

Abstract
We searched the PubMed database for clinical trials and observational human studies about postexposure vaccination effects, targeting infections with approved vaccines and vaccines licensed outside the United States against dengue, hepatitis E, malaria, and tick-borne encephalitis. Studies of animal models, serologic testing, and pipeline vaccines were excluded. Eligible studies were evaluated by definition of exposure; attempts to distinguish pre- and postexposure effects were rated on a scale of 1 to 4. We screened 4,518 articles and ultimately identified for this review 14 clinical trials and 31 observational studies spanning 7 of the 28 vaccine-preventable diseases. For secondary attack rate, the following medians were found for postexposure vaccination effectiveness: hepatitis A, 85% (interquartile range (IQR), 28; n = 5 sources); hepatitis B, 85% (IQR, 22; n = 5 sources); measles, 83% (IQR, 21; n = 8 sources); varicella, 67% (IQR: 48; n = 9 sources); smallpox, 45% (IQR, 39; n = 4 sources); and mumps, 38% (IQR, 7; n = 2 sources). For case fatality proportions resulting from rabies and smallpox, the median vaccine postexposure efficacies were 100% (IQR, 0; n = 6 sources) and 63% (IQR, 50; n = 8 sources), respectively. Many available vaccines can modify or preclude disease if administered after exposure. This postexposure effectiveness could be important to consider during vaccine trials and while developing new vaccines.
Keywords: immunization, immunotherapy, infectious disease, postexposure prophylaxis, vaccines
Abbreviations
- FDA
Food and Drug Administration
- IQR
interquartile range
INTRODUCTION
Since the advent of variolation in the early second millennium, vaccination has been considered a way to prevent healthy individuals from acquiring disease (1). However, to implement informed trials and curb future outbreaks and epidemics, postexposure effectiveness must be better understood. Substantial efforts have been made to develop therapeutic vaccines for treating chronic conditions such as cancer, diabetes, human immunodeficiency viruses, and obesity (2), but pre-exposure vaccination remains the focus for communicable disease. One notable exception is the rabies vaccine, which has achieved near total efficacy in exposed individuals for the last century. The smallpox vaccine also provided well-documented postexposure prophylaxis until the disease was eradicated 1980, with recommendations dating back to the mid-19th century (3). Nevertheless, uncertainty surrounding exposure status and length of incubation make postexposure properties difficult to estimate for any vaccine, and relatively few studies have done so for those that are currently available.
The effectiveness of postexposure vaccination varies widely depending on disease course, in terms of individual immune response and population-level spread. Although pre-exposure vaccination protects uninfected individuals from infection, postexposure vaccination modifies or prevents clinical disease among those who are already infected. As a result, postexposure trials must operate within a constrained time: participants must be identified and treated between exposure and symptom onset. Measurable benefits may occur if the vaccine stimulates an immune response faster or greater than that provoked by the natural infection alone. For smallpox, the vaccine induces antibody response 4–8 days before the variola virus does, probably because the response bypasses the initial respiratory-tract stages of a natural infection (4). These response kinetics explain historical evidence of a postexposure window and provide a basis for comparing surrogate models to humans in the case of reemergence (5). For rabies, though, this explanation has been unable to fully account for the vaccine’s postexposure mechanisms. Protection has generally been attributed to neutralizing antibodies, but rabies-exposed patients with human immunodeficiency viruses have been known to remain well despite poor or undetectable antibody levels after vaccination (6, 7).
At the community level, postexposure measures could be instrumental in reducing disease burden, especially when mass pre-exposure immunization is not feasible. Mathematical models for tuberculosis have been used to estimate that a postexposure vaccine would initially be more effective at reducing disease incidence compared with a preventive vaccine, although over time, a pre-exposure vaccine would result in increasing impact as more uninfected persons were vaccinated and protected against infection (8). One promising postexposure anti-tuberculosis candidate, the M72/AS01E vaccine, recently exhibited 54.0% efficacy against disease in a latently infected population (9). Although most diseases do not have such a large pool of hosts harboring latent infections—nearly a third of the global population carries tuberculosis—postexposure vaccination has already curtailed smaller outbreaks of varicella (10, 11), hepatitis A (12, 13), and measles (14, 15). These diseases tend to spread widely during outbreaks, but reactive vaccination studies usually operate under accelerated time frames and researchers have struggled to distinguish pre- and postexposure effects. One approach involves considering only the impact of vaccination on symptoms occurring before 1 incubation period after vaccination, which accounts for some of the uncertainty surrounding exposure status and timing. Variable incubation periods further complicate this method and make it especially difficult to draw conclusions about vaccination delays. As a result, the most robust information results from studies involving a known exposure during a definite interval before vaccination, as is the case for most percutaneous exposures or in settings that practice quarantine.
To address postexposure effectiveness across multiple diseases, we reviewed all infections that currently have a US Food and Drug Administration (FDA)-licensed vaccine, plus dengue, hepatitis E, malaria, and tick-borne encephalitis, for which vaccines are available in areas outside the United States (Table 1). The evidence could guide treatment protocols and also concerns the design and interpretation of more informative vaccine trials. We evaluated vaccines administered between exposure and symptom onset, but we also discuss the current state of research on therapeutic vaccines. These are a subset of postexposure vaccines designed to intervene after the onset of clinical disease, about which we include a brief summary illustrating the broader territory of nonpreventive, postexposure vaccination.
Table 1.
All Infections With a US Food and Drug Administration–Licensed Vaccine, Plus Dengue, Hepatitis E, Malaria, and Tick-Borne Encephalitis
| Eligible Infection | Incubation Period, Days (Range) (83–85)a | Interval for Successful Postexposure Vaccination (Maximum) b | Current ACIP Recommendations for Postexposure Prophylactic Vaccine Use |
|---|---|---|---|
| Cholera | 0.08–5.00 | No data | None |
| Pneumococcal disease | 1–3 | No data | None |
| Anthrax | No data | 0, 2, 4 weeks | |
| Cutaneous | 1–7 | ||
| Inhalation | 7–60 | ||
| Rotavirus | 2 | No data | None |
| Diphtheria | 2–5 (1–10) | No data | Toxoid recommended |
| Haemophilus influenzae type b | 2–7 | No data | None |
| Meningococcal meningitis | 3–4 (2–10) | No data | None |
| Yellow fever | 3–6 | No data | None |
| Denguec | 5–7 (3–10) | No data | None |
| Influenza | 5–7 | No data | None |
| Japanese encephalitis | 5–15 | No data | None |
| Typhoid | 6–30 | No data | None |
| Pertussis | 7–10 (4–21) | No data | None |
| Malariac | 7–30 | No data | None |
| Poliomyelitis | 7–21 | No data | None |
| Tick-borne encephalitisc | 8 (4–28) | No data | None |
| Tetanus | 10 (3–21) | No data | Toxoid recommended |
| Measles | 11–12 (7–21) | ≤3 days | ≤3 days |
| Smallpox | 10–14 (7–19) | N/A (case-by-case decisions) | |
| For secondary attack | Insufficient data | ||
| For fatality | ≤3 days | ||
| Chickenpox/varicella | 14–16 (10–21) | ≤3 days | ≤5 days |
| Human papillomavirus | 14–240 | No data | None |
| Mumps | 16–18 (12–25) | Insufficient data | Vaccine recommended, no timing provided |
| Rubella | 17 (12–23) | No data | None |
| Hepatitis A | 28 (15–50) | ≤14 days | ≤14 days |
| Rabies | 30–90 | ≤5 days (+4 boosters) | 0, 3, 7, 14 days |
| Hepatitis Ec | 42 (14–63) | No data | None |
| Hepatitis B | 120 (45–160) | ||
| For infants | ≤1 month (+2 boosters) | Routine vaccine series | |
| For adults | Insufficient data | Vaccine series | |
| Tuberculosis | Weeks to years | No data | None |
Abbreviations: ACIP, Advisory Committee on Immunization Practices; N/A, not applicable.
a Infections are organized by minimum length of incubation according to the US Centers for Disease Control and Prevention.
b The maximum interval is defined as the longest delay, with at least 3 studies suggesting an effectiveness of >75%. Studies with no evidence are indicated with ”no data.”
c These infections have vaccines available in areas outside the United States.
METHODS
Strategy
We searched PubMed for clinical trials or observational studies pertaining to all FDA-licensed vaccines and their effectiveness after exposure. Search terms for each disease included but were not limited to “(disease) postexposure vaccine,” “(disease) postexposure vaccination,” “(disease) post-exposure vaccine,” “(disease) post-exposure vaccination,” “(disease) vaccine after exposure,” and “(disease) vaccination after exposure.”
Studies of animal models, serologic testing, or pipeline vaccines were excluded from this analysis. To ensure demonstration of a post- rather than pre-exposure effect, we limited consideration to secondary cases either confined to the first incubation period after vaccination or otherwise attributed to exposure before vaccination. Satisfactory evidence of such limitation included recording the time of vaccination and symptom onset within the vaccinated group or proving that exposure to the disease ended definitively before vaccination. In most studies, secondary attack rates were compared between vaccinated and unvaccinated groups, but for diseases with high rates of infection after exposure, such as rabies and smallpox, researchers sometimes looked to fatality proportions among secondary cases as a measure of vaccine effectiveness. We included both types of studies, along with reactive vaccination trials that met our susceptibility and exposure criteria. To determine the exposure ratings (defined in the following section), both authors conducted independent methodological assessments. Any discrepancies were resolved through discussion.
Definitions
Evidence of postexposure effectiveness was considered in terms of secondary attack and fatality outcomes. The effectiveness itself was defined as the relative reduction in outcome risk after having been exposed to a pathogen and subsequently vaccinated against it versus no vaccine or placebo. Because definitions of susceptibility and exposure vary, the exact descriptions have been compiled for each report in Web Appendix 1 and Web Tables 1–8 (available at https://academic.oup.com/aje). In most studies, susceptible individuals were characterized as those with negative history of vaccination, but this was confirmed with serologic testing in only a few studies. Especially in the case of smallpox, prior immunity was likely underestimated (4). An abridged summary of exposure certainty relative to vaccination is given in Table 2. Each study in our analysis was put in 1 of the following 4 exposure-rating classifications: 1) Exposure is uncertain or ongoing without a precise record of timing or timing is followed but without a control group; 2) study indicates a known point of exposure but authors offer no explanation for their approach; 3) point of exposure can be inferred with some confidence because timing has been followed closely and/or it is likely but not explicitly stated that index patients were isolated; and 4) there is a clear point where exposure occurs before vaccination.
Table 2.
Summary of Reports Meeting Inclusion Criteria
| First Author, Year (Reference No.) | Population | Study Type | Dates | Exposure Rating a | Vaccine Type | Outcome for Vaccinated Group | Outcome for Unvaccinated Group | Time After Exposure | Effectiveness | 95% CI |
|---|---|---|---|---|---|---|---|---|---|---|
| Chickenpox/Varicella | ||||||||||
| Asano, 1977 (16) | Children; household contacts | Cohort study | 1977 (?) | 1 | Oka/Biken | 0/18 SAR | 19/19 SAR | ≤3 days | 100 | 57, 100 |
| Asano, 1982 (17) | Children; household contacts | Prospective observational | 1982 (?) | 1 | Oka/Biken (800–15,000 PFU) | 0/30 SAR | None | ≤3 days | 100 ESTb | |
| Arbeter, 1986 (18) | Children 18 months–16 years; household contacts | Double-blind RCT with placebo | 1979–1982 | 1 | Oka/Merck (4,350 PFU) | 4/13 SAR | 12/13 SAR | ≤5 days | 67 | 24, 85 |
| Salzman, 1998 (19) | Children 14 months–12 years; Household contacts | Prospective observational | 1995–1997 | 1 | Oka/Merck | 5/10 SAR | None | ≤3 days | 38 EST | |
| Watson, 2000 (10) | Children <13; shelter contacts | Prospective, observational | 1998 | 3 | Oka/Merck (Varivax) | 2/42 SAR | 1/10 SAR | ≤36 hours | 52 | −375, 95 |
| Mor, 2004 (20) | Children 12 months–13 years; household contact | Double-blind RCT with placebo | 1999–2000 | 1 | Oka/RIT (Varilrix; GlaxoSmithKline, London, United Kingdom) | 9/22 SAR | 9/20 SAR | ≤3 days | 9 | −83, 55 |
| Brotons, 2010 (21) | Individuals >1 year old; household contacts | Prospective observational | 2002–2007 | 1 | Varilrix or Varivax | 22/67 SAR | None | ≤5 days | 59 EST | |
| Gétaz, 2010 (22) | Inmates in an overcrowded Swiss prison | Prospective observational | 2009 | 4 | Not specified | 0/14 SAR | None | 2–5 days | 100 EST | |
| Wu, 2018 (11) | Grade 8 students; school contact | Prospective observational | 2013 | 1 | VarV | 0/10 SAR | 4/27 SAR | Unclear; potentially ≤19 days | 100 | −483, 100 |
| Hepatitis A | ||||||||||
| Werzberger, 1992 (12) | Children 2–16 years; community contacts | Double-blind RCT with placebo | 1991 | 3 | Formalin inactivated | 7/519 SAR | 12/518 SAR | Unclear; potentially ≤8 days | 42 | −47, 77 |
| Sagliocca, 1999 (13) | Individuals 1–40 years; household contacts | RCT | 1997 | 3 | Havrix (GlaxoSmithKline, London, United Kingdom) | 2/110 SAR | 12/102 SAR | ≤8 days | 84 | 33, 96 |
| Victor, 2007 (23) | Individuals 2–40 years; household and day-care contacts | Double-blind RCT with IG as control | 2002–2005 | 4 | Vaqta (Merck & Co.) | 25/568 SAR | None | ≤14 days | 78 EST | |
| Whelan, 2013 (24) | Any contact; household, sexual partner, cared for an infected child | Prospective observational | 2004–2012 | 2 | Not specified | 8/167 SAR | None | ≤14 days | 76 EST | |
| Parrón, 2017 (25) | Any community, household, daycare/school contact <40 years old | Retrospective cohort | 2006–2012 | 1 | Not specified | 17/2,381 SAR | 184/611 SAR | ≤14 days | 98 | 96, 99 |
| Hepatitis B | ||||||||||
| Szmuness, 1980 (26) | Homosexual men known to be at high risk for HBV | Double-blind RCT with placebo | 1978–1980 | 1 | Plasma-derived (Merck & Co.) | 1/549 SAR | 6/534 SAR | Unclear | 84 | −34, 98 |
| Beasley, 1983 (27) | Infants of e-antigen– positive/HbsAg carrier mothers | Double-blind RCT with placebo | 1981–1982 | 4 | Merck & Co. | 1/51 SAR | 74/84 SAR | 3, 4, 9 months | 98 | 84, 100 |
| 3/50 SAR | 4–7 days, 1, 6 months | 93 | 80, 98 | |||||||
| 5/58 SAR | 1, 2, 7 months | 90 | 77, 96 | |||||||
| Roumeliotou-Karayannis, 1985 (28) | Spouses of patients with acute hepatitis B | Double-blind, RCT with placebo | 1981–1982 | 3 | H-B-Vax (Merck & Co.) | 11/75 SAR | 12/71 SAR | ≤20 days | 13 | −84, 59 |
| Ip, 1989 (29) | Infants born to mothers positive for HbsAg and HbeAg | RCT with placebo | 1983–1986 | 4 | Heat-inactivated (CLB) | 11/64 SAR | 33/47 SAR | 0, 1, 2, 6 months | 76 | 57, 86 |
| Xu, 1995 (30) | Infants born to mothers positive for HbsAg and HbeAg | RCT with placebo | 1982–1984 | 4 | Plasma-derived (NIAID) | 3/27 SAR | 22/29 SAR | 0, 1, 6 months | 85 | 57, 95 |
| (BIVS) | 11/28 SAR | 48 | 14, 69 | |||||||
| Measles | ||||||||||
| Berkovich, 1963 (14) | Children with tuberculosis; hospital contacts | Prospective observational | 1961 | 3 | Edmonston strain | 3/6 SAR | None | 2–5 days | 44 EST | |
| Watson, 1963 (31) | Household contacts | Prospective observational | 1962 | 2 | Not specified | 0/3 SAR | 2/2 SAR | ≤3 days | 100 | −109, 100 |
| Ruuskanen, 1978 (32) | Children aged 1–5 years; daycare contacts | Prospective observational | 1975 | 2 | Rimevax (GlaxoSmithKline, London, United Kingdom) | 5/74 SAR | None | ≤14 days | 92 EST | |
| Sheppeard, 2009 (33) | Household, social, hospital, school contacts | Retrospective cohort | 2006 | 2 | MMR | 0/82 SAR | 13/288 SAR | ≤3 days | 100 | −125, 100 |
| Barrabeig, 2011 (34) | Children aged 6–47 months; daycare contacts | Retrospective cohort | 2006–2007 | 2 | MMR | 12/54 SAR | 13/21 SAR | ≤12 days | 64 | 35, 80 |
| Arciuolo, 2017 (15) | Household, community, and health care contacts | Prospective observational | 2013 | 2 | MMR | 2/44 SAR | 45/164 SAR | ≤3 days | 83 | 34, 96 |
| Mumps | ||||||||||
| Wharton, 1988 (35) | School contacts during countywide outbreak | Prospective observational | 1986 | 3 | MMR | 15/53 SAR | 51/125 SAR | Unclear | 31 | −12, 57 |
| Fiebelkorn, 2013 (36) | Household contacts | Prospective observational | 2009–10 | 3 | Not specified | 1/44 SAR | 8/195 SAR | 3 days | 45 | −332, 93 |
| Rabies | ||||||||||
| Bahmanyar, 1976 (37) | Individuals with potential rabies exposure | Prospective observational | 1975–1976 | 4 | PVRV | 0/45 CFP | None | ≤8 daysc (0, 3, 7, 14, 30 days) | 100 EST | |
| Anderson, 1980 (38) | Individuals with confirmed rabies exposure | Prospective observational | 1978–1979 | 4 | HDCV | 0/21 CFP | None | ≤10 daysc (0, 3, 7, 14, 28 days) | 100 EST | |
| Helmick, 1983 (39) | Individuals with confirmed rabies exposure | Prospective observational | 1980–1981 | 4 | HDCV | 0/374 CFP | None | ≤5 daysc (0, 3, 7, 14, 28 days) | 100 EST | |
| Wilde, 1995 (40) | Individuals with confirmed rabies exposure | Prospective observational | Not specified | 4 | HDCV | 0/100 CFP | None | ≤3 daysc (0, 3, 7, 14, 28 days) | 100 EST | |
| Wilde, 1996 (41) | Children who received unsuccessful postexposure prophylaxis after severe rabies exposure | Retrospective case study | 1998–1993 | 4 | PVRV or PCECV | 5/5 CFP | None | ≤66 hours (normal vaccine schedule; other deviations from WHO guidelines) | 0 EST | |
| Quiambao, 2000 (42) | Individuals with confirmed rabies exposure | Prospective trial | 1996–1999 | 4 | CPRV | 0/57 CFP | None | ≤5 daysc (0, 3, 7, 14, 28 days) | 100 EST | |
| Smallpox | ||||||||||
| Henderson, 2003 (3) | Secondary cases | Prospective observational (assumed) | 1882 | 3 | Not specified | 5/26 CFP | None | During incubation period | N/Ad | |
| McVail, 1902 (43) | Secondary cases after postexposure vaccination | Prospective observational | 1900–1902 | 3 | Not specified | 7/101 SARe | None | ≤3 days | N/A | |
| 47/101 SARe | 4–7 days | N/A | ||||||||
| 41/101 SARe | 8–11 days | N/A | ||||||||
| Hanna, 2002 (44) | Patients who received postexposure vaccination | Prospective observational | 1902–1911 | 3 | Not specified | 0/19 CFP | 60/220 CFP | During incubation period | 100 | −50, 100 |
| Sutherland, 1943 (45) | Secondary cases after postexposure vaccination | Retrospective cohort | 1920–1942 | 3 | Not specified | 1/12 CFP | 7/16 CFP | ≤3 days | 81 | −35, 97 |
| 5/12 CFP | 4–9 days | 5 | −127, 60 | |||||||
| Dixon, 1948 (46) | Household contacts | Retrospective cohort | 1946 | 3 | Not specified | 0/21 CFP | 34/132 CFP | ≤5 days | 100 | −45, 100 |
| 6/31 CFP | 6–10 days | 25 | −63, 65 | |||||||
| 1/4 CFP | ≥10 days | 3 | −443, 83 | |||||||
| Rao, 1972 (47) | Patients admitted to the Infectious Diseases Hospital, Madras, India | Retrospective cohort | 1961–1972 | 1 | Not specified | 118/502 CFP | 620/1,453 CFP | Unclear | 45 | 35, 52 |
| Douglas, 1962 (48) | Hospital contacts of a single smallpox case | Case studies | 1962 | 4 | Not specified | 6/14 CFP | None | ≤6 days | N/Ad | |
| Heiner, 1971 (49) | Household and compound contacts | Prospective observational | 1968–1970 | 1 | Not specified | 0/2 SAR | 73/92 SAR | ≤7 days | 100 | −248, 100 |
| Mack, 1972 (50) | Household contacts | Retrospective cohort | 1967 | 1 | Not specified | 12/16 SAR | 26/27 SAR | ≤10 days | 59 | −205, 94 |
| Mack, Smallpox in Europe, 1972 (51) | Secondary cases among hospital staff, hospital clientele, and general public | Retrospective cohort | 1950–1971 | 3 | Not specified | 20/70 CFP | 41/79 CFP | Unclear | 45 | 16, 64 |
| Sommer, 1974 (52) | Secondary cases among household contacts | Prospective observational | 1972 | 3 | Lyophilized; WHO potency standards | 14/1772 SAR | 4/277 SAR | ≤9 days | 45 | −65, 82 |
| Mazumder, 1975 (53) | Patients admitted to the Infectious Diseases Hospital, Calcutta, India | Prospective observational | 1973 | 3 | Not specified | 14/34 CFP | 482/901 CFP | During incubation period | 23 | −16, 49 |
Abbreviations: BIVS, Beijing Institute of Vaccine and Serum; CI, confidence interval; CFP, case fatality proportion among cases; CLB, heat-inactivated hepatitis B vaccine; CPRV, chromatographically purified Vero-cell rabies vaccine; EST, estimated efficacy; HbeAg, hepatitis B e antigen; HbsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HDCV, human diploid cell culture (rabies vaccine); MMR, measles-mumps-rubella; N/A, not applicable; NIAID, National Institute of Allergy and Infectious Diseases; PCECV, purified chick embryo cell vaccine; PVRV, purified Vero cell rabies vaccine; RCT, randomized controlled trial; SAR, secondary attack rate; VarV, varicella vaccine; WHO, World Health Organization.
a The exposure ratings are classified as follows: 1) exposure is uncertain or ongoing without a close record of timing or timing is followed but without a control group; 2) study indicates a known point of exposure no explanation for the approach is offered; 3) point of exposure can be extrapolated because timing has been followed closely and/or it is likely but not explicitly stated that index patients were isolated; and 4) there is a clear point when exposure occurs before vaccination.
b EST using accepted information about control group SAR/CFP (80% SAR for varicella, 20% for hepatitis A virus, 90% for measles, 100% for rabies, unknown for smallpox).
c Point of initiation (subsequent schedule in parentheses).
d Unable to determine a valid control to use for an efficacy estimation for evidence from Henderson et al. (3) and Douglas and Edgar (48).
e Of individuals vaccinated within incubation period, this is the fraction of secondary attacks arising within given time frames. These data show that significantly fewer cases arise among individuals vaccinated within 0–3 days of exposure compared with ≥3 days.
The vaccines included target infections with an FDA-licensed vaccine, plus dengue, hepatitis E, malaria, and tick-borne encephalitis, for which vaccines are available in areas outside of the United States. These vaccines are referred to as “eligible vaccines” in this report (Table 1). To illustrate the findings from this review, a maximum delay was calculated for each eligible vaccine with evidence, defined as the maximum timespan between exposure and vaccination with at least a 75% effectiveness according to 3 or more studies. This delay was then compared with the incubation distribution for each disease according to the US Centers for Disease Control and Prevention (Figure 1). For the smallpox vaccine, which has been studied using both secondary attack and fatality proportions as indicators, the included data concerned fatality.
Figure 1.
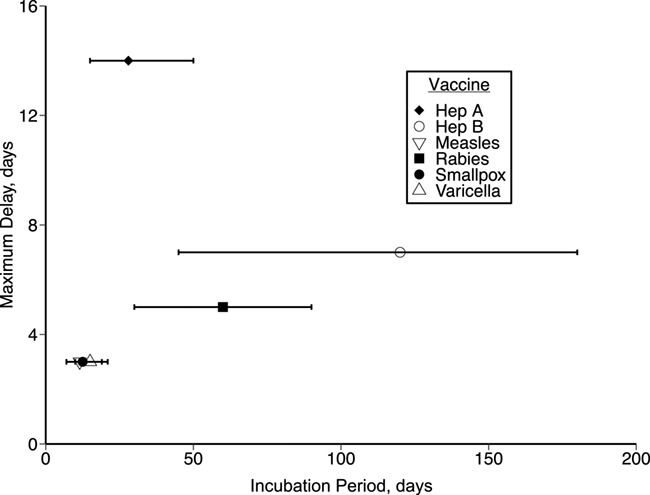
Interval for postexposure vaccination versus incubation period for all eligible infections with evidence. The horizontal axis displays the incubation distribution according to the US Centers for Disease Control and Prevention (83, 85); the vertical axis shows the maximum delay between exposure and vaccination with at least a 75% effectiveness according to 3 or more studies in this review (at that delay or longer). This effectiveness concerns secondary attack rate for all vaccines except rabies and smallpox, for which fatality is used as the measured outcome. The 2 variables have a nonsignificant correlation (ρ = 0.76; P = 0.08). Hep, hepatitis.
Where possible, primary data were re-extracted and recorded in Table 2. We elected not to conduct a meta-analysis of results, because the studies, and, in particular, the inclusion criteria and timing of vaccination, were highly heterogeneous for most vaccines, and an average effect across such studies would be difficult to interpret. Because all point estimates for all vaccines and all studies considered were positive, but not all 95% confidence intervals excluded zero, we simply classified vaccines as those for which statistical evidence of postexposure protection had been observed in at least 1 study and those for which it had not.
RESULTS
Of the 4,518 sources identified, 45 ultimately met inclusion criteria (Figure 2). We reviewed the abstracts of 434 studies after preliminary exclusion by title; most were excluded because they measured a preventive vaccine effect (n = 330 of 360 clinical trials; n = 51 of 73 observational studies). After discarding postexposure studies focused on immunoglobulin or surrogate models and adding 15 studies found through bibliographies, a total of 14 clinical trials and 31 observational studies reported data for chickenpox/varicella (10, 11, 16–22), hepatitis A (12, 13, 23–25), hepatitis B (26–30), measles (14, 15, 31–34), mumps (35, 36), rabies (37–42), and smallpox (3, 43–53). No clinical or observational studies that fit our criteria were located for 21 of the 28 eligible vaccines, although tetanus and diphtheria toxoids are effective forms of postexposure prophylaxis (1).
Figure 2.

Study selection process.
All vaccines but the mumps vaccine demonstrated statistical evidence of a positive postexposure effect in at least 1 study. Although the effects measured for smallpox were variable and the median was lower than for most other vaccines, reports in which effectiveness was stratified by delay after exposure showed a clear relation between prompt immunization and modified disease course. Vaccine effectiveness against secondary attack varied in strength across diseases, with medians of 85% (interquartile range (IQR), 28) for hepatitis A, 85% (IQR, 22) for hepatitis B, 83% (IQR, 21) for measles, 67% (IQR, 48) for varicella, 45% (IQR, 39) for smallpox, and 38% (IQR, 7) for mumps. These medians exclude the efficacies estimated using a historical control (Table 2) and incorporate only studies with an internal control population. For studies in which stratification was by vaccination delay (e.g., the Sutherland (45) and Dixon (46) smallpox studies), the included estimate refers to the shortest postexposure interval. Of the 46 studies, vaccine effectiveness against fatality was considered in 15—7 for rabies and 8 for smallpox—and median vaccine efficacies of 100% (IQR, 0) and 63% (IQR, 50) were determined for the 2 diseases, respectively.
Within these studies, vaccination timing varied widely and must be a factor when considering these results. According to data in this review, there was a nonsignificant correlation between the length of incubation and the length of delay between exposure and vaccination that allowed for at least 75% effectiveness (ρ = 0.76; P = 0.08), but it appears that a longer incubation period allows for a longer delay (Figure 1). Sample populations may also affect vaccine effectiveness: for instance, evidence for varicella and measles tends to be focused on children (7 of 9 and 4 of 6 studies, respectively), and that for hepatitis A tends to be from individuals younger than 40 years (n = 3 of 5 studies). Most data for these diseases, as well as for mumps and smallpox, derive from reactive vaccination campaigns, which often had large enough sample sizes to study. Still, their favorable characteristics sometimes came at the cost of exposure certainty, such as studies conducted in health care (15, 21, 47) and school (11, 25) settings in which researchers struggled to determine when exposure occurred. Exposure already is difficult to trace and isolate in outbreak settings, and many reactive attempts focused on disrupting an outbreak rather than investigating vaccination as postexposure prophylaxis to begin with. Conversely, percutaneous or mucosal exposure to viruses like hepatitis B and rabies is often much simpler to identify and link to infection.
DISCUSSION
Of the eligible vaccines with relevant postexposure evidence, all but mumps had compelling evidence of some form of postexposure protection. In previous reviews, authors have already investigated hepatitis A and B, smallpox, and varicella individually, and although this study is the first, to our knowledge, to incorporate findings on multiple diseases, our conclusions align with those of the targeted reports (54–58). Using historical smallpox data, Keckler et al. (54) and Henderson et al. (3). concluded that a 3–4 day interval suffices for significant postexposure protection, whereas a vaccine administered any time before symptom onset could be advantageous. Expert opinions culled using the Delphi technique corroborated this, estimating that vaccination is 93%, 90%, and 80% effective at preventing smallpox within 0–6 hours, 6–24 hours, and 1–3 days of exposure, respectively; and 80%, 80%, and 75% effective, respectively, at modifying disease among those in whom illness develops (4). In a review of varicella vaccines, researchers also determined a 3-day window but could not locate enough evidence to draw conclusions about vaccine effectiveness beyond 3 days (58). Perinatal hepatitis B vaccination was compared with placebo or no intervention in another review; authors found a relative risk of 0.28 (95% confidence interval: 0.20, 0.40), even with varying immunization schedules (56).
The findings here agree with those reported in previous reviews and indicate that even common vaccines have properties that have not been fully explored. Of course, postexposure trials are especially complicated because they involve a pool of infected individuals. The few studies that do exist were conducted in 2 main ways, largely depending on how easy it was to identify such a sample. The first approach was to record the time elapsed between vaccination and disease, then infer exposure timing and the window for effective vaccination on the basis of an incubation period estimate. This approach allows for less precise knowledge about exposure timing and thus lends itself to outbreak situations for diseases like hepatitis A, measles, mumps, varicella, and smallpox. However, authors of each study reconcile these uncertainties differently, so the study designs must be considered before comparing their results. For instance, reported events can vary in definition; for example, smallpox onset could refer to either fever (53) or rash (45, 49), which typically develops 2–3 days after the fever.
The second approach was more straightforward and involved restricting consideration to exposure that occurred in a distinct period before vaccine receipt. Examples include outbreak settings that enforced quarantine (22, 48), or diseases like hepatitis B and rabies for which transmission could be linked to specific events. Rabies is unique in that vaccines are typically administered after exposure; however, because current guidelines are successful, deviations longer than the typical 5-day delay have not been studied rigorously (59, 60). Most documented, postexposure prophylaxis failures tend not to have resulted from vaccine schedule changes but rather from insufficient wound infiltration or rabies immunoglobulin dose (41). Tetanus also spreads through cuts and punctures, although its established treatment protocol has been investigated even less systematically than that of rabies. The success of postexposure vaccination by tetanus toxoid has ruled out the option of randomized trials, and the success of preventive vaccination has reduced incidence of tetanus dramatically since the mid-1930s, eliminating most opportunity for case studies (1).
For both approaches, experimental designs create potential sources of variation across studies. Studies isolated exposure with varying levels of certainty, and although no significant pattern emerged between exposure rating and vaccine effectiveness, this rating scale indicates which of them are most likely capturing the desired effects. Other variables include vaccine types and doses; sample sizes, which range from 10 or fewer individuals (14, 19, 31, 41) to more than 2,000 (25, 52); prior immunity among participants, which was monitored in all but a few studies (25, 43, 48); and settings, whether in schools, hospitals, prisons, or households. More detailed information specific to each study and infection is reported in Web Tables 1–8 and Web Appendix 2.
In addition to these discrepancies, postexposure vaccination itself was assumed in most postexposure studies to not cause symptoms that could be mistaken for mild versions of the illness. If erroneous, this assumption could lead to an underestimation of vaccine effectiveness by mistaking vaccine-associated rash, for example, for breakthrough infection. In a study of healthy (presumably unexposed) children, 5.9% of measles, mumps, rubella, and varicella vaccine recipients and 1.9% of MMRII/VARIVAX (Merck & Co., Kenilworth, NJ) recipients experienced a very mild rash after vaccination, although both groups demonstrated greater than 90% response rates to the vaccine (61); therefore, in studies of postexposure vaccination for varicella and measles, minor adverse events may be conflated with secondary attacks and how often the vaccine works may be underestimated. For ethical and logistical reasons, some reports also lack information about important controls: individuals exposed to and untreated for rabies, for example, or individuals who received a postexposure smallpox vaccination and were protected from disease. This is the case for all but 3 historical smallpox reports (49, 50, 52); the rest include information only about people presenting with smallpox, such as the severity and outcome of their disease.
As for the vaccines without evidence of a postexposure effect, a likely explanation is that they do not have time to induce an adequate response before clinical disease manifests. The shortest incubation period among diseases with postexposure protection is 11–12 days for measles, whereas all but 4 of the 21 diseases without evidence have incubation periods of 10 days or less (Table 1). For diseases from which patients benefit from postexposure vaccination, a longer incubation period may permit a longer window for postexposure vaccination to be effective (Figure 1). Similar biological considerations already inform treatment guidelines when no trials are available. For instance, tetanus toxoid is recommended promptly after exposure, because too long a delay would allow additional tetanus neurotoxin to bind to neurons in the peripheral and central nervous systems (62). However, postexposure vaccination against tetanus produces an adequate amount of antitoxin in just 4–7 days, leaving a small window for a postexposure vaccine to outpace the natural, 10-day incubation (1). As discussed previously, the smallpox vaccine has a similar advantage over the natural infection and begins its course a few days ahead, spreading directly to regional lymph nodes and lymphoid organs (4). These results indicate that the success of postexposure prophylaxis depends on the time frames of the vaccine as it relates to disease mechanisms. It is important to note, though, that a postexposure vaccine could still supplement other treatments even if it cannot prevent or modify disease alone. Anthrax infections are 1 example and require antibiotics, because of a short incubation period and rapid onset. However, because anthrax spores can survive antibiotic prophylaxis, a vaccine should also be administered to counter long-lasting threats (1).
An exception to this generalization is the bacille Calmette-Guérin vaccine, which is the only licensed vaccine for tuberculosis and offers no known benefit to individuals with latent infection, despite that latent (asymptomatic) infection can last for years or decades (63). Better defense against tuberculosis ultimately will require a new vaccine and ideally 1 that functions before and after infection. More than a dozen candidates for priming and boosting have entered clinical trials to date, 6 of which are designed for individuals with latent or active infections—termed postexposure or therapeutic candidates, respectively (63). The M72/AS01E vaccine (GlaxoSmithKline, Brentford, United Kingdom), 1 of the most promising postexposure vaccines, recently exhibited 54.0% efficacy during a 2-year follow-up of a pool of healthy individuals infected with Mycobacterium tuberculosis (9). This finding, along with a recent bacille Calmette-Guérin revaccination trial in which 45% efficacy was reported within an uninfected population (64), has encouraged efforts toward new vaccine strategies for tuberculosis. Future solutions will have to reimagine how vaccines are implemented along the disease course, whether that involves a new way of using the bacille Calmette-Guérin vaccine or a new vaccine altogether.
In addition to these investigative tuberculosis vaccines, several others in the pipeline may have unexplored postexposure effects. Filoviruses incubate for a week or longer and thus might be promising candidates according to the findings of this review. In case reports, the recombinant vesicular stomatitis virus–Zaire Ebola virus vaccine has appeared to alter the course of Ebolavirus after several needlestick exposures in humans (65, 66), and in controlled studies, researchers have found a 50% postexposure efficacy in nonhuman primates after receiving a lethal challenge (6). Because the disease course is both faster than in humans and uniformly lethal in this nonhuman primate model, the protective effectiveness of the Ebolavirus vaccine could plausibly surpass 50% in humans (67). Preliminary research for Marburg virus indicated the recombinant vesicular stomatitis virus–Marburg virus vaccine had similar properties, demonstrating a significant effect if administered within 1 day of exposure in rhesus macaques (68). In light of the 2013–2016 Ebolavirus epidemic, filovirus countermeasures should remain a high priority, and systematic plans for gathering evidence should be set in place for the next outbreak.
An intermediate case not considered explicitly in this review is vaccination against herpes zoster disease. This disease, also called shingles, results from the reactivation of latent varicella-zoster virus infection primary, typically symptomatic, varicella disease (chickenpox). Two vaccines are licensed in the United States and have been proven effective in preventing herpes zoster (69, 70). Although technically a postexposure effect, we have not included herpes zoster vaccine in the main review because it is not an effect in preventing primary symptomatic disease but rather reactivation.
Classic vaccine efficacy trials are designed for study of the preventive effectiveness of vaccination against infection and disease. In most cases, if there were a postexposure effect of vaccination, it would have little effect on the outcome of such trials, because a small proportion of trial participants would be infected at the time of vaccination. Two classes of exceptions are worthy of note. First is vaccines against bacteria that colonize the respiratory or digestive tract asymptomatically and for which disease is a comparatively rare complication of colonization. For vaccines against such bacteria, the limited evidence available is that vaccination does not terminate the carriage state but rather reduces the acquisition of carriage and also the probability of disease, given carriage (71). If this is the case, then the postexposure effect should be modest for these vaccines and not complicate estimates of effectiveness. On the other hand, a setting where postexposure effectiveness could have greater consequences for the interpretation of vaccine trials is in ring-vaccination trials of vaccines against acute viral diseases, such as the Ebola Ça Suffit! (in English, “Ebola that’s enough!”) trial in which the recombinant vesicular stomatitis virus–Zaire Ebola virus vaccine was evaluated against Ebola virus disease in Guinea (72). In such a trial, by design, vaccination occurs close to the time of likely exposure to infection, and cases occurring within 1 incubation period of vaccination (plus 1 week for vaccine immunity to ramp up) were excluded from analysis as unpreventable by vaccination. On one hand, it is possible that postexposure effects, such as those observed in nonhuman primates with this vaccine, mean that some cases before that window could be preventable by vaccination, and it would be interesting to analyze the data from before the window in the main analysis to see if there is evidence of such an effect. On the other hand, because incubation periods are variable, it is possible that a window designed to exclude any individuals infected before vaccination would do so imperfectly, leading to some inclusion of a postexposure effect in the main effect estimate. If this design is used again, it would be valuable to quantify the likely impact of postexposure effectiveness on estimates obtained from the trial.
With the exception of tuberculosis, most postexposure benefits discussed so far arise as adverse effects of successful preventive vaccines. However, active therapeutic immunization has recently become a focus for chronic, mainly noncommunicable diseases. Many of these experimental vaccines induce antibody production, but the goal of their use is altering a disease that has already begun. Some vaccines treat drug abuse by binding to addictive substances like nicotine and cocaine (73), and others block tumor necrosis factor-α, an inflammatory cytokine linked to Crohn disease, rheumatoid arthritis, and psoriasis (74). Several active therapy candidates for Alzheimer disease have entered human clinical trials since 2000, mostly to target amyloid-β plaques that are thought to be causative agents (75). However, despite promising preclinical results, no significant cognitive benefit has been observed to date (76), to our knowledge. A similar narrative characterizes the efforts toward therapeutic HIV-1 vaccines: early optimism because of a slow and relatively well-understood disease progression, followed by decades of research and few positive clinical outcomes (77).
Other therapeutic vaccine candidates induce T cells rather than antibodies, an approach well suited to treating cancer. In theory, the paradigm mirrors that of classical viral vaccines in that tumor-associated antigens are used to activate T cells, which differentiate and proliferate to target the unwanted tumor cells (1). However, despite several promising phase III trials (78, 79), in an objective review of cancer vaccine trials, the authors found a response rate of less than 4% (80). The FDA has only approved 1 cancer vaccine, Sipuleucel-T (Dendreon Pharmaceuticals, Seal Beach, CA), which targets metastatic prostate cancer and prolongs median survival by 4.1 months (81). Still, the same phase III trial that led to its licensure presented no significant effect on other important disease factors, namely, time to disease progression, tumor regression, and long-term immunity. Interestingly, a different licensed vaccine may have the ability to eradicate other malignant tumors, specifically squamous cell carcinomas. In a recent case report, the 9-valent human papillomavirus vaccine (Gardisil-9; Merck & Co., Kenilworth, New Jersey) resolved all of a woman’s tumors within 1 year of her first injection (82). Although the human papillomavirus vaccine has already been linked to preventing cervical cancer and other diseases, its therapeutic properties remain unclear (1).
Therapeutic vaccination represents a promising frontier for disease treatment but also has implications for how we consider vaccines as a tool for prevention. As evidenced by this report, postexposure effectiveness has not been fully explored even for common vaccines, and there are several scenarios in which they are important, including responding to unpredictable health emergencies, designing new treatments, and interpreting vaccine trials. Especially in outbreak settings, attributing all outcomes to preventive effects could lead to an overestimation of a vaccine’s preventive effectiveness and underappreciation of its postexposure effectiveness. Therefore, postexposure effects not only concern innovative treatments for exposed or infected individuals but could also improve how we anticipate and understand the impact of any vaccine. This review represents the current body of evidence for vaccines that are already available, and our findings indicate there is still much to learn about postexposure vaccination.
Supplementary Material
ACKNOWLEDGMENTS
Author affiliations: Dartmouth College Department of Physics and Astronomy, Hanover, New Hampshire (Tara Gallagher); and Department of Epidemiology, Harvard School of Public Health, Boston, Massachusetts (Marc Lipsitch).
This project was supported by the National Institute of General Medical Sciences (grant U54GM088558).
We thank Dr. Mark Slifka for helpful discussions before this project began.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of General Medical Sciences or the National Institutes of Health.
Conflict of interest: M.L. discloses consulting or honoraria from Merck, Pfizer, Antigen Discovery, and Affinivax, and grant funding through his institution from Pfizer. T.E.G. reports no conflicts.
References
- 1. Plotkin S, Orenstein W, Offit P, et al. Plotkin’s Vaccines. 7th ed. Philadelphia, PA: Elsevier; 2017. [Google Scholar]
- 2. Sela M, Hilleman M. Therapeutic vaccines: realities of today and hopes for tomorrow. Proc Natl Acad Sci USA. 2004;10(suppl 2):14559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Henderson D, Inglesby T, O'Toole T, et al. Can postexposure vaccination against smallpox succeed? Clin Infect Dis. 2003;36(5):622–629. [DOI] [PubMed] [Google Scholar]
- 4. Massoudi M, Barker L, Schwarz B. Effectiveness of postexposure vaccination for the prevention of smallpox: results of a Delphi analysis. J Infect Dis. 2003;188(7):973–976. [DOI] [PubMed] [Google Scholar]
- 5. Melamed S, Israely T, Paran N. Challenges and achievements in prevention and treatment of smallpox. Vaccines (Basel). 2018;6(1):8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Feldmann H, Jones S, Daddario-DiCaprio K, et al. Effective post-exposure treatment of Ebola infection. PLoS Pathog. 2007;3(1):54–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Tantawichien T, Jaijaroensup W, Khawplod P, et al. Failure of multiple-site intradermal post-exposure rabies vaccination in patients with human immunodeficiency virus with low CD4+ T lymphocyte counts. Clin Infect Dis. 2001;33(10):e122–e124. [DOI] [PubMed] [Google Scholar]
- 8. Ziv E, Daley C, Blower S. Potential public health impact of new tuberculosis vaccines. Emerg Infect Dis. 2004;10(9):1529–1535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Van Der Meeren O, Hatherill M, Nduba V, et al. Phase 2b controlled trial of M72/AS01E vaccine to prevent tuberculosis. N Engl J Med. 2018;379(17):1621–1634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Watson B, Seward J, Yang A, et al. Postexposure effectiveness of varicella vaccine. Pediatrics. 2000;105(1):84–88. [DOI] [PubMed] [Google Scholar]
- 11. Wu QS, Liu JY, Wang X, et al. Effectiveness of varicella vaccine as post-exposure prophylaxis during a varicella outbreak in Shanghai, China. Int J Infect Dis. 2018;66:51–55. [DOI] [PubMed] [Google Scholar]
- 12. Werzberger A, Mensch B, Kuter B, et al. A controlled trial of a formalin-inactivated hepatitis A vaccine in healthy children. N Engl J Med. 1992;327(7):453–457. [DOI] [PubMed] [Google Scholar]
- 13. Sagliocca L, Amoroso P, Stroffolini T, et al. Efficacy of hepatitis A vaccine in prevention of secondary hepatitis A infection: a randomised trial. Lancet. 1999;353(9159):1136–1139. [DOI] [PubMed] [Google Scholar]
- 14. Berkovich S, Starr S. Use of live-measles-virus vaccine to abort an expected outbreak of measles within a closed population. N Engl J Med. 1963;269:75–77. [DOI] [PubMed] [Google Scholar]
- 15. Arciuolo RJ, Jablonski RR, Zucker JR, et al. Effectiveness of measles vaccination and immune globulin post-exposure prophylaxis in an outbreak setting—New York City, 2013. Clin Infect Dis. 2017;65(11):1843–1847. [DOI] [PubMed] [Google Scholar]
- 16. Asano Y, Nakayama H, Yazaki T, et al. Protection against varicella in family contacts by immediate inoculation with live varicella vaccine. Pediatrics. 1977;59(1):3–7. [PubMed] [Google Scholar]
- 17. Asano Y, Hirose S, Iwayama S, et al. Protective effect of immediate inoculation of a live varicella vaccine in household contacts in relation to the viral dose and interval between exposure and vaccination. Biken J. 1982;25(1):43–45. [PubMed] [Google Scholar]
- 18. Arbeter A, Starr S, Plotkin S. Varicella vaccine studies in healthy children and adults. Pediatrics. 1986;78(4):742–747. [PubMed] [Google Scholar]
- 19. Salzman M, Garcia C. Postexposure varicella vaccination in siblings of children with active varicella. Pediatr Infect Dis J. 1998;17(3):256–257. [DOI] [PubMed] [Google Scholar]
- 20. Mor M, Harel L, Kahan E, et al. Efficacy of postexposure immunization with live attenuated varicella vaccine in the household setting—a pilot study. Vaccine. 2004;23(3):325–328. [DOI] [PubMed] [Google Scholar]
- 21. Brotons M, Campins M, Méndez L, et al. Effectiveness of varicella vaccines as postexposure prophylaxis. Pediatr Infect Dis J. 2010;29(1):10–13. [DOI] [PubMed] [Google Scholar]
- 22. Gétaz L, Siegrist CA, Stoll B, et al. Chickenpox in a Swiss prison: susceptibility, post-exposure vaccination and control measures. Scand J Infect Dis. 2010;43(11–12):936–940. [DOI] [PubMed] [Google Scholar]
- 23. Victor J, Monto A, Surdina T, et al. Hepatitis A vaccine versus immune globulin for postexposure prophylaxis. N Engl J Med. 2007;357(17):1685–1694. [DOI] [PubMed] [Google Scholar]
- 24. Whelan J, Sonder G, Bovée L, et al. Evaluation of hepatitis A vaccine in post-exposure prophylaxis, the Netherlands, 2004–2012. PLoS One. 2013;8(10):e78914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Parrón I, Planas C, Godoy P, et al. Effectiveness of hepatitis A vaccination as post-exposure prophylaxis. Hum Vaccin Immunother. 2017;13(2):423–427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Szmuness W, Stevens C, Harley E, et al. Hepatitis B vaccine: demonstration of efficacy in a controlled clinical trial in a high-risk population in the United States. N Engl J Med. 1980;303(15):833–841. [DOI] [PubMed] [Google Scholar]
- 27. Beasley RP, Lee G, Roan CH, et al. Prevention of perinatally transmitted hepatitis B virus infections with hepatitis B immune globulin and hepatitis B vaccine. Lancet. 1983;322 (8359):1099–1102. [DOI] [PubMed] [Google Scholar]
- 28. Roumeliotou-Karayannis A, Papaevangelou G, Tassapoulos N, et al. Post-exposure active immunoprophylaxis of spouses of acute viral hepatitis B patients. Vaccine. 1985;3(1):31–34. [DOI] [PubMed] [Google Scholar]
- 29. Ip HM, Lelie PN, Wong VC, et al. Prevention of hepatitis B virus carrier state in infants according to maternal serum levels of HBV DNA. Lancet. 1989;1(8635):406–410. [DOI] [PubMed] [Google Scholar]
- 30. Xu ZY, Duan SC, Margolis HS, et al. Long-term efficacy of active postexposure immunization of infants for prevention of hepatitis B virus infection. J Infect Dis. 1995;171(1):54–60. [DOI] [PubMed] [Google Scholar]
- 31. Watson GI. Protection after exposure to measles by attenuated vaccine without gamma-globulin. Br Med J. 1963;1(5334):860–861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Ruuskanen O, Salmi TT, Halonen P. Measles vaccination after exposure to natural measles. J Pediatr. 1978;93(1):43–46. [DOI] [PubMed] [Google Scholar]
- 33. Sheppeard V, Forssman B, Ferson M, et al. The effectiveness of prophylaxis for measles contacts in NSW. N S W Public Health Bull. 2009;20(5–6):81–85. [DOI] [PubMed] [Google Scholar]
- 34. Barrabeig I, Rovira A, Rius C, et al. Effectiveness of measles vaccination for control of exposed children. Pediatr Infect Dis J. 2011;30(1):78–80. [DOI] [PubMed] [Google Scholar]
- 35. Wharton M, Cochi S, Hutcheson R, et al. A large outbreak of mumps in the postvaccine era. J Infect Dis. 1988;158(6):1253–1260. [DOI] [PubMed] [Google Scholar]
- 36. Fiebelkorn A, Lawler J, Curns A, et al. Mumps postexposure prophylaxis with a third dose of measles-mumps-rubella vaccine, Orange County, New York, USA. Emerg Infect Dis. 2013;19(9):1411–1417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Bahmanyar M, Fayaz A, Nour-Salehi S, et al. Successful protection of humans exposed to rabies infection. Postexposure treatment with the new human diploid cell rabies vaccine and antirabies serum. JAMA. 1976;236(24):2751–2754. [PubMed] [Google Scholar]
- 38. Anderson L, Sikes R, Langkop C, et al. Postexposure trial of a human diploid cell strain rabies vaccine. J Infect Dis. 1980;142(2):133–138. [DOI] [PubMed] [Google Scholar]
- 39. Helmick CG. The epidemiology of human rabies postexposure prophylaxis, 1980–1981. JAMA. 1983;250(15):1990–1996. [PubMed] [Google Scholar]
- 40. Wilde H, Glueck R, Khawplod P, et al. Efficacy study of a new albumin-free human diploid cell rabies vaccine (Lyssavac-HDC, Berna) in 100 severely rabies-exposed Thai patients. Vaccine. 1995;13(6):593–596. [DOI] [PubMed] [Google Scholar]
- 41. Wilde H, Sirikawin S, Sabcharoen A, et al. Failure of postexposure treatment of rabies in children. Clin Infect Dis. 1996;22(2):228–232. [DOI] [PubMed] [Google Scholar]
- 42. Quiambao B, Lang J, Vital S, et al. Immunogenicity and effectiveness of post-exposure rabies prophylaxis with a new chromatographically purified Vero-cell rabies vaccine (CPRV): a two-stage randomised clinical trial in the Philippines. Acta Trop. 2000;75(1):39–52. [DOI] [PubMed] [Google Scholar]
- 43. McVail J. Small-pox in Glasgow, 1900-02. Br Med J. 1902;July 5:40–July 5:43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Hanna W, Baxby D. Studies in smallpox and vaccination. 1913. Rev Med Virol. 2002;12(4):201–209. [DOI] [PubMed] [Google Scholar]
- 45. Sutherland I. Some aspects of the epidemiology of smallpox in Scotland in 1942. Proc R Soc Med. 1943;36(5):227–236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Dixon C. Smallpox in Tripolitania, 1946: an epidemiological and clinical study of 500 cases, including trials of penicillin treatment. J Hyg (Lond). 1948;46(4):351–377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Rao A. Smallpox. Bombay, India: Kothari Book Depot; 1972. [Google Scholar]
- 48. Douglas J, Edgar W. Smallpox in Bradford, 1962. Br Med J. 1962;1(5278):612–614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Heiner GG, Fatima N, McCrumb FR. A study of Intrafamilial transmission of smallpox. Am J Epidemiol. 1971;94(4):316–326. [DOI] [PubMed] [Google Scholar]
- 50. Mack T, Thomas D, Asghar A, et al. Epidemiology of smallpox in West Pakistan: I. Acquired immunity and the distribution of disease. Am J Epidemiol. 1972;95(2):157–168. [DOI] [PubMed] [Google Scholar]
- 51. Mack T. Smallpox in Europe, 1950–1971. J Infect Dis. 1972;125(2):161–169. [DOI] [PubMed] [Google Scholar]
- 52. Sommer A. The 1972 smallpox outbreak in Kuhlna municipality, Bangladesh: II. Effectiveness of surveillance and containment in urban epidemic control. Am J Epidemiol. 1974;99(4):303–313. [DOI] [PubMed] [Google Scholar]
- 53. Mazumder D, De S, Mitra A, et al. Clinical observations on smallpox: a study of 1233 patients admitted to the infectious diseases hospital, Calcutta, during 1973. Bull World Health Organ. 1975;52(3):301–306. [PMC free article] [PubMed] [Google Scholar]
- 54. Keckler MS, Reynolds MG, Damon IK, et al. The effects of post-exposure smallpox vaccination on clinical disease presentation: addressing the data gaps between historical epidemiology and modern surrogate model data. Vaccine. 2013;31(45):5192–5201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Nishiura H, Eichner M. Interpreting the epidemiology of postexposure vaccination against smallpox. Int J Environ Health. 2008;211(1–2):219–226. [DOI] [PubMed] [Google Scholar]
- 56. Lee C, Gong Y, Brok J, et al. Effect of hepatitis B immunisation in newborn infants of mothers positive for hepatitis B surface antigen: systematic review and meta-analysis. BMJ. 2006;332(7537):328–336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Link-Gelles R, Hofmeister MG, Nelson NP. Use of hepatitis a vaccine for post-exposure prophylaxis in individuals over 40 years of age: a systematic review of published studies and recommendations for vaccine use. Vaccine. 2018;36(20):2745–2750. [DOI] [PubMed] [Google Scholar]
- 58. Macartney K, Heywood A, McIntyre P. Vaccines for post-exposure prophylaxis against varicella (chickenpox) in children and adults. Cochrane Database Syst Rev. 2014;6:CD001833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Pandey P, Shlim D, Cave W, et al. Risk of possible exposure to rabies among tourists and foreign residents in Nepal. J Travel Med. 2002;9(3):127–131. [DOI] [PubMed] [Google Scholar]
- 60. Rupprecht C, Gibbons R. Prophylaxis against rabies. N Engl J Med. 2004;351:2626–2635. [DOI] [PubMed] [Google Scholar]
- 61. Shinefield H, Black S, Digilio L, et al. Evaluation of a quadrivalent measles, mumps, rubella and varicella vaccine in healthy children. Pediatr Infect Dis J. 2005;24(8):665–669. [DOI] [PubMed] [Google Scholar]
- 62. Collins S, White J, Ramsay M, et al. The importance of tetanus risk assessment during wound management. IDCases. 2015;2(1):3–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Hatherill M, Scriba TJ, Udwadia ZF, et al. BCG and new preventive tuberculosis vaccines: implications for healthcare workers. Clin Infect Dis. 2016;62(3):262–267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Nemes E, Geldenhuys H, Rozot V, et al. Prevention of M. tuberculosis infection with H4:IC31 vaccine or BCG revaccination. N Engl J Med. 2018;379(2):138–149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Wong G, Mendoza EJ, Plummer FA, et al. From bench to almost bedside: the long road to a licensed Ebola virus vaccine. Expert Opin Biol Ther. 2018;18(2):159–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Lai L, Davey R, Beck A, et al. Emergency postexposure vaccination with vesicular stomatitis virus–vectored Ebola vaccine after needlestick. JAMA. 2015;313(12):1249–1255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Fischer W, Vetter P, Bausch D, et al. Ebola virus disease: an update on post-exposure prophylaxis. Lancet. 2018;18(6):e183–e192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Cross RW, Mire CE, Feldmann H, et al. Post-exposure treatments for Ebola and Marburg virus infections. Nat Rev Drug Discov. 2018;17(6):413–434. [DOI] [PubMed] [Google Scholar]
- 69. Schmader KE, Levin MJ, Gnann JW, et al. Efficacy, safety, and tolerability of herpes zoster vaccine in persons aged 50–59 years. Clin Infec Dis. 2012;54(7):922–928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Cunningham AL, Lal H, Kovac M, et al. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older. N Engl J Med. 2016;375(11):1019–1032. [DOI] [PubMed] [Google Scholar]
- 71. Rinta-Kokko H, Dagan R, Givon-Lavi N, et al. Estimation of vaccine efficacy against acquisition of pneumococcal carriage. Vaccine. 2009;27(29):3831–3837. [DOI] [PubMed] [Google Scholar]
- 72. Henao-Restrepo AM, Camacho A, Longini IM, et al. Efficacy and effectiveness of an rVSV-vectored vaccine in preventing Ebola virus disease: final results from the Guinea ring vaccination, open-label, cluster-randomised trial (Ebola Ça Suffit!). Lancet. 2017;389(10068):505–518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Shen X, Orson FM, Kosten TR. Vaccines for drug abuse. Clin Pharmacol Ther. 2012;91(1):60–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Bachmann MF, Dyer MR. Therapeutic vaccination for chronic diseases: a new class of drugs in sight. Nat Rev Drug Discov. 2004;3(1):81–88. [DOI] [PubMed] [Google Scholar]
- 75. Lambracht-Washington D, Rosenberg RN. Advances in the development of vaccines for Alzheimer's disease. Discov Med. 2013;15(84):319–326. [PMC free article] [PubMed] [Google Scholar]
- 76. Herline K, Drummond E, Wisniewski T. Recent advancements toward therapeutic vaccines against Alzheimer’s disease. Expert Rev Vaccines. 2018;17(8):707–721. [DOI] [PubMed] [Google Scholar]
- 77. Gray GE, Laher F, Lazarus E, et al. Approaches to preventative and therapeutic HIV vaccines. Curr Opin Virol. 2016;17:104–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Schuster S, Neelapu S, Gause B, et al. Idiotype vaccine therapy (BiovaxID) in follicular lymphoma in first complete remission: phase III clinical trial results. J Clin Oncol. 2009;27(suppl 18):2.19047306 [Google Scholar]
- 79. Schwartzentruber D, Lawson D, Richards J, et al. A phase III multi-institutional randomized study of immunization with the gp100: 209–217(210M) peptide followed by high-dose IL-2 compared with high-dose IL-2 alone in patients with metastatic melanoma. J Clin Oncol. 2009;27(suppl):463S. [Google Scholar]
- 80. Klebanoff CA, Acquavella N, Yu Z, et al. Therapeutic cancer vaccines: are we there yet? Immunol Rev. 2011;239(1):27–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Cheever MA, Higano CS. Provenge (Sipuleucel-T) in prostate cancer: the first FDA-approved therapeutic cancer vaccine. Clin Cancer Res. 2011;17(11):3520–3526. [DOI] [PubMed] [Google Scholar]
- 82. Nichols AJ, Gonzalez A, Clark ES, et al. Combined systemic and intratumoral administration of human papillomavirus vaccine to treat multiple cutaneous basaloid squamous cell carcinomas. JAMA Dermatol. 2018;154(8):927–930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. US Centers for Disease Control and Prevention Diseases & conditions. https://www.cdc.gov/DiseasesConditions/. Accessed October 4, 2019.
- 84. Hamborsky J, Kroger A, Wolfe C, eds. Epidemiology and Prevention of Vaccine-Preventable Diseases. 13th ed. Washington, DC: Public Health Foundation; 2015. [Google Scholar]
- 85. US Centers for Disease Control and Prevention Diseases directory. https://wwwnc.cdc.gov/travel/diseases. Accessed October 4, 2019.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.