

Abstract
The emergence of COVID-19 in South Korea, and the public and private sector response to it, serves as a valuable case study for countries facing similar outbreaks. This article focuses on how Korean health officials implemented drive-through and walk-through diagnostic testing, and extensive movement and contact tracing, to identify and inform exposed members of the public. Mobile applications from both government agencies and private developers played an important role in guiding people to testing centers, communicating movement trajectories of confirmed cases on digital maps, and tracking the health and movements of travelers and others at risk of exposure. This case study illustrates the importance of rapid adaptation of transportation infrastructure and location-based information technology to respond to public health crises, and how governments can learn from experimentation and past experience to accelerate these responses.
Keywords: Coronavirus, COVID-19, Contact tracing, Drive-through testing, Movement tracking, Mobile applications
1. Introduction
In early 2020, the world watched as a novel coronavirus emerged in Wuhan, China, and dramatically transformed the lives and movement patterns of millions of its residents. Health officials in South Korea recognized the threat this outbreak posed to their nation, a close neighbor and trading partner with China. With constant exchange of tourists, workers, and academics between the nations, it was inevitable that the virus would enter Korea through a visitor or returning citizen. However, the strategies South Korea employed to control the disease's spread within its borders appear to be effective as of March 2020, and have received much media attention as other nations struggle to manage the crises at home (Jeong et al., 2020).
Rather than mobilize its security forces to lock down entire cities and cut off nearly all forms of in-person contact, South Korea focused on rapid and widespread testing, and close tracking of all contacts between the exposed. These two pillars, testing and tracking, have allowed the nation to blunt the exponential spread of the disease, without having to halt all internal movement and access between its cities (Park et al., 2020). In this paper, we briefly outline the progression of the outbreak within South Korea, local government implementation of low-contact testing to safely and efficiently detect its spread, and nationwide contact tracing and dissemination of individual movement patterns to identify and inform the exposed members of the public. This case study illustrates the importance of rapid adaptation of transportation infrastructure and location-based information technology to respond to public health crises, and how governments can learn from experimentation and past experience to accelerate these responses.
2. Coronavirus outbreak in Korea
The first confirmed case of COVID-19 in South Korea came on January 19, 2020 (Kim et al., 2020). A visitor had arrived at Incheon International Airport from Wuhan, China, and tested positive after being flagged for high body temperature at the entry screening using an infrared sensor. In response, the national government elevated its alert level from “Aware” to “Care” according to the standardized degrees of risk. The government announced increased entry screening and shared the patient's movement trajectories with the public (KCDC, 2020a).
After two additional patients were confirmed within the following week from the same origin point of Wuhan, the Korean government raised the alert level to “Caution” on January 28th, and began to reinforce local response strategies. The Korea Center for Disease Control & Prevention (KCDC) increased the number of local screening centers to discover potential asymptomatic carriers, and assigned local hospitals as infection control institutes to preserve medical capacity in case of expansion of infection. Moreover, the national government started to cooperate with local governments and the national health insurance agency to closely monitor all travelers entering from Wuhan. In case any of the monitored people experienced symptoms, they were guided to take the diagnostic test and placed under quarantine. All known contacts with the confirmed patients were also monitored under the same procedures to prevent further infections (KCDC, Jan 27–28, 2020g).
Despite such efforts, the number of confirmed patients grew steadily at the rate of 1–4 patients each day until mid-February. On February 3, the government expanded their search to include people with whom infected patients had even minor contact. In addition, the government approved the use of a diagnostic testing kit (PowerChek™ 2019-nCoV Real-time PCR Kit) developed by a private company called Kogene Biotech to facilitate the growing number of diagnostic tests (KCDC, Feb 3–4, 2020d). Several other private firms also quickly developed COVID-19 testing kits and won approval for their use.
With the deployment of low-contact screening clinics (described in Section 3) and wide availability of test kits, medical staff in Korea were able to conduct 15,000 laboratory tests per day as of February 28, 2020 (Jeong et al., 2020). The Korean government covers the cost for testing those with suspected symptoms or in recent contact with confirmed cases; anyone else can pay 150,000 KRW (~125 USD) to get tested, with fees reimbursable from the nation's single-payer health care (Yoon and Martin, 2020). Undocumented foreigners are also eligible for testing without any risk to their status of stay in the country (Moon, 2020). As of March 16, 2020, more than 250,000 people had been tested in South Korea, roughly 1 for every 200 citizens (Moon, 2020).
On February 18th, the 31st patient was confirmed in the city of Daegu, and by the next day, a KCDC investigation team discovered that she had close contact with hundreds in a church congregation (KCDC, Feb 18, 2020e). In the following weeks, the number of confirmed patients steeply increased from a rate of 20 to more than 200 new cases per day, as represented in the log-scale graph in Fig. 2. The government escalated the alert level to “Serious” on February 25th, announced guidelines to limit trips and outdoor activities, and imposed emergency safety measures, from basic hygiene rules to self-quarantine and social distancing (KCDC, Feb 25, 2020f).
Fig. 2.
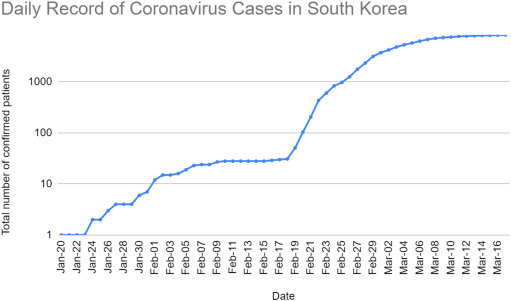
The total number of confirmed patients in Korea in log scale, until March 18, 2020 (KCDC, 2020c).
The daily rate of new case discovery peaked on February 29, 2020 with 813 patients, and since then has been slowly declining (see Fig. 1, Fig. 2 ) (KCDC, 2020b). In the following sections, we will discuss some of the major strategies used to respond to the outbreak, focusing on low-contact testing, information release, and large-scale contact tracing.
Fig. 1.
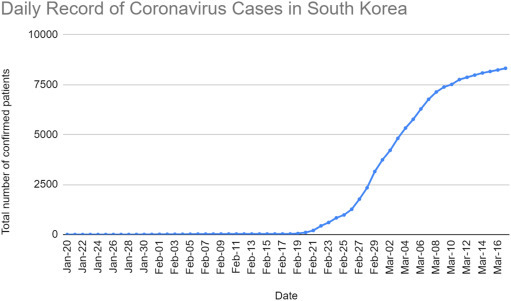
The total number of confirmed patients in Korea, until March 18, 2020 (KCDC, 2020c).
3. Low-contact testing centers
3.1. Drive-through testing
Drive-through testing was first suggested by Jaemyung Lee, the Governor of Gyeonggi Province, on February 23, 2020. At a government-held emergency coronavirus meeting, the governor explained the need for scaled-up, low-contact testing, as he worried about the safety of workers, limited space for social distancing, and rapid consumption of personal protective equipment from one-on-one medical consultation within existing healthcare facilities (윤종열, 2020).
The first drive-through test was implemented in Goyang, Gyeonggi province, at the city hall parking lot. The test, which included registration, symptom check, swab sampling, and car disinfection, lasted 10 min on average for each person, whereas previous testing procedures took ~30 min (노승혁, 2020). The test results were delivered directly to the patient via text message within three days (Watson and Jeong, 2020). As the number of drive-through test centers increased, the government announced operating standards for systematic scale-up and management (KCDC, Mar 4, 2020h).
The standard included the above mentioned four procedures (which could be curtailed depending on the situation), the minimum number of professional personnel with specific responsibilities, space requirements, and visiting vehicle restrictions. A total of 4–8 people are required to operate a drive-through; 1–3 administrators handle registration, vehicle entry/exit management, and education; 1–2 doctors conduct symptom check and sampling; and 1 person disinfects the vehicle. Although not strict, the standard required a minimum amount of dedicated space in the form of either shipping/storage containers or medical tents, for maximum space efficiency. Lastly, the patient must be the only person in the vehicle and must make reservations prior to visit (KCDC, Mar 4, 2020h). Fig. 3 shows one container-based testing site in South Korea, and Fig. 4 shows screening procedures at a Seoul tent-based testing site.
Fig. 3.

Container-based drive-through testing site, with separate stations for registration, health check, and specimen sampling.
Fig. 4.
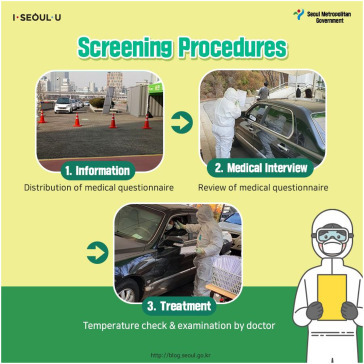
Infographic illustrating procedures for drive-through testing without leaving the vehicle.
Source: Seoul Metropolitan Government (2020).
3.2. Containers versus tents
In practice, initial attempts to use containers as testing centers were costly, since they required the patient to exit their vehicle and enter the container to be tested. Containers had to be equipped with depressurizers to minimize the release of pathogens and exposure of healthcare workers, and disinfected repeatedly. By contrast, when using open medical tents, the doctor could easily stick a swab through the vehicle's open window to take a sample from the patient's mouth or nose. For comparison, one testing center in Gyeonggi province with ten containers cost 879 million KRW to deploy (roughly 72,000 USD per container), while Goyang city installed eight screening tents for only 15 million KRW (roughly 1500 USD per tent) (한상봉, 2020). As a result, most drive-through test centers operated by local governments have employed medical tents, to save on cost and reduce exposure risk. Fig. 5 illustrates the difference in procedure.
Fig. 5.
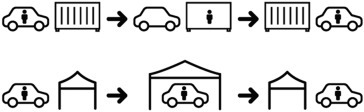
Illustration of difference between 2 types of drive-through testing centers (above: container-type, below: tent-type).
At the time of writing, an increasing number of South Korean medical centers, hospitals, public health centers and local governments were adopting drive-through tests using their open spaces and parking lots. However, information on their locations was not easily accessible to the public, because the government had only listed all testing centers without indicating which ones allowed drive-through testing (Ministry of Health and Welfare, n.d.). Therefore, the public had to rely on news articles or directly call the centers. For this reason, the mobile application OilNow, which normally helps customers locate gas stations, added a service that mapped all the drive-through test centers. As of March 9, 2020, 45 of the 613 test centers allowed drive-through (조재환, 2020). Table 1 lists the provinces of South Korea that deployed drive-through test centers, their respective location types, and number of confirmed patients.
Table 1.
National Status of All Drive-through Test Centers (as of March 9, 2020) (퍼즐벤처스, n.d.); population estimates retrieved from Korean Statistical Information Service (KOSIS, 2019).
| Province (population) | District | Location type | # confirmed patients |
|---|---|---|---|
| Gyeonggi (~13M) | Goyang-si | Public Health Center | 152 |
| Gwacheon-si | Public Health Center | ||
| Gimpo-si | Hospital | ||
| Gimpo-si | Welfare Center | ||
| Suwon-si | Parking Lot (World Cup stadium) | ||
| Suwon-si | Sports Culture Center | ||
| Ansan-si | Parking Lot (district office) | ||
| Yongin-si | Sports Park | ||
| Uijeongbu-si | Playground (gov't building) | ||
| Seoul (~9.6M) | Gangseo-gu | Hospital | 130 |
| Seocho-gu | HR Development Center | ||
| Songpa-gu | Parking Lot (sports stadium) | ||
| Eunpyeong-gu | Hospital | ||
| Incheon (~2.9M) | Seo-gu | Public Health Center | 9 |
| Yeonsu-gu | Parking Lot (sports center) | ||
| Daejeon (~1.5M) | Daedeok-gu | Public Health Center | 19 |
| Dong-gu | Hospital | ||
| Yuseong-gu | Public Health Center | ||
| Sejong (~0.3M) | Sejong | Public Health Center | 6 |
| Chungcheong (~3.6M) | Cheonan-si | Sports Stadium | 127 |
| Gongju-si | Public Health Center | ||
| Boeun-gun | Public Health Center | ||
| Daegu (~2.4M) | Nam-gu | Hospital | 5571 |
| Dalseo-gu | Welfare Center | ||
| Dalseong-gun | Parking Lot (traditional market) | ||
| Dong-gu | Soccer Field | ||
| Buk-gu | Tunnel Maintenance Center | ||
| Seo-gu | Local Sports Field | ||
| Seo-gu | Clinic | ||
| Suseong-gu | Parking Lot (sports stadium) | ||
| Gyeongsang (~6M) | Gumi-si | Parking Lot (park) | 1190 |
| Moonkyung-si | Public Health Center | ||
| Yeongdeok-gun | Local Sports Field | ||
| Jinju-si | Public Health Center | ||
| Changnyeong-gun | Public Health Center | ||
| Changwon-si | Vehicle Registration Center | ||
| Busan (~3.4M) | Jin-gu | Parking Lot (park) | 96 |
| Buk-gu | Parking Lot (sports field) | ||
| Haeundae-gu | Public Health Center | ||
| Jeolla (~3.6M) | Yeosu-si | Public Health Center | 11 |
| Gurye-gun | Clinic | ||
| Youngkwang-gun | Public Health Center | ||
| Yeongam-gun | Public Health Center | ||
| Gwangju (~1.5M) | Buk-gu | Parking Lot | 15 |
| Seo-gu | Sports Center |
3.3. Walk-through testing
While drive-through sites served well for testing patients with private vehicles, they were not optimal in dense urban environments with fewer drivers and less available space for car queues. To expand low-contact testing to these areas, hospitals created “walk-through” centers, rows of plastic booths (roughly the size of a phone booth) fitted with depressurizers, intercoms, and attached gloves for doctors outside the booth to interact with and collect samples from the patient. Introduced by H Plus Yangji Hospital in Seoul, these booths (named “Safe Assessment and Fast Evaluation Technical booth of Yangji Hospital” or “SAFETY”) have helped boost their testing capacity from 10 to 70 patients per day (김철중, 2020).
Subsequent variants have inverted them by placing the healthcare worker inside the booth, while the patient stands outside to be tested; this speeds up the process, since the booth does not need to be disinfected between patients (황선윤, 2020). These booths have made low-contact testing possible for non-drivers, and their small, mobile footprint allows them to be deployed in dense urban cores nearer to transit and residential areas. Fig. 6 shows an example of one testing booth with sample collection, decompression, and patient access equipment.
Fig. 6.

Photograph of healthcare worker disinfecting a walk-through COVID-19 testing booth.
Source: Kim Sun Joo (2020).
4. Information technology
4.1. Government daily briefing web posting
The Korea Center for Disease Control & Prevention (KCDC) posts the national counts of COVID-19 cases daily on its website. It used to update this twice a day, at 8 am and 5 pm, but switched to once a day at 10 am starting from March 10, 2020, to minimize confusion and pursue statistical consistency with local public authorities (뉴시스, 2020). The briefing information categorizes cases into three groups: tested positive, currently being tested, and tested negative. The group tested positive is further differentiated into three sub-groups: in quarantine, out of quarantine, and deaths; these counts are presented in daily statistics for each major province. Any update in response strategies or important regulatory revisions is also posted from the website.
This information disseminates through online news, social media, and the local government. Fig. 7 shows a daily infographic and chart provided by NAVER, a popular web and news portal in South Korea, using the KCDC briefing data. Citizens can quickly access information specific to their districts or neighborhoods; this includes the daily count of newly confirmed cases, along with their detailed movement trajectories within the last couple of days.
Fig. 7.
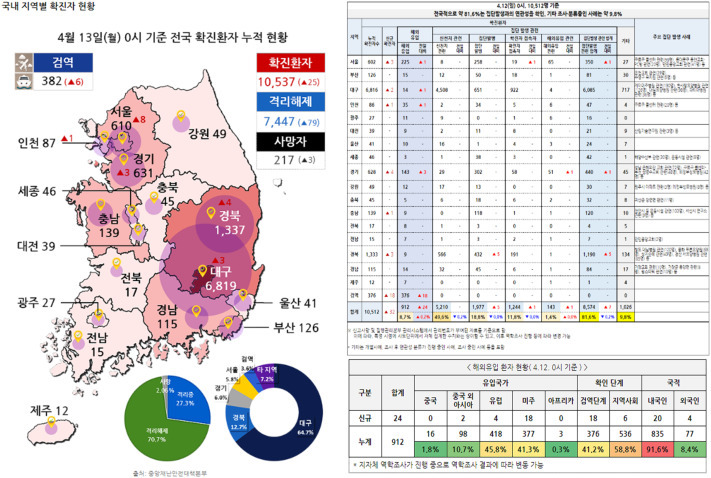
Daily infection status provided by NAVER, an online web and news portal. These charts and maps are linked from the homepage. On the left is a choropleth map of confirmed COVID-19 cases in each province; major cities have bubbles representing number of cases by size. The first pie chart depicts percentages of people in/out of quarantine or deceased, the second shows case share by province. On the right is a table also showing case counts by province, broken down by source of infection (brought in from international travel, community transmission, or “super-spreading events”).
4.2. Contact tracing
KCDC investigators use interviews, mobile phone tracking (every mobile account in South Korea is tied to the owner's national ID), credit card transaction history, and video footage from public surveillance cameras, to reconstruct the individual movements of confirmed COVID-19 cases in fine detail. They can also find or cross-check other people whom the patient had close contact with, prior to quarantine. Through manual effort, these officials can identify potential future cases, and target those people or areas for testing and precautionary self-quarantine (Sonn, 2020).
This form of contact tracing was originally meant for internal usage by health officials in tracking the epidemic. However, following the 2015 MERS outbreak in South Korea, public disclosure provisions were added to the country's Infectious Disease Control and Prevention Act to facilitate sharing these traces with the public. Government officials feared that releasing contact tracing data would negatively impact businesses and hospitals visited by diagnosed cases, but acquiesced to public pressure for more transparency (Spinazze, 2020). This has helped residents understand their personal risk, avoid infection hotspots, or review their own movement history and decide whether to get tested and self-quarantine.
Revealing the movement trajectories of confirmed patients this way has raised concerns of privacy infringement. The information released to the public often includes the exact names of places and specific timestamps the patients visited. Although other personal information such as names and faces are not released to the public, some individuals have attempted to find out their private information for harassment. This is possible because commuting patterns between home and work are clearly revealed in the public movement traces. For example, the 31st patient (whose attendance at the mass church meeting is believed to have caused the Daegu outbreak) was exposed to personal information release, public criticism, and direct threats (BBC News, 2020).
4.3. Text alerting
One of the most effective ways that the Korean government rapidly dispersed these daily updates is emergency SMS messages. All citizens receive daily alert messages through their mobile phones from their local authorities. The alert message arrives with a 40–60 db alarm sound, and contains information from KCDC about newly confirmed patients and their recent trajectories if available. This alert message system was originally implemented by the Ministry of Interior and Safety (MOIS) to inform citizens about any disaster, classified by its degrees of risk (전광준, 2020). These messages are written and sent from provincial governments to anyone within the boundaries of that province, based on their phone's current location. Furthermore, if a known case is discovered by contact tracing to have visited clinics or other public locations in a neighborhood, everyone in that neighborhood receives text messages with those details.
In the case of the coronavirus outbreak, many people found it useful to be promptly notified of the latest updates in nearly real-time, but some raised concerns about the quality and frequency of these alert messages. Because of the loud alarm sound, users reported annoyance at receiving frequent messages, especially when the content is just a reminder of basic safety drills such as “keep your hands clean, wash it thoroughly, or please avoid outdoor activities” (전광준, 2020). Such over-alerting carries risks of reducing user attention or crowding out more important information (National Academies of Sciences, Engineering, and Medicine et al., 2018) Al Jazeera encountered both opinions among South Korean citizens, quoted here (Kasulis, 2020):
“Now, I know which areas to avoid and I do feel like the government is doing a good job at keeping me informed.”
“I cannot disagree with the fact that it's good for people to know if there are infected people visiting the same places that they might go to. But I think the government is sending these messages too frequently … I know I stopped reading them.”
4.4. Digital mapping and alerts
Since the outbreak, many individuals, private companies, and local authorities have developed various applications to cope with this disaster. A common application type is the real-time exposure map, which visualizes the movement trajectories of confirmed cases (as reported in the government reports), along with timestamps and transport mode. For example, several websites (coronamap.site, coronamap.live, coronapath.info) were independently developed and updated regularly with government info from the early days of the epidemic. A mobile application named “Corona 100m” alarms the user when they are within 100 m from the trajectories of confirmed patients, and reached 1 million downloads by Feb 28 (Watson et al., 2020). These applications communicate the trajectories in a visual, interactive format, making it easier for the public to digest this information and adjust their own behavior in response (Fig. 8 ).
Fig. 8.
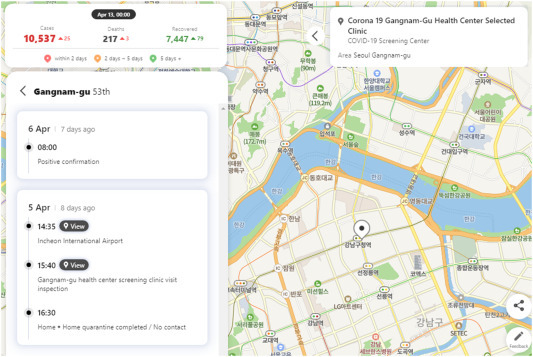
Screenshot of coronamap.live, one of many web and mobile applications developed during the COVID-19 outbreak to map the movement trajectories of confirmed cases in South Korea (홍준서, 2020).
4.5. Digital diagnosis and self-quarantine
While the above applications are focused on disseminating information, the Ministry of Health and Welfare (MOHW) developed a mobile app to monitor potential patients with symptoms. Every traveler or returning resident entering the country is obliged to install this application, and self-report their health condition and any symptoms using the app for 14 days from entry. In case of fever or respiratory discomfort, the users are required to report their health status and contact KCDC to register for testing. Travelers are also required to demonstrate that they can receive calls and be contacted by the government during their time in Korea (김아름, 2020). As of April 1, 2020, to reduce the spread of COVID-19 from international travelers, the Korean government has mandated 14-day self-quarantine for all long-term residents returning from overseas, using the GPS tracking function of the application and the threat of severe legal penalties to enforce this limit on movement.
Fig. 9 shows screenshots from this mobile application. Screen 1 provides language options in Korean, Mandarin, and English. Screen 2 is a series of questions on nationality, travel history, and contact information. Screen 3 provides links to self-diagnosis questions, clinic locations, and direct chat help channels. Screen 4 presents four self-diagnosis questions on fever, cough, sore throat, and dyspnea.
Fig. 9.
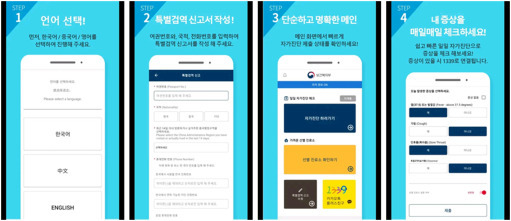
Corona self-check application developed by Ministry of Health and Welfare required for every traveler visiting Korea.
The Ministry of Interior and Safety (MOIS) has also developed an application to monitor self-quarantine and self-monitoring of people's health conditions. People who confirm that they were exposed to the trajectory of a known coronavirus patient should contact KCDC, to be monitored for 14 days. If they have any symptoms, they may receive diagnostic testing free of charge; otherwise, they self-quarantine and regularly respond to monitoring queries. The application also uses the GPS sensor to detect whether the user leaves the boundary of self-quarantine. This is intended to help local governments monitor a large pool of potential patients with minimal labor and cost (뉴시스, 2020; 김아름, 2020).
Fig. 10 shows screenshots from this application, which closely parallels the MOHW app. Screen 1 provides links to self-diagnosis, health advice, and contact lines for health officials. Screen 2 presents the same four self-diagnosis questions as the MOHW app: fever, sore throat, cough, and dyspnea.
Fig. 10.

Self-quarantine monitoring application developed by Ministry of Interior and Safety for tracking cases infected through community transmission.
However, unlike at an airport's border control where people must install the self-check application to pass through, use of the self-quarantine application is voluntary. The installation rate of the application is approximately 35% of the total number of people under monitoring based on the government's guidelines for self-quarantine. Awareness of the application is not widespread given its recent release on March 5, 2020 for Android phones, and March 15, 2020 for iPhone. Users must also carefully review the published movement traces of known infected, and trust in government health procedures enough to voluntarily self-report their condition (Yeonhap, 2020; 김아름, 2020). Further outreach, and mandatory screening in certain public places like transportation hubs or government offices, may help increase the use of the application, and reduce the risk of community transmission (virus spread between unconfirmed cases).
4.6. Automated contact tracing
As the number of active COVID-19 cases grew in the country, it became difficult for health officials to manually perform contact tracing for each individual known case. In response, South Korea's Ministry of Land, Infrastructure, and Transport (MOLIT) developed a “COVID-19 Smart Management System”, in collaboration with the KCDC and Ministry of Science and ICT (MSIT). The system was adapted from an existing “City Data Hub” platform that MOLIT originally developed for smart cities to analyze their traffic, energy use, environment and safety; it was repurposed to help automate contact tracing by combining data from the National Police Agency, three telecommunications firms, and twenty-two credit card companies (MOLIT, 2020). At its launch on March 26, 2020, MOLIT claimed the system would reduce the time consumed for contact tracing an individual from one day to under 10 min.
Prior to the system, KCDC officials needed to communicate by phone through the police or national credit agencies as intermediaries, in order to receive location trace information from the telecoms or credit card companies (see Fig. 11 ). The management system allows investigators to request this data directly from the companies, while enforcing security clearance on different types of data and levels of detail. Patients are only tracked after being interviewed by health investigators and informed that their phone and credit card usage will be monitored. System user activities are logged and subject to audit, and personal data is scheduled to be deleted at the close of the government's official response to COVID-19 (KTV, 2020).
Fig. 11.
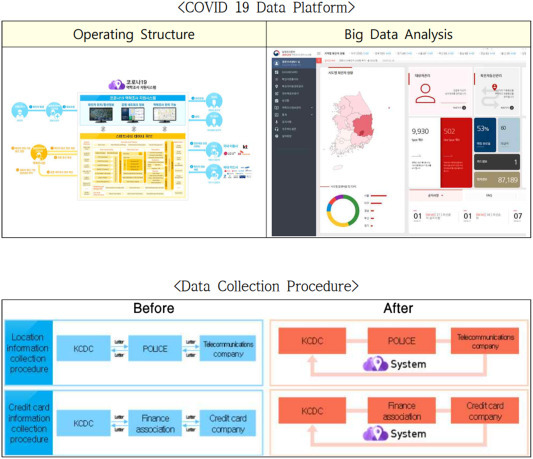
[Clockwise from top left] Operating diagram of MOLIT's COVID-19 Smart Management System; screenshot of user interface of the system; change in communication flow as a result of the system's implementation.
Source: MOLIT Press Release (2020).
5. Conclusion
In this article, we reported on the circumstances of the COVID-19 outbreak in South Korea, its implementation of low-contact testing to scale up diagnostics and reduce health care worker exposure, and how mobile apps and online mapping helped to track its spread and alert the public of their risk of exposure. By a combination of design and technological innovation, these steps have enabled the country to quickly detect, track, and quarantine new infections. Low-contact testing illustrates this well; health officials were able to quickly adapt infrastructure like parking lots into experimental drive-through testing sites, then iterate on their design to improve their hygiene and cost-effectiveness. To meet the challenge of extending low-contact testing to Korea's dense urban cores, they innovated again by developing compact, mobile testing booths accessible to pedestrians.
Part of this ability to rapidly innovate stems from preparation. The first mobile apps to map drive-through test centers and contact traces were created by private developers, highlighting the advantages of a highly-connected population and a thriving local software industry in filling the technology gap left by the public sector. The nation's transport ministry was also able to quickly create an integrated surveillance system for large-scale contact tracing, because it had previously researched and developed “smart city data platforms” meant to handle this sensitive, private information. At a policy level, the national government had already debated and legislated how it would balance patient privacy rights against public demand for contact tracing information years before the COVID-19 outbreak; thus, there was no ambiguity about what data local governments could share for the benefit of public health.
While it isn't clear how much each step directly reduced the rate of infection, it appears that South Korea's overall strategy has been effective in slowing the virus spread. The country faced several potential disadvantages in an outbreak: a highly urbanized population with little room for social distancing, a reluctance to apply complete bans on foreign entry and internal mobility, and unpredictable behaviors from sub-groups that resulted in super-spreading of the virus. These perceived disadvantages may have driven the government to lean on testing and tracking, and improve on its ability to scale up both, in order to maintain a degree of personal freedom in movement and association.
As of this writing, the United States, Canada, and other nations have adopted their own versions of drive-through testing. Singapore and China have implemented similar mobile app and phone tracking procedures for travelers. Yet ultimately their success or failure will depend on how well-prepared their societies were to adopt these strategies, and how quickly they can learn and iterate toward better designs. We hope that the South Korean experiences we've reported here provide useful knowledge for other countries following suit.
In this paper, we did not deeply investigate the rapid development and manufacturing of COVID-19 diagnostic tests, which was critical in enabling the government's strategy of widespread testing, and was the result of lessons learned and policy changes after the 2015 MERS epidemic (Normile, 2020). We also have not discussed in detail the ethical implications of the government's approach to contact tracing, which was effective in identifying future cases and building public trust, but at significant risk of violating individual privacy rights (Sonn, 2020). Also concerning is the disproportionate impact certain individuals or businesses may have experienced by the release of contact tracing information to the public. These issues rightfully invite more scrutiny, as other open, democratic societies grapple with the trade-offs between healthcare regulation vs. private initiative, and individual surveillance vs. privacy protections. For future studies, we hope to gather empirical evidence on these impacts, and take a more critical look at the risks other countries face in adopting South Korea's strategy.
Acknowledgments
We thank the members of Maturepolis Lab at KAIST for helping to identify sources and review the content of this article. We also thank Hee Eun Kim for helping research and translate news articles and other sources. This research was supported by a grant (20TSRD-B151228-02) from Urban Declining Area Regenerative Capacity-Enhancing Technology Research Program funded by the Ministry of Land, Infrastructure and Transport of the Korean government. It is the sole work of the authors, and we report no conflicts of interest.
References
- BBC News BBC; 2020. “At a love motel”: are S Korea virus alerts too revealing? https://www.bbc.com/news/world-asia-51733145 (March 5)
- Jeong G.H., Lee H.J., Lee K.H., Han Y.J., Yoon S., Lee J., Ryu S., Kim D.K., Park M.-B., Lee J.Y., Yang J.W., Effenberger M., Eisenhut M., Hong S.H., Kronbichler A., Shin J.I., COVID-19 Outbreak Research Group, Korea . 2020. Epidemiology and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in South Korea. [DOI] [Google Scholar]
- Kasulis K. Al Jazeera; 2020. S Korea's smartphone apps tracking coronavirus won't stop buzzing. https://www.aljazeera.com/news/2020/04/korea-smartphone-apps-tracking-coronavirus-won-stop-buzzing-200408074008185.html (April 8)
- KCDC KCDC; 2020. Daily briefing report, Jan 20, 2020. http://www.cdc.go.kr (January 20)
- KCDC KCDC; 2020. Daily briefing report and statistics, Feb 28-Mar 8, 2020. http://www.cdc.go.kr (March 8)
- KCDC KCDC; 2020. Daily government statistics, Jan 20-Mar 17, 2020. http://www.cdc.go.kr (March 18)
- KCDC KCDC; 2020. Daily briefing report, Feb 3–4, 2020. http://www.cdc.go.kr (Feb 3–4)
- KCDC KCDC; 2020. Daily briefing report, Feb 18, 2020. http://www.cdc.go.kr (Feb 18)
- KCDC KCDC; 2020. Daily briefing report, Feb 25, 2020. http://www.cdc.go.kr (Feb 25)
- KCDC KCDC; 2020. Daily briefing report, Jan 27–28, 2020. http://www.cdc.go.kr (Jan 27–28)
- KCDC KCDC; 2020. Daily briefing report, Mar 4, 2020. http://www.cdc.go.kr (Mar 4)
- Kim Sun Joo K. Flickr; 2020. COVID_19_Walking_Thru_screening_center_02. https://www.flickr.com/photos/koreanet/49728600513/ (April 2)
- Kim J.Y., Choe P.G., Oh Y., Oh K.J., Kim J., Park S.J., Park J.H., Na H.K., Oh M.D. The first case of 2019 novel coronavirus pneumonia imported into Korea from Wuhan, China: implication for infection prevention and control measures. J. Korean Med. Sci. 2020;35(5):e61. doi: 10.3346/jkms.2020.35.e61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- KOSIS. (2019). KOrean Statistical Information Service. https://kosis.kr/eng/statisticsList/statisticsListIndex.do?menuId=M_01_01&vwcd=MT_ETITLE&parmTabId=M_01_01&statId=1962001&themaId= (August 8)
- KTV Youtube; 2020. [FULL] MOLIT & KCDC Online Briefing on COVID-19 Smart Management System - 코로나19 역학조사 지원시스템 외신브리핑. https://www.youtube.com/watch?v=C9o_HGN6v8E (April 9)
- Ministry of Health and Welfare Coronavirus disease 19(COVID-19). Coronavirus Disease 19 (COVID-19) 2020. http://ncov.mohw.go.kr/en/ (February 25)
- Ministry of Health and Welfare 코로나19 선별진료소 및 국민안심병원 현황 (Corona 19 Screening Clinic and National Security Hospital) https://www.mohw.go.kr/react/popup_200128_3.html Retrieved March 20, 2020, from. (n.d.)
- MOLIT MOLIT Ministry of Land, Infrastructure and Transport; 2020. MOLIT, MSIT and KCDC launch the COVID 19 data platform. - Smart city technology reinvents contact tracing method. http://www.molit.go.kr/english/USR/BORD0201/m_28286/DTL.jsp?id=eng_mltm_new&mode=view&idx=2931 (March 26)
- Moon G. NBC News; 2020. This is how South Korea flattened its coronavirus curve. https://www.nbcnews.com/news/world/how-south-korea-flattened-its-coronavirus-curve-n1167376 (March 24)
- National Academies of Sciences, Engineering, and Medicine, Division on Engineering and Physical Sciences, Computer Science and Telecommunications Board, Committee on the Future of Emergency Alert and Warning Systems: Research Directions . National Academies Press; 2018. Emergency Alert and Warning Systems: Current Knowledge and Future Research Directions. [Google Scholar]
- Normile D. Coronavirus cases have dropped sharply in South Korea. What's the secret to its success? Science. 2020 https://www.sciencemag.org/news/2020/03/coronavirus-cases-have-dropped-sharply-south-korea-whats-secret-its-success (March 17) [Google Scholar]
- Park S.W., Sun K., Viboud C., Grenfell B.T., Dushoff J. Infectious Diseases (Except HIV/AIDS) medRxiv; 2020. Potential roles of social distancing in mitigating the spread of coronavirus disease 2019 (COVID-19) in South Korea. (No. medrxiv;2020.03.27.20045815v1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seoul Metropolitan Government Drive-Through Screening Stations -. 서울시 영문. 2020. http://english.seoul.go.kr/drive-through-screening-stations/ (March 24)
- Sonn J.W. The Conversation; 2020. Coronavirus: South Korea's success in controlling disease is due to its acceptance of surveillance. http://theconversation.com/coronavirus-south-koreas-success-in-controlling-disease-is-due-to-its-acceptance-of-surveillance-134068 (March 19)
- Spinazze G. Bulletin of the Atomic Scientists; 2020. South Korea learned its successful Covid-19 strategy from a previous coronavirus outbreak: MERS - Bulletin of the Atomic Scientists. https://thebulletin.org/2020/03/south-korea-learned-its-successful-covid-19-strategy-from-a-previous-coronavirus-outbreak-mers/ (March 20)
- Watson I., Jeong S. CNN; 2020. South Korea pioneers coronavirus drive-through testing station. https://www.cnn.com/2020/03/02/asia/coronavirus-drive-through-south-korea-hnk-intl/index.html (March 2)
- Watson I., Jeong S., CNN Business CNN; 2020. Coronavirus mobile apps are surging in popularity in South Korea. https://www.cnn.com/2020/02/28/tech/korea-coronavirus-tracking-apps/index.html (February 28)
- Yeonhap Yeonhap News; 2020. 정부 “코로나19 자가격리 앱 설치율 35%…아이폰용 오늘 배포”. https://n.news.naver.com/article/001/0011476220 (March 16)
- Yoon D., Martin T.W. WSJ Online; 2020. How South Korea put into place the world's most aggressive coronavirus testing. https://www.wsj.com/articles/how-south-korea-put-into-place-the-worlds-most-aggressive-coronavirus-testing-11584377217 (March 16)
- 김아름 Financial News; 2020. 원스토어, 코로나19 관련 앱 메인 배치. https://n.news.naver.com/article/014/0004390424 (March 16)
- 김철중 Chosun Ilbo; 2020. 이번엔 “워킹 스루”… 공중전화 박스 형태 코로나 검사 부스 개발. https://news.chosun.com/site/data/html_dir/2020/03/16/2020031600148.html (March 16)
- 노승혁 “드라이브스루 코로나19 검사”…고양시, 안심카 선별진료소 운영 | 연합뉴스. 연합뉴스; 노승혁. 2020. https://www.yna.co.kr/view/AKR20200226037200060 (February 26)
- 뉴시스 dongA; 2020. 질본, “10일부터 ‘코로나19 발생 현황’ 1회 발표…통계 일원화”. http://www.donga.com/news/article/all/20200309/100077766/1 (March 9)
- 윤종열 이재명, “마스크 생산물량 공공기관 통해 거래 필요.” 서울경제; 서울경제. 2020. http://www.sedaily.com/NewsView/1YZ1BAD7WR/GK0201 (February 23)
- 전광준 The Hankyoreh; 2020. [뉴스AS] “손씻기”까지 재난문자로 보내야 하나요? http://www.hani.co.kr/arti/society/society_general/932044.html (March 11)
- 조재환 ZDNet Korea; 2020. 코로나19 드라이브스루 진료소 43곳 지도로 제공. https://www.zdnet.co.kr/view/?no=20200309163117 (March 10)
- 퍼즐벤처스 OilNow [Android] https://www.oilnow.co.kr/ (n.d.)
- 한상봉 Seoul Public News; 2020. [단독] 비싸고 통풍 안 되고…경기도 “컨테이너 선별진료소” 도마에. https://go.seoul.co.kr/news/newsView.php?id=20200312011003&wlog_tag3=naver (March 11)
- 홍준서 코로나맵 라이브. 2020. https://coronamap.live/
- 황선윤 Joongang Ilbo; 2020. 진화하는 코로나 채취···이번엔 “초스피드 워킹 스루” 나왔다. https://n.news.naver.com/article/025/0002989001 (March 31)