

Abstract
Purpose:
Few studies have investigated recovery between sexes using objective outcome measures. Our purpose was to examine the independent association between biological sex and recovery of post-concussion gait among collegiate athletes.
Methods:
We evaluated participants with a diagnosed concussion <7 days post-injury, and approximately 1.5 months and 3.5 months post-injury. Participants completed a single/dual-task gait evaluation and symptom inventory. During dual-task trials, they completed a mental task (backwards subtraction, spelling, or month recitation). The primary outcome measure was height-adjusted gait velocity recovery, defined as achieving normal gait velocity using established values: >0.56 and >0.50 gait velocity (m·s−1)/height (m) under single and dual-task conditions, respectively. We used a multivariable Cox proportional hazard model to identify associations between sex and dual-task recovery, controlling for age, concussion history, symptom severity, and loss of consciousness at the time of injury.
Results:
Ninety-four individuals participated in the study: 47 (50%) were female athletes (mean age=20.1, SD=1.3 years) and 47 (50%) were male athletes (mean age=20.3, SD=1.3 years). Sex was not independently associated with height-adjusted single-task gait velocity recovery after controlling for potential confounders (hazard ratio=1.62, 95% confidence interval=0.87, 3.01). However, male sex was independently associated with longer dual-task gait recovery time after controlling for potential confounders (hazard ratio=2.43, 95% confidence interval=1.11, 5.35).
Conclusion:
Male athletes required a longer duration of time after concussion to achieve dual-task gait recovery than female athletes. Thus, functional dual-task abilities after concussion may be affected differentially by sex, and should be accounted for within individualized concussion management strategies.
Keywords: locomotion, attention, mild traumatic brain injury, sex difference
Introduction
Concussion is a clinical diagnosis defined as a complex pathophysiological process resulting from head trauma accompanied by the onset of signs or symptoms or changes in mental function (1). Clinical decision-making is challenging, and complicated by the reliance on self-reported symptoms, the lack of validated objective tests to identify post-injury deficits and track recovery, and potentially confounding individual factors such as sex, age, or pre-injury medical history (2). Following injury, alterations to many different brain functions have been documented (3). Additionally, patient-level factors such as the sex of the patient appear to affect post-injury outcomes (4). Female athletes oftentimes present with more severe concussion symptoms and may also require a longer duration of time before symptom resolution than their male counterparts (5). Although female athletes may be at higher risk of sustaining a sport-related concussion (6) and demonstrate worse outcomes than male athletes (4), females remain understudied and underrepresented in sport-related concussion studies (7). As such, the National Institutes of Health currently emphasize that clinical researchers provide valid analyses by sex (8). Given that the majority of work comparing post-concussion sex differences has used subjective self-reported symptoms as the primary outcome for recovery, further work is needed using objective and physiologically based assessment methods.
Recent systematic reviews have highlighted that gait assessments objectively identify post-concussion deficits, particularly under dual-task conditions (9, 10). Dual-tasks require the simultaneous execution of a motor and cognitive task, thus equipping clinicians and researchers with the ability to measure patient abilities during a demand more comparable to sports requirements than single-tasks (11). Since concussion commonly results in motor and cognitive deficits, divided attention tasks may be more sensitive to post-concussion impairments than single-task assessments (12). Our recent findings and those of others indicate that dual-task gait deficits continue to persist beyond other clinical assessments such as symptom severity, computerized neurocognitive tests, or quiet stance assessments, suggesting their utility to contribute to post-concussion recovery monitoring (9, 10, 13, 14). This approach might allow clinicians to examine recovery of sport-like functional abilities beyond what traditional clinical techniques such as symptom inventories are equipped to do, and assist with appropriate decision making regarding return to play and treatment.
Recently, we have developed single-task and dual-task normative reference ranges for healthy collegiate athletes to help guide expectations for gait performance following concussion (15). This builds upon the work of Schmidt and colleagues, which suggests that normative data may be useful to determine recovery in lieu of pre-injury baseline performance, given the high level of resources required to capture pre-injury data on all athletes who go on to sustain a concussion (16). Although we have recently used single-task and dual-task normative ranges to identify acute post-concussion deficits (17), we are aware of no experimental data using established normative data thresholds to objectively and longitudinally monitor gait recovery following concussion. Investigating sex differences in dual-task gait recovery across a longitudinal post-injury timeline might allow for a more objective understanding of individual recovery than subjective symptom reporting, and may be less susceptible to the effects of confounding variables such as social isolation, restrictions on activities, and falling behind in school or work (18). Therefore, our purpose was to examine the independent association between biological sex and post-concussion gait recovery among collegiate athletes. Given past work that has identified longer symptom recovery times for female athletes compared to male athletes, we hypothesized that female athletes would require a longer time to achieve dual-task gait recovery than male athletes (19, 20).
Methods
Study Design and Participants
We conducted a prospective longitudinal study of collegiate athletes who were evaluated at multiple points following a sport-related concussion. All participants were diagnosed with a concussion and initially evaluated within 7 days of injury (median=3 days; range=1–7 days), and re-evaluated approximately 1.5 months (median=39 days; range=30–100 days) post injury, and again approximately 4.5 months post-injury (median=133 days; range=87–209 days). We selected these time points to provide an initial post-injury functional assessment, a follow-up assessment after the time that we expected most athletes would be cleared to return to play, and a follow-up assessment well beyond this time. A single sports medicine physician diagnosed all participants with a concussion and provided medical care throughout the duration of the study alongside a staff of athletic trainers. Concussion was defined according to the latest international consensus statement as a complex pathophysiological process resulting from head trauma, resulting in the onset of the signs or symptoms of a concussion or changes in neurocognitive function (1). All participants were active varsity student athletes enrolled at a single NCAA Division 1 university, were 18 years of age or older, and provided written informed consent to participate in the study. Exclusion criteria included asymptomatic status at the initial test (to ensure that the athlete experienced a concussion and had not recovered by the time of the first assessment), the presence of an existing lower extremity injury which may have affected gait abilities, a current psychiatric condition, or a concussion within the previous 6 months excluding the current injury. The local institutional review board approved of this study.
Gait Assessment Protocol
All participants completed a single-task and dual-task gait assessment consistent with prior work that was used to develop the normative values used for recovered status determination (15). No participant data used to develop these previously established normative standards were included in the current study. During the assessment, participants walked at a self-selected and normal pace toward a target placed 8m in front of them, walked around it, and returned to the original starting position without shoes. They completed five single-task and dual-task trials; the mean from these five trials was used for further analysis. During single-task trials, participants only completed the walking task, while during dual-task trials they walked and concurrently completed a cognitive test. The cognitive test consisted of one of three different forms performed continuously throughout each trial. The three task forms included spelling five-letter words backwards, serial subtraction from a two-digit number by 6 s or 7 s, or reverse month recitation. The test form used rotated between trials so that no two consecutive trials used the same test form and no duplicate cues were used. Cognitive performance was recorded during the test as the accuracy obtained on dual-task trials. Accuracy was calculated as the number correct divided by the total number of responses across the dual-task trials completed.
To quantify gait performance, participants wore a set of three inertial sensors (Opal Sensor, APDM Inc., Portland, OR, USA) attached to the lumbar spine at the level of the lumbosacral junction and on the dorsum of each foot with an elastic belt (15, 17). Data were obtained at sampling frequency of 128 Hz, synchronized, and transmitted to a laptop computer wirelessly during each trial. The primary outcome of interest was average gait velocity (m·s−1), calculated using Mobility Lab 2.0 software. Average gait velocity during single-task and dual-task conditions has previously demonstrated acceptable test-retest reliability (ICCs= 0.68, 0.77) among healthy collegiate athletes (15) and utility in detecting acute post-concussion deficits (17).
Outcome Variables
We calculated height-adjusted average gait velocity for all participants. As we expected male athletes to be taller than female athletes, we calculated height-adjusted average gait velocity in single-task and dual-task conditions as gait velocity (m·s−1)/height (m), consistent with prior work (15). In order to determine recovery status, we then classified all participants as recovered or not recovered at each assessment time point based on whether or not they had achieved normal height-adjusted average gait velocity according to previously established values (15). These standards were derived from a similar sample of healthy collegiate athletes, and participants were classified as recovered if they walked at with a height adjusted average gait velocity > 0.56 m·s−1/m during single-task gait, and > 0.50 m·s−1/m during dual-task gait. The normative data sample (15) did not include specific gait velocity values differentiated by sex. However, as past observations have revealed similar walking speeds between healthy women and men (21, 22), we elected to use the height adjusted average gait velocity rather than unadjusted average gait velocity given the expected height discrepancy between female and male athletes. By using the normative value thresholds to determine recovery, our analysis was unable to account for inherent walking characteristics (e.g. someone who naturally walks slow independent of concussion).
Our primary statistical analysis was a time-to-event (i.e. time to gait recovery) analysis in order to determine the relationship between sex and the number of days required for a participant to walk above the single-task and dual-task adjusted gait velocity thresholds. If during the last recorded visit, the participant walked with an average gait velocity lower than these established thresholds, their data was included in the time-to-event analysis as censored data. We elected to classify athletes using these previously developed values to assess the generalizability and utility of their use in clinical practice.
We also assessed symptom severity at each assessment using the post-concussion symptom scale (PCSS). Participants rate the severity of 22 different concussion symptoms using a scale from 0 (asymptomatic) to 6 (maximum severity), resulting in a total score ranging from 0 – 132. The internal consistency of this scale is high among athletes with concussions (Cronbach’s alpha = .93) (23) and it is used as a component of the Sport Concussion Assessment Tool, Version 5 (1). Since many participants may endorse symptoms that are unrelated to a concussion, we instructed those who had sustained a concussion to only rate the symptoms that started at the time of injury and that they had been experiencing in the 24 hours prior to the assessment.
Statistical Analysis
Continuous variables are presented as means (standard deviations or 95% confidence intervals), and categorical variables are presented as the number included and corresponding percentages. We first compared participant demographic, injury history, time of injury, and recovery characteristics using independent samples t-tests and Fisher’s exact tests. Consistent with the purpose of our study, our primary grouping variable was sex. To assess univariable differences between female and male athletes on gait velocity, we constructed univariable Cox proportional hazards models. Sex (female vs. male athletes) was the predictor variable, and height-adjusted single-task and dual-task gait recovery was the outcome variable. These univariable comparisons were only performed for descriptive purposes, and no statistical inferences were made using this approach. We also calculated dual-task cognitive accuracy for both groups at each time point.
To identify sex-based differences in single-task and dual-task recovery after concussion, we used a time-to-event analysis where we constructed two multivariable Cox proportional hazards models. The outcome variable was height-adjusted gait velocity recovery in each model (single-task and dual-task), determined using the thresholds described above (recovered vs. not recovered at each assessment). The predictor variable was sex. We included several relevant covariates that were selected a-priori due to their potential confounding effect on post-concussion symptom and dual-task outcomes. These variables included age, prior history of concussion, initial symptom severity rating, and LOC at time of injury (4, 5, 20, 24–27). Multivariable Cox proportional hazards models were selected rather than ANOVA in order to examine the change in status (recovered vs. non-recovered) over time where the outcome variable of interest may or may not occur during the study observation period and to appropriately account for variable post-injury assessment times and loss to follow-up (28). We assessed collinearity using condition indices and corresponding variance inflation factors. A condition index >30 was determined to require individual collinearity assessments, which were performed using variance inflation factors. Collinearity between two variables was detected if the variance inflation factor (VIF) was >2.5 (26, 29). Statistical significance was set at α < 0.05 and all tests were two-sided. Statistical analyses were performed using Stata version 15 (StataCorp, College Station, TX).
Results
Ninety-four individuals participated in the study: 47 (50%) were female athletes and 47 (50%) were male athletes. Male athletes were significantly taller than females (Table 1). Female and male athletes were of similar ages, assessed at similar time increments following injury, reported similar symptom severity initially after injury, and had a similar proportion of individuals who reported LOC at the time of injury and a prior history of concussion (Table 1).
Table 1.
Demographic and injury characteristics for the female and male athletes in the study.
| Variable | Female athletes (n=47) | Male athletes (n=47) | P value | ||
|---|---|---|---|---|---|
| Age | 20.1 (1.3) | 20.3 (1.3) | 0.53 | ||
| Height (m) | 1.70 (0.07) | 1.85 (0.09) | < 0.001 | ||
| Prior history of concussion? | 32 (68%) | 28 (60%) | 0.52 | ||
| Initial symptom severity rating † | 15 [9, 26] | 13.5 [7, 34] | 0.97 | ||
| LOC at time of injury? | 1 (2%) | 3 (6%) | 0.62 | ||
| Symptom resolution time (days) † | 13 [11, 18] | 13 [9, 26] | 0.94 | ||
| Assessment 1 time (days post-injury) † | 3 [2, 4] | 3 [2, 4] | 0.59 | ||
| Assessment 2 time (days post-injury) † | 39.5 [31, 63.5] | 38 [30, 62] | 0.80 | ||
| Assessment 3 time (days post-injury) † | 169 [107, 187] | 115 [94, 168] | 0.08 | ||
| Sport | Soccer: | 9 (19%) | Football: | 25 (53%) | - |
| Field Hockey: | 6 (13%) | Baseball: | 5 (11%) | ||
| Rugby: | 6 (13%) | Wrestling: | 5 (11%) | ||
| Basketball: | 5 (11%) | Ice Hockey: | 3 (6%) | ||
| Ice Hockey: | 5 (11%) | Lacrosse: | 3 (6%) | ||
| Softball: | 4 (9%) | Sailing: | 2 (4%) | ||
| Volleyball: | 3 (6%) | Basketball: | 1 (2%) | ||
| Crew: | 2 (4%) | Soccer: | 1 (2%) | ||
| Sailing: | 2 (4%) | Volleyball: | 1 (2%) | ||
| Lacrosse: | 1 (2%) | Water Polo: | 1 (2%) | ||
| Skiing: | 1 (2%) | ||||
| Tennis: | 1 (2%) | ||||
| Track and Field: | 1 (2%) | ||||
| Water Polo: | 1 (2%) | ||||
Data presented as median [interquartile range].
Univariable analysis indicated that sex was not significantly associated with height-adjusted single-task gait velocity recovery (Figure 1a; HR=1.55, 95% confidence interval=0.855, 2.814, P=0.149). Univariable analyses also indicated that sex was associated with height-adjusted dual-task gait velocity recovery (Figure 1b; Figure 2; HR=1.231, 95% confidence interval=1.092, 4.885, P=0.029). Cognitive accuracy during dual-task gait data is described in Figure 3.
Figure 1.
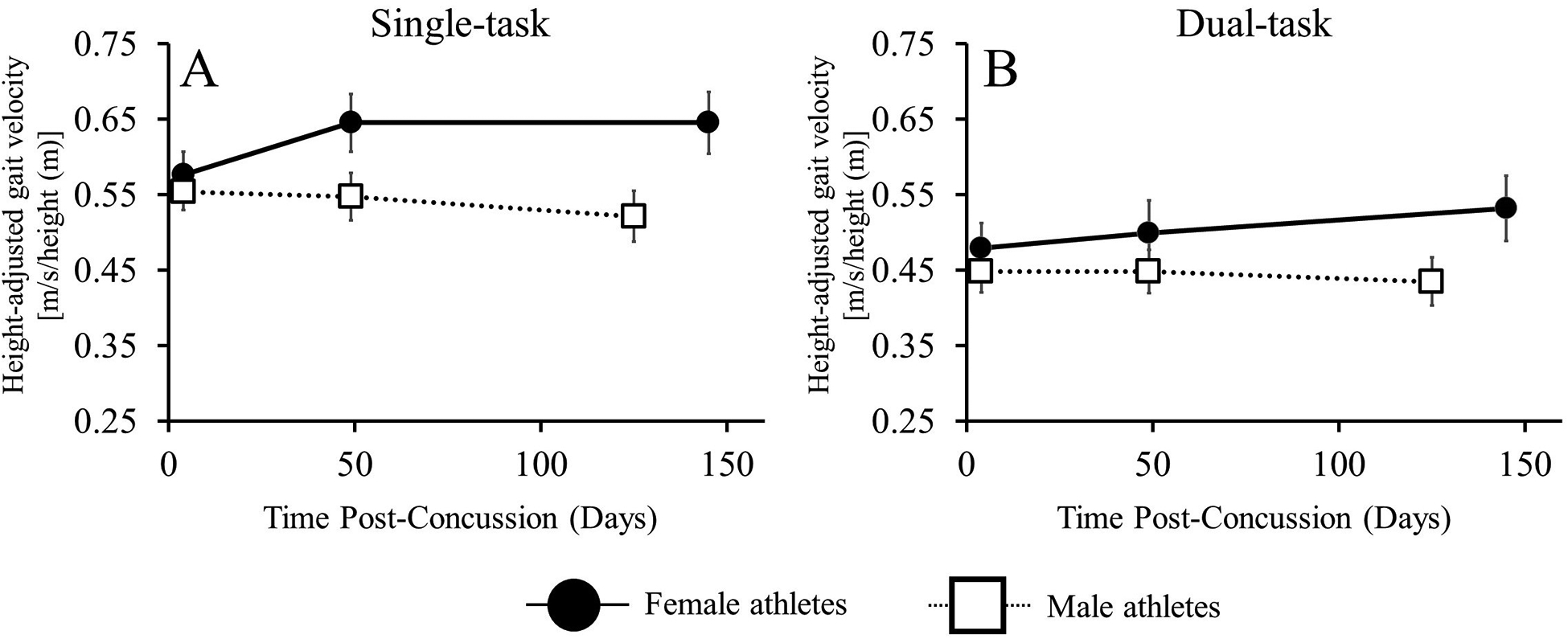
Height-adjusted single-task and dual-task average gait velocity recovery for female and male athletes. Data presented as means, error bars represent 95% confidence intervals.
Figure 2.
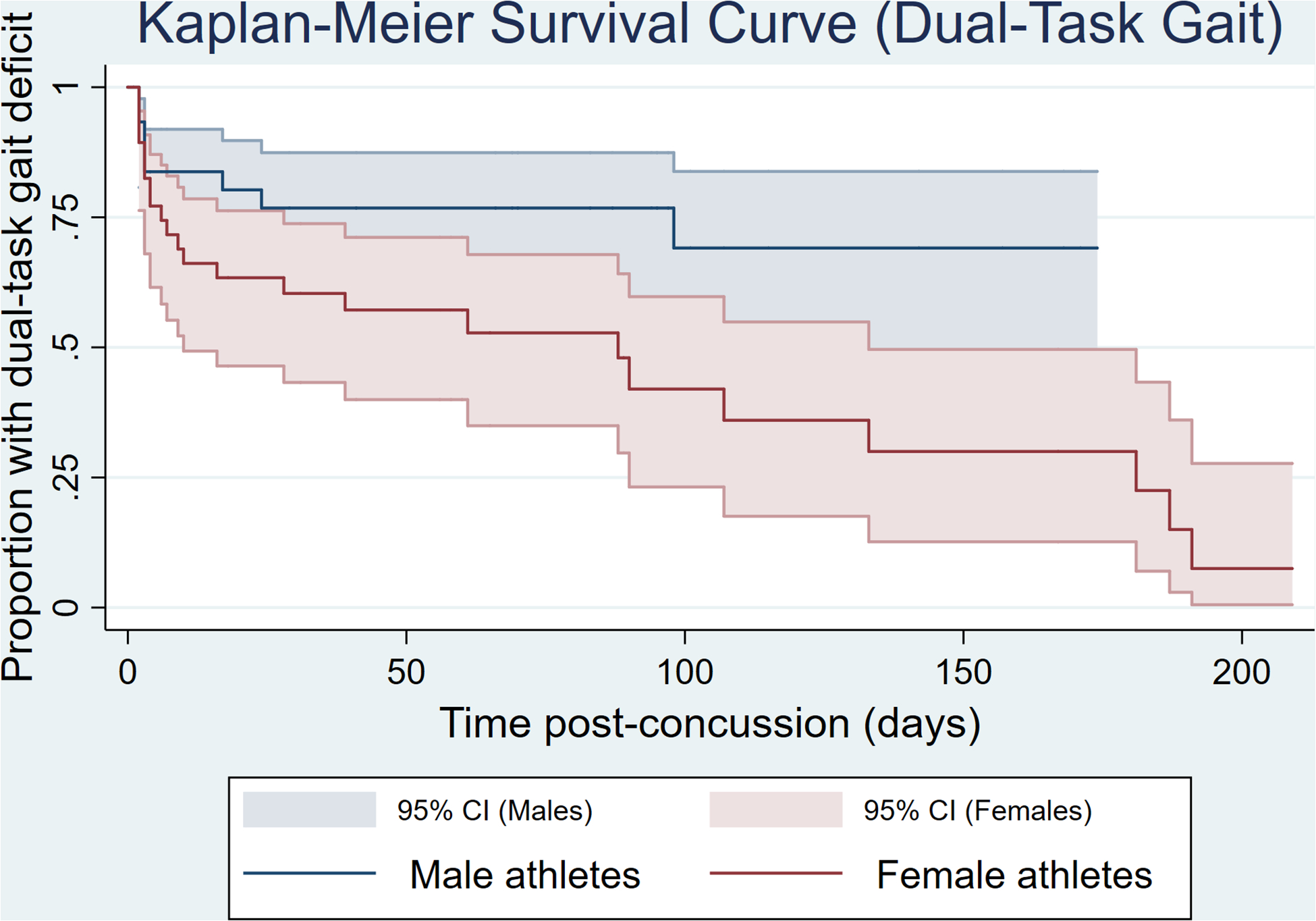
Kaplan-Meier Survival Curve for duration of time required for recovery of dual-task height-adjusted gait velocity.
Figure 3.
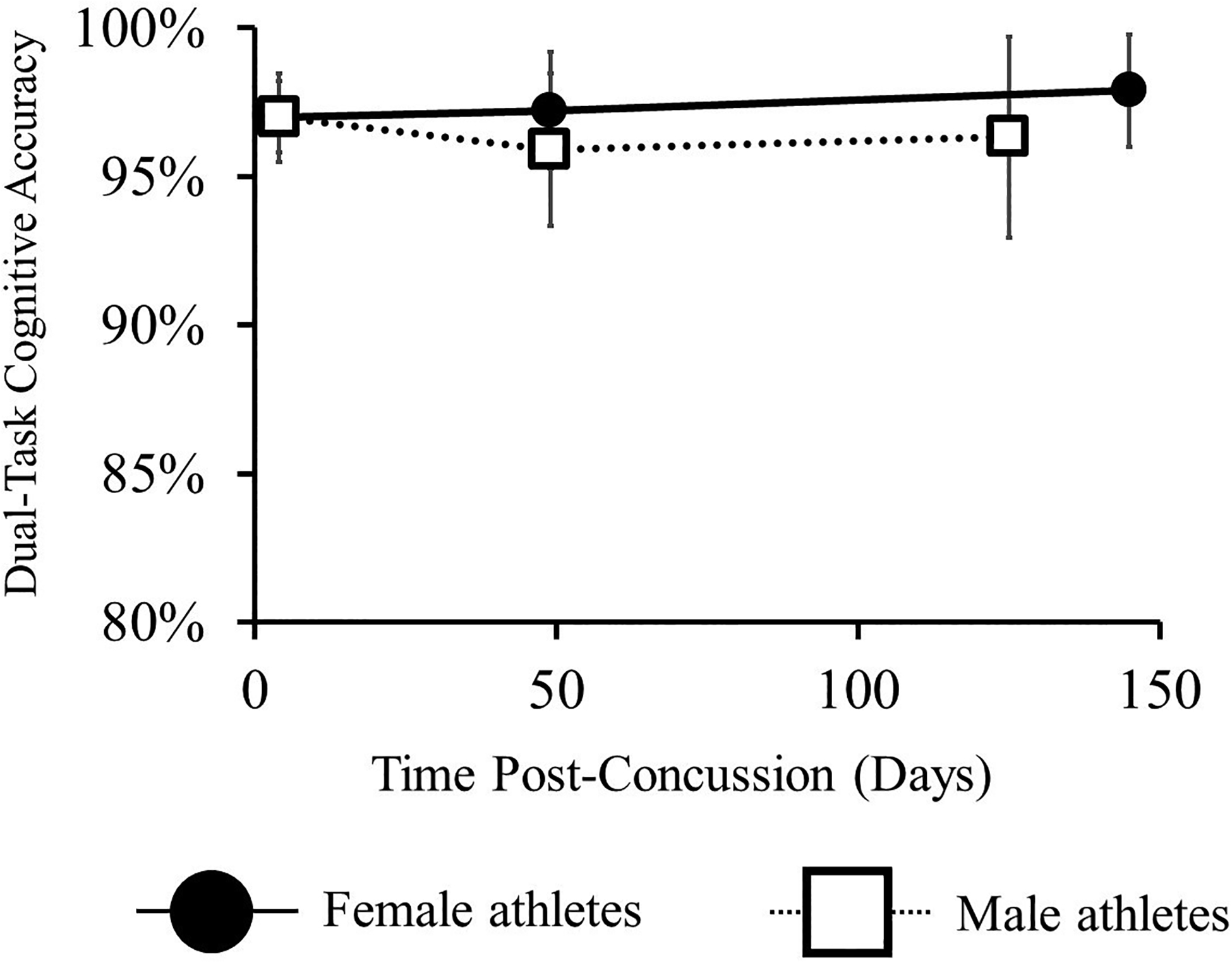
Cognitive accuracy data during dual-task gait for female and male athletes. Data presented as means, error bars represent 95% confidence intervals.
There were no significant associations between the predictor variables and height-adjusted single-task gait velocity recovery (Table 2). Both male sex and greater initial symptom severity rating were both independently associated with a longer dual-task gait recovery time (Table 2).
Table 2.
Multivariable analysis for single-task and dual-task height-adjusted gait speed recovery.
| Predictor Variable | Hazard Ratio | Standard Error | 95% Confidence Interval | P value |
|---|---|---|---|---|
| Model outcome: Height-adjusted single-task gait recovery | ||||
| Sex | 1.622 | 0.512 | 0.874, 3.013 | 0.13 |
| Age | 0.851 | 0.111 | 0.659, 1.099 | 0.22 |
| Prior history of concussion | 1.033 | 0.325 | 0.558, 1.914 | 0.92 |
| Initial symptom severity rating | 1.013 | 0.009 | 0.995, 1.032 | 0.15 |
| Loss of consciousness at time of injury | 0.291 | 0.216 | 0.068, 1.246 | 0.10 |
| Predictor Variable | Hazard Ratio | Standard Error | 95% Confidence Interval | P value |
| Model outcome: Height-adjusted dual-task gait recovery | ||||
| Sex* | 2.433 | 0.979 | 1.106, 5.352 | 0.02 |
| Age | 0.783 | 0.128 | 0.567, 1.079 | 0.14 |
| Prior history of concussion | 1.301 | 0.502 | 0.611, 2.772 | 0.50 |
| Initial symptom severity rating* | 1.029 | 0.011 | 1.007, 1.052 | 0.01 |
| Loss of consciousness at time of injury | 0.412 | 0.311 | 0.094, 1.808 | 0.24 |
Independently associated with height-adjusted dual-task gait recovery time.
Discussion
Contrary to our hypothesis and prior research examining post-concussion symptom recovery (4, 7), our findings indicate that male athletes were associated with a longer time from injury to dual-task gait recovery following concussion compared to female athletes. It is also possible that female athletes continued to improve throughout the testing timeline, while male athletes did not, and perhaps demonstrated some regression in dual-task abilities as documented previously among a group of athletes following concussion (30). In either case, recovery of functional abilities may therefore vary by sex following concussion and may need to be accounted for during further investigation and, perhaps, clinical assessments and return-to-play decision-making. Although the clinical significance of differences between sexes remains difficult to distinguish, our data add to the growing body of literature on this topic and suggest that further work to delineate the effects of individual factors on concussion recovery are needed.
Our data indicate that female athletes tended to walk with faster dual-task gait velocity at each subsequent assessment, while male athletes tended to maintain similar values at each time point. The reasons for this are not easily discernable. Using a task switching paradigm, researchers have reported that females outperform males, suggesting that females may possess better inherent simultaneous task execution abilities than males (31), similar to the demand imposed during a motor-cognitive dual-task paradigm. In this case, the ability of female athletes to perform a dual-task before the injury may have led them to demonstrate faster recovery than their male counterparts following concussion. However, other work using executive functioning and spatial ability test paradigms suggests that males outperform females (32). As such, the ability to perform a dual-task after concussion may be affected by sex, but concussion recovery is likely more complex and multifactorial, involving other aspects of function. Thus, in line with recommendations provided by leading medical organizations and consensus groups, recovery determination and return to play decision-making should be based upon a multimodal assessment of function that includes neurological status, self-reported symptoms, exercise tolerance, and gait and balance, neurocognitive, and oculomotor functions (1, 2).
Comparisons of locomotor behavior between healthy female and male young adults suggest that they walk at similar preferred walking speeds under single-task conditions (21). Our single-task data aligns with this observation, as we found that sex was not a significant predictor of single-task gait recovery following concussion. Thus, the addition of a secondary cognitive test during gait may increase the complexity of the task to a degree where differences are more apparent between sexes. The lack of sex-specific normative data, however, limits these comparisons. By using height-adjusted gait velocity thresholds rather than unadjusted values, we believe that this limitation was mitigated to some degree. For example, a dual-task adjusted gait velocity of 0.56 m·s−1/m may reflect someone who is 1.75 m tall and walks at 0.975 m·s−1 during dual-task conditions. Walking at or below this threshold may represent the lack of complete recovery. While the clinical ramifications of this incomplete recovery have not yet been fully elucidated, our previous work suggests it may be associated with an increased risk for further injury upon returning to sport (30, 33). Nonetheless, the lack of sex-specific normative data remains a limitation of our study. Although gait speed is a useful clinical measure that is reliable and correlates with functional abilities and balance confidence (34), there may be other measures of gait that better reflect balance control. Previously, researchers have used other measures such as whole body center-of-mass movement, trunk dynamic stability, or kinematic characteristics during a turning task to assess concussion recovery across time (9, 10). As such, these approaches may allow clinicians to better determine if physiological restoration of the brain after a concussion has occurred, and would lead to more informed and evidence-based return to play decisions.
Our findings align with several prior studies reporting that greater symptom severity acutely post-concussion is associated with a longer time to recovery (4, 20, 26, 29). Each of these prior studies, however, used symptom resolution as their primary recovery outcome variable. Our data extend these previous observations by suggesting that greater acute post-injury symptom severity is associated with a longer time to dual-task gait velocity recovery. As such, greater symptom severity after concussion may reflect a more severe injury overall, and expectations for recovery of both symptoms and dual-task abilities may be discussed early on with patients who report high levels of initial post-injury symptoms.
Interestingly, a relatively high percentage of all participants, and male athletes in particular, never achieved dual-task gait velocity recovery with the established thresholds we used in our investigation. Given that the mean time from injury to symptom resolution was approximately 19 days in our study cohort, the vast majority of athletes were cleared to return to sport during their participation within the longitudinal assessment timeline. Thus, it is possible that dual-task gait deficits, which are not tested as a part of most clinical concussion assessment batteries, continue to persist after symptom resolution and reintegration into sports. Recent meta-analytic work suggests that there is a significantly higher odds of sustaining a lower extremity MSK injury after clearance from a recent concussion when compared to healthy control athletes (35, 36). Researchers have theorized that continual physiological deficits may exist upon return to play clearance, as current clinical tests are not equipped to fully encapsulate concussion recovery, leading to an increased injury risk (37, 38). Given that attentional and neuromuscular control deficits relate to increased acute sport-related injury risk independent of a concussion (39, 40), attentional and/or neuromuscular deficits after concussion may lead to post-concussion MSK injuries. In line with this hypothesis, our previous work has demonstrated an association between worsening post-concussion dual-task gait and MSK injury (30). Therefore, as the full clinical implications of our findings will require further investigation, determining risk of re-injury following clearance to return to play after concussion is likely multifactorial and challenging to assess. Both sex (41) and dual-task gait abilities (30) may be individual factors that can help to determine this risk in future work.
Our study had limitations and our findings should be interpreted in light of them. Our participants were comprised of a group of varsity intercollegiate athletes at a single institution. Therefore, generalizations of our findings to other age groups, levels of play, or geographical locations should be made cautiously. We also had a relatively small number of female and male athletes who were injured during like sports (e.g. soccer, basketball, ice hockey). As a result, a large portion of the sample was injured during different types of sports, making the determination of biological differences between female and male athletes difficult. Given that cognitive-motor deficits may persist after symptom resolution (10), including athletes at the first assessment who had already recovered may have helped to better determine the utility of standardized gait velocity as a recovery marker. Finally, there are many individual characteristics beyond sex that may influence concussion recovery trajectories. Multifaceted approaches that account for these variables will lead to more robust clinical applications.
In conclusion, contrary to our hypothesis, we observed that male sex was independently associated with slower dual-task gait velocity recovery following a sport-related concussion. Thus, functional dual-task abilities after concussion may be affected differentially by sex. Further work investigating the individual factors that affect concussion recovery using objective outcomes to determine recovery is needed.
Funding Sources and Conflicts of interest disclosure:
Research reported in this work was supported by the National Institute of Neurological Disorders And Stroke of the National Institutes of Health under Award Number R01NS100952. Unrelated to this work, Dr. Howell has received research support from the National Institutes of Health (R03HD094560 and R41NS103698). Dr. Meehan receives royalties from 1) ABC-Clio publishing for the sale of his books, Kids, Sports, and Concussion: A guide for coaches and parents, and Concussions; 2) Springer International for the book Head and Neck Injuries in the Young Athlete and 3) Wolters Kluwer for working as an author for UpToDate. His research is funded, in part, by philanthropic support from the National Hockey League Alumni Association through the Corey C. Griffin Pro-Am Tournament and a grant from the National Football League. The remaining authors have conflicts to disclose.
Footnotes
Conflict of Interest
Unrelated to this work, Dr. Howell has received research support from the National Institutes of Health (R03HD094560 and R41NS103698). Dr. Meehan receives royalties from 1) ABC-Clio publishing for the sale of his books, Kids, Sports, and Concussion: A guide for coaches and parents, and Concussions; 2) Springer International for the book Head and Neck Injuries in the Young Athlete and 3) Wolters Kluwer for working as an author for UpToDate. His research is funded, in part, by philanthropic support from the National Hockey League Alumni Association through the Corey C. Griffin Pro-Am Tournament and a grant from the National Football League. The remaining authors have conflicts to disclose. The results of the present study do not constitute endorsement by ACSM. The results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation.
References
- 1.McCrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. 2017;51(11):838–47. [DOI] [PubMed] [Google Scholar]
- 2.Harmon KG, Clugston JR, Dec K, et al. American Medical Society for Sports Medicine position statement on concussion in sport. Br J Sports Med. 2019;53(4):213–25. [DOI] [PubMed] [Google Scholar]
- 3.Toledo E, Lebel A, Becerra L, et al. The young brain and concussion: imaging as a biomarker for diagnosis and prognosis. Neurosci Biobehav Rev. 2012;36(6):1510–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Iverson GL, Gardner AJ, Terry DP, et al. Predictors of clinical recovery from concussion: a systematic review. Br J Sports Med. 2017;51(12):941–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zuckerman SL, Lee YM, Odom MJ, Solomon GS, Forbes JA, Sills AK. Recovery from sports-related concussion: Days to return to neurocognitive baseline in adolescents versus young adults. Surg Neurol Int. 2012;3:130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Abrahams S, Fie SM, Patricios J, Posthumus M, September AV. Risk factors for sports concussion: an evidence-based systematic review. Br J Sports Med. 2014;48(2):91–7. [DOI] [PubMed] [Google Scholar]
- 7.Resch JE, Rach A, Walton S, Broshek DK. Sport Concussion and the Female Athlete. Clin Sports Med. 2017;36(4):717–39. [DOI] [PubMed] [Google Scholar]
- 8.NOT-OD-18–014: Revision: NIH Policy and Guidelines on the Inclusion of Women and Minorities as Subjects in Clinical Research[date unknown]; [cited 2018 Jan 9] Available from: https://grants.nih.gov/grants/guide/notice-files/NOT-OD-18-014.html.
- 9.Fino PC, Parrington L, Pitt W, et al. Detecting gait abnormalities after concussion or mild traumatic brain injury: A systematic review of single-task, dual-task, and complex gait. Gait Posture. 2018;62:157–66. [DOI] [PubMed] [Google Scholar]
- 10.Büttner F, Howell DR, Ardern CL, et al. Concussed athletes walk slower than non-concussed athletes during cognitive-motor dual-task assessments but not during single-task assessments 2 months after sports concussion: a systematic review and meta-analysis using individual participant data [Internet]. Br J Sports Med. 2019; doi: 10.1136/bjsports-2018-100164. [DOI] [PubMed] [Google Scholar]
- 11.Plummer P, Eskes G. Measuring treatment effects on dual-task performance: a framework for research and clinical practice. Front Hum Neurosci. 2015;9:225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Register-Mihalik JK, Littleton AC, Guskiewicz KM. Are divided attention tasks useful in the assessment and management of sport-related concussion? Neuropsychol Rev. 2013;23(4):300–13. [DOI] [PubMed] [Google Scholar]
- 13.Howell DR, Osternig LR, Chou LS. Detection of acute and long-term effects of concussion: dual-task gait balance control vs. computerized neurocognitive test. Archives of Physical Medicine and Rehabilitation. 2018;99(7):1318–24. [DOI] [PubMed] [Google Scholar]
- 14.Berkner J, Meehan WP, Master CL, Howell DR. Gait and Quiet-Stance Performance Among Adolescents After Concussion Symptom Resolution. J Athl Train. 2017;52(12):1089–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Howell DR, Oldham JR, DiFabio M, et al. Single-task and dual-task gait among collegiate athletes of different sport classifications: implications for concussion management. J Appl Biomech. 2017;33(1):24–31. [DOI] [PubMed] [Google Scholar]
- 16.Schmidt JD, Register-Mihalik JK, Mihalik JP, Kerr ZY, Guskiewicz KM. Identifying Impairments after concussion: normative data versus individualized baselines. Med Sci Sports Exerc. 2012;44(9):1621–8. [DOI] [PubMed] [Google Scholar]
- 17.Howell DR, Buckley TA, Berkstresser B, Wang F, Meehan WP. Identification of Post-Concussion Dual-Task Gait Abnormalities Using Normative Reference Values. J Appl Biomech. 2019;1–23. [DOI] [PubMed] [Google Scholar]
- 18.DiFazio M, Silverberg ND, Kirkwood MW, Bernier R, Iverson GL. Prolonged Activity Restriction After Concussion: Are We Worsening Outcomes? [Internet]. Clin Pediatr (Phila). 2015; doi: 10.1177/0009922815589914. [DOI] [PubMed] [Google Scholar]
- 19.Baker JG, Leddy JJ, Darling SR, Shucard J, Makdissi M, Willer BS. Gender Differences in Recovery From Sports-Related Concussion in Adolescents. Clin Pediatr (Phila). 2016;55(8):771–5. [DOI] [PubMed] [Google Scholar]
- 20.Zemek R, Barrowman N, Freedman SB, et al. Clinical risk score for persistent postconcussion symptoms among children with acute concussion in the ED. JAMA. 2016;315(10):1014–25. [DOI] [PubMed] [Google Scholar]
- 21.Bruening DA, Frimenko RE, Goodyear CD, Bowden DR, Fullenkamp AM. Sex differences in whole body gait kinematics at preferred speeds. Gait & Posture. 2015;41(2):540–5. [DOI] [PubMed] [Google Scholar]
- 22.Smith LK, Lelas JL, Kerrigan DC. Gender differences in pelvic motions and center of mass displacement during walking: stereotypes quantified. J Womens Health Gend Based Med. 2002;11(5):453–8. [DOI] [PubMed] [Google Scholar]
- 23.Lovell MR, Iverson GL, Collins MW, et al. Measurement of symptoms following sports-related concussion: reliability and normative data for the post-concussion scale. Appl Neuropsychol. 2006;13(3):166–74. [DOI] [PubMed] [Google Scholar]
- 24.Howell DR, Osternig LR, Chou L-S. Adolescents demonstrate greater gait balance control deficits after concussion than young adults. Am J Sports Med. 2015;43(3):625–32. [DOI] [PubMed] [Google Scholar]
- 25.Howell DR, Beasley M, Vopat L, Meehan W. The effect of prior concussion history on dual-task gait following a concussion. J Neurotrauma. 2017;34(4):838–44. [DOI] [PubMed] [Google Scholar]
- 26.Meehan WP, Mannix RC, Monuteaux MC, Stein CJ, Bachur RG. Early symptom burden predicts recovery after sport-related concussion. Neurology. 2014;83(24):2204–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chermann JF, Klouche S, Savigny A, Lefevre N, Herman S, Bohu Y. Return to Rugby After Brain Concussion: A Prospective Study in 35 High Level Rugby Players [Internet]. Asian Journal of Sports Medicine. 2014. [cited 2019 Apr 29];5(4) available from: http://asjsm.com/en/articles/21600.html. doi: 10.5812/asjsm.24042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dudley WN, Wickham R, Combs N. An Introduction to Survival Statistics: Kaplan-Meier Analysis. J Adv Pract Oncol. 2016;7(1):91–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Meehan WP, Mannix RC, Stracciolini A, Elbin RJ, Collins MW. Symptom severity predicts prolonged recovery after sport-related concussion, but age and amnesia do not. J Pediatr. 2013;163(3):721–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Howell DR, Buckley TA, Lynall RC, Meehan III WP. Worsening dual-task gait costs after concussion and their association with subsequent sport-related injury. Journal of Neurotrauma. 2018;35(14):1630–6. [DOI] [PubMed] [Google Scholar]
- 31.Stoet G, O’Connor DB, Conner M, Laws KR. Are women better than men at multi-tasking? BMC Psychology. 2013;1(1):18. [Google Scholar]
- 32.Mäntylä T Gender Differences in Multitasking Reflect Spatial Ability. Psychol Sci. 2013;24(4):514–20. [DOI] [PubMed] [Google Scholar]
- 33.Howell DR, Lynall RC, Buckley TA, Herman DC. Neuromuscular control deficits and the risk of subsequent injury after a concussion: a scoping review. Sports Med. 2018;48(5):1097–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Fritz SP, Lusardi MP. White Paper: “Walking Speed: the Sixth Vital Sign.” Journal of Geriatric Physical Therapy 2009. 2009;32(2):2–5. [PubMed] [Google Scholar]
- 35.McPherson AL, Nagai T, Webster KE, Hewett TE. Musculoskeletal Injury Risk After Sport-Related Concussion: A Systematic Review and Meta-analysis. Am J Sports Med. 2018;363546518785901. [DOI] [PubMed] [Google Scholar]
- 36.Reneker JC, Babl R, Flowers MM. History of concussion and risk of subsequent injury in athletes and service members: A systematic review and meta-analysis [Internet]. Musculoskeletal Science and Practice. 2019. [cited 2019 Apr 22]; available from: http://www.sciencedirect.com/science/article/pii/S2468781218304260. doi: 10.1016/j.msksp.2019.04.004. [DOI] [PubMed] [Google Scholar]
- 37.Lynall RC, Mauntel TC, Padua DA, Mihalik JP. Acute lower extremity injury rates increase after concussion in college athletes. Med Sci Sports Exerc. 2015;47(12):2487–92. [DOI] [PubMed] [Google Scholar]
- 38.Fino PC, Becker LN, Fino NF, Griesemer B, Goforth M, Brolinson PG. Effects of Recent Concussion and Injury History on Instantaneous Relative Risk of Lower Extremity Injury in Division I Collegiate Athletes [Internet]. Clin J Sport Med. 2017; doi: 10.1097/JSM.0000000000000502. [DOI] [PubMed] [Google Scholar]
- 39.Guy JA, Knight LM, Wang Y, Jerrell JM. Factors associated with musculoskeletal injuries in children and adolescents with attention-deficit/hyperactivity disorder [Internet]. Prim Care Companion CNS Disord. 2016;18(3) doi: 10.4088/PCC.16m01937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Read PJ, Oliver JL, De Ste Croix MBA, Myer GD, Lloyd RS. Neuromuscular risk factors for knee and ankle ligament injuries in male youth soccer players. Sports Med. 2016;46(8):1059–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Houston MN, Hoch JM, Cameron KL, Abt JP, Peck KY, Hoch MC. Sex and number of concussions influence the association between concussion and musculoskeletal injury history in collegiate athletes. Brain Inj. 2018;1–6. [DOI] [PubMed] [Google Scholar]