

Abstract
A 27 years old sedentary woman presented bilateral femoral neck stress fractures after having clinically recovered from anorexia nervosa and was treated with bilateral internal fixation.
Conclusion
Although light exercise is usually considered after recovery from anorexia nervosa to improve bone quality, this case of a sedentary patient suggests that weight gain, per se, could increase the stress fracture risk. Because of the physiological and psychological characteristics, these patients should be treated with a multi-disciplinary approach.
Keywords: Bilateral femoral neck stress fracture, Hip fracture, Anorexia nervosa
Introduction
Anorexia nervosa (AN) is a disorder characterized by severe weight loss, fear to obesity and partial self-starvation. Most commonly found in women but increasing in men, it is currently the third most frequent chronic disease in adolescents [1,2]. Orthopaedic implications include a significant and sometimes permanent loss of bone stock, with a corresponding increase of fracture risk, including stress fractures (SF) [3,4].
The two main causes of reduction of bone density in AN are body composition changes and hormonal alterations. The reduction of body fat is coupled with a paradoxical increase in bone marrow fat, resulting from higher levels of preadipocyte factor-1 [5,6], a growing factor which inhibits the differentiation of the stem cell to osteoblast, with a subsequent reduction in the mechanical resistance of bone [2], increasing fracture risk and reducing bone healing potential.
In women, recovery parameters include that they must maintain a BMI >18 kg/m2 and have neither engaged in binging and purging behavior nor severely restricted food intake during the past year [7,8]. Psychological characteristics of patients with AN are complex and clinical recovery should be supported by psychological treatment and patient's understanding and control of the disease [2]. While gradually increasing mechanical bone loading by exercise should be beneficial for bone quality, considering that patient's BMI and bone health do not improve simultaneously, the initiation of physical activity or sports upon recovery from AN should be carefully considered to avoid stress fractures [2,9,10].
In addition, there is a higher incidence of treatment failure for hip fractures in AN patients, probably related to bone quality and healing potential as well as to lower patient treatment compliance due to psychological factors [11,12].
We report a case of a sedentary patient with AN, who sustained bilateral femoral neck SF. The patient was informed and acknowledged publication of her case, and the hospital's IRB approved publication.
Case report
The patient was a 27 year-old sedentary woman, lawyer, that had never engaged in any sport activity. A history of smoking (4 packs year according to smoking index [13]), on psychiatric medication due to panic attacks and chronic eating disorders which resulted, 5 years before admission for the fractures, in a BMI of 16.6 kg/m2 (height 1.57 mt – weight 41 kg) and amenorrhea. For a 5-year period (from 20 to 25 years old) her diet consisted on cookies, coffee and cigarettes. She partially modified this conduct 2 years before admission, when she weighed 62 kg (BMI 25.2 kg/m2 and still considering herself obese) and with regular menstrual periods, which confirmed that the patient had clinically recovered from AN.
She presented mild to moderate bilateral groin pain for 18 months, starting when she initiated weight gain. At this time she would not recognize her alimentary disorder and denied the previous AN condition.
Standard radiographs showed a calcar compression fracture in both hips (Fig. 1) and MRI showed a change of intensity in both femoral necks and bone oedema in the right, suggesting a compressive non displaced fracture at the inferior aspects of both femoral necks (Fig. 2-A). The bone scan revealed increase uptake of both femoral necks, also suggesting bilateral SF (Fig. 2-B), and finally, a CT scan confirmed the fracture in both hips (Fig. 3).
Fig. 1.

AP and lateral X-rays of both hips. Compression fracture at the inferior cortical of both hips femoral necks.
Fig. 2.

A- MRI: The intensity change in both femoral necks can be observed as well as bone oedema in the right femoral neck. B- Total body bone scan: Focal area of activity increase in the internal region of both femoral necks.
Fig. 3.

CT-scan. Both neck fractures are clearly seen.
Blood tests showed values for serum total proteins of 5.7 g/dl (6.6–8.7 g/dl), albumin of 3.2 g/dl (3.5–5.2 g/dl) and vitamin D of 16.4 ng/ml (30–50 ng/ml).
Using a minimally invasive procedure, bilateral internal fixation with a DHS (Dynamic Hip Screw - Synthes™ De Puy™, J&J™, Raynham, MA, USA) was performed. During surgery, 2 bone biopsies for histological analysis were taken (Fig. 4).
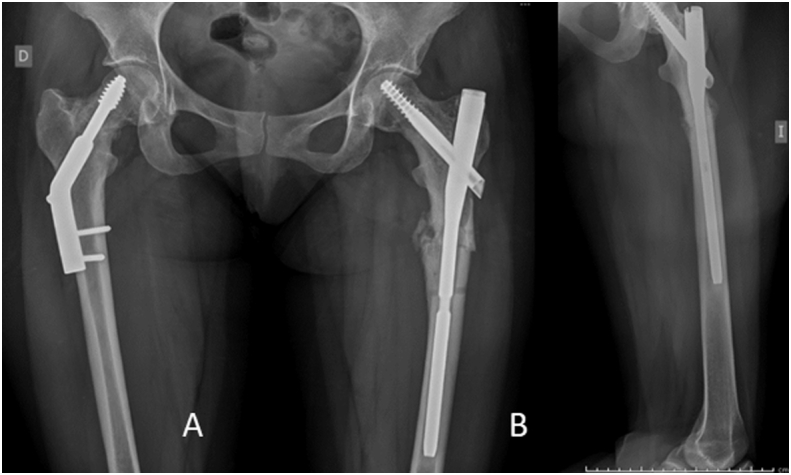
Fig. 4.

A- Location where biopsies were taken for the histological analysis (black dots). B & C- AP and lateral X-ray of both hips. The plate screws look shorter because they were placed in a divergent way.
The patient was started with partial weight bearing with a walker the day after surgery and was treated with vitamin D, calcium and a special diet.
The histological analysis informed normal bone.
The patient suffered a fall 3 days after surgery as a result of walking without assistance when going to the bathroom, and sustained a fracture of the left femur just below the DHS (Fig. 5A).
Fig. 5.

A- AP X-ray of both hips. Left femur fracture. B- Dynamic osteosynthesis with a proximal femoral nail and bone allograft.
A new internal fixation with a proximal femoral nail (PFNA -Synthes™ De Puy™, J&J™, Raynham, MA, USA) was performed (Fig. 5B) and, as the patient had not previously followed the walking instructions and to prevent a new fall, a non-weight bearing non-walking period of 3 weeks was enforced. Three months after surgery, the distal dynamic screw had reached its maximum sliding capacity and was removed to improve fracture site compression (Fig. 6). At 8 months after surgery, X rays showed the healing progression of the fractures (Fig. 7). The patient was deeply depressed and aggressive, walked indoors only, referring moderate bilateral generalized lower limb pain and using 1 cane. We then again emphasized the need for psychological and psychiatric assistance, to which she was initially reluctant and finally accepted. At 13 months after surgery, the patient walked with no assistance or pain, and the fractures were healed (Fig. 8).
Fig. 6.
A- 3 months after surgery. A- The fracture in the right hip is more evident than in previous X-rays. The removal of the dynamic screw allowed the impaction of the left femoral fracture. B- Left femur lateral view.
Fig. 7.

A- 8 months after surgery. The patient was still walking with 1 or 2 cane assistance and a generalized hip and bilateral lower limb pain. B- Left femur lateral view.
Fig. 8.

13 months after surgery. A fractures are healed. B- patient walked without assistance and no pain.
Discussion
Even if AN is not a rare condition, bilateral femoral neck stress fractures in these patients are not common and are even rarer in those with sedentary habits [1]. In this patient, excessive loading of weak bone due to body weight gain seems to be the key factor that generated the stress fractures.
Trabecular and cortical bone quality are usually compromised in AN, increasing the hip fracture risk [14]. Bone tissue disorders result from multiple factors involving both nutritional deficits and hormonal changes and generate not only loss of mineral bone density but also an alteration in bone architecture, with cortical porosity and decreased trabecular volume and thickness, condition that compromises the bone healing potential [9,10].
Tension fractures of the femoral neck occur on the superior aspect, with a vertical pattern that usually makes them unstable [15,16], whereas compression fractures occur on the inferior aspect and are generally stable [17]. Both types are low velocity repetitive injuries and some large studies show an avascular necrosis incidence ranging from 23 to 42% in displaced ones [[18], [19], [20]], rendering it essential to avoiding displacement.
Serum albumin may be surprisingly normal in patients with AN, and protein levels do not correlate with the severity of the condition [21,22]. In this particular case, the decision was to treat simultaneously the stress fractures and the nutritional imbalance.
Reduction of bone density is related to the reduction of trabecular volume and thickness [10], and in patients with AN, also to a reduction in the total number of trabeculae [23], producing a decrease in bone resistance. Nevertheless, even if bone density values are within normal parameters as in this case, patients who recover from AN do not totally recover the optimal bone quality corresponding to their age [3]. For recovering the best bone quality possible, the best strategy is still the normalization of body weight and menstrual cycle, but a total catch up is not usually observed [2,9], generating a period when bone load increases (because of higher body weight or sports) and bone resistance is still compromised.
When walking, the forces transmitted through the hip are 4 to 5 times body weight [24]. In our case, the forces increased from 205 kg to 310 kg when she improved her diet and gained weight, which is when hip pain began. Thus, since in patients with AN the recovery of bone quality is slower than recovery of body weight, it is important to be aware of this situation to avoid fractures.
The early diagnosis and treatment of SF is essential to ensure the return to complete function without side effects [25], and pain from a stress fracture could be the first symptom in patients with AN. Therefore, in young patients without other risk factors such as steroid therapy, alcohol abuse or high performance sports, AN should be suspected, especially if the patient has a low BMI. A high degree of suspicion is necessary as radiographs can be normal at the beginning and will reveal changes 2 or 3 weeks after the symptoms appeared, with only a 10% to 29% sensitivity [26]. Bone scan and MRI have a sensitivity of 98% and are the gold standard for diagnosis of SF in an early stage [17,27]. In our case, however, the fractures were only clearly visible in the CT scan.
Treatment of femoral neck SF is a matter of debate [1,2,12,28]. Nevertheless, just considering that the fracture might displace and dramatically worsen its prognosis suggests that it is best to perform prophylactic surgery.
For treatment of a compression type stress fracture of the femoral neck, the DHS system seems to be the ideal and less invasive fixation device [2,29]. In this particular case, we consider that the cause of failure of the initial left limb surgery was a combination of the patient's lack of self-protection and femoral weakness. In this case the SF occurred when the patient improved her diet. The 50% increase in body weight (41 Kg to 62 Kg) and the slower recovery of bone volume and quality were possibly related to the genesis of the fractures.
Women who have recovered from AN appear to maintain a lower BMI in association with a high level of physical activity, and the SF risk increases according the sport activity increases (particularly running, but also volleyball, tennis, basketball, and so on) [[30], [31], [32]]. The risk is probably much higher in patients who have recovered from AN [2].
Hernigou et al. [2] reported on a bilateral femoral neck SF in a patient already cured from AN, that occurred when starting sport activities. They proposed that the cause of the SF may be increased load in a bone that was not completely recovered. Rigotti et al. [33] reported an increased fracture risk in women with AN, and Lucas et al. [34] found that the cumulative incidence of fracture at forty years after diagnosis of AN was 57%.
The treatment of AN must involve physical activity to stimulate recovery of bone quality, but always within a multi-disciplinary approach involving psychiatrists, nutritionists and endocrinologists to attain the real cure of AN and not only body weight gain [9,10].
Carpintero et al. [1] proposed that changes in bone tissue in patients with AN are multifactorial and include nutritional deficits and hormonal disorders. They reported a 32-year-old patient with AN and bilateral femoral neck fracture treated with femoral nailing that developed bilateral femoral head avascular necrosis. A right total hip arthroplasty was performed, and before the left side was replaced, the patient committed suicide. This case highlights that in patients with AN not only the fracture healing could be compromised but also that their psychological characteristics are very complex.
Patients with AN are complex and require a long and personalized treatment. In this case, the psychological approach that included a pain therapy specialist's assistance was key for improvement. The patient was sedentary when she suffered the bilateral femoral neck SF, and this must draw our attention in order to consider what kind of low impact sporting activity such as swimming we should recommend in order to improve bone quality without exposing bone to an excessive load.
Statement of informed consent
The patient included in this paper was informed about the intention of publishing all about her case, and gave her personal consent about publishing all the information related to her pathology, treatment and final outcome.
The hospital IRB approved the publication of this case.
CRediT authorship contribution statement
P. Vedoya Santiago: Conceptualization, Methodology, Validation, Writing - review & editing. Alfredo Montero: Data curation, Writing - original draft, Visualization, Investigation. Hernán del Sel: Supervision, Validation, Writing - review & editing.
References
- 1.Carpintero P., Lopez-Soroche E., Carpintero R.R., Morales R. Bilateral insufficiency fracture of the femoral neck in a male patient with anorexia nervosa. Acta Orthop. Belg. 2013;79(1):111–113. [PubMed] [Google Scholar]
- 2.Hernigou J., Koulischer S., Maes R. Bilateral simultaneous femoral neck stress fracture despite clinical recovery from anorexia nervosa: a case report. JBJS Case Connect. 2017;7(1):e12. doi: 10.2106/JBJS.CC.16.00047. [DOI] [PubMed] [Google Scholar]
- 3.Misra M., Katzman D.K., Cord J. Bone metabolism in adolescent boys with anorexia nervosa. J. Clin. Endocrinol. Metab. 2008;93(8):3029–3036. doi: 10.1210/jc.2008-0170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Misra M., Aggarwal A., Miller K.K. Effects of anorexia nervosa on clinical, hematologic, biochemical, and bone density parameters in community-dwelling adolescent girls. Pediatrics. 2004;114(6):1574–1583. doi: 10.1542/peds.2004-0540. [DOI] [PubMed] [Google Scholar]
- 5.Bredella M.A., Fazeli P.K., Miller K.K. Increased bone marrow fat in anorexia nervosa. J. Clin. Endocrinol. Metab. 2009;94(6):2129–2136. doi: 10.1210/jc.2008-2532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fazeli P.K., Bredella M.A., Freedman L. Marrow fat and preadipocyte factor-1 levels decrease with recovery in women with anorexia nervosa. J. Bone Miner. Res. 2012;27(9):1864–1871. doi: 10.1002/jbmr.1640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bang L., Rø Ø., Endestad T. Normal gray matter volumes in women recovered from anorexia nervosa: a voxel-based morphometry study. BMC Psychiatry. 2016;16(1):144. doi: 10.1186/s12888-016-0856-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bang L., Rø Ø., Endestad T. Normal white matter microstructure in women long-term recovered from anorexia nervosa: a diffusion tensor imaging study. Int. J. Eat. Disord. 2018;51(1):46–52. doi: 10.1002/eat.22802. [DOI] [PubMed] [Google Scholar]
- 9.Misra M., Klibanski A. Anorexia nervosa and bone. J. Endocrinol. 2014;221(3):R163–R176. doi: 10.1530/JOE-14-0039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lawson E.A., Miller K.K., Bredella M.A. Hormone predictors of abnormal bone microarchitecture in women with anorexia nervosa. Bone. 2010;46(2):458–463. doi: 10.1016/j.bone.2009.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chadha M., Balain B., Maini L. Spontaneous bilateral displaced femoral neck fractures in nutritional osteomalacia – a case report. Acta Orthop. Scand. 2001;72(1):94–96. doi: 10.1080/000164701753606770. [DOI] [PubMed] [Google Scholar]
- 12.Gurdezi S., Trehan R.K., Rickman M. Bilateral undisplaced insufficiency neck of femur fractures associated with short-term steroid use: a case report. J. Med. Case Rep. 2008;2(1):79. doi: 10.1186/1752-1947-2-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Guaraldi G., Raggi P., Gomes A. Lung and heart diseases are better predicted by pack-years than by smoking status or duration of smoking cessation in HIV patients. PLoS One. 2015;10(12) doi: 10.1371/journal.pone.0143700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Vestergaard P., Emborg C., Støving R.K., Hagen C., Mosekilde L., Brixen K. Fractures in patients with anorexia nervosa, bulimia nervosa, and other eating disorders-a nationwide register study. Int. J. Eat. Disord. 2002;32(3):301–308. doi: 10.1002/eat.10101. [DOI] [PubMed] [Google Scholar]
- 15.Egol K.A., Koval K.J., Kummer F.F.V. Stress fractures of the femoral neck. Clin. Orthop. Relat. Res. 1998;(348):72–78. Mar. [PubMed] [Google Scholar]
- 16.Devas M.B. Stress fractures of the femoral neck. J. Bone Joint Surg. (Br.) 1965;47:728–738. [PubMed] [Google Scholar]
- 17.Humphrey J.A., Jandoo R., Tofighi M., Wiik A., Tindall A. Internal fixation of femoral neck stress fractures in young female athletes with a dynamic locking plate. Acta Orthop. Belg. 2015;81(3):358–362. [PubMed] [Google Scholar]
- 18.Pihlajamäki H.K., Ruohola J.-P., Weckström M., Kiuru M.J., Visuri T.I. Long-term outcome of undisplaced fatigue fractures of the femoral neck in young male adults. J. Bone Joint Surg. (Br.) 2006;88–B(12):1574–1579. doi: 10.1302/0301-620X.88B12.17996. [DOI] [PubMed] [Google Scholar]
- 19.Visuri T., Vara A., Meurman K.O. Displaced stress fractures of the femoral neck in young male adults: a report of twelve operative cases. J. Trauma. 1988;28(11):1562–1569. doi: 10.1097/00005373-198811000-00007. Nov. [DOI] [PubMed] [Google Scholar]
- 20.Lee C.H., Huang G.S., Chao K.H., Jean J.L.W.S. Surgical treatment of displaced stress fractures of the femoral neck in military recruits: a report of 42 cases. Arch. Orthop. Trauma Surg. 2003;123(10):527–533. doi: 10.1007/s00402-003-0579-8. Dec. [DOI] [PubMed] [Google Scholar]
- 21.Narayanan V., Gaudiani J.L., Mehler P.S. Serum albumin levels may not correlate with weight status in severe anorexia nervosa. Eat. Disord. 2009;17(4):322–326. doi: 10.1080/10640260902991202. [DOI] [PubMed] [Google Scholar]
- 22.Krantz M.J., Lee D., Donahoo W.T., Mehler P.S. The paradox of normal serum albumin in anorexia nervosa: a case report. Int. J. Eat. Disord. 2005;37(3):278–280. doi: 10.1002/eat.20129. [DOI] [PubMed] [Google Scholar]
- 23.Milos G., Spindler A., Rüegsegger P. Cortical and trabecular bone density and structure in anorexia nervosa. Osteoporos. Int. 2005;16(7):783–790. doi: 10.1007/s00198-004-1759-2. [DOI] [PubMed] [Google Scholar]
- 24.Giarmatzis G., Jonkers I., Wesseling M., Van Rossom S., Verschueren S. Loading of hip measured by hip contact forces at different speeds of walking and running. J. Bone Miner. Res. 2015;30(8):1431–1440. doi: 10.1002/jbmr.2483. [DOI] [PubMed] [Google Scholar]
- 25.Haddad F.S., Bann S., Hill R.A., Jones H.A. Case reports displaced stress fracture of the femoral neck in an active amenorrhoeic adolescent. Br. J. Sports Med. 1997;31:70–75. doi: 10.1136/bjsm.31.1.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Clough T.M. Femoral neck stress fracture: the importance of clinical suspicion and early review. Br. J. Sports Med. 2002;36(4):308–309. doi: 10.1136/bjsm.36.4.308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Murray S.R., Reeder M.T., Udermann B.E., Pettitt R.W. High-risk stress fractures: pathogenesis, evaluation, and treatment. Compr. Ther. 2006;32(1):20–25. doi: 10.1385/comp:32:1:20. [DOI] [PubMed] [Google Scholar]
- 28.Torrengo F., Paús V., Cédola J. Fracturas Por Estrés En Deportistas. http://www.clinicadeldeporte.com.ar/documentos/2010/2010_Fracturas_estris.pdf
- 29.Haddad F.S., Mohanna P.-N., Goddard N.J. Bilateral femoral neck stress fractures following steroid treatment. Injury. 1997;28(9–10):671–673. doi: 10.1016/s0020-1383(97)00047-8. [DOI] [PubMed] [Google Scholar]
- 30.Rizk M., Lalanne C., Berthoz S., Kern L., Godart N. Problematic exercise in anorexia nervosa: testing potential risk factors against different definitions. Stengel A. PLoS One. 2015;10(11):e0143352. doi: 10.1371/journal.pone.0143352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Schebendach J.E., Klein D.A., Foltin R.W., Devlin M.J., Walsh B.T. Relative reinforcing value of exercise in inpatients with anorexia nervosa: model development and pilot data. Int. J. Eat. Disord. 2007 Jul;40(5):446–453. doi: 10.1002/eat.20392. [DOI] [PubMed] [Google Scholar]
- 32.Field A.E., Gordon C.M., Pierce L.M., Ramappa A., Kocher M.S. Prospective study of physical activity and risk of developing a stress fracture among preadolescent and adolescent girls. Arch. Pediatr. Adolesc. Med. 2011;165(8):723. doi: 10.1001/archpediatrics.2011.34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Rigotti N.A., Neer R.M., Skates S.J., Herzog D.B., Nussbaum S.R. The clinical course of osteoporosis in anorexia nervosa. A longitudinal study of cortical bone mass. JAMA. 1991;265(9):1133–1138. [PubMed] [Google Scholar]
- 34.Lucas A.R., Melton L.J., Crowson C.S., O’Fallon W.M. Long-term fracture risk among women with anorexia nervosa: a population-based cohort study. Mayo Clin. Proc. 1999;74(10):972–977. doi: 10.4065/74.10.972. [DOI] [PubMed] [Google Scholar]