

Sir,
Occipital neuralgia is a common form of headache with pain in the occipital region and posterior scalp. The pain can be debilitating and typically occurs in the distribution of the greater, lesser, or third occipital nerves.[1] Third occipital neuralgia is a form of occipital headaches characterized by frequent burning or stabbing pain in the posterior part of the scalp. Diagnosis can be difficult but is very likely when the headache is abolished following diagnostic blockade of the third occipital nerve. Third occipital neuralgia headaches are commonly managed conservatively with the use of oral analgesics including nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, antiepileptics, and neuropathic agents. When medical management fails, this condition may be treated with more invasive therapies such as trigger point injections, peripheral nerve blocks, or high cervical medial branch blocks.[2,3] Radiofrequency neurotomy of the third occipital nerve has typically been reserved for more severe cases as it is more invasive, time-consuming, and requires additional expertise in the field of pain management. Using radiofrequency neurotomy for this condition may allow patients to obtain significant longstanding relief of their pain condition.[4] Here, we describe our experience with this technique in a patient who suffered severe and longstanding headaches.
The patient was a male in his late 50s who developed chronic neck pain and occipital headaches after a work-related injury. The patient was hospitalized several times for pain control. Conservative medical management with NSAIDs, muscle relaxants, and neuropathic agents failed to alleviate his pain. The patient then underwent trigger point injections as well as greater and lesser occipital nerve blocks with minimal relief. He underwent diagnostic medial branch blocks of C4, C3, and the third occipital nerve with significant improvement of his pain. After a successful response to diagnostic nerve blocks, the patient proceeded to radiofrequency neurotomy of the third occipital nerve along with the medial branches of C4 and C3. Following this procedure, the patient obtained greater than 80% improvement in his headache frequency and pain levels. He was able to discontinue all his pain medications. The patient's pain was improved for 9 months, at which time his procedure was repeated with ongoing positive results [Figure 1].
Figure 1.
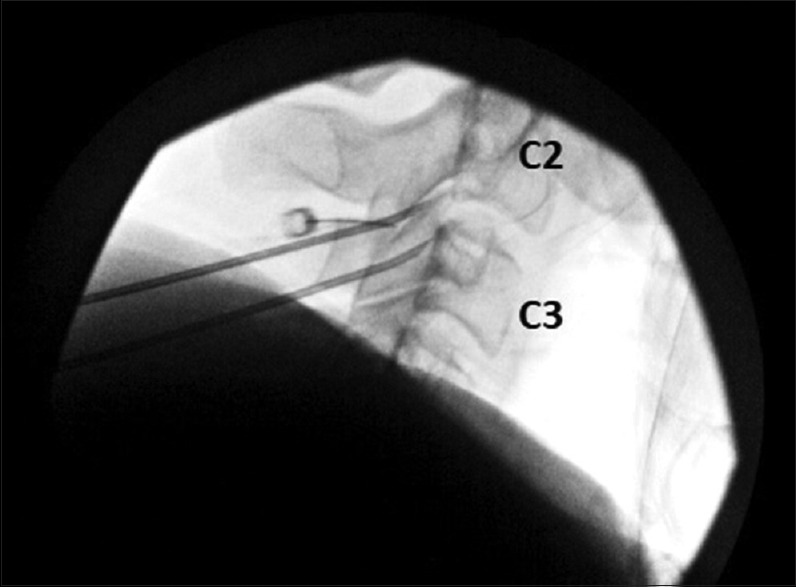
Radiographic imaging demonstrating a lateral view of the radiofrequency neurotomy of the third occipital nerve using a 16-gauge RFA probe. A third RFA probe was eventually placed between the two probes shown in this image ensuring coagulation of the third occipital nerve
Radiofrequency neurotomy of the third occipital nerve is an invasive procedure that may be used by anesthesiologists specializing in pain management for patients with debilitating headaches related to third occipital neuralgia. We describe our experience with this procedure and believe it can be of significant value for patients with this condition who fail more conservative management.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Headache Classification Committee of the International Headache Society (HIS) The International classification of headache disorders, 3rd Ed (beta version) Cephalalgia. 2013;33:629–808. doi: 10.1177/0333102413485658. [DOI] [PubMed] [Google Scholar]
- 2.Blumenfeld A, Ashkenazi A, Napchan U, Bender SD, Klein BC, Berliner R, et al. Expert consensus recommendations for the performance of peripheral nerve blocks for headaches – A narrative review. Headache. 2013;53:437–46. doi: 10.1111/head.12053. [DOI] [PubMed] [Google Scholar]
- 3.Zhou L, Hud-Shakoor Z, Hennessey C, Ashkenazi A. Upper cervical facet joint and spinal rami blocks for the treatment of cervicogenic headache. Headache. 2010;50:657–63. doi: 10.1111/j.1526-4610.2010.01623.x. [DOI] [PubMed] [Google Scholar]
- 4.Govind J, King W, Bailey B, Bogduk N. Radiofrequency neurotomy for the treatment of third occipital headache. J Neurol Neurosurg Psychiatry. 2003;74:88–93. doi: 10.1136/jnnp.74.1.88. [DOI] [PMC free article] [PubMed] [Google Scholar]