

Abstract
Natural disasters are the result of a hazard overwhelming highly vulnerable community, often resulting in mortality and morbidity. Over the past decade, over 300 natural disasters occur yearly around the world affecting millions and cost billions. The disaster cycle is a framework used to base a coordinated plan to respond, recover, prevent, and prepare for a disaster. Access to clean water, proper sanitation, food/nutrition, shelter, and the threat of communicable diseases are concerns that have the potential to be detrimental to the management of a natural disaster, slowing the recovery process.
Keywords: Disasters, Hazards, Management, Natural, Preparedness, Public health, Response, Risk, Trends, Vulnerability
Glossary
- Biological disaster
Disasters originating from biological hazards such as the threat of an epidemic.
- Geophysical disaster
Disasters originating from geophysical hazards that are related to changes due to tectonic plates or fault shifting as well as mass movement of solid mass.
- Hazard
Anything that causes harm to life or destruction property and environment.
- Hydrometerological disaster
Disasters originating from hydrometerological hazards related to the climate, oceans, or movement of wet mass such as floods, droughts, and heat waves.
- Natural disaster
The overwhelming consequences of a natural hazard. Typically associated with resource depletion, mortality, and morbidity.
- Vulnerability
The degree to which an individual/community/country is capable of coping with the effects of a hazard.
Introduction
The 2004 Indian Ocean tsunami, 2010 earthquake in Haiti, and the 2011 tsunami in Japan are just a few of the natural disasters that have significantly made historic impact on the world in the past decade. Together, these disasters accounted for 471 346 deaths, costing hundreds of billions of dollars (CRED, 2012; U.N. ISDR, 2011). But these events are just a few among the hundreds of natural disasters that occur yearly around the world crippling economies, devastating crops, and displacing millions. The threat of natural disasters continues as population levels are on rise, climates are shifting, and economic instability persists, making populations more vulnerable to hazards. However, proper assessments of potential disaster impact, management strategies, and efficient use of resources can mitigate the effects of disasters or even potentially prevent them.
The topic of natural disasters is broad and highly compassing, drawing experts from all disciplines to comprehend the science, as well as methods of coping with the devastating consequences. Given the recent emergence of natural events in the past few decades, large organizations such as the World Health Organization (WHO) and the United Nations have devoted considerable effort to research and education surrounding natural disasters. The United Nations International Strategy for Disaster Reduction (UNISDR), created in 1999 with the mandate of spearheading and coordinating disaster risk reduction, is an example of increased attention to disaster reduction.
The purpose of this article is to provide further insight on natural disasters by supporting the work of the established organizations like the United Nations and WHO. Specifically, summarizing current theory, trends and management strategies will be covered in addition to identifying myths that continue to hinder appropriate disaster procedure.
Hazard versus Disaster
While most hazards may be inevitable, disasters are not.
It is important to begin this article by differentiating between a hazard and a disaster because it is often used synonymously and therefore erroneously. A hazard is any phenomena, physical event, or human behavior (floods, hurricanes, droughts, epidemics, nuclear spills, etc.) that can result in harm to humans, destruction of property, social disruption, or environmental degradation (U.N. ISDR, 2004). A disaster, on the other hand, is the potential consequence of a hazard, where a community or population is unable to handle the effects of the hazard, given the resources at their disposal. Although distinct from each other, Figure 1 shows the conceptualization of how a hazard relates to a disaster given the ability of a population to utilize available resources. So as stated by the ISDR in the above quote, a hazard may be an event that will occur regardless of human effort, but with what will be discussed further in detail this article, the impact of a disaster could be reduced or even prevented.
Figure 1.
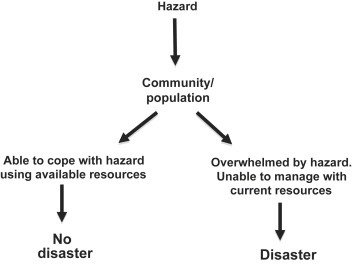
Differentiating between a hazard and a disaster.
Although it is understood that once a community is overwhelmed by a hazard, the likelihood of a disaster is high, the classification of a disaster may not be so clear, so the question remains: What exactly must occur for a disaster to be declared? The Center for Research on the Epidemiology of Disasters, a collaborator of WHO's initiative: Global Program for Emergency Preparedness and Response, has developed a classification system for declaring a disaster. Although this classification standardizes the definition of a disaster it is important to understand that different communities and countries will experience mortality, morbidity, and resource depletion in different capacities.
Classification of a Disaster – If any of the following criteria are met after an event, it is classified as a disaster (Guha-Sapir et al., 2012):
-
•
10 or more people reported killed;
-
•
100 or more people reported affected;
-
•
Declaration of state of emergency;
-
•
Call for international assistance.
Types of Disasters
The type of hazard from which they are rooted, typically defines disasters; therefore in order to understand the different types of disasters, it is important to establish the hazards that they originate from. Hazards are grouped into three categories: technological, natural, and environmental degradation hazards (U.N. ISDR, 2004). Technological hazards are industrial (pollution), nuclear (nuclear leak), or structural (dam collapse), while environmental degradation hazards include events that disrupt the environment, ecosystem, or natural resources (i.e., deforestation, forest fires, change in climate). Both technological hazards and environmental degradation hazards are the result of human behavior while natural hazards are events that are a direct result of natural processes. Natural hazards are the focal point of this article and are further categorized into hydrometerological, geological, and biological. Hydrometerological hazards, the most common natural hazards, are related to the climate, oceans, or movement of wet mass such as floods, droughts, and heat waves like the 2010 Russian heat wave (resulted in a disaster that claimed 56 000 lives (U.N. ISDR, 2011)). Geological hazards involve changes due to tectonic plates or fault shifting (tsunamis result from shifting of faults) or mass movement of solid mass. Biological hazards are events that involve the rapid incidence and prevalence of vector-driven diseases, toxins, or pathogens. The emergence of severe acute respiratory syndrome in 2003 is an example of a biological hazard that resulted in disastrous effects (spread through air travel), killing over 400 people (U.N. ISDR, 2004).
Figure 2 is a classification of hazards adopted and modified from the UNISDR, showing the three categories of hazards, focusing on natural disasters (U.N. ISDR, 2004). Additionally, the figure displays that although separate components of natural disasters, hydrometerological, geological, and biological disasters can interact. For example, floods and droughts can create a prime environment for biological hazards through vector-borne illnesses, such as cholera and malaria (U.N. ISDR, 2004).
Figure 2.
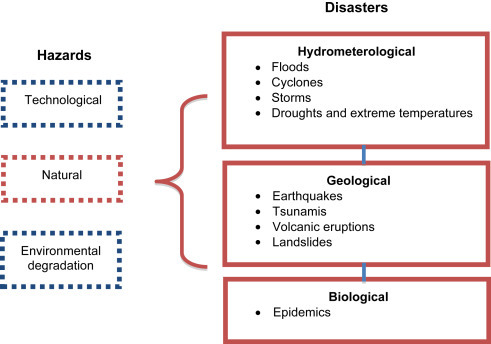
Classification of hazards and natural disasters.
Are Natural Disasters Increasing?
Over the past decade, natural disasters have become topical in the media prompting many people to grow in concern of whether the incidence of natural disasters is increasing. Figure 3 provides a visual understanding of the number of natural disasters that have occurred between 2000 and 2011 and although a slight downward trend, for the past 10 years between 350 and 550 reported natural disasters every year. The average number of disaster to occur per year between 2001 and 2010 was 384, while the average number in 2011 was 302 (CRED, 2012). Interestingly, despite a slight decrease in the reported number of natural disasters, Figure 4 shows that the number of deaths per year due to natural disasters is slightly increasing. Furthermore, the average yearly economic impact of natural disaster in 2011 of US$366 billion far exceeds the decade average of US$108 billion (CRED, 2012). Both figures imply that when quantifying natural disasters, it is important to not only observe the frequency, but severity, in terms of deaths and economic impact, as well.
Figure 3.
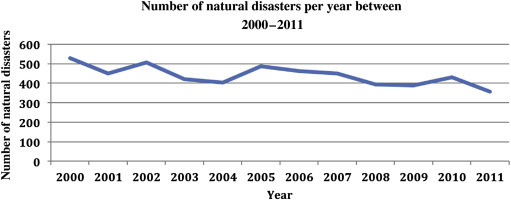
Number of natural disasters per year between 2000 and 2011.
EM-DAT: The OFDA/CRED International Disaster Database – www.emdat.net – Université catholique de Louvain – Brussels–Belgium.
Figure 4.
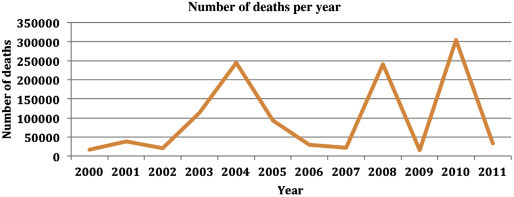
Number of deaths due to natural disasters per year between 2000 and 2011.
EM-DAT: The OFDA/CRED International Disaster Database – www.emdat.net – Université catholique de Louvain – Brussels–Belgium.
Disasters That Cause the Greatest Impact
According to the United Nations, 2010 marked the ‘deadliest year in at least two decades’ as approximately 373 natural disasters claimed nearly 300 000 lives, costing US$110 billion (U.N. ISDR, 2011). Among the highest contributors of mortality was the earthquake that rattled Haiti on 12 January 2010 resulting in 225 500 lives lost. Table 1 provides the list of the top five most common natural disasters that occurred between 2000 and 2011. Floods and storms topped the list with over 3000 events; however, the most common natural disasters may not cause the most destruction, as the leading cause of deaths was the result of earthquakes with over 700 000 deaths (Table 2 ). Moreover, earthquakes and storms carried a substantial economic cost between 2000 and 2011, with a combined price tag of nearly US$1 trillion (Table 3 ).
Table 1.
Top five most common natural disasters between 2000 and 2011
| Disaster | Number of events |
|---|---|
| Flood | 2066 |
| Storms | 1231 |
| Epidemic | 666 |
| Earthquake | 344 |
| Extreme temperature | 265 |
EM-DAT: The OFDA/CRED International Disaster Database – www.emdat.net – Université catholique de Louvain – Brussels–Belgium.
Table 2.
Top five natural disasters causing mortality between 2000 and 2011
| Disaster | Number of deaths |
|---|---|
| Earthquake | 701 307 |
| Storm | 176 822 |
| Extreme temperature | 148 684 |
| Epidemic | 72 234 |
| Flood | 68 685 |
EM-DAT: The OFDA/CRED International Disaster Database – www.emdat.net – Université catholique de Louvain – Brussels–Belgium.
Table 3.
Top five most costly natural disasters between 2000 and 2011
| Disaster | Cost, $ (US billion) |
|---|---|
| Storm | 545 |
| Earthquake | 450 |
| Flood | 285 |
| Extreme temperature | 38 |
| Drought | 35 |
EM-DAT: The OFDA/CRED International Disaster Database – www.emdat.net – Université catholique de Louvain – Brussels–Belgium.
The mortality and financial cost of a natural disaster is certainly linked to the severity of the hazard, but also dependent on how vulnerable a population is to potential disastrous effects. The next section will explain why the risk of a hazard becoming a disaster is contingent on several variables, many of which are based on human lifestyle.
What Is the Risk of a Natural Disaster?
The risk of a natural disaster occurring is the product of the severity of the hazard present and the vulnerability of the population at risk. Vulnerability is the concept defined by the WHO as a “predisposition to suffer damage due to external events” (Inter-American Development Bank, 1999). Essentially, it is a condition or set of conditions increases vulnerability if it hinders a population from coping with a hazard; thus promoting conditions for a disaster. As defined by the United Nations, vulnerability is the culmination of four factors: social, environmental, physical, and economic, each contributing to the vulnerability of a population alone or by interacting with each other (U.N. ISDR, 2004). An example of vulnerability can be a population residing on an island below sea level near a fault line (physical factor). This population is identified as vulnerable because a hazard exists (earthquake and potential tsunami) and they are isolated from mainland resources. Interacting factors can also contribute to increasing vulnerability. Financial strain (economic) brought on by a corrupt government (social) can increase the vulnerability to a hazard and therefore increase the risk of a natural disaster (Inter-American Development Bank, 1999).
Rapid urbanization considerably increases the vulnerability to hazards (UNDP, 2004). When the population of a city grows too quickly, building adequate infrastructure and basic settlements becomes a challenge. Poor housing and shanty communities pose significant risks as protection against even small hazards becomes compromised. Large populations create social economic disparities resulting in reduced access to resources (UNDP, 2004). The 2011 United Nations World Urbanization Prospects report explains that nearly 60% of the most populous cities in the world are exposed to a high-risk natural hazard (World health Organization, 2012).
Variability of Disasters and Vulnerability
This article focuses on the term disaster, defined above as a situation where a community or country's resources are exceeded by the demand created by an event – this can occur in many ways. Natural disasters vary drastically in terms of the impact that it creates on individuals, society, as well as government. One natural event may create destruction differently than another natural event (i.e., a tornado is entirely different from an earthquake). Not only do natural events vary, but the vulnerability of populations or communities can also differ. A severe natural event that rips through an open, unpopulated area may not be disastrous whereas a mild natural event that goes through a heavily populated city could, indeed, create a situation where the community is overwhelmed. Additionally, the resources available, (as well as methods of resource access), financial stability, and type of governing bodies significantly differ between communities and countries thus impacting the severity of the natural event. Given the high variability of natural disasters, as well as varying vulnerability, managing disasters is certainly unique to the parameters of the situation.
Disaster Management
There is no gold standard method for managing a natural disaster. Total prevention of all disasters is not possible; however, the goal of management strategists following a disaster is to help as many people as possible using the resources available. Learning from past experiences, as well as learning from other communities is imperative in reducing the impact of future disasters.
Many countries have developed emergency management strategies to cope with broad-range unforeseeable events, including natural disasters. Figure 5 is a modified version of the disaster management cycle from WHO that outlines four phases in the management of an emergency. The purpose of the disaster cycle is to conceptualize the processes that occur following a disaster so that effective planning strategies can be developed.
Figure 5.

Disaster cycle.
Each country or jurisdiction may have different management strategies for each type of emergency; however, the disaster cycle is a well-established framework that provides the basis for developing a strategy. Below is a summary of the four phases in the disaster cycle, described in further detail in WHO Environmental Health in Emergencies and Disasters: A Practical Guide (Wisner and Adam, 2002).
Emergency Response
Emergency response is a series of crucial tasks that are concurrently undertaken during a time of turmoil, instability, and fear; therefore this phase is heavily dependent on proper preparedness and planning. The main objective for the emergency response component of the disaster cycle is to locate the necessary resources to maintain and preserve life in the coming days or weeks. Natural disaster responses will vary depending on the type and severity of the disaster itself; however, governing bodies work closely with medical staff to utilize the skills and detailed plans established in the preparedness phase of the cycle to execute an appropriate response.
The first 3 days following a natural disaster are considered the ‘crucial period’ as this time frame is critical for finding survivors who are without food or aid (Sheu, 2007). Communication with primary care providers is pivotal for administering proper care. Following a disaster, many health-care providers flock to disaster zones with exorbitant amounts of medical supplies; however, a poorly coordinated response plan may result in wasted supplies and skilled labor (Wasay and Shafqat, 2006). Additionally, communication between health care providers and community leaders is important, as ignoring local cultural practices may hinder the response process (Wasay and Shafqat, 2006).
Interestingly, after a disaster strikes, immediate aid is often administered by surviving members of the community (Noji, 2005). The strength of community members in their altruistic attempt to help another human being is commonly witnessed during disasters and is certainly underreported. First responders who assess the situation usually handle the coordination of a natural event and request further assistance from government once the event has been assessed as a disaster.
Immediately following a natural event that has disaster potential, preliminary aid in the form of food, water, sanitation, and shelter is the main objective in this phase, but equally important could also be aid in the form of minor structural repairs. Amidst the chaos, assessment of the potential disaster is where officials rapidly determine how bad the event is and it is here where the potential disaster may be termed a disaster. The assessment allows officials to mobilize initial resources and aid in addition to analyzing whether national or even international assistance may be necessary.
Humanitarian aid following a disaster is the primary source of funding during a disaster (Fink and Redaelli, 2011). The U.N. Office for the Coordination of Humanitarian Affairs organizes the relief effort, following a formal request from the affected country (Krin et al., 2010). Funds from the U.N come in three types to help in the response phase: Central Emergency Response Fund, Common Humanitarian Funds, and Emergency Response Funds (OCHA, 2012). Despite well-coordinated relief efforts, as well as generous outpouring of international aid, humanitarian aid can become scarce. Following a disaster, roads may not be safe, traditional airports may be out of commission and storage facilities could also be destroyed; therefore a substantial delay in time between aid deployment and getting it to those who need often occurs (Krin et al., 2010).
Recovery
While the objective in the response phase of the disaster cycle is to contain the catastrophic effects of the event, the recovery phase brings order to the shocked system swirling in entropy. The initial needs of water, shelter, sanitation, and food addressed in the response phase are further established through activities, programs, and initiatives to provide stability and foundation for those uprooted. But beyond on the physical aid, recovery plans contain efforts to cope with the economic and social strife that resulting from the disaster. Loss of life can create devastating consequences for broken families long after the events of the disaster; therefore, programs must be in place to provide social support for those affected.
Prevention/Mitigation
Full prevention of a disaster is highly unlikely, but steps can be taken to prevent small hazards from becoming disasters (prevention) or reduce the impact and devastation resulting from a disaster (mitigation). With respect to large nation and international disaster prevention organizations like the United Nations, we are starting to see a shift from recovery and response focus to a devotion to prevention and mitigation.
WHO suggests proper hazard and vulnerability assessments be done during this phase to identify key areas that could potentially create a disastrous situation (Wisner and Adam, 2002). An example of prevention measures would be building levees to prevent high-flowing rivers from flooding while mitigation could be an effective warning system. The Board on Natural Disaster of the National Research Council has outlined four mitigation strategies (BOND, 1999):
-
1.
Identify the location and nature of the potential hazard(s).
-
2.
Determine the characteristics of the population and structures that are vulnerable to the hazards.
-
3.
Determine an acceptable standard for levels of risk.
-
4.
Use mitigation strategies that are realistic and based on cost and benefit analysis.
Preparedness
According to WHO, the objective of disaster preparedness is to ensure that a community has the capability of bringing a system in turmoil from recovery to sustained development (World Health Organization, 1995). It is important that this phase integrates the assessment strategies from the prevention and mitigation phase to ensure readiness for a plethora of possible hazards.
Governmental policies are examples of activities that propel a community into disaster preparedness (Wisner and Adam, 2002). Legislation at the local and national level with well-established goals can substantially improve the response of a disaster. Examples of such policy include initiating public education programs focusing on informing the community about evacuation procedures, first aid, family emergency plans, as well as available resources. The Maldives is a good example of how good policy is implemented into a community as they utilize the strong association between schools and the community to disseminate emergency preparedness plans to students and their families (UNESCO, 2007). WHO provides a disaster-planning model that can be used at the local, national, and international level. This model includes 12 key steps to prepare for a potential hazard (Wisner and Adam, 2002):
-
1.
Identify potential hazard(s).
-
2.
Assess and discuss the needs that are likely going to be compulsory.
-
3.
Prioritize.
-
4.
Delegate responsibilities.
-
5.
Inventory of resources.
-
6.
Review steps 2–5.
-
7.
Look for areas of the system that may experience the greatest detriment.
-
8.
Confirm the priorities.
-
9.
Finalize the plan.
As an added measure, it would certainly benefit communities to encourage the practice of emergency plans at the individual, local, and even national level, if possible.
What Are Important Public Health Concerns after a Disaster?
Clean Water
Access to water is imperative to survival following disaster. During a disaster, 15–20 l of water per person is recommended (Noji, 2005; Sphere Project, 2000), which is often difficult to achieve. Many countries around the world struggle to supply drinking water to their citizens even when there is no disaster; therefore the sudden necessity to provide basic resources coupled with a natural disaster can be unfathomable. Contrary to natural though, it is has been shown that relative to smaller amounts of clean quality water, a larger quantity of moderate quality water is preferred (Wisner and Adam, 2002).
Proper Sanitation
Proper sanitation is important to disaster management because poor sanitation can be detrimental to relief efforts. Cross-contamination of food/water sources with fecal matter can result in diseases or infections such as diarrhea, cholera, and even typhoid. Urine is typically of little concern for cross-contamination. Garbage, old clothing, or even old bandages that are not properly contained can attract animals and vermin that have the potential to carry disease. Often, during a natural disaster, it is not the disaster that directly causes disease or epidemics, but the poor management of sanitation that puts victims in highly susceptible situations. Proper sanitation would include preserving the use of functional toilets, but utilizing sewage tankers if necessary. In extreme cases, the use of rivers or streams can be used, but is highly discouraged for waste disposal.
Food/Nutrition and Shelter
Food shortages during natural disasters are rare; however, if the main supply of food in the region is destroyed or the avenue in which food is supplied is hindered, food shortage can quickly become an issue (Noji, 2005).
Self housing is common and encouraged after a disaster, while tent villages, seen on television, are used in extreme situations and are not recommended since illness susceptibility is higher. Survivors find shelter among relatives or friends; however, sheltering following a natural disaster is of concern if survivors house themselves in structures that are not fit for occupancy anymore. Further casualty resulting from inadequate shelters should be a priority among emergency response officials. Tent settlements create health risks as these temporary shelters have sanitary limitations creating risk for disease and illness. Furthermore, occupants can sometimes use temporary tent settlements as a permanent home. This not only creates a health concern, but also increases the vulnerability to future hazards of those in the settlements.
Communicable Diseases
Communicable disease is an aspect of natural disasters that can be both overexercised by myth and completely disregarded. Poor hygiene and improper water, sanitation, and food supply strategies in addition to inadequate care of wounds and injuries can create an environment polluted with bacteria and viruses (Ligon, 2006). Described are common types of diseases associated with a natural disaster setting (Watson et al., 2007).
Water-related diseases: Include diarrheal diseases such as Escherichia coli and Salmonella, as well as hepatitis A and E.
Diseases associated with overcrowding: Measles, meningitis, and acute respiratory infections.
Vector-borne diseases: Malaria and dengue.
Other: Tetanus.
Fear of communicable diseases from the bodies of the deceased can certainly gain momentum during a disaster, as witnessed with mass cremations in the 2004 Indian Ocean tsunami. Currently, there is no evidence to support the notion that mass numbers of dead bodies from effects of disasters create epidemics (Pan American Health Organization, 2004) as most deaths from natural disasters are due to trauma rather than due to disease (Alexander, 1996). Furthermore, many forms of bacteria and viruses (even the most resistant kinds) are unable to survive in a dead body very long. As the body degrades, the temperature quickly drops, leaving an environment not conducive for bacteria or virus growth. Even though dead bodies pose little threat of epidemics during disasters, caution should be taken if the disaster takes place in an area prone to epidemics prior to the disaster. Not knowing the cause of death of a dead body can pose slight risk for those in direct contact if the death was due to an epidemic. HIV is a disease that can withstand the lower temperatures of a deceased body, lasting up to 16 days and therefore should be handled with extreme caution (Pan American Health Organization, 2004).
Myths about Natural Disasters
Once a natural disaster strikes, there is an enormous amount of immediate tasks and information that need to be conducted and sorted within a short period of time. Unfortunately, there are a number of mindsets that may contribute to hindering the time-sensitive processes required for maintaining the health and safety of those affected.
| Myth | Reality |
|---|---|
| Dead bodies are an immediate concern for the health and well-being of surrounding people. | It is widely shown in literature that dead bodies do not warrant a swift action to control for epidemics during a disaster (Morgan and De Goyet, 2005). Death due to trauma is not a health concern unless they are in direct contact with water or food supply. |
| Disasters kill at random. | Vulnerable populations and communities are those that suffer from disaster effects. |
| International volunteers are always needed. | Many communities are capable of assessing their needs themselves. International action should only be taken when they request it. |
| Rooting, rioting, and general misbehavior is highly common after disasters. | Altruism is often demonstrated during times of strife; however, there are always going to be certain cases of misbehavior. |
What to Do to Prepare for a Natural Disaster – Individually?
To conclude this article, it is fitting to provide information that can be useful during a disaster. Again, disasters are very unique and individual preparation should be catered toward the identifiable hazard with the most risk to the individual. The Centre for Disease Control (see Relevant Website) provides information for individuals in the event of a disaster and a few key strategies include the following:
-
1.
Identify the type of disasters that can occur in your area.
-
2.
Know the warning signals.
-
3.
Understand the disaster plans in work and school settings for yourself and family members.
-
4.
Determine how to turn the water, gas, and electricity off.
-
5.
Take a first aid course.
Summary
Natural disasters can strike with overwhelming power and create devastation that lasts for decades. Given the complexity of hazards and the dynamic components that make it a disaster, the field of natural disasters will continue to grow and remain a global issue. As a broad and multifaceted topic, there are several books, reports, and articles stemming from a variety of disciplines that describe a specific facet. This article provided a brief overview of the theory of natural disasters, trends, and management strategies, contributing to an emerging field.
A natural disaster is the result of a natural hazard wreaking havoc on a population to a point where resources become exhausted and mass mortality and morbidity occur. Despite preventative measures, as well as mitigation strategies, over 300 natural disasters occur around the world, yearly. Between 2000 and 2011, the most frequent natural disaster to strike was flooding while the highest mortality rates were attributed to earthquakes.
The risk of a disaster occurring is dependent on the severity of the threatening hazard as well as the vulnerability of the exposed population. Vulnerability is composed of social, environmental, economic, and physical factors that influence the degree to which a population is able to cope with a hazard. Rapid urbanization is of particular concern throughout the world, contributing to vulnerability as high population concentration, social disparity, and depletion of resources exacerbates susceptibility to disasters.
The disaster cycle is the description of a series of processes that occur from the time a disaster strikes, to the response and recovery of the disaster and through to the prevention, mitigation, and preparedness of future events. The purpose of disaster cycle is to conceptualize a disaster into relating components so that management strategies can be developed.
There are several public health concerns that affect survivors immediately following a natural disaster. Beyond the primary aid for trauma that is administered, adequate water, food, sanitation, and shelter are pivotal for the health and well-being of those affected. If these concerns are not met with proper procedures, a substantial risk for disease can arise. Additionally, further injuries or death from sheltering in dilapidated buildings with a compromised structure can exacerbate the relief efforts.
See also
Epidemic Investigation; Geographic Information Systems (GIS) in Public Health; Humanitarian Response to Complex Emergencies and Natural Disasters; Social Dimensions of Epidemics.
Biographies

Abhaya S. Prasad completed his Masters of Science in Epidemiology and currently holds a position as a Policy and Evaluation Consultant with the Ministry of Health in the Government of Alberta. He has worked on several projects with Dr Louis H. Francescutti in the subject area of injury prevention and health promotion. Such projects include the Coalition for Cellphone-Free Driving, as well as Injury Alberta.
Other research interests of Mr Prasad include concussion management, arthritis management, continuing care, and survey methodologies.

Dr Louis Hugo Francescutti is a native Montrealer who went west, fell in love with the open space and clear blue skies of Alberta and never left. Previously, he has worked as an emergency medical technician in the Arctic and as a professional photographer with a studio in Old Montreal.
For many Albertans, Dr Francescutti has become synonymous with public health and safety. He received his combined MD/PhD from the University of Alberta in 1987 and, while training as a general surgery resident, became fascinated with the subject of trauma. He went on to complete further studies in injury while doing a Masters of Public Health and a preventive medicine residency at Johns Hopkins University School of Public Health in Baltimore. He is a Fellow of the Royal College of Physicians and Surgeons of Canada and a Fellow of the American College of Preventive Medicine.
In 1995, he returned to Edmonton to become an emergency and preventive medicine physician at the Royal Alexandra Hospital. In that role, he continued to witness first hand the devastating impact of preventable injuries and made it his mission to continue to promote injury prevention. Over the past two and a half decades, Dr Francescutti spearheaded a number of public safety awareness initiatives and campaigns, including the development of an award winning multimedia injury prevention program for teens called HEROES. He has also developed an innovative emergency medical response computer program that lets emergency responders better treat and track injuries at the scene. Dr Francescutti is also the founder of the Coalition for Cellphone-Free Driving and former director of the Alberta Centre for Injury Control and Research.
He has chaired numerous committees and task forces that deal with public health and injury prevention. He is also a professor at the University of Alberta and a frequent national health columnist for television and radio. He has given over a 1000 presentations world wide on the topic of injuries.
In 2005, he was selected as one of Alberta's 100 Physicians of the Century.
In 2007, he was awarded a Champion for Children Award and a Paul Harris Fellowship from the North East Edmonton Rotary Club.
In 2010, he became the 41st President of the Royal College of Physicians and Surgeons of Canada.
In 2011, he was appointed as Honorary Colonel of 1 Field Ambulance Edmonton.
In 2011, he was selected by Alberta Venture as one of Alberta's most influential people.
In 2013, he became the President of the Canadian Medical Association.
References
- Alexander D. The health effects of earthquakes in the mid-1990s. Disasters. 1996;20(3):231–247. doi: 10.1111/j.1467-7717.1996.tb01036.x. [DOI] [PubMed] [Google Scholar]
- BOND Mitigation emerges as major strategy for reducing losses caused by natural disasters. Board of Natural Disasters. Science (New York, NY) 1999;284(5422):1943–1947. [PubMed] [Google Scholar]
- CRED . Centre for Research on the Epidemiology of Disasters; Brussels, Belgium: February 2012. Disaster Data: A Balanced Perspective. issue 27. [Google Scholar]
- Fink G., Redaelli S. Determinants of international emergency aid—humanitarian need only? World Dev. 2011;39(5):741–757. [Google Scholar]
- Guha-Sapir D., Vos F., Below R., Ponserre S. CRED; Brussels: 2012. Annual Disaster Statistical Review 2011: The Numbers and Trends. [Google Scholar]
- Inter-American Development Bank . 1999. Reducing Vulnerability to Natural Hazards: Lessons from Hurricane Mitch. (Working paper ed., Stockholm, Sweden) [Google Scholar]
- Krin C.S., Giannou C., Seppelt I.M., Walker S., Mattox K.L., Wigle R.L., Crippen D. Appropriate response to humanitarian crises. Br. Med. J. 2010;340 doi: 10.1136/bmj.c562. [DOI] [PubMed] [Google Scholar]
- Ligon B.L. Infectious diseases that pose specific challenges after natural disasters: a review. Semin. Pediatr. Infect. Dis. 2006;17(1):36–45. doi: 10.1053/j.spid.2006.01.002. [DOI] [PubMed] [Google Scholar]
- Morgan O., De Goyet C.D.V. Dispelling disaster myths about dead bodies and disease: the role of scientific evidence and the media. Rev. Panam. Salud Publ. 2005;18(1):33–36. doi: 10.1590/s1020-49892005000600006. [DOI] [PubMed] [Google Scholar]
- Noji E.K. Public health issues in disasters. Crit. Care Med. 2005;33(Suppl. 1):S29–S33. doi: 10.1097/01.ccm.0000151064.98207.9c. [DOI] [PubMed] [Google Scholar]
- OCHA . 2012. Humanitarian Financing – Overview [Homepage of United Nations]http://www.unocha.org/what-we-do/coordination/response/overview [Online] (accessed 08.01.12.) [Google Scholar]
- Pan American Health Organization . PAHO; Washington, DC: 2004. Management of Dead Bodies in Disaster Situations. [Google Scholar]
- Sheu J. An emergency logistics distribution approach for quick response to urgent relief demand in disasters. Transp. Res. Part E Logist. Transp. Rev. 2007;43(6):687–709. [Google Scholar]
- Sphere Project . Oxfam; Oxford: 2000. The Sphere Project: Humanitarian Charter and Minimum Standards in Disaster Response. [DOI] [PubMed] [Google Scholar]
- U.N. ISDR . United Nations; Geneva, Switzerland: 2004. Living with Risk: A Global Review of Disaster Reduction Initiatives. [Google Scholar]
- U.N. ISDR . United Nations; Geneva, Switzerland: 2011. Killer Year Caps Deadly Decade – Reducing Disaster Impact Is “Critical” Says Top UN Disaster Official. [Google Scholar]
- UNDP . United Nations; Geneva, Switzerland: 2004. Reducing Disaster: A Challenge for Development. [Google Scholar]
- UNESCO . 2007. Natural Disaster Preparedness and Education for Sustainable Development. [Google Scholar]
- Wasay M., Shafqat S. Preparing for the next natural disaster–need for a WHO coordinating centre. Bull. World Health Organ. 2006;84(10):767. doi: 10.2471/blt.06.035022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson J.T., Gayer M., Connolly M.A. Epidemics after natural disasters. Emerg. Infect. Dis. 2007;13(1):1–5. doi: 10.3201/eid1301.060779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wisner B., Adam J., editors. Environmental Health in Emergencies and Disasters: A Practical Guide. first ed. World Health Organization; Geneva, Switzerland: 2002. [Google Scholar]
- World Health Organization . World Health Organization; Geneva, Switzerland: 1995. Coping with Major Emergencies: WHO Strategy and Approaches to Humanitarian Action. [Google Scholar]
- World Health Organization . United Nations; New York: 2012. World Urbanization Prospects: The 2011 Revision. [Google Scholar]
Relevant Website
- http://www.emergency.cdc.gov/preparednesss/kit/disasters/ – Centre for Disease Control (accessed 19.03.16.).