

Abstract
There are several modalities described to manage postoperative pain after a total knee replacement (TKR). Presently the regional anaesthesia techniques used after TKR focus on more peripheral, motor sparing blocks so as to facilitate early ambulation along with good quality pain relief. We describe use of ultrasound guided 3 point genicular nerve block (GNB) for managing postoperative pain successfully after a TKR.
Keywords: Genicular nerve, knee replacement, postoperative pain, ultrasound
Introduction
There are several modalities described to manage postoperative pain after a total knee replacement (TKR). Presently, the regional anaesthesia techniques used after TKR focus on more peripheral, motor sparing blocks so as to facilitate early ambulation along with good quality pain relief. Genicular nerve block (GNB) and ablation have been used for managing chronic pain from knee osteoarthritis with good success.[1] Here, we report a case of postoperative pain management (POPM) following TKR with GNB.
Case Report
A 63-year gentleman came for right TKR, following left TKR, which was done a week ago. He had received adductor canal block (ACB) for POPM following left TKR. This time, GNB was done on the right side at three locations, i.e., superomedial, superolateral, and inferomedial locations of the condyle-shaft junction as described in the literature [Figure 1].[2,3,4] Under ultrasound (USG) guidance and strict asepsis, we injected 2.5 ml of 0.5% bupivacaine with 2 mg of dexamethasone at every three locations (Figures 2 and 3 shows needle placement for superomedial injection and local anesthetic spread). Then, spinal anesthesia was given with 15 mg of bupivacaine heavy and 100 μg of morphine. Intraoperatively, the patient received local infiltrative analgesia (LIA) by the surgeon, ketorolac 30 mg, paracetamol 1 gm, and morphine 5 mg intravenously (IV). LIA included 100 mg of ropivacaine, 0.5 mg epinephrine, and 30 mg ketorolac diluted in 100 ml of normal saline. POPM was done by paracetamol 1 gm thrice daily, ketorolac 30 mg thrice daily, and tramadol 50 mg thrice daily, all IV.
Figure 1.

Ultrasound-guided 21 gauze block needle placement for Superomedial Genicular Nerve Block in the transverse axis
Figure 2.
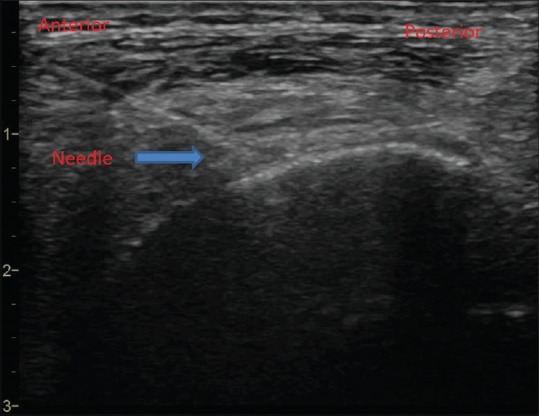
Sonoanatomy of Superomedial Genicular block showing in-plane needle placement from anterior to posterior
Figure 3.
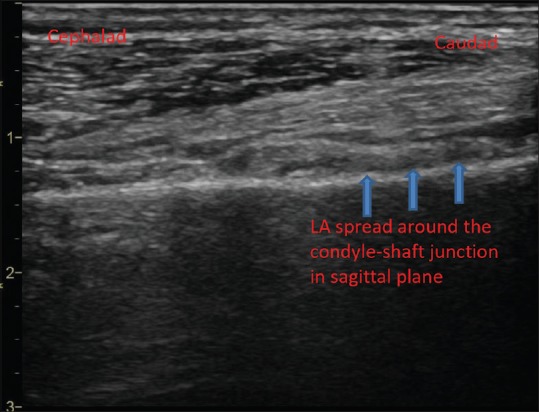
Sagittal Ultrasound scan showing local anesthetic spread in cephalo-caudad direction during genicular nerve block
At 6 h and 12 h post-TKR, his numerical pain rating (NRS) score at rest was 0 on both occasions. At 6 h, he was able to extend the knee fully and stand with support. At 24 h post-TKR, his NRS at rest and physiotherapy were 4 and 6, respectively. He was able to ambulate with support at 24 h post-TKR. He needed an additional 10 mg of IV morphine for rescue analgesia in 24–48 h period. While at discharge, he informed that he had better pain control on the side where GNB was done compared with the other side where he received ACB.
Discussion
Traditionally, POPM following TKR is done by various regional nerve blocks, periarticular infiltration, and epidural analgesia with other systemic analgesia.[5] In the last few years, there has been a paradigm shift in the care of these patients where early ambulation and discharge is being facilitated with motor-sparing nerve blocks. GNB has traditionally been used for managing chronic knee pain from osteoarthritis. In recent times, an extensive cadaveric study has been conducted to describe the precise location of genicular nerves and targets for the USG-guided needle placement for the block and ablation. We used GNB after discussing the same with the surgeon and patient which was done under US guidance and strict asepsis. In addition, we used other multimodal techniques like low-dose intrathecal morphine, LIA, and systemic analgesia, which is considered as part of the multimodal technique to provide adequate analgesia, thereby facilitating early rehabilitation. We found only one case series in the literature, where the authors injected 4 ml of dye at four locations (inferolateral in addition to regular three locations) in a fresh cadaver, where they found a wide periarticular spread of the dye in the computed tomography (CT) scan without any intraarticular spread. Subsequently, they did a case series of 12 TKRs with encouraging results.[6]
GNB selectively blocks articular branches and is motor-sparing. This can possibly be helpful in early ambulation and faster discharge of the patient following TKR. However, there is a need to do GNB in many patients and see if the consistent analgesic effect can be produced. Similarly, future study is needed to find out the optimal volume of local anesthetic needed to carry out the block. In addition, comparative studies of GNB with standard nerve blocks like ACB may give us an idea about the role of GNB in fast-track TKR.
Declaration
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Choi WJ, Hwang SJ, Song JG, Leem JG, Kang YU, Park PH, et al. Radiofrequency treatment relieves chronic knee osteoarthritis pain: Adouble-blind randomized controlled trial. Pain. 2011;152:481–7. doi: 10.1016/j.pain.2010.09.029. [DOI] [PubMed] [Google Scholar]
- 2.Franco CD, Buvanendran A, Petersohn JD, Menzies RD, Menzies LP. Innervation of the anterior capsule of the human knee: Implications for radiofrequency ablation. Reg Anesth Pain Med. 2015;40:363–8. doi: 10.1097/AAP.0000000000000269. [DOI] [PubMed] [Google Scholar]
- 3.Tran J, Peng PWH, Lam K, Baig E, Agur AMR, Gofeld M. Anatomical study of the innervation of anterior knee joint capsule: Implication for image-guided intervention. Reg Anesth Pain Med. 2018;43:407–14. doi: 10.1097/AAP.0000000000000778. [DOI] [PubMed] [Google Scholar]
- 4.Santana Pineda MM, Vanlinthout LE, Moreno Martín A, van Zundert J, Rodriguez Huertas F, Novalbos Ruiz JP. Analgesic effect and functional improvement caused by radiofrequency treatment of genicular nerves in patients with advanced osteoarthritis of the knee until 1 year following treatment. Reg Anesth Pain Med. 2017;42:62–8. doi: 10.1097/AAP.0000000000000510. [DOI] [PubMed] [Google Scholar]
- 5.Terkawi AS, Mavridis D, Sessler DI, Nunemaker MS, Doais KS, Terkawi RS, et al. Pain management modalities after total knee arthroplasty: A network meta-analysis of 170 randomized controlled trials. Anesthesiology. 2017;126:923–37. doi: 10.1097/ALN.0000000000001607. [DOI] [PubMed] [Google Scholar]
- 6.González Sotelo V, Maculé F, Minguell J, Bergé R, Franco C, Sala-Blanch X. Ultrasound-guided genicular nerve block for pain control after total knee replacement: Preliminary case series and technical note. Rev Esp Anestesiol Reanim. 2017;64:568–76. doi: 10.1016/j.redar.2017.04.001. [DOI] [PubMed] [Google Scholar]