

Epidemiology, Risk Factors, and Pathophysiology
Rhinitis and sinusitis are terms that refer to inflammatory conditions of the nose and paranasal sinuses characterized by symptoms of:
-
•
Rhinorrhea (anterior or posterior)
-
•
Itching
-
•
Sneezing
-
•
Nasal obstruction
Secondary symptoms include:
-
•
Headache
-
•
Cough
-
•
Facial pain
-
•
Poor olfaction
-
•
Disturbed sleep
-
•
Pharyngitis
-
•
Poor concentration
-
•
Exacerbation of lower respiratory tract problems
In practice, inflammatory changes are usually continuous from nasal to sinus mucosa (Figure 32-1 ); therefore, the terminology rhinosinusitis is more accurate, but cumbersome—the two will be used interchangeably in this chapter.
Figure 32-1.
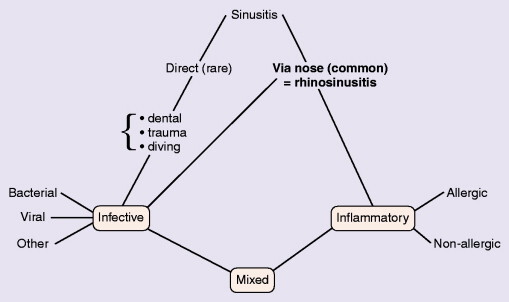
Causes of sinusitis.
The condition has marked effects on quality of life and is responsible for reduced school and workplace attendance (by 3–4%) and performance (by 30–40%). The resulting economic burden is high, and rhinosinusitis and related conditions occupy approximately one third of primary care consultations.
The causes of rhinitis can be simply considered as:
-
•
Allergy
-
•
Infections
-
•
Other causes or unknown
The recent classification of rhinitis taken from the ARIA (Allergic Rhinitis and its Impact on Asthma) guidelines is shown in Table 32-1 , with the differential diagnoses shown in Table 32-2 .
Table 32-1.
Classification of Rhinitis
| Infectious | Viral Bacterial Other infectious agents |
| Allergic | Intermittent Persistent |
| Occupational (allergic and non-allergic) | Intermittent Persistent |
| Drug-induced | Aspirin Other medications |
| Hormonal | |
| Other causes | NARES Irritants Food Emotional Atrophic Gastroesophageal reflux |
| Idiopathic |
NARES, Nonallergic rhinitis with eosinophilia syndrome.
Table 32-2.
Differential Diagnosis of Rhinitis
| Polyps | |
| Mechanical factors | Deviated septum Adenoidal hypertrophy Foreign bodies Choanal atresia |
| Tumors | Benign Malignant |
| Granulomas | Wegener's granulomatosis Sarcoid Infectious Malignant-midline destructive granulomas |
| Ciliary defects | |
| Cerebrospinal rhinorrhea |
Considerable overlap between causes occurs; for example, allergic rhinitis characterized by sneezing, itching, and watery discharge results in considerable mucosal swelling, which may result in reduced sinus drainage and allow secondary infection to occur. Both allergic and infective inflammatory rhinosinusitis may be exacerbated by the presence of anatomic and mechanical defects, such as a deviated nasal septum or enlarged turbinates.
It is also important to consider the possibility of serious underlying conditions and their early recognition, which may be necessary to prevent later damage (e.g., defects of immunity, defects of cilial motility, vasculitic and granulomatous disease).
Rhinosinusitis is frequently associated with lower respiratory disease; for example, approximately one third of patients who have bronchiectasis also have chronic sinusitis, and patients who have cystic fibrosis invariably have sinusitis and frequently have nasal polyps develop. Rhinitis is practically ubiquitous in asthmatics, with 10% of adults with late-onset asthma exhibiting aspirin hypersensitivity, often with nasal polyps (Samter's triad). Most asthma exacerbations begin with rhinitis, either infective, allergic, or both.
Rhinitis is a global problem with increasing prevalence. It is common in Westernized societies, with up to one third of the population affected (Figure 32-2 ).
Figure 32-2.

Global prevalence of hay fever in 13- to 14-year-olds.
From Strachan D, Sibbald B, Weiland S, et al: Worldwide variations in prevalence of symptoms of allergic rhinoconjunctivitis in children: the International Study of Asthma and Allergies in Childhood [ISAAC]. Pediatr Allergy Immunol 1997; 8[4]:161–176.
Genetics
Risk factors for allergic rhinitis are both genetic—with an affected parent or sibling being associated with increased risk—and environmental. Westernization seems to be associated with an increased prevalence of allergic disorders (asthma, eczema, rhinitis); the mechanisms involved are still under investigation, but several lines of evidence exist for a deviation of the immune response away from Th1 (protective immunoglobulin IgG immunity and delayed hypersensitivity) toward Th2 (atopy with IgE production) by decreased bacterial contact. As in asthma, multiple genes are involved, many of these code for epithelial molecules concerned with innate immunity. Nasal polyposis also demonstrates a strong heritable component with a relative risk of 18 times the normal rate and 6 times the normal rate with an affected father and mother, respectively. There are a number of genes associated with aspirin-exacerbated respiratory disease—e.g., leukotriene C4 synthase promoter region—which vary among different populations. HLA-DQB1 is associated with allergic fungal sinusitis. The genetics of cystic fibrosis are discussed in Chapter 46; heterozygotes for cystic fibrosis are overrepresented in the chronic rhinosinusitis population. Primary ciliary dyskinesia is also genetic, with an incidence of approximately 1 in 20,000. Various structural ciliary defects have been described, but one common defect—a lack of inducible nitric oxide synthase in nasal mucosa—has recently been found.
Allergy
Allergic Rhinosinusitis
Apart from viral colds, allergic rhinosinusitis is the most common cause of nasal symptoms; it results from IgE-mediated immediate hypersensitivity reactions that occur in the mucous membranes of the nasal airways. Allergic rhinitis occurs in atopic individuals who have the genetic predisposition to produce IgE antibody responses to allergens, which are innocuous to normal individuals. The allergens responsible are usually airborne, so-called aeroallergens, and consist of plant pollen, fungal spores, house dust mite and cockroach aeroallergens, and dander from domestic pets. Allergic rhinitis was formerly categorized as seasonal, perennial, and occupational; however, the recent World Health Organization ARIA guidelines suggest that intermittent and persistent are better divisions, because they are globally applicable and influence treatment.
In the United Kingdom and other North European countries, symptoms in the spring are frequently caused by allergy to tree pollens such as birch, plane, ash, and hazel. In late spring and early summer—the classic hay fever season—allergic rhinitis results from allergy to grasses such as rye, timothy, and cocksfoot. In late summer, weed pollens, such as nettle and mugwort, are responsible, whereas in autumn the fungi Cladosporium spp, Alternaria spp, and Aspergillus spp provoke symptoms. In the United States, ragweed pollen allergy is a common cause of rhinitic symptoms, usually from mid-August to mid-September.
Allergy to grass pollen is probably the most common in the United Kingdom, and symptoms correlate with the presence of high airborne pollen counts. Perennial rhinitis—in which symptoms occur throughout the year—in the United Kingdom is most commonly caused by allergy to the fecal pellets of the house dust mite (Dermatophagoides pteronyssinus), which flourishes in warm, humid environments and lives in bedding and soft furnishings.
Allergy to dander from domestic pets (such as cats, dogs, rabbits, and hamsters) can account for perennial rhinitis, whereas allergens encountered in the workplace are responsible for occupational rhinitis. Examples include sensitization to latex, flour, and grain (bakers); allergies to small mammals among laboratory workers; and allergy to wood dust, biologic products (such as antibiotic powder and enzyme-enhanced detergents), and rosin (colophony) from solder flux.
Allergic rhinitis is caused by a specific, immediate hypersensitivity reaction in the nasal mucosa that arises from IgE production to allergens. The allergic reaction can exhibit two phases: immediate and late (Figure 32-3 ). Mast cell degranulation with release of mediators such as histamine, leukotrienes, prostaglandins, bradykinin, and other mediators (platelet-activating factor, substance P, tachykinins) causes immediate symptoms of sneezing, itching, and running, typically seen where allergen contact is intermittent—for example, hay fever.
Figure 32-3.
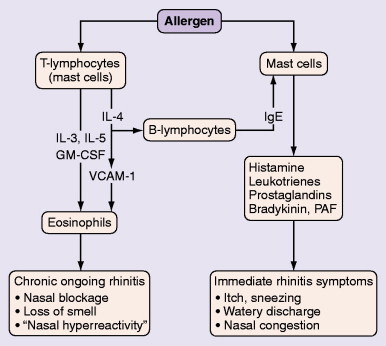
Immediate and late phases of the allergic rhinitis reaction. Mast cell degranulation leads to immediate symptoms, which are easily recognized. The late reaction, seen predominantly in persistent rhinitis, involves inflammation and produces nasal congestion and hyperreactivity, often unrecognized as allergic.
Courtesy of Professor Stephen Durham.
The late phase response involves ingress of inflammatory cells, particularly eosinophils, and is characterized by obstruction, decreased olfaction, and mucosal irritability—changes similar to those seen in chronic asthma. Similar, but more marked, inflammatory changes occur in aspirin-sensitive disease, without the involvement of interleukin-4 and systemic IgE. Constant allergen contact or very high levels produce such symptoms, the allergic nature of which may not be recognized. Symptoms produced by consequent hyperreactivity to nonspecific irritants, such as inhaled fumes, dusts, and cold air, may lead to an erroneous diagnosis of “vasomotor” rhinitis.
True food allergy is rarely the cause of isolated rhinitis but may be relevant in small children with multisystem allergies.
Table 32-3 shows the similarities and differences between the pathophysiology of asthma and rhinitis.
Table 32-3.
Pathophysiology of Rhinitis and Asthma
| Rhinitis | Asthma |
|---|---|
| Epithelium intact | Epithelium disrupted |
| Basement membrane normal | Basement membrane abnormal |
| No airway smooth muscle | Bronchial smooth muscle hypertrophy |
| Venous sinusoids | None |
| Submucosal glands | Less prominent |
| Antihistamine effective | Ineffective |
| β2-agonists ineffective | Effective |
Nonallergic Rhinosinusitis
Infectious Rhinosinusitis
The nasal and sinus mucosa can be infected by all types of organisms: viruses, bacteria, fungi, and protozoa. Of these, viral infections are the most frequent.
Acute Coryza—The Common Cold
Most people have approximately three colds per year, but small children have from six to eight. Humans spend 2 years of their lives with colds, of which 50% result from rhinoviruses, a further 20% from coronaviruses, and a further 20% from influenza, parainfluenza, adenoviruses, and respiratory syncytial virus; the remainder are caused by other viruses, including enteroviruses. Viral invasion occurs at the point of infection usually in the posterior nasopharynx and results in transient vasoconstriction of the mucous membrane followed by vasodilatation and edema with mucus production. A leukocytic inflammatory infiltrate develops, followed by desquamation of mucous epithelial cells. Initially, a clear watery secretion is produced, but it is followed by epithelial desquamation with opacification of secretions, which does not necessarily indicate bacterial infection, which complicates only approximately 2% of colds. Resolution occurs in a few days in uncomplicated viral infections; however, allergic individuals have more colds of greater severity than no atopic individuals. Rhinovirus infections in asthmatic children exposed to allergens to which they are sensitized give an odds ratio of 20 for hospitalization with asthma.
Acute Sinusitis
Although the nose harbors bacteria, the sinuses are normally largely sterile, possibly because of the nitric oxide concentrations therein and continuous mucociliary clearance. Acute sinusitis rarely occurs directly after trauma, dental infections, and diving into polluted water but usually arises from the secondary bacterial infection of a common cold. The mucous membranes of the nose and sinuses become swollen, which leads to blockage of the ostiomeatal complex and bacterial infection of the sinuses, particularly with Haemophilus influenzae and Streptococcus pneumoniae, with other causative bacteria being Staphylococcus aureus, Moraxella catarrhalis, Streptococcus pyogenes, and gram-negative bacteria such as Klebsiella spp and Pseudomonas spp. Anaerobic organisms may also be involved.
Chronic Rhinosinusitis
This, with or without nasal polyps, is defined clinically in the EPOS (European Position Paper on Chronic Rhinosinusitis and Nasal Polyposis) document as:
-
1Two or more of the major symptoms:
-
•Blockage/congestion
-
•Reduced olfaction
-
•Discharge anterior/postnasal drip
-
•Facial pain/pressure
and either
-
•
-
2Endoscopic signs of
-
•Polyps
-
•Mucopurulent discharge from middle meatus
-
•Edema/mucosal obstruction primarily in middle meatus
or
-
•
-
3CT changes
-
•Mucosal changes within ostiomeatal complex and/or sinuses
-
•
Cough is a predominant symptom in children, leading to a possible misdiagnosis of asthma.
Chronic sinusitis can occur after failure of resolution of acute sinusitis after weeks with the same bacterial pathogens involved. However, there are often other factors present such as eosinophilic inflammation (allergic or nonallergic rhinosinusitis), immune deficiency (innate or adaptive), or structural abnormalities; the role of pathogens is disputed. One possibility is persistence of organisms as a biofilm that continually stimulates a damaging immune response.
Drug-Induced Rhinitis
Antihypertensives, particularly β-blockers, can cause nasal obstruction by abrogation of the normal sympathetic tone, which maintains nasal patency. Exogenous estrogens in oral contraceptives or hormone replacement therapy also invoke rhinitis in some patients. Overuse of α-agonists results in rhinitis medicamentosa: a tachyphylaxis of α-receptors to extrinsic and intrinsic stimuli. The mucosa becomes swollen and reddened.
Aspirin hypersensitivity develops usually in adult life in patients with rhinitis (often nonallergic rhinitis with eosinophilia syndrome) with subsequent development of nasal polyps and asthma. Mast cell and eosinophil degranulation are seen in biopsies, and polyclonal local IgE production stimulated by superantigens from staphylococci has been described. Cox I inhibition by aspirin or nonsteroidal antiinflammatory drugs seems to promote leukotriene production, whereas inhibiting that of prostaglandins, including PGE-2, a bronchodilator. Leukotrienes cause bronchoconstriction, mucosal swelling, and excess mucus production, and sensitivity to their effects is high in aspirin sensitivity, probably because of increased numbers of specific receptors. The clinical picture is often one of aggressive polyposis, severe asthma with life-threatening reactions to aspirin, nonsteroidal antiinflammatory drugs, and frequent need for oral corticosteroids. A subgroup reacts also to E numbers (i.e., additives and preservatives, such as sulfites in wine), and high-salicylate foods such as herbs, spices, dried fruit, and jams.
Hormonal Rhinitis
Hormonal rhinitis is seen in pregnancy, occasionally in relation to menstruation, and at puberty. Chronic nasal obstruction can be a feature of hypothyroidism and acromegaly.
Food-Induced Rhinitis
Much rarer than popularly supposed, food allergy rarely causes isolated rhinitis, but in small children, milk or egg allergy can cause it as part of a spectrum that can include atopic dermatitis, gut symptoms, asthma, and failure to thrive.
In older people, food reactions are seen in association with rhinitis as part of the oral allergy syndrome in which sensitization to pollen results in cross-reactivity to components such as profilin in fresh fruit and vegetables. For example, an individual allergic to tree pollen may notice irritation of the lips and mouth on eating raw apples. These give rise to itching of mouth and lips, sometimes with swelling, rarely severe enough to compromise the airway, and provision of an EpiPen is usually unnecessary. Profilin is heat labile, so cooked fruits and vegetables are usually tolerated. Cross-reacting foods are shown in Table 32-4 . An individual will react to only one or two of the fruits and vegetables on the list and, therefore, does not need to avoid all of them.
Table 32-4.
Oral Allergy Syndrome—Cross-Reacting Foods
| Plant Material | Cross-Reacting Foods | |
|---|---|---|
| Silver birch pollen | Almond | Mango |
| Anise seed | Nectarine | |
| Apple (raw) | Onion (raw) | |
| Apricot | Orange | |
| Caraway | Parsley | |
| Carrot (raw) | Peach | |
| Celery (raw) | Pepper (capsicum) | |
| Cherry | Plum | |
| Coriander | Potato (raw) | |
| Hazelnut | Tomato (raw) | |
| Kiwi | Walnut | |
| Lychee | ||
| Grass pollen | Kiwi | Tomato (raw) |
| Melon | Watermelon | |
| Peanut | Wheat | |
| Daisy family pollens | Lychee | Sunflower seeds |
| Mugwort (weed) pollen | Aniseed | Fennel |
| Carrot (raw) | Parsley | |
| Celery (raw) | Spices (some) | |
| Celery salt | ||
| Latex (contact and/or inhaled allergy) | Avocado | Papaya |
| Banana | Peach | |
| Chestnut | Peppers | |
| Kiwi | Pineapple | |
| Mango | Plum | |
| Melon | Tomato (raw) | |
| Orange | ||
| Animal material | Cross-reacting foods | |
|---|---|---|
| House dust mite | Shellfish | Snails |
Allergy to food may be confused with food intolerance (in which IgE-mediated mechanisms are not involved). Some foods are rich in histamines (cheese, some fish, and some wines) that may result in flushing, headache, and rhinitis, and the same may occur with tyramine-rich foods (bananas). Food additives and coloring agents (such as sulfites, benzoates, and tartrazine) may also provoke reactions, especially in aspirin-sensitive subjects. Finally, alcohol or spicy, hot food containing capsaicin may irritate c fibers and nonspecifically provoke rhinitic symptoms.
Atrophic Rhinitis
Atrophic rhinitis is characterized by atrophy of mucosa plus the bone beneath. The nose is widely patent, but there is crusting and an unpleasant smell. Klebsiella ozaenae has been found in many patients, and cure with long courses of ciprofloxacin has been reported. However, it is uncertain whether this condition is primarily infective. It may follow extensive surgery, radiation, chronic granulomatous disease, or trauma. Possibly, the primary problem is failure of normal mucociliary clearance mechanisms.
Other Causes
Emotional stimuli such as sexual arousal and stress have powerful effects on the nasal mucosa through the autonomic system. Gastroesophageal reflux is thought to be a cause of rhinitis, especially in small children. Chronic exposure to dry air or occupational irritants—for example, those found in the shipbuilding industry—can lead to nasal mucosal changes, often with squamous cell abnormalities.
Nonallergic, Noninfectious Rhinitis
Patients with none of the aforementioned causes are usually divided according to the presence or absence of nasal eosinophilia.
Nonallergic Rhinitis with Eosinophilia Syndrome
The presence of eosinophils in nasal smears (more than 5–25% according to different authorities) characterizes a condition that is probably the counterpart of intrinsic asthma and may precede nasal polyposis and aspirin sensitivity. It is usually responsive to topical nasal corticosteroids.
Noneosinophilic Nonallergic Rhinitis
Autonomic Rhinitis
In autonomic rhinitis, there is no evidence of nasal inflammation, but of autonomic dysfunction. Nasal and, in some patients, cardiovascular reflexes are abnormal, and there may be associated chronic fatigue syndrome. Topical ipratropium is useful in decreasing watery rhinorrhea; capsaicin applications may also relieve symptoms for several months after a few weeks of treatment.
The nasal mucosa receives a rich innervation from both the sympathetic and parasympathetic nervous system. Adrenaline and other sympathomimetics lead to vasoconstriction of the nasal mucosa, with increased nasal patency. Both α- and β-adrenergic blockers increase nasal resistance and can produce symptoms of nasal stuffiness. Stimulation of the parasympathetic system leads to an increase in nasal secretions. However, patients who have this condition also have increased responsiveness to both histamine and methacholine, which results in nasal blockage and rhinorrhea. It is also associated with hypertrophy of the inferior turbinates, and nasal polyps are sometimes present. Certain stimuli such as cold air, exercise, mechanical or thermal, and humidity changes result in rhinorrhea and other symptoms of rhinitis, and a period of nasal hyperresponsiveness often follows viral infection.
Idiopathic or Intrinsic Rhinitis
Idiopathic or intrinsic rhinitis is a diagnosis of exclusion with no evidence for any of the aforementioned causes. Symptoms tend to be perennial, and local allergy has been suggested as a cause, on the basis of histologic findings of mast cells and eosinophils in resected turbinates and on positive responses to local nasal allergen challenge in a subgroup.
Direct release of mediators from mast cells or neurogenic mechanisms may be involved here.
Finally, emotional factors may play a part, ranging from stress that compounds nasal blockage and discharge to the patient emphatically or consistently complaining of gross nasal symptoms, yet with no abnormal findings on examination.
Structural Causes
Variant anatomy was thought to predispose to rhinosinusitis as a result of interference with normal drainage and aeration of the paranasal sinuses (Figure 32-4 ) at the ostiomeatal complex, the crucial point at which the maxillary, frontal, and anterior ethmoid sinuses drain into the nose. However, in three recent studies, patients with chronic rhinosinusitis showed no greater prevalence of structural abnormalities than did normal controls.
Figure 32-4.
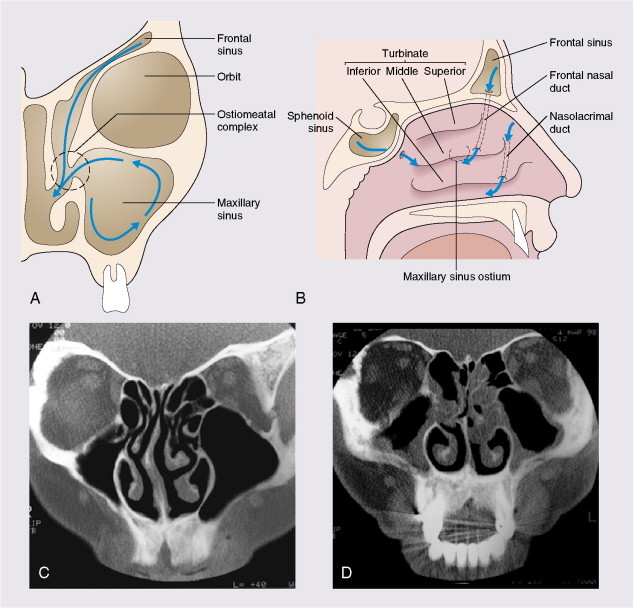
The top diagrams show sinus drainage pathways. A, In the left coronal diagram, the ostiomeatal complex is seen to drain the frontal, anterior ethmoid, and maxillary sinuses. B, The right diagram demonstrates these from the lateral view. C, The left coronal computed tomography (CT) scan shows clear paranasal sinuses in a patient with a deviated nasal septum. D, In the right scan, significant thickening of the mucosal lining is seen. CT changes do not correlate well with nasal symptoms but do relate to eosinophil counts in blood and sputum and to pulmonary function in accompanying asthma.
CT scans courtesy of Mr. Ian Mackay.
Neoplasms, foreign bodies, and trauma can all produce symptoms of obstruction, pain, purulent discharge, and epistaxis. In adults, the possibility of neoplasm is always considered in patients who have persistent symptoms, particularly if these are unilateral. In children, the presence of foreign bodies should be considered if nasal discharge is unilateral and foul smelling. Local disease in the pharynx and larynx may also have an impact on the nose and paranasal sinuses (e.g., enlarged adenoids), as may dental disease (e.g., maxillary dental root infection), which may spread to the maxillary sinus.
Immune Defects
Panhypogammaglobulinemia is a severe condition with variable absence of all classes of immunoglobulin; it presents with bacterial and other infections at many sites. Initial presentation may be to the otorhinolaryngologist with symptoms of recurrent acute or chronic rhinosinusitis. It is important to make the diagnosis early before irreversible damage occurs at other sites (the lungs) and so that appropriate immunoglobulin therapy can be instituted. Total or relative absence of IgA may be present in the absence of any obvious clinical disease. However, IgA deficiency is now known to be associated in some patients with IgG2 subclass deficiency, and such individuals may be more prone to episodes of sinusitis caused by capsulated bacteria such as H. influenzae and S. pneumoniae. Acute, chronic, and recurrent sinusitis are common in individuals who have human immunodeficiency virus infection, the most common organisms being S. pneumoniae and H. influenzae. A tendency to chronicity and to relapse is found, and in addition, fungal (Cryptococcus spp, Alternaria spp, and Aspergillus spp) and viral (cytomegalovirus) sinusitis may occur.
Mucus Clearance Defects
The nose and paranasal sinuses are lined with ciliated epithelium, which in a coordinated fashion moves a mucus blanket toward the nasopharynx. This mucus is important for the entrapment and removal of particulate material and toxic substances, which include bacteria and allergens. The integrity of the mucociliary clearance pathway is vital to the appropriate drainage and ventilation of the paranasal sinuses and the nose (see Figure 32-4). Primary ciliary dyskinesia is inherited as an autosomal-recessive trait and is characterized by the presence of sinusitis, bronchiectasis, situs inversus (Kartagener's syndrome, present in 50% of these patients), and male infertility that results from dyskinetic sperm. Various ciliary structural defects have been described (e.g., absence of inner or outer dynein arms or both), but some cilia appear normal (Young's syndrome). Recent work suggests that deficiency of iNOS (inducible nitric oxide synthase) may be the common underlying abnormality. Presentation is with chronic sinusitis, bronchiectasis or bronchitis, and obstructive azoospermia.
Secondary ciliary defects may arise after viral or bacterial infections; a number of mechanisms are involved:
-
•
Mucous membranes become swollen and inflamed, which may result in blockage of the sinus ostia and thus prevent clearance (this is particularly critical at the ostiomeatal complex).
-
•
If viruses or bacteria damage the epithelial cell layer, the integrity of cilial clearance is destroyed.
-
•
Some bacteria produce toxins that inhibit cilial clearance mechanisms.
-
•
Mucus during infection becomes thick and difficult to clear.
Granulomas/Vasculitis
A number of granulomatous diseases may involve the nose and sinuses as part of the generalized disease, or nasal symptoms may be the first manifestation. These include Wegener's granulomatosis, Churg–Strauss syndrome, and sarcoidosis, particularly in Afro-Caribbean individuals. Mucous membrane infiltration and thickening with granulomas may be present and may involve the septum, inferior turbinates, and occasionally the sinuses. Nasal congestion is a prominent symptom, sometimes with epistaxis and marked crusting. Sufferers feel unwell, with fatigue and malaise. Infective granulomatous disease may involve the nose and sinuses; examples are tuberculosis, leprosy, syphilis, blastomycosis, histoplasmosis, and aspergillosis.
Nasal Polyps
Nasal polyps (Figure 32-5 ) result from prolapse of the mucous membrane that lines the nose and present as pale, grapelike protuberances arising predominantly from the middle meatus. They are insensitive to pain but produce symptoms of nasal blockage and loss of sense of smell and may be associated with aspirin hypersensitivity and asthma. Nasal polyps may also be related to infection and are common in patients who have cystic fibrosis. Nasal polyps are rare in children, but when they do occur, they are often associated with cystic fibrosis. Classification of nasal polyps is similar to that of rhinitis (Table 32-5 ).
Figure 32-5.

Speculum examination of nostril shows a pale watery polyp (arrow). Polyps are insensate and grayish, unlike turbinates, which are sensitive and bluish pink.
Courtesy of St. Mary's Hospital Audio-Visual Department.
Table 32-5.
Classification of Nasal Polyps
| Allergic | Eosinophil rich Skin prick tests may be negative Allergic fungal Sinusitis Aspirin sensitive Churg-Strauss |
| Infective | Neutrophil-rich Cystic fibrosis Immune deficiency |
| Structural | Antrochoanal |
| Other | Malignancy |
Occupational Rhinitis
Occupational rhinitis can be allergic or nonallergic, with the former nearly always preceding or developing concurrently with occupational asthma.
Clinical Features
Allergy
Allergic Rhinitis
This presents in two forms.
Runners/Sneezers/Itchers
Symptoms tend to be intermittent and changeable and are often closely related to allergen exposure during the day. Severity varies from trivial to extremely disabling. In addition, itching and injection of the conjunctivae may occur, with watery discharge and conjunctival swelling, and itching in the mouth, oropharynx, and ears. This form of allergic rhinitis tends to be a disorder of children and young adults, and up to one third have associated asthma.
Blockers
The nose is chronically obstructed, with little in the way of immediate allergic symptoms.
Facial ache, headache, nasal hyperreactivity, and loss of sense of smell may also be present. Examination of the nose reveals pale or bluish mucosa, which is boggy and swollen, and a watery discharge may be present. Examination of the nose is important to exclude the concomitant presence of polyps, septal deviation, prominent turbinates, and evidence of other systemic disease and tumors.
Nonallergic Rhinosinusitis
Infections
Acute Coryza (The Common Cold)
The prodrome normally consists of a feeling of dryness, itching, and heat in the nose, which may last for a few hours and is often followed by a dry, sore throat; sneezing; watery discharge; and constitutional symptoms of feverishness and malaise. This phase is followed in a day or so with symptoms of nasal obstruction and mucopurulent discharge, feverishness, and malaise, which may continue until resolution after 5–10 days. Initially, the symptoms of allergic rhinitis and coryza may be difficult to distinguish.
Acute Sinusitis
Acute maxillary sinusitis is characterized by facial pain, localized to the cheek, but also in the frontal area or the teeth, that is made worse by stooping down or straining. The pain can be unilateral or bilateral, and tenderness may overlie the sinus. Acute frontoethmoidal sinusitis may cause pain around the eye and in the frontal region, with overlying tenderness and erythema of the skin. There is usually fever, and toxemia may occur. Differential diagnosis of facial pain is wide and includes dental disease and the numerous causes of headache. Recently, all the accepted clinical signs and symptoms noted here have been shown to be unreliable as diagnostic aids to acute sinusitis, with the combination of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) giving the best guide.
Chronic sinusitis is frequently pain free and presents with a sensation of congestion, poor concentration, tiredness, and malaise. Other symptoms of chronic sinusitis include purulent nasal discharge (often postnasal), sore throat, and a productive cough, especially in children in whom misdiagnosis of asthma is not uncommon. Loss of smell and halitosis are additional features.
Noninfective Rhinosinusitis
Symptoms are similar to those of blockers, as mentioned previously. The differential diagnosis from allergic rhinitis depends on skin prick or other allergy testing.
Clinical Presentations that Need Physician Referral
Unilateral symptoms, bloody discharge, polyps presenting for the first time, and systemically ill patients should be seen by an otorhinolaryngologic surgeon. Orbital cellulitis and sinusitis with severe headache or vomiting demand urgent referral.
Diagnosis, Evaluation, and Tests
Examination
It is frequently possible to arrive at a diagnosis of rhinosinusitis on the basis of a good detailed history. Physical examination should never be omitted, and it is vitally important that chronic symptoms are appropriately investigated.
Observation of the patient's face may reveal an allergic crease or salute, a deviated nose, or more sinister collapse of the nasal bridge.
Anterior rhinoscopy with a bright light or head mirror by use of a Thudicum speculum allows simple examination of the anterior nasal cavity; also, the mucous membrane can be viewed, and the presence of nasal polyps and disorders of the anterior part of the nasal septum can be seen.
Nasal endoscopy by use of either a rigid or fiberoptic flexible endoscope allows more detailed examination and assessment. Congenital defects, such as cleft palate and atresia, septal deviation and perforation, abnormalities of the turbinates, state of the mucous membranes, presence of purulent secretions, polyps, neoplasms, and foreign bodies can be determined.
Diagnosis of Coryza
Coryza is normally diagnosed on the basis of a patient's history, and further investigations are rarely required. Viral culture or immunofluorescent techniques can identify specific viruses.
Diagnosis of Acute Sinusitis
On examination, red, swollen nasal mucous membranes are present, and pus may be seen in the middle meatus. Endoscopy, together with imaging techniques, allows assessment of the severity and extent of involvement (diagnostic antral puncture and lavage are now rarely required). Middle meatal swabs provide material for bacteriologic culture. Immunoglobulin classes and subclasses are checked in cases of recurrent or chronic sinusitis.
Imaging Techniques
Radiography is rarely needed for diagnosis, unless a tumor is suspected. There is a high incidence of abnormalities in the general population: one third of unselected adults and 45% of children have abnormal scans. After a cold, computed tomography (CT) scans show changes for at least 6 weeks. The role of imaging is largely to provide a road map for the surgeon after failure of medical treatment.
Since the advent of computed tomography, plain sinus radiographs now have only a very limited role in acute rather than chronic sinusitis, because opacification or a fluid level may be seen in a sinus or gross soft tissue swelling may be evident. The imaging investigation of choice is CT, which is the best technique to demonstrate mucosal disease and underlying anatomic abnormalities (see Figure 32-4). The detailed anatomy of both bone and soft tissue is provided, and axial and coronal sections can be obtained. The coronal cuts provide views of the ostiomeatal complex, important for planning surgery for acute and chronic sinusitis (Figure 32-6 ). Preoperatively, coronal sections at 3–4 mm give maximal anatomic detail, whereas axial views provide vital information regarding the relation of the optic nerve to the posterior ethmoidal and sphenoid sinuses. Magnetic resonance imaging is of very limited value, because bone is not well imaged. It is useful in distinguishing one soft tissue from another and has the advantage of avoiding irradiation.
Figure 32-6.

Coronal computed tomography scan of paranasal sinuses showing almost complete opacification of maxillary and ethmoid sinuses with polyps that obstruct the ostiomeatal complex.
Courtesy of Mr. Ian Mackay.
Mucociliary Function Tests
Saccharin Clearance
One quarter of a grain of saccharin is placed on the lateral nasal wall, 1 cm behind the anterior end of the inferior turbinate. A sweet taste is detected within 20 min if cilial function is normal—that is, the mucociliary mechanism is able to transport the particle to the nasopharynx and the pharynx, where taste is detected. If abnormal, more sophisticated tests of cilial activity by use of cells detached by brushings taken from the turbinate undertaken by use of phase contrast microscopy. Significant abnormalities on this test lead to electron microscopic examination of cilia.
Confirmation of observations of very low nasal nitric oxide (NO) in primary ciliary dyskinesia means that a nasal NO of greater than 250 ppb excludes this diagnosis with 95% sensitivity.
Nasal Airway Tests
Dynamic tests include nasal inspiratory peak flow (by use of a mask attached to a peak flow meter, the patient sniffs hard with a closed mouth) and rhinomanometry. The technique is used to assess nasal airway resistance by measuring airflow across a pressure gradient with a pneumotachograph and facemask. Acoustic rhinometry uses a sound pulse to measure the nasal cross-sectional area.
Nasal resistance can change very dramatically within a few minutes. Congestion is produced by engorgement of venous erectile tissue within the nose; the mucous membrane receives dense, autonomic innervation. Nasal resistance falls with adrenaline and other sympathomimetic drugs, but also with exercise, rebreathing, and adoption of the erect posture. Nasal resistance increases in rhinitis and, in some individuals, with alcohol, aspirin, and other drugs, as well as when the supine posture is adopted.
Evaluation of Allergic Rhinitis
The diagnosis is usually obvious from a careful history and examination but can easily be missed in chronic blockers; thus, skin prick tests should be performed in all rhinitis clinic patients. Skin tests that use allergen extracts to elicit IgE-mediated immediate hypersensitivity responses can be used to confirm or exclude atopy. If all the skin tests are negative, it is unlikely that the rhinitis is allergic. However, positive tests do not confirm the diagnosis, because many asymptomatic individuals have positive skin tests to common allergens. Correlation between skin prick tests and history should be sought, because occasionally it is possible to identify an allergen that can be avoided. Measurement of total IgE is not helpful; however, measurement of specific IgE levels to common aeroallergens by means of radioallergosorbent testing may be useful, and the results show a good correlation with skin test results. Occasionally, particularly where occupational rhinitis may be a possibility, nasal challenge and provocation tests (with the offending allergen, histamine, aspirin, or methacholine) may be required.
Nasal Cytology
It may be of value to determine the presence or absence of eosinophils in patients who have perennial rhinitis, negative skin tests, and who are not atopic. A subset of these patients have nasal secretion eosinophilia and are more likely to have allergic features such as sneezing and congestion; they may also respond to topical corticosteroids.
Treatment
Allergic Rhinitis
The basis of treatment for allergic rhinitis is:
-
1
Allergen avoidance
-
2
Pharmacotherapy
-
3
Immunotherapy
-
4
Rarely surgery
-
5
Patient education (vital)
Identify and Avoid Allergens
In practice, the identification and avoidance of allergens may be extremely difficult. House dust mites are responsible for much perennial allergic rhinitis. Mites flourish at temperatures of approximately 15°C and 60–70% relative humidity, conditions present in many homes that contain central heating. They flourish particularly in soft furnishings, mattresses, pillows, and bed covers, as well as in carpets. Allergen avoidance and measures to reduce the load (i.e., wooden floors rather than carpets, regular vacuum cleaning, and barrier covers for mattresses and pillows) effectively reduce rhinitic symptoms. Acaricides that kill the mites do not eliminate the antigen, which is present in the fecal pellets. Removal of a pet may not remove symptoms, because allergens may persist in rooms for many months, if not years. Avoidance of pollen is difficult, but vacationing or, failing that, staying indoors when the pollen count is high, closing windows, shutting car windows, and avoiding open grassy spaces may help.
Medical Suppressive Therapy
The treatment plan for allergic rhinitis according to ARIA is shown in Figure 32-7, Figure 32-8 .
Figure 32-7.
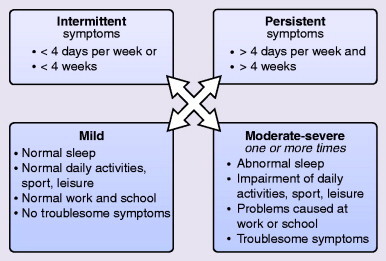
Division of rhinitis according to frequency and severity.
From Bousquet J, Van Cauwenberge P, Khaltaev N: J Allergy Clin Immunol 2001; 108[Suppl]:5147–5276.
Figure 32-8.
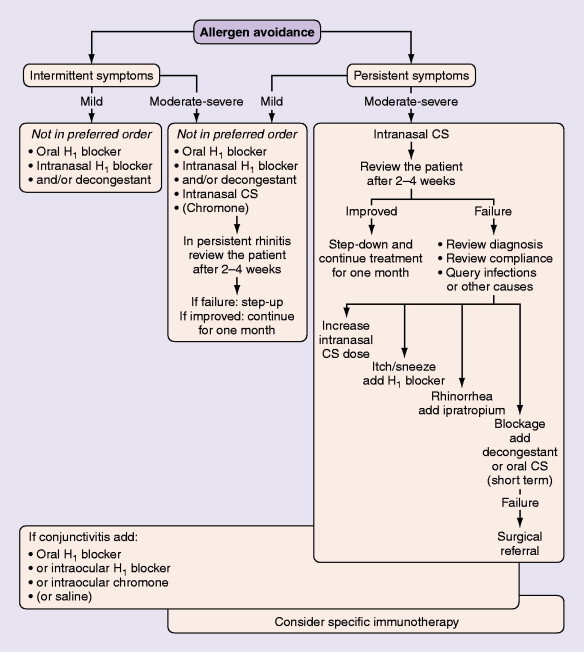
Rhinitis treatment on the basis of the subdivision in Figure 32-6.
From Bousquet J, Van Cauwenberge P, Khaltaev N: J Allergy Clin Immunol 2001; 108[Suppl]:5147–5276.
Topical Corticosteroids
Meta-analysis has shown that these are the most effective treatment for allergic rhinitis. Regular use is needed and preseasonal dosing reduces development of seasonal rhinitis symptoms. For polyps or marked nasal blockage, betamethasone drops or oral corticosteroids for the first 2 weeks of therapy may be needed, followed by a nonabsorbed drop formulation, Flixonase nasules, in the long term for polyps (Figure 32-9 ). Side effects of topical corticosteroids include local irritation and minor epistaxis. Steroid absorption is low except for betamethasone and dexamethasone, which should be used only short term.
Figure 32-9.
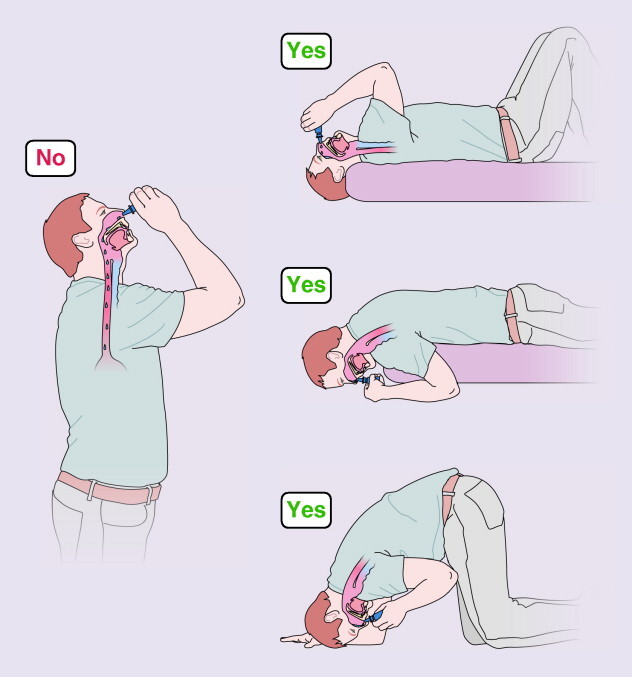
Correct instillation of nasal drops.
Adapted from BSACI Rhinitis Management Guidelines.
Sodium cromoglycate is less effective nasally, but may be suitable for small children, whereas severe conjunctival symptoms are best treated with sodium cromoglicate or nedocromil sodium. Corticosteroid eye drops are avoided.
Antihistamines
Antihistamines provide excellent relief of sneezing, itching, and rhinorrhea, but not congestion; oral ones have the advantage of being effective for mouth and eye symptoms. Chlorpheniramine is best avoided, because it is sedating and reduces driving ability and academic performance. Newer H1-antagonists are largely nonsedating. Certain molecules (terfenadine, astemizole, and diphenhydramine in particular) can produce QT prolongation and fatal cardiac arrhythmias, especially if blood levels are high because of overdosing or combining with other hepatically metabolized drugs. Fexofenadine cetirizine, levocetirizine, and desloratadine seem safe in this respect and possess some measurable nasal unblocking activity. Azelastine and levocabastine are useful topical antihistamines.
Other Agents
Vasoconstrictors are useful in the short term for marked congestion, but long-term use must be avoided because of the risk of rhinitis medicamentosa. Anticholinergics such as ipratropium bromide may be useful if extensive, watery secretion is a major problem.
Antileukotrienes are of similar efficacy to antihistamines in allergic rhinitis, with no major benefits from a combination of the two. However, in some patients with polyps, they can reduce symptoms and polyp size when used with a topical steroid.
Douching the nose with isotonic saline can reduce symptoms of allergic rhinitis and improve endoscopic appearances and quality of life in chronic rhinosinusitis.
Immunotherapy
This is the only treatment that has been shown to influence the course of disease. Three years treatment reduces symptoms for several years thereafter. In children with rhinitis, subcutaneous immunotherapy reduces progression to asthma at 3, 5, and 10 years afterwards. There is also a reduction in new allergic sensitization.
Desensitization involves the administration of increasing doses of relevant allergen extract by subcutaneous injection over a period of months and has been shown to effectively diminish symptoms of allergic seasonal rhinitis to grass pollen, ragweed, and birch pollen. Some studies also suggest efficacy to house dust mite and some animal danders. Desensitization has largely been superseded by the success of effective medical therapy in the suppression of allergic inflammation and so is reserved for nonresponders with severe disease. It is not always effective, and concerns have been raised regarding occasional anaphylactic reactions and deaths after the procedure, so it must be undertaken by well-trained individuals in a hospital setting with cardiorespiratory resuscitation facilities at hand.
Safer sublingual approaches have now been demonstrated to be effective, and grass pollen tablets will become available in the United Kingdom in 2007. The first sublingual dose needs to be under medical supervision; after this, each dose is taken every day at home. Eight weeks preseasonal therapy followed by continuation throughout the pollen season is suggested. Trials are in progress to assess the long-term effects of 3 years regular treatment.
Surgical Intervention
When medical treatment is only partially successful, a full otorhinolaryngologic assessment is performed because correction of a deviated nasal septum or reduction of hypertrophied mucosa may improve the symptoms. With coexistent chronic sinus infection, functional endoscopic sinus surgical techniques (FESS) may be necessary to facilitate sinus drainage, aeration, and access for medications, although a recent study showed that medical therapy with corticosteroid and long-term macrolide use was equally effective. Both improved concomitant asthma.
Infections
Coryza—The Common Cold
Treatment is essentially symptomatic with analgesics, antipyretics, rest, and broad-spectrum antibiotics if secondary infection is present. Oral or topical nasal zinc may decrease symptoms and their duration.
Acute Sinusitis
Most cases resolve spontaneously. Analgesics and antipyretics provide symptomatic relief, but aspirin must be avoided in those who may be hypersensitive. Acetaminophen (paracetamol) and codeine are satisfactory alternatives. Decongestants such as oxymetazoline and xylometazoline reduce edema and may improve sinus drainage. Broad-spectrum antibiotics are appropriate but must have activity against the most common pathogens, namely S. pneumoniae, H. influenzae, and M. catarrhalis. Amoxicillin, trimethoprim-sulfamethoxazole (co-trimoxazole), or a macrolide such as clarithromycin are appropriate. Amoxicillin-clavulanate has the added advantage of activity against S. aureus and penicillin-resistant H. influenzae. If anaerobic infection is suspected, a combination of amoxicillin-clavulanate and metronidazole or clindamycin is appropriate.
Chronic Rhinosinusitis
The aims of treatment are to remedy any underlying cause (e.g., immunologic defect, anatomic abnormality that prevents drainage) and to restore the integrity of the mucous membranes to allow normal ventilation of the sinuses and drainage (see Figure 32-3). Nasal douching with saline improves symptoms and endoscopic appearances. Topical corticosteroids may help to reduce mucous membrane swelling and improve drainage. Initially, betamethasone drops taken in the head-down position are briefly used, but no absorbed Fluticasone nasules are safer in long-term use. Prolonged courses of macrolide antibiotics produced improvements equivalent to FESS surgery, possibly because of their antiinflammatory activity. Amphotericin douching is ineffective.
Surgical Interventions for Acute and Chronic Sinusitis
Major changes have occurred in recent years as a result of the advent of high-resolution CT scans and FESS. Better demonstration of the nasal and sinus anatomy is achieved with CT scans, as well as of the important ostiomeatal complex, the vital region where sinus drainage by mucociliary clearance occurs. Obstruction in this zone is very important in the generation of chronic sinus disease. The main aim of FESS is to restore adequate drainage for the frontal, maxillary, and ethmoidal sinuses (see Figure 32-4). When this fails, more radical sinus surgery may be needed, but complete investigation for underlying medical factors (e.g., immune deficiency) should be undertaken first.
Noninfectious Causes
Intrinsic Rhinitis (Figure 32-10)
Figure 32-10.
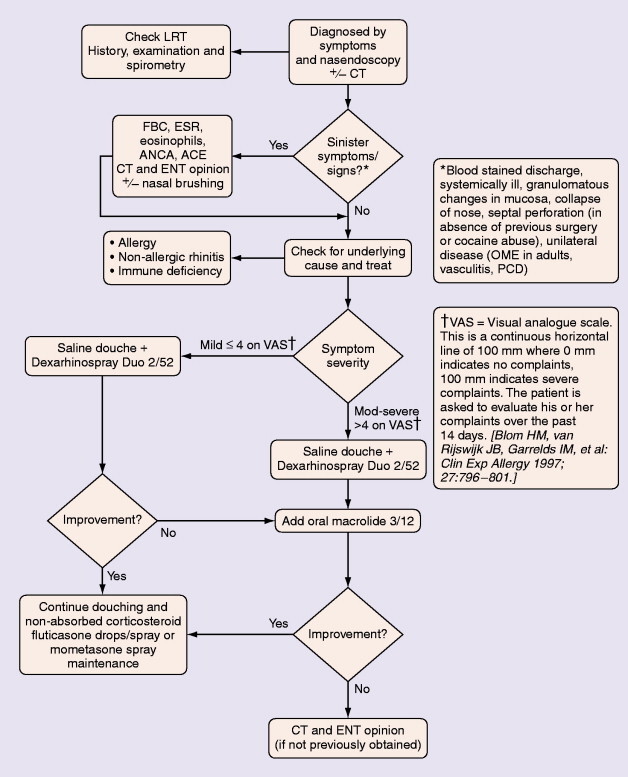
Management of chronic nonpolyp rhinosinusitis.
Adapted from BSACI Rhinitis Management Guidelines.
Anticholinergics (ipratropium bromide) are useful for troublesome rhinorrhea, particularly when eosinophils are absent from nasal secretions. When eosinophilia is present, a response to topical corticosteroid therapy is usual. α-Agonist decongestants, such as pseudoephedrine and xylometazoline, are used sparingly. Surgical procedures may help if nasal obstruction is predominant.
Structural Defects
Occasionally, topical corticosteroid therapy may ameliorate structural defects, but normally surgical correction is required.
Immune Defects
Therapy of immune defects is directed toward correction of the immunologic defect.
Mucus Clearance Defect
It is not possible to correct the underlying mucus clearance defect, so therapy relies on regular douching, improved drainage and aeration, and prevention of secondary infection.
Granulomas
Appropriate, specific antimicrobial therapy is required for infectious causes of granulomatous disease. Sarcoidosis that involves the nose responds to either local or systemic glucocorticoid therapy.
Drug-Induced Disease
A careful drug history must be taken and the incriminated drug excluded.
Nasal Polyps (Figure 32-11)
Figure 32-11.
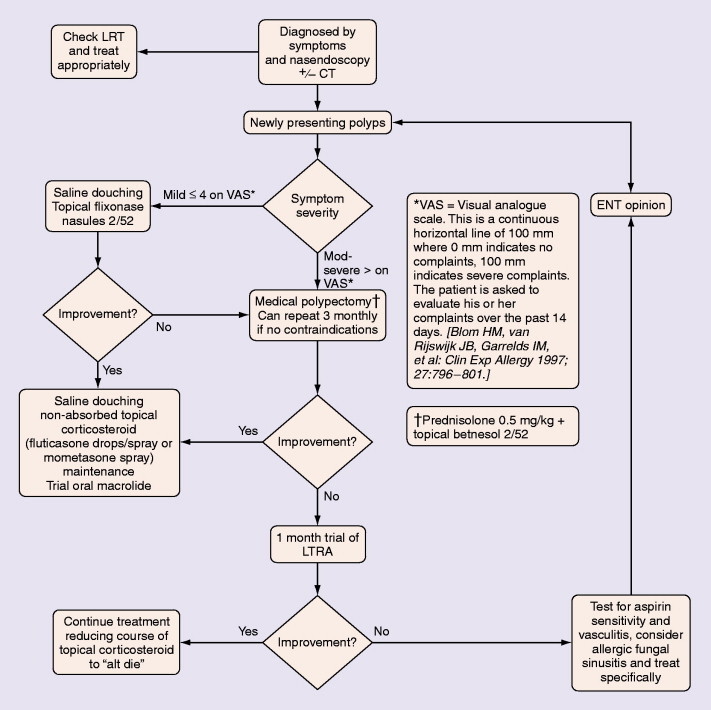
Treatment of polypoid rhinosinusitis. Symptoms and signs on visual analogue scale. See Figure 32-10.
Adapted from BSACI Rhinitis Management Guidelines.
Unilateral nasal polyps must be referred to exclude transitional cell papilloma, squamous cell carcinoma, encephalocoele, or other sinister pathology. When there are no contraindications and no suspicions about the nature of the polyp, a medical polypectomy by use of prednisolone (0.5 mg/kg, enteric-coated) plus betamethasone drops (two in each nostril three times a day with the head upside down) for 5 days can prove as effective as surgery and is superior with respect to improvements in concomitant asthma. This should be followed by long-term corticosteroid drops—initially betamethasone for 2 weeks, then nonabsorbed fluticasone. Subsequently, a trial of a leukotriene receptor antagonist should be undertaken for 2–4 weeks, with continuation if beneficial. Other measures being evaluated include regular saline douching and topical lysine aspirin in patients sensitive to this on nasal challenge. Failure of medical treatment is an indication for surgery.
Patients with aspirin-exacerbated respiratory disease should be warned to avoid all Cox-1 inhibitors and to watch for exacerbation by similar substances: E numbers, preservatives, high-salicylate foods. Most can tolerate 500 mg paracetamol or Cox-2 inhibitors.
Clinical Course and Prevention
Allergic Rhinosinusitis
The clinical course is variable. With good compliance, allergen avoidance, and regular pharmacotherapy, symptoms are usually minimal. Understandably, patients want a cure. Immunotherapy remains of limited value, but with development in understanding of the mechanism of generation of IgE responses and of ways in which this can be modulated, it may become more useful.
Infections
Coryza—The Common Cold
Unfortunately, avoidance of the common cold is virtually impossible, and prevention by immunization has so far been a failure. However, colds are self-limiting and normally last approximately 5 days. Clinical trial data support the value of zinc in reducing the duration and severity of symptoms of the common cold when administered within 24 h of the onset of common cold symptoms.
Most asthma exacerbations (80% in children and 60% in adults) start with a viral upper respiratory tract infection. Synergy between allergen sensitization, exposure, and rhinoviral infection leads to an almost 20-fold likelihood of an asthmatic child needing hospital admission. Other complications include acute sinusitis, pharyngitis, otitis media, mastoiditis, and tonsillitis. The common cold frequently leads to lower respiratory infection, including laryngotracheitis, bronchitis, and occasionally pneumonia. Those who have other cardiorespiratory diseases may also experience exacerbations.
Acute Bacterial Sinusitis
Before the antibiotic era, acute sinusitis had a significant morbidity and mortality because of spread of bacterial sepsis beyond the sinuses. Osteolysis of the sinus wall occurred often, with abscess formation and direct spread to neighboring structures, in addition to local spread and thrombophlebitis. These local complications include orbital cellulitis with or without abscess formation, cavernous sinus thrombosis, sagittal sinus thrombosis, intracranial abscess, meningitis and encephalitis, osteomyelitis, and septicemia.
Complications are now rarely seen, because most patients are prescribed broad-spectrum antibiotics.
Intrinsic Rhinitis
Intrinsic rhinitis often has an onset in middle age or later and is often refractory to treatment. Combinations of therapy may prove helpful.
Pitfalls and Controversies
Points to consider in patients with rhinitis and sinusitis:
-
•
Not all patients who have nasal symptoms have allergic rhinitis—neoplasm or foreign body could be present.
-
•
Unilateral discharge in children is probably a foreign body, but in adults it may be carcinoma.
-
•
Unilateral lesions must be biopsied to exclude malignancy.
-
•
Nasal decongestants must be used sparingly, if at all.
-
•
Most medical treatment failures result from poor compliance—once daily treatment is best, if possible.
-
•
Common cold, a cause of widespread morbidity, remains a major research challenge.
-
•
Intrinsic rhinitis can be troublesome to treat, and further research is required.
-
•
Turbinates and polyps are difficult to distinguish—turbinates are rigid and pain-sensitive, polyps are mobile and insensitive to pain.
-
•
Facial pain in the absence of nasal symptoms is rarely caused by sinus disease, so other causes such as migraine, dental problems, and temporomandibular joint syndrome are considered.
-
•
Chronic refractory sinusitis stimulates investigation for underlying immune or other defects.
-
•
CT scan is the investigation of choice—plain radiographs or magnetic resonance imaging has a limited role.
-
•
Treatment of rhinosinusitis benefits asthma.
SUGGESTED READINGS
- Bousquet J, Van Cauwenberge P, Khaltaev N. The Aria Workshop Panel—Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol. 2001;108(Suppl):5147–5276. doi: 10.1067/mai.2001.118891. [DOI] [PubMed] [Google Scholar]
- British Society of Clinical Immunology and Allergy Rhinitis Management Guidelines. Clin Exp Allergy. 2007 (in press) [Google Scholar]
- Fokkens WF, Lund VJ, Bechert C. EAACI Position Paper on rhinosinusitis and nasal polyps. Allergy. 2005;60:583–601. doi: 10.1111/j.1398-9995.2005.00830.x. [DOI] [PubMed] [Google Scholar]
- Pharmacologic and anti-IgE treatment of allergic rhinitis ARIA update (in collaboration with GA2LEN) Allergy. 2006;61(9):1086–1096. doi: 10.1111/j.1398-9995.2006.01144.x. [DOI] [PubMed] [Google Scholar]
- Ragab S, Scadding GK, Lund VJ, Saleh H. Treatment of chronic rhinosinusitis and its effects on asthma. Eur Respir J. 2006;28(1):68–74. doi: 10.1183/09031936.06.00043305. Epub 2006 Mar 1. [DOI] [PubMed] [Google Scholar]