

Abstract
With increasing numbers of Coronavirus Disease 2019 (COVID19) cases due to efficient human-to-human transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in the United States, preparation for the unpredictable setting of labor and delivery is paramount. The priorities are 2-fold in the management of obstetric patients with COVID-19 infection or persons under investigation (PUI): (1) caring for the range of asymptomatic to critically ill pregnant and postpartum women; (2) protecting health care workers and beyond from exposure during the delivery hospitalization (health care providers, personnel, family members). The goal of this review is to provide evidence-based recommendations or, when evidence is limited, expert opinion for anesthesiologists caring for pregnant women during the COVID19 pandemic with a focus on preparedness and best clinical obstetric anesthesia practice.
The management of obstetric patients infected with Coronavirus Disease 2019 (COVID-19) due to human-to-human transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) requires quite unique considerations—from caring for critically ill pregnant and postpartum women to protecting health care workers from exposure during the delivery hospitalization (health care providers, personnel, family members, and beyond). The goal of this review is to provide evidence-based recommendations or, when evidence is limited, expert opinionfor anesthesiologists caring for pregnant women during the COVID 19 pandemic with a focus on preparedness and best clinical obstetric anesthesia practice.
CLINICAL MANIFESTATION OF COVID-19 INFECTION IN PREGNANCY
In principle, the clinical characteristics reported in pregnant women with confirmed COVID-19 infection in China have been consistent with those reported among nonpregnant adults, with better maternal and neonatal outcomes with COVID-19 infection compared with the 2002–2003 severe acute respiratory syndrome (SARS) outbreak from SARS CoV 1 infection.1–3
The signs and symptoms of COVID-19 infection in a large data set in nonpregnant patients from China were fever (99%), fatigue (70%), cough (59%), shortness of breath (31%), myalgias (35%), headache (6.5%), sore throat (17%), diarrhea (10%), nausea (10%), and vomiting (4%).4 An additional manifestation noted among patients with COVID-19 infection is the sudden loss (or reduction) of the sense of smell and taste, which is currently recommended by the American Academy of Otolaryngology-Head and Neck Surgery as part of screening for COVID-19 infection.5
In pregnancy, presentation of COVID-19 infection appears similar, but many of these nonspecific symptoms may be attributed to symptoms of pregnancy and labor.2 For example, signs of latent labor may include myalgias and diarrhea; preeclampsia can present with headache; shortness of breath is perceived during pregnancy and labor; and chorioamnionitis may cause tachycardia and fever, thus,leading clinicians to overlook COVID-19 infection as a possible diagnosis. In addition, women infected with COVID-19 may be asymptomatic until their admission in labor and beyond,6 which in itself poses a significant risk of exposure for their family members (including the newborn) and all providers involved in their clinical care.
CONSIDERATIONS FOR TESTING ON ADMISSION
Screening criteria for COVID-19 infection usually include the following: (1) fever, (2) cough or shortness of breath, (3) diarrhea, and (4) any possible exposure to COVID-19. However, because women with COVID-19 infection may be asymptomatic at the time of admission and because some may present with overlapping pregnancy symptoms, universal screening may miss pregnant women infected with SARS-CoV-2 in communities with a high prevalence or high projected infection rate (eg, New York, New Orleans, Detroit, Chicago, Miami).7,8 Universal testing with real-time reverse transcriptase–polymerase chain reaction (RT-PCR) tests for SARS-CoV-2 viral ribonucleic acid (RNA) may improve case detection in high prevalence communities. However, current assays may return false-negative results if the viral load is low or if specimen collection is incomplete.
The goals of COVID-19 testing specific to pregnant patients admitted to labor and delivery units are 2-fold: (1) to prevent vertical transmission and ensure separation of the neonate after birth and (2) to protect health care workers by ensuring use of appropriate personal protective equipment (PPE). Besides the unclear sensitivity of RT-PCR testing, the time for nucleic acid detection varies between 6 and 8 hours or longer depending on availability. Therefore, management of women on Labor and Delivery Units located in a community with a high prevalence of COVID-19 infection should err on the side of caution.
For purposes of clinical management and PPE use, women may therefore be categorized as follows (1) COVID-19 negative, (2) asymptomatic, (3) symptomatic (persons under investigation [PUI]), and (4) personally positive for COVID-19 testing. This information should be made available to all health care providers and updated at all times as it may change during the course of labor (from asymptomatic to symptomatic or, if tested, once the result becomes available).
Women who are COVID-19 positive (or high-risk PUI) should ideally be placed in an isolation room. Airborne infection isolation rooms (single-patient negative-pressure rooms with a minimum of 6 air changes per hour), if available, should be used if performance of aerosolizing procedures is anticipated. In general, isolation rooms suitable for droplet and contact precautions are recommended.9 Strategies for exposure mitigation and cohorting, as well as considerations for transportation of patients who are PUI or COVID-19 should follow the same recommendations as for general patient cases.10
SYSTEMS PREPARATION
A multidisciplinary team of anesthesiologists, obstetricians, labor and delivery nurses, neonatologists, critical care experts, infectious disease and infection control experts, employee health services, environmental health services, and telemedicine services should create and implement protocols to support the management of patients with COVID-19 infection in the setting of a Labor and Delivery Unit. A side-by-side comparison of recommendations from many professional societies for labor and delivery units is presented in Table 1. For institutions with multiple labor and delivery sites, consideration should be given to designating 1 institution to care for patients with COVID-19 infection. This proved useful in managing patients during the SARS epidemic and for cases in the recent COVID-19 outbreak in Wuhan, China.11–13
Table 1.
Professional Society Recommendations for Labor and Delivery Comparison of Recommendations for Intrapartum Anesthetic Care of Known or Suspected COVID-19 Patients
| SOAP | ACOG | SMFM-SOAP | SOGC | RANZCOG | RCOA-OAA | RCOG | |
|---|---|---|---|---|---|---|---|
| Initial publication | March 15, 2020 | March 23, 2020 | March 25, 2020 | March 17, 2020 | March 23, 2020 | March 16, 2020 | March 15, 2020 |
| Date updated | March 23, 2020 | March 26, 2020 | March 27, 2020 | March 26, 2020 | March 29, 2020 | March 27, 2020 | March 28, 2020 |
| Isolation room | Yes, preferably negative pressure | - | Yes, negative pressure for AGP | - | Yes | - | Yes |
| Mask on patient | - | Yes, surgical | Yes, surgical | Yes, surgical | Yes, surgical | Yes, surgical | Yes, surgical |
| Visitors and support people | Limit visitors and support people | Limit visitors and support people | Limit or eliminate visitors, special considerations apply | Yes, single asymptomatic | Yes, limited, asymptomatic | - | Yes, single asymptomatic, limit visitors to wards |
| PPE for non-AGP, first stage labor | Droplet and contact | Droplet and contact, airborne preferred | Droplet and contact | Droplet and contact | - | - | Droplet and contact |
| PPE for vaginal delivery, second stage labor | Droplet and contact | Droplet and contact, airborne preferred | Airborne reasonable, consider surgical drapes as additional barrier | Droplet and contact, consider airborne if risk of sudden deterioration | - | - | Droplet and contact |
| PPE neuraxial analgesia | Droplet and contact | Droplet and contact, airborne preferred | - | - | - | Droplet and contact | - |
| Neuraxial analgesia and anesthesia COVID-specific concerns | Labor analgesia encouraged early; performedby most experienced provider | - | Labor analgesia encouraged early | Labor analgesia encouraged early; performedby most experienced provider | - | Labor analgesia encouraged early, suggestion to check platelet count | Labor analgesia encouraged early |
| Use of nitrous oxide | Consider suspending use | - | Consider suspending use | - | Yes, no evidence of AGP, use filter | Yes, no evidence of AGP, use filter | Yes, no evidence of AGP, use filter |
| Use of postoperative NSAIDs | Data lacking, likely safe if asymptomatic | Data lacking | Data lacking, continue to use in asymptomatic and mildly symptomatic patients | - | - | - | - |
| Mode of delivery | - | Per obstetric indications | - | Per obstetric indications | Per obstetric indications | - | Per obstetric indications, no water births |
| Operative delivery | - | Follow usual clinical indications | Not precluded, consider performing in OR | - | - | - | Individualized decision |
| Elective cesarean or induction of labor with current COVID-19 infection | - | - | - | - | Preferable to delay until completion of isolation period, if possible | - | Evaluate safety of delaying procedure |
| PPE for cesarean delivery | Anesthesia team: droplet, contact, ideally airborne; ifGA planned: all staff wear airborne, minimize staff in room at time of intubation and extubation |
Ideally airborne for all staff | Ideally airborne for all staff for all cases | Airborne advised; if GA planned: all staff wear airborne, minimize staff in room at time of intubation and extubation |
- | Neuraxial planned (and low risk of GA): droplet and contact; emergency cesarean: as above, risk assess need for airborne PPE; if GA planned: airborne PPE for all staff in room during intubation and extubation, minimize staff present, airborne for all staff if no time to allow for air turnover |
Neuraxial planned (and low risk of GA): droplet, scrubbed staff waits outside of room until block successful; emergency cesarean: droplet for neuraxial, airborne if risk of GA; if GA planned: airborne for all staff |
Abbreviations: ACOG, xxx; AGP, xxx; COVID-19, Coronavirus disease 2019; GA, xxx; NSAIDs, nonsteroidal anti-inflammatory drugs; OR, xxx; PPE, personal protective equipment; RANZCOG, xxx; RCOA-OAA, xxx; RCOG, xxx; SMFM-SOAP, xxx; SOAP, xxx; SOGC, xxx.
Resource allocation within the Labor and Delivery Unit as well as other units (including intensive care unit) should be proactively addressed. It is imperative to establish a back-up team to care for patients without COVID-19 infection due to the time-intensive tasks of donning/doffing PPE, transporting the patient, providing anesthetic care, and performing surgery in patients with active COVID-19 infection.
From a logistical standpoint, a designated operating room within the Labor and Delivery Unit should be prepared. Dedicated trays (or carts) containing the most commonly used supplies and drugs for both neuraxial labor analgesia and cesarean delivery should be available to minimize traffic and contamination of anesthesia workstations and other anesthesia equipment.
PATIENT EVALUATION AND MONITORING
A pregnant woman who is PUI or COVID-19 positive should be evaluated (limiting unnecessary encounters) including vital signs, physical examination, and review of laboratory tests (complete blood count, comprehensive metabolic panel, and arterial blood gas, if needed) to assess appropriate level of care and monitoring plan for potential deterioration. Early multidisciplinary collaboration should be arranged to determine level of care, fetal monitoring, and delivery plan. Discussion of the risks and benefits for administering steroids for fetal lung maturity, magnesium for neuroprotection, and indomethacin for tocolysis should be addressed, since there is concern those drugs may worsen COVID-19 infection (Table 2).9
Table 2.
Specific Considerations for Medication Use in PUI or COVID-19–Positive Patients During Labor, Delivery, and the Postpartum Period
| Considerations | Case Context | Mechanism | |
|---|---|---|---|
| Oxygen9 | The routine use of oxygen for fetal indications should be suspended | Overall, the use of oxygen for fetal indications is controversial | The use of high-flow nasal cannula or facemask oxygen may be an aerosolizing procedure |
| Nitrous oxide9 | Discuss the relative risks and benefits of nitrous oxide for labor analgesia and consider suspending its use | Overall, for all parturients | “There is currently insufficient information about the cleaning, filtering, and potential aerosolization of nitrous oxide in labor analgesia systems in the setting of COVID-19” |
| Remifentanil/ fentanyl14 |
Consider avoiding the use of IV PCA opioids (remifentanil/fentanyl) for labor analgesia | Women at risk for respiratory depression and opioid-induced nausea and vomiting | Opioid-induced respiratory depression increases the risk of sedation, respiratory depression, and oxygen desaturation, and increases the risk for emergent airway instrumentation and aerosolizing procedures |
| Ketorolac/ ibuprofen9,15 |
For women who are asymptomatic or mildly symptomatic that require analgesic medication beyond acetaminophen, NSAIDs can continue to be used, as the alternative of opioids likely poses more clinical risks. For sick COVID-19 patients, consider avoiding NSAIDs |
It has been suggested that the use of NSAIDs for management of COVID-19 symptoms may aggravate COVID-19 infection trajectory (although the evidence is not robust) The use of ACE inhibitors was suggested to increase the risk for COVID-19 infection |
NSAIDs are associated with increased ACE2, to which COVID-19 binds |
| Dexamethasone9 | Consider avoiding the use of dexamethasone for PONV prophylaxis | In all women undergoing cesarean delivery, alternative antiemetics should be administered to prevent vomiting | Prolonged exposure to high-dose steroids has been associated with worsening COVID-19 outcomes in the general population |
| Carboprost (Hemabate)14 | Consider avoiding the use of carboprost for treatment of uterine atony | For women at risk of bronchospasm, use alternative second-line uterotonics | Prostaglandin F2 alpha causes bronchoconstriction and pulmonary vasoconstriction |
| Magnesium sulfate9 | Consider avoiding or as an alternative to usual dosing, a 4g bolus dose may be preferred in the setting of mild respiratory distress | For women with increasing oxygen requirement, the risk:benefit ratio should be considered before using magnesium for fetal neuroprotection, or for preeclampsia without severe features | Magnesium sulfate has central nervous system and respiratory depressant effects |
Abbreviations: ACE, xxx; COVID-19, Coronavirus Disease 2019; IV, xxx; NSAIDs, nonsteroidal anti-inflammatory drugs; PCA, xxx; PONV, xxx; PUI, persons under investigation.
Avoiding urgent cesarean delivery is essential to reduce the risk for general anesthesia and provider exposure during uncontrolled transfers to the operating room. Therefore, ongoing assessment of both maternal and fetal statuses are key to balance risks of prolonged labor versus cesarean delivery. It is unclear whether uterine decompression improves maternal respiratory status and how the potential benefit balances against the known operative risks in the setting of COVID-19. On the other hand, prolonged maternal hypoxemia may ultimately cause fetal acidemia, leading to a more urgent cesarean delivery.9
Routine monitoring should include frequent vital signs (tailored to the current clinical status and adjusted as necessary) with the addition of continuous pulse oximetry and strict input and output measurements to assure fluid restriction. Pulse oximetry goal should be an oxygen saturation ≥95%. Early warning criteria systems specific for obstetric patients may aid in early detection and prompt escalation of care.16
Women requiring supplemental oxygen, who develop increasing oxygen requirements or worsening hypoxia (pulse oximetry [Spo2] < 95%), should have prompt arterial blood gas analysis with frequent clinical reassessment to guide the requirement for escalation of care and mechanical ventilation. High-flow nasal oxygen or noninvasive ventilation may be considered as temporizing measures but are generally discouraged due to the potential for greater aerosolization. In addition, increasing oxygen requirements serve as a marker of disease progression, with increasing risk of atelectasis and pulmonary consolidation. It is recommended to perform early endotracheal intubation in a controlled manner minimizing exposure to health care workers and equipment with airborne precautions in an urgent/emergent situation.17
One of the frequent complications of patients with COVID-19 is acuterespiratorydistresssyndrome(ARDS). Ventilator management strategies for ARDS involve lung-protective strategies such as low tidal volumes (6 mL/kg using predicted body weight), plateau pressure <30 cm H2O, and the combined use of reduced Fio2with increases in positive end-expiratory pressure (PEEP) to maintain a Pao2 of 65–90 mm Hg.18 Useful ventilator titration techniques using the ARDSnet ventilator protocol can be found in http://www.ardsnet.org/files/ventilator_protocol_2008-07.pdf.17 Pregnant patients have a physiological decrease in Paco2, and it is recommended to maintain a Paco2 of 28–32 mm Hg with ventilation to augment off-loading of oxygen to the fetus. However, the priority is maintaining oxygenation with low tidal volumes and PEEP, and this strategy may not allow for maintaining the physiologic Paco2 in pregnancy. Multidisciplinary discussion should determine the fetal monitoring and delivery plan during mechanical ventilation.
LABORING PATIENTS WITH ACTIVE COVID-19 INFECTION
Neuraxial labor analgesia remains a mainstay of obstetric care even with concurrent COVID-19 infection. In fact, early epidural placement is desirable to avoid exacerbation of respiratory symptoms with labor pain and to reduce the likelihood of general anesthesia if intrapartum cesarean delivery becomes needed.
The benefits of neuraxial analgesia in the setting of COVID-19 pneumonia are 2-fold: (1) for the patient, it will help avoid any exacerbation of respiratory status with intubation and mechanical ventilation and (2) for health care providers, it reduces the risks associated with aerosol exposure and transmission of COVID-19 infection during intubation and extubation, if general anesthesia is provided.
The risk of COVID-19 exposure for the anesthesiologist during neuraxial labor analgesia placement is presumably low, since this is not an aerosol-generating procedure. All health care workers in the room should wear contact (impervious gown and gloves) and droplet (surgical mask and eye protection) precautions. The patient should wear a surgical mask at all times to limit droplet spread, and the number of personnel present during placement of neuraxial labor analgesia should be minimized but with assistance readily available. Several strategies may minimize contamination of equipment and COVID-19 exposure in anesthesiologists, while also minimizing the consumption of PPE (Box 1 and Figure).
Figure.
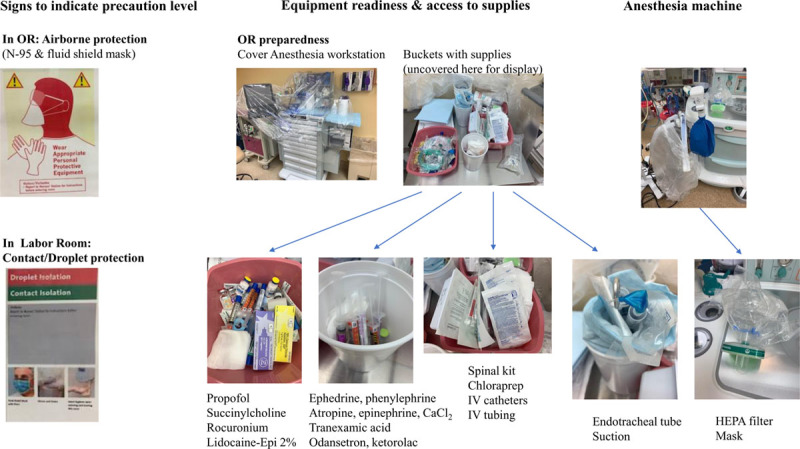
Set-up for operating room and labor epidural analgesia. HEPA indicates xxx; IV, xxx; OR, xxx.
Box 1. Empirical Strategies That May Be Implemented to Minimize Contamination of Equipment and COVID-19 Exposure of Anesthesiologists to Reduce the Use of PPE.
Limit in-person encounters for preanesthesia evaluations by utilization of video—consultations (including for antenatal consultations for high-risk patients).
Limit encounters on admission to the labor floor—consider using mounted iPads in each labor room for hourly evaluations.
Limit the use of electronic devices or pens for written consents by use of electronically documented witnessed verbal consents.
Avoid bringing into the patients’ room the epidural cart or tray—the required equipment (epidural kit) and drugs should be prepared and brought into the room in a bag before the procedure.
Have the most experienced anesthesiologist perform the procedure to ensure adequate placement and reduce the risk of accidental dural puncture that may require an epidural blood patch.
Increase the dosing of neuraxial medications for labor analgesia (eg, increasing the bupivacaine concentration from 0.0625% to 0.1%) or changing the setting of the programmed epidural intermittent bolus (eg, increasing the volume from 5 to 8 mL, or decreasing the interval from every 45 to 30 minutes) or adding neuraxial adjuvants (eg, epidural clonidine) to minimize intrapartum breakthrough pain requiring epidural top-up.
Round on parturients with video or phone calls into the patient’s room for hourly assessments of general status and effects of neuraxial analgesia.
Ensure appropriate cleaning of all equipment in the room including the epidural pump and the on demand-button.
Limit encounters for postpartum rounds by utilization of video—consultations.
Consider suspending prolonged patient-controlled epidural analgesia services (if applicable).
A parturient who is symptomatic PUI, or COVID-19 positive, should have a complete blood count before neuraxial analgesia placement. Early studies from China suggested that thrombocytopenia may be associated with COVID-19 infection; in a cohort of 1099 patients, 36.2% had thrombocytopenia (<150,000 × 106/L).19 A meta-analysis of 1779 patients with COVID-19 infection observed that platelet counts are lower in patients with more severe disease.20 Though less common, a platelet count <100,000 × 106/L can occur; 3 studies of 243 patients reported a total of 6.6% patients with that level of thrombocytopenia.21–23
We suggest a platelet count on admission without the need to check serial counts before needle placement unless there is a major change in clinical symptoms. It is generally safe to perform neuraxial procedures at platelet counts of 70,000 × 106/L or above,24 and, given the rare risk of spinal/epidural hematoma and the much higher risk of respiratory compromise with general anesthesia, neuraxial procedures at even lower platelet counts should be considered.
While theoretically possible, the risk of epidural or subarachnoid space seeding with viremic blood, causing encephalitis or meningitis, is exceedingly rare. At the time of this writing, there are 77 pregnant women reported in the literature who received uneventful neuraxial procedures for cesarean or vaginal delivery (4 combined spinal-epidural, 27 epidural, 46 spinal procedures; Table 3).6,25–29 Spinal, combined spinal-epidural, epidural procedures all are acceptable, and no technique confers more risk that the other based on the literature available. None of the patients experienced neurologic sequelae.
Table 3.
Neuraxial Procedures Performed in Pregnant Women With COVID-19 Infection
| Author | n | Neuraxial Procedure | Respiratory Status at the Time of Delivery | Febrile Before Procedure? | Neurologic Sequelae |
|---|---|---|---|---|---|
| Bauer et al25 | 14 | 1 CSE, 13 epidural | CT or radiological evidence of pneumonia 14 (100%), 1 patient on maximal noninvasive ventilation at time of CD | 10 (71%) | None |
| Chen et al26 | 14 | 14 epidural | 14 (100%) CT evidence of pneumonia | 4 (29%) | None |
| Xia et al28 | 1 | 1 spinal | Spo2 =92% on room air, CT evidence of pneumonia | 1 (100%) | None |
| Song et al27 | 1 | 1 CSE | Spo2 =86%–90% on room air, CT evidence of pneumonia | 1 (100%) | None |
| Breslin et al6a | 2 | 2 CSE | Asymptomatic at the time of placement, found to have COVID-19 infection postpartum | 0 | None |
| Zhong et al29 | 45 | Spinal | Mild symptoms, no cases of severe pneumonia | While hospitalized, 5 (11%) of entire cohort including 4 orthopedic patients | None |
Abbreviations: CD, cesarean delivery; COVID-19, Coronavirus Disease 2019; CSE, combined spinal-epidural; CT, computed tomography; Spo2, pulse oximetry.
aPersonal communication with Ruth Landau on March 29, 2020.
Current recommendations on the use of nitrous oxide (Entonox) for labor analgesia suggest “there is insufficient information about the cleaning, filtering, and potential aerosolization of nitrous oxide in the setting of COVID-19.” Individual Labor and Delivery Units should consider suspending use.9 Additionally, the practice of high-flow oxygen for fetal distress does not improve fetal outcomes and should be suspended due to the risk of aerosolization.9
ANESTHESIA FOR CESAREAN DELIVERY
In reports from China, most women with a diagnosis of COVID-19 infection underwent a cesarean delivery.25 In the absence of universal testing and rapid availability of results, COVID-19 status may not necessarily be known at the time of cesarean delivery. The baseline failure rate for conversion of labor epidural analgesia to cesarean delivery anesthesia is 5%.30 Urgent intrapartum cesarean delivery represents an important risk factor for failed conversion from intrapartum neuraxial labor analgesia to cesarean delivery anesthesia―therefore, ongoing communication with the obstetricians is crucial to allow safe transfer to the operating room, and adequate time for initiation of surgical block to avoid general anesthesia.30 To minimize the risk of exposure during urgent endotracheal intubation, airborne protection (N95 respirator mask) is recommended for all providers in the operating room unless the patient is known to be COVID-19 negative.
A publication from Wuhan, China, describing outcomes in 17 COVID-19–positive women undergoing cesarean delivery, concluded that “excessive hypotension” occurred in 12 of 14 cases with epidural anesthesia in comparison with the 3 women who had received general anesthesia; however, information about the blood pressure trends and description of the use of vasopressors is not reported.26 A larger case series of 49 patients receiving spinal anesthesia (45 for cesarean delivery and 4 for orthopedic procedures) was welltolerated with stable blood pressure.29
In our early experience, maternal hypotension during cesarean delivery with epidural or spinal anesthesia has not been noted, most likely because prevention of hypotension with phenylephrine is part of our routine clinical practice. Along with antihypotensive medication, antiemetic medication should also be administered. However, we recommend using an alternative to dexamethasone in a PUI or patient with known COVID-19 infection given the risk of worsening clinical severity.14 Specific considerations for medication use in PUI or COVID-19–positive patients during labor, delivery, and the postpartum period are described in Table 2.
VERTICAL TRANSMISSION
Current understanding is that there is little evidence for vertical transmission in women who develop COVID-19 pneumonia in late pregnancy.2,31–35 However, cases of possible in utero infection seem to be emerging including a recent report of a neonate born to a COVID-19 infected mother. This suggests in utero infection during the 23 days between maternal infection and delivery 23 days later and supported by elevated immunoglobulinM (IgM)antibodies, which are not transferred to the fetus via the placenta.36–39 Serological testing of virus-specific IgG and IgM antibodies may alternatively be used if RT-PCR testing is not available or if RT-PCR seems to be yielding a false-negative result.40
POSTPARTUM CONSIDERATIONS
Postpartum considerations for parturients with COVID-19 infection include adequate management of usual postpartum issues (postpartum hemorrhage, pain, hemodynamic status) as well as judicious fluid management, surveillance for respiratory decompensation, and early involvement of subspecialty care as needed. Appropriate isolation of mother and child on the postpartum unit is also recommended.41
Postpartum Hemorrhage
In the setting of postpartum hemorrhage due to uterine atony, carboprost tromethamine (Hemabate) followed by endotracheal intubation was reported to have precipitated immediate and prolonged bronchospasm in a patient who was subsequently found to be COVID-19 positive.6,42 Oxytocin and methylergonovine as a second-line choice may be preferred, due to the potential for bronchospasm with carboprost tromethamine (Hemabate), and aerosolization of viral particles during bronchospasm management.
Postpartum PainManagement
It has been posited that nonsteroidal anti-inflammatory drugs (NSAIDs) for management of symptoms suggestive of COVID-19 infection may worsen the clinical course of COVID-19 patients; however, this remains controversial and robust data are lacking. At this point, for women who are asymptomatic or mildly symptomatic with pain not wellcontrolled with acetaminophen, NSAIDs can continue to be used, as the alternative of opioids likely poses more clinical risks.9
Management of Postdural PunctureHeadache
There are no reported cases of accidental dural puncture resulting in postdural puncture headache (PDPH) in a patient with a COVID-19 infection, and consequently, no available guidance. Similar to usual care, conservative measures should be initially provided.
Usual contraindications to the performance of an epidural blood patch (eg, fever, thrombocytopenia, or other coagulation issues) should apply in a COVID-19 patient. Mitigating the risk of a serious neurologic complications with untreated PDPH43 versus that of viral seeding in the epidural space with an epidural blood patch will require a case-by-case approach. Postponing the epidural blood patch is recommended in women who are actively ill. Individual assessment of the benefits and risks should be assessed and shared decision-making should be engaged with the patient before proceeding.
Because a nasal sphenopalatine ganglion (SPG) block is likely an aerosol-generating procedure due to the injection/insertion directly into the nasal cavity, it should be avoided to minimize the risk of transmission to health care workers.
CONCLUSIONS
Key points emerging in the past weeks from the literature and our experience in Labor and Delivery Units in the United States are that pregnant women may be asymptomatic on admission in labor, and that symptoms of COVID-19 infection may initially be missed or obscured if chorioamnionitis is suspected during labor. Although most women with COVID-19 infection will not present with pneumonia and respiratory decompensation during labor, escalation of care and advanced critical care resources may become necessary in the postpartum period.
In fact, most of the considerations surrounding management of the parturient with suspicion of or known COVID-19 infection include not only best strategies to ensure safe care for the parturient but also thoseto prevent health care worker exposure to SARS-CoV-2 and contracting COVID-19.
Anesthesiologists are deemed at significant risk of viral exposure during endotracheal intubations of COVID-19–infected patients, and all strategies should be applied to avoid general anesthesia in women who are either untested or known to be COVID-19 positive.
Early neuraxial labor analgesia is strongly recommended to ensure availability of neuraxial anesthesia in the event of an intrapartum cesarean delivery, and spinal anesthesia should be provided if needed. If deemed necessary and unavoidable, provision of general anesthesia should follow general recommendations for intubation and extubation in the setting of COVID-19–infected patients.
The changes in workflow that result from the need to ensure adequate PPE (contact/droplet protection for nonaerosolizing procedures such as [eg,epidural placement] or airborne protection for cesarean deliveries due to the possible conversion to general anesthesia) are considerable and require thorough planning and preparedness.
Close communication around COVID-19 status of all patients admitted to the Labor and Delivery Unit is essential, and anticipation of emergencies is of the essence. Overall, providing thebest clinical care for pregnant and postpartum women with COVID-19 infection also must take into account strategies to prevent health care worker exposure to SARS-CoV-2 and contracting COVID-19.
DISCLOSURES
Name: Melissa Bauer, DO.
Contribution: This author helped write the manuscript and edit the critical content.
Name: Kyra Bernstein, MD.
Contribution: This author helped write the manuscript and edit the critical content.
Name: Emily Dinges, MD.
Contribution: This author helped write the manuscript and edit the critical content.
Name: Carlos Delgado, MD.
Contribution: This author helped write the manuscript and edit the critical content.
Name: Nadir El-Sharawi, MD.
Contribution: This author helped write the manuscript and edit the critical content.
Name: Pervez Sultan, MD.
Contribution: This author helped write the manuscript and edit the critical content.
Name: Jill M. Mhyre, MD.
Contribution: This author helped write the manuscript and edit the critical content.
Name: Ruth Landau, MD.
Contribution: This author helped write the manuscript and edit the critical content.
This manuscript was handled by: Thomas R. Vetter, MD, MPH.
FOOTNOTES
GLOSSARY
- ACE
- xxx
- ACOG
- xxx
- AGP
- xxx
- ARDS
- acute respiratory distress syndrome
- CD
- cesarean delivery
- COVID-19
- Coronavirus Disease 2019
- CSE
- combined spinal-epidural
- CT
- computed tomography
- Fio2
- = xxx
- GA
- xxx
- HEPA
- xxx
- IgM
- immunoglobulin M
- IV
- xxx
- NSAIDs
- nonsteroidal anti-inflammatory drugs
- OR
- xxx
- Paco2
- partial pressure of carbon dioxide
- Pao2
- xxx
- PCA
- xxx
- PEEP
- positive end-expiratory pressure
- PDPH
- postdural puncture headache
- PONV
- xxx
- PPE
- personal protective equipment
- PUI
- persons under investigation;
- RANZCOG
- xxx
- RCOA-OAA
- xxx
- RCOG
- xxx
- RNA
- ribonucleic acid
- RT-PCR
- real-time reverse transcriptase–polymerase chain reaction
- SMFM-SOAP
- xxx
- SOAP
- xxx
- SOGC
- xxx
- Spo2
- pulse oximetry
- SARS
- severe acute respiratory syndrome
- SARS-CoV-2
- severe acute respiratory syndrome coronavirus 2
- SPG
- sphenopalatine ganglion
Funding: None.
The authors declare no conflicts of interest.
Reprints will not be available from the authors.
REFERENCES
- 1.Qiao J. What are the risks of COVID-19 infection in pregnant women? Lancet. 2020;395:760–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395:809–815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liu Y, Chen H, Tang K, Guo Y. Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy. J Infect. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.American Academy of Otolaryngology-Head and Neck Surgery. COVID-19 Anosmia Reporting Tool for Clinicians. 2020. Available at: https://www.entnet.org/content/reporting-tool-patients-anosmia-related-covid-19. Accessed March 28, 2020. [DOI] [PubMed]
- 6.Breslin N, Baptiste C, Miller R. COVID-19 in pregnancy: early lessons. Am J Obstet Gynecol MFM. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Coronavirus Disease 2019 (COVID-19): Cases in the U.S. Centers for Disease Control and Prevention. 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html. Accessed March 27, 2020.
- 8.Institute for Health Metrics and Evaluation (IHME). COVID-19 Projections. 2020Available at: http://www.healthdata.org/data-visualization/covid-19-us-state-state-projections. Accessed March 27, 2020.
- 9.Society for Maternal-Fetal Medicine, Society for Obstetric and Anesthesia and Perinatology. Labor and Delivery COVID-19 Considerations. 2020Available at: https://s3.amazonaws.com/cdn.smfm.org/media/2277/SMFM-SOAP_COVID_LD_Considerations_3-27-20_(final)_PDF.pdf. Accessed March 27, 2020.
- 10.Center for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/infection-control/control-recommendations.html#Patient_Placement. Accessed March 27, 2020.
- 11.Zhang HF, Bo LL, Lin Y, et al. Response of Chinese Anesthesiologists to the COVID-19 outbreak. Anesthesiology. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Haines CJ, Chu YW, Chung TK. The effect of severe acute respiratory syndrome on a hospital obstetrics and gynaecology service. BJOG. 2003;110:643–645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Maxwell C, McGeer A, Tai KFY, Sermer M. Maternal Fetal Medicine Committee; Infectious Disease Committee. Management guidelines for obstetric patients and neonates born to mothers with suspected or probable severe acute respiratory syndrome (SARS). J Obstet Gynaecol Can. 2009;31:358–364.19497157 [Google Scholar]
- 14.Society for Obstetric and Anesthesia and Perinatology. Interim Considerations for Obstetric Anesthesia Care related to COVID19. 2020. Available at: https://soap.org/wp-content/uploads/2020/03/SOAP_COVID-19_Obstetric_Anesthesia_Care_032320.pdf. Accessed March 27, 2020.
- 15.Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mhyre JM, D’Oria R, Hameed AB, et al. The maternal early warning criteria: a proposal from the national partnership for maternal safety. J Obstet Gynecol Neonatal Nurs. 2014;43:771–779. [DOI] [PubMed] [Google Scholar]
- 17.Jin YH, Cai L, Cheng ZS. for the Zhongnan Hospital of Wuhan University Novel Coronavirus Management and Research Team, Evidence-Based Medicine Chapter of China International Exchange and Promotive Association for Medical and Health Care (CPAM). A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil Med Res. 2020;7:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Duarte AG. ARDS in pregnancy. Clin Obstet Gynecol. 2014;57:862–870. [DOI] [PubMed] [Google Scholar]
- 19.Guan Wj, Ni Zy, Hu Y, et al. Clinical characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lippi G, Plebani M, Henry BM. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: ameta-analysis. Clin Chim Acta. 2020;506:145–148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Huang C, Wang Y, Li X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Liu Y, Yang Y, Zhang C. Clinical and biochemical indexes from 2019-nCoV infected patients linked to viral loads and lung injury. Sci China Life Sci. 2020;63:364–374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhou F, Yu T, Du R. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lee LO, Bateman BT, Kheterpal S, et al. Multicenter Perioperative Outcomes Group Investigators. Risk of epidural hematoma after neuraxial techniques in thrombocytopenic parturients: a Report from the Multicenter Perioperative Outcomes Group. Anesthesiology. 2017;126:1053–1063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bauer ME, Chiware R, Pancaro C. Neuraxial procedures in COVID-19 positive parturients: a review of current reports. Anesth Analg. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chen R, Zhang Y, Huang L. Safety and efficacy of different anesthetic regimens for parturients with COVID-19 undergoing cesareandelivery: a case series of 17 patients. Can J Anaesth. 2020:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Song L, Xiao W, Ling K, et al. Anesthetic management for emergent cesarean delivery in a parturient with recent diagnosis of coronavirus disease 2019 (COVID-19): a case report. Transl Perioper Pain Med. 2020;7:234–237. [Google Scholar]
- 28.Xia H, Zhao S, Wu Z. Emergency caesareandelivery in a patient with confirmed coronavirus disease 2019 under spinal anaesthesia. Br J Anaesth. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Zhong Q, Liu YY, Luo Q, et al. Spinal anaesthesia for patients with coronavirus disease 2019 and possible transmission rates in anaesthetists: retrospective, single-centre, observational cohort study. Br J Anaesth. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bauer ME, Kountanis JA, Tsen LC, Greenfield ML, Mhyre JM. Risk factors for failed conversion of labor epidural analgesia to cesarean delivery anesthesia: a systematic review and meta-analysis of observational trials. Int J Obstet Anesth. 2012;21:294–309. [DOI] [PubMed] [Google Scholar]
- 31.Fan C, Lei D, Fang C, et al. Perinatal transmission of COVID-19 associated SARS-CoV-2: should we worry? Clin Infect Dis. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Li Y, Zhao R, Zheng S, et al. Lack of vertical transmission of severe acute respiratory syndrome coronavirus 2, China. Emerg Infect Dis. 2020;26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Schwartz DA. An analysis of 38 pregnant women with COVID-19, their newborn infants, and maternal-fetal transmission of SARS-CoV-2: maternal coronavirus infections and pregnancy outcomes. Arch Pathol Lab Med. 2020. [DOI] [PubMed] [Google Scholar]
- 34.Zhu H, Wang L, Fang C. Clinical analysis of 10 neonates born to mothers with 2019-nCoV pneumonia. Transl Pediatr. 2020;9:51–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Stower H. Lack of maternal–fetal SARS-CoV-2 transmission. Nat Med. 2020;26:312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Dong L, Tian J, He S, et al. Possible vertical transmission of SARS-CoV-2 from an infected mother to her newborn. JAMA. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zeng H, Xu C, Fan J, et al. Antibodies in infants born to bothers with COVID-19 pneumonia. JAMA. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kimberlin DW, Stagno S. Can SARS-CoV-2 infection be acquired in utero?: more definitive evidence is needed. JAMA. 2020. [DOI] [PubMed] [Google Scholar]
- 39.Wang S, Guo L, Chen L, et al. A case report of neonatal 2019 coronavirus disease in China. Clin Infect Dis. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Dong X, Cao Yy, Lu Xx, et al. Eleven faces of coronavirus disease 2019. Allergy. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Rasmussen SA, Smulian JC, Lednicky JA, et al. Coronavirus disease 2019 (COVID-19) and pregnancy: what obstetricians need to know. Am J Obstet Gynecol. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Landau R, Bernstein K, Mhyre J. Lessons learned from first COVID-19 cases in the United States. Anesth Analg. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Guglielminotti J, Landau R, Li G. Major neurologic complications associated with postdural puncture headache in obstetrics: a retrospective cohort study. Anesth Analg. 2019;129:1328–1336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.NIH-NHLBI ARDS Network. NIH NHLBI ARDS Clinical Network Mechanical Ventilation Protocol Summary. 2008Available at: http://www.ardsnet.org/files/ventilator_protocol_2008-07.pdf. Accessed March 28.