

Abstract
Significance.
Access to digital text is increasingly widespread, but its impact on low-vision reading is not well understood.
Purpose.
We conducted an online survey of people with low vision to determine what assistive technologies they use for visual reading, their preferred text characteristics, and the time they devote to reading digital and hard-copy text.
Methods.
One hundred and thirty-three low vision participants completed an online survey. Participants reported the nature and history of their low vision, their usage of different assistive technologies, and time devoted to five visual reading activities.
Results.
The three largest diagnostic categories were albinism (n = 36), retinitis pigmentosa (n = 20), and glaucoma (n = 15). Mean self-reported acuity was 0.93 logMAR (range 0.1 to 1.6). Mean age was 46 years (range 18 to 98). Participants reported on percentage time spent reading using vision, audio or touch (braille). Seventy-five percent of our participants did more than 50% of their reading visually. Across five categories of reading activities—work or education, news, pleasure, spot reading, and social networking—participants reported more time spent on digital reading than hard-copy reading. Eighty-nine percent of our participants used at least one technology from each of our two major categories of assistive technologies (Digital Content Magnifiers and Hard-Copy Content Magnifiers) for visual reading.
Conclusions.
Despite the growing availability of digital text in audio or braille formats, our findings from an online sample of people with low vision indicate the continuing importance of visual reading. Our participants continue to use technology to access both hard-copy and digital text, but more time is devoted to digital reading. Our findings highlight the need for continued research and development of technology to enhance visual reading accessibility.
By a recent estimate, there are 5.7 million people in the United states with acuity poorer than 20/40.1 For many of them, the primary consequence of their low vision is difficulty reading.2
The advent of digital media and the ever-expanding variety of digital reading devices on the market have changed people’s reading habits. People now can easily access digital materials, such as web pages, e-books, and online user manuals. Hence, digital reading has become a major activity in modern society. A 2010 survey3 revealed that 83% of normally sighted participants spent more time on digital reading than before. However, over 90% of participants in the same study preferred hard-copy material to digital material for reading.3 While these percentages may have changed, it seems clear that normally sighted readers make use of both digital and hardcopy text.
Current digital devices offer low-vision readers flexibility in customizing the layout and appearance of text. Magnification can be achieved by zooming functions on smartphones and tablets. Laptops and desktop computers with bigger displays can present larger print sizes and in turn can enable a low-vision user to achieve a higher level of magnification. These useful features make digital media more accessible to people with low vision. An online survey of visually impaired people conducted in the UK found that over three quarters of participants (81%) had a smartphone and almost half of them used tablets.4 Another study showed that normally sighted and visually impaired people were equally likely to own a handheld video device, like an iPad or a PlayStation Portable.5
Some laboratory studies have demonstrated the benefit of using these digital devices for reading. For instance, people with AMD can read faster on an iPad than on hard-copy paper or an E-book reader, when given the same print size across all media, but hard-copy paper was still considered easier to use.6 In another study testing reading ability with the iPad in a large group of people with low vision, 87% were able to read a digital news article comfortably by zooming in and changing the contrast polarity.7 Morrice et al.8 found that only experienced low-vision iPad readers can read as fast as low-vision closed-circuit television (CCTV) readers, but average reading speed was not significantly different between an iPad and CCTV for non-experienced readers. Helpful built-in features, like zoom and contrast polarity, can possibly make mainstream digital devices accessible to visually impaired users.9
People with low vision are no longer limited to the use of optical magnifiers but instead have a variety of choices to help them read in their daily lives. Fok et al.10 showed that many digital devices and technologies, such as screen magnification software, large monitors, and screen reader software, serve as important and useful assistive technologies for people with low vision. Another online survey conducted by an online community, Web Accessibility In Mind (WebAIM), also reported that people with low vision make use of different assistive features, such as screen readers, zooming and contrast polarity options, to access web content.11
We have reported detailed results from one section of the survey in a separate publication.12 This part of the survey asked participants to view a sample text passage on their primary reading display and report on the viewing distance, screen size, number of lines visible and number of characters per line. Our goal in obtaining this information was to determine how people with low vision arrange their viewing configuration to achieve adequate magnification. In brief, most of the low-vision participants from our sample achieved their desirable magnification by a combination of two factors: reduced viewing distance compared to normally sighted controls and increased on-screen letter size. A majority (72%) of those who completed this part of the survey relied more on increased on-screen letter size.
The primary aim of our online survey was to understand the reading behavior of people with low vision in the digital era. This report describes findings from our survey concerning what devices people with low vision use for visual reading, their preferred display settings, how much time they spend on different reading activities, and how their acuity affects their choice of device or the amount of time they spend on reading.
METHODS
Participants
The research protocol was approved by the University of Minnesota institutional Review Board and followed the tenets of the Declaration of Helsinki. Online consent was provided by each participant before proceeding to the survey. One hundred and thirty-three participants were recruited by word of mouth and through several visual-impairment related organizations in the United States, such as the American Council of the Blind and Foundation Fighting Blindness. One hundred and twenty-six of our participants were from 33 U.S. states, two from Canada, one from Taiwan, one from Uruguay, and three undesignated. The three most cited states were Minnesota (n = 31), California (n = 9) and Pennsylvania (n = 9). Screening questions ensured that participants were aged 18 or older, read visually in their daily lives for some purposes, and had low vision with no major changes to their vision within the past year. For purposes of this survey, low vision was defined as an acuity of less than 20/60 with best corrected glasses in the better eye or a visual field less than 20 degrees.
Materials
Participants completed the online survey on their own time and with their own devices between January 2017 and March 2018. The online survey was designed to be accessible by screen-magnification and screen-reading software. The questions used in the survey can be found in the Appendix, available at [LWW insert link].
The survey consisted of five sections:
Demographics: Questions about age, education level, and employment status.
Nature and history of low vision: Questions about the participant’s cause of low vision, visual acuity, type of visual field loss, if any, and percentage of time spent on visual, audio and braille reading.
Usage of assistive devices/technologies: Participants reported the devices they used for visual reading. Two categories of assistive technologies were included in this section: Digital Content Magnifiers and Hard-Copy Magnifiers. Digital Content Magnifiers refer to hardware or software that magnify text within digital materials, such as online webpages, online news, e-books or scanned materials. This category includes smartphones, tablets, E-book readers, laptops, desktop computers and screen magnification software installed on laptops or desktops. Hard-Copy Magnifiers include devices that are designed for reading hard-copy materials, such as printed books, newspapers, medicine labels and food packaging. This category includes optical magnifiers (handheld, stand, and mounted on glasses), CCTVs, and portable handheld electronic magnifiers. Magnification apps on mobile devices were included in this category because these apps use the built-in camera to magnify hard-copy text.
Assessment of Magnification: The participant viewed a paragraph of text from Alice in Wonderland on their chosen reading display and reported properties of viewing configuration, including the viewing distance, dimensions of the display, and the number of characters on a line. These data were used to estimate the roles of viewing-distance magnification and letter-size magnification in relation to the participant’s acuity. Detailed findings from this section of the survey were reported in Granquist et al.12 and will not be further described here.
Reading habits: Participants rated how much time they spent on several categories of reading in digital or hard-copy format in the past year, using a five-point scale -- 1 = rarely or never; 2 = occasionally, once a week or less; 3 = frequently, at least a few days per week; 4 = almost every day, at least once; and 5 = daily heavy use. Five different activities were (I) Work or educational reading, (II) News reading, (III) Pleasure reading of books or articles, (IV) Spot reading, such as recipes, food labels, restaurant menus, phone numbers, TV listings, etc., and (V) Social networking, such as email communication and social media. For all except social networking, participants provided separate ratings for hard-copy and digital reading. Participants who learned to read prior to the onset of low vision were also asked to provide ratings for their reading habits while they had normal vision, but these data on reading with normal vision are not included in this report.
RESULTS
Characteristics of the Participant Sample
The mean age of our 133 participants was 46.03 (SD = 17.42, Median = 48, range: 18 to 98). Most of the participants reported acuity as Snellen ratios. We converted these values to corresponding logMAR values for purposes of calculation. The average self-reported binocular acuity was 0.93 logMAR (SD = 0.35 logMAR, range: 0.1 to 1.6 logMAR) from a subgroup of 106 participants providing numerical acuities. Fifty-four percent of our participants reported that they experienced nystagmus. The group with nystagmus had a significantly worse average acuity (0.99 logMAR, SD = 0.31) than those without nystagmus (0.85 logMAR, SD = 0.39, t(78.11) =2.01, P < .05). We did not find important differences in our other measures between the participants with and without nystagmus. Forty-six percent of participants reported they had peripheral-field vision loss, 14% had central-field loss, and 38% had no visual field loss. Nine percent of our participants reported they had hearing loss.
Participants were asked to report the cause(s) of their low vision. The three most common causes were albinism (36), retinitis pigmentosa (RP) (20), and glaucoma (15). Twelve participants listed multiple causes of their low vision. Table 1 lists the self-reported diagnoses.
Table 1.
Number of Participants Reporting Diagnoses: Unknown includes those who did not report a cause, or the responses were not specific (e.g. poor vision, genetics, inherited genetic factors, etc.)
| Causes | n | Causes | n |
|---|---|---|---|
| Albinism | 36 | Cone-rod dystrophy | 4 |
| Retinitis Pigmentosa | 20 | Stargardt’s disease | 3 |
| Glaucoma | 15 | Uveitis, inflammatory and autoimmune diseases | 3 |
| Miscellaneous retinal disorders | 11 | Achromatopsia | 2 |
| Retinopathy of prematurity | 10 | Other macular disorders. | 2 |
| Optic nerve disease | 9 | Multiple sclerosis | 1 |
| Cataract | 8 | Traumatic brain injury | 1 |
| Anterior segment (meaning cornea, lids, etc.) | 7 | Unknown | 9 |
| Age-related Macular Degeneration | 6 |
Seventy-five percent of the participants identified as female, and 78% of them had a college/university degree or higher. Forty-nine percent of them were employed, 30% were unemployed, and 21% were retired. Sixty-three percent had low vision since birth, 14% developed low vision before 18 years old and 20% had late onset low vision after age 18. The late-onset group had better average acuity (mean: 0.63 logMAR, SD: 0.36) and was older (mean: 61.8, SD: 12.92) than the rest of the sample.
To assess the reliability of self-reported acuities, we assembled data for 20 participants for whom we had both self-reported acuities and lab-measured acuities. Figure 1 shows a scatterplot of the values. The mean difference was 0.03 logMAR (SD = 0.18), and the mean absolute difference was 0.13 logMAR (SD = 0.11). The correlation between the two measures was 0.93 (p < .001). Our results were similar to our analysis of findings from Zhao et al. (2017)13 for 17 participants with low vision—mean difference between self-reported and measured acuity was 0.06 logMAR (SD = 0.24), and mean absolute difference was 0.16 logMAR (SD = 0.18). The generally good agreement between self-reported and lab-measured acuities gave us confidence in using self-reported acuities in additional analyses.
Figure 1.
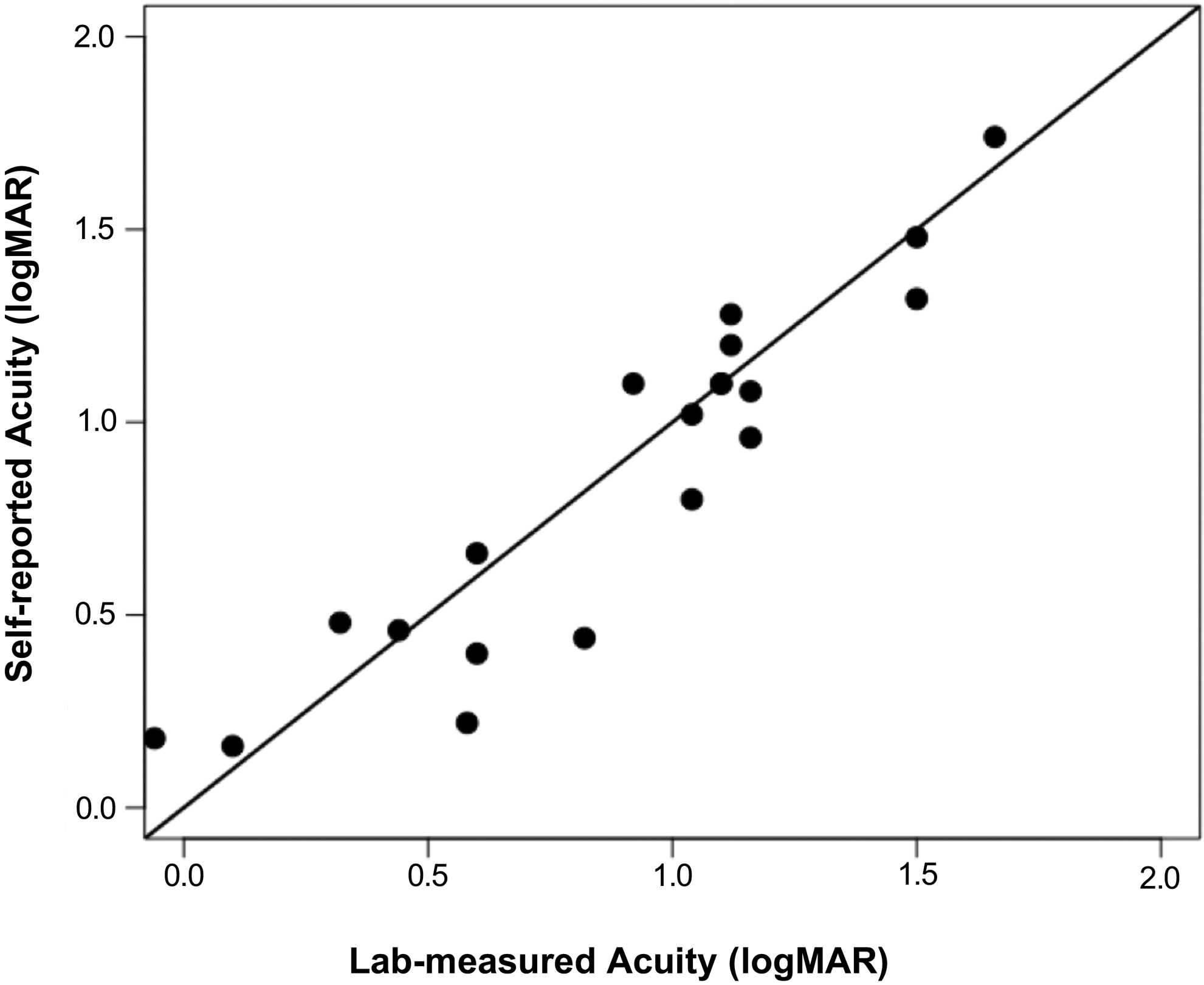
The scatterplot shows the relationship between self-reported visual acuities and lab measured visual acuities from a sample of 20 participants. The solid, diagonal line represents equality between the two measures.
Reading Habits
In Section 2 of the survey, we asked our participants how they distributed their daily reading between visual, auditory and braille sources. Figure 2 plots the proportion of visual reading as a function of acuity. Averaged across all participants, 64% of reading was visual, 33% was auditory and 3% was braille. Twenty-two participants reported some braille reading, ranging from 1% to 60% of their total reading. Only seven of them did more than 10% of their reading with braille. For a subgroup of participants with self-reported hearing loss (9%), the proportion of reading time on the three modalities was not different from the rest of the sample.
Figure 2.
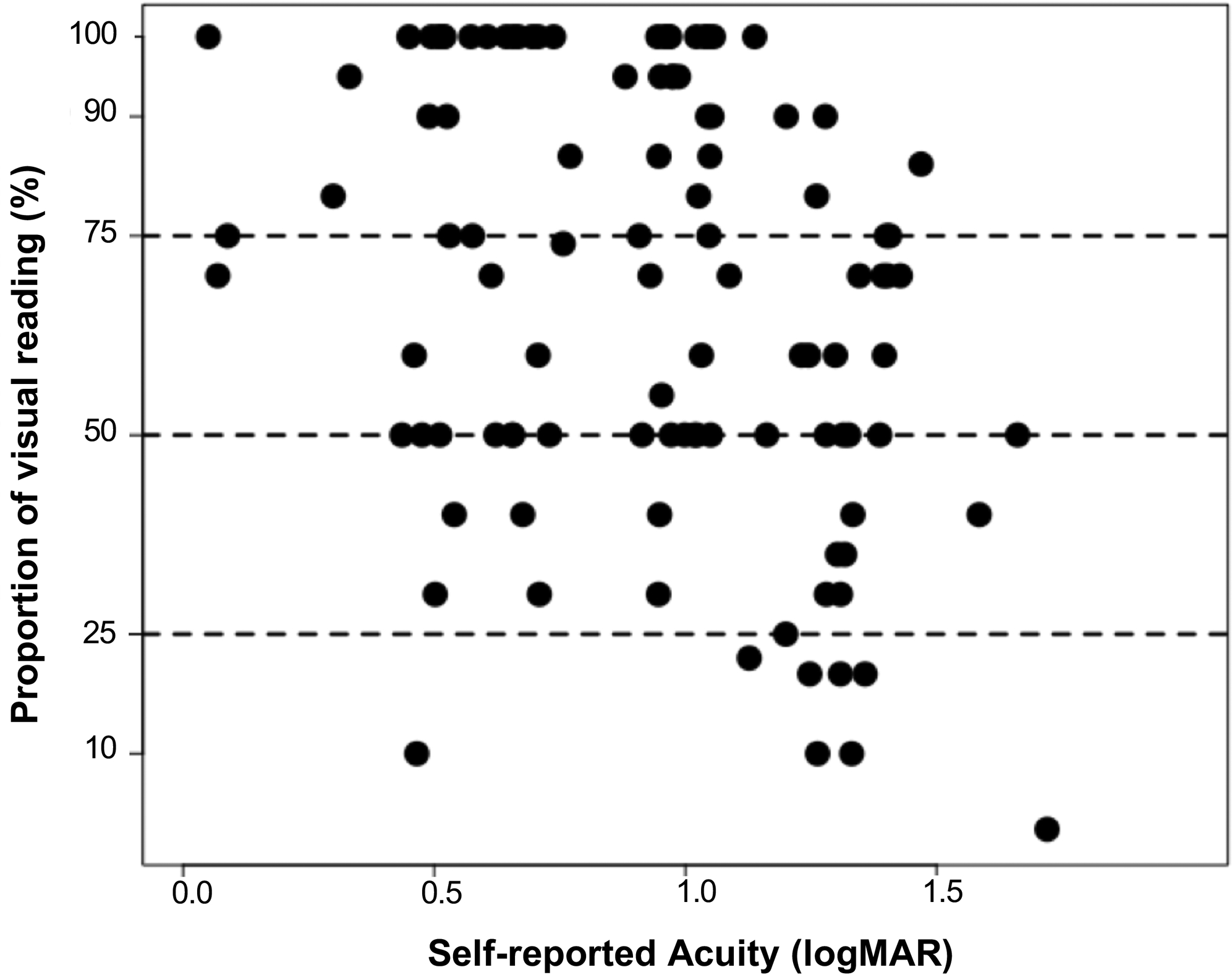
The scatterplot shows the proportion of visual reading as a function of self-reported acuity for 106 participants. The three dashed horizontal lines represent 75%, 50% and 25% of time spent on visual reading.
A chi-square goodness-of-fit test revealed that the number of participants who spent more than 50% on visual reading (n = 101), was significantly greater than the number who spent more than 50% of time on auditory reading (n = 31) or Braille reading (n = 1) (χ2(2) = 118.8, P < .001). The effect size (Cohen’s W) was 0.95. Forty-four percent of our participants did more than 75% of their reading visually (Vision Primary subgroup), and only 11% did less than 25% of their reading visually (Nonvisual subgroup). The Vision Primary subgroup had a better average acuity (mean: 0.82 logMAR, SD = 0.3 logMAR) than the Nonvisual subgroup (mean: 1.18 logMAR, SD = 0.31 logMAR, t(11.58) = 3.18, P < .01), with Cohen’s effect size (d) value of 1.18.
A multi-variate logistic regression model revealed that acuity (but not age or education level) was a predictor of whether a participant would spend more than 75% of reading time on visual reading (Vision Primary Group, coef: −2.12, P < .01, Appendix Table A1, available at [LWW insert link]). The negative coefficient of acuity means that better acuity was associated with a greater probability of 75% or more visual reading. Thirty-seven participants in the Vision Primary Group had an acuity better than 1.0 logMAR, and 5 had an acuity worse than 1.0 logMAR.
In Section 5 of the survey, we were interested in both the overall amount of visual reading and the differences between hard-copy and digital reading. For four of the five activities, more than half of our participants reported that they used digital reading on a daily basis (ratings 4 or 5)—work/education (65%), news reading (50%), spot reading (59%) and social networking (77%). Fewer (44%) reported using digital reading for pleasure on a daily basis (ratings 4 or 5). Clearly, this group of low-vision participants engages in extensive daily use of digital reading. Figure 3 shows the proportion of ratings on each activity.
Figure 3.
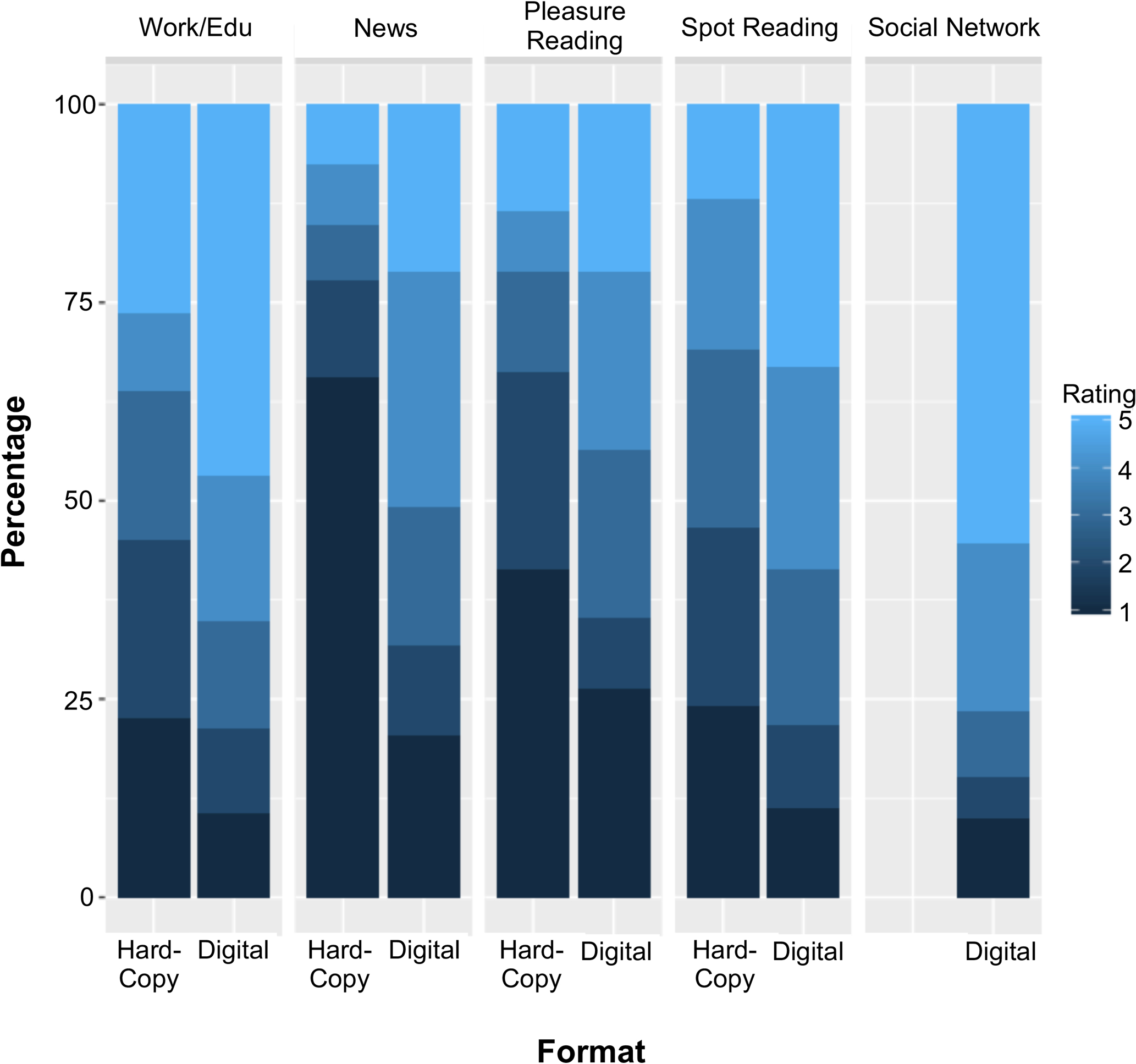
The stacked bar plot shows the percentage of participants providing each of the ratings from 1 to 5 on the y-axis. The x-axis represents the five activities listed in the survey with separate bars for Hard-Copy and Digital reading. The darker color represents lower rating, which refers to less time spent on a specific activity.
Wilcoxon signed-rank tests showed that our participants spent significantly more time on digital reading than hard-copy reading across all four reading activities—Work/Educational reading (Z = −5.44, P < .001, effect size (r) = 0.47), News reading (Z=6.5, P < .001, effect size (r) = 0.57), Pleasure reading (Z = −4.44, P < .001, effect size (r) = 0.38), and Spot reading (Z = −5.16, P < .001, effect size (r) = 0.45).
Assistive Devices
In Section 3 of our survey, participants reported the devices they used for visual reading (Table 2). The devices can be categorized into two groups: Digital Content Magnifiers and Hard-Copy Magnifiers. Most of our participants (98%) used two or more devices for visual reading. Ninety-four percent of them reported using at least one type of Digital Content Magnifier, and 95% used at least one Hard-Copy Magnifier. Eighty-nine percent of our participants used devices from both categories. The three most frequently reported devices all came from the Digital Content Magnifier category: smartphones (69%), screen magnification software (62%), and tablets (59%). The two least used devices were in the Hard-Copy Magnifier category: stand magnifiers (10%) and magnifiers mounted on glasses (16%). Additional analysis revealed that 87% of our participants used either laptop or desktop computers for visual reading. For this group of laptop and desktop users, 68% of them used magnification software on their computers. Eighty percent of our participants used either a smartphone or tablet, and 44% of these smartphone or tablet users used magnification apps.
Table 2.
Percentage of participants using various types of devices.
| Digital Content Magnifiers | |
|---|---|
| Smartphone | 69% |
| Screen magnification software | 62% |
| Tablet | 59% |
| Desktop Computer | 58% |
| Laptop | 56% |
| E-book reader | 35% |
| Use at least one device in the category | 94% |
| Hard-Copy Content Magnifiers | |
| Handheld magnifier | 55% |
| CCTV | 47% |
| Portable Handheld Electronic Magnifier | 44% |
| Telescope | 42% |
| Magnification apps | 41% |
| Magnifier mounted on glasses | 16% |
| Stand magnifier | 10% |
| Use at least one device in the category | 95% |
We used logistic regression to explore the use of acuity, education and age in predicting device usage. The only significant relationship occurred for acuity and whether a participant used a CCTV (see Appendix Table A2, available at [LWW insert link]). The coefficient of the logistic model was statistically significant (coef. = 2.45, P < .001).
Preferred Text Characteristics
We asked our participants about their preferences for contrast polarity and font. Thirty-nine percent reported that they preferred black text on a white background. A larger group of participants (46%) preferred reversed contrast (white text on a black background), and 14% of participants had no preference for contrast setting. On average, the group that preferred reversed contrast had significantly worse acuity (1.03 logMAR, SD = 0.35) than the group who preferred black-on-white (0.82 logMAR, SD = 0.33) (t(85.86) = 2.86, P < .01). For the three largest diagnostic categories in our survey (Table 1), the number of participants preferring standard contrast (black-on-white) and reversed contrast (white-on-black) were—albinism (16 and 15), RP (5 and 13), and glaucoma (3 and 8), respectively. Although there were only 6 participants with AMD in our group, 5 of them preferred black-on-white contrast.
We also asked our participants to report their preferred font type, if any. Only 51 participants expressed a preference for one or more fonts. The most frequent fonts reported were Arial (n = 37), Times New Roman (n = 16), and Verdana (n = 7) (Table 3).
Table 3.
Preferred text characteristics.
| Contrast Polarity Preference | n = 133 |
| Black Text on White Background | 39% |
| White Text on Black Background | 46% |
| No Preference | 14% |
| Not Answered | 1% |
| Font Preferences | n = 51 |
| Sans Serif font types | |
| Arial | 37 |
| Verdana | 7 |
| Any Sans Serif font | 6 |
| Helvetica | 4 |
| APHont | 3 |
| Comic Sans | 3 |
| Calibri | 3 |
| Serif font | |
| Times New Roman | 16 |
DISCUSSION
Our goal in the current study was to learn about visual-reading activities by people with low vision and the devices they use. Given the growing availability of text in audio formats and technology for text-to-speech and text-to-braille, we wondered if our participants might show diminished reliance on visual reading as a whole. To the contrary, four of our findings indicate the continuing importance of visual reading to low-vision individuals. First, for all five categories of digital reading activities in our survey, our participants reported substantial visual reading. For four of the five categories (pleasure reading excepted), they read daily.
Second, there was a high rate of adoption of multiple visual-reading devices (by more than 90% of our participants), and 89% had at least one aid from our two main categories (digital-content devices and hard-copy reading devices.) Third, vision was the primary reading modality for most of our participants, even for many with moderate to severe acuity loss. Presumably, those with low acuity who continue to read visually make use of high magnification.
Fourth, we found that our participants spent significantly more time reading digital text than hard-copy text across the different activities listed in our survey. This result is similar to the trend found in the normally sighted population.3 The growing range of digital materials enhances text accessibility for visually impaired people. The expansion of built-in features, such as screen magnification, the ability to adjust print size and contrast polarity, makes digital reading more accessible than hard-copy reading.
These findings reinforce our view of the importance of continued research on low-vision reading in the digital era and ongoing efforts to enhance the visual accessibility of text.
Devices and Technologies Used
Our findings on everyday reading activities indicated that more time was devoted to digital reading than hard-copy reading. The overall most used devices (Table 2) were from the Digital Content Magnifier category: smartphones (used by 69% of our participants), screen magnification software (62%), and tablets (59%). By comparison, the two least used devices were from the Hard-Copy Magnifier category: stand magnifiers (10%), and magnifiers mounted on glasses (16%).
Despite a smaller screen size, smartphones were the reading devices used most frequently by our participants. The popularity of smart devices, like smartphones and tablets, among both normally sighted and visually impaired individuals may indicate that the features of accessibility built in those devices facilitate their use for reading despite their small displays. Crossland et al.4 found an even higher adoption of smartphones in a survey of visually impaired users (81%), but their survey focused on general use and not specifically on visual reading. For our participants, it is likely that smartphones were used for spot reading tasks, and not for continuous reading. In support of this conjecture, in the portion of our survey described by Granquist et al.,12 we asked our participants to report on the device used for reading a sample passage from Alice in Wonderland. For the 75 participants who completed this portion of the survey, 60 used a desktop or laptop computer, 10 a tablet, two a CCTV and only three a smartphone. Moreover, Crossland et al.,4 found that most of their visually impaired participants used smartphones for text messaging (90%) and internet browsing (80%), which are spot reading tasks.
Despite the shift to digital reading, our participants continue to read hard copy materials. Ninety-five percent of our participants reported using at least one type of Hard-Copy Magnifier for visual reading. Additionally, almost half of our participants reported using CCTVs, which are designed for reading hard-copy materials. Our analysis showed that participants with worse acuities were more likely to use a CCTV for visual reading.
Preferred Text Characteristics
Our participants included a surprisingly large number (46%) who preferred reversed-contrast text (white letters on a black background) compared with 39% who preferred standard black-on-white text. It has long been known that some people with low vision read better with reversed-contrast text.14,15 Legge16 reviewed research indicating that participants with cloudy ocular media (from cataract, corneal damage or vitreous debris) sometimes have better reading performance with reversed-contrast. In the current study, nine of fifteen participants with cataract or other disorders with cloudy ocular media reported a preference for reversed contrast. Many in our largest categories—albinism, RP and glaucoma— also reported a preference for white-on-black text. The preference of reversed contrast could be the result of photophobia, which is a common symptom shared by people with albinism17 and retinitis pigmentosa18. Ehrlich19 has reported that 21 of 23 patients with severe retinitis pigmentosa read better with reversed-contrast text. We note that our participants who preferred reversed contrast had overall poorer acuity than the remaining participants. We also note that five of our six AMD participants preferred regular black-on-white text. Further study would be required to determine if preferences correlate highly with measurable properties of reading performance such as reading speed or critical print size.
Although only 51 participants expressed font preferences, the Arial font family was the most cited font style (Table 3). This finding coincides with the guideline for large-print documents recommended by the American Council of the Blind,20 which suggests using sans-serif fonts such as Arial. Only 3 of our participants mentioned the APHont font, which was designed for low vision by the American Printing House for the Blind.21 None of our participants mentioned Tiresias, a font designed by the Royal National Institute of Blind People in London. Previous studies have been unable to demonstrate a consistent benefit of specially-designed fonts for low vision or for specific mainstream fonts.5,22,23 There is some evidence, however, that fonts with increased between-letter spacing, such as courier, can be helpful.23–25
Study Limitations
We address three significant limitations of our study.
First, we acknowledge that our low-vision sample is not representative of the low-vision population as a whole. In contrast to patients visiting low-vision clinics, many of whom are older and have macular degeneration,26 a majority of our participants had early-onset low vision, more had peripheral-field loss than central-field loss, and most of them had a college degree or higher. Our online survey targeted a group of people who are familiar and comfortable with computer technology and who make regular use of digital reading in their daily lives, and as such the current study provides information about visual reading among a technologically savvy group of people with low vision. The characteristics of our sample were similar to the sample composition of other online survey studies aiming for understanding the technology usage among people with low vision4,11. One advantage of an online survey over a clinic-based survey is the possibility of reaching people who do not have easy geographical access to a low-vision clinic. It is certainly possible that access to low-vision aids and also access to digital content might depend on rural vs. urban residency or other geographical variables. Our study shares with most clinical studies the difficulty in recruiting a truly representative sample of low-vision participants.
Second, in some cases, we have related our findings to the visual acuities of our participants. In so doing, we have relied on self-reports rather than direct clinical data, an inherent limitation of a survey study. It is known that self-reported subjective ratings of vision status are influenced by non-visual factors such as race and socioeconomic status.27–29 These studies asked participants to rate the quality of their vision on a numerical scale (1–10) or using descriptors such as Excellent, Fair and Poor. We did not ask our participants to make subjective ratings of their vision, but to report acuity scores, presumably obtained from their eye doctors. Our sample of low-vision participants tended to be fairly young and well educated. Most (81%) reported an eye exam within the past year, and our eligibility criteria included stable vision over the past year. Furthermore, we encouraged our participants to check their clinical records or check with their eye doctor to acquire their visual acuity if they did not know it. These are factors which contribute to reliable self-reporting of eye conditions. Compared to the findings of Kiser et al. (2005)30 on repeat reliability, which reported that the criterion for a significant change in low-vision acuity should be two to three lines (0.2 – 0.3 logMAR), our data shown in Figure 1 from a sample of 20 low-vision participants from whom we have both self-reported and lab measurements showed a mean absolute difference of only 0.13 logMAR. Nevertheless, we acknowledge that the self-reported clinical information is likely to be noisier than corresponding clinical or laboratory data. The 95% limit of agreement (LoA) in our 20-participant data was 0.35 logMAR, which is larger than the range of 0.2 to 0.3 logMAR found in the Kiser et al. study30. Factors contributing to inaccuracy in reported acuity would include changes since the last clinic visit, inaccuracies in the clinical measurements themselves, and faulty memory. In addition, we converted visual acuities, reported as Snellen ratios, into logMAR units for the purpose of calculation and for the journal’s international readership. It is likely that the acuities reported by our participants may have often been measured with Snellen charts rather than logMAR charts, contributing noise to our data.
Finally, given the rapid progress in digital distribution of information and the continuing development of assistive technology, we recognize that our findings provide only a fleeting snapshot of the ecology of low-vision reading. It will be valuable to compare our results with similar data in future years.
Despite these limitations, our study sheds light on the reading behavior of an online group of people with low vision in the current digital era. Given the increasing number of low-vision individuals and the popularity of digital content, our findings reinforce our view of the importance of continued research on low-vision reading and ongoing efforts to enhance the visual accessibility of text at the design stage.
Supplementary Material
ACKNOWLEDGMENTS
The authors thank Andrew Sell and Thomas Lindsay of the Liberal Arts Technologies and Innovation Services (LATIS) at the University of Minnesota, and Elaine Kitchel of the American Printing House for the Blind. This study was supported by NIH grant EY002934 and the Helen Keller Foundation.
APPENDIX
Appendix A contains the questions in our survey of low-vision digital reading in the order they were presented, and is available at [LWW insert link]. The questions were formatted for convenient web access with screen-magnification software and screen-reading software. The format of the appendix is a more compact representation. The survey had six sections: Section 0. Eligibility, Section 1. Demographics, Section 2. Nature and History of Low Vision, Section 3. Usage of Assistive Devices/Technologies, Section 4. Assessment of Magnification, Section 5. Past and Current Reading Habits. The findings from the items in Section 4 on assessment of magnification were described in a separate publication.11
Appendix Table A1 and Appendix Table A2 show the results of two logistic regression models, and are available at [LWW insert link].
Appendix Table A1.
Multiple logistic regression for the association between visual reading (visual reading time < 75% or visual reading time >= 75%) and other predictors, including Age, Educational level, and Self-reported acuity (logMAR).
| Predictor | β | SE β | Z | P | Odds ratio (95% Cl) |
|---|---|---|---|---|---|
| (Intercept) | 3.35 | 1.27 | 2.64 | <.01** | N/A |
| Age | −0.02 | 0.02 | −1.1 | 0.27 | 0.98 (0.95 – 1.02) |
| Education Level | 0.42 | 0.36 | 1.13 | 0.26 | 1.51 (1.74 – 3.17) |
| - 0 = primary school | |||||
| -1 = High school | |||||
| - 2 = University/College degree | |||||
| - 3 = Advanced Graduate or Professional Degree | |||||
| Self-reported Visual Acuity (logMAR) | −2.05 | 0.61 | −2.53 | < .05** | 0.13 (0.02 – 0.58) |
Appendix Table A2.
Multiple logistic regression for the association between the usage of CCTV (0 = not used, 1 = used) and other predictors, including Age, Educational level, and Self-reported acuity (logMAR).
| Predictor | β | SE β | Z | P | Odds ratio (95% Cl) |
|---|---|---|---|---|---|
| (Intercept) | −2.69 | 1.02 | −2.63 | < .01 ** | NA |
| Age | 0.02 | 0.01 | 1.59 | 0.11 | 1.02 (1 – 1.05) |
| Education Level | −0.38 | 0.31 | −1.22 | 0.22 | 0.68 (0.37 – 1.25) |
| - 0 = primary school | |||||
| -1 = High school | |||||
| - 2 = University/College degree | |||||
| - 3 = Advanced Graduate or Professional Degree | |||||
| Self-reported Visual Acuity (logMAR) | 2.45 | 0.69 | 3.58 | <.001 *** | 11.63 (3.24 – 48.49) |
REFERENCES
- 1.Chan T, Friedman DS, Bradley C, Massof R. Estimates of Incidence and Prevalence of Visual Impairment, Low Vision, and Blindness in the United States. JAMA Ophthalmol 2018;136:12–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Owsley C, McGwin G, Lee PP, et al. Characteristics of Low-vision Rehabilitation Services in the United States. Arch Ophthalmol 2009;127:681–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.White S, Chen J, Forsyth B. Reading-related Literacy Activities of American Adults: Time Spent, Task Types, and Cognitive Skills Used. J Lit Res 2010;42:276–307. [Google Scholar]
- 4.Crossland MD, Silva RS, Macedo AF. Smartphone, Tablet Computer and E-reader Use by People with Vision Impairment. Ophthalmic Physiol Opt 2014;34:552–7. [DOI] [PubMed] [Google Scholar]
- 5.Woods RL, Satgunam P. Television, Computer and Portable Display Device Use by People with Central Vision Impairment. Ophthalmic Physiol Opt 2011;31:258–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gill K, Mao A, Powell AM, Sheidow T. Digital Reader vs Print Media: The Role of Digital Technology in Reading Accuracy in Age-related Macular Degeneration. Eye 2013;27:639–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Haji SA, Sambhav K, Grover S, Chalam KV. Evaluation of the iPad as a Low Vision Aid for Improving Reading Ability. Clin Ophthalmol 2014;9:17–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Morrice E, Johnson AP, Marinier JA, Wittich W. Assessment of the Apple iPad as a Low-vision Reading Aid. Eye 2017;31:865–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Irvine D, Zemke A, Pusateri G, et al. Tablet and Smartphone Accessibility Features in the Low Vision Rehabilitation. Neuroophthalmology 2014;38:53–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fok D, Polgar JM, Shaw L, Jutai JW. Low Vision Assistive Technology Device Usage and Importance in Daily Occupations. Work 2011;39:37–48. [PubMed] [Google Scholar]
- 11.Web Accessibility In Mind (WebAIM). Survey of Users with Low Vision Results; 2018. Available at: https://webaim.org/projects/lowvisionsurvey/. Accessed April 26, 2019.
- 12.Granquist C, Wu YH, Gage R, et al. How People with Low Vision Achieve Magnification in Digital Reading. Optom Vis Sci 2018;95:711–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zhao Y, Hu M, Hashash S, Azenkot S. Understanding low vision people’s visual perception on commercial augmented reality glasses. Proc SIGCHI Conf Hum Factor Comput Syst 2017;4170–81. [Google Scholar]
- 14.Silver J Reading Aids for the Partially Sighted: A Systematic Classification and Procedure for Prescribing. Br J Ophthalmol 1978;62:195. [Google Scholar]
- 15.Legge GE, Rubin GS, Pelli DG, Schleske MM. Psychophysics of Reading-II. Low Vision. Vision Res 1985;25:253–65. [DOI] [PubMed] [Google Scholar]
- 16.Legge GE. Chapter 3: Visual mechanisms in reading In: Psychophysics of Reading in Normal and Low Vision. Boca Raton: CRC Press; 2007:43–106. [Google Scholar]
- 17.Pérez-Carpinell J, Capilla P, Illueca C, Morales J. Vision Defects in Albinism. Optom Vis Sci 1992;69:623–8. [DOI] [PubMed] [Google Scholar]
- 18.Gawande AA, Donovan WJ, Ginsburg AP, Marmor MF. Photoaversion in Retinitis Pigmentosa. Br J Ophthalmol 1989;73:115–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ehrlich D A Comparative Study in the Use of Closed‐Circuit Television Reading Machines and Optical Aids by Patients With Retinitis Pigmentosa and Maculopathy. Ophthalmic Physiol Opt 1987;7:293–302. [PubMed] [Google Scholar]
- 20.American Council of the Blind. Best Practices and Guidelines for Large Print Documents Used by the Low Vision Community. 2011. Available at: https://archive.org/details/bestpracticesgui00coun. Accessed April 26, 2019.
- 21.American Printing House for the Blind. APHontTM: A Font for Low Vision. 2001. Available at: https://www.aph.org/products/aphont/. Accessed April 26, 2019.
- 22.Legge GE. Psychophysics of Reading in Normal and Low Vision. Boca Raton: CRC Press; 2007. [Google Scholar]
- 23.Xiong YZ, Lorsung EA, Mansfield JS, et al. Fonts Designed for Macular Degeneration: Impact on Reading. Investig Ophthalmol Vis Sci 2018;59:4182–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pelli DG, Legge GE, Schleske MM. Psychophysics of Reading. III. A Fiberscope Low-vision Reading Aid. Investig Ophthalmol Vis Sci 1985;26:751–63. [PubMed] [Google Scholar]
- 25.Tarita-Nistor L, Lam D, Brent MH, et al. Courier: A Better Font for Reading with Age-related Macular Degeneration. Can J Ophthalmol 2013;48:56–62. [DOI] [PubMed] [Google Scholar]
- 26.Goldstein JE, Massof RW, Deremeik JT, et al. Baseline Traits of Low Vision Patients Served by Private Outpatient Clinical Centers in the United States. Arch Ophthalmol 2012;130:1028–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.El-Gasim M, Munoz B, West SK, Scott AW. Discrepancies in the Concordance of Self-reported Vision Status and Visual Acuity in the Salisbury Eye Evaluation Study. Ophthalmology 2012;119:106–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Whillans J, Nazroo J. Assessment of Visual Impairment: The Relationship between Self-reported Vision and ‘Gold-standard’ Measured Visual Acuity. Br J Vis Impair 2014;32:236–48. [Google Scholar]
- 29.Quandt SA, Schulz MR, Chen H, Arcury TA. Visual Acuity and Self-reported Visual Function among Migrant Farmworkers. Optom Vis Sci 2016;93:1189–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kiser AK, Mladenovich D, Eshraghi F, et al. Reliability and Consistency of Visual Acuity and Contrast Sensitivity Measures in Advanced Eye Disease. Optom Vis Sci 2005;82:946–54. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.