

Abstract
Background
Parenting issues can affect physicians' choice of specialty or subspecialty, as well as their selection of individual training programs, because of the distinctive challenges facing residents and fellows with children. Specific information about how residents perceive these challenges is limited.
Objective
We sought to better understand the challenges associated with parenting during residency and fellowship training in order to inform policy and research.
Methods
In 2017, a voluntary online questionnaire was distributed to all 2214 Partners HealthCare graduate medical education trainees across 285 training programs. The survey queried attitudes of and about trainees with children and assessed needs and experiences related to parental leave, lactation, and childcare. Responses were compared between subgroups, including gender, surgical versus nonsurgical specialty, parental status, and whether the respondent was planning to become a parent.
Results
A total of 578 trainees (26%) responded to the questionnaire. Of these, 195 (34%) became parents during training. An additional 298 (52%) planned to become parents during training. Respondents overwhelmingly agreed that their institution should support trainees with children (95%) and that doing so is important for trainee wellness (98%). However, 25% felt that trainees with children burden trainees without children. Childcare access, affordability, and availability for sufficient hours were identified as key challenges, along with issues related to parental leave, lactation facilities, and effect on peers.
Conclusions
This survey highlights trainees' perspectives about parenting during their clinical training, signaling parental leave, lactation facilities, and childcare access and affordability as particular challenges and potential targets for future interventions.
What was known and gap
Residents and fellows with children face unique challenges that can affect a physician's choice in specialty or training program, but information about how these trainees perceive the challenges they face is limited.
What is new
A voluntary questionnaire that queried attitudes of and about trainees with children and assessed needs and experiences related to parental leave.
Limitations
The survey was conducted in one multi-hospital healthcare system, limiting generalizability, and was not tested for validity evidence.
Bottom line
Parental leave, lactation facilities, and childcare access and affordability are important challenges faced by trainees with children and potential targets for future interventions.
Introduction
Many physicians are or become parents during their clinical training, with important implications for work-life balance, burnout, and career development.1,2 The proportion of graduate medical education (GME) trainees who are parents is not tracked, but an Association of American Medical Colleges survey indicated that 8% of graduating medical students have children. Furthermore, the age (18% > 29 years) and marital status (25% partnered) of these medical students implied that considerably more of them will become parents during residency or fellowship.3 Experts and prior research have reported that stressors facing trainees with children deserve greater attention from GME leaders.4–6
Parenting-related considerations can affect specialty and program choice as well as the training experience, including the possibility of extending the duration of training.7–10 However, trainee perceptions about parenting challenges and resources are not completely understood. Most studies examining trainees with children focus on 1 specialty9,11–16 or examine 1 aspect of parenting—parental leave,17–20 childcare,1 or lactation.21 Information about the needs of trainees with children across specialties is needed to inform institutional and national policies.
The aims of this study were to better understand trainee attitudes, plans, and experiences relating to parenting overall, and as related to gender, specialty, and other individual characteristics in greater detail than previously available.
Methods
We conducted a needs assessment based on trainee perceptions and experiences of parental leave, lactation, and childcare across all specialties and postgraduate years (PGYs) of training at 6 Partners HealthCare system hospitals, including Brigham & Women's Hospital (BWH) and Massachusetts General Hospital (MGH). At the time of the survey, these institutions provided childbearing mothers with 8 weeks of paid leave, but paid leave for nonchildbearing parents was at each program's discretion.
The survey tool was developed by the majority of authors (K.M., T.S.C.N., A.G.B., M.A.K., S.E.S., D.F.W.) and included 18 to 67 survey items depending on gender, parenting experience and plans, and student loan status of the respondent (provided as online supplemental material). Thirty-four questions were multiple choice, 27 were Likert-type scale, 2 were numerical fill-ins, and 4 were open-ended.
The survey was piloted with 25 trainees, and minor changes were made to the wording of questions to improve clarity based on feedback. The survey took an average of 5 minutes to complete. No further testing for validity was done. Trainees were contacted via e-mail on March 15, 2017, seeking anonymous, voluntary responses to an online survey without a participation incentive (LimeSurvey GmbH, Hamburg, Germany). All program directors were contacted to remind their trainees about the survey 4 weeks later. The survey closed after 8 weeks.
Descriptive statistics were determined with RStudio (RStudio Inc, Boston, MA) and Microsoft Excel (Microsoft Corp, Redmond, WA). Respondent characteristics used for subsequent preplanned analysis include gender (male, female, or other); trainee type (resident or fellow); specialty (surgical [general surgery, neurological surgery, obstetrics and gynecology, oral and maxillofacial surgery, orthopedic surgery, plastic surgery, thoracic surgery, and urology] or nonsurgical [all others]); whether trainees were parents (yes, no); whether trainees were planning to have children (yes, no, or not sure); and relationship status (single, married, in a long-term relationship, or divorced). MATLAB and Prism were used for further statistical analysis: the Mann-Whitney U test was used for parental leave and Likert-scale comparisons, and Pearson's chi-square test was used for the remaining comparisons. P values less than .05 were considered statistically significant.
Respondents were asked to indicate the amount paid in posttax dollars for monthly childcare (< $1,500: $750; $1,500–$3,000: $2,250; $3,000–$4,500: $3,750; > $4,500: $5,250). We then calculated this cost as a percentage of pretax salary using institutional salary metrics (provided as online supplemental material).
Operating hours for daycare centers within 3 miles of BWH and MGH were determined in August 2018 via website, e-mail, or telephone.
The Partners Institutional Review Board deemed this study exempt.
Results
A total of 578 of 2214 eligible subjects (26%) responded. Respondents were similar to the survey population with regard to PGY, specialty, age, institution, and trainee type, although women were moderately overrepresented (Table). All training years and specialties were represented (provided as online supplemental material).
Table.
Respondent Characteristics and Family Status—General Demographics
| Variable | Total Respondents, No. (%) | All GME Trainees, No. (%) |
| Gender (n = 578) | ||
| Female | 352 (61) | 990 (45) |
| Male | 226 (39) | 1224 (55) |
| Age, y, (n = 517) | ||
| 25–29 | 155 (30) | 642 (29) |
| 30–34 | 282 (55) | 1218 (55) |
| ≥ 35 | 80 (16) | 332 (15) |
| Institution (n = 514) | ||
| BWH | 199 (39) | 952 (43) |
| MGH | 206 (40) | 1173 (53) |
| Combined BWH/MGH program | 94 (18) | N/Aa |
| Other Partners hospital sites | 15 (3) | 73 (3) |
| Trainee type (n = 517) | ||
| Resident | 335 (65) | 1483 (67) |
| Fellow | 182 (35) | 708 (32) |
| Training year (n = 517) | ||
| PGY-1–2 | 195 (38) | 1483 (67) |
| PGY-3–5 | 232 (45) | 1114 (50) |
| PGY-6+ | 90 (17) | 297 (13) |
| Surgical versus nonsurgical specialties (n = 497) | ||
| Surgical | 83 (17) | 483 (22) |
| Nonsurgical | 414 (83) | 1731 (78) |
| Relationship status (n = 512) | ||
| Single | 66 (13) | |
| Married | 348 (70) | |
| In a long-term relationship | 98 (19) | |
| Trainees with children (n = 578) | ||
| No | 383 (66) | |
| Yes | 195 (34) |
Most respondents were partnered; one-third had children (Table). Most trainees with children became parents during training and had 1 child under 2 years old. Twenty-seven percent (158 of 576) of respondents did not plan to have children during training, and cited work hours, focus on career, financial constraints, and childcare costs as factors (Table; more information provided as online supplemental material).
General Attitudes
Trainees overwhelmingly agreed that their institutions should support trainees with children (95%, 546 of 574) and considered it important for trainee wellness (98%, 561 of 574). Trainees with children, partnered respondents, and women were more likely to agree; respondents not planning to have children during training agreed less (provided as online supplemental material). Twenty-five percent (141 of 574) of respondents indicated that trainees with children burden trainees without children. Surgical trainees were more likely to agree than nonsurgical trainees (mean ± SE/mean ranks = 2.9 ± 0.2/285.9 versus 2.5 ± 0.05/243.6; U = 9388; P = .038), as were nonparents (mean ± SE/mean ranks = 2.7 ± 0.06/303.8 versus 2.3 ± 0.08/255.3 for others; U = 30 554; P < .001).
Parental Leave
Approximately one-third of respondents knew how to access parental leave policies for their program (37%, 200 of 537) or institution (32%, 170 of 537). Women took significantly more parental leave (5.5 weeks, SD = 4.3) than men (1.9 weeks; SD = 1.9; P < .001; Figure 1). Female surgical trainees took significantly less leave (6.6 weeks, SD = 2.9) than female nonsurgical trainees (8.9 weeks; SD = 2.9; P = .040). There was no significant difference in overall satisfaction with parental leave by gender, resident versus fellow, or surgical versus nonsurgical specialties (provided as online supplemental material).
Figure 1.
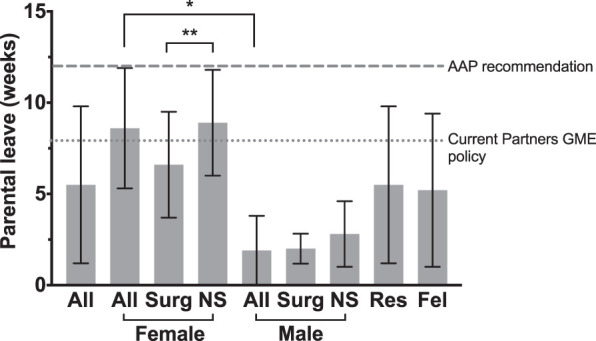
Parental Leave Taken by Trainees (n = 159)
Abbreviations: GME, graduate medical education; Surg, surgical specialties; NS, nonsurgical specialties; Res, resident; Fel, fellow.
Note: For reference, lines delineating the 12 weeks' leave (as advocated by the American Academy of Pediatrics [AAP], dashed line) and 8 weeks (paid parental leave allowed by Partners HealthCare as of September 2018, dotted line) are indicated (*P < .001, **P = .040).
Lactation
Eighty-one percent (140 of 172) of female trainees intending to have a child during training planned to breastfeed, and 85% (81 of 95) of those who had a child during training did breastfeed. Most breastfeeding trainees felt supported (provided as online supplemental material). Additional responses highlighted the potential for improvement in lactation facilities (Figure 2).
Figure 2.
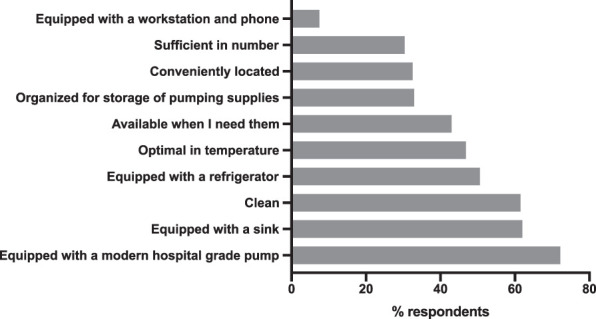
Lactation Room Amenities (n = 79)
Childcare
Sixty-three percent (117 of 187) of respondents reported difficulty in arranging childcare and relied on multiple sources for childcare (provided as online supplemental material). Approximately 10% (18 of 190) reported using a daycare facility affiliated with their institution, with nonuse most often attributed to a long waitlist and convenience. Most desired extended and weekend daycare hours, which were not available locally (provided as online supplemental material).
The median proportion of pretax salary used for childcare in PGY-1 and PGY-2 was 43% (interquartile range 41%–71%) and decreased modestly with increasing PGY (Figure 3). Perceptions of financial strain were greater among trainees with children, despite reported higher household income and comparable student loan debt (provided as online supplemental material).
Figure 3.
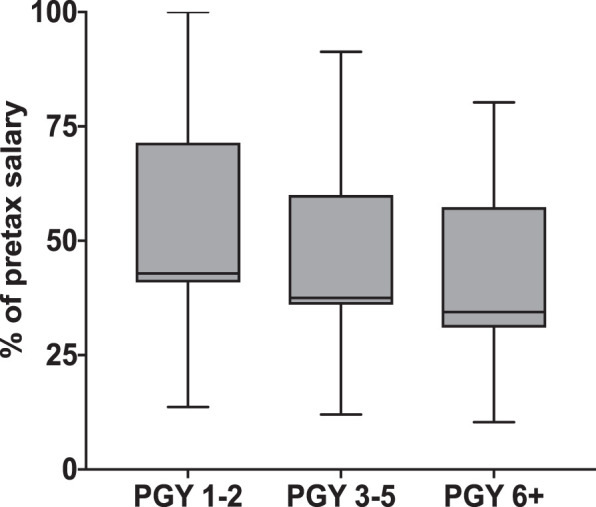
Cost of Childcare Relative to PGY Salary in Boston (n = 186)a
a Displayed as median with interquartile range.
Abbreviation: PGY, postgraduate year.
Discussion
The respondents in this study overwhelmingly agreed that teaching institutions should support trainees with children. The type of support needed can be informed by our findings: (1) a sizable minority feel trainees with children burden other trainees; (2) awareness of parental leave policies is limited; (3) lactation facilities are considered suboptimal; and, particularly, (4) childcare cost and access are seen as formidable obstacles.
Concern about trainees with children burdening other trainees was identified by Rangel et al9 who found that 60% of survey participants reported a negative stigma associated with being pregnant as a surgical resident. This may reflect that parental leave results in short staffing, with the remaining residents carrying an increased clinical load. It may also relate to a perceived stigmatization of pregnant trainees and trainees with children reported in surgery, and we found that female surgical trainees took less parental leave than female nonsurgical trainees. Institutions can address this by ensuring adequate coverage for trainees on leave.
GME leave policies vary widely across and within institutions.4,17,19 Our finding that most trainees were unaware of their parental leave policy mirrors prior research15 and underscores the need to more actively communicate these policies to facilitate family and career planning. With regard to lactation, these results indicate that trainees with children are strongly inclined toward breastfeeding and that specific features of lactation facilities beyond availability are important, especially when short parental leave, unpredictable pumping schedules, and long work hours make lactation challenging.17,21,22
Finally, this study highlights childcare cost as a critical issue as most respondents spent more than one-third of their pretax salary on childcare and, consistent with prior research,23 parents reported more financial stress than nonparents. This is likely relevant even in lower-cost areas, since 39% of US medical students are graduating with at least $200,000 in educational debt.3 Thus, some advocate for subsidizing trainees' childcare costs.23 Respondents also reported a need for extended daycare hours, better aligned with GME work schedules, as has been previously reported.1 Institutions that help trainees with children access and afford necessary childcare may be better positioned to recruit trainees.
These findings are limited in generalizability due to the low response rate (26%) from 2 hospitals in the same hospital system in a high-cost urban setting. Trainees with children or planning to have children may have been more likely to respond to the survey. Also, as the survey was not tested for validity evidence, respondents may not have interpreted questions as intended.
Since this survey was conducted, the GME parental leave policies and other parenting resources have changed at our institutions. We plan to periodically reassess the needs of trainees with children and will employ methods to enhance the response rate on future surveys.
Conclusions
This study provides new information on perspectives surrounding parental leave, lactation facilities, and childcare access and affordability for trainees with children, highlighting economic issues and current resource gaps.
Supplementary Material
Footnotes
Funding: This work was supported in parts by the NIH T32EB001631, the Radiological Society of North America R&E Foundation, and the Society of Abdominal Radiology.
Conflict of interest: The authors declare they have no competing interests.
The authors would like to thank Karen Donelan, Anne Rigg, Diane Sheehan, and Tina Gelsomino for their assistance and support.
References
- 1.Snyder RA, Tarpley MJ, Phillips SE, Terhune KP. The case for on-site child care in residency training and afterward. J Grad Med Educ . 2013;5(3):365–367. doi: 10.4300/JGME-D-12-00294.1. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jagsi R, Tarbell NJ, Weinstein DF. Becoming a doctor, starting a family—leaves of absence from graduate medical education. N Engl J Med . 2007;357(19):1889–1891. doi: 10.1056/NEJMp078163. doi: [DOI] [PubMed] [Google Scholar]
- 3.Association of American Medical Colleges. Medical School Graduation Questionnaire: 2018 All Schools Summary Report. https://www.aamc.org/download/490454/data/2018gqallschoolssummaryreport.pdf Accessed January 6, 2020.
- 4.Weinstein DF, Mangurian C, Jagsi R. Parenting during graduate medical training—practical policy solutions to promote change. N Engl J Med . 2019;381(11):995–997. doi: 10.1056/nejmp1904721. doi: [DOI] [PubMed] [Google Scholar]
- 5.Young-Shumate L, Kramer T, Beresin E. Pregnancy during graduate medical training. Acad Med . 1993;68(10):792–799. doi: 10.1097/00001888-199310000-00019. doi: [DOI] [PubMed] [Google Scholar]
- 6.Finch SJ. Pregnancy during residency: a literature review. Acad Med . 2003;78(4):418–428. doi: 10.1097/00001888-200304000-00021. doi: [DOI] [PubMed] [Google Scholar]
- 7.Willett LL, Wellons MF, Hartig JR, Roenigk L, Panda M, Dearinger AT, et al. Do women residents delay childbearing due to perceived career threats? Acad Med . 2010;85(4):640–646. doi: 10.1097/ACM.0b013e3181d2cb5b. doi: [DOI] [PubMed] [Google Scholar]
- 8.Aagaard EM, Julian K, Dedier J, Soloman I, Tillisch J, Pérez-Stable EJ. Factors affecting medical students' selection of an internal medicine residency program. J Natl Med Assoc . 2005;97(9):1264–1270. [PMC free article] [PubMed] [Google Scholar]
- 9.Rangel EL, Lyu H, Haider AH, Castillo-Angeles M, Doherty GM, Smink DS. Factors associated with residency and career dissatisfaction in childbearing surgical residents. JAMA Surg . 2018;153(11):1004–1011. doi: 10.1001/jamasurg.2018.2571. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Vassallo P, Jeremiah J, Forman L, Dubois L, Simmons DL, Chretien K, et al. Parental leave in graduate medical education: recommendations for reform. Am J Med . 2019;132(3):385–389. doi: 10.1016/j.amjmed.2018.11.006. doi: [DOI] [PubMed] [Google Scholar]
- 11.Holliday EB, Ahmed AA, Jagsi R, Stentz NC, Woodward WA, Fuller CD, et al. Pregnancy and Parenthood in Radiation Oncology, Views and Experiences Survey (PROVES): results of a blinded prospective trainee parenting and career development assessment. Int J Radiat Oncol . 2015;92(3):516–524. doi: 10.1016/j.ijrobp.2015.02.024. doi: [DOI] [PubMed] [Google Scholar]
- 12.Tang AL, Miller A, Hauff S, Myer CM, III, Takiar V, Howell RJ, et al. Maternity and paternity leave in otolaryngology residency training in the United States. Laryngoscope . 2019;129(5):1093–1099. doi: 10.1002/lary.27328. doi: [DOI] [PubMed] [Google Scholar]
- 13.Weiss J, Teuscher D. What provisions do orthopaedic programs make for maternity, paternity, and adoption leave? Clin Orthop Relat Res . 2016;474(9):1945–1949. doi: 10.1007/s11999-016-4828-x. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Garza RM, Weston JS, Furnas HJ. Pregnancy and the plastic surgery resident. Plast Reconstr Surg . 2017;139(1):245–252. doi: 10.1097/PRS.0000000000002861. doi: [DOI] [PubMed] [Google Scholar]
- 15.Dixit A, Feldman-Winter L, Szucs KA. Parental leave policies and pediatric trainees in the United States. J Hum Lact . 2015;31(3):434–439. doi: 10.1177/0890334415585309. doi: [DOI] [PubMed] [Google Scholar]
- 16.Hariton E, Matthews B, Burns A, Akileswaran C, Berkowitz LR. Pregnancy and parental leave among obstetrics and gynecology residents: results of a nationwide survey of program directors. Am J Obstet Gynecol . 2018;219(2):199.e1–199.e8. doi: 10.1016/j.ajog.2018.04.017. doi: [DOI] [PubMed] [Google Scholar]
- 17.Magudia K, Bick A, Cohen J, Ng TSC, Weinstein D, Mangurian C, et al. Childbearing and family leave policies for resident physicians at top training institutions. JAMA . 2018;320(22):2372–2374. doi: 10.1001/jama.2018.14414. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Varda BK, Glover M. Specialty board leave policies for resident physicians requesting parental leave. JAMA . 2018;320(22):2374–2377. doi: 10.1001/jama.2018.15889. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Humphries LS, Lyon S, Garza R, Butz DR, Lemelman B, Park JE. Parental leave policies in graduate medical education: a systematic review. Am J Surg . 2017;214(4):634–639. doi: 10.1016/j.amjsurg.2017.06.023. doi: [DOI] [PubMed] [Google Scholar]
- 20.Blair JE, Mayer AP, Caubet SL, Norby SM, O'Connor MI, Hayes SN. Pregnancy and parental leave during graduate medical education. Acad Med . 2016;91(7):972–978. doi: 10.1097/ACM.0000000000001006. doi: [DOI] [PubMed] [Google Scholar]
- 21.Gupta A, Meriwether K, Hewlett G. Impact of training specialty on breastfeeding among resident physicians: a national survey. Breastfeed Med . 2019;14(1):46–56. doi: 10.1089/bfm.2018.0140. doi: [DOI] [PubMed] [Google Scholar]
- 22.Cantu RM, Gowen MS, Tang X, Mitchell K. Barriers to breastfeeding in female physicians. Breastfeed Med . 2018;13(5):341–345. doi: 10.1089/bfm.2018.0022. doi: [DOI] [PubMed] [Google Scholar]
- 23.Key LL., Jr Child care supplementation: aid for residents and advantages for residency programs. J Pediatr . 2008;153(4):449–450. doi: 10.1016/j.jpeds.2008.05.028. doi: [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.