

Summary
The objectives were to systematically investigate the multiple dimensions of sleep and their association with overweight or obesity among primary school‐aged children. CINHAL, PsycINFO, SPORTDiscus, Medline, Cochrane, Embase, and PubMed databases were searched for papers reporting on an association between children's sleep and weight status. Studies on clinical populations, published in languages other than English, without objectively measured weight status, or where weight status was reported outside the outlined age bracket (5‐13 years) were excluded. A total of 34 248 citations were extracted from our systematic search protocol, of which 112 were included for detailed review. Compared with sleep duration, of which 86/103 articles found a significant inverse association between sleep duration and measured weight status, few studies examined other dimensions of sleep, such as quality, efficiency and bed/wake times, and relationship with weight status. Where studies existed, variation in defining and measurement of these dimensions restricted comparison and potentially influenced discrepancies across results. Overall, the findings of this review warrant the need for further research of the outlined dimensions of sleep. Future research would benefit from clarity on definitions across the different dimensions, along with the use of valid and reliable tools.
Keywords: children, obesity, overweight, sleep, sleep dimensions
Abbreviations
- BMI
body mass index
- BT
bed time
- OR
odds ratio
- Ow/Ob
overweight and obesity
- PSG
polysomnography
- SMP
sleep mid‐point
- SWP
sleep wake pattern
- WT
wake time
1. INTRODUCTION
There is growing evidence internationally that declines in the duration of sleep children obtain is inversely associated with overweight and obesity (Ow/Ob).1, 2, 3, 4 Studies have shown that where children were classified as sleeping for shorter or insufficient durations they had significantly increased odds of being affected by overweight/obesity, compared with those who slept for sufficient durations.5, 6 The proposed etiology of this association suggests that insufficient sleep leads to an energy imbalance via altered hormone regulation, reducing physical activity levels, increasing sedentary time, and a higher caloric intake.6, 7, 8 While several reviews have examined the available literature on the link between sleep duration and rates of overweight and obesity among children,9, 10, 11, 12, 13, 14 there is argument that these overlook more nuanced and potentially important dimensions of children's sleep that might influence this association.
Buysse critiqued the reliance on duration as a measure of sleep, arguing that the dimensions of children's sleep such as efficiency, quality, and sleep timing (onset/off‐set) should also be considered as part of the sleep‐obesity relationship.15 Definitions and categorization of these dimensions differ slightly across studies; however, as guided by definitions from the previous literature,15, 16, 17 these four sleep dimensions can be defined as: Sleep duration: the quantity/length of sleep time obtained; Sleep quality: objectively measured architecture of sleep (adequacy of time spent in the different sleep wave cycles), or subjectively reported satisfaction/perceived problems with sleep; Sleep efficiency: a measure of sleep continuity, incorporating the ease to initiate (sleep latency) and maintain sleep (minimal wake episodes) in an efficient manner, or the percentage of sleep time achieved between bed and wake times; and Sleep timing: the placement of sleep within the 24‐hours of the day, including factors such as bed/wake times.
Beyond the prominent focus of children's sleep duration on the sleep‐obesity association of previous reviews, 9, 10, 11, 12, 13, 14 there is emerging literature for each of these additional dimensions. For example Jarrin et al studied 240 Canadian children and adolescents (aged 8‐17 years) and found that, independent of self‐reported sleep duration, children with delayed sleep timing (late to bed and late to wake) related to a higher risk of being affected by overweight and obesity relative to early to bed/wake counterparts.18 An Australian study found later bedtimes were linked with higher body mass index (BMI) z‐scores and lower diet quality scores regardless of self‐reported wake time.19 Sleep quality and sleep efficiency have also been highlighted as important dimensions of sleep associated with overweight and obesity risk among children.20, 21, 22 Lui et al used polysomnography (PSG) to analyze sleep quality by recording stages of sleep among a sample of American children and adolescents (7‐17 years). It is suggested that nonrapid eye movement (REM) sleep could be an important stage of sleep for endocrine and metabolic regulation as reduced REM was associated with higher BMI z‐scores.23 Furthermore, the authors also reported that higher sleep efficiency (determined by the percentage of time spent asleep between sleep onset to wake time, measured via PSG) was a significant dimension of sleep associated with reduced risk of overweight and obesity.23 While PSG is considered the gold standard for measuring multiple sleep components, it is quite invasive and costly and therefore not always practical for use in larger samples.24 Self‐reported proxies for sleep quality and efficiency have therefore often been used, with results appearing to support those from more objective measures. Studies have reported that those with lower self‐perceived sleep quality (ie, less likely to report sleeping “well”) or lower perceived sleep efficiency (reported issues around waking up during the night or issues falling asleep) are more likely to experiences poorer weight status outcomes.25
With emerging empirical evidence of associations between the specific dimensions of sleep and weight status, a more nuanced understanding of these associations is now possible and needed to adequately inform future obesity prevention initiatives.11, 12 A systematic understanding of the current conceptions and measurements of the dimensions of sleep is needed; and an examination of variability of results across the different dimensions of sleep will help determine the importance of these on the sleep‐obesity association, among population samples.
As sleep requirements notably vary across the life span, with quite considerable differences in optimal sleep duration recommendations for primary school aged children (5‐13 years; 9‐11 hours per night) compared with those for adolescents (14‐18 years; 8‐10 hours per night), the association between sleep habits and obesity needs to be unpacked across the age groups.26, 27 Furthermore, there is a particular need to better understand the etiology of obesity among early primary school‐aged children. Data from the National Child Measurement Program in England found that of children with obesity at the beginning of primary school only 10% were of a healthy weight by the end of primary school, while more than two thirds remained in the category of being with obesity or severe obesity.26 Therefore, with strong evidence for the tracking of obesity and health behaviors from this age through to adolescence and beyond, 26, 27, 28, 29 along with the differences in sleep needs, there is a need to better understand the sleep‐obesity nexus of this particular at risk age group. This article presents a systematic review of the peer‐reviewed literature with data on the association between different dimensions of sleep and weight status among primary school‐aged children (5‐13 years old).
2. METHOD
2.1. Literature search
Following the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) review process, a systematic search was conducted across CINHAL, PsycINFO and SPORTDiscus (via EBSCOhost), Medline, Cochrane, Embase, and PubMed databases. A search strategy (available in Table S1) was used to extract literature published up until March 2018. Our search strategy was informed by previous systematic reviews of sleep and weight status of children,9, 10, 11, 12, 13, 14 including all appropriate search terms and additional terms for dimensions of sleep. The search strategy was adapted to search each database for original research articles published in English and in peer‐reviewed journals.
2.2. Inclusion/exclusion criteria
Included studies were restricted to (a) peer‐reviewed original research; (b) contain some measure of sleep; (c) had objectively measured weight status; (d) report on the association between the two variables (sleep and weight status); (e) participants were primary school aged children (aged 5‐13 years); and (f) sample was nonclinical/free‐living population. Reviews, meta‐analyses, dissertations, expert opinions, conference abstracts, unpublished studies, and studies published in a language other than English were excluded from the review. Studies were also excluded if the main outcome variable (children's weight status) was reported outside the age bracket (5‐13 years).
2.3. Recording and synthesis of findings
For each included article, the two reviewers (B.M. and C.S.) independently utilized a developed data extraction tool (available in Table S2) to obtain relevant information for each study (eg, study design, sample characteristics, dimension[s] of sleep analyzed, association of each dimension, and the main findings). The study quality was also assessed for each article utilizing an adjusted version of the Newcastle‐Ottawa Scale (NOS),30, 31 with a 10‐point star scale (10 as the highest quality) to critic studies based on the selection of the study groups (two points), the comparability of the groups (three points), and the ascertainment of either the exposure or outcome of interest (five points).
The two data sets were then cross checked and discrepancies amended, using a third reviewer (S.A.) if required. Once included in the review, a narrative synthesis of the data was conducted. Studies were grouped by dimension of sleep and then measurement type categories, enabling comparison of results and measurements across and within each of the different dimensions of sleep.
3. RESULTS
A total of 34 248 citations were extracted from the outlined databases using the key search terms, and duplicate citations (n = 11 001) were removed (see Figure 1). Following the inclusion/exclusion criteria, abstracts were screened and a total of 22 852 irrelevant articles were excluded. The remaining 393 articles were read in full, with 281 excluded: 120 did not meet the age criteria (5‐13 years); 8 were of clinical or nonfree‐living population groups; 8 did not measure weight status objectively; 68 did not analyze the association between sleep‐obesity; and 77 were excluded either due to being non‐English, not peer‐reviewed, review/meta‐analysis, duplicate data, or a conference abstract/other unpublished data. This left 112 articles deemed relevant and included in the analysis (Table 1).8, 20, 21, 22, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137, 138, 139, 140, 141
Figure 1.
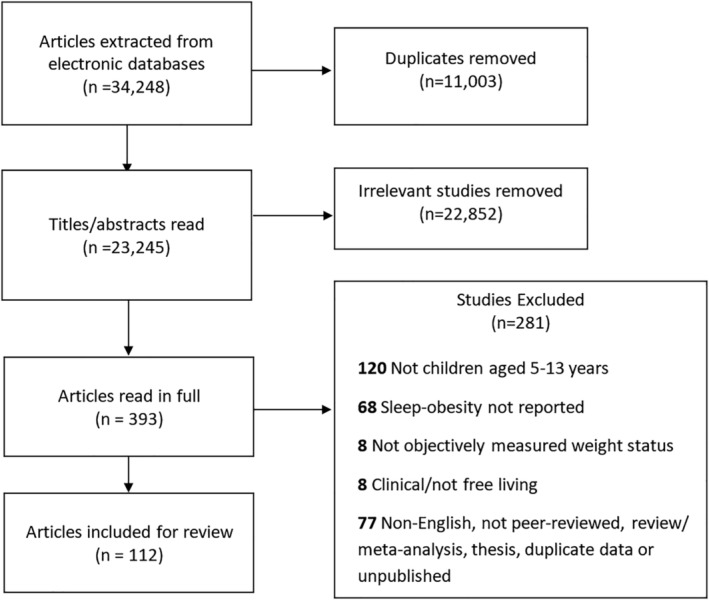
Flow chart of article selection process
Table 1.
Study characteristics and main resultsa
| First author (year) | Sample size; country; study design | Age group | Measure of sleep | Measure of weight status | Report association | Study quality | |||
|---|---|---|---|---|---|---|---|---|---|
| Sleep duration | Sleep efficiency | Sleep quality (low to high) | Sleep timing | ||||||
| Agras et al (2004)32 | 150; USA; LT | 9.5 y (from birth) | Parent report | BMI >85th percentile = OW/OB | ✓ NEG | 3 | |||
| Alamian et al (2016)33 | 895; USA; LT | 11 ± 2 | Parent report | BMI z (CDC) | ✓ NEG | 7 | |||
| Alqaderi et al (2017)34 | 6316; Kuwait; LT | 12 (from 10) | Self‐report | WC | ✓ POS | 6 | |||
| Altenburg et al (2013)35 | 5757; Belgium, Greece, Hungary, The Netherlands, Norway, Slovenia and Spain; CS | 10‐12 y | Parent report | BMI (IOTF); WC | ✓ NEG | 10 | |||
| Amigo et al (2014)36 | 291; Spain; CS | 9‐10 y | Self‐report | BMI (IOTF) | ✓ NEG | ✓ POS (BT) | 6 | ||
| Anderson et al (2017)37 | 10 995; UK; LT | 11 (from 3) | Parent report | BMI z (IOTF) | ✓ SIG (BT consistency) | 8 | |||
| Anujuo et al (2016)38 | 2384; Amsterdam; CS | 5 | Parent report | BMI z (IOTF) | NS | 6 | |||
| Arora and Taheri (2015)39 | 511; UK; CS | 11‐13 y | Accelerometry | BMI‐z | ✓ NEG | NS (%) | 8 | ||
| Bagley and El‐Sheikh (2013)40 | 228; USA; CS | 9‐12 y | Accelerometry | BMI z (CDC) | ✓ NEG | ✓ NEG (%) | 7 | ||
| Bagley and El‐Sheikh (2014)20 | 235; USA; CS | 8‐10 y | Accelerometry | BMI z (CDC) | ✓ NEG | ✓ NEG (%) POS (LWE) | 7 | ||
| Barlett et al (2012)41 | 1156; USA; LT | 6‐12 y | Self‐report | BMI z (CDC) | ✓ NEG (CS and L) | 6 | |||
| Bayer et al (2009)42 | 7767; Germany; CS | 3‐10 y | Parent report | BMI z (IOTF); BF% (skin folds‐KFA) | ✓ NEG | 3 | |||
| Bell and Zimmerman (2010)43 | 1108; USA; LT | 5‐8 y (from 0 to 4) | Parent report | BMI z (CDC) | ✓ NEG (CS and L) | 7 | |||
| Berentzen et al (2014)44 | 1481; Netherlands; CS | 11‐12 y | Self‐report | BMI z (IOTF); WC | ✓ NEG | NS (night awakenings) | NS | NS (SWP) | 5 |
| Busto‐Zapico et al (2014)45 | 291; Spain; CS | 9‐10 y | Parent report | BMI z (ITOF) | NS | ✓ POS (BT) | 5 | ||
| Cameron et al (2013)46 | 7234; Europe (Belgium, Greece, Hungary, the Netherlands, Norway, Slovenia and Spain); CS | 10‐12 y | Parent report | BMI z (IOTF); WC | ✓ NEG | 6 | |||
| Cao et al (2015)47 | 8760, China, CS | 6‐12 | Self‐report | BMI | ✓ NEG (girls), POS (boys) | 6 | |||
| Carrillo‐Larco et al (2014)48 | 1929; Ethiopia, India, Peru and Vietnam; CS | 7‐8 y | Parent report | BMI z (IOTF) | NS | 5 | |||
| Carter et al (2011)49 | 202; NZ; LT | 7 y (from 3 and 5) | Accelerometry | BMI; BF% (bioelectrical impedance) | ✓ NEG (CS and L) | 10 | |||
| Casazza et al (2011)50 | 104 (subsample); UK; CS | 7‐12 y | Parent report | BF% (DXA); BMI z (CDC) | NS | 6 | |||
| Cassimos et al (2011)51 | 353; Greece; CS | 11‐12 y | Self‐report | BMI z (IOTF) | NS | NS (BT) | 4 | ||
| Chahal et al (2013)52 | 3398; Canada; CS | 10‐11 y | Parent report | BMI z (IOTF) | NEG | 8 | |||
| Chaput and Tremblay (2006)53 | 422; Canada; CS | 5‐10 y | Parent report | BMI z (IOTF); WC | ✓ NEG | 6 | |||
| Colley et al (2012)54 | 878; Canada; CS | 6‐11 y | Accelerometer (nonwear time) and; parent report | BMI; WC | ✓ NEG (accel only) | 8 | |||
| Combs et al (2016)55 | 348, USA, CS (LT out of age range) | 7.6‐10.1 | Parent report | BMI z (CDC) | ✓ NEG (weekday only, NS weekend) | ✓ POS (BT) NS (WT) | 5 | ||
| De Jong et al (2012)56 | 840; Netherlands; CS | 9‐13 (subsample) | Parent report | BMI z (IOTF); WC | ✓ NEG | 7 | |||
| Del Pozo‐Cruz et al (2017)57 | Subsample of 1812, New Zealand, CS | 5‐9 | Self‐report | BMI | ✓ NEG | 6 | |||
| Diethelm et al (2011)58 | 481; Germany; LT | 7 y (from 2) | Parent report | BMI z (IOTF); BF% (skin fold‐Deurenberg); FMI; FFMI | ✓ NEG | 7 | |||
| Drescher et al (2011).59 | 319; USA; CS | 10‐13 y | Parent report | BMI z (CDC); skin fold | ✓ NEG | 4 | |||
| Duncan et al (2008)60 | 1229; NZ; CS | 5‐11 y | Parent report | BMI; BF% (bioelectrical impedance) | ✓ NEG | 7 | |||
| Duran and Haro (2016)61 | 1810; Chile; CS | 6‐11 | Parent report | BMI | ✓ NEG | 8 | |||
| Eisenmann et al (2006)62 | 6324; Australia; CS | 7‐13 y (subsample) | Self‐report | BMI z; WC | ✓ NEG (boys Only) | 8 | |||
| Ekstedt et al (2013)63 | 1231; Sweden; CS | 6‐10 y | Accelerometry | BMI z | ✓ NEG | NS (%) | NS (BT; WT) | 4 | |
| El‐Sheikh et al (2007)64 | 167; USA; CS | 8‐9 y | Accelerometry | BMI z (CDC) | ✓ NEG | ✓ NEG (%) | 7 | ||
| El‐Sheikh et al (2014)21 | 269; USA; LT | 9(T1), 10(T2), 11(T3) | Accelerometry (duration); self‐report (sleep problems) | BMI (CDC) | ✓ NEG (CS and LT) | ✓ POS (sleep problems) | 6 | ||
| Fernandez‐Mendoza et al (2014)65 | 327; USA; CS | 5‐12 y | PSG (duration); Parent report (sleep problems) | BMI z (CDC); WC | ✓ NEG | NS | 6 | ||
| Ferrari et al (2017)66 | 328, Brazil, CS | 9‐o 11 | Self‐report | BMI (WHO) | NS | NS | 8 | ||
| Firouzi et al (2013)67 | 183; Malaysia; CS | 6‐12 y | Parent report | BMI z (WHO) | NS | NS (sleep onset) | ✓ NEG (sleep disorder score) | NS (BT; WT) | 5 |
| García‐Hermoso et al (2017)68 | 395; Chile; CS | 12‐13 | Self‐report | BMI z (IOTF) | ✓ NEG (girls only) | ✓ NEG (girls only) | 7 | ||
| Gentile et al (2014)69 | 1323; USA; LT (only reports CS) | 9 (±0.94) y | Self‐report | BMI | ✓ NEG (CS) | 6 | |||
| Giovaninni et al (2014)70 | 370; Brazil; CS | 6‐13 y | Parent report | BMI, waist and hip circumferences | ✓ NEG | 6 | |||
| Gomes et al (2014)71 | 686; Portugal; CS | 9‐11 y | Accelerometry | BMI z (IOTF) | NS | 9 | |||
| Harrex et al (2017)72 | 439, New Zealand, CS | 9‐11 | Accelerometry | BMI (WHO) | NS (SWP) | 7 | |||
| Hense et al (2011)73 | 4348 (subsample); Europe (Italy, Estonia, Cyprus, Belgium, Sweden, Hungary, Germany and Spain); CS | 6‐9 y (subsample) | Parent report | BMIz (IOTF) | ✓ NEG | 8 | |||
| Hiscock et al (2011)74 | 4464 (subsample); Australia; LT | 6‐7 y (from 4 to 5) | Parent report | BMI z (CDC/IOTF) | ✓ NEG (CS only) | NS | 7 | ||
| Hjorth et al (2014)75 | 785 CS; 708 LT; Denmark; LT | 8‐11 y | Accelerometry (duration); parent (quality) | BMI z (WHO) Fat Mas Index (DXA) | ✓ NEG (CS only) | NS | 7 | ||
| Ievers‐Landis et al (2008)76 | 819; USA; CS | 8‐11 y | Parent report | BMI (CDC) | ✓ NEG | 6 | |||
| Jiang et al (2014)77 | 1309; China; CS | 10‐12 | Parent report | BMI z; waist/height ratio; bf% (skin fold) | ✓ NEG (girls only) | 8 | |||
| Jing Jing et al (2017)78 | 894, Hong Kong, CS | 9‐12 | Self‐report | BMI | ✓ NEG | NS | 6 | ||
| Katzmarzyk et al (2015)79 | 6025, Australia, Brazil, Canada, China, Colombia, Finland, India, Kenya, Portugal, South Africa, United Kingdom, United States, CS | 9‐11 | Accelerometry | BMIz (WHO) | ✓ NEG | 7 | |||
| Kelly et al (2016)80 | 16 936, UK, LT | 11 (from 3 to 5 to 7) | Parent report | BMI | ✓ NEG (non‐regular BT) POS (BT > 9 pm; LT) | 6 | |||
| Khan et al (2015)82 | 5560, Canada, CS | 10‐11 | Parent report | BMI z (IOTF) | ✓ NEG | ✓ POS | 7 | ||
| Khan et al (2017)81 | 2261, Canada, CS | 10‐11 | Parent report | BMI z (IOTF) | ✓ NEG | ✓ NEG | 6 | ||
| Kim et al (2012)83 | 936; Korea; CS | 10‐11 y | Parent report | BMI z (2007 Korean National Growth Charts); | ✓ NEG | 7 | |||
| Kong et al (2011)84 | 779 (the primary school sample); Hong Kong; CS | 6‐14 y | Self‐report | BMI, WC | ✓ NEG | 8 | |||
| Kovács et al (2015)85 | 8848, Estonia, Sweden, Germany, Belgium, Hungary, Italy, Spain and Cypru, CS | 6‐9.9 | Parent report | BMI z (IOTF) | ✓ NEG | 6 | |||
| Krishnan et al (2017)86 | 643, New Zealand, CS | 6 | Accelerometry | BMI z (IOTF) | NS | 8 | |||
| Labree et al (2015)87 | 1943; Netherlands; CS | 8‐9 | Parent report | BMI z (IOTF) | ✓ NEG | 6 | |||
| Larsen et al (2017)88 | 206; Netherlands; CS | 7‐12 | Parent report | BMI z | ✓ NEG (boys only) | 4 | |||
| Laurson et al (2014)89 | 674; USA; CS | 7‐12 y | Self‐report | BMI z (CDC) | ✓ NEG (Boys Only) | 6 | |||
| Lee et al (2012)90 | 1504; South Korea; LT | 7‐11 y (baseline) | Self‐report | BMI z (2007 growth chart for Korean children) | ✓ NEG (LT only) | 6 | |||
| Lehto et al (2011)91 | 604; Finland; CS | 9‐11 y | self‐report | WC and waist to height ratio | ✓ NEG | 8 | |||
| Liu et al (2011)92 | 606; Canada; CS | 11‐13 y | Parent report | BMI z (IOTF) | ✓ NEG | ✓ POS (Awakenings) NS (sleep onset) | ✓ NEG (overall sleep problem score) | 7 | |
| Lu et al (2015)93 | 2457, China, CS | 7‐10 | Self‐report | BMI | NS | 3 | |||
| Lumeng et al (2007)94 | 785; USA; LT | 11.61 (±0.15) y (from 8 y) | Parent report | BMI z (National Center for Health Statistics norms) | ✓ NEG (CS and LT) | NS (night awakenings) | NS (CHSQ score; CS and LT) | ✓ POS (BT) NS (WT) | 8 |
| Magee et al (2013)95 | 1079; Australia; LT | 10‐11 y (from 4 to 5) | Parent report | BMI z (IOTF) — three trajectories (early onset, late onset, and healthy) | ✓ NEG (CS and LT) | 8 | |||
| Magee et al (2013)96 | 1833; Australia; CS | 8‐9 y (from 6 to 7) | Parent report | BMI z (IOTF) | NS | 6 | |||
| Magee et al (2014)8 | 2984; Australia; LT | 8‐9 y (from 4 to 5) | Parent report | BMI | ✓ NEG | 9 | |||
| Martinez et al (2014)98 | 229; U.S.A; LT | 10‐12 y (from 8 to 10) | Accelerometry | BMI z (CDC); waist‐to‐height ratio | ✓ NEG | 6 | |||
| Martinez et al (2014)97 | 303; U.S.A; CS | 8‐10 y | Accelerometer (actical) and parent report | BMI z (CDC) | ✓ NEG (both Ob and Sub) | 7 | |||
| Martoni et al (2016)99 | 115, Italy, CS | 10 | Accelerometry | BMI z (IOTF) | ✓ NEG | ✓ POS (mid‐point) | 5 | ||
| McNeil et al (2015)22 | 515; Canada; CS | 9‐11 y | Accelerometry | BMI z (IOTF); BF% (portable Tanita); WC | NS | ✓ NEG (%) | NS (BT; WT; MP) | 8 | |
| Meng et al (2012)100 | 6576; China; CS | 7‐11 y | Self‐report | BMI, WC, BF% | ✓ NEG | 8 | |||
| Miller (2011)101 | 11 400; USA; LT | 11.23 y (from 6.23) | Parent Report | BMI | ✓ NEG (CS only) | 6 | |||
| Morrissey et al (2016)102 | 298; Australia; CS | 9‐13 | Self‐report | BMI z (WHO) | ✓ NEG | 6 | |||
| Munakata et al (2010)103 | 216; Japan; CS | 9‐10 y | Self‐report | BMI; BF% (bioelectrical impedance) | ✓ NEG | 4 | |||
| Ochiai et al (2012)104 | 3433; Japan; CS | 9‐10 y | Parent report | BMI z (IOTF) | ✓ NEG (Boys Only) | NS (BT; WT) | 6 | ||
| O'Dea et al (2012)105 | 939; Australia; CS (longitudinal out of age group) | 7‐12 y | Self‐report | BMI z (IOTF) | ✓ NEG (CS) | 7 | |||
| Ortega Anta et al (2013)106 | 7659; Spain; CS | 6‐9 y | Parent report | BMI z (reference tables for Spanish children) | ✓ NEG | 6 | |||
| Padez et al (2009)107 | 4511; Portugal; CS | 7‐9 y | Parent report | BMI z (IOTF); BF% | ✓ NEG (only in boys when analyzed separately) | 7 | |||
| Peach et al (2015)108 | 1364; USA; CS | 11‐13 y | Self‐report | BMI | ✓ NEG (boys Only) | 7 | |||
| Pesonen et al (2009)109 | 289; USA; CS | 8(±0.3) y | Accelerometer (wrist) | BMI | NS (%) | 3 | |||
| Pileggi et al (2013)110 | 542; Italy; CS | 9.9(± 0.4) ys | Parent report | BMI z (SIEDP) | ✓ NEG | 8 | |||
| Prats‐Puig et al (2013)111 | 297; Spain; CS | 5‐9 y | Self‐report | BMI z; WC; visceral fat | ✓ NEG | 6 | |||
| Pryor et al (2015)112 | 1552, Canada, longitudinal | 6‐12 (from 2.5‐5) | Parent report | BMI z (IOTF) | ✓ NEG | 4 | |||
| Quach et al (2016)115 | 3631, Australia, LT | 8‐9 (followed from 4 to 5) | Parent report | BMI z (CDC) | ✓ POS (BT and timing cats) | 7 | |||
| Ramos and Barros (2007)116 | 2161; Portugal; CS | 13 y | Self‐report | BMI z (CDC/IOTF) | ✓ NEG (Boys Only) | 7 | |||
| Reilly et al (2005)117 | 7758; UK; LT | 7 y (from 2.5) | Self‐report | BMI z | ✓ NEG | 6 | |||
| Rosi et al (2017)118 | 690, Italy, CS | 9‐11 | Self‐report | BMI z (WHO) | ✓ NEG | NS | 3 | ||
| Rudnicka et al (2017)119 | 4525, UK, CS | 9‐10 | Self‐report | BMI; bioelectrical impedance | ✓ NEG | 6 | |||
| Santiago et al (2013)120 | 2814; Spain; CS | 6‐12 y | Self‐report | BMI | ✓ NEG (boys only) | 4 | |||
| Scharf and DeBoer (2015)121 | 7000; USA; CS and LT | 5 y (from 4) | Parent report | BMI z (CDC); BMI tradectories | ✓ NEG (LT only) | ✓ POS (BT) NEG (WT) | 4 | ||
| Sekine et al (2002)122 | 8274; Japan; CS | 6‐7 y | Parent report | BMI z (WHO) | ✓ NEG | ✓ POS (BT) NS (WT) | 8 | ||
| Shah et al (2013)123 | 200; India; CS | 10‐12 y | self‐report | BMI | NS | 4 | |||
| Silva et al (2011)124 | 304; USA; CS (longitudinal out of age group) | 6‐11 y | PSG (home) | BMI | NS | 7 | |||
| Stone et al (2013)125 | 856; Canada; CS | 10‐12 y | Parent report | BMI z | ✓ NEG | 4 | |||
| Sugimori et al (2004)126 | 8170; Japan; LT | 6 y (from 3) | Parent report | BMI | ✓ NEG (boys only) | ✓ NEG (BT: girls only) | 4 | ||
| Suglia et al (2013)127 | 1589; USA; CS | 5 y | Parent report | BMI z (CDC) | ✓ NEG | 3 | |||
| Sun et al (2009)128 | 5753; Japan; CS | 12‐13 y | Self‐report | BMI z | ✓ NEG (girls only) | NS (BT; WT) | 8 | ||
| Taveras et al (2014)129 | 1046; USA; LT | 7 yrs (from 1) | Parent report | BMI z, fat mass (DEXA); waist/hip ratio (at age 7) | ✓ NEG | 7 | |||
| Thasanasuwan et al (2016)130 | 1345, Malaysia, Indonesia, Vietnam, and Thailand, CS | 7‐12 | Self‐report | BMI z (WHO) | ✓ NEG | 6 | |||
| Thivel et al (2015)131 | 236; France; CS | 6‐10 y | Parent report | BMI z; Fat Mas% | ✓ POS (SMP) | 3 | |||
| Tovaret al (2012)132 | 401; USA; CS | 6‐11 y | Parent report | BMI z (CDC) | ✓ POS (OW NS OB) | 7 | |||
| Tuyet et al (2017)133 | 559, Vietnam, CS | 6‐11 | Parent report | BMI z (IOTF) | ✓ NEG | 4 | |||
| Von Kries et al (2002)134 | 6645; Germany; CS | 5‐6 y | Parent report | BMI z; Body fat mass (BIA) | ✓ NEG | 7 | |||
| Wang et al (2016)135 | 16 028; China; LT | 5 (from 3) | Parent report | BMI | ✓ NEG | 6 | |||
| Wang et al (2017)136 | 5518; China; CS | 9‐12 | Self‐report | BMI z (WHO); BF% | ✓ NEG | NS | ✓ POS (BT) | 9 | |
| Wells et al (2008)137 | 4452; Brazil; CS | 10‐12 y | Self‐report | BMI, Skinfolds | ✓ NEG | 9 | |||
| Wijnhoven et al (2015)138 | 15 643, Bulgaria, the Czech Republic, Lithuania, Portugal and Sweden, CS | 6‐9 | Parent report | BMI z (WHO) | ✓ NS (all) NEG (Sig Portugal and Sweden) | 7 | |||
| Williams et al (2013)139 | 1215; New Zealand; LT | 7 y (from 3) | Parent report | BMI z | ✓ NEG | 5 | |||
| Wong et al (2013)140 | 333; USA; CS | 9‐12 y | Accelerometry | BMI z | ✓ NEG | 7 | |||
| Zhang et al (2016)141 | 3766, China, CS | 7‐12 | Self‐report | BMI z (WGOC) | ✓ NEG | 6 | |||
Abbreviations: Key: ✓, significant association reported; BMI, body mass index; NEG, negative association report; POS, positive association report; NS, no significant association report; BT, bed time; WT, wake time; SWP, sleep wake pattern; SMP, sleep midpoint; CS, cross sectional; LT, longitudinal; %, sleep efficiency percentage; LWE, long wake episodes; IOTF, International Obesity Task Force 113; CDC, Centers for Disease Control 114; OW, overweight; OB, obese.
Expanded notes on findings can be found in Table S3.
The included studies examined sleep across four dimensions (duration, timing, efficiency, and quality). Sleep duration was the most frequent dimension analyzed, with all but nine of the 112 studies reviewed assessing sleep duration. Of these 103 studies: 73 reported solely on the association between children's sleep duration and their weight status, 22 assessed duration and one other dimension, and seven assessed at least another two. Of the nine articles not reporting sleep duration, six solely reported on sleep timing factors, two on sleep quality, and one on sleep efficiency.
3.1. Sleep duration
Overall, there was strong evidence in support of an inverse association between primary school‐aged children's sleep duration and measured weight status. Of the 103 articles reporting on sleep duration: 86 (83%) reported a significant negative association between duration of sleep and measured weight status, where shorter sleep durations were linked with poorer weight status measures. In contrast, one study132 reported overweight and obesity to be higher among longer sleepers (>10 hours/night); while another study indicated mixed results, where girls with short sleep displayed higher weight status and boys with short sleep displayed lower weight status measures.47 Only 15 articles (14%) found no significant association between children's sleep duration and measured weight status.
Comparing measurement methods, sleep duration was mostly assessed subjectively through a calculation from self/proxy report bed (or sleep onset) and wake times, or self/proxy report duration (ie, “How many hours does your child usually sleep per day?”) (n = 84); with limited use of objectively assessed time spent asleep as determined through polysomnography (PSG) or accelerometry scoring of activity (n = 19). However, results were relatively similar across measurement methods, with a similar proportion of articles reporting an inverse association between longer sleep duration and healthier weight status as assessed via subjectively reported sleep duration (71/84; 85%), compared with objectively measured duration (16/19; 84%).
The longitudinal relationship between children's sleep duration and weight status outcomes was investigated by 22 studies, of which a significant negative association between shorter sleep durations and poorer weight status outcomes over time was reported across all but three.74, 75, 101 These three studies did however report significant cross‐sectional associations. While Hiscock et al74 reported a significant association between short sleep and higher weight status among children aged 6‐7 years, cross sectionally, initial sleep at 4 years did not significantly predict later weight status at age seven. Miller 101 and Hjorth et al 75 reported similar results.
There was also some evidence for gender patterning: with nine of the 103 reviewed articles reporting on sleep duration indicating the association between sleep duration and Ow/Ob as significant among boys only 62, 88, 89, 104, 107, 108, 116, 120, 126; while three reported it as significant among girls only44, 77, 128; and one reported mixed results across genders, as mentioned above.47
3.2. Sleep timing
Out of 112 reviewed articles, there were only 24 articles that reported on an association between the timing of children's sleep and their weight status (Table 2). Assessed components of sleep timing across these studies included either the timing of going to bed (bed time = BT) (n = 19), the time of waking (wake time = WT) (n = 10), sleep midpoint (n = 3), or sleep‐wake cycles (n = 4). Fifteen out of the 24 found a significant association between a timing componentry of sleep and Ow/Ob among children.
Table 2.
Findings from sleep timing articles
| Article | Timing factor/s | Measure of timing | ||
|---|---|---|---|---|
| Bed time | Wake time | Other | ||
| Alqaderi et al (2017)34 | ✓ Pos (LT) | Self‐report | ||
| Amigo et al (2014)36 | ✓ Pos | Self‐report | ||
| Anderson et al (2017)37 | ✓ Neg (consistent bed‐time at age 3; compared with inconsistent) | Parent report | ||
| Berentzen et al (2014)44 | NS (sleep‐wake pattern) | Self‐report | ||
| Busto‐Zapico et al (2014)45 | ✓ Pos | Parent report | ||
| Cassimos et al (2011)51 | NS | Self‐report | ||
| Combs et al (2016)55 | ✓ Pos (weekday) | NS (weekday) | Parent report | |
| Ekstedt et al (2013)63 | NS | NS | Accelerometry | |
| Firouzi et al (2013)67 | NS | NS | Parent report | |
| Harrex et al (2017)72 | NS (sleep‐wake pattern) | Accelerometry | ||
| Kelly et al (2015)80 | ✓ NEG (nonregular BT) POS (BT > 9 pm; LT) | Parent report | ||
| Khan et al (2017)81 | ✓ Pos (weekday) | Parent report | ||
| Lumeng et al (2007)94 | ✓ Pos | NS | Parent report | |
| Martoni et al (2016)99 | ✓ Pos (sleep midpoint) | Accelerometry | ||
| McNeil et al (2015)22 | NS | NS | NS (Sleep midpoint) | Accelerometry |
| Ochiai et al (2012)104 | NS | NS | Parent report | |
| Quach et al (2016)115 | ✓ Pos (LT: as dichotomous categorization of LTB) | ✓ Pos (LT: wave 2 only) (sleep‐wake pattern) | Parent report | |
| Rosi et al (2017)118 | NS (sleep‐wake pattern) | Self‐reported | ||
| Scharf and DeBoer (2015)121 | ✓ Pos (CS and LT) | ✓ Neg (CS only) | Parent report | |
| Sekine et al (2002)122 | ✓ Pos | NS | Parent report | |
| Sugimori et al (2004)126 | ✓ Pos (Girls Only; LT) | NS | Parent report | |
| Sun et al (2009)128 | NS | NS | Self‐report | |
| Thivel et al (2015)131 | ✓ Pos (sleep midpoint) | Parent report | ||
| Wang et al (2017)136 | ✓ Pos | Self‐report | ||
Abbreviations: Key: ✓ = significant association reported; NS = no significant association with weight status; Pos = positive association (later BT OR WT ➔ higher weight status); Neg = negative association (earlier BT OR WT ➔ higher weight status); BT = Bed Time; WT = Wake Time; LTB = late to bed; CS = cross‐sectional association; LT = longitudinal association.
A trend was found supporting a positive association for the relationships between later bed‐timing/sleep onset and Ow/Ob among children. Of the 19 articles reporting on children's bedtime (BT), 12 indicate later bed‐times/sleep onset were linked with significantly poorer weight status (though one of these was significant among girls only; and two for weekday BT only). These findings were consistent across both self‐reported and parent‐reported BT, cross sectionally and longitudinally, with 10 of 12 studies with parent‐reported BT and three of five studies with self‐reported BT reporting significant links between later or inconsistent bed times and increased overweight/obesity. The remaining six out of the 19 articles (32%) reporting on BT and Ow/Ob among children, found no association between BT and children's weight status, two of which were the only studies with accelerometry determined BT.22, 63
Results were mostly consistent when assessing the impact of wake time (WT), regardless of being assessed from parent report, self‐report or measured via accelerometry. Of the total 112 reviewed articles, only 10 papers examined the association between WT and weight status among children, of which only one reported a significant association. Scharf and DeBoe121 reported that children aged five waking before 6:30 am were significantly more likely to be affected by obesity (OR = 1.23, 95%CI 1.01‐15.51, P < .05), although this association was not observed amongst their longitudinal sample comparing WT at 4 years of age and weight status at 5 years of age.
There was less examination across the other aspects of sleep timing including sleep midpoint (the half‐way point/time between sleep onset and wake time) and sleep‐wake patterns. Only three studies reported on sleep midpoint, of which two reported significant positive associations. Both Thivel et al131 and Martoni et al)99 indicated that measures of overweight and obesity were significantly higher among children who demonstrated a later sleep midpoint.
The final aspect of sleep assessed was sleep‐wake patterns, determined according to consideration of combined dichotomized categorization of BT and WT, creating the sleep timing labels of early to bed/early to rise; early to bed/late to rise; late to bed/early to rise; and late to bed/late to rise. Only one of the four studies assessing this factor found a significant association reporting higher BMI z‐scores among late to bed/early to rise profiles compared with early to bed/early to rise sleepers, although this was only significant among 6‐7 year olds and not 8‐9 year olds. 115
Of the total 112 reviewed studies and 24 timing studies, only four22, 63, 72, 99 measured sleep timing objectively via accelerometry. One of these assessed sleep‐wake timing,72 which supported the general nonsignificance consensus. Two of the studies22, 67 reported on the association between BT and WT with children's BMI z‐scores, both reporting nonsignificant results. While these findings were consistent with those from both parent reported and self‐reported WT, these contrasted the general consensus found for later self‐/parent‐reported BT and increased weight status among children.
McNeil et al22 also assessed sleeping midpoint, as did and Martoni et al .99 These studies had converse findings with Martoni reporting a significant positive association, which contrasted the nonsignificant findings reported by McNeil. However, the only other study reporting on sleep midpoint, findings from Thivel et al found a positive association between parent reported later sleep midpoints and higher percentage fat mas among children, further supporting the positive association.131
3.3. Sleep efficiency
Twelve studies examined an aspect sleep efficiency; analyzing either sleep latency (the efficiency of initiating sleep), maintaining sleep (wake episodes), or as a time percentage variable.
The percentage of time spent asleep, calculated as the time between sleep onset and waking, was assessed by seven of the 12 papers. These seven studies used accelerometry to objectively measure the efficiency, with four reporting a significant negative association between higher sleep efficiency scores and poorer anthropometric outcomes among children, while three found no significant association (Table 3).
Table 3.
Findings from sleep efficiency articles
| Article | Classification of efficiency measure | Measure method | |||
|---|---|---|---|---|---|
| Efficiency % | Sleep onset delay | Night awakenings | Measure | ||
| Arora and Taheri (2015)39 | NS | The percent of time between sleep onset and wake time spent asleep | Accelerometry (wrist) | ||
| Bagley and El‐Sheikh (2013)40 | ✓ Neg | The percent of time between sleep onset and wake time spent asleep | Accelerometry (wrist) | ||
| Bagley and El‐Sheikh (2014)20 | ✓ Neg | ✓ NS (sleep activity) Pos (long wake episodes) |
The percent of time between sleep onset and wake time spent asleep; long sleep wake episodes; sleep activity |
Accelerometry (wrist) | |
| Berentzen et al (2014)44 | NS | Frequency/length of night awakenings | Self‐report | ||
| Ekstedt et al (2013)63 | NS | The percent of time between sleep onset and wake time spent asleep | Accelerometry (wrist) | ||
| El‐Sheikh et al (2007)64 | ✓ Neg | The percent of time between sleep onset and wake time spent asleep | Accelerometry (wrist) | ||
| Fernandez‐Mendoza et al (2014)65 | ✓ (combined) NS | “has trouble falling asleep” or “wakes up often in the night” | Parent report | ||
| Firouzi et al (2013)67 | NS | Sleep onset delay | Parent report | ||
| Liu et al (2011)92 | NS | ✓ Pos | One item on trouble falling asleep; one item on waking up during night; One item restless at night | Parent report | |
| Lumeng et al (2007)94 | NS | Night waking problems | Parent report | ||
| McNeil et al (2015)22 | ✓ Neg | The percent of time between sleep onset and wake time spent asleep | Accelerometry (waist) | ||
| Pesonen et al (2009)109 | NS | Actual sleep time divided by the time in bed | Accelerometry (wrist) | ||
Abbreviations: Key: ✓ = significant association reported; NS = no significant association with weight status; Pos = positive association (higher % or high problems or high awakenings leads to higher weight status); Neg = negative association (lower % or low problems or low awakenings leads to higher weight status); CS = cross‐sectional analysis.
Two further aspects of sleep efficiency were identified across six of the 12 papers; sleep latency issues (delay/difficulty initiating sleep), and night awakenings (problems with or frequency/duration of wake episodes). Sleep initiation was assessed by two studies,67, 92 night awakenings by four,20, 44, 92, 94 and one paper combined the two factors as a single item.65 No significant association between sleep onset delays and children's weight status was reported (both parent reported). Only night awakenings were found to be a significant predictor across two studies. Liu et al reported significantly higher proportion of Ow/Ob children had issues with sleep maintenance, reporting more night awakening problems (parent reported) compared with normal weight children (P < .05),92 while Bagley and El‐Sheikh reported that the number of wake episodes (assessed via accelerometry) was only significant if these episodes were ≥ 5 minutes each.20
3.4. Sleep quality
Of all 112 studies reviewed, 13 analyzed the association between quality of sleep and children's weight status (Table 4). All 13 studies collected subjective measures of sleep quality, ranging from a single item question on whether sleep problems were present, to the sum of scores across 10‐33 items relating to multiple aspects of sleep quality. The measurement method across the studies was different for all 13 studies. While the Child Sleep Health Questionnaire was used in four studies, each used different adaptations or modified version. Results were mixed, with four of six studies with self‐reported sleep quality and three of seven studies with parent‐reported sleep quality reporting no significant association between children's anthropometric measurements and the reported quality of sleep. The remaining six studies indicate a negative association, where higher levels of reported sleep problems lead to higher risk of Ow/Ob.
Table 4.
Findings from sleep quality articles
| Article | Measure | Measure method | Association |
|---|---|---|---|
| Alamian et al (2016)33 | Infant sleep problems: score of multiple sleep measure, according to three classifications | Parent report | ✓ NEG (LT) |
| Berentzen et al (2014)44 | Difficulty getting up, feeling rested, daytime sleepiness | Self‐report | NS |
| El‐Sheikh et al (2014)21 | School Sleep Habits Survey (10 item sleep wake problem scale) | Self‐report | ✓ NEG (LT, girls only) |
| Ferrari et al (2017)66 |
The Diet and Lifestyle Questionnaire (how well slept) |
Self‐report | NS |
| Firouzi et al (2013)67 | CSHQ: parent report total sleep disorder score (34 items) | Parent report | ✓ NEG |
| García‐Hermoso et al (2017)68 | Sleep Self‐Report (SSR), Spanish version (19 items) | Self‐report | ✓ NEG (girls only) |
| Hiscock et al (2011)74 | Parent report: on sleep problem (single question‐none/mild); sleep problem (mod/severe) | Parent report | NS |
| Hjorth et al (2014)75 | CSHQ: parent report sleep disturbances (33 item) | Parent report | NS (CS and LT) |
| Jing Jing et al (2017)78 | Likert scale (very good, good, fair, poor, very poor) | Self‐reported | NS |
| Khan et al (2017)81 | Likert scale (child snores, if they ever wake up unrefreshed in the morning and if they were sleepy during the daytime), dichotomized into good vs poor | Parent report | ✓ NEG |
| Liu et al (2011)92 | Sleep Behavior Questionnaire: total sleep behavior score (11 items on sleep problems) | Parent report | ✓NEG |
| Lumeng et al (2007)94 | CSHQ: parent report sleep disturbances General sleep problem score (27 items) | Parent report | NS (CS and LT) |
| Wang et al (2017)136 | CSHQ: self‐report total sleep disorder score (21 items) | Self‐report | NS |
Abbreviations: CSHQ = Child Sleep Health Questionnaire; ✓ = significant association reported; NS = no significant association with weight status; NEG = negative association with weight status (better sleep quality reduces weight status); CS = cross‐sectional association; LT = longitudinal association.
Results also varied longitudinally, with two of the four studies assessing the impact of sleep quality on weight status over time reported results to be non‐significant. Hiscock et al74 and Lumeng et al94 found no significant association across their time points. Furthermore, out of the two studies indicating lower sleep quality to be associated with poorer weight status,21, 33 one found the association as significant among girls only.21 El‐Sheikh et al,21 found that those who reported higher sleep problems at T1 (9 years old) had higher BMI scores at T3 (11 years old), although this was only significant among girls.
4. DISCUSSION
This systematic review highlights a strong importance on assessing sleep as a behavioral factor associated with increased risk of Ow/Ob among primary school aged children across multiple studies set in multiple countries. Out of the 112 reviewed studies, 98 reported a significant association with a dimension of sleep and increased weight status. Supporting findings from previous reviews, the current review found 86 of 103 (83%) studies found a significant negative association between sleep duration and overweight and obesity among children aged between five to thirteen years old. As previously reported,9, 10, 11, 13, 14 this association has been demonstrated cross sectionally as well as longitudinally, using both subjectively and objectively measured duration of children's sleep.
Of particular interest to the current review, is the in‐depth investigation of the association between other dimensions of sleep (namely sleep efficiency, quality, and the timing of both bed and wake times) and Ow/Ob among primary school aged children. Beyond those of previous reviews, the current article highlights that outside the heavily researched influence of the duration of sleep, aspects of the outlined sleep dimensions potentially have significant and independent influence in the sleep‐obesity association.
Compared with sleep duration, we found less evidence of studies examining other dimensions of sleep, such as quality, efficiency and bed/wake times, in attempts to understand the sleep‐obesity relationship. Where studies exist, there is evidence of associations across these additional dimensions on the sleep‐obesity nexus, particularly supporting a positive association with later bed timing and increased weight status. Less consistent findings were found across studies exploring components of sleep efficiency and sleep quality; however, the variations in these findings appear to relate to the inconsistencies of outlined definitions and measurement tools utilized. From previous definitions, sleep efficiency relates to the ease and continuity of initiating and maintaining sleep, while quality surrounds either measurement of specific sleep wave or perceived satisfaction/perceived problems with sleep.15, 16 The term sleep quality appeared to be used as an interchangeable/overreaching term for many of these aspect of sleep, some which appear more relevant to sleep maintenance/efficiency. Each of the reviewed studies also utilized a unique variation to obtain perceived quality or an overall sleep quality score. The variation in measurement approach and definition of these dimensions creates difficulties in comparing results across the literature. However, despite these discrepancies, this review indicates the importance of considering the influence of different dimensions when examining the sleep‐obesity nexus.
This review identified several timing factors that can be measured, including bedtime, wake time, sleep midpoint, and sleep timing patterns. Across the reviewed articles bedtime appears to be more influential than wake time, with a much stronger evidence for the association of later bedtimes and increased weight status among school children,36, 45, 94, 121, 122 than that of later wake times.121 Considering the target population, this could mostly be due to the commonality of the daily school routine, acting as a regulator on morning wake times/schedules, and more individual variability on bedtime routines.142
One of the other two measures of sleep timing minimally outlined included sleep midpoint, which used as a single marker (the midpoint) to assess the timing of sleep, taking duration completely out of the equation. 22, 99, 131 The second measure was sleep wake cycles, almost a combined sleep timing/duration variable, categorising children as late to bed/wake early (shortest duration), early to bed/wake early or late to bed/wake late (mid duration), and early to bed/wake late (long duration).44, 72, 115, 118 While results from the reviewed studies potentially suggest a stronger importance of sleep midpoint than sleep‐wake patterns, it is still unclear how reliable/useful these measures of sleep timing are when analyzing the sleep‐obesity association, due to the limited number of studies with these measures of timing and the discrepancies across results. It could be hypothesized that compared with WT and sleep‐wake patterns, bedtime and sleep midpoint might be more significant factors in the sleep‐obesity nexus, independently from sleep duration,18, 45 due to potential night‐time behaviors associated with delayed sleep.
With limited articles reporting on the longitudinal association between sleep timing and children's weight status, the etiology of the association is hard to determine. However, one proposed mechanism suggests children with later bedtimes have higher TV viewing/screen time and poorer snacking/dietary habits.36, 45, 121, 131 Busto‐Zapico et al indicate children with later bedtimes are more likely to have a higher BMI, especially when they use the time that they should be sleeping engaged in sedentary leisure activities (watching TV, computer games, etc.),45 while Thivel et al found children with later sleep midpoint, compared with normal sleepers, had poorer eating habits measured by number of cumulated eating risk factors (eg, snacking and sweetened beverage consumption).131 It could be proposed that later sleep timing not only contribute to a disrupted energy balance directly through reduced restorative sleep (reduced duration due to consistent WT) but also by generating increased time available for these additional obesity risk factor behaviors. Further evidence is required to unpack these associations.
This review found contrasting evidence across both night awakenings and objectively measured efficiency percentage (percentage of time spent asleep during the period between sleep onset and waking).20, 22, 40, 64, 92 While most subjectively assessed awakenings were reported as non‐significant, Bagley and El‐Sheikh,20 the only study with objectively measured night awakenings (via accelerometry), reported that although the number of wake episodes alone was nonsignificant with BMI, however the number of long wake episodes (those longer than 5 minutes) was associated with a significant increase in BMI among children. Contrasting evidence was also reported among sleep quality studies, with significant associations of poorer sleep quality and increased obesity risk reported among less than half of those exploring self or parent determined sleep quality. There was a lack of consistency in measurement approach across all reviewed studies reporting on children's sleep quality and efficiency. While four of the sleep quality studies used the same tool (the Child Sleep Habits Questionnaire [CSHQ]), minor alterations and differing questionnaire items were included across these. The variation in measurement approach and definition of these dimensions could be impacting findings. There is also a risk of error associated with potential recall bias from self‐report among young children, or reporter bias through proxy report by parents.143 The use of measures such as PSG or accelerometry might provide more objective assessment of these dimensions and should be used where possible. However, self‐/proxy‐reported measures are practical and cost‐effective and are deemed more suitable in population‐based research.143, 144 Pragmatic considerations on research methodology therefore call for enhanced clarity around definitions along with development of further psychometrically tested measurement tools to examine these dimensions among the target population.
Despite the variations, understanding the impact of both sleep efficiency and quality of sleep on the sleep‐obesity association should be of interest of future research as some research has indicated this association could be independent from the duration of sleep.67, 145 Delayed sleep initiation and poor sleep maintenance not only potentially reduce overall sleep duration but can also, as with delayed sleep timing, present available time for snacking. As the length of wake episodes is reportedly more influential on weight status outcomes, rather than simply the number of episodes,20 it could be suggested that these periods provide opportunity for snacking. Higher caloric intake has been recorded among clinical samples of adults with sleep related eating disorders in America, where higher wake‐episode frequencies were associated with increased snacking after initial sleep onset and overall daily calorie consumption.146, 147 However, research on this mechanism is limited, particularly among children. Future research would benefit from exploring how time in wake episodes is spent and the impact this might have on the sleep‐obesity nexus.
Furthermore, factors such as reduced sleep duration, later timing and poor sleep maintenance could impact sleep quality, altering hormone levels due to disrupted structure and timing of specific sleep wave cycles.148 Optimal sleep quality usually involves around four cycles of sleep, through slow wave sleep to REM sleep, which is important for endocrine and metabolic regulation. Kim et al review how impeded sleep quality and disruptions to these sleep cycles has been linked with insulin insensitivity, dysregulation of appetite hormones (leptin and ghrelin), decreased melatonin and metabolic disruption among adults.148 Sleep curtailment studies among adults have shown altered hormones such as leptin could negatively impact weight status outcomes through altered hunger signals, resulting in higher caloric consumptions.149 Additionally, disruptions to melatonin have been associated with increased daytime sleepiness among clinical samples of adults and children,150, 151, 152 which has been shown to influence physical activity levels and increased obesity risk among samples of adults in America153, 154 and school‐aged children in Japan.155
In agreeance with a recent review that evaluated the association between sleep quality and obesity among children and young adults,145 more research is required to explore how these factors impact each other and the sleep‐obesity relationship, along with the need for clarity on defining and assessing these dimensions.
4.1. Implications of the study
This review highlights the importance of assessing and understanding the impact of the multiple dimensions of sleep when investigating the association between sleep and weight status among children. The results propose that children's bedtimes, quality of sleep, and sleep efficiency could be equally as influential on the sleep‐obesity association (among children) as the prolifically researched dimension of sleep duration. While the consensus of this association appears stronger for the duration of sleep, this review also highlighted the importance of bed times/sleep patterns in the sleep‐obesity nexus. Less congruent findings were found for sleep quality and efficiency measures; however, this could be due to the comparatively limited studies investigating these dimensions when assessing adequate/inadequate sleep among children. The inconsistencies of measurement methods and definitions across the literature also create some discrepancies in results. To better understand the role of these dimensions on the sleep‐obesity association, future research would benefit from clarity on definitions across the different dimensions along with the use of valid and reliable tools.
Furthermore, due to the scarce longitudinal data across the reviewed studies (outside of sleep duration), the etiology of the association is hard to determine. To better determine the causality on the association between children's weight status and the multiple sleep dimensions, changes in these variables need to be examined over time among population samples, as well as exploring the impact of potential covariates (ie, screen time, diet, and physical activity).
Whilst further research is needed, there is consensus in the literature around the importance of the timing of sleep and not only sleep duration on the sleep‐obesity nexus. Clinicians should therefore consider all dimensions of sleep but particularly children's sleep timing and duration in their practice.
4.2. Strength and Limitations
To the authors' knowledge, this is the first systematic review that has explored and compared several dimension of sleep in relation to the sleep‐obesity association among children. A strength of the current study was the large number of studies systematically reviewed in order to broadly cover several active dimensions in the sleep‐obesity association among children. However, while the inclusion criterion of objectively measured weight status may have created a limitation on the number of included studies (potentially limiting a greater representation of each of the sleep dimensions), this criterion minimized the risk of variability due to measurement of the outcome variable.
Furthermore, focusing on free‐living populations and the defined age group allowed for a clearer indication of the association on children, as opposed to adolescents, as sleep needs and behaviors can be affected/altered among some clinical populations and across age groups.
While the large spread of studies provides a greater exploration of the multiple dimensions in the sleep‐obesity association among children, it also creates some restrictions. The multiple measurement and definition discrepancies within the dimensions complicated and limited comparisons of results across studies and dimensions, hence why no meta‐analysis was conducted. This review was also limited in the capacity to compare findings across potentially linked/covariate factors (that might influence the sufficiency of sleep attained (across the dimensions) and influence the sleep‐obesity association. For example, one factor potentially relevant to the sleep‐obesity relationship not detailed in this review was the impact of tanner stage/maturation. This was due to the limited number of studies22, 50, 71, 90, 97, 98, 125, 137 reporting/controlling for this covariate making it impossible to include this in comparisons of papers.
5. CONCLUSIONS
Similar to previous reviews, this study found strong evidence for a negative association between sleep duration and overweight and obesity among primary school‐aged children. However, inconsistencies in both measurement method and definition of sleep quality, sleep efficiency, and sleep timing limited the conclusions that could be drawn for these dimensions. To better understand the role of these dimensions on the sleep‐obesity association, future research would benefit from clarity on definitions across the different dimensions along with the use of valid and reliable tools. Furthermore, a combined approach should be incorporated in future research, to investigate these dimensions simultaneously and longitudinally so that the potential influence of the multiple dimensions of sleep on children's weight status can be analyzed overtime and as sleep needs change.
CONFLICT OF INTEREST
The authors have no conflicts to disclose.
AUTHOR CONTRIBUTIONS
B.M. and C.S. were responsible for the literature review and data extraction. B.M. was responsible for the data analysis and drafting of paper. S.A., C.S., and E.T. provided critical review for the final manuscript.
Supporting information
Appendix Supporting Figures and Tables
ACKNOWLEDGMENT
Morrissey is supported by a Deakin University Postgraduate Research Scholarship. Allender is supported by funding from an Australian National Health and Medical Research Council (NHMRC)/Australian National Heart Foundation Career Development Fellowship (APP1045836). Morrissey, Allender and Strugnell are researchers within the NHMRC Centre for Research Excellence in Obesity Policy and Food Systems (APP1041020).
Morrissey B, Taveras E, Allender S, Strugnell C. Sleep and obesity among children: A systematic review of multiple sleep dimensions. Pediatric Obesity. 2020;15:e12619 10.1111/ijpo.12619
REFERENCES
- 1. Lytle LA, Murray DM, Laska MN, Pasch KE, Anderson SE, Farbakhsh K. Examining the longitudinal relationship between change in sleep and obesity risk in adolescents. Health Educ Behav. 2013;40(3):362‐370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Azadbakht L, Kelishadi R, Khodarahmi M, et al. The association of sleep duration and cardiometabolic risk factors in a national sample of children and adolescents: the CASPIAN III study. Nutrition (Burbank, Los Angeles County, Calif). 2013;29(9):1133‐1141. [DOI] [PubMed] [Google Scholar]
- 3. Guidolin M, Gradisar M. Is shortened sleep duration a risk factor for overweight and obesity during adolescence? A review of the empirical literature. Sleep Med. 2012;13(7):779‐786. [DOI] [PubMed] [Google Scholar]
- 4. Hitze B, Bosy‐Westphal A, Bielfeldt F, et al. Determinants and impact of sleep duration in children and adolescents: data of the Kiel Obesity Prevention Study. Eur J Clin Nutr. 2009;63(6):739‐746. [DOI] [PubMed] [Google Scholar]
- 5. Seegers V, Petit D, Falissard B, et al. Short sleep duration and body mass index: a prospective longitudinal study in preadolescence. Am J Epidemiol. 2011;173(6):621‐629. [DOI] [PubMed] [Google Scholar]
- 6. Shi Z, Taylor AW, Gill TK, Tuckerman J, Adams R, Martin J. Short sleep duration and obesity among Australian children. BMC Public Health. 2010;10:609‐609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Hart CN, Cairns A, Jelalian E. Sleep and obesity in children and adolescents. Pediatr Clin North Am. 2011;58(3):715‐733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Magee C, Caputi P, Iverson D. Lack of sleep could increase obesity in children and too much television could be partly to blame. Acta Paediatr. 2014;103(1):e27‐e31. [DOI] [PubMed] [Google Scholar]
- 9. Cappuccio FP, Taggart FM, Kandala N‐B, et al. Meta‐analysis of short sleep duration and obesity in children and adults. Sleep. 2008;31(5):619‐626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Chen X, Beydoun MA, Youfa W. Is sleep duration associated with childhood obesity? a systematic review and meta‐analysis. Obesity. 2008;16(2):265‐274. [DOI] [PubMed] [Google Scholar]
- 11. Fatima Y, Doi SAR, Mamun AA. Longitudinal impact of sleep on overweight and obesity in children and adolescents: a systematic review and bias‐adjusted meta‐analysis. Obesity Rev. 2015;16(2):137‐149. [DOI] [PubMed] [Google Scholar]
- 12. Liu J, Zhang A, Li L. Sleep duration and overweight/obesity in children: review and implications for pediatric nursing. J Spec Pediatr Nurs. 2012;17(3):193‐204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Magee L, Hale L. Longitudinal associations between sleep duration and subsequent weight gain: a systematic review. Sleep Med Rev. 2012;16(3):231‐241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Patel SR, Hu FB. Short sleep duration and weight gain: a systematic review. Obesity. 2008;16(3):643‐653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Buysse DJ. Sleep health: can we define it? does it matter? Sleep. 2014;37(1):9‐17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. National Sleep Health Foundation . Sleeptionary: definitions of common sleep terms. https://sleepfoundation.org/sleeptionary. Accessed 1st March 2017.
- 17. Kushida C. Encyclopedia of Sleep. Standford, USA: Academic Press; 2012. [Google Scholar]
- 18. Jarrin DC, McGrath JJ, Drake CL. Beyond sleep duration: distinct sleep dimensions are associated with obesity in children and adolescents. Int J Obes (Lond). 2013;37(4):552‐558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Golley RK, Maher CA, Matricciani L, Olds TS. Sleep duration or bedtime? Exploring the association between sleep timing behaviour, diet and BMI in children and adolescents. Int J Obes (Lond). 2013;37(4):546‐551. [DOI] [PubMed] [Google Scholar]
- 20. Bagley EJ, El‐Sheikh M. Relations between daytime pre‐ejection period reactivity and sleep in late childhood. J Sleep Res. 2014;23(3):335‐338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. El‐Sheikh M, Bagley EJ, Keiley MK, Erath SA. Growth in body mass index from childhood into adolescence: the role of sleep duration and quality. J Early Adolesc. 2014;34(8):1145‐1166. [Google Scholar]
- 22. McNeil J, Tremblay MS, Leduc G, et al. Objectively‐measured sleep and its association with adiposity and physical activity in a sample of Canadian children. J Sleep Res. 2014;22(2):131‐139. [DOI] [PubMed] [Google Scholar]
- 23. Liu X, Forbes EE, Ryan ND, Rofey D, Hannon TS, Dahl RE. Rapid eye movement sleep in relation to overweight in children and adolescents. Arch Gen Psychiatry. 2008;65(8):924‐932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Tiihonen P, Pääkkönen A, Mervaala E, Hukkanen T, Töyräs J. Design, construction and evaluation of an ambulatory device for screening of sleep apnea. Med Biol Eng Comput. 2009;47(1):59‐66. [DOI] [PubMed] [Google Scholar]
- 25. Narang I, Manlhiot C, Davies‐Shaw J, et al. Sleep disturbance and cardiovascular risk in adolescents. CMAJ. 2012;184(17):E913‐E920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Copley V, Ells L, Bray C, et al. Changes in the weight status of children between the first and final years of primary school: A longitudinal analysis of data from the National Child Measurement Programme in four local authorities in England between 2006/07 and 2014/15. London, UK: Public Health England; 2017. [Google Scholar]
- 27. Biddle SJH, Pearson N, Ross GM, Braithwaite R. Tracking of sedentary behaviours of young people: a systematic review. Prev Med. 2010;51(5):345‐351. [DOI] [PubMed] [Google Scholar]
- 28. Foster BA, Farragher J, Parker P, Sosa ET. Treatment interventions for early childhood obesity: a systematic review. Acad Pediatr. 2015;15(4):353‐361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Singh AS, Mulder C, Twisk JWR, Van Mechelen W, MJM C. Tracking of childhood overweight into adulthood: a systematic review of the literature. Obes Rev. 2008;9(5):474‐488. [DOI] [PubMed] [Google Scholar]
- 30. Wells G, Shea B, O'connell D, et al. The Newcastle‐Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta‐Analyses. Oxford: Ottawa Hospital Research Institute; 2014, 2015. [Google Scholar]
- 31. Herzog R, Álvarez‐Pasquin MJ, Díaz C, Del Barrio JL, Estrada JM, Gil Á. Are healthcare workers' intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health. 2013;13(1):154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Agras WS, Hammer LD, McNicholas F, Kraemer HC. Risk factors for childhood overweight: a prospective study from birth to 9.5 years. J Pediatr. 2004;145(1):20‐25. [DOI] [PubMed] [Google Scholar]
- 33. Alamian A, Wang L, Hall AM, Pitts M, Ikekwere J. Infant sleep problems and childhood overweight: effects of three definitions of sleep problems. Prev Med Rep. 2016;4:463‐468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Alqaderi H, Redline S, Tavares M, Goodson JM. Effect of late bedtime on salivary glucose and abdominal obesity in children. Sleep Biol Rhythms. 2017;15(3):227‐233. [Google Scholar]
- 35. Altenburg TM, Chinapaw MJM, van der Knaap ETW, Brug J, Manios Y, Singh AS. Longer Sleep ‐ Slimmer Kids: The ENERGY‐Project. PLoS One. 2013;8(3):1‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Amigo I, Pena E, Errasti JM, Busto R. Sedentary versus active leisure activities and their relationship with sleeping habits and body mass index in children of 9 and 10 years of age. J Health Psychol. 2014;21(7):1472‐1480. [DOI] [PubMed] [Google Scholar]
- 37. Anderson SE, Sacker A, Whitaker RC, Kelly Y. Self‐regulation and household routines at age three and obesity at age eleven: longitudinal analysis of the UK Millennium Cohort Study. Int J Obes (Lond). 2017;41(10):1459‐1466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Anujuo KO, Vrijkotte TG, Stronks K, Jean‐Louis G, Agyemang CO. Ethnic differences in sleep duration at 5 years, and its relationship with overweight and blood pressure. Eur J Public Health. 2016;26(6):1001‐1006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Arora T, Taheri S. Associations among late chronotype, body mass index and dietary behaviors in young adolescents. Int J Obes (Lond). 2015;39(1):39‐44. [DOI] [PubMed] [Google Scholar]
- 40. Bagley EJ, El‐Sheikh M. Familial risk moderates the association between sleep and zBMI in children. J Pediatr Psychol. 2013;38(7):775‐784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Barlett ND, Gentile DA, Barlett CP, Eisenmann JC, Walsh DA. Sleep as a mediator of screen time effects on US children's health outcomes: a prospective study. J Child Media. 2012;6(1):37‐50. [Google Scholar]
- 42. Bayer O, Rosario AS, Wabitsch M, von Kries R. Sleep duration and obesity in children: is the association dependent on age and choice of the outcome parameter? Sleep. 2009;32(9):1183‐1189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Bell JF, Zimmerman FJ. Shortened nighttime sleep duration in early life and subsequent childhood obesity. Arch Pediatr Adolesc Med. 2010;164(9):840‐845. [DOI] [PubMed] [Google Scholar]
- 44. Berentzen NE, Smit HA, Bekkers MBM, et al. Time in bed, sleep quality and associations with cardiometabolic markers in children: the prevention and incidence of asthma and mite allergy birth cohort study. J Sleep Res. 2014;23(1):3‐12. [DOI] [PubMed] [Google Scholar]
- 45. Busto‐Zapico R, Amigo‐Vazquez I, Pena‐Suarez E, Fernandez‐Rodriguez C. Relationships between sleeping habits, sedentary leisure activities and childhood overweight and obesity. Psychol Health Med. 2014;19(6):667‐672. [DOI] [PubMed] [Google Scholar]
- 46. Cameron AJ, van Stralen MM, Brug J, et al. Television in the bedroom and increased body weight: potential explanations for their relationship among European schoolchildren. Pediatr Obes. 2013;8(2):130‐141. [DOI] [PubMed] [Google Scholar]
- 47. Cao M, Zhu Y, He B, et al. Association between sleep duration and obesity is age‐ and gender‐dependent in Chinese urban children aged 6‐18 years: a cross‐sectional study. BMC Public Health. 2015;15:1029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Carrillo‐Larco RM, Bernabe‐Ortiz A, Miranda JJ. Short sleep duration and childhood obesity: cross‐sectional analysis in Peru and patterns in four developing countries. PLoS ONE. 2014;9(11):e112433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Carter PJ, Taylor BJ, Williams SM, Taylor RW. Longitudinal analysis of sleep in relation to BMI and body fat in children: the FLAME study. BMJ. 2011;342(7809):1‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Casazza K, Hanks LJ, Fernandez JR. Shorter sleep may be a risk factor for impaired bone mass accrual in childhood. J Clin Densitom. 2011;14(4):453‐457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Cassimos D, Sidiropoulos H, Batzios S, Balodima V, Christoforidis A. Sociodemographic and dietary risk factors for excess weight in a greek pediatric population living in Kavala, Northern Greece. Nutr Clin Pract. 2011;26(2):186‐191. [DOI] [PubMed] [Google Scholar]
- 52. Chahal H, Fung C, Kuhle S, Veugelers PJ. Availability and night‐time use of electronic entertainment and communication devices are associated with short sleep duration and obesity among Canadian children. Pediatr Obes. 2013;8(1):42‐51. [DOI] [PubMed] [Google Scholar]
- 53. Chaput JP, Brunet M, Tremblay A. Relationship between short sleeping hours and childhood overweight/obesity: Results from the ‘Quebec en Forme’ project. Int J Obes (Lond). 2006;30(7):1080‐1085. [DOI] [PubMed] [Google Scholar]
- 54. Colley RC, Wong SL, Garriguet D, Janssen I, Connor Gorber S, Tremblay MS. Physical activity, sedentary behaviour and sleep in Canadian children: parent‐report versus direct measures and relative associations with health risk. Health Rep. 2012;23(2):45‐52. [PubMed] [Google Scholar]
- 55. Combs D, Goodwin JL, Quan SF, Morgan WJ, Parthasarathy S. Longitudinal differences in sleep duration in Hispanic and Caucasian children. Sleep Med. 2016;18:61‐66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. de Jong E, Stocks T, Visscher TLS, HiraSing RA, Seidell JC, Renders CM. Association between sleep duration and overweight: the importance of parenting. Int J Obes (Lond). 2012;36(10):1278‐1284. [DOI] [PubMed] [Google Scholar]
- 57. Del Pozo‐Cruz B, Gant N, Del Pozo‐Cruz J, Maddison R. Relationships between sleep duration, physical activity and body mass index in young New Zealanders: an isotemporal substitution analysis. PLoS One. 2017;12(9):e0184472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Diethelm K, Bolzenius K, Cheng G, Remer T, Buyken AE. Longitudinal associations between reported sleep duration in early childhood and the development of body mass index, fat mass index and fat free mass index until age 7. Int J Pediatr Obes. 2011;6(2–2):e114‐e123. [DOI] [PubMed] [Google Scholar]
- 59. Drescher AA, Goodwin JL, Silva GE, Quan SF. Caffeine and screen time in adolescence: associations with short sleep and obesity. J Clin Sleep Med. 2011;7(4):337‐342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Duncan JS, Schofield G, Duncan EK, Rush EC. Risk factors for excess body fatness in New Zealand children. Asia Pac J Clin Nutr. 2008;17(1):138‐147. [PubMed] [Google Scholar]
- 61. Duran Aguero S, Haro RP. Association between the amount of sleep and obesity in Chilean schoolchildren. Arch Argent Pediatr. 2016;114(2):114‐119. [DOI] [PubMed] [Google Scholar]
- 62. Eisenmann JC, Ekkekakis P, Holmes M. Sleep duration and overweight among Australian children and adolescents. Acta Paediatr (Oslo, Norway: 1992). 2006;95(8):956‐963. [DOI] [PubMed] [Google Scholar]
- 63. Ekstedt M, Nyberg G, Ingre M, Ekblom Ö, Marcus C. Sleep, physical activity and BMI in six to ten‐year‐ old children measured by accelerometry: a cross‐sectional study. Int J Behav Nutr Phys Act. 2013;10:82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. El‐Sheikh M, Erath SA, Keller PS. Children's sleep and adjustment: the moderating role of vagal regulation. J Sleep Res. 2007;16(4):396‐405. [DOI] [PubMed] [Google Scholar]
- 65. Fernandez‐Mendoza J, Vgontzas AN, Calhoun SL, et al. Insomnia symptoms, objective sleep duration and hypothalamic‐pituitary‐adrenal activity in children. Eur J Clin Invest. 2014;44(5):493‐500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Ferrari GLDM, Matsudo V, Katzmarzyk PT, Fisberg M. Prevalence and factors associated with body mass index in children aged 9–11 years. J Pediatr (Rio J). 2017;93(6):601‐609. [DOI] [PubMed] [Google Scholar]
- 67. Firouzi S, Koon PB, Noor MI, Sadeghilar A. Sleep pattern and sleep disorders among a sample of Malaysian children. Sleep Biol Rhythms. 2013;11(3):185‐193. [Google Scholar]
- 68. García‐Hermoso A, Aguilar MM, Vergara FA, Velásquez EJA, Marina R. Obesity, cardiorespiratory fitness, and self‐reported sleep patterns in Chilean school‐aged children. Behav Sleep Med. 2017;15(1):70‐80. [DOI] [PubMed] [Google Scholar]
- 69. Gentile DA, Reimer RA, Nathanson AI, Walsh DA, Eisenmann JC. Protective effects of parental monitoring of children's media use a prospective study. JAMA Pediatr. 2014;168(5):479‐484. [DOI] [PubMed] [Google Scholar]
- 70. Giovaninni NP, Fuly JT, Moraes LI, et al. Study of the association between 3111T/C polymorphism of the CLOCK gene and the presence of overweight in schoolchildren. J Pediatr (Rio J). 2014;90(5):500‐505. [DOI] [PubMed] [Google Scholar]
- 71. Gomes TN, Katzmarzyk PT, dos Santos FK, Souza M, Pereira S, Maia JAR. Overweight and obesity in Portuguese children: prevalence and correlates. Int J Environ Res Public Health. 2014;11(11):11398‐11417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Harrex HAL, Skeaff SA, Black KE, et al. Sleep timing is associated with diet and physical activity levels in 9–11‐year‐old children from dunedin, new zealand: the pedals study. J Sleep Res. 2017:1‐10. [DOI] [PubMed] [Google Scholar]
- 73. Hense S, Pohlabeln H, De Henauw S, et al. Sleep duration and overweight in European children: is the association modified by geographic region? Sleep. 2011;34(7):885‐890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Hiscock H, Scalzo K, Canterford L, Wake M. Sleep duration and body mass index in 0‐7‐year olds. Arch Dis Child. 2011;96(8):735‐739. [DOI] [PubMed] [Google Scholar]
- 75. Hjorth MF, Chaput JP, Ritz C, et al. Fatness predicts decreased physical activity and increased sedentary time, but not vice versa: support from a longitudinal study in 8‐ to 11‐year‐old children. Int J Obes (Lond). 2014;38(7):959‐965. [DOI] [PubMed] [Google Scholar]
- 76. Ievers‐Landis CE, Storfer‐Isser A, Rosen C, Johnson NL, Redline S. Relationship of sleep parameters, child psychological functioning, and parenting stress to obesity status among preadolescent children. J Dev Behav Pediatr. 2008;29(4):243‐252. [DOI] [PubMed] [Google Scholar]
- 77. Jiang YR, Spruyt K, Chen WJ, et al. Associations between parent‐reported sleep duration and adiposity in Chinese early adolescents. J Public Health (Oxford, England). 2014;37(2):277‐285. [DOI] [PubMed] [Google Scholar]
- 78. Jing Jing W, Yang G, Lau PWC. Prevalence of overweight in Hong Kong Chinese children: its associations with family, early‐life development and behaviors‐related factors. J Exerc Sci Fit. 2017;15(2):89‐95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Katzmarzyk PT, Barreira TV, Broyles ST, et al. Relationship between lifestyle behaviors and obesity in children ages 9–11: results from a 12‐country study. Obesity. 2015;23(8):1696‐1702. [DOI] [PubMed] [Google Scholar]
- 80. Kelly Y, Patalay P, Montgomery S, Sacker A. BMI Development and Early Adolescent Psychosocial Well‐Being: UK Millennium Cohort Study. Pediatrics. 2016;138(6):84‐84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Khan MKA, Faught EL, Chu YL, Ekwaru JP, Storey KE, Veugelers PJ. Is it nutrients, food items, diet quality or eating behaviours that are responsible for the association of children's diet with sleep? J Sleep Res. 2017;26(4):468‐476. [DOI] [PubMed] [Google Scholar]
- 82. Khan MKA, Yen Li C, Kirk SFL, Veugelers PJ, Chu YL. Are sleep duration and sleep quality associated with diet quality, physical activity, and body weight status? A population‐based study of Canadian children. Can J Public Health. 2015;106(5):e277‐e282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Kim C‐W, Choi M‐K, Im H‐J, et al. Weekend catch‐up sleep is associated with decreased risk of being overweight among fifth‐grade students with short sleep duration. J Sleep Res. 2012;21(5):546‐551. [DOI] [PubMed] [Google Scholar]
- 84. Kong AP, Wing Y‐K, Choi KC, et al. Associations of sleep duration with obesity and serum lipid profile in children and adolescents. Sleep Med. 2011;12(7):659‐665. [DOI] [PubMed] [Google Scholar]
- 85. Kovács E, Hunsberger M, Reisch L, et al. Adherence to combined lifestyle factors and their contribution to obesity in the IDEFICS study. Obes Rev. 2015;16:138‐150. [DOI] [PubMed] [Google Scholar]
- 86. Krishnan M, Shelling AN, McCowan LME, et al. Gene‐by‐environment interactions of the CLOCK, PEMT, and GHRELIN loci with average sleep duration in relation to obesity traits using a cohort of 643 New Zealand European children. Sleep Med. 2017;37:19‐26. [DOI] [PubMed] [Google Scholar]
- 87. Labree W, van de Mheen D, Rutten F, Rodenburg G, Koopmans G, Foets M. Differences in overweight and obesity among children from migrant and native origin: the role of physical activity, dietary intake, and sleep duration. PLoS One. 2015;10(6):e0123672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Larsen JK, Sleddens EFC, Vink JM, van den Broek N, Kremers SPJ. The sex‐specific interaction between food responsiveness and sleep duration explaining body mass index among children. Sleep Med. 2017;40:106‐109. [DOI] [PubMed] [Google Scholar]
- 89. Laurson KR, Lee JA, Gentile DA, Walsh DA, Eisenmann JC. Concurrent associations between physical activity, screen time, and sleep duration with childhood obesity. ISRN Obes. 2014;2014:204540‐204540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Lee HH, Park HA, Kang JH, et al. Factors related to body mass index and body mass index change in korean children: preliminary results from the obesity and metabolic disorders cohort in childhood. Korean J Fam Med. 2012;33(3):134‐143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Lehto R, Ray C, Lahti‐Koski M, Roos E. Health behaviors, waist circumference and waist‐to‐height ratio in children. Eur J Clin Nutr. 2011;65(7):841‐848. [DOI] [PubMed] [Google Scholar]
- 92. Liu J, Hay J, Joshi D, Faught BE, Wade T, Cairney J. Sleep difficulties and obesity among preadolescents. Can J Public Health. 2011;102(2):139‐143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Lu JK, Yin XJ, Xiong JP, Liu JJ, Watanabe T, Tanaka T. Comparison of the status of overweight/obesity among the youth of local Shanghai, young rural‐to‐urban migrants and immigrant origin areas. Int J Clin Exp Med. 2015;8(2):2804‐2814. [PMC free article] [PubMed] [Google Scholar]
- 94. Lumeng JC, Somashekar D, Appugliese D, Kaciroti N, Corwyn RF, Bradley RH. Shorter sleep duration is associated with increased risk for being overweight at ages 9 to 12 years. Pediatrics. 2007;120(5):1020‐1029. [DOI] [PubMed] [Google Scholar]
- 95. Magee CA, Caputi P, Iverson DC. The longitudinal relationship between sleep duration and body mass index in children: a growth mixture modeling approach. J Dev Behav Pediatr. 2013;34(3):165‐173. [DOI] [PubMed] [Google Scholar]
- 96. Magee CA, Caputi P, Iverson DC. Patterns of health behaviours predict obesity in Australian children. J Paediatr Child Health. 2013;49(4):291‐296. [DOI] [PubMed] [Google Scholar]
- 97. Martinez SM, Greenspan LC, Butte NF, et al. Mother‐reported sleep, accelerometer‐estimated sleep and weight status in Mexican American children: sleep duration is associated with increased adiposity and risk for overweight/obese status. J Sleep Res. 2014;23(3):326‐334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Martinez SM, Tschann JM, Greenspan LC, et al. Is it time for bed? Short sleep duration increases risk of obesity in Mexican American children. Sleep Med. 2014;15(12):1484‐1489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Martoni M, Carissimi A, Fabbri M, Filardi M, Tonetti L, Natale V. 24‐h actigraphic monitoring of motor activity, sleeping and eating behaviors in underweight, normal weight, overweight and obese children. Eat Weight Disord. 2016;21(4):669‐677. [DOI] [PubMed] [Google Scholar]
- 100. Meng LP, Liu AL, Hu X, et al. Report on childhood obesity in China (10): association of sleep duration with obesity. Biomed Environ Sci: BES. 2012;25(2):133‐140. [DOI] [PubMed] [Google Scholar]
- 101. Miller DP. Associations between the home and school environments and child body mass index. Soc Sci Med. 2011;72(5):677‐684. [DOI] [PubMed] [Google Scholar]
- 102. Morrissey B, Malakellis M, Whelan J, et al. Sleep duration and risk of obesity among a sample of Victorian school children. BMC Public Health. 2016;16(1):1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103. Munakata H, Sei M, Ewis AA, et al. Prediction of Japanese children at risk for complications of childhood obesity: gender differences for intervention approaches. J Med Invest. 2010;57(1–2):62‐68. [DOI] [PubMed] [Google Scholar]
- 104. Ochiai H, Shirasawa T, Shimada N, et al. Sleep duration and overweight among elementary schoolchildren: a population‐based study in Japan. Acta Med Okayama. 2012;66(2):93‐99. [DOI] [PubMed] [Google Scholar]
- 105. O'Dea JA, Dibley MJ, Rankin NM. Low sleep and low socioeconomic status predict high body mass index: a 4‐year longitudinal study of Australian schoolchildren. Pediatr Obes. 2012;7(4):295‐303. [DOI] [PubMed] [Google Scholar]
- 106. Ortega Anta RM, López‐Solaber AM, Pérez‐Farinós N. Associated factors of obesity in Spanish representative samples. Nutr Hosp. 2013;28(Suppl 5):56‐62. [DOI] [PubMed] [Google Scholar]
- 107. Padez C, Mourao I, Moreira P, Rosado V. Long sleep duration and childhood overweight/obesity and body fat. Am J Hum Biol. 2009;21(3):371‐376. [DOI] [PubMed] [Google Scholar]
- 108. Peach H, Gaultney JF, Reeve CL. Sleep characteristics, body mass index, and risk for hypertension in young adolescents. J Youth Adolesc. 2015;44(2):271‐284. [DOI] [PubMed] [Google Scholar]
- 109. Pesonen A‐K, Räikkönen K, Matthews K, et al. Prenatal origins of poor sleep in children. Sleep. 2009;32(8):1086‐1092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110. Pileggi C, Lotito F, Bianco A, Nobile CG, Pavia M. Relationship between chronic short sleep duration and childhood body mass index: a school‐based cross‐sectional study. PLoS One. 2013;8(6):e66680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Prats‐Puig A, Grau‐Cabrera P, Riera‐Pérez E, et al. Variations in the obesity genes FTO, TMEM18 and NRXN3 influence the vulnerability of children to weight gain induced by short sleep duration. Int J Obes. 2013;37(2):182‐187. [DOI] [PubMed] [Google Scholar]
- 112. Pryor LE, Brendgen M, Tremblay RE, et al. Early risk factors of overweight developmental trajectories during middle childhood. PLoS ONE. 2015;10(6):1‐17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320(7244):1240‐1243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114. Ogden CL, Kuczmarski RJ, Flegal KM, et al. Centers for Disease Control and Prevention 2000 Growth Charts for the United States: improvements to the 1977 National Center for Health Statistics Version. Pediatrics. 2002;109(1):45‐60. [DOI] [PubMed] [Google Scholar]
- 115. Quach J, Price AMH, Bittman M, Hiscock H. Sleep timing and child and parent outcomes in Australian 4–9‐year‐olds: a cross‐sectional and longitudinal study. Sleep Med. 2016;22:39‐46. [DOI] [PubMed] [Google Scholar]
- 116. Ramos E, Barros H. Family and school determinants of overweight in 13‐year‐old Portuguese adolescents. Acta Paediatr. 2007;96(2):281‐286. [DOI] [PubMed] [Google Scholar]
- 117. Reilly JJ, Armstrong J, Dorosty AR, et al. Early life risk factors for obesity in childhood: Cohort study. BMJ. 2005;330(7504):1357‐1357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Rosi A, Calestani MV, Parrino L, et al. Weight status is related with gender and sleep duration but not with dietary habits and physical activity in primary school Italian children. Nutrients. 2017;9(6):1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119. Rudnicka AR, Nightingale CM, Donin AS, et al. Sleep Duration and Risk of Type 2 Diabetes. Pediatrics. 2017;140(3):1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120. Santiago S, Zazpe I, Martí A, Cuervo M, Martínez JA. Gender differences in lifestyle determinants of overweight prevalence in a sample of Southern European children. Obes Res Clin Pract. 2013;7(5):e391‐e400. [DOI] [PubMed] [Google Scholar]
- 121. Scharf RJ, DeBoer MD. Sleep timing and longitudinal weight gain in 4‐ and 5‐year‐old children. Pediatr Obes. 2015;10(2):141‐148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Sekine M, Yamagami T, Handa K, et al. A dose‐response relationship between short sleeping hours and childhood obesity: results of the Toyama birth cohort study. Child Care Health Dev. 2002;28(2):163‐170. [DOI] [PubMed] [Google Scholar]
- 123. Shah JS, Patel PK, Patel B. Determinants of overweight and obesity among school children in Mehsana District, India. Ann Trop Med Public Health. 2013;6(4):408‐412. [Google Scholar]
- 124. Silva GE, Goodwin JL, Parthasarathy S, et al. Longitudinal association between short sleep, body weight, and emotional and learning problems in Hispanic and Caucasian children. Sleep. 2011;34(9):1197‐1205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. Stone MR, Stevens D, Faulkner GEJ. Maintaining recommended sleep throughout the week is associated with increased physical activity in children. Prev Med. 2013;56(2):112‐117. [DOI] [PubMed] [Google Scholar]
- 126. Sugimori H, Yoshida K, Izuno T, et al. Analysis of factors that influence body mass index from ages 3 to 6 years: a study based on the Toyama cohort study. Pediatr Int. 2004;46(3):302‐310. [DOI] [PubMed] [Google Scholar]
- 127. Suglia SF, Duarte CS, Chambers EC, Boynton‐Jarrett R. Social and behavioral risk factors for obesity in early childhood. J Dev Behav Pediatr. 2013;34(8):549‐556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128. Sun Y, Sekine M, Kagamimori S. Lifestyle and overweight among Japanese adolescents: the Toyama Birth Cohort Study. J Epidemiol. 2009;19(6):303‐310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Taveras EM, Gillman MW, Peña M‐M, Redline S, Rifas‐Shiman SL. Chronic sleep curtailment and adiposity. Pediatrics. 2014;133(6):1013‐1022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Thasanasuwan W, Srichan W, Kijboonchoo K, et al. Low sleeping time, high TV viewing time, and physical inactivity in school are risk factors for obesity in pre‐adolescent Thai children. J Med Assoc Thai. 2016;99(3):314‐321. [PubMed] [Google Scholar]
- 131. Thivel D, Isacco L, Aucouturier J, et al. Bedtime and sleep timing but not sleep duration are associated with eating habits in primary school children. J Dev Behav Pediatr. 2015;36(3):158‐165. [DOI] [PubMed] [Google Scholar]
- 132. Tovar A, Chui K, Hyatt RR, et al. Healthy‐lifestyle behaviors associated with overweight and obesity in US rural children. BMC Pediatr. 2012;12:1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Tuyet LT, Nhung BT, Dao DTA, et al. The brain‐derived neurotrophic factor Val66Met polymorphism, delivery method, birth weight, and night sleep duration as determinants of obesity in vietnamese children of primary school age. Child Obes. 2017;13(5):392‐399. [DOI] [PubMed] [Google Scholar]
- 134. Von Kries R, Toschke AM, Wurmser H, Sauerwald T, Koletzko B. Reduced risk for overweight and obesity in 5‐ and 6‐y‐old children by duration of sleep ‐ a cross‐sectional study. Int J Obes (Lond). 2002;26(5):710‐716. [DOI] [PubMed] [Google Scholar]
- 135. Wang F, Liu H, Wan Y, et al. Sleep duration and overweight/obesity in preschool‐aged children: a prospective study of up to 48,922 children of the Jiaxing Birth Cohort. Sleep. 2016;39(11):2013‐2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136. Wang J, Adab P, Liu W, et al. Prevalence of adiposity and its association with sleep duration, quality, and timing among 9‐12‐year‐old children in Guangzhou, China. J Epidemiol. 2017;27(11):531‐537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137. Wells JCK, Hallal PC, Reichert FF, Menezes AMB, Araújo CLP, Victora CG. Sleep patterns and television viewing in relation to obesity and blood pressure: evidence from an adolescent Brazilian birth cohort. Int J Obes (Lond). 2008;32(7):1042‐1049. [DOI] [PubMed] [Google Scholar]
- 138. Wijnhoven TM, van Raaij JM, Yngve A, et al. WHO European Childhood Obesity Surveillance Initiative: health‐risk behaviours on nutrition and physical activity in 6‐9‐year‐old schoolchildren. Public Health Nutr. 2015;18(17):3108‐3124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139. Williams SM, Taylor RW, Taylor BJ. Secular changes in BMI and the associations between risk factors and BMI in children born 29 years apart. Pediatr Obes. 2013;8(1):21‐30. [DOI] [PubMed] [Google Scholar]
- 140. Wong WW, Ortiz CL, Lathan D, et al. Sleep duration of underserved minority children in a cross‐sectional study. BMC Public Health. 2013;13:648‐648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141. Zhang T, Cai L, Ma L, Jing J, Chen Y, Ma J. The prevalence of obesity and influence of early life and behavioral factors on obesity in Chinese children in Guangzhou. BMC Public Health. 2016;16:954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142. Boergers J, Gable CJ, Owens JA. Later school start time is associated with improved sleep and daytime functioning in adolescents. J Dev Behav Pediatr. 2014;35(1):11‐17. [DOI] [PubMed] [Google Scholar]
- 143. Erwin AM, Bashore L. Subjective sleep measures in children: self‐report. Front Pediatr. 2017;5:22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144. Johnson TP. Handbook of Health Survey Methods. Chicago, USA: Wiley; 2014. [Google Scholar]
- 145. Fatima Y, Mamun A. Sleep quality and obesity in young subjects: a meta‐analysis. Obes Rev. 2016;17(11):1154‐1166. [DOI] [PubMed] [Google Scholar]
- 146. Birketvedt GS, Florholmen J, Sundsfjord J, et al. Behavioral and neuroendocrine characteristics of the night‐eating syndrome. JAMA. 1999;282(7):657‐663. [DOI] [PubMed] [Google Scholar]
- 147. Gluck ME, Venti CA, Salbe AD, Krakoff J. Nighttime eating: commonly observed and related to weight gain in an inpatient food intake study. Am J Clin Nutr. 2008;88(4):900‐905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148. Kim TW, Jeong J‐H, Hong S‐C. The impact of sleep and circadian disturbance on hormones and metabolism. Int J Endocrinol. 2015;2015:1‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149. Spiegel K, Tasali E, Penev P, Van Cauter E. Brief communication: sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann Intern Med. 2004;141(11):846‐850. [DOI] [PubMed] [Google Scholar]
- 150. Müller HL. Increased daytime sleepiness in patients with childhood craniopharyngioma and hypothalamic tumor involvement: review of the literature and perspectives. Int J Endocrinol. 2010;2010:519607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. Muller HL, Handwerker G, Wollny B, Faldum A, Sorensen N. Melatonin secretion and increased daytime sleepiness in childhood craniopharyngioma patients. J Clin Endocrinol Metabol. 2002;87(8):3993‐3996. [DOI] [PubMed] [Google Scholar]
- 152. Pickering L, Jennum P, Gammeltoft S, Poulsgaard L, Feldt‐Rasmussen U, Klose M. Sleep‐wake and melatonin pattern in craniopharyngioma patients. Eur J Endocrinol. 2014;170(6):873‐884. [DOI] [PubMed] [Google Scholar]
- 153. Chasens ER, Sereika SM, Weaver TE, Umlauf MG. Daytime sleepiness, exercise, and physical function in older adults. J Sleep Res. 2007;16(1):60‐65. [DOI] [PubMed] [Google Scholar]
- 154. McClain JJ, Lewin DS, Laposky AD, Kahle L, Berrigan D. Associations between physical activity, sedentary time, sleep duration and daytime sleepiness in US adults. Prev Med. 2014;66:68‐73. [DOI] [PubMed] [Google Scholar]
- 155. Gaina A, Sekine M, Hamanishi S, et al. Daytime sleepiness and associated factors in Japanese School Children. J Pediatr. 2007;151(5):518‐522. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix Supporting Figures and Tables