is to use it as a screening tool for early detection of abnormal, unhealthy growth in a child so that referral for investigation of underlying reasons can be put in place.3 Detection of unhealthy growth relies on a clear understanding of what normal healthy growth should look like for an individual child. By virtue of the use of a careful selected homogeneous and recently born population as a basis, the references presented here provide a clearer picture of normal growth than given by the three references in use in Sweden today. The use of a more recently born cohort, in particular, allowed the new reference to take into account changes in height that had occurred in recent years. Data showed that the secular trend for height to increase over time was in fact continuing in Sweden, with height at all ages being greater on average in children born in 1990 than in those born one or two decades earlier. Furthermore, the careful selection of data from as homogeneous as possible a group of healthily growing children served to reduce variability in height owing to the influence of external factors. The reference generated shows the normal distribution of height during infancy and childhood, defined as within ±2SDS, to be a narrower range than indicated by previous growth references; this means that the new reference will be relatively more sensitive at picking up abnormal growth.
As is the case for the height reference used for growth charts in Sweden since the millennium, we present a graphical prepubertal height reference for the adolescent period showing the growth to arise independently of puberty. This so‐called basic growth was modelled using the Q and E functions of the QEPS model17 in a similar way as the childhood component of the ICP model which was used in the earlier references.7, 18 This type of prepubertal growth reference allows the assessment of height in children who have not yet undergone puberty relative to other children at the same chronological age. This has become a valuable tool for identifying individuals in whom height gain is suboptimal during adolescence, as well as for distinguishing between those children with a low growth rate owing to delayed puberty as opposed to diseases affecting growth during the adolescent period.
4.1. A selected reference population
As noted earlier, the narrow range of normal growth associated with the present height reference was obtained by selecting a population that was as homogeneous as possible. To achieve this, the reference population included only healthy children born at term to non‐smoking mothers; children with known diseases and syndromes affecting growth were excluded, as were infants born preterm owing to known differences in postnatal growth pattern compared with those born at term.26 We also selected only children with Nordic parents. The latter served to minimise the influence of different pace of secular trends related to differences in origin.20
Infants born to non‐smoking mothers were selected; by using only children born in Sweden, we were able to obtain data from the Medical Birth Registry about maternal smoking habits. Nicotine intake is known to decrease both intrauterine27 and postnatal growth.13 Our results showed individuals born to mothers who smoked during pregnancy to be on average as much as 2 cm shorter as adults than those born to non‐smoking mothers. However, smoking as the major reason for the finding of short stature should be interpreted with caution as smoking is known to be a proxy marker of socioeconomic status, which has long been known to influence childhood growth.28, 29
In the present study, we showed that Swedish infants and children grew taller than expected based on the WHO growth standard. This finding was not completely unexpected because, although the WHO standard was generated based on data from carefully selected normally growing children (born at term to non‐smoking, breastfeeding mothers of the highest socioeconomic class), it deliberately included data from ethnic groups of different stature owing to the intention to create a growth standard applicable to children across the globe.8 While this decision was made based on the assumption that the positive secular trend in infancy and early childhood growth had stopped, a Finnish study among others highlighted that the WHO standard was of limited usefulness for detecting abnormal growth in counties with tall population with positive ongoing secular trends for height.15, 16 In Sweden, as well as the population being taller than expected based on WHO standards, we know that there is an ongoing secular trend for height to increase by 0.6‐0.8 cm per decade12; in this scenario, it is likely that children with growth disorders will appear to be growing normally relative to WHO standards at a time when measures to improve growth should ideally be implemented. The new population‐specific reference presented here has the potential to improve the detection of growth disorders owing to its more precise and up‐to‐date reflection of height in the Swedish population. Furthermore, the potential to adjust our reference according to the target height of the individual may make it of wider utility in other populations.
4.2. Why was the QEPS model method used?
The main reason for using the QEPS model to generate the height reference was to allow the separation of growth that was specific to puberty from that arising independently of puberty. This was achieved by generating a reference for total growth using the Q, E, P and S functions, and a reference for basic growth arising independently of puberty based on the Q and E functions. Reassuringly, the total growth reference obtained using the QEPS model appeared to be similar to the one obtained using the LMS method.17, 25
4.3. Strengths and limitations
One of the challenges of studies involving longitudinal monitoring of growth is data completeness. In the GrowUp 1990 Gothenburg study, the team was only able to measure adult height in 59% of students in the twelfth school year, and 54% were born in 1989‐1991 and were eligible for inclusion in the present study; out of the latter group, around one‐third fulfilled the inclusion criteria for the reference population. One of the limitations of this approach will be that information based on such a select subpopulation will not tell us about growth in the entire population.28 Consistent with this, we have previously shown that different subgroups of the 1990 cohort end up with somewhat different adult heights.12 However, to describe the growth of the entire population is not the aim when making a reference to be used for identifying individuals with growth problems. In contrast, the usefulness for monitoring normal growth of the resulting reference in healthcare settings will improve.
Another challenge that applies to growth data is the reliability of the measurements made. Most of the measurements in the current study were made during routine clinical practice, at birth in obstetric clinics, and thereafter at well‐baby‐clinics and in schools, and may be subject to some variability owing to differences in measurement techniques used at sites/by different individuals. Importantly, however, a trained team was involved in the measurement and collection of data at adult height for all children, including boys with delayed puberty, thus ensuring that measurements of adult height were reliable. Moreover, the GrowUp 1974 Gothenburg cohort was followed up in the same way that strengthened comparisons between these two cohorts.
A strength of the present height references was that all postnatal heights were corrected for GA, even though the reference population used was born within the short range defined as at term (37‐43 gestational weeks). However, an updated GA‐related reference remains to be added, as previously done from GA 24 weeks through to 24 months after birth that also took prematurity into account, and which has been used within well‐baby clinics in the Swedish healthcare system since 2005.21
5. CONCLUSION
We present up‐to‐date references for total and prepubertal length/height from birth to adulthood that have been developed using the QEPS model based on longitudinal data from a population of healthy children born in Sweden. One of the strengths of the new references is the narrow range of normal growth obtained during infancy and childhood, thanks to the use of as homogeneous as possible a group of the healthiest children. The use of a recently born cohort as a basis for the reference is an important factor, as this allows the reference to reflect the ongoing secular changes in height within Sweden. The reference is not only for total height but also for prepubertal growth, thereby allowing the assessment of growth independently of whether or not the child is already undergoing puberty. Including these features means that, when used in clinical practice, these references will have the potential to be more sensitive at identifying growth disorders in children than the references used in Sweden today.
CONFLICT OF INTEREST
AFMN works for Muvara, Multivariate Analysis of Research Data, Statistical Consultation, in the Netherlands. The other authors have no conflicts of interest to declare.
Supporting information
ACKNOWLEDGEMENTS
The authors are grateful for the contributions of the twelfth grade students in 1998‐1999 from the Gothenburg area schools and their school nurses; the study team led by Carola Pfeiffer‐Mosesson and Annika Olsson: Ingela Larsson, Erik Niklasson, Emil Häger, Louise Olsson, Lisa Flink, Camilla Oldberg, Niklas Norlander, Emma Hermansson, Lotta Moraeus and Elisabeth Gramatkowski. Thanks also for data support given by Lillemor Ljungberg and Bengt Bengtsson. We would also like to thank the 1974 study team. The careful editing and language revision by Harriet Crofts is highly appreciated.
Albertsson‐Wikland K, Niklasson A, Holmgren A, Gelander L, Nierop AFM. A new Swedish reference for total and prepubertal height. Acta Paediatr. 2020;109:754–763. 10.1111/apa.15129
Funding information
The authors acknowledge financial support from the Swedish Research Council (VR no 7509, 2006‐1506), and grants from The Swedish Council for Working Life and Social Research (2006‐1624), the Government grants under the ALF agreement (ALFGBG‐719041, ALFGBG‐812951), the Region Halland and the Foundation Växthuset for children.
REFERENCES
- 1. van Dommelen P, van Buuren S, Zandwijken GR, Verkerk PH. Individual growth curve models for assessing evidence‐based referral criteria in growth monitoring. Stat Med. 2005;24:3663‐3674. [DOI] [PubMed] [Google Scholar]
- 2. Sankilampi U, Saari A, Laine T, Miettinen PJ, Dunkel L. Use of electronic health records for automated screening of growth disorders in primary care. JAMA. 2013;310:1071‐1072. [DOI] [PubMed] [Google Scholar]
- 3. Cole TJ. The development of growth references and growth charts. Ann Hum Biol. 2012;39:382‐394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Key A.Läroverkskomiténs underdåniga utlåtande och förslag angående organisationen af rikets allmänna läroverk och dermed sammanhängande frågor. 1885.
- 5. Broman B, Dahlberg GN, Lichtenstein A. Height and weight during growth. Acta Pædiatrica. 1942;30:1‐66. [Google Scholar]
- 6. Karlberg P, Taranger J, Engström I, et al. Physical growth from birth to 16 years and longitudinal outcome of the study during the same age period. Acta paediatrica Scandinavica. 1976;65(s258):7‐76. [DOI] [PubMed] [Google Scholar]
- 7. Albertsson‐Wikland K, Luo ZC, Niklasson A, Karlberg J. Swedish population‐based longitudinal reference values from birth to 18 years of age for height, weight and head circumference. Acta Paediatr. 2002;91:739‐754. [DOI] [PubMed] [Google Scholar]
- 8. de Onis M; Who Multicentre Growth Reference Study G . WHO child growth standards based on length/height, weight and age. Acta Paediatr. 2006;95:76‐85. [Google Scholar]
- 9. Werner B, Bodin L. Growth from birth to age 19 for children in Sweden born in 1981: descriptive values. Acta Paediatr. 2006;95:600‐613. [DOI] [PubMed] [Google Scholar]
- 10. de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school‐aged children and adolescents. Bull World Health Organ. 2007;85:660‐667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Tinggaard J, Aksglaede L, Sorensen K, et al. The 2014 Danish references from birth to 20 years for height, weight and body mass index. Acta Paediatr. 2014;103:214‐224. [DOI] [PubMed] [Google Scholar]
- 12. Holmgren ANA, Aronson AS, Sjöberg A, Lissner L, Albertsson‐Wikland K. Nordic populations are still getting taller ‐secular changes in height from the 20th to 21stcentury. Acta Paediatr. 2019;108:1311‐1320. [DOI] [PubMed] [Google Scholar]
- 13. Matijasevich A, Brion MJ, Menezes AM, Barros AJ, Santos IS, Barros FC. Maternal smoking during pregnancy and offspring growth in childhood: 1993 and 2004 Pelotas cohort studies. Arch Dis Child. 2011;96:519‐525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Holmgren A, Niklasson A, Nierop AFM, et al. Estimating secular changes in longitudinal growth patterns underlying adult height with the QEPS model: the Grow Up Gothenburg cohorts. Pediatr Res. 2018;84:41‐49. [DOI] [PubMed] [Google Scholar]
- 15. Saari A, Sankilampi U, Dunkel L. Multiethnic WHO growth charts may not be optimal in the screening of disorders affecting height: Turner syndrome as a model. JAMA Pediatr. 2013;167:194‐195. [DOI] [PubMed] [Google Scholar]
- 16. Juliusson PB, Roelants M, Hoppenbrouwers K, Hauspie R, Bjerknes R. Growth of Belgian and Norwegian children compared to the WHO growth standards: prevalence below ‐2 and above +2 SD and the effect of breastfeeding. Arch Dis Child. 2011;96:916‐921. [DOI] [PubMed] [Google Scholar]
- 17. Nierop AF, Niklasson A, Holmgren A, Gelander L, Rosberg S, Albertsson‐Wikland K. Modelling individual longitudinal human growth from fetal to adult life ‐ QEPS I. J Theor Biol. 2016;406:143‐165. [DOI] [PubMed] [Google Scholar]
- 18. Karlberg J. On the modelling of human growth. Stat Med. 1987;6:185‐192. [DOI] [PubMed] [Google Scholar]
- 19. Rikken B, Wit JM. Prepubertal height velocity references over a wide age range. Arch Dis Child. 1992;67:1277‐1280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Sjöberg A, Barrenäs ML, Brann E, et al. Body size and lifestyle in an urban population entering adulthood: the 'Grow up Gothenburg' Study. Acta Paediatr. 2012;101:964‐972. [DOI] [PubMed] [Google Scholar]
- 21. Niklasson A, Albertsson‐Wikland K. Continuous growth reference from 24th week of gestation to 24 months by gender. BMC Pediatr. 2008;8:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. National Board of Health and Welfare . Pregnancies, deliveries and newborn infants, the Swedish medical birth register 1973–2014, assisted reproduction, treatment 1991–2013. 2015.
- 23. Holmgren A, Niklasson A, Gelander L, Aronson AS, Nierop AFM, Albertsson‐Wikland K. Insight into human pubertal growth by applying the QEPS growth model. BMC Pediatr. 2017;17:107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Rigby RA, Stasinopoulos DM. Smooth centile curves for skew and kurtotic data modelled using the Box‐Cox power exponential distribution. Stat Med. 2004;23:3053‐3076. [DOI] [PubMed] [Google Scholar]
- 25. Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med. 1992;11:1305‐1319. [DOI] [PubMed] [Google Scholar]
- 26. Niklasson A, Engstrom E, Hard AL, Wikland KA, Hellstrom A. Growth in very preterm children: a longitudinal study. Pediatr Res. 2003;54:899‐905. [DOI] [PubMed] [Google Scholar]
- 27. Kawakita A, Sato K, Makino H, et al. Nicotine acts on growth plate chondrocytes to delay skeletal growth through the alpha7 neuronal nicotinic acetylcholine receptor. PLoS ONE. 2008;3:e3945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Hancock C, Bettiol S, Smith L. Socioeconomic variation in height: analysis of national child measurement programme data for England. Arch Dis Child. 2016;101:422‐426. [DOI] [PubMed] [Google Scholar]
- 29. Siahpush M, Farazi PA, Maloney SI, Dinkel D, Nguyen MN, Singh GK. Socioeconomic status and cigarette expenditure among US households: results from 2010 to 2015 Consumer Expenditure Survey. BMJ open. 2018;8:e020571. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials