

Abstract
Objectives:
To explore among older adults whether multivariate neighborhood profiles were associated with physical activity (PA) and BMI.
Methods:
Adults (66–97 years) were recruited from Baltimore-Washington, DC (n=360), and Seattle-King County, Washington (n=368), regions. Latent profile analyses were conducted using the Neighborhood Environment Walkability Scale. ANCOVA models tested for criterion validity of profiles by examining relationships to PA and BMI.
Results:
Neighborhood profiles differed significantly by as much as 10 minutes/day for moderate-to-vigorous PA, 1.1 hours/week for walking for errands, and almost 50 minutes/week for leisure PA.
Conclusions:
Environmental variables resulted in meaningful neighborhood patterns that explained large differences in seniors’ health outcomes.
Keywords: policy, exercise, obesity, built environment, finite mixture modeling
In the United States, the population of adults over age 65 increased from about 20 to 40 million over the last 40 years, and this population is projected to double by 2050.1 Physically active older adults are less likely to experience a variety of health problems than are their inactive peers, suggesting that physical activity has a protective health effect.2–4 For adults 65 years and older, national physical activity guidelines are similar to those for younger adults: at least 150 minutes of moderate-to-vigorous physical activity (MVPA) per week or as ability and health conditions allow.5 Less than 3% of adults 60 years of age and older meet physical activity (PA) guidelines based on objective measures.6
There is consistent evidence that physical activity is shaped by neighborhood-built environment features.7–9 Neighborhood influences may be particularly important for older adults who, after occupational retirement, likely spend much of their day within their neighborhoods.10 Studies among adults have found that neighborhood-built environments characterized as “walkable” are associated with greater prevalence of physical activity and less obesity than are low-walkable neighborhoods.11–18 Walkable features include high residential density, diverse mixes of land uses, and a connected street pattern.7 However, research of neighborhood environment features among older adults is limited.15
Neighborhood environments include not only walkable features but also recreation and social features that coexist and that evolved for several reasons including era of development, regional location, politics, and economics.19,20 For example, some urban neighborhoods may have low residential density, few shops and sidewalks, poor access to public transportation, but easy access to aesthetically pleasing parks and recreation facilities, whereas in other parts of the same city, neighborhoods have different combinations of the same features. Several types of features have been independently associated with physical activity. Transport-related physical activity or “active transportation” for adults, such as walking or biking to retail, office, or public transportation destinations, appears related to walkable features.8,21,22 Recreation environments (eg, parks, trails) have been associated with increased recreational and leisure activity.9,22,23 Meanwhile, some social aspects of the environment, such as crime, have been inconsistently related to PA.
A difficult challenge is how to capture complex coexisting patterns of built, recreation, and social environments. Several approaches hold promise for characterizing patterns of neighborhood features including a priori selection of disparate variables for a single index (such as walkability),24 factor analysis,25–27 and classification of individuals into subgroups based on multivariate patterns.28,29 This latter approach could be especially helpful if specific neighborhood patterns or typologies are identified that have functionally different relationships with older adults’ health-related outcomes.
Only a few studies have explored multivariate patterns, primarily among adolescents and middle-aged adults.28–31 Using a set of objective and self-reported variables in a study of adolescents, Yan and colleagues identified 4 neighborhood types.30 Health outcomes were not examined in this study, but the authors noted their profiles resembled classifications used by urban designers. Nelson and colleagues examined socio-demographic and objectively measured built environment factors also among adolescents and extracted 6 neighborhood types.31 They found that characteristics of newer suburban areas, but not rural or exurban areas, were related to adolescent physical activity and weight status. Norman and coauthors explored objectively measured aspects of neighborhood recreation environments and identified 3 multivariate profiles.28 Differences in adolescents’ physical activity, sedentary time, and weight status were found by profile. For adults aged 20–65 years, Adams and colleagues examined self-reported neighborhood walkable and recreation aspects in Baltimore/Washington, DC, and Seattle regions and identified 4 multivariate neighborhood profiles that appeared to generalize across the 2 regions.29 Neighborhood profiles were associated with differences in adults’ accelerometer-assessed and self-reported physical activity and body mass.
Older adults represent the least studied age-group for built environment—physical activity relations,14,21 and no study to date has explored multivariate patterns of built, recreation, and social environment features for older adults. Ecological models hypothesize that different patterns of walkable, recreation, and social features exist in neighborhoods and those areas with synergistic patterns typically related to PA should produce the strongest effects for physical activity.32 Other patterns of perceived neighborhood features may also exist for older adults and may be associated differentially with physical activity and body mass index (BMI). The purposes of the current analysis were (1) to explore whether reported walkability, social, and recreational environment variables hypothesized to be associated with adults’ physical activity produced distinct neighborhood environment profiles for older adults and (2) to test whether older adults’ physical activity and body mass differed by the neighborhood environment profiles after adjusting for confounding factors.
METHODS
Design and Sampling
The sample was obtained from the existing Senior Neighborhood Quality of Life Study (SNQLS). SNQLS was an observational study of the relation of neighborhood environments to health outcomes and well-being among ambulatory older adults.17,33 SNQLS sampled participants from areas stratified on objectively measured built environment factors conceptually related to walkability (ie, residential density, land use mix, intersection density, and retail floor area ratio) and median household income from the 2000 US Census.24 Participants were recruited between 2005 and 2008 from 100 block groups from the Baltimore–Washington, DC, region (n = 360) and 116 block groups from Seattle-King County, Washington, region (n = 368). A commercial marketing company provided contact information for older adults living in the designated areas.33 Individuals were randomly selected from the marketing lists and were sent an invitation to participate by mail followed by recruitment telephone calls. Participant eligibility included being 66 years or older, able to walk 10 feet with or without assistive devices, and able to complete informed consent and surveys in English. Participants were recruited and measured simultaneously across walkability and income strata to control for seasonal bias. Overall enrollment rate defined as those that returned the survey divided by eligible contacts was 21.4%.33 Institutional review boards from participating institutions approved the study, and participants provided written informed consent.
Measures
Neighborhood Environment Walkability Scale (NEWS).
The NEWS is a validated survey that assesses urban form and recreation environment variables in individuals’ neighborhoods.34–37 A version adapted for seniors was used in SNQLS that preserved original items from an abbreviated version25,36 and scored according to original NEWS scoring procedures.17,34 The adapted NEWS includes 8 subscales that assessed residential density (6 items), land use mix-diversity (23 items; alpha = .94), land use mix-access (6 items; alpha = .66), street connectivity (3 items; alpha = .42), walking and cycling facilities (4 items; alpha = .69), aesthetics (4 items; alpha = .77), pedestrian/traffic safety (6 items; alpha = .61), and crime safety (3 items; alpha = .82). The NEWS and subscale scoring procedures are available from www.drjamessallis.sdsu.edu. For all variables, response options were coded or recoded so that higher values were ordered in the direction expected for more physical activity. Residential-density subscale items were rated on a 5-point Likert type scale from none to all, with a weighted scale computed as an approximate density of each household type relative to a single-family detached residence (see Web site for scoring). Land use mix-diversity items assessed the time to walk from the home to 23 facilities (eg, grocery store, restaurant, post office) on a 5-point Likert type scale from 31 minutes or more to 1–5 minutes; scale was computed as the mean of responses. Participants rated items from remaining NEWS sections on 4-point Likert scales ranging from strongly disagree to strongly agree; scales were computed as the mean of responses. Test-retest reliability and validity of the NEWS have been supported in multiple studies across several countries using a variety of validity criteria.25,34–37
Several additional items were selected for analysis a priori because they are not represented by a NEWS subscale, they have an expected association with transportation or recreational physical activity, and they are modifiable aspects of the environment that have specific relevance to policies that promote physical activity. These items included distance to the nearest bus or train stop, park, and recreation center or gym or fitness facility. Time to walk to these places was measured on the same Likert-type scale as land use mix-diversity.
Objective physical activity.
The Actigraph accelerometer (Pensacola, FL; model 7164 or 71256) measured moderate-to-vigorous physical activity (MVPA). Participants wore the Actigraph on their right hip using an elastic belt during all waking hours for 7 days. For scoring MVPA, a valid day was defined as ≥8 valid hours of wear, with a valid hour consisting of <45 consecutive 1-minute epochs with zero values. To accumulate at least 5 days or 66 valid hours, participants were asked to rewear the accelerometer x number of days if <5 valid days or <66 valid hours across 7 days were observed. Accelerometer data were scored using MeterPlus version 4.0 software (Santech, Inc). On valid days, each minute was scored as meeting or not meeting a criterion of at least moderate intensity based on the Freedson cut-point for adults (≥1952 counts/min), and an average MVPA minutes per valid wearing day was computed for this analysis.38 Actigraph accelerometers have produced reliable and valid estimates of physical activity.39
CHAMPS Activities Questionnaire for Older Adults.
The CHAMPS questionnaire asked participants to recall age-appropriate types of activity done over the last 4 weeks. Participants were asked to report their typical weekly cumulative duration of “walking for errands” and “leisure-time” types of activity. Response options ranged from less than 1 hour per week to 9 or more hours per week on a 6-point scale. Walking for transportation was operationalized as hours per week of walking for errands. Hours per week of leisure-time physical activities was computed by summing the duration of leisure-time activities (eg, walking, tennis, swimming, golf) and other moderate- and vigorous-intensity physical activities done for leisure. The CHAMPS questionnaire was designed and validated for older populations.40
Body Mass Index (BMI).
Self-reported weight and height were used to estimate BMI (kg / m2).
Demographics.
Demographics included self-reported sex, age (years), ethnicity (non-Hispanic white versus nonwhite or Hispanic), annual household income (11 levels from <$US10,000 to >$US100,000), education (7 levels from seventh grade to completed graduate degree), number of motor vehicles per adults in household (continuous), marital or cohabitation status (married or living together versus other), number of people in household (continuous), and years at current address (continuous).
Statistical Analyses
Descriptive statistics for all variables were examined. A latent profile analysis (LPA) was conducted independently in each region with 11 reported environmental variables (8 NEWS subscales and 3 items) using Mplus (version 6.0). LPA, a special case of latent class analysis using continuous indicators, statistically derives mutually exclusive subgroup profiles that maximize between-group variance and minimize within-group variance based on model fit criteria.41 LPA allows for subgroups within a population to be identified from their response patterns to environmental variables and allows for classification of individuals into derived profiles. Derived profiles are a function of the patterns produced from the 11 environmental variables. Robust standard errors for conditional-response probabilities were computed using sandwich estimators.
Solutions of 1 to 6 profiles were tested in Seattle and Baltimore–Washington regions separately. A bootstrapped Lo-Mendell-Rubin test (LMRT), interpretability of the profiles, and sample sizes per profile were compared across solutions to determine the number of latent profiles. The LMRT statistically compared a higher-profile solution to a solution with 1 fewer profiles; a significant LMRT test (ie, P-value <.05) indicated the higher-profile solution fit the data better (eg, 2-profile better than 1-profile). Profiles with ≥5% of the sample were considered viable. Z scores of observed variables within and between profiles were graphed for visual interpretation. The maximum posterior probability from the vector of profile posterior probabilities was used to assign individuals to a specific latent profile. Mean posterior probabilities per latent profile were calculated by averaging the maximum posterior probabilities for individuals classified to a specific profile. Mean values close to 1 indicate a strong degree of classification certainty, the most important characteristic of a good latent class/profile model.41
To explore criterion validity, we regressed physical activity (accelerometer MVPA minutes/day, CHAMPS walking for errands and leisure-time hours/week) and BMI on neighborhood profiles using ANCOVA models in SPSS version 18. The least significant difference (LSD) post hoc test was selected because of its sensitivity to detect differences between subgroups after an omnibus test, its appropriate use for unbalanced subgroups, and our interest in reporting confidence intervals. Natural log transformed variables were used in regression models and antilogged to provide geometric means and 95% confidence intervals for tables. ANCOVA models were adjusted for covariates including sex, age, annual household income, education, ethnicity, motor vehicles/adults in household, marital status, number of people in household, and years at current address.
RESULTS
Table 1 presents descriptive statistics on participants’ demographics, physical activity and BMI for Seattle and Baltimore–Washington regions. Complete survey data were available for 354 (98.3% of enrolled) adults from the Baltimore–Washington and 360 (97.8%) adults from the Seattle regions and were included in the LPA analysis. Participants with complete survey data ranged from 66 to 97 years of age (M=74.4 SD± 6.3), 53.0% were women, and 29.2% were nonwhite or Hispanic racial-ethnic minority.
Table 1.
SNQLS Participant Demographics and Characteristics in Baltimore-Washington, DC, and Seattle Regions
| Baltimore-Washington, DC (N=354) |
Seattle (N=360) |
|
|---|---|---|
| Sex (% women) | 55.11 | 50.83 |
| Age (years) | 73.77 (5.83) | 74.95 (6.61) |
| Household Income ($ year - median) | 40,000–49,999 | 30,000–39,999 |
| Education (% at least college degree) | 49.43 | 48.33 |
| Race/Ethnicity (% nonwhite) | 42.74 | 15.88 |
| Vehicles Per adult | 0.88 (0.43) | 0.98 (0.49) |
| Married or Living w/Partner (%) | 54.99 | 58.50 |
| # People in Household | 1.81 (0.76) | 1.81 (0.77) |
| Years at Current Address | 24.85 (14.48) | 24.51 (16.51) |
| MVPA (min/d) | 12.74 (15.65) | 14.24 (17.40) |
| CHAMPS Errands (hr/wk) | 0.48 (0.71) | 0.48 (0.66) |
| CHAMPS Leisure (hr/wk) | 1.10 (0.80) | 1.23 (0.80) |
| BMI (kg/m2) | 26.81 (4.77) | 26.11 (4.69) |
Note. Table values shown are means (standard deviations) unless noted otherwise.
A 4-profile solution in the Baltimore–Washington region and a 3-profile solution in the Seattle region provided the best fit to the data based on model fit criteria, reasonable sample sizes per profile (≥5%), and interpretable neighborhood profiles. Figures 1a and 1b present the profiles with z scores of environmental variables by region.
Figure 1a.
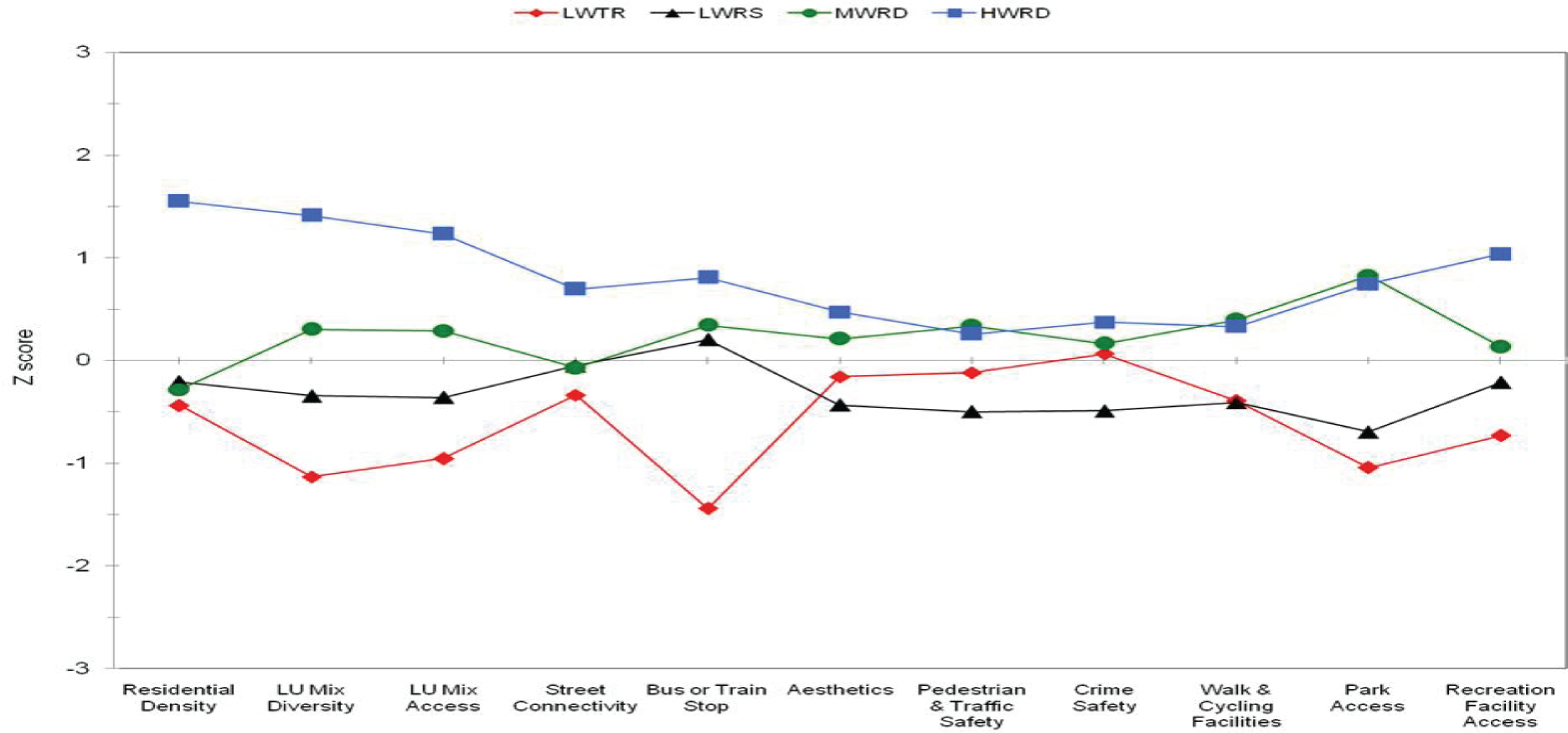
Four Latent Neighborhood Profiles for the Baltimore–Washington, DC, Region (Z Scores)
Figure 1b.
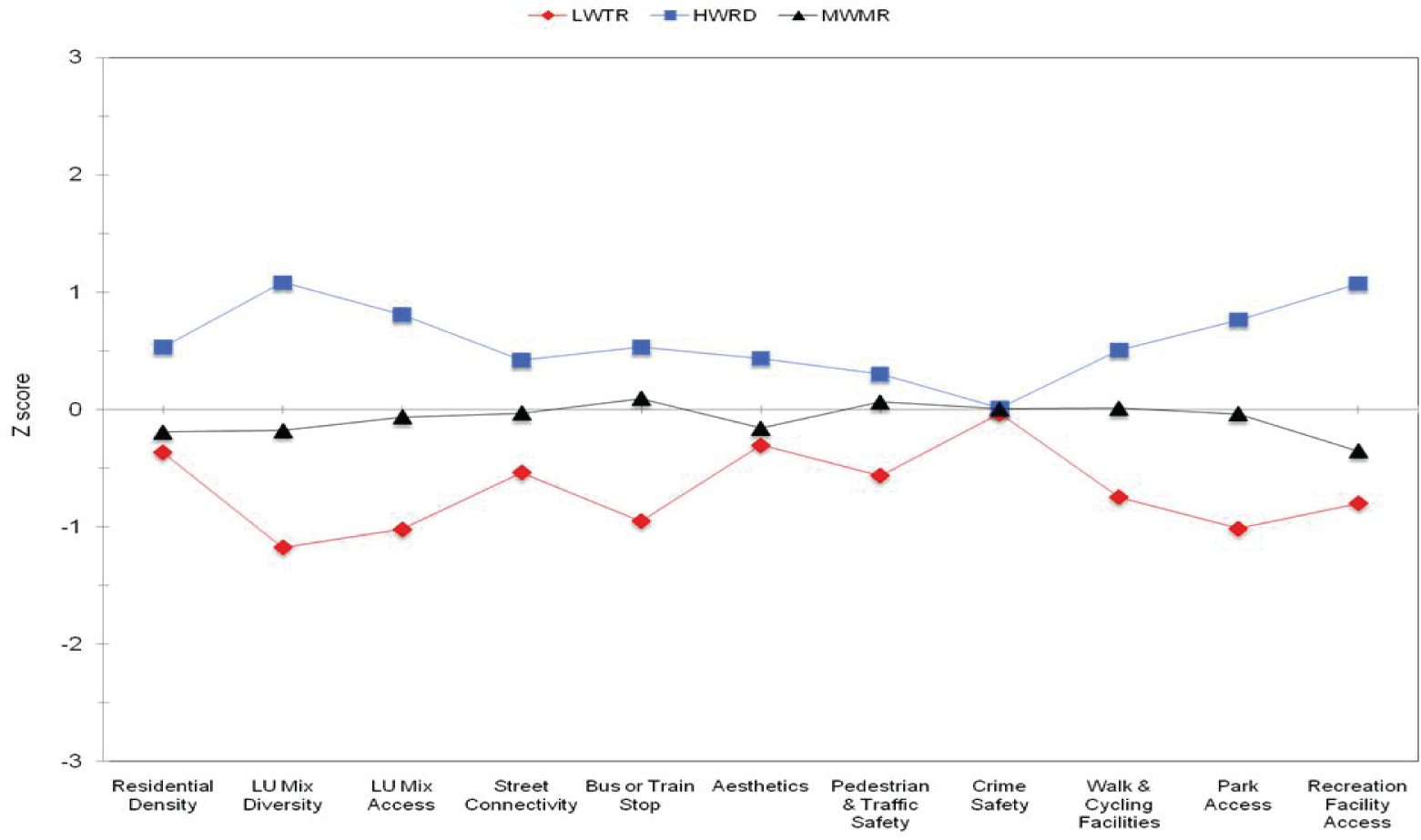
Three Latent Neighborhood Profiles for the Seattle Region (Z Scores)
Table 2 shows the mean posterior probability and variation of each latent profile. Mean probabilities were equal to or greater than .90, providing evidence for a strong degree of profile homogeneity and separation.
Table 2.
Average Maximum Posterior Probabilities Per Profile by Region
| Average (±SD) probability for… Baltimore-Washington, DC | ||||
|---|---|---|---|---|
| Classified into… | LWTR | LWRS | MWRD | HWRD |
| Low Walkable, Transit, and Recreation (LWTR) | 0.95 (.10) | 0.04 (.10) | 0.00 (.00) | 0.00 (.00) |
| Low Walkable / Recreationally Sparse (LWRS) | 0.04 (.08) | 0.90 (.12) | 0.06 (.06) | 0.00 (.00) |
| Moderately Walkable / Recreationally Dense (MWRD) | 0.00 (.00) | 0.03 (.06) | 0.94 (.10) | 0.03 (.08) |
| High Walkable / Recreationally Dense (HWRD) | 0.00 (.00) | 0.01 (.06) | 0.04 (.07) | 0.95 (.10) |
| Seattle | ||||
| LWTR | MWMR | HWRD | ||
| Low Walkable, Transit, and Recreation (LWTR) | 0.91 (.13) | 0.09 (.13) | 0.00 (.00) | |
| Moderately Walkable / Moderately Recreational (MWMR) | 0.06 (.11) | 0.91 (.12) | 0.03 (.08) | |
| High Walkable / Recreationally Dense (HWRD) | 0.00 (.00) | 0.06 (.11) | 0.94 (.11) | |
For the Baltimore–Washington region, the first profile contained a group that represented 21.2% of the sample and was labeled as “Low Walkability, Transit, and Recreation (LWTR)” because it had the lowest z scores for residential density; land use mix diversity and access; intersection density; and access to public transit, parks, and recreational facilities relative to the other profiles. This profile also had lower than average access to walking and cycling facilities and slightly higher than average regional values for perceived safety from crime. Profile 2 included 27.7% of the Baltimore–Washington sample and was characterized as “Low Walkable and Recreationally Sparse (LWRS)” because of moderately low values (z scores less than zero) for walkability – except public transit access — and recreation variables. This profile also had the lowest z scores of all profiles in the region for aesthetics, pedestrian and traffic safety, and crime safety. Profile 3 contained 35.3% of the Baltimore–Washington sample and was labeled “Moderately Walkable / Recreationally Dense (MWRD)”. This profile was characterized by moderately positive z scores of a similar magnitude for all environmental variables, except for residential density and street connectivity, which were lower. This profile also had the highest values for walking and cycling facilities, pedestrian and traffic safety, and park access. Profile 4 contained 15.8% of the sample and was labeled “High Walkable / Recreationally Dense (HWRD)” because the profile had positive values on all walkability, social, and recreation variables. This profile had the highest values for residential density, land use mix and access, street connectivity, access to public transportation (bus or train stop), aesthetics, crime safety, and recreation facilities. In addition, this profile had high values for park access, pedestrian and traffic safety, and walking and cycling facilities.
For the Seattle region, the first profile contained 21.4% of the sample and was labeled as “Low Walkability, Transit, and Recreation (LWTR)” because of the lowest z scores relative to the other Seattle region profiles on all variables, except crime safety. Interestingly, there was a lack of variance in reported crime safety across Seattle profiles; crime did not discriminate neighborhoods. Profile 2 contained 46.4% of the Seattle sample and was characterized as “Moderately Walkable / Moderately Recreational (MWMR)” because of average values for many environmental variables, except residential density, land use mix, aesthetics, and access to recreation facilities, which were slightly lower than average. Profile 3 contained 32.2% of the Seattle sample and was labeled “High Walkable / Recreationally Dense (HWRD)” because this profile had the highest z score values for the Seattle region on all built, social, and recreation variables.
Criterion Validity of Profiles
ANCOVA-adjusted means for physical activity and BMI by neighborhood profile are presented in Table 3 by region. After adjusting for covariates, participants differed significantly on accelerometer-derived MVPA by neighborhood profile in Baltimore–Washington and Seattle regions, respectively (both omnibus P values ≤.05). The greatest minutes/day of MVPA occurred in the High Walkable / Recreationally Dense profile for both regions. Compared to the least active profile in each region (LWTR), participants in the HWRD profile groups had 7.3 MVPA mins/day more and 9.8 MVPA mins/day more in Baltimore–Washington and Seattle regions, respectively. Profiles in the 2 regions also differed significantly on self-reported hours of walking for errands, after adjusting for covariates (both omnibus Ps ≤.001). In Baltimore–Washington, walking for errands was 8.5 times greater in HWRD compared to LWTR profiles (0.15 versus 1.28 hrs/wk). Interestingly, all 4 profiles differed significantly from each other on walking for errands, with greater durations of walking occurring as walkability and recreation features increased. In Seattle, participants classified into the HWRD profile reported 4.5 times more walking for errands than that of those living in the LWTR neighborhoods (0.19 versus 0.88 hrs/wk) and 2.5 times more than that of those living in the Moderately Walkable / Moderately Recreational neighborhoods (.35 versus .88 hrs/wk). In addition, self-reported leisure-time physical activity in the Baltimore–Washington region varied significantly across neighborhood profiles after adjusting for covariates (omnibus P≤.001). Participants in the HWRD neighborhoods reported about a 2-fold increase in leisure activity hours per week compared to those living in the LWRS (.81 versus 1.64) and LWTR (0.91. versus 1.64 hrs/wk) neighborhoods. In Seattle, the pattern for HWRD was similar for leisure activity, but this effect was not statistically significant.
Table 3.
Adjusted Means for Physical Activity and Body Mass Index (BMI) Variables by Latent Profile and Region
| Baltimore-Washington, DC Region | ||||||
|---|---|---|---|---|---|---|
| n | Omnibus P-values | Low Walkable, Transit, & Recreationa Mean (95% CI) | Low Walkable Recreationally Sparseb Mean (95% CI) | Moderately Walkable / Recreationally Densec Mean (95% CI) | High Walkabled Recreationally Densed Mean (95% CI) | |
| MVPA (min/d) | 311 | ≤.05 | 9.60a,b,c | 11.08a,b,c,d | 14.21a,b,c,d | 16.87b,c,d |
| (5.88 – 13.33) | (7.98 – 14.18) | (11.41 – 17.01) | (12.26 – 21.48) | |||
| CHAMPS | 322 | ≤.001 | 0.15a | 0.34b | 0.53c | 1.28d |
| errands (hr/wk) | (0.03 – 0.29) | (0.22 – 0.48) | (0.41 – 0.67) | (0.98 – 1.63) | ||
| CHAMPS | 321 | ≤.001 | 0.91a,b,c | 0.81a,b | 1.22a,c,d | 1.64c,d |
| leisure (hr/wk) | (0.65 – 1.20) | (0.60 – 1.04) | (0.99 – 1.47) | (1.20 – 2.17) | ||
| BMI | 322 | ns | 27.33a,b,c,d | 27.26a,b,c,d | 26.35a,b,c,d | 26.65a,b,c,d |
| (26.16 – 28.50) | (26.30 – 28.22) | (25.48 – 27.21) | (25.20 – 28.11) | |||
| Seattle Region | ||||||
| Low Walkable, Transit, & Recreationa Mean (95% CI) | Moderately Walkable / Moderately Recreationalb Mean (95% CI) | High Walkable / Recreationally Densec Mean (95% CI) | ||||
| MVPA (min/d) | 318 | ≤.05 | 10.09a,b | 13.17a,b | 19.86c | |
| (5.91 – 14.26) | (10.54 – 15.80) | (16.75 – 22.96) | ||||
| CHAMPS errands | 323 | ≤.001 | 0.19a,b | 0.35a,b | 0.88c | |
| (hr/wk) | (0.06 – 0.34) | (0.25 – 0.45) | (0.72 – 1.05) | |||
| CHAMPS leisure | 323 | ns | 1.14a,b,c | 1.20a,b,c | 1.40a,b,c | |
| (hr/wk) | (0.84 – 1.49) | (1.00 – 1.43) | (1.15 – 1.69) | |||
| BMI | 323 | ≤.001 | 27.54a | 25.73b,c | 25.71b,c | |
| (26.39 – 28.69) | (25.00 – 26.45) | (24.84 – 26.57) | ||||
Note. Superscripted letters next to profile labels show the letter’s reference profile. Mean values with similar superscript letters on the horizontal plane are not statistically different based on post hoc follow-up tests. Post hoc tests were performed within city only. All models were adjusted for sex, age, ethnicity, annual household income, education, # motor vehicles/adults in household, marital status, number of people in household, and length of time at current address.
For both regions, the lowest BMI was observed in the High Walkable / Recreationally Dense profiles. Participants in Seattle differed significantly by neighborhood profile on BMI, after adjusting for covariates (omnibus P ≤.001). BMI was lower by 1.83 kg/m2 in the HWRD profile and lower by 1.81 kg/m2 in MWMR profile in Seattle. Profile differences for BMI were not statistically significant in the Baltimore–Washington region.
DISCUSSION
Patterns of perceived built, social, and recreation environment variables were identified among older adults, resulting in meaningful neighborhood profiles. Neighborhood profiles in each region were associated with statistically significant and practically important differences in older adults’ objectively measured and self-reported physical activity, even though the derived number of neighborhood profiles differed slightly by region. The High Walkable/Recreationally Dense profile was associated with the best physical activity outcomes in both regions. This profile indicates a neighborhood typology that supported both active transportation and active recreation, so these could be considered physical activity-friendly neighborhoods. Because neighborhoods with these attributes are expected to support physical activity for utilitarian travel and recreational purposes, the higher levels of physical activity and lower levels of BMI suggest living in these neighborhoods is salutogenic for seniors.
The present results extend previous results indicating that walkability characteristics are related to active transportation, and recreation characteristics are related to active recreation among adults and seniors.8,22,23,42 The profiles included less often studied variables such as access to public transportation (bus or train stops), which varied substantially across profiles, and perceived safety from traffic, which can be measured only by self-report. The profiles integrate a wide variety of conceptually relevant neighborhood attributes from ecological models, and the present results suggest the cumulative impact of the multivariate profiles on seniors’ health outcomes may be substantial. Few studies have identified specific patterns from this set of environmental factors and their combined influence.
Neighborhood profiles were characterized by unique combinations and magnitudes of environmental factors. Although a 4-profile solution was observed in the Baltimore–Washington region and a 3-profile solution observed in the Seattle region, one profile type (HWRD) had a similar pattern of variables and was labeled the same in both regions. The HWRD profiles had a favorable — if not the most favorable — magnitude of reported residential density, land use mix-access and land use mix-diversity, street connectivity, access to public transit, walking and cycling facilities, aesthetics, pedestrian safety, and access to parks and recreation facilities compared to the other profiles. As predicted by ecological models for physical activity,32,43 a synergistic pattern of variables in the expected direction was associated with the best behavioral and health characteristics for seniors.
The Low Walkable, Transit, and Recreation profiles in both regions were associated with the poorest physical activity levels (and highest BMI in Seattle). Relative to other profiles, the LWTR profiles were characterized by very low residential density, land use mix, street connectivity (ie, walkability components), and access to public transportation. Additionally, these profiles revealed low access to walking/cycling facilities, parks, and recreation facilities and poor aesthetics and pedestrian safety. Thus, low values on social and recreational environment variables clustered along with a low-walkable environment. Notably, safety-from-crime scores in the Low Walkable, Transit and Recreation profiles were equal to or greater than the average scores of any built, social, or recreation factors in each region. This may indicate higher socioeconomic status for participants of physical-activity-unfriendly environments. Examination of household median income by profile confirmed that Baltimore–Washington and Seattle income levels correlated with less activity-friendly environments, but this observation was statistically significant for Baltimore–Washington only (data not shown). Importantly, household income was adjusted for in all models evaluating physical activity and BMI. These profile results suggest that seniors of higher SES may be at greater risk of being inactive as a consequence of an inactivity-promoting neighborhood design when walkability, social, and recreation factors are considered.
The results also suggest that profiles modestly better in some built, social, and recreation environment features were associated with improved physical activity outcomes. For example, reports of modestly greater land use mix, street connectivity, public transportation, and access to parks and recreation facilities, as seen by participants in the LWRS and MWRD neighborhoods in Baltimore, were associated with greater minutes/week of walking for errands. Users of public transportation may be more physically active and have a lower body mass.44,45 However, sufficient residential density is needed to support acceptable levels of transit service in neighborhoods.46 For leisure activities, seniors living in the LWRS neighborhoods unexpectedly had the fewest minutes. Interestingly, although perceived access to parks and recreational facilities was modestly better in the LWRS profile relative to the LWTR profile, aesthetic and traffic and crime safety variables were modestly weaker in the LWRS neighborhoods. Some research supports the relation between microscale aesthetic and safety variables and leisure activities, but this literature remains equivocal.22 This environmental pattern and physical activity relation did not occur in the Seattle region.
Results of the present analysis of perceived neighborhood environments may be compared to the outcomes from an objective GIS-analysis of walkability for older adults.16 In the current analysis, perceived environment factors were associated with larger differences for physical activity and BMI across neighborhoods. This finding may be a result of the greater diversity (ie, built, recreation, and social factors) and number of environment factors measured and used as part of the NEWS to define neighborhoods. Objective measures are limited by the reduced availability of data relative to the larger number of variables that are more easily assessed by self-report. Another possibility is that subtle neighborhood characteristics that influence physical activity may be captured better by self-reported rather than block-group level objective built environment features. For example, some researchers warn that static definitions of neighborhoods do not reflect participants’ definitions of their neighborhood or travel patterns.47 Self-reports of environments may circumvent this issue by allowing participants to define neighborhood boundaries. It is also possible the patterning of region-specific environment features captured by the LPA allowed for greater ability to explain physical activity and BMI outcomes. Most likely the sum of these reasons accounted for the stronger effects observed by neighborhood profiles.
The latent profile approach was recently used to characterize neighborhoods in the Baltimore–Washington and Seattle regions among younger adults (aged 20–65 years) participating in the Neighborhood Quality of Life Study (NQLS).29 The SNQLS and NQLS studies, although sharing a similar study name and design, were independent in their sampling and measures. Compared to NQLS participants, SNQLS participants were on average 29 years older and lived at their current residences longer, but were less educated and lived on a lower median income. As expected, older SNQLS participants also were less physically active. Interestingly, a 4-profile solution was observed in the Baltimore–Washington region in both studies, and the patterning of NEWS variables in Baltimore–Washington was surprisingly similar upon visual inspection for each profile. Additionally, the High Walkable Recreationally Dense profile revealed the best health outcomes in both studies. However, in the Seattle region the number of and patterning of profiles had some variation between studies. This region had one fewer lower-walkable profiles for seniors, which could reflect a trend for older adults to avoid low-walkable suburbs that are more pronounced in the Seattle region. A moderately walkable / recreationally dense profile was identified in the SNQLS Seattle region, but it had too few members (<3%) to be viable. These observations provide preliminary evidence that the neighborhood profiles were partially generalizable across individuals of different age-groups living in the same region.
Methodological Strengths and Considerations
Strengths of the present analysis included the examination of environmental relationships among an understudied older adult sample, use of a validated measure of diverse neighborhood environment features, use of validated self-report and objective measures of seniors’ physical activity, and excellent profile separation and homogeneity. Neighborhood profiles were related to 2 modalities of measuring physical activity: self-report and accelerometer measures. The profile-environment relations were robust after controlling for several potential confounding variables. Thus, self-report bias was less likely and evidence of criterion validity was stronger than would be expected with only one type of activity measure.
Limitations included the inability to separate cause-effect relationships inherent in a cross-sectional design and use of self-reported BMI and environment features. Further study of BMI outcomes is needed to confirm these results. Previous studies have found a mismatch between reported and objectively measured built environments,48 and concordance appears to interact with physical activity status and some demographic variables.37,48 If physical activity level improved knowledge of environment features present, then the associations observed between perceived environments and self-reported physical activity may be upwardly biased (same source bias). However, profile relationships were similar for our accelerometer measures, which decreases this possibility. Future applications of latent profile analysis could include both self-reported and objective built environment variables to potentially increase the predictive utility of profiles. Self-reported built environment measures could be enhanced by objective measures of accessible environment features surrounding each participant’s residence via a road network buffer. It is also possible that derived profiles are underspecified with respect to the wide range of neighborhood characteristics that could be considered. Different characterizations of neighborhoods may develop when further environmental features are included, such as the presence and quality of sidewalks or park amenities. Because of the current study’s sampling approach, proportions of individuals classified into specific subgroups should not be interpreted as prevalence estimates of each profile in a region. Future studies should extend present results by investigating other regions, using population-representative samples of older adults, and examining the impact of the number of variables on the interpretability and explanatory power of neighborhood profiles.
Although it is well known that neighborhoods include built and recreation environment features associated with physical activity, the specific patterns and combinations that occur among a wide range of environmental features are less well known, especially among older adults. This study found that a range of self-reported environment features produced unique neighborhood patterns that were associated with differing levels of seniors’ physical activity and BMI. The results appeared similar, in part, to those previously found for younger adults and could lead to the identification of optimal patterns of neighborhood attributes that facilitate physical activity.
Acknowledgments
This project was supported by grants from the National Heart, Lung and Blood Institute (HL67350, HL077141 & T32HL079891).
Contributor Information
Marc A. Adams, University of California, San Diego, Division of Behavioral Medicine, Department of Family and Preventive Medicine, La Jolla, CA..
James F. Sallis, University of California, San Diego, Division of Behavioral Medicine, Department of Family and Preventive Medicine, La Jolla, CA..
Terry L. Conway, University of California, San Diego, Division of Behavioral Medicine, Department of Family and Preventive Medicine, La Jolla, CA..
Lawrence D. Frank, University of British Columbia, School of Community and Regional Planning, Vancouver, BC, Canada..
Brian E. Saelens, Seattle’s Children’s Hospital, University of Washington, MPW 8-1 Child, Health and Behavioral Development, Seattle, WA..
Jacqueline Kerr, University of California, San Diego, Division of Behavioral Medicine, Department of Family and Preventive Medicine, La Jolla, CA..
Kelli L. Cain, University of California, San Diego, Division of Behavioral Medicine, Department of Family and Preventive Medicine, La Jolla, CA..
Abby C. King, Stanford University School of Medicine, Division of Epidemiology, Department of Health Research & Policy, and Stanford Prevention Research Center, Department of Medicine, Stanford, CA..
REFERENCES
- 1.Federal Interagency Forum on Aging-Related Statistics. Older Americans 2004: Key Indicators of Well-Being. Washington, DC: US Government Printing Office, 2004. [Google Scholar]
- 2.Nelson ME, Rejeski WJ, Blair SN, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39:1435–1445. [DOI] [PubMed] [Google Scholar]
- 3.Centers for Disease Control and Prevention, Merck Company Foundation. The State of Aging and Health in America 2007. Whitehouse Station, NJ: The Merck Company Foundation, 2007. [Google Scholar]
- 4.Physical Activity Guidelines Advisory Committee 2008. Physical Activity Guidelines Advisory Committee Report. Washington, DC: U.S. Department of Health and Human Services, 2008. [Google Scholar]
- 5.U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. Report No. ODPHP #U0036. Washington, DC: U.S. Department of Health and Human Services, 2008. [Google Scholar]
- 6.Troiano RP, Berrigan D, Dodd KW, et al. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40:181–188. [DOI] [PubMed] [Google Scholar]
- 7.Saelens BE, Sallis JF, Frank LD. Environmental correlates of walking and cycling: findings from the transportation, urban design, and planning literatures. Ann Behav Med. 2003;25:80–91. [DOI] [PubMed] [Google Scholar]
- 8.Heath GW, Brownson RC, Kruger J, et al. Task Force on Community Preventive Services. The effectiveness of urban design and land use and transport policies and practices to increase physical activity: a systematic review. J Phys Act Health. 2006;3:S55–S76. [DOI] [PubMed] [Google Scholar]
- 9.Gebel K, Bauman AE, Petticrew M. The physical environment and physical activity: a critical appraisal of review articles. Am J Prev Med. 2007;32:361–369. [DOI] [PubMed] [Google Scholar]
- 10.Kerr J, Rosenberg D, Frank L. The role of the built environment in healthy aging community design, physical activity, and health among older adults. Journal of Planning Literature. in press. [Google Scholar]
- 11.Sallis JF, Saelens BE, Frank LD, et al. Neighborhood built environment and income: examining multiple health outcomes. Soc Sci Med. 2009;68:1285–1293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Van Dyck D, Cardon G, Deforche B, et al. Neighborhood SES and walkability are related to physical activity behavior in Belgian adults. Prev Med. 2010;50(Suppl 1):S74–S79. [DOI] [PubMed] [Google Scholar]
- 13.Owen N, Cerin E, Leslie E, et al. Neighborhood walkability and the walking behavior of Australian adults. Am J Prev Med. 2007;33:387–395. [DOI] [PubMed] [Google Scholar]
- 14.Van Cauwenberg J, De Bourdeaudhuij I, De Meester F, et al. Relationship between the physical environment and physical activity in older adults: a systematic review. Health Place. 2011;17:458–469. [DOI] [PubMed] [Google Scholar]
- 15.Yen IH, Michael YL, Perdue L. Neighborhood environment in studies of health of older adults: a systematic review. Am J Prev Med. 2009;37:455–463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.King A, Sallis J, Frank L, et al. Neighborhood design, physical function, and healthful lifestyles in older adults: results from the Seniors Neighborhood Quality of Life Study. Int J Behav Med. 2010;17:252–253. [Google Scholar]
- 17.Shigematsu R, Sallis JF, Conway TL, et al. Age differences in the relation of perceived neighborhood environment to walking. Med Sci Sports Exerc. 2009;41:314–321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Frank L, Kerr J, Rosenberg D, King A. Healthy aging and where you live: community design relationships with physical activity and body weight in older Americans. J Phys Act Health. 2010;7:S82–S90. [DOI] [PubMed] [Google Scholar]
- 19.Frank LD, Engelke PO, Schmid TL. Health and Community Design: The Impact of the Built Environment on Physical Activity. Washington, DC: Island Press, 2003. [Google Scholar]
- 20.Putnam RD. Bowling Alone: The Collapse and Revival of American Community. New York: Simon & Schuster, 2000. [Google Scholar]
- 21.Sallis JF, Kerr J. Physical activity and the built environment. In Young D, Pangrazi RP and Ainsworth BE (eds), President’s Council on Physical Fitness and Sports Research Digest (Vol. 4), 2006. [Google Scholar]
- 22.Saelens BE, Handy SL. Built environment correlates of walking: a review. Med Sci Sports Exerc. 2008;40:S550–S566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kaczynski AT, Henderson KA. Parks and recreation settings and active living: a review of associations with physical activity function and intensity. J Phys Act Health. 2008;5:619–632. [DOI] [PubMed] [Google Scholar]
- 24.Frank LD, Sallis JF, Saelens BE, et al. The development of a walkability index: application to the Neighborhood Quality of Life Study. Br J Sports Med. 2010;44(13):924–33. [DOI] [PubMed] [Google Scholar]
- 25.Cerin E, Conway TL, Saelens BE, et al. Cross-validation of the factorial structure of the Neighborhood Environment Walkability Scale (NEWS) and its abbreviated form (NEWS-A). Int J Behav Nutr Phys Act. 2009;6:32. doi: 10.1186/1479-5868-6-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cervero R, Duncan M. Walking, bicycling, and urban landscapes: evidence from the San Francisco Bay Area. Am J Public Health. 2003;93:1478–1483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Messer LC, Laraia BA, Kaufman JS, et al. The development of a standardized neighborhood deprivation index. J Urban Health. 2006;83: 1041–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Norman GJ, Adams MA, Kerr J, et al. A latent profile analysis of neighborhood recreation environments in relation to adolescent physical activity, sedentary time, and obesity. J Public Health Manag Pract. 2010;16:411–419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Adams MA, Sallis JF, Kerr J, et al. Neighborhood environment profiles related to physical activity and weight status: a latent profile analysis. Prev Med. 2011;52:326–331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Yan AF, Voorhees CC, Clifton K, Burnier C. “Do you see what I see?” - correlates of multidimensional measures of neighborhood types and perceived physical activity-related neighborhood barriers and facilitators for urban youth. Prev Med. 2010;50(Suppl 1):S18–S23. [DOI] [PubMed] [Google Scholar]
- 31.Nelson MC, Gordon-Larsen P, Song Y, Popkin BM. Built and social environments associations with adolescent overweight and activity. Am J Prev Med. 2006;31:109–117. [DOI] [PubMed] [Google Scholar]
- 32.Sallis JF, Owen N, Fisher E. Ecological models of health behavior In Glanz K, Rimer BK, Viswanath K, (Eds), Health Behavior and Health Education: Theory, Research, and Practice (4th). San Francisco: Jossey-Bass, 2009: 465–482. [Google Scholar]
- 33.King AC, Sallis JF, Frank LD, et al. Aging in neighborhoods differing in walkability and income: associations with physical activity and obesity in older adults. Soc Sci Med. 2011. doi: 10.1016/j.socscimed.2011.08.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Saelens BE, Sallis JF, Black JB, Chen D. Neighborhood-based differences in physical activity: an environment scale evaluation. Am J Public Health. 2003;93:1552–1558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Brownson RC, Chang JJ, Eyler AA, et al. Measuring the environment for friendliness toward physical activity: a comparison of the reliability of 3 questionnaires. Am J Public Health. 2004;94:473–483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cerin E, Saelens BE, Sallis JF, Frank LD. Neighborhood Environment Walkability Scale: validity and development of a short form. Med Sci Sports Exerc. 2006;38:1682–1691. [DOI] [PubMed] [Google Scholar]
- 37.Adams MA, Ryan S, Kerr J, et al. Validation of the Neighborhood Environment Walkability Scale (NEWS) Items Using Geographic Information Systems. J Phys Act Health. 2009;6:S113–S123. [DOI] [PubMed] [Google Scholar]
- 38.Freedson PS, Melanson E, Sirard J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med Sci Sports Exerc. 1998;30:777–781. [DOI] [PubMed] [Google Scholar]
- 39.Welk GJ, Schaben JA, Morrow JR Jr. Reliability of accelerometry-based activity monitors: a generalizability study. Med Sci Sports Exerc. 2004;36:1637–1645. [PubMed] [Google Scholar]
- 40.Stewart AL, Mills KM, King AC, et al. CHAMPS physical activity questionnaire for older adults: outcomes for interventions. Med Sci Sports Exerc. 2001;33:1126–1141. [DOI] [PubMed] [Google Scholar]
- 41.Collins LM, Lanza ST. Latent Class and Latent Transition Analysis with Application in the Social, Behavioral, and Health Sciences. Hoboken, New Jersey: John Wiley & Sons, 2010. [Google Scholar]
- 42.Owen N, Humpel N, Leslie E, et al. Understanding environmental influences on walking; review and research agenda. Am J Prev Med. 2004;27:67–76. [DOI] [PubMed] [Google Scholar]
- 43.Sallis JF, Owen N. Physical Activity and Behavioral Medicine. Thousand Oaks, California: Sage Publications, 1999. [Google Scholar]
- 44.Besser LM, Dannenberg AL. Walking to public transit: steps to help meet physical activity recommendations. Am J Prev Med. 2005;29:273–280. [DOI] [PubMed] [Google Scholar]
- 45.MacDonald JM, Stokes RJ, Cohen DA, et al. The effect of light rail transit on body mass index and physical activity. Am J Prev Med. 2010;39:105–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Newman PWG, Kenworthy JR. Transport and urban form in thirty-two of the world’s principal cities. Transport Reviews. 1991;11: 249–272. [Google Scholar]
- 47.Matthews SA, Moudon AV, Daniel M. Work group II: using Geographic Information Systems for enhancing research relevant to policy on diet, physical activity, and weight. Am J Prev Med. 2009;36:S171–S176. [DOI] [PubMed] [Google Scholar]
- 48.Gebel K, Bauman A, Owen N. Correlates of non-concordance between perceived and objective measures of walkability. Ann Beh Med. 2009;37:228–238. [DOI] [PubMed] [Google Scholar]