

One use of cytology is to classify lesions so as to assist with the diagnosis, prognosis, and management of a case. Cytologic interpretations are generally classified into one of five cytodiagnostic groups (Box 2-1 ). A sixth category can be used for nondiagnostic or artifact interpretations. Nondiagnostic samples usually result from insufficient cellular material or excessive blood contamination.
KEY POINT Interpretation of cytologic material may include more than one category, such as inflammation along with a response to tissue injury or neoplasia with inflammation.
Box 2-1. General Categories of Cytodiagnostic Interpretation.
Normal or hyperplastic tissue
Cystic mass
Inflammation or cellular infiltrate
Response to tissue injury
Neoplasia
Nondiagnostic sample
Normal Tissue
Normal tissue is generally composed primarily of mature cell types, although some organs such as integumentary normally contain immature basal epithelium. Normal cells display uniformity in cellular, nuclear, and nucleolar size and shape. Cytoplasmic volume is usually high relative to the nucleus (Figure 2-1, Figure 2-2 ).
Figure 2-1.
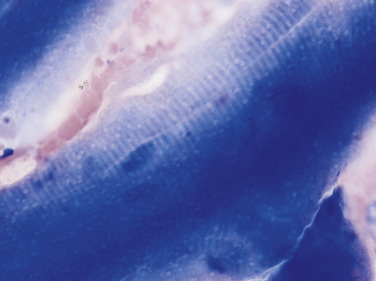
Normal skeletal muscle. Tissue aspirate. Dog.
Numerous threadlike myofibrils compose each cell with small, condensed, and oval nucleus. Cross-striations, characteristic of skeletal muscle, are visible against the dark blue cytoplasm. (Modified Wright; HP oil.)
Figure 2-2.

Normal salivary gland. Tissue aspirate. Dog.
The gland has uniform features of nuclear size, nuclear-to-cytoplasmic ratio, and cytoplasmic content. (Wright-Giemsa; HP oil.)
Hyperplastic Tissue
Hyperplasia is a non-neoplastic enlargement of tissue that can occur in response to hormonal disturbances or tissue injury. Hyperplastic tissue has a tendency to enlarge symmetrically in comparison to neoplasia. Cytologically, hyperplastic cells may appear similar to normal tissue but have a higher nuclear-to-cytoplasmic ratio than normal mature cells. Examples of hyperplastic responses include nodular proliferations within the parenchyma of the prostate (Fig. 2-3 ), liver (see Fig. 9-20A), and pancreas (Fig. 2-4 ).
Figure 2-3.

Canine prostatic hyperplasia. Tissue aspirate. Dog.
The presenting clinical sign in this case involves blood dripping from the prepuce. Cytologically, the nuclear size is uniform; however, the nuclear-to-cytoplasmic ratio is increased as indicated by the close proximity of nuclei to each other. (Wright-Giemsa; HP oil.)
Figure 2-4.

Nodular hyperplasia of the pancreas. Tissue aspirate. Dog.
Ultrasound examination revealed a hypoechoic mass in the area of the pancreas. Cytologically, hyperplastic parenchymal organs commonly display binucleation (arrows). (Wright-Giemsa; HP oil.)
Cystic Mass
Cystic lesions contain liquid or semisolid material. The low-protein liquid usually contains a small number of cells. These benign lesions may result from proliferation of lining cells or tissue injury. Examples include seroma (Fig. 2-5 ), salivary mucocele, apocrine sweat gland cyst, epidermal/follicular cyst (see Fig. 3-2), and cysts associated with noncutaneous glands such as the mammary gland or prostate (Fig. 2-6 ).
Figure 2-5.

Seroma. Tissue aspirate. Dog.
Blood-tinged fluid is removed from a swelling on the neck. There is low cellularity (3800/μL) and low protein content (2.5 g/dL). Cytologically, the direct smear contains a mixed cell population with large mononuclear cells having fine cytoplasmic granularity along with low numbers of erythrocytes. (Wright-Giemsa; HP oil.)
Figure 2-6.
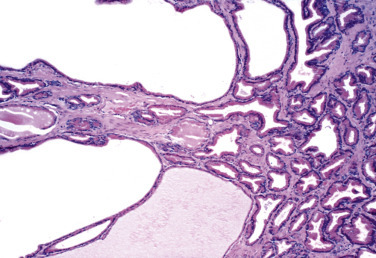
Prostatic cyst. Histopathology. Dog.
Cuboidal epithelial cells line large cystic spaces that represent dilated ducts. (H&E; LP.)
Inflammation or Cellular Infiltrate
Inflammatory conditions are classified cytologically by the predominance of the cell type involved. Recognition of the inflammatory cell type often suggests an etiologic condition.
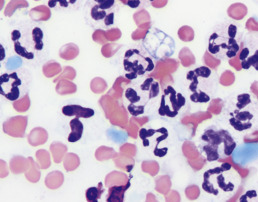
Purulent or suppurative lesions contain greater than 85% neutrophils; they are then classified by the presence or absence of nuclear degeneration of the neutrophil. Nondegenerate neutrophils are morphologically normal with mature condensed chromatin and well-segmented purple lobes. These neutrophils predominate in relatively nontoxic environments such as immune-mediated diseases (Fig. 2-7A ), neoplastic lesions (Fig. 2-7B), and sterile conditions caused by irritants such as urine and bile (Fig. 2-7C). Degenerate neutrophils display early signs of oncotic necrosis with observable cellular and nuclear swelling with decreased nuclear stain intensity. In cytology, this early recognizable change is termed karyolysis (Fig. 2-8 ). Karyolysis is attributed to decreased mitochondria function to produce ATP that maintains transmembrane ion pumps resulting in an influx of sodium, calcium, and water (hydropic degeneration) as well as to damaged cell membranes that result in release of endonucleases that degrade RNA and DNA. This often indicates rapid cell death in a toxic or injurious environment (Perman et al., 1979). Degenerate neutrophils predominate in bacterial infections, particularly gram-negative types that produce endotoxins. Cytologically, under conditions of neutrophil degeneration, small infectious agents must be found intracellularly to confidently report it as septic neutrophilic inflammation (Fig. 2-9 ).
Figure 2-7.

Nondegenerate neutrophils. Dog.
A, Synovial fluid from a Doberman Pinscher with an immune-mediated response to trimethoprim-sulfadiazine. There are eight neutrophils and five large mononuclear cells in a windrowing formation. (Wright-Giemsa; HP oil.) B, Nonseptic inflammation of synovial fluid with predominately well-segmented neutrophils appears secondary to adjacent neoplasia of the bone. (Wright-Giemsa; HP oil.) C, Abdominal fluid following bile duct rupture with intact neutrophils, one of which has phagocytized green-grey mucus. (Modified Wright; HP oil).
Figure 2-8.

Degenerate neutrophils, karyorrhexis.Tissue aspirate. Dog.
Mild to moderate karyolysis of neutrophils is evident by the decreased nuclear stain intensity and swollen nuclear lobes. Pyknosis of multiple nuclear segments appears as dark, dense, round structures, termed karyorrhexis (arrows), in this case of bacterial dermatitis. (Wright-Giemsa; HP oil.)
Figure 2-9.

Bacterial sepsis. Tissue aspirate. Dog.
Markedly karyolytic neutrophils are present with intracellular coccoid bacteria. Karyolysis is so severe that the cells are barely recognizable as neutrophils. A fragmenting erythrocyte is helpful for size comparison to demonstrate neutrophil swelling. (Modified Wright; HP oil.)
Karyolysis as a histologic term describes cell death in the form of a ghost nucleus or nuclear remnants that precede eventual nuclear loss or dissolution. In contrast to acute cell injury involving cellular and nuclear swelling, cell death may occur more slowly through a shrinkage phenomenon (apoptosis). While apoptosis often occurs in isolated cells during normal physiologic cell aging (Fig. 2-10A ), it may be found alongside pathologic cell death characterized by widespread nuclear destruction and necrosis.
Figure 2-10A.

Pyknosis. Blood. Dog.
Two-day-old blood displays cell aging and early pyknosis with rounded dense nuclear condensation and increased cytoplasmic eosinophilia. This change in the color of the cytoplasm is attributed to consolidation of cellular components or loss of ribosomal RNA which is responsible for cytoplasmic basophilia. (Modified Wright; HP oil.)
Increased nuclear staining (hyperchromia) with coalescence of the nucleus into a single or two dark basophilic round segments characterizes pyknosis (Fig. 2-10B ). If pyknosis is related to a slow, progressive change within a relatively nontoxic environment, an intact cell membrane may be present around the shrunken, more eosinophilic cell as occurs with normal cell aging. An end stage of nuclear breakdown termed karyorrhexis or karyorhexis (Mastrorilli et al., 2013) may be seen as the result of pyknosis of hypersegmented nuclei (Fig. 2-8) or fragmentation of chromatin of an individual dying cell (Fig. 2-11 ) as seen on both cytology and histology. Histiocytic or macrophagic lesions contain a predominance of macrophages, suggesting chronic inflammation (Fig. 2-12 ). Foamy, often vacuolated, and phagocytic cells characterize this type of inflammation. In contrast, granulomatous lesions consisting of activated macrophages that morphologically resemble epithelial cells form in response to foreign material or persistent intracellular infectious agents and have a secretory rather than phagocytic activity. These cells are therefore termed epithelioid macrophages and recognized by their abundant basophilic cytoplasm and large polygonal shape (Fig. 2-13A ). Epithelioid macrophages under the influence of cytokines and other inflammatory mediators undergo macrophage fusion to form giant multinucleated forms (Fig. 2-13B ). Granulomas are often associated with foreign body reactions and mycobacterial infections and may be recognized cytologically by the presence of epithelioid macrophages and/or multinucleate cells.
Figure 2-10B.

Pyknosis. Chylous effusion. Dog.
Chronic inflammation of this fluid produces neutrophils with nuclei that have condensed into a large, often single, dark, round structure (arrow) related to the slow progression of cellular change in this nonseptic environment. The pyknotic cell (arrow) in this case also contains a second, smaller round nuclear fragment. (Wright; HP oil.)
Figure 2-11.

Karyorrhexis. Bone marrow aspirate. Dog.
Fragmentation of the nucleus in this leukemic patient. (Modified Wright; HP oil.)
Figure 2-12.

Macrophagic inflammation. Tissue imprint. Dog.
Nodular lung disease with numerous large mononuclear cells having abundant foamy gray cytoplasm that also contains multiple colorless vacuoles. (Wright-Giemsa; HP oil.)
Figure 2-13A.

Pyogranulomatous inflammation. Tissue aspirate. Dog.
Long-standing bacterial infection created a mixture of degenerate neutrophils, epithelioid macrophages (arrows), binucleated giant cell, lymphocytes, and a vacuolated phagocytic macrophage. Note the presence of two cells displaying karyorrhexis. A plump fibroblast is seen in the upper left. (Modified Wright; HP oil.)
(From Raskin RE: Tail mass in a dog, NAVC Clinician’s Brief Nov:13-15, 2006.)
Figure 2-13B.

Multinucleate giant cell. Tissue aspirate. Cat.
Skin lesion with pyogranulomatous inflammation, including many giant cells related to the presence of fungal hyphae (not shown). Pictured is a cell with seven distinct nuclei and abundant blue-gray granular cytoplasm. (Wright-Giemsa; HP oil.)
Mixed cell inflammatory lesions contain a mixture of neutrophils and macrophages (Fig. 2-14 ) that also may include increased numbers of lymphocytes or plasma cells. This type of inflammation is often associated with foreign body reactions, fungal infections, mycobacterial infections, panniculitis, lick granulomas, and other chronic tissue injuries. The term pyogranulomatous should be reserved for a population of neutrophils and epithelioid macrophages with or without multinucleate giant cells (Fig. 2-13A).
Figure 2-14.

Mixed cell inflammation. Chylous effusion. Dog.
Chronic chylous effusion contains a variety of cell types, including nondegenerate neutrophils, vacuolated macrophages, small to medium lymphocytes, and two mature plasma cells. (Wright; HP oil.)
Eosinophilic lesions contain greater than 10% eosinophils in addition to other inflammatory cell types (Fig. 2-15 ). They are seen with or without mast cell involvement. It is not uncommon to see rust or brown granules in the cytoplasm of eosinophils on cytology in contrast to the pink red cell color. This inflammatory response is associated with eosinophilic granuloma, hypersensitivity or allergic conditions, parasitic migrations, fungal infections, mast cell tumors, and other neoplastic conditions that induce eosinophilopoiesis. This combination of eosinophilic inflammatory conditions has been referred to as “worms, wheezes, and weird diseases.”
Figure 2-15.

Eosinophilic inflammation. Transtracheal wash. Cat.
Clinical presentation of a chronic cough in this cat with suspected pulmonary allergy. Fluid contains 95% eosinophils. Pictured are several eosinophils that stain pale pink to blue-green and adhere to pink mucous material that prevents full stain penetration. (Wright-Giemsa; HP oil.)
Lymphocytic or plasmacytic infiltration is often associated with allergic or immune reactions, early viral infections, and chronic inflammation. The lymphoid population is heterogeneous, with small or intermediate-sized lymphocytes and plasma cells mixed with other inflammatory cells (Fig. 2-14). In contrast, a monomorphic population of lymphoid cells without other inflammatory cells present suggests lymphoid neoplasia.
Response to Tissue Injury
Cytologic samples often contain evidence of tissue injury in addition to cyst formation, inflammation, or neoplasia. These changes include hemorrhage, proteinaceous debris, cholesterol or calcium crystals, necrosis, and fibrosis.
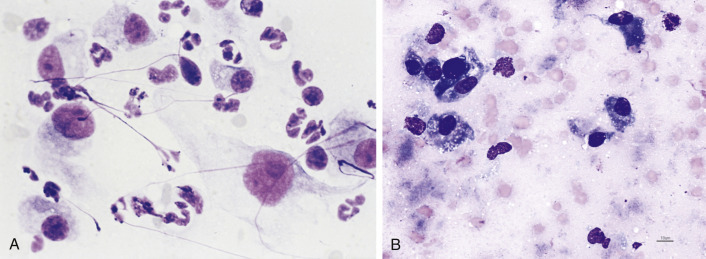
Hemorrhage that is pathologic can be distinguished from blood contamination encountered during the cytologic collection: Blood contamination is associated with the presence of numerous erythrocytes and platelets, whereas acute hemorrhage is associated with engulfment of erythrocytes by macrophages termed erythrophagocytosis (Fig. 2-16A ). Care must be taken to evaluate direct smears first prior to reporting the findings of processed materials. For example, the simple act of centrifugation to create a sediment smear from body fluids can activate macrophages to engulf nearby erythrocytes, which is not observed in the direct smear (Fig. 2-16B ). Chronic hemorrhage is associated with active macrophages containing degraded blood pigment within their cytoplasm—for example, blue-green to black hemosiderin granules (Figure 2-17, Figure 2-18 ) or yellow rhomboid hematoidin crystals (Fig. 2-18). Hemosiderin represents an excess aggregation of ferritin molecules or micelles. This form of iron storage becomes visible by light microscopy and stains blue with the Prussian blue reaction. Hematoidin crystals do not contain iron and are often formed during anaerobic breakdown of hemoglobin such as may occur within tissues or cavities. Hematomas often contain phagocytized erythrocytes if the lesion is acute or hemosiderin-laden macrophages if the lesion is chronic.
Figure 2-16A.

Erythrophagocytosis. Cerebrospinal fluid. Cat.
Many erythrocytes are in the background of this direct smear along with one large macrophage that has engulfed numerous intact red cells. The cat had a confirmed infection (titer 1:1600) with feline coronavirus (feline infectious peritonitis). Erythrophagocytosis in this case supports the presence of acute hemorrhage. (Wright; HP oil.)
Figure 2-16B.

Erythrophagocytosis post-centrifugation artifact. Pleural fluid. Dog.
Sedimentation of the fluid induced macrophage engulfment of erythrocytes. Blood contamination, not acute hemorrhage, is present in this case; this was supported by frequent platelets and the absence of erythrophagocytosis in the direct smear. (Modified Wright; HP oil.)
Figure 2-17.

Chronic hemorrhage with hemosiderin. Tissue aspirate. Dog.
Several foamy macrophages are present in this follicular cyst lesion. The macrophage directly below the cholesterol crystal contains blue-green granular material the cytoplasm consistent with hemosiderin, a breakdown product of erythrocytes. On the left edge is a macrophage with large black granules suggestive of hemosiderin. (Wright; HP oil.)
Figure 2-18.

Chronic hemorrhage with hematoidin and hemosiderin. Pericardial fluid. Dog.
Vacuolated macrophages with bright yellow rhomboid crystals (hematoidin) of variable size appear in this hemorrhagic fluid related to hemoglobin breakdown in an anaerobic environment. Several macrophages also contain black granular material consistent with hemosiderin. (Wright-Giemsa; HP oil.)
Proteinaceous debris may be seen within the background of the preparation. Mucus stains lightly basophilic and appears amorphous (Fig. 2-19 ). Lymphoglandular bodies (Fig. 2-20 ) are cytoplasmic fragments from fragile cells, usually lymphocytes, which are discrete, round, lightly basophilic structures (Flanders et al., 1993). Nuclear streaming refers to linear pink to purple strands of nuclear remnants (Fig. 2-21 ) produced by excessive tissue handling during cytologic preparation or with necrotic material when sampled. Clear to light-pink amorphous strands representing collagen (Fig. 2-22A ) may be admixed with spindle cells and endothelium within a fibrovascular stroma. However, when these collagen fibers undergo damage (as in the collagenolysis associated with mast cell tumor), degranulating eosinophils release collagenase that produces dense, hyalinized pink collagen bands (Fig. 2-22B). Amyloid is an uncommon pathologic protein found in tissues composed of several types between cells (Woldenmeskel, 2012). It appears amorphous, eosinophilic, and hyaline and may be associated with chronic inflammation, plasma cell tumors (see Fig. 3-54E&F), or familial amyloidosis (Fig. 2-22C).
Figure 2-19.

Mucus. Salivary mucocele. Dog.
The background contains pale pink-blue amorphous material representative of mucus. Numerous activated macrophages or mucinophages compose the predominant population. (Wright; HP oil.)
Figure 2-20.

Lymphoglandular bodies. Tissue aspirate. Dog.
The background of this lymph node preparation contains numerous small, blue-gray cytoplasmic fragments called lymphoglandular bodies that are related to the rupture of the fragile neoplastic lymphocytes. A large vacuolated macrophage has phagocytized cellular debris appearing as large blue-black particles. (Wright; HP oil.)
Figure 2-21.

Nuclear streaming. Tissue aspirate.
Purple strands of nuclear material are formed from ruptured cells either as an artifact of slide preparation or from fragile cells that are frequently neoplastic. (Wright-Giemsa; HP oil.)
(Courtesy of Denny Meyer, University of Florida.)
Figure 2-22.

A, Collagenous fibers. Tissue aspirate. Dog. Clear to light pink strands of intact fibrous connective tissue may resemble fungal hyphae. Collagenous fibers will have poorly defined margins and a variable diameter, unlike hyphae, which have uniform width and distinct borders. (Wright-Giemsa, HP oil.) B, Collagenolysis. Tissue aspirate. Dog. Haphazard bands of collagen appear bright pink and hyalinized owing to the breakdown of the fibers through release of collagenase by degranulating eosinophils. This type of connective tissue damage occurs commonly in canine mast cell tumors. Interspersed among tumor cells are eosinophils and their granules. (Wright; IP.) C, Amyloid. Tissue aspirate. Dog. Amorphous magenta material surrounds a hepatocyte from a Shar Pei with familial amyloidosis. (Modified Wright, HP oil.)
Cholesterol crystals represent evidence of cell membrane damage with lipid degeneration that may be found in the background of some cytologic preparations. These rectangular, plated crystals are transparent unless background staining is enhanced—for example, with new methylene blue stain (Fig. 2-23 ). The crystals are most often associated with epidermal/follicular cysts.
Figure 2-23.

Cholesterol crystal. Tissue aspirate.
Clear rectangular plates with notched corners are characteristic of cholesterol. This is often associated with degenerate squamous epithelium, as in follicular cysts. Crystals may be highlighted with background cellular debris or stain. (New methylene blue; HP oil.)
(Courtesy of Denny Meyer, University of Florida.)
Necrosis and fibrosis may occur together or separately in some cytologic preparations. The death of cells is represented by fuzzy, indistinct cell outlines and definition of cell type (Fig. 2-24A&B ). A reparative response accompanying tissue injury involves increased fibroblastic activity. It is common to see very reactive fibrocytes (Fig. 2-25A&B ) along with severe inflammation. One must be careful not to overinterpret this reactivity as a neoplastic condition because fibroblasts display anaplastic features such as open and ropy chromatin, prominent nucleoli, and high nuclear-to-cytoplasmic ratios (see Fig. 3-10A) compared with mature fibrocytes.
Figure 2-24.

Necrosis. Tissue aspirate. Dog.
A, Prominent nucleoli remain visible while other tissue has degenerated into dark blue-gray amorphous debris representative of necrotic material. The sample was taken from a case of prostatic carcinoma in which the necrotic site was focal. (Wright-Giemsa; HP oil.) B, Cell outlines remain visible while nuclear swelling is evident during this example of acute cell death. Same case as A. (Wright-Giemsa; HP oil.)
Figure 2-25.
A, Reactive fibroplasia. Tissue scraping. Cat. Oral mass with associated septic inflammation. Pictured are several plump mesenchymal cells with a stellate to spindle appearance and prominent nucleoli along with suppurative inflammation. The severity of the inflammatory response warrants caution in suggesting a malignant mesenchymal mass or sarcoma. Note the nuclear streaming appears as purple strands. (Aqueous Romanowsky; HP oil.) B, Postnecrosis fibroplasia. Tissue aspirate. Dog. Facial swelling related to myositis. The background contains amorphous grey material supportive of necrosis. Several fibroblasts indicate a reparative process following tissue damage. (Modified Wright; HP oil.)
Mitosis may be evident with increased cell turnover under normal physiologic and reparative influences in addition to a neoplastic proliferation (Fig. 2-26A-I ). Normal appearing mitotic figures are common in hyperplastic lymph nodes and regenerative bone marrow. Differences between normal and abnormal mitotic figures was previously discussed (Tvedten, 2009).
Figure 2-26.

Normal mitotic figures. Dog.
A, Prophase and telophase. Binucleated cell in the center undergoing prophase within a membrane-bound nucleus while the cell at 7 o’clock is in telophase with two sets of daughter chromosomes at either pole. B, Metaphase. The chromosomes are lined up at the equator. C, Metaphase. The chromatids are visible as individualized chromosomes along the equator. D, Early anaphase. A break between the chromatids has begun to separate the chromosomes into two daughter cells. E, Anaphase. A circle of chromosomes appears. F, Telophase. The two sets of chromosomes have been pulled to opposite poles of the mitotic spindle. G, Late telophase. Following condensation of the chromosomes, there is the beginning of a division in the cytoplasm. H, Late telophase and cytokinesis. The bottom cell is in telophase as it begins to divide, and the top two cells have just formed from complete division of the cytoplasm, creating two daughter cells. I, Metaphase and telophase. Note the cell in metaphase at 3 o’clock and the cell in telophase at 9 o’clock in this histologic section of a canine melanoma. (HE; HP oil.) Images A-H are from a canine bone marrow aspirate (Aqueous Romanowsky; HP oil.)
Neoplasia
General Features
Neoplasia is initially diagnosed when a monomorphic or monotypic cell population is present and significant inflammation is lacking. Further division into benign and malignant types is based on cytomorphologic characteristics. Benign cells display uniformity in nuclear and cell size, nuclear-to-cytoplasmic ratio, and other nuclear features. Malignant cells often display three or more criteria (Table 2-1 and Figure 2-27, Figure 2-28, Figure 2-29, Figure 2-30, Figure 2-31, Figure 2-32, Figure 2-33 ) of cellular immaturity or atypia, which should be identified before a diagnosis of malignancy is made. In cases of an equivocal diagnosis or severe inflammation, histopathologic examination is recommended.
Table 2-1.
Cytologic Criteria Used to Identify Malignant Cells
| Criterion | Morphologic Features |
|---|---|
| Pleomorphism | Variation in the size, shape, or maturation state of cells and their nuclei (Fig. 2-27) |
| Nuclear-to-cytoplasmic ratio | High or variable nuclear-to-cytoplasmic ratio between cells of similar origin (Fig. 2-28) |
| Anisokaryosis | Variation in nuclear size between cells of similar origin (Fig. 2-28) |
| Coarse chromatin | Ropy chromatin or clumping of nuclear chromatin is common in immature cells (Fig. 2-29) |
| Nucleolar changes | Variation in nucleolar size (anisonucleoliosis), enlarged, multiple, or variably shaped nucleoli (Fig. 2-30) |
| Nuclear molding | Abnormal nuclear shape related to the rapid growth of cells in which tight cell spacing occurs without normal crowd inhibition (Fig. 2-31) |
| Multinucleation | Two or more nuclei occupy the same cell. Binucleation may be found in hyperplasia of some tissues (Fig. 2-32) |
| Abnormal mitotic figures | Abnormal chromosomal fragments may appear with uneven length of chromatin strands and as isolated or lag chromatin. Increased numbers may be suggestive but not definitive for malignancy (Fig. 2-33) |
Figure 2-27.

Pleomorphism. Tissue aspirate. Dog.
Transitional cell carcinoma cells display variability in size and shape supportive of malignancy. (Wright-Giemsa; HP oil.)
Figure 2-28.

Anisocytosis, anisokaryosis. Tissue aspirate. Dog.
Lung adenocarcinoma specimen has several features of malignancy. These features include high and variable nuclear-to-cytoplasmic ratio, anisokaryosis, binucleation, and coarse nuclear chromatin. (Wright-Giemsa; HP oil.)
Figure 2-29.

Coarse chromatin. Tissue aspirate. Dog.
Same case as Fig. 2-26. The ropy nuclear material is mottled with light and dark spaces clearly evident. This appearance is often associated with neoplastic transitional epithelium but may be seen with other tissues. Binucleation is seen in one cell, and a mitotic figure is present on the bottom edge. (Wright-Giemsa; HP oil.)
Figure 2-30.

Prominent nucleoli. Tissue aspirate.
Dog. Same case as Fig. 2-24. A binucleate cell with very large single nucleoli in each nucleus is present. A prominent nucleolus is noted in the adjacent cell, which also displays coarse chromatin or chromatin clumping. (Wright-Giemsa; HP oil.)
Figure 2-31.

Nuclear molding. Tissue aspirate. Dog.
Nasal chondrosarcoma pictured with a binucleate cell in which one nucleus is wrapped around the other within the same cell. This feature is present in malignant tissues and is related to the lack of normal inhibition of cell growth. (Wright-Giemsa; HP oil.)
Figure 2-32.

Multinucleation. Tissue imprint. Dog.
Pheochromocytoma with two multinucleate cells, one in the lower left side with three nuclei and the other to the right of center with an irregularly shaped nuclear region. Multinucleation may also be found in epithelial, mesenchymal, and round cell neoplasms. (Wright-Giemsa; HP oil.)
Figure 2-33.

Abnormal mitosis. Tissue and bone marrow aspirates. Dog.
A-F,Multiple views of abnormal mitotic figures, which divide unevenly compared with normal divisions (Fig. 2-26). Chromosomal fragments are dispersed irregularly with some isolated from the rest, termed lag chromatin. Increased mitotic activity may suggest malignancy, but abnormal division is more diagnostic for malignancy. (Wright-Giemsa; HP oil.)
Cytomorphologic Categories
Neoplasms may be divided into four general categories to assist in making the cytologic interpretation by restricting the list of differential diagnoses (Perman et al., 1979, Alleman and Bain, 2000). The categories listed in Table 2-2 are NOT based on cell origin or function but rather on their general cytomorphologic characteristics that include their general association to one another (Table 2-2). The first two terms, epithelial and mesenchymal, are taken from embryologic histology (Noden and de Lahunta, 1985).
Table 2-2.
Four Cytomorphologic Categories of Neoplasia
| Category | General Features | Examples |
|---|---|---|
| Epithelial | Clustered, tight arrangement of cells | Transitional cell carcinoma, lung tumors, sebaceous adenoma |
| Mesenchymal | Individualized, spindle to oval cells | Hemangiosarcoma, osteosarcoma, fibroma |
| Round cell | Individualized, round, discrete cells | Transmissible venereal tumor, lymphoma, mast cell tumor, plasmacytoma, histiocytic tumors |
| Naked nuclei | Loosely adherent cells with bare round nuclei | Thyroid tumors, Sertoli cell tumors, paragangliomas, neuronal cells |
Epithelial Neoplasms
Epithelial neoplasms often originate from glandular or parenchymal tissue and lining surfaces, and they are associated with a clustered arrangement of cells into ball shapes or monolayer sheets. Examples of epithelial neoplasms include lung adenocarcinoma (Fig. 2-34 ), perianal adenoma (hepatoid tumor), basal cell tumor, sebaceous adenoma, transitional cell carcinoma (Fig. 2-35 ), and mesothelioma. Specific cytologic features of epithelial neoplasms are listed in Box 2-2 (Fig. 2-36 ).
Figure 2-34.

Epithelial neoplasm. Lung lavage. Dog.
Large clusters of cohesive cells having distinct cell borders from a case of lung adenocarcinoma. (Wright-Giemsa; IP.)
(Courtesy of Robert King, Gainesville, Florida, United States.)
Figure 2-35.

Epithelial neoplasm. Tissue aspirate. Dog.
Same case as Fig. 2-26. Cells are formed into tight balls or as sheets. Nuclei are round to oval and cells are large, round to polygonal with distinct cytoplasmic borders. (Wright-Giemsa; HP oil.)
Box 2-2. Specific Cytologic Features of Epithelial Neoplasms.
-
•
Cells exfoliate in tight clumps or sheets
-
•
Cells adhere to each other and may display distinct tight junctions, termed desmosomes (Fig. 2-36)
-
•
Cells are large and round to polygonal with distinct, intact cytoplasmic borders
-
•
Nuclei are round to oval
Figure 2-36.

Desmosomes. Tissue aspirate. Dog.
Same case as Fig. 2-24. A sheet of carcinoma cells with prominent desmosomes. These clear lines (arrow) between adjacent cells represent tight junctions that are characteristic of epithelial cells. (Wright-Giemsa; HP oil.)
Mesenchymal Neoplasms
Neoplasms with a mesenchymal appearance resemble the embryonic connective tissue, mesenchyme. This tissue is loosely arranged with usually abundant extracellular matrix (Noden and de Lahunta, 1985) and individualized spindle, oval, or stellate cells (Bacha and Bacha, 2000). Benign and malignant mesenchymal neoplasms often originate from connective tissue elements, such as fibroblasts, osteoblasts, adipocytes, myocytes, and vascular lining cells. Examples of mesenchymal neoplasms include hemangiosarcoma (Fig. 2-37 ), osteosarcoma (Fig. 2-38 ), fibroma (see Fig. 3-39), and amelanotic melanoma (Fig. 2-39 ). Specific cytologic features of mesenchymal neoplasms are listed in Box 2-3 .
Figure 2-37.

Mesenchymal neoplasm. Tissue imprint. Dog.
Neoplastic cells exfoliate individually and appear oval, spindle, or fusiform. This bone lesion was confirmed as hemangiosarcoma on histologic examination. Characteristic of hemangiosarcoma cytology is a poorly cellular sample with large plump mesenchymal cells that contain numerous small punctate colorless cytoplasmic vacuoles. (Wright-Giemsa; HP oil.)
Figure 2-38.

Mesenchymal neoplasm. Tissue aspirate. Dog.
The finding of individualized pleomorphic cells with abundant extracellular eosinophilic osteoid material is consistent with osteosarcoma. Binucleate and multinucleate forms are common and seen in this sample. (Wright-Giemsa; HP oil.)
Figure 2-39.

Mesenchymal neoplasm. Tissue imprint. Dog.
Round to oval nuclei, anisokaryosis, high nuclear-to-cytoplasmic ratio, prominent and variably shaped nucleoli, and individualized cells with poorly distinct cytoplasmic borders suggest a malignant mesenchymal neoplasm. This lesion is from a gum mass with a histologically confirmed diagnosis of amelanotic melanoma. One cell in the center contains small amounts of melanin pigment granules. (Aqueous Romanowsky; HP oil.)
Box 2-3. Cytologic Features of Mesenchymal Neoplasms.
-
•
Cells usually exfoliate individually (however, aggregates of cells are seen occasionally bound by an extracellular matrix)
-
•
Cells are oval, stellate, or fusiform with often indistinct cytoplasmic borders
-
•
Samples are often poorly cellular
-
•
Cells are usually smaller than epithelial cells
-
•
Nuclei are round to elliptical
Round Cell Neoplasms
Round cell neoplasms have discrete, round cellular shapes and are associated with hematopoietic cells. Therefore, their nuclear size is roughly two to four times the diameter of an erythrocyte. The five categories of round cell neoplasms include transmissible venereal tumor (Fig. 2-40 ), lymphoma (Fig. 2-41 ), mast cell tumor (see Fig. 3-53D), plasmacytoma (see Fig. 3-54A&B), and histiocytic tumors (see Figs. 3-49C and 3-51AFig. 3-49CFig. 3-51A); these can be remembered by the acronym T-LyMPH. Specific cytologic characteristics of round cell neoplasms are listed in Box 2-4 .
Figure 2-40.

Round cell neoplasm. Tissue aspirate. Dog.
Discrete cells with a round shape, distinct cytoplasmic borders, and a very high nuclear-to-cytoplasmic ratio are characteristic of lymphoid cells. This sample is taken from a lymph node effaced by lymphoma cells. (Wright-Giemsa; HP oil.)
Figure 2-41.

Round cell neoplasm. Tissue aspirate. Dog.
This fleshy vulvar mass is composed of round cells bearing a single prominent nucleolus and moderately abundant cytoplasm with frequent punctate colorless cytoplasmic vacuolation. The cytologic diagnosis is transmissible venereal tumor. (Wright-Giemsa; HP oil.)
Box 2-4. Specific Cytologic Characteristics of Round Cell Neoplasms.
-
•
Cells exfoliate individually, having distinct cytoplasmic borders
-
•
Cells are generally round
-
•
Samples are moderately cellular
-
•
Cells are usually smaller than epithelial cells
-
•
Nuclei are round to indented
Naked Nuclei Neoplasms
Neoplasms with a naked nuclei cytomorphology have a loosely adherent cellular arrangement with free nuclei. This cytologic appearance is an artifact related to the fragile nature of these cells. These neoplasms are usually associated with endocrine, neuroendocrine, and neural tumors (Perman et al., 1979). In addition, anal sac adenocarcinoma frequently displays this pattern when aspirated (see Fig. 3-36). Typical examples include thyroid tumors (Fig. 2-42 ), islet cell tumors, paragangliomas (Fig. 2-43 ), and neuropil (see Fig. 14-37). Specific cytologic features of naked nuclei neoplasms include those listed in Box 2-5 .
KEY POINT The use of these four cytomorphologic categories may help classify neoplastic lesions by their general cellular appearance and arrangement, thereby suggesting specific tumor types. Remember that these categories may not fit well for some neoplasms, especially for poorly differentiated tumors. It is recommended that biopsy specimens for histopathologic examination be taken to determine the specific tumor type and extent of the lesion under most circumstances.
Figure 2-42.

Naked nuclei neoplasm. Tissue aspirate. Dog.
Cervical mass in the area of the thyroid from an animal with a honking cough. Cytologically, the sample presents as a syncytium of round nuclei with relatively uniform features. This is characteristic of an endocrine mass. Typically the distinction between hyperplasia, adenoma, and carcinoma is difficult cytologically and sometimes histologically. (Wright-Giemsa; HP oil.)
Figure 2-43.

Naked nuclei neoplasm. Tissue imprint. Dog.
Clinical signs include a head tilt and temporal muscle atrophy. Magnetic resonance imaging suggested a mass involving the osseous bulla. Surgery found a mass at the bifurcation of the common carotid artery. Cytologically, the preparation contains mostly loose or free round nuclei against a finely granular eosinophilic background. While most nuclei are similarly sized, an occasional cell appears larger. Few intact cells remain with pale cytoplasm at the edges and center. Adjacent to the center intact cell is a nucleated red cell (arrow) suggestive of extramedullary hematopoiesis. The histologic diagnosis is paraganglioma, specifically a malignant chemodectoma in this case, because it metastasized and was thought to involve the chemoreceptor organ in that site. (Wright-Giemsa; HP oil.)
Box 2-5. Specific Cytologic Features of Naked Nuclei Neoplasms.
-
•
Cells often exfoliate in loosely attached sheets with many free nuclei present and indistinct cytoplasmic borders
-
•
Occasional cell clusters may be present with distinct cell outlines
-
•
Cells are generally round to polygonal
-
•
Samples are highly cellular
-
•
Nuclei are round to indented, often with none to minimal anisokaryosis
Artifacts and other Questionable Findings
Specimen Acquisition and Processing
Sometimes it is difficult to differentiate artifact from a pathologic/diagnostic finding. The following examples illustrate some of the more common materials or structures associated with cytologic specimens that may be puzzling or distracting. In some cases artifacts are induced by specimen processing (Fig. 2-44A-C ), rough handling (Fig. 2-44D), excess blood with formation of hemoglobin crystals (Fig. 2-44E-F), presence of ultrasound gel (Fig. 2-44G), precipitate formation from methanolic Romanowsky stain (Fig. 2-44H), and talc or starch granules from surgical gloves (Fig. 2-44I).
Figure 2-44.

Artifacts from sample acquisition and processing.
A-C, Centrifugation alterations. Dog. A, Direct fluid smear. B, Cytocentrifuge specimen. C, Sediment preparation smear. Cytocentrifuge preparations spread out nucleated cells and may lyse erythrocytes. Samples centrifuged for 5 minutes may result in artifactual erythrophagocytosis by macrophages. This finding should always be compared with the direct smear to be confident it is a real finding. It was not real in this case because the direct smear contained no evidence of erythrophagocytosis. (Modified Wright; HP oil.) D, Scratches. Linear clear streaks in the stained background typically arise from slides contacting other slides during staining or accidental wiping of the slide. E-F, Hemoglobin crystals. Dog. Variable magnifications of pink needle-like crystals that may arise from slow drying of a highly blood contaminated sample. (Modified Wright; HP oil.) G, Ultrasound gel. Dog. Presence of magenta granular precipitate should be ignored if known to be a specimen from material taken under ultrasound guidance. The material is significant when taken from the site of a previous vaccination (see Fig. 3-4). (Modified Wright; HP oil.) H, Stain precipitate and bacteria. Dog. The lower left dark granular material represents residue following methanolic Romanowsky staining. Compare a similar granularity and color to coccoid bacteria in the upper right. (Modified Wright; HP oil.) I, Talc powder or starch granules. Cat. This foreign material is characteristic by the cross mark in the center of the crystal cell. (Modified Wright; HP oil.)
Crystalline Structures
Background material often reflects degenerative changes such as dystrophic calcification (Fig. 2-45A ) or urate crystals in tissues (Fig. 2-45B). When viewed against a proteinaceous background, crystals such as cholesterol crystal needles may be seen (Fig. 2-45C). However, these fragments should not be confused with certain bacteria such as mycobacterial species that have thick outer lipid cell walls that do not take up stain well and appear as negative rods against a proteinaceous background (Fig. 2-45D).
Figure 2-45.

Crystals and crystal-like structures.
A, Calcium mineralization. Lung aspirate. Cat. Refractile crystalline material stains light blue in the area of tissue necrosis. (Modified Wright; HP oil.) B, Urate crystals. Joint aspirate. Tortoise. Gout arthritis is noted by the presence of long thin needle-like crystals. (Unstained; HP oil.) C, Cholesterol needle crystals. Perianal mass aspirate. Dog. The background contains numerous linear streaks of various lengths and widths having sharp sides. It is likely the result of tissue damage with release of cell membrane lipids. (Modified Wright; HP oil.) D, Mycobacterial infection. In the proteinaceous background, lipids from the bacterial cell wall create negative streaks of uniform width and length in contrast to crystals. (Romanowsky; HP oil.) (D, Courtesy of Andrew Torrance, Exeter, UK.)
Linear Shapes
Linear shapes can be confusing within samples. Although commonly associated with respiratory specimens, Curschmann spirals represent inspissated mucus and have been seen rarely in dermal lesions (Fig. 2-46A ). Capillaries lined by endothelium that occasionally contain erythrocytes are common with lymphoid organs and other highly vascularized tissues (Fig. 2-46B&C). Organic or synthetic fibers may resemble hyphae or hair shafts but are usually distinguished by a refractile or colored feature (Fig. 2-46D). In contrast, fungal hyphae may appear pigmented or nonpigmented (Fig. 2-46E) with uniform width and sometimes distinctive septation or presence of a fruiting body (Fig. 2-46F). Large deeply basophilic thick fibers may indicate skeletal muscle tissue (Fig. 2-46G). Upon close inspection of the muscle tissue, one often observes surface nuclei along with cross-striations. Fig. 2-46H&I demonstrates the typical location and appearance of keratin bars, which is suggestive of fingerprints.
Figure 2-46.

Linear structures.
A, Curschmann’s spiral. Skin aspirate. Dog. Long linear corkscrew strand is indicative of inspissated mucus that may be found in sites other than the respiratory tract. (Modified Wright; HP oil.) B-C, Blood vessel. Nasal aspirate. Cat. Two magnifications are shown to demonstrate the curving pattern and morphologic components of a capillary. Note the endothelial-lined tube with red blood cells inside. (Modified Wright; IP and HP oil.) D, Synthetic fiber. Blood. Cat. Blue transparent thread found on top red cells as a contaminant structure. The variable width and color are helpful features. (Modified Wright; HP oil.) E, Fungal hyphal segment. Urine. Dog. Degenerate neutrophils surround the structure, which is septated. (Modified Wright; HP oil.) F, Aspergillus fruiting body with conidia. Nasal plaque imprint. Dog. The swollen part of the conidiophore termed the vesicle is covered by a dense cap or phialides from which small round conidia arise, each measuring 3 μm in diameter. (New methylene blue; HP oil.) G, Muscle fragments. Tissue aspirate. Dog. Presence of deeply basophilic rectangular pieces suggests skeletal muscle. Confirmation is made by higher magnification to see cross-striations (Fig. 2-1) (Modified Wright; IP.) H-I, Fingerprint keratin bars. Near the glass slide edges are numerous individualized squamous epithelial cells represented by dense dark keratin bars. These surface epithelial cells related to excessive handling of the slide may confuse the diagnosis if they appear within the center of the slide and specimen. (Aqueous Romanowsky; LP and IP.)
Blue-Green Materials
The background may contain regular or irregularly shaped materials that stain basophilic or green. Fig. 2-47A&B demonstrates the sulfur granular seen grossly in actinomycosis in which mats of bacterial filaments appear as amorphous junk-like material. Always examine this material and especially around the periphery to find the typical beaded filamentous bacteria. In addition to the yellow bile material found within the abdominal cavity upon rupture of the biliary ducts, amorphous mucus of various size and shape appears pale blue within cells or extracellularly (Fig. 2-47C). Plant pollen or spores that are green are often found within the respiratory tract or in areas with easy access to the environment. These should be considered contaminants under most circumstances (Fig. 2-47D).
Figure 2-47.

Blue-green material.
A-B, Actinomycosis. Nasal imprint. Cat. Low and higher magnification of bacterial mats and purulent inflammation. Bacteria are rarely found in areas away from the large mats of bacteria (not shown). However, just adjacent to the basophilic granular masses are numerous thin beaded filamentous bacteria. (Modified Wright; LP and HP oil.) C, Bilious effusion. Abdominal fluid direct smear. Dog. The background contains several pale blue-green amorphous proteins seen as small pieces (shown) or large lakes (not shown). This is consistent with mucus from the biliary tree. (Modified Wright; HP oil.) D, Pollen grains. Urine cytospin preparation. Dog. An aggregate of blue-green ovoid spores are found in voided urine. Although there is an inflammatory process occurring, these extracellular structures are considered to be contaminants. (Modified Wright; HP oil.)
References
- Alleman A.R., Bain P.J. Diagnosing neoplasia: the cytologic criteria for malignancy. Vet Med. 2000;95:204–223. [Google Scholar]
- Bacha W.J., Bacha L.M. ed 2. Lippincott Williams & Wilkins; Philadelphia: 2000. Color atlas of veterinary histology. pp 13–15. [Google Scholar]
- Flanders E., Kornstein M.J., Wakely P.E. Lymphoglandular bodies in fine-needle aspiration cytology smears. Am J Clin Pathol. 1993;99:566–569. doi: 10.1093/ajcp/99.5.566. [DOI] [PubMed] [Google Scholar]
- Mastrorilli C., Welles E.G., Hux B. Botryoid nuclei in the peripheral blood of a dog with heatstroke. Vet Clin Pathol. 2013;42:145–149. doi: 10.1111/vcp.12041. [DOI] [PubMed] [Google Scholar]
- Noden D.M., de Lahunta A. Williams & Wilkins; Baltimore: 1985. The embryology of domestic animals. pp 10–11. [Google Scholar]
- Perman V., Alsaker R.D., Riis R.C. American Animal Hospital Association; South Bend,: 1979. Cytology of the dog and cat. pp 4–7. [Google Scholar]
- Tvedten H. Atypical mitoses: morphology and classification. Vet Clin Pathol. 2009;38:418–420. doi: 10.1111/j.1939-165X.2009.00201.x. [DOI] [PubMed] [Google Scholar]
- Woldemeskel M. A concise review of amyloidosis in animals. Vet Med Internatl. 2012;2012:427296. doi: 10.1155/2012/427296. [DOI] [PMC free article] [PubMed] [Google Scholar]