

Supplemental Digital Content is available in the text
Keywords: Coronary bifurcation lesions, Drug-eluting balloon, Target lesion stenosis, Late lumen loss
Abstract
Background
Treatment of coronary bifurcation lesions remains challenging; a simple strategy has been preferred as of late, but the disadvantage is ostium stenosis or even occlusion of the side branch (SB). Only a few single-center studies investigating the combination of a drug-eluting stent in the main branch followed by a drug-eluting balloon in the SB have been reported. This prospective, multicenter, randomized study aimed to investigate the safety and efficacy of a paclitaxel-eluting balloon (PEB) compared with regular balloon angioplasty (BA) in the treatment of non-left main coronary artery bifurcation lesions.
Methods
Between December 2014 and November 2015, a total of 222 consecutive patients with bifurcation lesions were enrolled in this study at ten Chinese centers. Patients were randomly allocated at a 1:1 ratio to a PEB group (n = 113) and a BA group (n = 109). The primary efficacy endpoint was angiographic target lesion stenosis at 9 months. Secondary efficacy and safety endpoints included target lesion revascularization, target vessel revascularization, target lesion failure, major adverse cardiac and cerebral events (MACCEs), all-cause death, cardiac death, non-fatal myocardial infarction, and thrombosis in target lesions. The main analyses performed in this clinical trial included case shedding analysis, base-value equilibrium analysis, effectiveness analysis, and safety analysis. SAS version 9.4 was used for the statistical analyses.
Results
At the 9-month angiographic follow-up, the difference in the primary efficacy endpoint of target lesion stenosis between the PEB (28.7% ± 18.7%) and BA groups (40.0% ± 19.0%) was –11.3% (95% confidence interval: –16.3% to –6.3%, Psuperiority <0.0001) in the intention-to-treat analysis, and similar results were recorded in the per-protocol analysis, demonstrating the superiority of PEB to BA. Late lumen loss was significantly lower in the PEB group than in the BA group (–0.06 ± 0.32 vs. 0.18 ± 0.34 mm, P < 0.0001). For intention-to-treat, there were no significant differences between PEB and BA in the 9-month percentages of MACCEs (0.9% vs. 3.7%, P = 0.16) or non-fatal myocardial infarctions (0 vs. 0.9%, P = 0.49). There were no clinical events of target lesion revascularization, target vessel revascularization, target lesion failure, all-cause death, cardiac death or target lesion thrombosis in either group.
Conclusions
In de novo non-left main coronary artery bifurcations treated with provisional T stenting, SB dilation with the PEB group demonstrated better angiographic results than treatment with regular BA at the 9-month follow-up in terms of reduced target lesion stenosis.
Trial registration
ClinicalTrials.gov, NCT02325817; https://clinicaltrials.gov
Introduction
Coronary bifurcations lesions account for 15% to 20% of all percutaneous coronary interventions (PCI) and remain one of the most challenging lesions in interventional cardiology in terms of procedural success rate as well as long-term cardiac events,[1] and a simple strategy is the preferred treatment compared with more complex strategies. In the past decade, randomized trials[2–7] and meta-analyses[8–11] have indicated “simple is better” for treating coronary bifurcation lesions, mostly due to a high incidence of myocardial infarction (MI) and in-stent thrombosis following complex strategies. Indeed, a simple strategy not only reduces procedure-related complications but also decreases device-related clinical events during long-term follow-up. The disadvantage of a simple strategy is ostium stenosis or even occlusion of the side branch (SB) due to plaque dislocation after stent implantation in the main branch. The advent of drug-eluting balloons (DEBs) provides a novel therapeutic strategy for bifurcation lesions.
A DEB is a balloon catheter-based device for local drug delivery to a lesion. Paclitaxel is applied on the surface of the balloon, which is then squeezed into the narrow vessel wall during dilation, and the lipid-soluble paclitaxel is rapidly absorbed by the endothelial tissue through cell absorption and osmosis.[12] Paclitaxel can significantly block early proliferative initiation factors, which play a key role in the subsequent formation of intima, and blocking early intimal hyperplasia can effectively prevent the occurrence of restenosis.[13] This effect contradicts the traditional theory stating that maintaining the sustained effect of localized drugs is the basis for anti-neointimal hyperplasia.[14,15]
DEB was first proposed by Dr. Harvey Wolinsky in 1991 as a way to prevent restenosis after percutaneous transluminal coronary angioplasty (PTCA).[16] In 2006, the study called the Treatment of In-Stent Restenosis by Paclitaxel-Coated Balloon Catheters (PACCOCATH ISR) showed that the paclitaxel-eluting balloon (PEB) treatment of 52 patients with restenosis had no need for concurrent drug stent implantation, relying on the PEB to prevent restenosis.[17] Since then, DEB research has gradually received the attention of medical scientists. Notably, in 2014, the U.S. Food and Drug Administration approved a drug balloon for the treatment of peripheral arterial disease.[18]
Several published studies[19–23] have reported the design of DEB in the main branch (MB) and/or SB in combination with a bare metal stent (BMS) in the MB. To the best of our knowledge, only a few single-center studies[24,25] investigating the combination of a drug-eluting stent (DES) in the MB followed by a DEB in the SB have been published to date.
Our study, BEYOND, was a multicenter, randomized controlled trial to investigate a PEB for the treatment of de novo non-left main (LM) coronary artery bifurcation lesions. It was also a pre-market clinical trial for the first PEB (Bingo®, Yinyi Biotech, Dalian, China) made in China, which subsequently received approval from the China Food and Drug Administration in December 2017.
Methods
Ethical approval
This study was performed according to the Declaration of Helsinki, and the study protocol was approved by the ethics committee at each participating site. All patients provided written informed consent.
Study design
The BEYOND trial was a prospective, multicenter, randomized study to investigate the superiority of PEBs for the treatment of de novo non-LM coronary artery bifurcation lesions compared with regular balloon angioplasty (BA). The MB was implanted with a DES followed by a PEB or BA in the SB. This trial was sponsored by Yinyi (Liaoning) Biotech Co., Ltd. (Dalian, China) and was registered at the ClinicalTrials.gov website (Identifier NCT02325817).
Patients
In this study, we enrolled patients at ten centers in China [Supplementary File 1] between December 2014 and November 2015. Eligible patients were males and non-pregnant females from 18 to 80 years of age with angina pectoris (stable or unstable), an old MI or evidence of asymptomatic myocardial ischemia; de novo coronary bifurcation stenotic lesion in the MB scheduled for implantation with a DES, while the SB was only scheduled for receiving balloon dilation, diameter stenosis of the SB ≥70% by visual estimate and residual stenosis ≤50% after pre-dilation by regular balloon dilation. The target lesion had to have a reference vessel diameter ≥1.25 and ≤5.00 mm and a lesion length ≤40 mm. Major exclusion criteria were unprotected left main disease and its bifurcation; in-stent restenosis; heavy calcification or not suitable for balloon dilation; life expectancy <1 year; severe heart failure (New York Heart Association [NYHA] grade ≥III) or left ventricular ejection fraction <35%; inability to tolerate dual-antiplatelet therapy for 12 months; or inability to provide written informed consent. After successful target lesion pre-dilation, block randomization (block size of 4) by center was used by means of sealed, opaque envelopes to assign patients in a 1:1 ratio to receive BA for the target lesion with a PEB (Bingo®, Yinyi Biotech) or an uncoated regular balloon. Patients received outpatient or telephone follow-up at 30, 180, and 270 days after surgery and angiographic follow-up at 270 days after surgery to evaluate the safety and efficacy of the test products. Among them, one person was lost to follow-up, and 47 people refused angiography follow-up at 270 days after surgery.
Procedures
The surface of the Bingo® PEB was homogenously coated with 3 μg/mm2 paclitaxel incorporated in a proprietary delivery matrix of iohexol. Paclitaxel is a lipophilic anti-proliferative substance that allows rapid drug absorption by the surrounding tissue.
Cardiac catheterization was performed according to standard practice. Patients received a loading dose of 300 mg aspirin and 300 mg colpidogrel (or 180 mg ticagrelor) before the procedure and then continued with 100 mg aspirin once per day, 75 mg clopidogrel once per day or 90 mg ticagrelor twice per day before the procedure. Glycoprotein IIb/IIIa antagonists were administered at the operator's discretion. The baseline angiography of the target vessel was performed in at least two near-orthogonal views showing the target lesion free of foreshortening and vessel overlap. The choice of PEB was left at the operator's discretion in all cases. PEBs were available in lengths of 8 to 40 mm with diameters of 1.25 to 5.0 mm, and regular balloons (Yinyi®, Yinyi Biotech) were available in lengths of 10 to 30 mm with diameters of 1.5 to 4.0 mm. Dual-antiplatelet therapy with aspirin and clopidogrel/ticagrelor was indicated for at least 12 months after the procedure.
After wiring both branches, pre-dilation of the MB and SB was performed at the operator's discretion. A DES was deployed in the MB, and post-dilation was performed at the operator's discretion to achieve optimal stent deployment. After MB stenting, guidewires were switched, and kissing balloon inflation had to be performed with the regular balloons. If the residual diameter stenosis of the SB ≤50%, the PEB or regular balloon was inflated for 30 to 60 s in the SB. Bail-out stenting of the SB was deemed appropriate in the following cases: dissection impeding the flow in the SB or acute coronary closure.
Quantitative coronary angiography
Angiographic analysis was performed by an independent core laboratory (R&G PharmaStudies Co, Ltd. CoreLab, Beijing, China). For the quantitative coronary angiographic analysis, QAngio XA Version 7.3 Analysis Software (Medis Medical Imaging System Inc, Leiden, the Netherlands) was used.
Endpoint definitions and follow-up
The primary efficacy endpoint was target lesion stenosis (TLS) at 9 months (as evaluated by quantitative coronary analysis [QCA]).
TLS was defined as (1 – minimal lumen diameter [MLD]/reference vessel diameter) × 100. Bifurcation lesions were defined according to the Medina classification. We defined the target lesion as the ostium of the SB in the bifurcation. The target vessel was defined as the SB in the bifurcation.
Secondary efficacy and safety endpoints were late lumen loss (LLL) at 9 months; target lesion revascularization (TLR); target vessel revascularization (TVR); target lesion failure (TLF) (a composite of cardiac death, target vessel MI and TLR); major adverse cardiac and cerebral events (MACCEs) (a composite of all-cause death, MI, stroke, and TVR); the individual components of the composite endpoints and non-fatal MI at 1, 6, and 9 months; an thrombosis in the target vessel (acute, <1 day; sub-acute, 1–30 days; and late, >30 days).
LLL was defined as the difference between the MLD measured post-procedure and the MLD measured at angiographic follow-up. Death was defined as the occurrence of death from any cause during the study period. Cardiac death was defined as any death due to an evident cardiac cause, any death related to PCI, unwitnessed death, or death of unknown causes. MI was defined as an elevation of troponin (cTn) ≥5 times above the upper limit of normal with any associated elevation in the myocardial band or the development of new pathologic Q waves in two contiguous electrocardiographic leads. TLR was defined as a new intervention (surgical or percutaneous) to treat significant luminal stenosis (>50% diameter stenosis by visual estimation) in the treated segment (including the stented segment and the adjacent 5 mm proximal and distal in the MB and the balloon-treated zone plus 5 mm distal in the SB). Thrombosis in the target vessel was considered according to the criteria for definite stent thrombosis described by the Academic Research Consortium.[26] Procedure success was defined as the PEB or regular balloon successfully passing through and inflating in the SB without bailout stenting.
Statistical analysis
Based on previously reported studies,[27,28] we assumed a TLS of 38% in the BA group and 29% in the PEB group at 9 months. Using a superiority design, with at least 80% power and a one-sided alpha level of 0.025, assuming a maximal dropout rate of 20%, 216 patients (108 per group) needed to be enrolled.
The primary efficacy endpoint was pre-specified to be tested in the intention-to-treat (ITT) population as the primary analysis and the per-protocol population as a secondary analysis. The missing data of the primary endpoint in the ITT population were imputed by using the last observation carried forward method. Covariance analysis was performed to estimate the least-square mean (LS mean) of the primary efficacy endpoint, and the LS mean difference between the two groups with a 95% confidence interval (CI) was calculated. The model included the factors of treatment, baseline, and center. Kaplan-Meier analysis was used to estimate the event rates for time-to-event outcomes, including TLR, TVR, TLF, and MACCE, and the data were compared with the log-rank test.
Categorical data were expressed as count and percentage and compared by Chi-square or Fisher exact test, as appropriate. Continuous data were expressed as mean ± standard deviation or median and interquartile range, and compared by Student's t test or the Wilcoxon rank-sum test. All statistical tests were two-sided, and a P value <0.05 was considered statistically significant unless otherwise specified. SAS version 9.4 (SAS Institute Inc., NC, USA) was used for statistical analyses.
Results
Patient and procedural characteristics
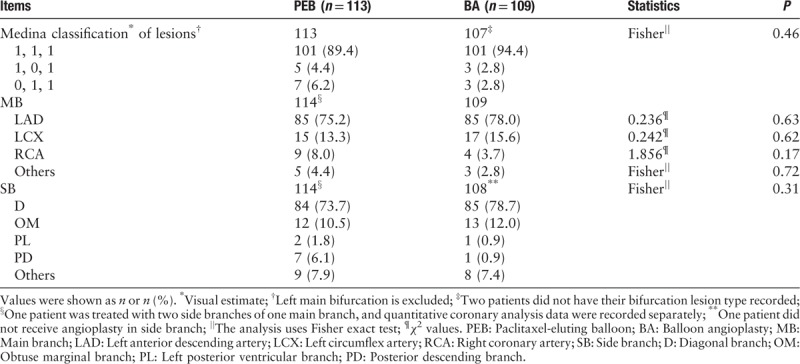
A total of 222 consecutive patients were randomly assigned to receive either a PEB (n = 113) or BA (n = 109) between December 2014 and November 2015 at ten Chinese centers [Figure 1]. The two groups of patients were generally well balanced in terms of baseline clinical characteristics [Table 1], except for a higher percentage of males in the PEB group. The most commonly treated bifurcation in both groups was left anterior descending with the diagonal branch. All patients were accompanied with true bifurcation lesions according to the Medina classification based on visual estimates by the investigators, and the most common lesion type was 1,1,1 [Table 2].
Figure 1.
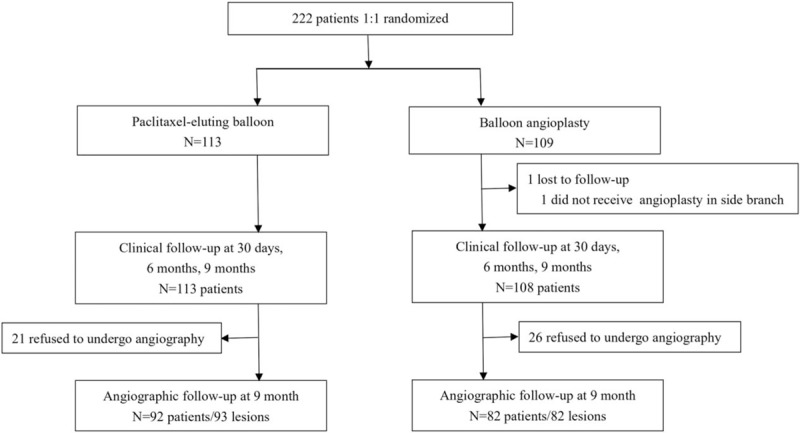
Study flow chart. Follow-up window: 30 days: ±7 days, 6 months: ±30 days; 9 months: ±30 days.
Table 1.
Baseline characteristics of patients with bifurcation lesions enrolled in this study.
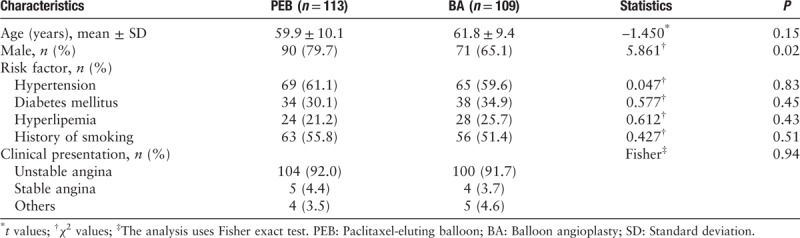
Table 2.
Lesion types of patients with bifurcation lesions enrolled in this study.
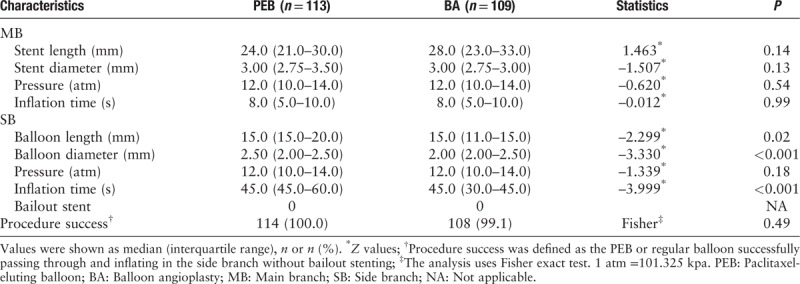
The MB was pre-dilated in 207 (93.2%) patients (106 in the PEB group and 101 in the BA group), and the SB was pre-dilated in 184 (82.9%) patients (102 in the PEB group and 82 in the BA group). After pre-dilation, the PEB could be successfully deployed. There was no dissection in the SB in either group. In the PEB group, one patient was treated in two SBs of one MB, and QCA data were recorded separately. In the BA group, one patient did not receive BA in the SB because the balloon failed to cross the lesion, QCA data were not available, and the patient did not complete clinical follow-up. In total, the procedure was successful in 99.5% of cases. Table 3 shows the procedural characteristics. There were no significant differences between the two groups in the MB. In the SB, the balloon length, balloon diameter, and inflation time were larger in the PEB group. This might be explained by the fact that most investigators had a good understanding of the recommendation by the German consensus group: a DEB should extend 4 to 5 mm into the MB and 2 to 3 mm distal beyond the PTCA area into the SB, with a balloon to vessel ratio of 0.8 to 1.0, and be inflated for at least 30 s at nominal pressure.[29,30]
Table 3.
Procedure characteristics of patients with bifurcation lesions enrolled in this study.
Angiographic results
Angiographic analysis was possible for all patients before and immediately after the procedure, whereas angiographic follow-up at 9 months was performed on 174 patients (78.4%), 92 patients with 93 lesions in the PEB group and 82 patients with 82 lesions in the BA group.
The results of angiographic analysis are shown in Table 4. PEB was superior to BA in terms of the primary efficacy endpoint (TLS) at 9-month angiographic follow-up in the ITT analysis (difference –11.3%, 95% CI: –16.3% to –6.3%, Psuperiority <0.0001) and its covariance analysis (LS mean difference –11.1%, 95% CI: –15.8% to –6.4%, Psuperiority <0.0001) [Figure 2]. We recorded similar results when data were analysed according to the per-protocol analysis (difference –12.3%, 95% CI: –16.6% to –8.0%, Psuperiority <0.0001) and its covariance analysis (LS mean difference –12.0%, 95% CI: –16.0% to –8.0%, Psuperiority <0.0001) [Figure 2]. LLL at 9 months was significantly lower in the PEB group than in the BA group (–0.06 ± 0.32 vs. 0.18 ± 0.34 mm, P < 0.0001) [Table 4]. Representations of the MLD in the SB, including cumulative frequency curves for all the patients at pre-procedure, post-procedure and at 9-month follow-up, are presented in Figure 3. Figure 4 shows the angiographic baseline and follow-up of a patient treated with the PEB.
Table 4.
Pre-procedure, post-procedure, and 9-month angiographic follow-up quantitative coronary analysis.
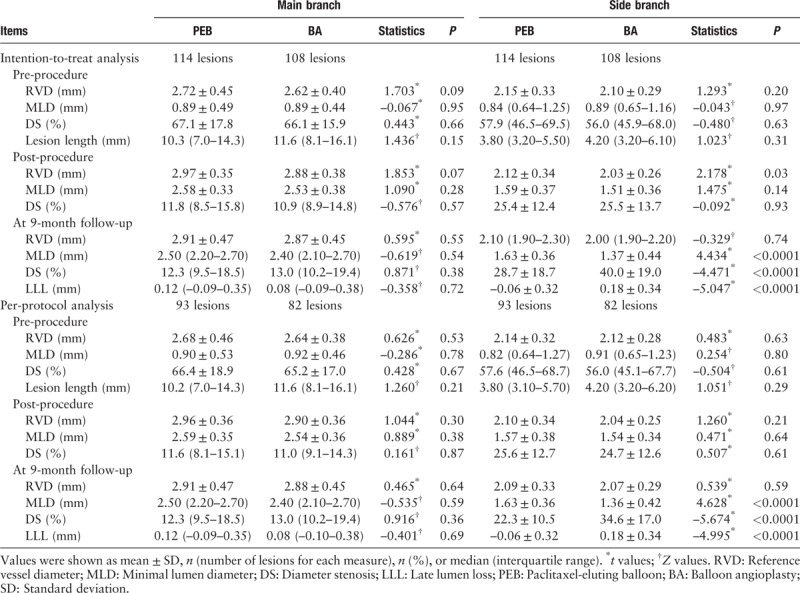
Figure 2.
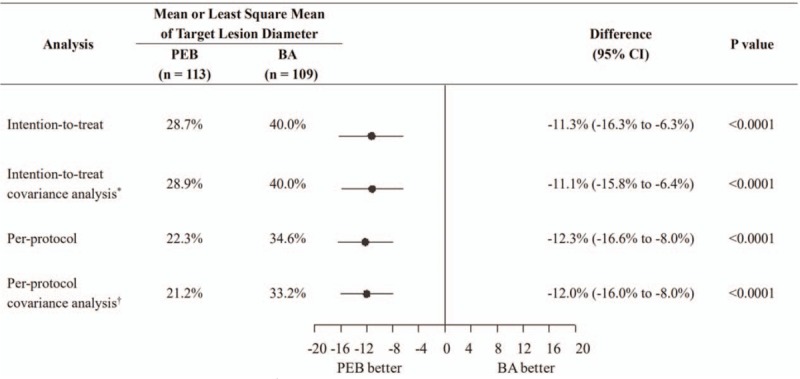
Primary endpoint of target lesion stenosis at 9 months. ∗Covariance analysis model included the factors of group, center, and pre-procedure diameter of the stenosis of target lesion. Four centers that had a small number of patients were consolidated as one center for analysis. BA: Balloon angioplasty; CI: Confidence interval; PEB: Paclitaxel-eluting balloon.
Figure 3.
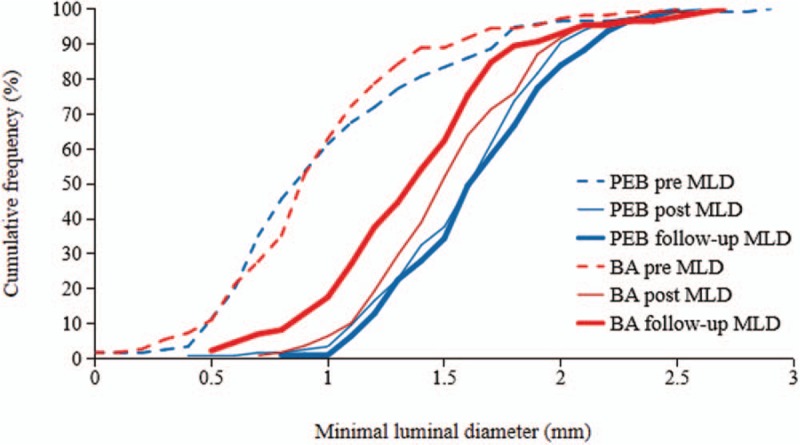
Cumulative frequency distribution of MLD determined by quantitative coronary angiography. PEB vs. BA: Pre-procedure (pre), post-procedure (post), and at 9 months (follow-up). BA: Balloon angioplasty; MLD: Minimal lumen diameters; PEB: Paclitaxel-eluting balloon.
Figure 4.
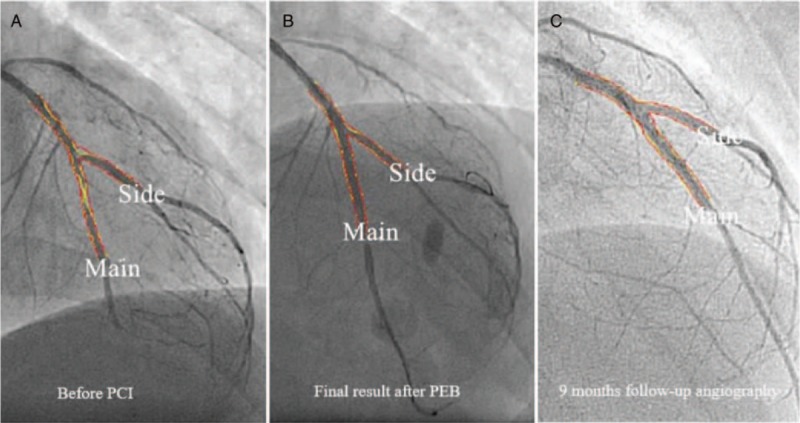
A patient treated with the PEB for a bifurcation lesion. (A) High-grade stenosis in the proximal first diagonal branch. (B) Final result after angioplasty and PEB. (C) Angiographic control after 9 months without any signs of restenosis. PCI: Percutaneous coronary interventions; PEB: Paclitaxel-eluting balloon.
Clinical outcome
A total of 221 (99.5%) patients completed clinical follow-up. One patient in the BA group was lost to follow-up. At the 9-month follow-up, there were no clinical events of TLR, TVR, TLF, all-cause death, cardiac death, and target lesion thrombosis in either group [Table 5]. A total of five MACCEs were noted during follow-up (PEB vs. BA, 0.9% vs. 3.7%, P = 0.16) [Table 5, Figure 5], mainly caused by stroke. The percentage of non-fatal MI was similar between the two groups (0 vs. 0.9%, P = 0.49) [Table 5].
Table 5.
Clinical outcomes at 30 days, 6 months, and 9 months in the intention-to-treat analysis, n (%).
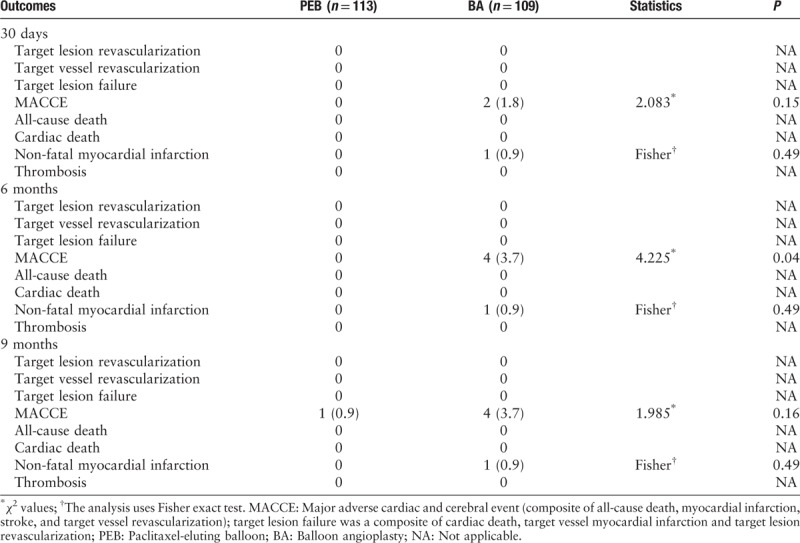
Figure 5.
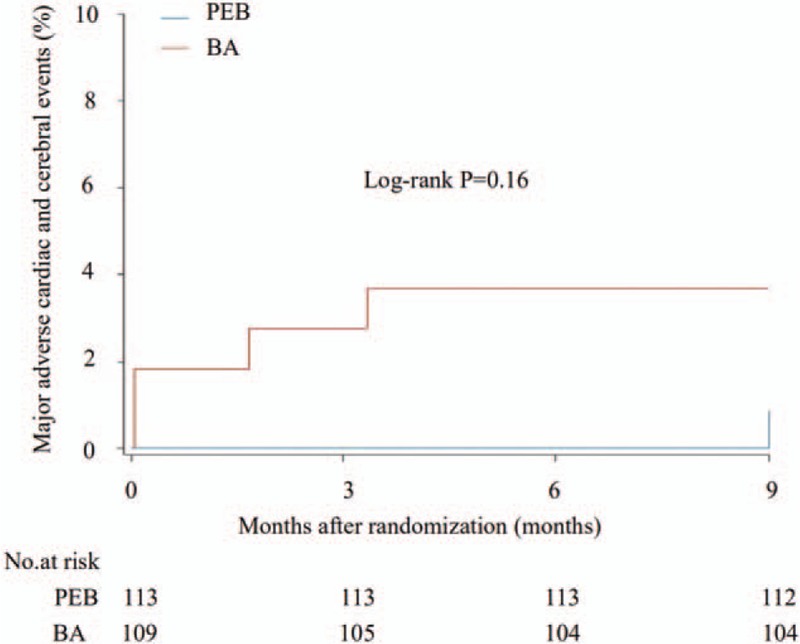
Time-to-event curves for the composite endpoints of major adverse cardiac and cerebral events through 9 months in the intention-to-treat population. The event rates presented here were calculated by the Kaplan-Meier methodology and compared with the log-rank test. BA: Balloon angioplasty; PEB: Paclitaxel-eluting balloon.
Discussion
Bifurcation lesion treatment is a challenge in the field of coronary artery intervention treatment at present, and many studies have confirmed that the application of double stents, such as double-kissing crush, culotte, and T-and-protrusion, can achieve very good results. However, not all types of bifurcation lesions are suitable for the use of double stents in small coronary vessels. Indeed, the greatest challenge is the protection of SBs. Treatment of bifurcation lesions by means of double stents, regardless of the type of operation, may have different complications because of the variable pathological and anatomical features. Therefore, the management of SBs in bifurcation lesions has become the most concerning issue for interventional cardiologists.
The BEYOND study is a prospective, multicenter, randomized controlled trial to evaluate the superiority of the PEB for the treatment of de novo non-LM coronary artery bifurcation lesions in comparison with regular BA. The main results showed better angiographic characteristics in the SB after treatment with a PEB than with a regular balloon at 9 months post-procedure.
The PEPCAD V study showed that a PEB was excitingly effective in treating bifurcation lesions.[21] The SB and MB were successively dilated with a PEB (twenty-eight patients). Then, a BMS was implanted within the “footprint” of the PEB in the MB. The ostium of the SB was post-dilated with an uncoated balloon. There were no MACCEs for up to 30 days, and no TLR was performed. Two stent thromboses were reported. At the 9-month angiographic follow-up, the success rate of the MB was 97% and that of the SB was 89%. The angiographic results showed an in-stent LLL of 0.38 ± 0.46 mm in the MB and an in-lesion unsatisfactory LLL of 0.21 ± 0.48 mm in the SB.
The DEBSIDE study[25] enrolled fifty-two patients with coronary artery bifurcation lesions. A DES was deployed in the MB after the pre-dilation step in both the MB and SB, and final kissing inflation with regular balloons was performed. The DEB was placed into the SB. The procedural success rate was 100%. Angiographic control at 6 months post-procedure was performed in 48 patients (96%), and two patients with no reported clinical events refused angiographic control. At the six-month follow-up, the primary end point of SB LLL was −0.04 ± 0.34 mm, and the secondary endpoint of MB LLL was 0.54 ± 0.60 mm.
In our study, the operation method was similar to that of the DEBSIDE compared to the PEBCAD V. In our study, the MB and SB were pre-dilated at the operator's discretion, and then a DES was deployed in the MB. Final kissing inflation with regular balloons was performed, after which the PEB was placed into the SB. The PEB diameter was sized at a 0.8-1 ratio to the artery diameter to minimize the negative impact of the expansion of the PEB on the DES in the MB. In contrast, the method applied in the PEPCAD V study easily led to stenosis in the ostium of the SB.
There were 222 patients enrolled in our study (113 in PEB vs. 109 in BA), which was nearly four times the number of patients with a DEB in the PEBCAD V and twice that in the DEBSIDE. The angiographic and clinical outcomes were compared in the PEB group and BA group. Although only 174 patients (78.4%) completed angiographic follow-up at 9 months, the primary endpoint of our study was achieved. A total of five MACCEs were noted during the 9-month follow-up (1 vs. 4, P = 0.16). There was no reported cardiac death, all-cause death or TLR in the SB. There was no significant difference in clinical outcomes between the PEB and BA groups, perhaps because of the short follow-up duration. Therefore, we still followed up the patients to evaluate the long-term outcomes.
The BEYOND study shows that the 9-month effect of the PEB for small coronary vessels was positive. This study enrolled patients with bifurcated lesions evaluated as 1,1,1-, 1,0,1- or 0,1,1- types by the Medina classification, of whom 33% patients had SB diameters less than 2.0 mm and 31% patients had diabetes. Therefore, the PEB may be expected to have better long-term efficacy in patients with small vessel disease, especially those with diabetes mellitus with bifurcated small vessel disease.
In our study, the PEB showed no significant difference from regular balloons in the success rate of passing through and dilatating the lesions. Furthermore, there was no significant difference in the safety indexes between the PEB group and the BA group. It was concluded that the clinical usability and safety of the PEB was not inferior to that of the regular balloon.
Although this study enrolled more patients than previous studies in DEB treatment of bifurcation lesions, the limitations should be noted. While the study underwent a stringent screening of the patients’ conditions, we still need longer follow-up to understand the long-term impact of the PEB compared to that of BA. At present, the PEB group has shown no significant change in TLR, TVR, TLF, MACCEs, death, thrombosis, or non-fatal MI compared to the BA group at 9 months, demonstrating the non-inferiority of the PEB to BA. We expect to examine whether the PEB would perform better in these clinical outcomes in 2 to 5 years.
In summary, the PEB was significantly superior to the BA for the treatment of de novo non-LM coronary artery bifurcation lesions. In de novo non-LM coronary bifurcations treated with provisional T stenting, SB dilation with the Bingo® PEB demonstrated better angiographic results than treatment with regular BA at the 9-month follow-up in terms of reduced TLS.
Acknowledgements
The authors thank the study participants and their families and caregivers. The authors would like to thank all colleagues for their valuable advice in operation procedures.
Conflicts of interest
None.
Supplementary Material
Footnotes
How to cite this article: Jing QM, Zhao X, Han YL, Gao LL, Zheng Y, Li ZQ, Yang P, Cong HL, Gao CY, Jiang TM, Li H, Li JX, Wang DM, Wang G, Cong ZC, Zhang Z. A drug-eluting Balloon for the trEatment of coronarY bifurcatiON lesions in the side branch: a prospective multicenter ranDomized (BEYOND) clinical trial in China. Chin Med J 2020;133:899–908. doi: 10.1097/CM9.0000000000000743
References
- 1.Lassen JF, Holm NR, Stankovic G, Lefèvre T, Chieffo A, Hildick-Smith D, et al. Percutaneous coronary intervention for coronary bifurcation disease: consensus from the first 10 years of the European Bifurcation Club meetings. EuroIntervention 2014; 10:545–560. doi: 10.4244/EIJV10I5A97. [DOI] [PubMed] [Google Scholar]
- 2.Banning AP, Lassen JF, Burzotta F, Lefèvre T, Darremont O, Hildick-Smith D, et al. Percutaneous coronary intervention for obstructive bifurcation lesions: the 14th consensus document from the European Bifurcation Club. EuroIntervention 2019; 15:90–98. doi: 10.4244/EIJ-D-19-00144. [DOI] [PubMed] [Google Scholar]
- 3.Chen SL, Santoso T, Zhang JJ, Ye F, Xu YW, Fu Q, et al. Clinical outcome of double kissing crush versus provisional stenting of coronary artery bifurcation lesions: The 5-year follow-up results from a randomized and multicenter DKCRUSH-II study (randomized study on double kissing crush technique versus provisional stenting technique for coronary artery bifurcation lesions). Circ Cardiovasc Interv 2017; 10:e004497.doi: 10.1161/CIRCINTERVENTIONS.116.004497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Colombo A, Bramucci E, Saccà S, Violini R, Lettieri C, Zanini R, et al. Randomized study of the crush technique versus provisional side-branch stenting in true coronary bifurcations: the CACTUS (coronary bifurcations: application of the crushing technique using sirolimus-eluting stents) study. Circulation 2009; 119:71–78. doi: 10.1161/CIRCULATIONAHA.108.808402. [DOI] [PubMed] [Google Scholar]
- 5.Colombo A, Moses JW, Morice MC, Ludwig J, Holmes DR, Jr, et al. Randomized study to evaluate sirolimus-eluting stents implanted at coronary bifurcation lesions. Circulation 2004; 109:1244–1249. doi: 10.1161/01.CIR.0000118474.71662.E3. [DOI] [PubMed] [Google Scholar]
- 6.Ferenc M, Ayoub M, Büttner HJ, Gick M, Comberg T, Rothe J, et al. Long-term outcomes of routine versus provisional T-stenting for de novo coronary bifurcation lesions: five-year results of the Bifurcations Bad Krozingen I study. EuroIntervention 2015; 11:856–859. doi: 10.4244/EIJV11I8A175. [DOI] [PubMed] [Google Scholar]
- 7.Bai J, Yue Y, Feng HQ, Hao SX, Peng L, Zhang M, et al. Impact of main vessel calcification on procedural and clinical outcomes of bifurcation lesion undergoing provisional single-stenting intervention: a multicenter, prospective, observational study. J Geriatr Cardiol 2019; 16:156–163. doi: 10.11909/j.issn.1671-5411.2019.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Katritsis DG, Siontis GC, Ioannidis JP. Double versus single stenting for coronary bifurcation lesions: a meta-analysis. Circ Cardiovasc Interv 2009; 2:409–415. doi: 10.1161/CIRCINTERVENTIONS.109.868091. [DOI] [PubMed] [Google Scholar]
- 9.Zhang F, Dong L, Ge J. Simple versus complex stenting strategy for coronary artery bifurcation lesions in the drug-eluting stent era: a meta-analysis of randomised trials. Heart 2009; 95:1676–1681. doi: 10.1136/hrt.2009.168641. [DOI] [PubMed] [Google Scholar]
- 10.Lv YH, Guo C, Li M, Zhang MB, Wang ZL. Modified double-stent strategy may be an optimal choice for coronary bifurcation lesions: a systematic review and meta-analysis. Medicine (Baltimore) 2018; 97:e13377.doi: 10.1097/MD.0000000000013377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hakeem A, Khan FM, Bhatti S, Samad Z, Effat MA, Eckman MH, et al. Provisional vs. complex stenting strategy for coronary bifurcation lesions: meta-analysis of randomized trials. J Invasive Cardiol 2009; 21:589–595. doi: 10.1590/S0373-55241966000100005. [PubMed] [Google Scholar]
- 12.Speck U, Stolzenburg N, Peters D, Scheller B. How does a drug-coated balloon work? Overview about coating technologies and their impact. J Cardiovasc Surg (Torino) 2016; 57:3–11. doi: 10.2514/1.A32956. [PubMed] [Google Scholar]
- 13.Scheller B, Speck U, Abramjuk C, Bernhardt U, Böhm M, Nickenig G. Paclitaxel balloon coating, a novel method for prevention and therapy of restenosis. Circulation 2004; 110:810–814. doi: 10.1161/01.CIR.0000138929.71660.E0. [DOI] [PubMed] [Google Scholar]
- 14.Gershlick AH. Treating atherosclerosis: local drug delivery from laboratory studies to clinical trials. Atherosclerosis 2002; 160:259–271. doi: 10.1016/s0021-9150(01)00618-9. [DOI] [PubMed] [Google Scholar]
- 15.Moses JW, Kipshidze N, Leon MB. Perspectives of drug-eluting stents: the next revolution. Am J Cardiovasc Drugs 2002; 2:163–172. doi: 10.2165/00129784-200202030-00004. [DOI] [PubMed] [Google Scholar]
- 16.Wolinsky H, Lin CS. Use of the perforated balloon catheter to infuse marker substances into diseased coronary artery walls after experimental postmortem angioplasty. J Am Coll Cardiol 1991; 17:174B–178B. doi: 10.1016/0735-1097(91)90955-9. [DOI] [PubMed] [Google Scholar]
- 17.Scheller B, Hehrlein C, Bocksch W, Rutsch W, Haghi D, Dietz U, et al. Treatment of coronary in-stent restenosis with a paclitaxel-coated balloon catheter. N Engl J Med 2006; 355:2113–2124. doi: 10.1056/NEJMoa061254. [DOI] [PubMed] [Google Scholar]
- 18.Sarode K, Spelber DA, Bhatt DL, Mohammad A, Prasad A, Brilakis ES, et al. Drug delivering technology for endovascular management of infrainguinal peripheral artery disease. JACC Cardiovasc Interv 2014; 7:827–839. doi: 10.1016/j.jcin.2014.05.008. [DOI] [PubMed] [Google Scholar]
- 19.Cortese B, di Palma G, Latini RA, Elwany M, Orrego PS, Seregni RG. Immediate and short-term performance of a novel sirolimus-coated balloon during complex percutaneous coronary interventions. The FAtebenefratelli SIrolimus COated-balloon (FASICO) registry. Cardiovasc Revasc Med 2017; 18:487–491. doi: 10.1016/j.carrev.2017.03.025. [DOI] [PubMed] [Google Scholar]
- 20.Chen YC, Lin FY, Cheng SM, Chang CC, Chuang CL, Lin RH, et al. Wide-angle coronary bifurcation stenotic lesions treated with one drug-eluting stent and sequential balloon technique: a better strategy? Heart Lung Circ 2020; 29:437–444. doi: 10.1016/j.hlc.2019.02.189. [DOI] [PubMed] [Google Scholar]
- 21.Mathey DG, Wendig I, Boxberger M, Bonaventura K, Kleber FX. Treatment of bifurcation lesions with a drug-eluting balloon: the PEPCAD V (paclitaxel eluting PTCA balloon in coronary artery disease) trial. EuroIntervention 2011; 7: Suppl K: K61–K65. doi: 10.4244/EIJV7SKA11. [DOI] [PubMed] [Google Scholar]
- 22.Stella PR, Belkacemi A, Dubois C, Nathoe H, Dens J, Naber C, et al. A multicenter randomized comparison of drug-eluting balloon plus bare-metal stent versus bare-metal stent versus drug-eluting stent in bifurcation lesions treated with a single-stenting technique: six-month angiographic and 12-month clinical results of the drug-eluting balloon in bifurcations trial. Catheter Cardiovasc Interv 2012; 80:1138–1146. doi: 10.1002/ccd.23499. [DOI] [PubMed] [Google Scholar]
- 23.López Mínguez JR, Nogales Asensio JM, Doncel Vecino LJ, Sandoval J, Romany S, Martínez Romero P, et al. A prospective randomised study of the paclitaxel-coated balloon catheter in bifurcated coronary lesions (BABILON trial): 24-month clinical and angiographic results. EuroIntervention 2014; 10:50–57. doi: 10.4244/EIJV10I1A10. [DOI] [PubMed] [Google Scholar]
- 24.Herrador JA, Fernandez JC, Guzman M, Aragon V. Drug-eluting vs. conventional balloon for side branch dilation in coronary bifurcations treated by provisional T stenting. J Interv Cardiol 2013; 26:454–462. doi: 10.1111/joic.12061. [DOI] [PubMed] [Google Scholar]
- 25.Berland J, Lefèvre T, Brenot P, Fajadet J, Motreff P, Guerin P, et al. DANUBIO - a new drug-eluting balloon for the treatment of side branches in bifurcation lesions: six-month angiographic follow-up results of the DEBSIDE trial. EuroIntervention 2015; 11:868–876. doi: 10.4244/EIJV11I8A177. [DOI] [PubMed] [Google Scholar]
- 26.Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation 2007; 115:2344–2351. doi: 10.1161/CIRCULATIONAHA.106.685313. [DOI] [PubMed] [Google Scholar]
- 27.Galassi AR, Tomasello SD, Capodanno D, Barrano G, Ussia GP, Tamburino C. Mini-crush versus T-provisional techniques in bifurcation lesions: clinical and angiographic long-term outcome after implantation of drug-eluting stents. JACC Cardiovasc Interv 2009; 2:185–194. doi: 10.1016/j.jcin.2008.12.005. [DOI] [PubMed] [Google Scholar]
- 28.Xu B, Qian J, Ge J, Wang J, Chen F, Chen J, et al. Two-year results and subgroup analyses of the PEPCAD China in-stent restenosis trial: a prospective, multicenter, randomized trial for the treatment of drug-eluting stent in-stent restenosis. Catheter Cardiovasc Interv 2016; 1:624–629. doi: 10.1002/ccd.26401. [DOI] [PubMed] [Google Scholar]
- 29.Kleber FX, Mathey DG, Rittger H, Scheller B. German Drug-eluting Balloon Consensus Group. How to use the drug-eluting balloon: recommendations by the German consensus group. EuroIntervention 2011; 7: Suppl K: K125–K128. doi: 10.4244/EIJV7SKA21. [DOI] [PubMed] [Google Scholar]
- 30.Kleber FX, Rittger H, Bonaventura K, Zeymer U, Wöhrle J, Jeger R, et al. Drug-coated balloons for treatment of coronary artery disease: updated recommendations from a consensus group. Clin Res Cardiol 2013; 102:785–797. doi: 10.1007/s00392-013-0609-7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.