

To the Editor
Airway management of patients with Coronavirus Disease 2019 (COVID-19) poses significant risk to involved staff because of the aerosolizing nature of airway interventions.1 Aerosolization can occur during facemask and supraglottic airway ventilation, intubation, extubation, and cardiopulmonary resuscitation.2 These activities require increased precautions and containment of viral respiratory particles. It has been demonstrated that a containment system can limit the spray of a significant portion of respiratory particles during a simulated cough or extubation.3,4
We applaud innovation of new protective barrier enclosures to protect the laryngoscopist and theroom during airway interventions. When selecting such a barrier device, one should consider the importance of access to the airway, containment of aerosolization, time required to set up the device for patient use, and patient tolerance of the device. One should also be cognizant of the cost and necessary time for production and deployment of the device. Some barrier devices, while superior at containing aerosolization, unfortunately restrict the laryngoscopist’s hand movements and would require abandoning a laryngoscopy attempt to remove the barrier if it proved too cumbersome. In some cases, it is important to allow a second pair of hands to access the patient’s airway to aid in the intubation should it prove difficult (providing lip traction, assisting with the stylet, etc). This may not be possible with some barrier devices. In addition, an ideal device could be set up quickly for patient use and not cause patient agitation, which isparticularly important in the pediatric population.
We propose an inexpensive clear plastic drape on bag barrier system made from materials that are ubiquitous in the hospital (Figure). The barrier can be easily removed even mid-laryngoscopy attempt. This drape on bag system consists of a 40-gallon drawstring bag covering the head of bed space that can be set up before patient arrival. The patient lies on top of it with the bag underneath head and shoulders. A 90 ×95 cm clear rectangular plastic drape (2 clear drapes can be cut from a single drawstring bag) is taped to the patient’s chest and is flipped over the patient’s head and laryngoscopist’s arms during preoxygenation and intubation. A plastic drape clamp attached to the clear drape weighs it down so it stays between the laryngoscopist’s arms. The ease, speed, and patient experience of having this plastic drape taped to the chest is similar to application of electrocardiogram leads. The total cost of disposable materials for this system is $1.44. There is nothing restricting access to the airway from under the drape, so one could easily assist the laryngoscopist or remove the drape during laryngoscopy if required. After intubation is performed and endotracheal tube secured, the clear plastic drape can be tucked into the drawstring bag, which now contains the contaminated airway space for the duration of the case. The patient could be later extubated under the clear drape, and the drape can then be removed and placed in the drawstring bag along with disposable airway equipment such as the suction catheter and stylet. The drawstring bag is then cinched closed, containing the contaminated drape and head of bed space, and can be disposed. We also recommend sealing used laryngoscopy equipment in a Ziplock Biohazard bag (Thermo Fisher Scientific, Waltham, MA).
Figure.
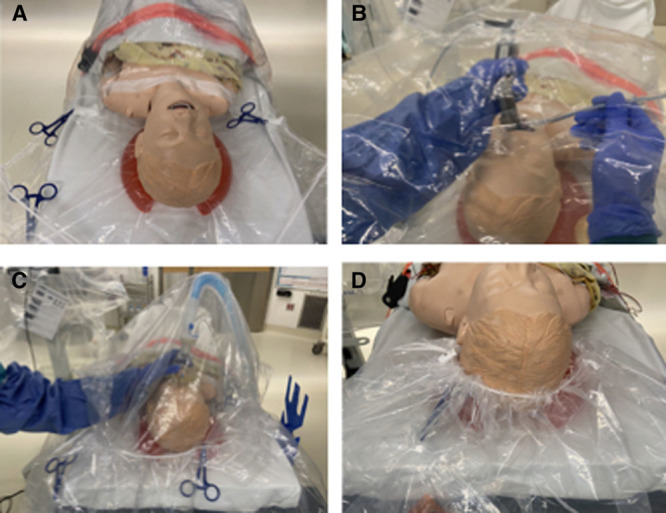
Use of plastic on bag barrier drape system. A, Patient lays on top of drawstring bag at shoulder level; clear drape is taped to chest. B, Flip clear drape over laryngoscopist’s arms during airway intervention. C, Extubate with drape tucked into drawstring bag to contain aerosolization. D, Dispose of clear drape in drawstring bag and cinch drawstring bag to contain contaminated head of bed space.
This plastic drape on bag system is being trialed at our hospital in the operating rooms and in the emergency department and intensive care unit. In simulated settings at our institution, it provides an added layer of protection from spray of contaminated viral particles for personnel present at airway procedures. The system contains the most contaminated surface surrounding the patient’s airway and can easily be disposed of to maintain a cleaner hospital environment. We found that the best use of this device is for nonemergent intubation of a tolerant or sedated patient.
Sarah Brown, MD
Fiona Patrao, MBBS
Shilpa Verma, MBBS
Alexa Lean, MD
Sean Flack, MB ChB
David Polaner, MD
Department of Anesthesiology & Pain Medicine
University of Washington
Seattle, Washington
sarah.brown@seattlechildrens.org
REFERENCES
- 1.Liu Y, Yan L, Wan L, et al. Viral dynamics in mild and severe cases of COVID-19. Lancet Infect Dis. 2020 March 19. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Coronavirus Disease 2019 (COVID-19). Centers of Disease Control and Prevention. Published March 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-risk-assesmenthcp.html. Accessed March 27, 2020.
- 3.Canelli R, Connor CW, Gonzalez M, Nozari A, Ortega R. Barrier enclosure during endotracheal intubation. N Engl J Med. 2020 April 3. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Matava C, Yu J, Denning S. Clear plastic drapes may be effective at limiting aerosolization and droplet spray during extubation: implications for COVID-19. Can J Anaesth. 2020 April 3. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]