

Abstract
Infection by coronavirus (CoV-19) has led to emergence of a pandemic called as Coronavirus Disease (COVID-19) that has so far affected about 210 countries. The dynamic data indicate that the pandemic by CoV-19 so far has infected 2,403,963 individuals, and among these 624,698 have recovered while, it has been fatal for 165,229. Without much experience, currently, the medicines that are clinically being evaluated for COVID-19 include chloroquine, hydroxychloroquine, azithromycin, tocilizumab, lopinavir, ritonavir, tocilizumab and corticosteroids. Therefore, countries such as Italy, USA, Spain and France with the most advanced health care system are partially successful to control CoV-19 infection. India being the 2nd largest populous country, where, the healthcare system is underdeveloped, major portion of population follow unhygienic lifestyle, is able to restrict the rate of both infection and death of its citizens from COVID-19. India has followed an early and a very strict social distancing by lockdown and has issued advisory to clean hands regularly by soap and/or by alcohol based sterilizers. Rolling data on the global index of the CoV infection is 13,306, and the index of some countries such as USA (66,148), Italy (175,055), Spain (210,126), France (83,363) and Switzerland (262,122) is high. The index of India has remained very low (161) so far, mainly due to early implementation of social lockdown, social distancing, and sanitizing hands. However, articles on social lockdown as a preventive measure against COVID-19 in PubMed are scanty. It has been observed that social lockdown has also drastic impacts on the environment especially on reduction of NO2 and CO2 emission. Slow infection rate under strict social distancing will offer time to researchers to come up with exact medicines/vaccines against CoV-19. Therefore, it is concluded that stringent social distancing via lockdown is highly important to control COVID-19 and also to contribute for self-regeneration of nature.
Abbreviations: ACE2, angiotensin-converting enzyme 2; BBC, British Broadcasting Corporation; CDC, Centers for Disease Control and Prevention; CoV, coronavirus; COVID-19, coronavirus disease-19; FDA, Food and Drug Administration; MERS, Middle East respiratory syndrome; NIH, National Institutes of Health; SARS, Severe Acute Respiratory Syndrome; SL-Cov-ZC45, SARS Like Coronavirus ZC45; SL-Cov-ZXC21, SARS Like Coronavirus; TGI, Tele Graph India; WHO, World Health Organization; ZXC21, HKU1, NL63, OC43 and 229E, different strains of coronavirus
Keywords: COVID-19, Clinical management, Environmental effect, Pandemic, Social distancing, Social lockdown
Graphical abstract
1. Introduction
Coronavirus (CoV) disease (COVID-19) has emerged as the largest pandemic experienced globally as it has already affected 210 countries (CDC, 2020, Fig. 1 ). Rolling data specify that the 2,403,963 individuals are infected by the disease out of which 624,698,168 have recovered and 165,229 did not survive the infection (WHO, 2020c). This infectious disease is caused by a new strain of the CoV for which treatment is not yet available (FDA, 2020; Jin et al., 2020). The disease is diagnosed mainly with symptoms such as dry cough, fever, fatigue and difficulty in breathing, which may be due to fibrosis and accumulation of cough in the air sacs of lungs (Huang et al., 2020). Moreover, wide variety of clinical symptoms related to common cold, fever and respiratory issues are noticed in infected persons and the severity of the disease can lead to death. The morbidity rate by the disease is found to be very high in elderly patients, and also in patients suffering from co-morbidity such as asthma, diabetes, cancer and cardiac diseases (Chu et al., 2004; Dong et al., 2020; Zhou et al., 2020). It is because, in disease4s such as cancer, multiple unwanted cellular events take place that lead to lower down the immunity of patients (Iswariya et al., 2019; Ilango et al., 2020). The first known case on the severe illness made by a CoV was reported in 2003, and it was called as “Severe Acute Respiratory Syndrome” (SARS) that lead to a severe epidemic in China (W.H.O., 2020c). A second severe epidemic by a CoV was reported in 2012 in Saudi Arabia, and it was referred as the “Middle East Respiratory Syndrome” (MERS) (Chafekar and Fielding, 2018; W.H.O., 2020a; Yao et al., 2020a, Yao et al., 2020b). In December 2019, the third severe case by CoV was diagnosed first in China which is now a pandemic almost in entire world affecting 210 countries. The present CoV is found to be a mutated form (ID-19) of its earlier two forms and has been named SARS-CoV-2 or CoV-19 and the disease caused by it is therefore, named as COVID-19.
Fig. 1.

Confirmed cases of COVID 19 positive cases worldwide. The intensity of color indicates number of affected people per 1 million people in world as of now on 02.04.2020 (Source https://google.com/covid19-map/?hl=en), b.-numerical values for the total number of cases in C-19 as on 04.03.2020.
CoVs constitute a large family of viruses (10). Structural analyses have confirmed that COVID-19 causing strain (CoV-19) is closely associated to two bat-derived SARS-like coronaviruses namely bat-SL-Cov-ZC45 and bat-SL-Cov-ZXC21, and both were isolated in 2018 from Zhoushan, eastern China. Genomic analysis on CoV-19 has revealed that it has 79% genetic similarity with SARS creating CoV (SARS-CoV) and 50% similarity with MERS creating CoV (MERS-CoV). It conforms that CoV-19 is a mutated form of the above two. The debate and rumors about man-made mutation or bio-engineering to produce the present causative CoV-19 from the above two forms are disproved as of now (Andersen et al., 2020; Science News, 2020).
Till today, no specific medicine has been identified or invented for the treatment of the disease COVID-19 because of mutation in strain CoV-19. Few drugs are contextually used for its treatment. Hydroxychloroquine and azithromycin (Gautret et al., 2020), lopinavir; ritonavir, remdesivir (GS-5734) (W.H.O., 2020c; Agostini et al., 2018; Brown et al., 2019; Cao et al., 2020; Gordon et al., 2020; Ko et al., 2020; Wang et al., 2020a, Wang et al., 2020b; Wit et al., 2020), tocilizumab, corticosteroids (Loutfy et al., 2003; Smith et al., 2020), certain nucleotide as inhibitors (Elfiky, 2020), COVID-19 protease inhibitors (Liu and Wang, 2020, Table 1 ) are few to name them. However, they are demonstrated to be beneficial for contextual treatment of COVID-19 patients. World Health Organization (WHO) has also not strongly recommended any specific drug for its treatment, hence, clinical management of COVID-19 with a specific medicine is still under investigation. The fact is well proved by the failure of the healthcare system of most developed counties such as Italy, USA, Spain and France, to save their citizens from COVID-19. These counties are found with high infection as well as high morbidity rate as compared to the other countries of the world. So, the whole world is struggling to bring out a specific treatment schedule against COVID-19 at this time point.
Table 1.
FDA and WHO recommended drugs for the treatment of COVID-19.
| Name of drug | Working root | Risk Factors | Overall efficacy |
|---|---|---|---|
| Chloroquine (Antimalarial) |
|
|
In vitro and limited clinical data suggest potential benefit. |
| Hydroxychloroquine (Antimalarial) |
Same as above | Same as above | Same as above |
| Lopinavir; Ritonavir (HIV Protease Inhibitor) |
|
|
Role in the treatment of COVID-19 is unclear. Preclinical data suggested potential benefit; however, more recent data has failed to confirm. |
| Remdesivir (Investigational Nucleoside Analogue) |
|
|
Investigational and available only through expanded access and study protocols; several large clinical trials are underway. |
| Azithromycin (Macrolide Antibacterial) |
|
|
Used in some protocols based on theoretical mechanism and limited preliminary data as adjunct therapy. |
| Tocilizumab (Interleukin-6 (IL-6) Receptor-Inhibiting Monoclonal Antibody) |
|
|
Immunomodulating agent used in some protocols based on theoretical mechanism and limited preliminary data as adjunct therapy. |
| COVID-19 convalescent plasma (Plasma collected from persons who have recovered from COVID-19 that may contain antibodies to CoV-19) |
|
|
Investigational use is being studied. |
| Corticosteroid therapy |
|
|
Not recommended for viral pneumonia; however, use may be considered for patients with refractory shock or acute respiratory distress syndrome. |
The table is prepared after Smith et al. (2020), an open access article with common creative attribution.
On the other hand, India, being the 2nd largest populous country, where, the healthcare system is severely suffering due to lack of infrastructure (0.7 hospital beds per 1000 people), medical equipments and doctors (doctor: population ratio is 1: 1800 instead of 1:1000), is surprisingly far from the predicted high rate of infection and mortality under COVID-19. The whole world is keenly watching, how India is successful in saving its people (since large portion of its population suffer from less hygienic life style) from COVID-19. As per government sources, at the capital of the country New Delhi, two key factors are believed to control the infection rate in India. They are through stringent social distancing via lockdown in the entire country and hand washing with soap and/or to sterilize with alcohol based sterilizers. Additionally, other associated societal or daily life activities supporting the above two steps are also imposed by the Government on its citizens. The above two activities appeared to be highly social in nature. As India is fully aware that it cannot afford sufficient clinical care to all infected, incase major portion of total 1.3 billion population will contract COVID-19. However, the results are quite impressive for the Central Government, New Delhi that India as the 2nd most populous country is not at all under the grip of the disease as compared to other countries. Rolling data indicate that the infection and death rate are still low (i.e. 9152 and 306 per 1.3 billion population for infection and death, respectively) in India as on 13th April 2020. Accordingly, the federal Government of India had declared a very strict social distancing for 21 days, and allowed some emergency services such as security, health and food chain to be available. Social distancing was very stringent during those 21 days (many opine it as harsh), however, so far it has yielded a positive result. Therefore, the Nation has received applause form World Health Organization (WHO), United States of America (USA) etc. Were above social measures the key strategies for the government to give a checkmate to both the rate of infection and mortality in India, is the central focus of this article. All authentic news sources such as Science magazine, Reuters, BBC news, Times, Hindustan India, India Today, WHO etc. along with scientific literature were carefully analyzed to reply to the above question positively. Apparently, it is concluded that social distancing is highly important at this time point to control the rate of infection of COVID-19 along with clinical management in India, to offer time to the researchers to come up with suitable medicine or vaccine against CoV-19 infection. Perhaps a strict social distancing gives India a prize value of 0.2 deaths per million people (rolling data) under COVID-19, which is quite low in comparison to other countries. May be this is the reason, there was a high chance for India and other countries to extend (as USA has been adapted) the lockdown period to 45 days instead of 21 days, and it is implemented. Other nations who have not maintained social distancing must take a page from the lessons learnt in India, that to observe a harsh social distancing covering their entire nation to fight COVID-19 disease. It was observed that the search result in PubMed with the term “social lockdown” (in relation to COVID-19) yields zero result, indicating no article published on this social move although, it is the only prevailing defense available for prevention of COVID-19 infection. On the other hand, due lack of human activity, the environment is found to self-regenerate. Many countries are experiencing low NO2 and CO2 emissions. So, air pollution is dropped and similar ecological events have been also observed in rivers and canals of many cities. It may result in proving a pollution free, clearer, stress free world during post-COVID-19 time (Chainy et al., 2016; Giraud-Billoud et al., 2019; Paital et al., 2016, Paital et al., 2019). Research on the medical invention of specific medicine and vaccine against COVID-19 is although the need of the present day, it is suggested that extensive studies must be done on social lockdown and its effects on combating COVID-19 as well as on the self-regeneration of the environment. Results will be helpful to take measure against any future deadly pandemic or epidemic that the planet may experience.
2. COVID-19 infection and its outbreak
2.1. Structural integrity of CoVs and CoV-19
Coronaviruses are a large family (four genera namely alpha, beta, gamma and delta) of viruses and all strains do not have virulent capacity (Peiris et al., 2003; Woo et al., 2009). CoVs are enveloped viruses with positive sense, and has single-stranded RNA genomes (Lai et al., 2007; Lu and Liu, 2012, Fig. 2 ). Out of 7 strains of CoVs, three strains namely, CoV i.e. SARS-CoV, MERS-CoV and SARS-CoV-19 (COVID-19) are found to be fatal because they cause severe clinical sickness (Mackay and Arden, 2015), whereas, the other four stains such as HKU1, NL63, OC43 and 229E CoVs are not that much fatal and only cause mild clinical symptoms in patients (Corman et al., 2018). On the basis of structural studies and biochemical experiments, Andersen et al. (2020) have noticed that CoV-19 appears to be optimized for binding to the human receptor Angiotensin-Converting Enzyme 2 (ACE2); and the spike protein of SARS-CoV-2 has a functional polybasic (furin) cleavage site at the S1–S2 boundary through the insertion of 12 nucleotides, which additionally led to the predicted acquisition of three O-linked glycans around the site. However, the viruses can have several receptor binding proteins such as receptor binding domain, polybasic cleavage site, proteinaceous peptidases binding site, human aminopeptidase N binding site and human dipeptidyl peptidase-4-site that help to bind to host cell surface (Corman et al., 2018; Wang et al., 2020a, Wang et al., 2020b). Once the virus binds to the host cell surface, it multiplies using the general viral pathway and causes severe blockage of lungs and air passages resulting in respiratory obstruction and death of patients (Yu et al., 2019).
Fig. 2.

A typical figure of COVID-19. White arrows indicate its receptors protein on its surface and the red arrows indicate the envelop protein. b) A single stranded RNA is enclosed by envelop protein layer (modified after Scripps Research Institute (89)).
2.2. Outbreak of SARS, MERS and COVID-19
The virulent strains of CoV can be responsible for causing severe illness with wide variety of symptoms mainly associated with common cold and respiratory syndromes. The first recognized case of severe clinical sickness caused by a CoV was reported in 2003 in China, and it was referred as SARS. It was an epidemic and highly contagious in China and death toll was 774 (BBC, 2020a; Caly et al., 2020; Guo et al., 2020; Habibzadeh and Stoneman, 2020; She et al., 2020). The second outbreak of severe medical sickness by CoV was started in 2012 in Saudi Arabia, and it was called as MERS, and its lethal zoonosis has contributed to 35·7% fatality as of now. Till February 2018, 2182 cases of CoV infection in MERS was reported, with 779 deaths. It was wide spread and seen in 27 countries with the very worst condition detected in Saudi Arabia which alone experienced 1807 infections and 705 deaths. The third case of CoV is the current pandemic case of COVID-19. It is the seventh CoVs identified to infect humans that has killed almost 114,215 people as on 10th April 2020. It is seen to affect mostly elderly and patients with co-morbidity, probably due to their low immunity (Fig. 3 ).
Fig. 3.

Death rate of patients as a function of age. Analyses of the data till 05.04.2020 indicates that elderly patients are with a high risk of death under COVID-19 infection, while, young and children are not totally safe (CDC, 2020).
2.3. History of COVID-19 outbreak
The world is now witnessing the most developed countries such as USA, France, Italy and Spain where best health care systems are available for their citizens as compared to the other developing nations experiencing the worst outbreak. However, the end of 2019 and entry of 2020 years, shall be considered as black days in world due to inefficiency of the medical care to control the COVID-19 outbreak, because it took away almost 1.14 million human lives as on 10th April 2020 from 210 countries. The most affected countries are with the most advanced medical care. As declared by WHO, the outbreak of COVID-19 has gradually moved to various countries. On 31st December 2019, the Chinese government had alerted WHO about an outbreak of a mutated strain of CoV that caused severe illness leading to fatality, and, it was subsequently named as SARS-CoV-2 or COVID-19. The story started when pneumonia in a patient under undiagnosed condition was detected in Wuhan city, China on 31st December 2019. WHO had taken it seriously and had worked on it continuously to analyze data, provide advice, coordinate with partners, help countries to prepare, increase supplies and manage expert networks regarding the virus. WHO had declared the outbreak of the unknown infection as a “Public Health Emergency of International Concern” on 30th January 2020. This international community then had asked for help of US$675 million for the people in states where, people suffer with weaker health care systems, as part of its “Strategic Preparedness and Response Plan”. On 11 February 2020, WHO had again officially announced a name for the new “coronavirus disease” as COVID-19. Following the severe infection rate and fatality, nearly 167,500 COVID-19 infected positive cases including 6600 deaths was reported with a belief that many mild or asymptomatic cases were still to be clinically diagnosed. This was reported by WHO up-to February 20, 2020. And by 6th April 2020, the virus was able to kill 89,954 infected patients, out of total 1,537,168 COVID-19 positive cases from 210 countries (CDC, 2020; Chafekar and Fielding, 2018; Zhou et al., 2020; Fig. 1). Most of them were found to be elderly as the pattern of death gets a sharp rise as a function of age of the patients (Fig. 3), although the fact is clear that it can kill all ages of people, especially patients with co-morbidity. The observed high rate and death in elders could be due to their inherent low immunity and co-morbidity. So, people with high natural immunity contract the disease at a low risk, and if infected, they may not develop severe symptoms. Their natural immunity keeps them safe with mild or no symptoms even if they are diagnosed as COVID-19 positive patients. Moreover, the recovery rate could be high in those patients with high natural immunity. At this early stage of understanding about the new coronavirus, it is unclear where COVID-19 falls on the immunity spectrum. Although, IL-6 is found to be modulated in patients infected with CoV-19. Role of complementary systems, specific antibodies, natural and induced immune-molecules are still to be investigated. Therefore, analyses of the immune-spectrum of such people (asymptomatic cases and patients who have recovered or with mild symptoms) may provide clue(s) to identify the sector where immunity works against CoV-19. If the answer is to develop antibody, then structural analysis could lead health care researchers to develop therapy against it (Chu et al., 2004; Chafekar and Fielding, 2018; Dong et al., 2020; Jin et al., 2020; Huang et al., 2020; Vellingiri et al., 2020; Zhou et al., 2020).
2.4. Mode of COVID-19 infection
Infection of Cov-19 in human host cells is similar to other SARS and MERS viruses. It has been demonstrated that CoV-2 spike (S) glycoprotein binds to the cell membrane protein ACE2 in order to fuse with the plasma membrane and enters into the host cell. Then a protein in CoV-19 called as the “S” protein, is cleaved into two parts. One subunit is called as S1 and the other unit is called as S2. The former one i.e. S1 contains the receptor binding domain which allows it to directly interact and bind to the peptidase domain present in the ACE2 of human host cell. Then the virus needs to fuse to the host cell to release its nucleic acid. This role is discharged by S2 protein of the virus. Therefore, S2 plays a role in membrane fusion. Structural analyses on ACE2 reveal that CoV-2 binds to its typical ligand (amino acid transporter i.e. B0AT1) to form ACE2-B0AT1 complex. However, SARS-CoV-19- receptor binding domain is not same in SARS or MERS. Therefore, ACE2-B0AT1 complex is proposed to be targeted for COVID-19 therapy. Also any antibody that target human ACE2 or coronavirus spike proteins can also be used to clinically investigate its efficacy in preventing the disease (Chu et al., 2004, Chafekar and Fielding, 2018; Dong et al., 2020; Jin et al., 2020; Huang et al., 2020; Vellingiri et al., 2020; Zhou et al., 2020)
2.5. Pathogenicity and histopathology in COVID-19 patients
Once a person contracts the disease, the virus exhibits several pathogenic symptoms. The pathogenic features from a cell biology point of view in COVID-19 patients are explained mainly by three stages. The lungs seem to be the main target site of the virus. In mild cases, the air passages are infected while in severe cases, gas exchange sites are affected. Stage 1) it spans 1–2 days of infection. After the CoV-19 enters into the host cell by inhalation as mentioned in Section 2.3 and 2.4, it starts replication mainly targeting the ciliated cells in the nasal cavity. Although throat infection and associated issues are common but nasal swab are suggested to be the right sample for the detection of the virus via RT-PCR. Stage 2) it covers next few days of infection where the patient develops common cold associated symptom such as dry cough, fever, tiredness. During this time, problems in the upper airway and conducting airway responses are seen in the patient. It is because the virus replicates and migrates to the lower respiratory tract along the conducting air passages. A strong innate immune system is induced by the host cells. Epithelial cells secrete more β and λ interferons, thus can be used as bio-markers along with the nasal swab and sputum of the patients for detection of the virus via RT-PCR. About 80% of infected patients show such mild symptoms and the viruses are mostly restricted in upper and conducting airways. Stage-3) this is the last stage of the viral infection under COVID-19 and the patients show clinical symptoms such as hypoxia, ground glass infiltrates, and progression to acute respiratory distress syndrome. <20% of the patients may reach this stage out of which few develop pulmonary infiltrates and manifest severity of the disease. At the severe stage, the virus infects the gas exchange units of the lung, mainly infects alveolar type II cells. It leads to rapid propagation of the virus leading to release of large viral particles and resulted in huge alveolar damage by forming fibrin rich hyaline membranes. Large areas of fibrosis in lungs lead to respiratory choking and death of the patients (Chu et al., 2004; Chafekar and Fielding, 2018; Dong et al., 2020; Jin et al., 2020; Huang et al., 2020; Vellingiri et al., 2020; Zhou et al., 2020).
Macroscopic studies indicate that CoV-19 is likely to affect the chest intensely and may include pleurisy, pericarditis, lung consolidation and pulmonary oedema (Jin et al., 2020). As a result the weight of lungs is elevated in patients. In patients with co-morbidity, it is believed that they are also attacked by viral infection which in turn leads to inflammation in the lungs (Huang et al., 2020). It is similar to a typical bacterial infection in lungs. Early histopathological study in patients with co-morbidity especially cancer was found that CoV-19 was also a causative factor for complication of their respiratory issues (Zhou et al., 2020). The patient detected as CoV-19 positive during operation in lung adenocarcinoma indicates that non-specific attributes included oedema, pneumocyte hyperplasia, focal inflammation and multinucleated giant cell formation as common histopathological characters with no hyaline membranes. Such patients usually show asymptomatic characters for CoV-19 (Dong et al., 2020). Therefore, early detection of COVID-19 is suggested. South Korea had followed rapid testing for which the country could restrict massive infection and death of its citizens from COVID-19. In some cases, postmortem biopsy report indicates that elderly patients have multiple ground glass opacities as also observed in their chest X-ray. Diffused alveolar damage with exudates, predominant lymphocytic inflammation and multinucleated giant cells, along with large atypical pneumocytes could be the dominant features in CoV-19 patients, especially in elderly cases. In such patients, microvesicular steatosis with mild inflammation may be noticed in the liver, and these features are also common in SARS and MERS patients as well. In some patients, renal histological changes and may include paramesangial and sub-endothelial deposits with segmental mesangial interposition and increased lamina rara interna, scattered sub-epithelial “hump-like” deposits in their kidney. Diabetes patients may show a clinical manifestation of characteristic changes of diabetic nephropathy including increased thickness of the glomerular basement membrane without deposits, mesangial expansion and segmental foot process effacement, and microvillous transformation. Abundant erythrocytes may obstruct peritubular capillary lumens with activation of endothelium in COVID-19 patients (Chafekar and Fielding, 2018; Dong et al., 2020; Jin et al., 2020; Huang et al., 2020; Vellingiri et al., 2020; Zhou et al., 2020).
2.6. Clinical management of COVID-19, the current scenario
As per WHO, the disease COVID-19 causes respiratory illness (like the flu) with symptoms such as dry cough, cold, fever, and in more severe cases, difficulty in breathing that leads to death of patients. No drugs are discovered for this virus as it is a new form (mutated) of its earlier versions. Some of the existing drug types such as anti-HIV, antibacterial and antimalarial drugs are repurposed to be useful to combat COVID-19. WHO has been repeatedly recommended social distancing and reveals that “you can protect yourself by washing your hands frequently, avoiding touching your face, and avoiding close contact (1 meter or 3 feet) with people who are unwell, because the disease is believed to spread primarily through contact with an infected person when they cough or sneeze. It also spreads when a person touches surfaces or objects that has the virus on them, then touches their eyes, nose, or mouth”. Organizations such as U.S. Food and Drug Administration (FDA), Centers for Disease Control and Prevention (CDC) and WHO have recommended but not yet approved few drugs namely chloroquine or hydroxychloroquine (both are antimalarial drugs), lopinavir; ritonavir which are HIV protease inhibitors, azithromycin which is a macrolide antibacterial medicine, tocilizumab that is an interleukin-6 receptor-inhibiting monoclonal antibody, COVID-19 convalescent plasma (plasma collected from persons who have recovered from COVID-19 and may contain antibodies to CoV-19), and corticosteroid therapy. Nevertheless, all these drugs have their limitations and risk factors as well as context dependent prescription to patients (Smith et al., 2020, Table 1). Eventually, it is clear that no direct or specific drugs are invented for the treatment of COVID-19 and all the available drugs focus on a particular aspect of the clinical consequences in COVID-19 patients (Caly et al., 2020). Although many alternative broad spectrum medicines are suggested to be helpful against COVID-19, but no research yet has been initiated on them (Hati et al., 2012; Paital et al., 2014; Paital et al., 2017; Mishra et al., 2019; Raja et al., 2020). Also, in silico screening of inhibitors against the viral replicase enzymes can be done but research on it is scanty (Paital et al., 2013). Therefore, currently, the emphasis lies on prevention rather than cure and most international clinical bodies understand that prevention could save many and the sharp rise of daily infection and mortality rate could be checked.
2.7. Role of specific drugs for the COVID-19 management
As discussed earlier there are no precise treatments accepted by the FDA for COVID-19, however, quite a few medicines being used are under clinical trials, and therefore, prescribed with limited clinical experiences. World Health Organization, CDC and FDA have currently placed an advisory for the use of certain drugs for the treatment of COVID-19. Each drug, their effectiveness and limitations are summarized below (Smith et al., 2020).
2.7.1. Chloroquine
It is an antimalarial drug and has in vitro activity against COVID-19 and is believed to have immune-modulating activities. Its works via inhibition of viral enzymes or processes such as viral DNA and RNA polymerase, viral protein glycosylation, virus assembly, new virus particle transport and virus release. It has also ACE2 cellular receptor inhibition activity; it can also acidify the surface of the cell membrane inhibiting fusion of the virus into the host cell. Some studies also have indicated its immune-modulation role in releasing cytokine. Pre-clinical data have proved its activity against COVID-19. In some cases, it also exhibits potential inhibitory role in the exacerbation of pneumonia patients under CODID-19 infection. However, its use is not recommended in patients with cardiac arrhythmias (it may also induce the same in patients) and, may create retinal damage, under long term consumption. Patients with G6PD deficiency, diabetics are recommended not to use this drug. It has also substantial drug interactions with other medicines. The EC50 values for chloroquine were found to be >100 μM at 24 h (Yao et al., 2020a, Yao et al., 2020b).
2.7.2. Hydroxychloroquine
It is an antimalarial medicine works in similar way to chloroquine. It is in vitro activity against COVID-19 has been proved and it has immune-modulating role in patients via cytokine release. Like chloroquine, it also mediates ACE2 cellular receptor inhibition and acidification at the surface of the host cell membrane that prevents the viral fusion to the host cell. Pre-clinical in vitro data suggest that it works against COVID-19 with more efficacy than chloroquine and it may be due to its higher in vitro antiviral effect compared to chloroquine when the drug was added prior to the viral challenge. The EC50 values for hydroxychloroquine was reported to be 6.25 μM at 24 h and 5.85 μM at 48 h. Data suggest that about 70% of hydroxychloroquine-treated patients were virologically cured compared to 12.5% in the untreated control group. Like chloroquine, it also has limitations for use because it can lead to cardiac arrhythmias, can mediate retinal damage, especially under long term use. This drug should not be prescribed to patients with G6PD deficiency and diabetics (Science News, 2020).
2.7.3. Lopinavir or ritonavir
These two drugs are used against HIV because the viral protease enzyme is inhibited by them. Their anti-viral activity against the SARS and MERS CoV has been proved in studies using in vitro and animal models. These two drugs are found to bind to Mpro enzyme that is used by CoV for its replication. Pre-clinical data recommend its use against COVID-19. A retrospective cohort study of hospitalized patients reviewing clinical course and risk factors for mortality included 29 patients who received lopinavir; ritonavir. No difference was noted in the duration of viral shedding after treatment with lopinavir; ritonavir. However, few critical COVID-19 patients were found to be recovered by treatment with these two drugs. The risk factors for these drugs include cardiac arrhythmias and are avoided for administration to patients with hepatic disease or hepatitis. It also has significant drug interactions like chloroquine and hydroxychloroquine (Cao et al., 2020).
2.7.4. Remdesivir
It is an investigational nucleoside analogue and it has a broad-spectrum antiviral activity in vitro and also specific in vitro inhibitory activity against wide verity of CoVs. It is a monophosphoramidate pro-drug of remdesivir- triphosphate which is an adenosine analog that acts as an inhibitor of RNA-dependent RNA polymerases. Remdesivir-TP competes with adenosine-triphosphate for incorporation into nascent viral RNA chains, therefore inhibits viral RNA production. After incorporation into the viral RNA, it terminates RNA synthesis because RDV-TP does not cause immediate chain termination. Therefore the drug is believed to evade proofreading by viral exo-ribonuclease activity. Clinical administration of this drug to several hundred COVID-19 positive patients in USA, Europe, and Japan resulted into satisfactory recovery rate. It has a high genetic barrier to resistance and it works against wide variety of CoV. Its EC50 value was found to be 0.77 μM, and half-cytotoxic concentration (CC50) was >100 μM with a selective index (SI) >129.87. Its pre-clinical study for prophylactic and therapeutic efficacy in mouse model is also well established. However, use of this drug is still under investigation (Ko et al., 2020).
2.7.5. Azithromycin
It is a macrolide antibacterial drug that inhibits the growth of bacteria. It may inhibit bacterial super-infection by preventing their growth, and is found to have immune-modulatory properties as an adjunct molecule. Clinical results of this drug in pulmonary inflammatory disorders are highly satisfactory. It down-regulates inflammatory responses and reduces the excessive cytokine production associated with respiratory viral infections; however, its direct effects on viral clearance are uncertain. Its immuno-modulatory mechanisms may include reducing chemo-taxis of neutrophils (PMNs) to the lungs by inhibiting cytokines especially, IL-8), inhibition of mucus hyper secretion, decreased production of reactive oxygen species, accelerating neutrophil apoptosis, and blocking the activation of nuclear transcription factors. Its action is enhanced when used with hydroxychloroquine therefore, is used as adjunct therapy. As an adjuvant along with hydroxychloroquine, it works against COVID-19 but clinical trials on it are under investigation. It has also present risk of cardiac arrhythmias and has significant drug interaction activity (Science News, 2020).
2.7.6. Tocilizumab
It is a monoclonal antibody that acts as inhibitor to interleukin-6 receptor. Since, it releases cytokine, it is suggested to be used against COVID-19. It mediates cytokine release signaling system by competitively binding to both, the soluble and membrane-bound interleukin-6 receptors. Therefore, it used as standard adjunct therapy against COVID-19 therapy. Further data on it concerning clinical effectiveness for COVID-19 are being investigated. It has risk of GI perforation, hepatotoxicity and is not recommended to patients with thrombocytopenia and neutropenia. It has infusion-related reactions (Smith et al., 2020).
2.7.7. Other immune-modulators
For COVD-19 treatment, few immune-modulators are used as adjuvants. COVID-19 convalescent plasma, corticosteroids, non-steroidal anti-inflammatory drugs are few to name them. However, clinical investigation on them is still going on (Smith et al., 2020).
Vaccination against an endemic or pandemic is considered as the best preventive measure. Although no specific vaccines are available in market to immunize people against CoV-19, work on it is going on and, sooner or later, the world expects it to come out for human immunization. Many existing vaccines are repurposed to be tested against the disease. There is an argument in favor of the Bacille Calmette-Guérin vaccine (BCG) being useful against infection with CoV-19 virus. However, the clinical evidence is not available. Two sets of clinical trials with COVID-19 patients are underway and shall be communicated by WHO, when and if result will be successful (WHO, 2020a). However, experimental evidence on human and non-human studies may disprove clinical relevance for use of the vaccine as a preventive measure against COVID-19. Although two protocols for clinical trial of BCG were reported, both were administered to health care workers who were directly involved in the care of patients infected with CoV-19, and no specific outcome was seen. Hence, use of BCG as a vaccine against CoV-19 is completely irrelevant. Therefore, WHO strongly discourages the use of BCG vaccine for immunization against CoV-19, but continues to recommend for its use in neonatal cases, to immunize them against tuberculosis disease (W.H.O, 2020a, W.H.O, 2020b, W.H.O, 2020c). However, it is expected that a typical time span required to develop a vaccine from the deadly CoV-19 would take 12–18 months assuming that all other factors are in place. The expected news about vaccine production may come first from the Dr. Sarah Gilbert, Professor of Vaccinology and her group at the Oxford University, who are going to conduct a human trial within few weeks with the vaccine that they have developed against CoV-19.
On the other hand, as discussed in Section 3.3., analyses of the full spectrum of immunity in asymptomatic CoV-19 positive cases, or those who have recovered from COVID-19 or with mild symptoms, could give an idea about the particular sector where the immunity works on CoV-19. Logically, although IgM would be the first one to be raised followed by IgG for any infection (including CoV-19), the exact variable (V), diversity (D) and joining (J) genes recombination (commonly called as VDJ recombination, Roth, 2014) which generates unique receptors (known as antigen receptors) that can collectively recognize many different types of antigen molecules (RBD of CoV-19 in current case) would provide the next clue for therapeutic purpose. Therefore, immunological analyses of the plasma of the patients who have recovered from COVID-19 are very important. Clinical trials are being conducted to evaluate the use of COVID-19 convalescent plasma to treat patients with severe or immediately life-threatening COVID-19 infections. COVID-19 convalescent plasma is not intended for prevention of the infection rather it would serve as the source of antibody that would be able block RBD of CoV-19 or ACE2 of human host cells. However, the eligible patients from where the plasma needs to be collected must fulfill the following criteria. The patient, must have laboratory confirmed COVID-19, must have severe or immediate life-threatening COVID-19, must have severe disease defined as: dyspnea, respiratory rate 30 breaths/min or greater, blood oxygen saturation must be 93% or less, partial pressure of arterial oxygen to fraction of inspired oxygen ratio should be <300, and/or, lung infiltration should be >50% within 24 to 48 h, must have life-threatening disease defined as: respiratory failure, septic shock, and/or, multiple organ dysfunction or failure and must provide informed consent for plasma therapy (Smith et al., 2020).
2.8. Preventives for COVID-19, the social lockdown
Social lockdown is a direction for restriction of inter-individual physical contacts. An instruction not to go out of homes is given in order to avoid outer environmental contacts including (asymptomatic) infected persons. Under this condition, minimal and emergency movement of general public is allowed. People providing emergency services such as medical care, food security, general security and medicine supply chain are usually allowed, so that makes it slightly different from a curfew. However, few emergency services such as food and medical supply chain can also be closed if the lockdown is done on emergency basis and the period of lockdown is less i.e. for one to two days or for few hours. Mass or community movement and physical contacts are not allowed during the lockdown periods. The central objective of this social movement under government direction is to forbid two people from different families or nearby inhabitants to come in close contact with each other.
COVID-19 is a transmissible disease that mainly infects healthy subjects when the person comes in (close) contact with infected persons. External or internal body fluid discharges such as cough, sneeze, saliva etc. of infected patients can infect healthy persons. COVID-19 also can be communicated to a healthy person through any object(s) that carries the virus. Under the global emergency of CoV-19 infection, many experts recommended for social lockdown as a preventive measure, mainly to protect healthy persons from infection. On the other hand, it may also lead to restriction of accumulation of total number of infected patients at a particular time point, so that, it would lead to better consequences by 1) preventing huge load on healthcare system at a certain time point, 2) restricting mass/community infection, 3) providing better health care to the infected persons. Social lockdown has also another important benefit that is, it may also allow the community to develop mild or full resistance to the mutated virus with low exposure via media of transport of the virus. Social lockdown also would provide more time to the researchers to work on the virus for production of medicine or vaccines against COVID-19. Owing to the importance of social lockdown, many nations started following it at different time points of the infection of their citizens by CoV-19.
2.9. Scientific background behind social lockdown
It was observed that not a single article was found in PubMed on social lockdown despite it being the only existing weapon for prevention against endemic, epidemic or the current pandemic COVID-19. An article published by Doremalen et al. (2020) on the undocumented COVID-19 indicates the potential sources of pandemic of this disease. They have noticed that about 86% of all infections were not documented in China prior to 23 January 2020 (including those with travel restrictions). The transmission rate of undocumented infections was 55% of documented infections per person. Further, they had noticed that the longevity of similar CoVs in aerosols (up to 1.2 h), on metals (up to 5.6 h) and on plastics (up to 6.8 h) was up to many hours (Doremalen et al., 2020). Therefore, social distancing was suggested by many experts to prevent the disease, so nations across world follow it with mild to stringent level of severity. In this context, various important reports on social distancing are coming up in PubMed. However, lockdown as a tool to contain CoV infection has not been well reported.
2.10. International progress on social lockdown under COVID-19
2.10.1. China
In relation to COVID-19 and the idea of social lockdown, China tops the list because both were initiated in China. After experiencing the COVID-19 outbreak, China initiated social lockdown in the last week of January 2020 in Wuhan city, the epicenter of the COVID-19 outbreak. Following social lockdown in Beijing, buses and cars were allowed to run but domestic flights and trains were cancelled. Then it was extended to the other parts of the country. So, the Wuhan city and its population were entirely isolated from other parts of the country for which the nation had gained the benefit of very low contamination in other parts. China, being the most populous country of the world, has experienced low (although initially it was very high) infection and fatality rate as compared to the other nations (W.H.O, 2020a, W.H.O, 2020b, W.H.O, 2020c). Therefore, WHO has praised China as “perhaps the most ambitious, agile and aggressive disease containment effort in history” (W.H.O, 2020a, W.H.O, 2020b, W.H.O, 2020c). This was one of the biggest social control campaigns in history and it had covered about 760 million people, a little more than half of the country's population (Zhong et al., 2020). However, India's ambition was even bigger given its three-week lockdown, it covers 1.3 billion people-almost double the number of Chinese people under lockdown (Zhong et al., 2020).
2.10.2. Italy
Italy was the second country after China whose citizens had contracted the disease very rapidly and therefore, was also the second country to adopt social lockdown. Social lockdown was declared in Italy on 21st February 2020 in north Italy covering only 50,000 people. However, practically and predictably the nation was unable to control the disease. The Federal government of Italy had declared the whole country under lockdown on 9th March 2020 allowing public transport to run partially, and it has initiated a public pass system for public to ride buses or board flights on emergency basis (BBC, 2020b). Therefore, the lockdown was not that strict in Italy. This and more infection to the elderly fraction of its population were the contributing factors for the high mortality rate in Italy.
2.10.3. The United States of America
The cause of high number and stiff rise in COVID-19 positive cases along with high death rate in America were caused mainly due to three reasons. 1) High percentage of migrants in comparison to the native Americans and their frequent international travel, 2) high rate of clinical diagnosis by the federal government and, 3) late and less stricter steps for social lockdown by the government, apart from the initial casual attitude of its citizen towards this social move (Rasheed et al., 2020). Hence, following the severe death and infection rate in USA under the grip of COVID-19, the American government on 29th March 2020, has extended the lockdown period for another 30 days up to April 30th 2020. The social distancing was extended by keeping the warning given by the public health expert in mind that the death in USA may touch 200,000 people in the US. The Trump government has explained that “The better you do, the faster this whole nightmare will end. Therefore, we will be extending our guidelines to April 30th to slow the spread.” Owing to the lack of ventilators in some public hospitals in USA, Mr. Trump directed that “hospitals not using ventilators will have to release them and that there was hoarding of the devices” (Rasheed et al., 2020). To start deep involvement of public for social distancing, the Director of NIH has also recommended people in USA in general to adapt this social act voluntarily and very stringently (Collins, 2020).
2.10.4. South Asia
2.10.4.1. Bangladesh
Bangladesh started implementing the act of social distancing very late on 25th March 2020 as per the direction of the Prime Minister Sheikh Hasina. Following 25th March, a 10-day “holiday,” was started in the country, when it was directed to shut down all industries excluding the essential ones and also had restricted transport system in the country. The Prime Minister warned the people early on 20th March 2020 which allowed people to move to their natives as soon as possible. People were also allowed to move to their villages after lockdown (TGI, 2020).
2.10.4.2. Sri Lanka
Sri Lanka is a very small (~20 million population) country and its population is little more than total population of Mumbai city of India (~14 million). The cost of loss of human life could be more in such condition. However, the country had experienced no scenes of chaos. The Sri Lankan government had first declared a holiday in entire country. However, it was observed that people did not consider the concept of social distancing seriously (Daniyal, 2020). Then its government declared a curfew to strictly maintain social distancing. Nevertheless, before the curfew, the Sri Lanka government made available bus and train facilities to avoid the rush of people from Colombo to their native places. The government had run special trains and buses to allow its citizen to reach their respective villages and cities before lockdown was announced (The Morning, 2020).
2.10.4.3. Pakistan
While the disease was spreading fast in European countries and slowly in South Asian countries, Pakistani Prime Minister Mr. Imran Khan and his government were yet to act. Later on 23rd March 2020, Mr. Khan formally declared lockdown and social distancing for his entire nation, but with least strictness as compared to the entire South Asian nations. He had a thought against the idea of a total lockdown. So, Mr. Khan Government placed an advisory to its citizens to follow social distancing with all possible measures. The argument was not to affect the socio-economic status of the country more unrealistic. His logic was “the situation is not that severe in comparison to the near neighboring nation China or countries like Italy”. However, the country took special measures for de-containment in various infected places like Sindh, where the lockdown was later made the most severe (Malik, 2020). As a preliminary measure, Pakistani government allowed more time to its citizens to move to their homes before declaring lockdown. However, Sindh was shut down for inter-city transport on 18th March 2020. And, the Pakistan government had allowed all passenger trains to move for six more days to allow people to reach their destination. Therefore, people were able to reach their native before full lockdown (Azam, 2020).
2.10.5. Social lockdown in India and its environmental impact
India is the 2nd most populous nation and the nation is still struggling to improve its health care system. A large portion of Indian population lives an unhygienic life style and contracts infectious and epidemic diseases frequently (Zaveri, 2019). Unhygienic life style is one of the important causes of infection in the community leading to endemics and other outbreaks (Naidoo et al., 2018). Therefore, India could be suspected as one of the finest home for the outbreak of the pandemic COVID-19. Moreover, as per World Bank studies, India is still struggling hard to provide sufficient hospital beds to its citizens. Infrastructure wise, India lags behind most of the countries because it can afford only 0.7 hospital beds per 1000 people, although many similar countries such as Afghanistan (0.5), Bangladesh (0.8), Cambodia (0.8), Ethiopia (0.3), Ghana (0.9), Guinea (0.3), Madagaskar (0.2), Mozambique (0.7), Nigeria (0.5), Pakistan (0.6), Sudan (0.8), Uganda (0.5) and Yemen (0.7) are also unable to provide >1 hospital beds per (their) 1000 citizens (World Bank, 2020, Fig. 4 ). India also stands far behind in the list of countries able to provide sufficient equipment to its public hospitals especially, ventilators at this point of time during the COVID-19 pandemic. As per a report by BBC news, India has only an estimated 48, 000 ventilators available for its entire 1.3 billion population (Biswas, 2020). As per WHO, number of doctors for people must be in the ratio of 1:1000. As per the last update, doctor: population ratio was 1:1800 in India. Although, some claims say that the required ratio of 1:1000 was achieved in 2018, one of the drawbacks in the study was that all AYUSH doctors were also included in the count (Kumar and Pal, 2018).
Fig. 4.

Number of beds available nation wise in respective years. India lags behind the far in the list and joins among counties such as Afghanistan, Bangladesh, Cambodia, Ethiopia, Ghana, Guinea, Madagaskar, Mozambique, Nigeria, Pakistan, Sudan, Uganda and Yemen. Data are as per the latest updates on 06.04. 2002 in Word Bank website.
Keeping this view in mind, the federal government in India lead by the Prime Minister Mr. Narendra Damodardas Modi took a very strict (some called it harsh) decision for the entire nation by declaring early lockdown. On 11th March 2020, WHO declared the outbreak of COVID-19 as an emergency and appealed to all nations to take stringent actions for detection and treatment of diseased persons in order to save their citizens. Analyses of the Indian scenario clearly indicated that the pandemic has really showed its intensity of infection and death after 9th March 2020 (Fig. 5a). And, after experiencing a slow movement of the disease, on 24th March 2020, Mr. Modi had declared the entire nation to maintain a lockdown for 21 days. The number of days was calculated to track infected persons, who would express their symptoms within 14 days, and another week was reserved to observe the situation over infection, death and recovery rate (Fig. 5a). Up to 5th April 2020, 6:00 pm, according to the Ministry of Health and Family Welfare, New Delhi, a total of 3577 COVID-19 cases including 65 foreign nationals, 274 recovered, 83 deaths, and 1 migrated, had been identified in its 29 states/union territories. Hospital/home (social) quarantine of all confirmed/suspected cases was still on-going (Fig. 5b). However, there may be many reasons for the low detection and death rate in India under CODID-19. There was a general opinion that low infection number could be due to lack of enough testing and diagnosis of people for COVID-19. The hot and humid climate of India could also possibly restrict the virus from propagating and therefore has lost potential to infect. Although scientific fidelity of these facts is not yet proven as India still has low positivity rate of infection as compared to other nations. On the other hand, at least the lockdown time has allowed all the non-resistant asymptomatic infected patients to exhibit clinical symptoms in different time intervals. It was detected that after 14 days of lockdown was completed on 6th April 2020, the infection rate was not as much as USA, Spain and Italy. If the upcoming hot and humid, summer climate will be harsh for the virus to grow and infect in India, it would be good news for the entire world to control the disease. One of the first studies on the effects of temperature on time taken for the virus to lose its infectivity has been done by Chin and group and reported in Lancet Microbe 2020 (Chin et al., 2020). They have shown that rising temperature definitely has an adverse effect on the activity of the virus. They report that the virus loses its activity by 5 min at 70 °C and in 30 min at 56 °C. However, these laboratory experiments will be tested in the upcoming summer season. Keeping all the above in mind, the extension of the lockdown was urged from many sectors including health experts, public figures, and institutions to control the disease. Following this, the Indian Government had extended the social lockdown up to 3rd May 2020.
Fig. 5.

Status of COVID-19 pandemic in India (Data obtained from the Ministry of Health & Family Welfare, Government of India, New Delhi). a) Although the first positive case was started in 1st January 2020, the rate of increase of the pandemic was not that much high I comparison to the other developed counties. The number of confirmed cases has gained a sharp increase from 9th March 2020 to 5th April 2020, but the number remained within hundreds up to 28th March and with 4000 up to 5th April 2020. It shows a great control over the disease. Similarly, recoveries and death rate were very slow limiting within 100, indicating a positive aspect in favor of control of the disease. b) The percentage of increase of the infection, recoveries death case was very slow and the graph have showed different spikes but overall a steady stable growth indicating a strong grip of the federal government of India over the diseases.
The above data indicate that with minimal health care facility; India had the only option to declare social lockdown as the measure against COVID-19. Many international news agencies made propaganda against the strict lockdown by the Indian government, describing it as harsh, intensive and mismanaged (Daniyal, 2020; Abidi and Jacinto, 2020). Nonetheless, the result from social lockdown is still encouraging for which WHO is closely working with India on preparedness and response measures for COVID-19 infection. They took surveillance and contact tracing, laboratory diagnosis, risk communications, community engagement, hospital preparedness, infection prevention and control, and implementation of containment plan in the infected area. However, the question remains unclear how 1.3 billion people were motivated by the Indian Government, being the largest social movements that the world would have experienced in its history (W.H.O, 2020a, W.H.O, 2020b, W.H.O, 2020c).
It is believed that the federal government officials of India must have done a lot of homework to implement national lockdown initially for three weeks. Gradual steps were taken in a very careful planned manner by the Modi government. The mentality of 1.3 billion people was perhaps first tested psychologically by observing “Janata Curfew”. Janata curfew or “people's curfew” was described by his as a curfew imposed by people, for the people and to be observed by the people on 22th March 2020 to combat COVID-19 outbreak. Except emergency services, all other services including bus, passenger trains were cancelled and, markets, malls were closed on that day from 7 am to 9 pm. Another social move was also coupled with Janata curfew. He had also requested his citizens to ring a bell, or to make similar sound using utensils etc. for 5 min at 5 pm on 22nd March 2020 on the terrace or balcony. This act was meant to encourage the people working at medical and paramedical sectors, cleaning sectors and police, who were rendering their services even under the threat of infection to their own lives. The Modi government received an overwhelming response from its citizens. However, it was very unrealistic and unscientific to stop COVID-19 spreading by one day lockdown; therefore, probably it was meant to uplift and involve the psyche of the 1.3 billion citizen during the long period of a stringent lockdown, in which the government had received a grand success.
Adding another feather to his careful move, the Modi Government had also suspended all international commercial flights very early from 22nd March 2020 for a week which was completely cancelled until further order. And, the government had also suspended issue of majority of visas. Both steps were meant to prevent entry of COVID-19 to its land via human host and non-human objects (APT, 2020).
Taking a day break after Janata Curfew, the Prime Minister had declared on 24th March 2020, about a 21-day lockdown, for the in entire nation covering its 1.3 billion people. Akin to the Janata curfew, he had announced that “In order to protect the country, and each of its citizens, from midnight tonight, a complete ban is being imposed on people from stepping out of their homes.” However, different state governments were allowed to issue special pass for movement of people for emergency services (Das and Paital, 2020a). And, unbelievable to many, again the federal government of India had received massive success on its plan, except an intelligence failure of Tablighi Jamaat event, a Muslim religious event observed at Nizamuddin in Delhi's where about 8000 indigenous and foreign Muslims were gathered (Business Today, 2020). The people attended the event from different countries and almost from all states of India, have responsible for 30% of the total COVID-19 positive cases in India, and still counting (Chandrashekhar, 2020).
After people had already participated for two weeks in the social lockdown, the Prime Minister had expressed his gratitude to all his citizens and gave another simple, beautiful and positive task to every residing family in the country. It was meant to show their integrity to fight against COVID-19 with social distancing as preventive measures. He had asked to his country residents to light candles, mobile lights and torch lights on their balcony or terrace etc. but had urged them to keep other lights of home switched off for 9 min at 9 pm on 5th March 2020. This measure was to encourage the people to practice social distancing. It indicates that Indians were united and would possibly co-operate with their government to fight and defeat COVID-19.
The social move in India for lockdown was criticized by many, saying “India is probably the first large developing country and democracy into which this pandemic will arrive and many of the advantages of the Chinese (state) control and of having the health systems of Europe or the U.S.A. are not available to India (Chandrashekhar, 2020; Daniyal, 2020). This was obvious from the current healthcare system present in India. Many international agencies including WHO had suspected that only lockdown in entire nation would not be helpful to eradicate or control COVID-19 in India. Rather quick diagnosis of large number of asymptomatic suspected individuals must be done to isolate them from the healthy persons and vice versa and to provide them with medical treatment. It would lead to restrict the new infection (W.H.O., 2020a). Although, there was a dwindling expectation of getting success with lockdown against COVID-19 by international bodies, social distancing was the only option with India (Chandrashekhar, 2020). In the meantime, COVID hospitals are being set up in all the states and many districts of the country. Personal protective equipment and emergency medical equipment are being procured on war footing. On the other hand, it had a massive negative impact on society especially on weaker section population but huge positive impact on environment.
The lockdown in India had enormous negative impacts on the poor people especially on the daily wage laborers, interstate migrant workers and small scale vendors, as they were unable to earn their daily bread and were in no condition to move (Abidi and Jacinto, 2020). A period of a few days to travel back to their homes in villages might have been helpful for them. However, intrastate and interstate travel was already restricted on announcement of lockdown. The whole country was on stand still beyond imagination giving success to the government while putting the weaker section into the worst condition. Large-scale inter and intra state migrant workers were trying to walk hundreds of kilometers to their homes due to lack of transport services, while complaining of human rights violation for not providing them with transport and food facilities (Livemint, 2020a). However, legal instructions from the respective high courts of states were directed to stop such migration of people, because they could initiate stage III infection i.e. spreading of infection among communities. Nevertheless, the direction also included that the government should take care of the people for their shelter and food (Emmanuel, 2020). False social media about the special inter-state bus service by government to native also resulted to rush of people into several bus stands; Anand Vihar bus terminal, New Delhi, was considered as the most active case. Similar incidents have been observed in Mumbai too. While, the government allowed two international flights to bring back the Indians from two countries like Iran, it could not make secure arrangements for the local migrants (PTI India Today, 2020a). On one hand, few criticized the lockdown for its mismanagement that Indian policies during COVID-19 outbreak were only made to protect the rich and middle class not for the weaker class people, lockdown was arrogant and domineering declarations which had brutal consequences, especially on poor, $22.6 billion economic package for cash and food was too little, too late. On the other hand, many also opined that this pandemic has also sparked unexpected acts of assistance and communal mobilization to support (food and shelter) Indian's stranded and needy by the lockdown and it happened with least red-tapeism (Abidi and Jacinto, 2020). However, in four major cities such as Delhi, Mumbai, Chennai and Bengaluru of India, the economic loss was distinctly observed (Livemint, 2020a). Together, the above factors had given a challenge to the federal government to tackle the situation (Fig. 6 ).
Fig. 6.

Major economic associated change in three main cities of India. Data are as per the daily foot prints in terms of walk-ins from Goole India data (in first week of lockdown) to the respective sectors in first week of lockdown. The average changeover of foot prints (%) are represented in Delhi, Mumbai, Bengaluru and Chennai for a) banking and petrol pump sector, b) grocery shops and in c)diagnostic centres (sources Livemint (60)). Reproduced under a creative commons license (60).
During this crisis, the service rendered by different non-government organizations (NGOs), private companies, state governments, several personal contributors and gurudwaras made the task easy for the federal government. Local governments and NGOs took excellent action to halt the issues of immediate sufferers i.e. the migrants and daily wages. However, owing to the huge population of migrant laborers, daily wage workers, destitute etc. in the country, it is undoubtedly difficult to cover all of them. Attempts have been made to provide them with shelter and food in nearby areas for the entire lockdown period (Livemint, 2020b). At least 100–200 daily wage laborers per village cluster (called as Gram Panchayat) were provided with food and shelter for the entire lockdown period (Livemint, 2020a, Livemint, 2020b; Panda, 2020). Furthermore, the small scale vendors and others whose transactions were totally sealed under lockdown were provided with a lump sum amount by governments (for example, 3000 INR by the Odisha state government to its 65, 000 vendors (PTI India Today, 2020b), 5000 INR to auto rickshaw and taxi drivers by New Delhi state government, BT, 2020). Each state was advised to take care of their own residents as well as the other state's migrant workers. Toll free telephone numbers (eg.104 in the state of Odisha) were also issued to help people to identify COVID-19 infection, advice the people and direct them for diagnosis and treatment to the free COVID-19 hospitals set up by the states (Suffian, 2020).
On the financial front, India had a budget of $23 billion to help the weaker section people who are affected by COVID-19 indirectly i.e. by lockdown (Ahmed, 2020). India was also able to receive a generous help from global agencies and nations to protect its citizens form COVID-19. The World Bank had announced $1 billion support to India to combat COVID-19 and it is the largest ever health sector support from the Bank that was given to India (Noronha, 2020). Similarly, USA had declared a $2.9 million financial assistance package for India to develop laboratory systems, activate case-finding and event-based surveillance, and support technical experts for response and preparedness against COVID-19 (Chaudhury, 2020; TET, 2020). Subsequently, the federal government of India had also released around $1450 million to each of its states from its own disaster management fund to combat COVID-19 outbreak (TET, 2020). In addition, the Indian government has been richly supported by the business sector and various other fields by contributing funds in a big way to manage the COVID 19 crisis. May be his officials far sight for which; it has received lauds from global agencies. Despite this, it was suspected that at least 75,000 COVID-19 infections in India are present as carrier of the disease in the form of asymptomatic cases (Dogan, 2020).
WHO declared that “the measures taken by India to break the communities spread of COVID-19 by the lockdown was very early, scientific and timely decision” (Kumar, 2020). In the words of Dr. David Nabarro, special envoy on the disease, WHO (Sharma, 2020) “The lockdown in India was quite early on, when there was relatively a small number of cases detected. This was really a far-sighted decision because it gave the whole country the opportunity to come to terms with the reality of this enemy. People understood that there is a virus in our midst. It gave time to develop capacities at the local level for interrupting transmission and sorting out hospitals. Of course, there is a lot of debate and criticism, and inevitably with a lot of frustration and anger that life is being disturbed in this way. It is very, very upsetting. I think it is courageous of the government, honestly, to take this step and provoke this enormous public debate and let the frustration come out, to accept that there will be hundreds of millions of people whose lives are being disrupted. For poor people on daily wages, this is a massive sacrifice they are making. And to do it now at an early stage as opposed to waiting three or four weeks later when the virus is much more widespread was very courageous (Sharma, 2020).”
The decision of 21 days national lockdown followed by another phase of lockdown up to 3rd May 2020 had also other scientific effects especially on protection of environment in the country. India currently is also experiencing the drastic reduction of pollution in many of its metro cities. As a result of lockdown and in some places complete shutdown in India (where the disease COVID-19 hit to make hot spots), air pollution was reduced to multi-folds. The reason was attributed to reduction in NO2 and CO2 emission from fossil fuels from different sectors. The average nitrogen dioxide level in major cities such as Mumbai, Pune and Ahmedabad was reduced by 40–50% by March 2020 as compared to March 2019 (Wright, 2020). The sky of New Delhi was clearly visible than four months ago. Also the effects of lockdown were very clear on water bodies. Some of the river water bodies are found to exhibit never seen glittering scenery. The Yamuna River and its sky in New Delhi can be considered as an active example. Locals claimed that they have never seen such sparkling Yamuna river water and the blue sky canopy over it. It may be due to the shutdown of industries in New Delhi and lack of release of their effluents into it (Gandhiok, 2020, Supplementary Figs. 1 and 2).
Overall take home messages observed by society due to COVID-19 outbreak and subsequent social lockdown are 1) the economy of the world can be changed rapidly without any physical war, 2) European countries were more sufferers from COVID-19 due to their casual response to social lockdown, 3) the superstition in India that priest can save live and cure patients in India is disproved in current COVID-19 infection condition, 4) still 5–10% citizens in India are always casual even under any emergency condition in nation because they do not consider social lockdown seriously (W.H.O., 2020c; Tripathi, 2020), 5) for the first time in history, Indian government has spent billions of rupees on poor without any red-tapeism, 6) researchers, medical and paramedical professionals worth more than any one especially the high paid players such as footballers or cricketers, 7) fossil fuels are worthless in a society without consumption and its consumption lead to pollution, 8) many people could feel that how it would be difficult for the animals when kept in zoo for human entertainment, 9) the planet regenerates quickly without humans into play, as observed in Yamuna river and air pollution in New Delhi, India, 10) majority of people can work from home efficiently, so offices must give importance on work output not on attendance, 11) all can survive well without junk food and avoid to contract the associated disease to it, 12) living a hygienic life is so easy and it does not required much expenditure, 13) there are a lot of good people in the world who feed animals (Das and Paital, 2020b), take care of the needy and put their life into risk to save mankind and education converts such persons from man to human being, hence, 14) if more schools, colleges and universities are build, no need to construct more hospitals, 15) life can be easy without so much false and unhealthy competition to grow, 16) government must learn how to management several works in an eco-friendly way.
2.10.6. Countries not affected by CoV-19
Another scientific proof in favor of lockdown is North Korea, maintaining isolation from the rest of the world and not contracted COVID-19. As on 7th April 2020, Turkmenistan was another country who has reported no infection of its citizens by CoV-19. Such instances are also found in few African countries. Two countries in Africa namely Lesotho and Comoros are free of CoV-19 infection. Officially, both the countries have reported zero positive cases. In recent days, both South Sudan and Sierra Leone have reported their instances of very low infection or first cases. The virus also remains mostly undetected in the smaller Pacific island nations such as the Solomon Islands and Vanuatu. As of 2nd April 2020, 18 countries were reported having no COVID-19 infection. Those countries were Comoros, Kiribati, Lesotho, Marshall Islands, Micronesia, Nauru, North Korea, Palau, Samoa, Sao Tome and Principe, Solomon Islands, South Sudan, Tajikistan, Tonga, Turkmenistan, Tuvalu, Vanuatu and Yemen. Even on 12th April 2020, countries such as Comoros, Kiribati, Lesotho, Marshall Islands, Micronesia, Nauru, North Korea, Palau, Samoa, Solomon Islands, Tajikistan, Tonga, Turkmenistan, Tuvalu, Vanuatu and Yemen were not affected by the deadly infectious virus. Out of many, less human traffic, high immunity, isolated pockets (location that indirectly indicates lockdown) of the county from rest of the world could be the contributing factors for lack of COVID-19 infection; however, a systematic scientific studies are required to prove the fact (BBC, 2020b; Habibzadeh and Stoneman, 2020; WHO, 2020a).
As per many, social lockdown really provides opportunity to spend time with family members. Therefore, it meant for real social interaction among family and friends but without physical meeting. It has positive effects on health and immunity. Social lockdown is a social move that will restrict the rate of both infection and death by COVID-19 (Das and Paital, 2020a). The disease spreads through various modes other than social contact and infects human subjects though different mode of actions (Doremalen et al., 2020; Li et al., 2020a, Fig. 7 , for details please see Sections 3.3 and 3.4). Therefore, scientific background behind a strict social lockdown along with health care of the infected individuals will prohibit the virus to infect healthy human subjects (Ashour et al., 2020). Although many drugs work in contextual manner against COVID-19, but unsuccessful rate is also high among elders (Arabi et al., 2019; Colson et al., 2020; Cortegiani et al., 2020; Gao et al., 2020; Xu et al., 2020, 82–86). Hence, social lockdown and medical care to infected patients will prohibit the infection or will infect with a slow rate; as a result it may allow researchers to produce specific medicine or vaccine against the disease (N.I.H, 2020; Shereen et al., 2020; Scripps Research Institute, 2020; Li et al., 2020b).
Fig. 7.

Propagation of CoV-19 in host cells via S protein that binds ACE2.
a)After S binds to ACE2, the conformation change in the S protein to cleave it into S1 and S2 proteins that facilitates viral envelope fusion with the cell membrane through the endosomal pathway. Then CoV-19 releases RNA into the host cell and its RNA is translated into viral replicase polyproteins pp1a and 1ab, which are then cleaved into small products by viral proteinases. The polymerase produces a series of sub-genomic mRNAs by discontinuous transcription and at the end, translated into relevant viral proteins. Viral proteins and genome RNA are subsequently assembled into virions in the ER and Golgi and then transported via vesicles and released out of the cell. ACE2, angiotensin-converting enzyme 2; ER, endoplasmic reticulum; ERGIC, ER–Golgi intermediate compartment (reproduced from Shereen et al. (2020) under a Creative Commons license). b) Different stages of growth and propagation of COVID-19 in human lungs (reproduced from Li et al. (2020b) under a creative commons license).
3. Conclusion
COVID-19 is one of the most dangerous pandemics the whole world has ever encountered. It is caused by the CoV-19 virus that is believed to be mutated from two of its earlier forms found in bat. No vaccine or specific medicines are invented to combat the disease but prevention with social distancing and cleaning hands is found to be most effective. Countries such as Italy, USA, Spain, and France, with the most advanced health care systems have failed in controlling the infection possibly due to lack of social distancing. On the other hand, India being the world's second highest populous country with poor hygiene and health care systems has controlled the disease successfully with a very low infection and death rate under COVID-19. Nevertheless, it is important to note that pundits remark that not enough testing has been carried out for COVID-19 in India. However, at the moment, social lockdown is the only preventive found to be feasible and effective, and therefore, it is recommended that other counties with low infection rate could follow this scientific but a strict social move for a considerable period to handle the CoV-19 pandemic (Fig. 8 ). Eventually, research leading to development of vaccines and medicines is required for healthcare systems to take care of the disease and infected as well as, healthy people. Nevertheless, governments, research bodies and common people, look forward with optimism that the world will emerge with a new hope, research and tools for eradicating this infection. At this juncture, it is extremely important to note that individual management under social lockdown seems to go a long way in combating the COVID-19 pandemic. On the other hand, social lockdown mediated drastic reduction of environmental pollution is one of the positive outcomes of this social move.
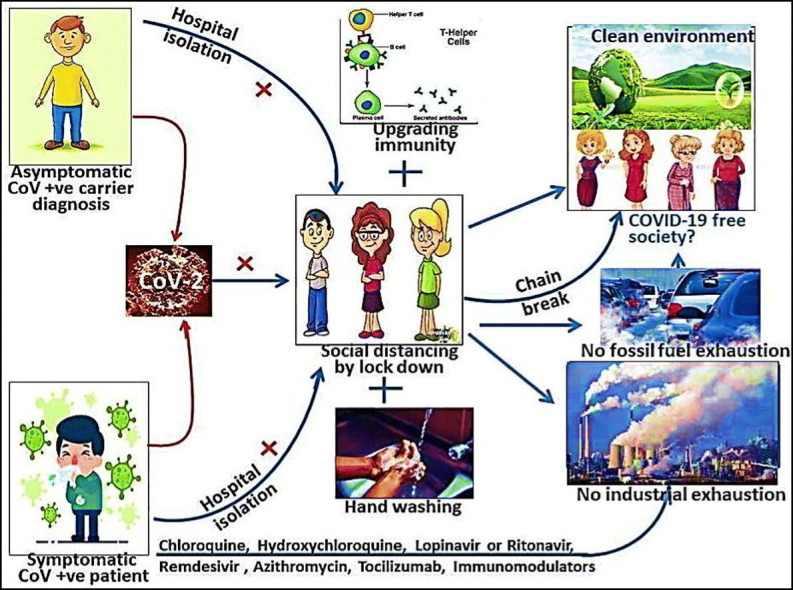
Fig. 8.

A cartoon showing the management of COVID-19 with the advisable medicines or preventive measures by social distancing. “X” symbol indicates the prevention the disease and “+” indicates the additional effort required along with social distancing to prevent the disease. Immuno-modulating life style by changing food habit, exercise etc. may be adapted.
Authors contribution
Conceptualization: BRP, KD, SKP; roles/Writing - original draft: BRP; writing - review & editing: BRPKD, SKP; funding acquisition: BRP, KD.
Funding
Schemes (number no. ECR/2016/001984 by Science Engineering Research Board, Department of Science and Technology, Government of India and 1188/ST, Bhubaneswar, dated 01.03.17, ST-(Bio)-02/2017 by Department of Biotechnology, DST, Government of Odisha, India) to BRP are acknowledged. Funding to KD (36 Seed/2019/Philosophy-1, letter number 941/69/OSHEC/2019 dt 22.11.19) from Department of Higher Education, Government of Odisha, India under OURIIP scheme is dully acknowledged.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgements
Thanks to Prof. Pawan Kumar Agrawal, honorable Vice Chancellor of Odisha University of Agriculture and Technology, Prof. Bikash Kumar Panda, honorable Director, College of Basic Science and Humanities, Bhubaneswar to allow working from home under lockdown period for which this article could be written. Language correction by Dr. Shravani Bhanja is duly acknowledged.
Editor: Jianmin Chen
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.scitotenv.2020.138914.
Appendix A. Supplementary data
Inter nation social lockdown versus medical care against COVID-19, a mild environmental insight with special reference to India Biswaranjan Paital1,*, Kabita Das2, Sarat Kumar Parida31Redox Regulation Laboratory, Department of Zoology, Odisha University of Agriculture and Technology, College of Basic Science and Humanities, Bhubaneswar-751003, India, 2Post Graduate Department of Philosophy, Utkal University, VaniVihar, Bhubaneswar, India, 3Department of Nephrology, Srirama Chandra Bhanja Medical College and Hospital, Mangalabag, Cuttack, Odisha, India.
References
- A.P.T COVID-19: India suspends entry of international flights for one week. 2020. https://www.airport-technology.com/news/COVID-19-india-suspends-entry-of-international-flights-for-one-week/ (Retrieved on 11.04.2020)
- Abidi A., Jacinto L. REUTERS; 2020. Lack of Compassion, More Than Resources, Marks India’s Deadly Lockdown Mismanagement.https://www.france24.com/en/20200401-lack-of-compassion-more-than-resources-marks-india-s-deadly-lockdown-mismanagement (retrieved on 11.04.2020) [Google Scholar]
- Agostini M.L., Andres E.L., Sims A.C., Graham R.L., Sheahan T.P., Lu X., Smith E.C., Case J.B., Feng J.Y., Jordan R., Ray A.S., Cihlar T., Siegel D., Mackman R.L., Clarke M.O., Baric R.S., Denison M.R. Coronavirus susceptibility to the antiviral remdesivir (GS-5734) is mediated by the viral polymerase and the proofreading exoribonuclease. mBio. 2018;9(2) doi: 10.1128/mBio.00221-18. e00221-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahmed A. India outlines $23 billion stimulus to help poor hit by lockdown. 2020. https://www.weforum.org/agenda/2020/03/india-stimulus-support-lockdown-pandemic-covid19-epidemic-economics/ (retrieved on 11.04.2020)
- Andersen K.G., Rambaut A., Lipkin W.I., Holmes E.C., Garry R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020 doi: 10.1038/s41591-020-0820-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arabi Y.M., Deeb A.M., Al-Hameed F., Mandourah Y., Almekhlafi G.A., Sindi A.A., Al-Omari A., Shalhoub S., Mady A., Alraddadi B., Almotairi A.A., Khatib K., Abdulmomen A., Qushmaq I., Solaiman O., Al-Aithan A.M., Al-Raddadi R., Ragab A.A., Harthy A., Kharaba A., Jose J., Dabbagh T., Fowler R.A., Balkhy H.H., Merson L., Hayden F.G., Saudi Critical Care Trials group Macrolides in critically ill patients with Middle East Respiratory Syndrome. Int. J. Infect. Dis. 2019;81:184–190. doi: 10.1016/j.ijid.2019.01.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashour H.M., Elkhatib W.F., Rahman M.M., Elshabrawy H.A. Insights into the recent 2019 novel coronavirus (SARS-CoV-2) in light of past human coronavirus outbreaks. Pathogens. 2020;9(3):E186. doi: 10.3390/pathogens9030186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Azam O. Seven rickshaws crammed full of people leave for Rahim Yar Khan. 2020. https://www.thenews.com.pk/print/634951-seven-rickshaws-crammed-full-of-people-leave-for-rahim-yar-khan (retrieved on 11.04.2020)
- B.B.C. Coronavirus deaths exceed Sars fatalities in 2003. 2020. https://www.bbc.com/news/world-asia-china-51431087 (retrieved on 11.04.2020)
- B.B.C. Coronavirus: Venice carnival closes as Italy imposes lockdown. 2020. https://www.bbc.com/news/world-europe-51602007
- B.T Coronavirus lockdown: Delhi govt to give Rs 5,000 to auto, cab drivers. 2020. https://www.businesstoday.in/current/economy-politics/coronavirus-lockdown--delhi-govt-to-give-rs-5000-to-auto-cab-drivers/story/400001.htmlm (retrieved on 11.04.2020)
- Biswas S. BBC news. Coronavirus: India's race to build a low-cost ventilator to save COVID-19 patients. 2020. https://www.bbc.com/news/world-asia-india-52106565
- Brown A.J., Won J.J., Graham R.L., Dinnon K.H., Sims A.C., Feng J.Y., Cihlar T., Denison M.R., Baric R.S., Sheahan T.P. Broad spectrum antiviral remdesivir inhibits human endemic and zoonotic deltacoronaviruses with a highly divergent RNA dependent RNA polymerase. Antivir. Res. 2019;169:1–10. doi: 10.1016/j.antiviral.2019.104541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Business Today Coronavirus update: who gave permission for Tablighi Jamaat event in Delhi. 2020. https://www.businesstoday.in/current/economy-politics/coronavirus-update-who-gave-permission-for-tablighi-jamaat-event-in-delhi-asks-sharad-pawar/story/400282.html
- C.D.C CDC Website. 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidancemanagement-patients.html (retrieved on 11.04.2020)
- Caly L., Druce J.D., Catton M.G., Jans D.A., Wagstaff K.M. The FDA-approved drug Ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antivir. Res. 2020;104787 doi: 10.1016/j.antiviral.2020.104787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cao B., Wang Y., Wen D., Liu W., Wang J., Fan G., Ruan L., Song B., Cai Y., Wei M., Li X., Xia J., Chen N., Xiang J., Yu T., Bai T., Xie X., Zhang L., Li C., Yuan Y., Chen H., Li H., Huang H., Tu S., Gong F., Liu Y., Wei Y., Dong C., Zhou F., Gu X., Xu J., Liu Z., Zhang Y., Li H., Shang L., Wang K., Li K., Zhou X., Dong X., Qu Z., Lu S., Hu X., Ruan S., Luo S., Wu J., Peng L., Cheng F., Pan L., Zou J., Jia C., Wang J., Liu X., Wang S., Wu X., Ge Q., He J., Zhan H., Qiu F., Guo L., Huang C., Jaki T., Hayden F.G., Horby P.W., Zhang D., Wang C. A trial of lopinavir-ritonavir in adults hospitalized with severe COVID-19. N. Engl. J. Med. 2020 doi: 10.1056/NEJMoa2001282. NEJMoa2001282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chafekar A., Fielding B.C. MERS-CoV: understanding the latest human coronavirus threat. Viruses. 2018;10(2):93. doi: 10.3390/v10020093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chainy G.B.N., Paital B., Dandpat J. An overview of seasonal changes in oxidative stress and antioxidant defence parameters in some invertebrate and vertebrate species. Scientifica. 2016;6126570:1–8. doi: 10.1155/2016/6126570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chandrashekhar V. 1.3 billion people. A 21-day lockdown. Can India curb the coronavirus? Science. 2020 doi: 10.1126/science.abc0030. [DOI] [Google Scholar]
- Chaudhury D.R. USA announces $2.9 million package to help India combat COVID-19. 2020. https://economictimes.indiatimes.com/news/international/business/usa-announces-2-9-million-package-to-help-india-combat-COVID-19/articleshow/74882445.cms?from=mdr (retrieved on 11.04.2020)
- Chin A.W.H., Chu J.T.S., Perera M.R.A., Hui K.P.Y., Yen H.L., Chan MlCW, Peiris M., Poon L.L.M. Stability of SARS-CoV-2 in different environmental conditions. Lancet. 2020 doi: 10.1016/S2666-5247(20)30003-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chu C.M., Cheng V.C.C., Hung I.F.N., Wong M.M.L., Chan K.H., Chan K.S., Kao R.Y.T., Poon L.L.M., Wong C.L.P., Guan Y., Peiris J.S.M., Yuen K.Y., HKU/UCH SARS Study Group Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings. Thorax. 2004;59(3):252–256. doi: 10.1136/thorax.2003.012658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins F. To beat COVID-19, social distancing is a must. 2020. https://directorsblog.nih.gov/2020/03/19/to-beat-COVID-19-social-distancing-is-a-must/
- Colson P., Rolain J., Lagier J., Brouqui P., Raoult D. Chloroquine and hydroxychloroquine as available weapons to fight COVID-19. Int. J. Antimicrob. Agents. 2020:105932. doi: 10.1016/j.ijantimicag.2020.105932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corman V.M., Muth D., Niemeyer D., Drosten C. Hosts and sources of endemic human coronaviruses. Adv. Virus Res. 2018;100:163–188. doi: 10.1016/bs.aivir.2018.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cortegiani A., Ingoglia G., Ippolito M., Giarratano A., Einav S. A systematic review on the efficacy and safety of chloroquine for the treatment of COVID-19. J. Crit. Care. 2020 doi: 10.1016/j.jcrc.2020.03.005. press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daniyal S. India is enforcing the harshest and most extensive COVID-19 lockdown in the world. 2020. https://qz.com/india/1828915/indias-coronavirus-lockdown-harsher-than-china-italy-pakistan/ (retrieved on 11.04.2020)
- Das K., Paital B. The synergy between philosophy and science, need of the contemporary society. Int. J. Humanities Soc. Sci. Res. 2020;6(1):45–51. [Google Scholar]
- Das K., Paital B. First Week of Social Lockdown versus Medical Care against COVID-19 - with Special Reference to India. Curr. Trend Biotechnol. Pharmacol. 2020;14(2) doi: 10.1016/j.scitotenv.2020.138914. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dogan I. There are at least 75,000 coronavirus infections in India TODAY: 21 days not enough. 2020. https://finance.yahoo.com/news/least-75-000-coronavirus-infections-041207265.html
- Dong L., Hu S., Gao J. Discovering drugs to treat coronavirus disease 2019 (COVID-19) Drug. Discov. Ther. 2020;14(1):58–60. doi: 10.5582/ddt.2020.01012. [DOI] [PubMed] [Google Scholar]
- Doremalen N., Bushmaker T., Morris D.H., Holbrook M.G., Gamble A., Williamson B.N., Tamin A., Harcourt J.L., Thornburg N.J., Gerber S.I., Lloyd-Smith J.O., Wit E., Munster V.J. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020 doi: 10.1056/NEJMc2004973. press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elfiky A.A. Anti-HCV, nucleotide inhibitors, repurposing against COVID-19. Life Sci. 2020;248 doi: 10.1016/j.lfs.2020.117477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emmanuel M. (Coronavirus) Orissa HC directs government to engage specialist doctors, provide personal protective equipment to doctors treating COVID-19. 2020. https://www.barandbench.com/news/litigation/coronavirus-orissa-hc-directs-government-to-engage-specialist-doctors-provide-personal-protective-equipment-to-doctors-treating-COVID-19
- F.D.A. Emergency preparedness and response to coronavirus disease 2019 (COVID-19) 2020. https://www.fda.gov/emergency-preparedness-and-response/mcmissues/coronavirus-disease-2019-COVID-19 (retrieved on 11.04.2020)
- Gandhiok J. Delhi: factories shut, Yamuna water sparkles. 2020. https://m.timesofindia.com/city/delhi/delhi-factories-shut-yamuna-water-sparkles/amp_articleshow/74988548.cms#referrer=https%3A%2F%2Fwww.google.com&_tf=From%20%251%24s
- Gao J., Zhenxue T., Yang X. Breakthrough: chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci. Trends. 2020;14(1):72–73. doi: 10.5582/bst.2020.01047. [DOI] [PubMed] [Google Scholar]
- Gautret P., Lagier J.C., Parola P., Hoang V.T., Meddeb L., Mailhe M., Doudier B., Courjon J., Giordanengo V., Vieira V.E., Dupont H.T., Honoré S., Colson P., Chabrière E., Scola B.L., Rolain J.M., Brouqui P., Raoult D. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents. 2020:105949. doi: 10.1016/j.ijantimicag.2020.105949. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- Giraud-Billoud M., Rivera-Ingraham G.A., Moreira D.C., Burmester T., Castro-Vazquez A., Carvajalino-Fernández J.M., Dafre A., Niu C., Tremblay N., Paital B., Rosa R., Storey J.M., Vega I.A., Zhang W., Yepiz-Plascencia G., Zenteno-Savin T., Storey K.B., Lima M.H. Twenty years of the ‘Preparation for Oxidative Stress’ (POS) theory: ecophysiological advantages and molecular strategies. Comp. Biochem. Physiol. A. 2019;234:36–49. doi: 10.1016/j.cbpa.2019.04.004. [DOI] [PubMed] [Google Scholar]
- Gordon C.J., Tchesnokov E.P., Feng J.Y., Porter D.P., Götte M. The antiviral compound remdesivir potently inhibits RNA-dependent RNA polymerase from Middle East respiratory syndrome coronavirus. J. Biol. Chem. 2020;295(15):4773–4779. doi: 10.1074/jbc.AC120.013056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo Y.R., Cao Q.D., Hong Z.S., Tan Y.Y., Chen S.D., Jin H.J., Tan K.S., Wang D.Y., Yan Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak - an update on the status. Mil. Med. Res. 2020;7(1):11. doi: 10.1186/s40779-020-00240-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Habibzadeh P., Stoneman E.K. The novel coronavirus: a bird’s eye view. Int. J. Occup. Environ. Med. 2020;11(2):65–71. doi: 10.15171/ijoem.2020.1921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hati A.K., Paital B., Naik K.N., Mishra A.K., Chainy G.B.N., Nanda L.K. Constitutional, organopathic and combined homeopathic treatment of benign prostatic hypertrophy: a clinical trial. Homeopathy. 2012;101:217–223. doi: 10.1016/j.homp.2012.08.005. [DOI] [PubMed] [Google Scholar]
- Huang C., Wang Y., Li X., Ren L., Zhao J., Hu Y., Zhang L., Fan G., Xu J., Gu X., Cheng Z., Yu T., Xia J., Wei Y., Wu W., Xie X., Yin W., Li H., Liu M., Xiao Y., Gao H., Guo L., Xie J., Wang G., Jiang R., Gao Z., Jin Q., Wang J., Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ilango S., Priyanka J., Paital B., Padma P.R., Nirmaladevi R. Epigenetic alterations in cancer. Front. Biosci. Landmark Ed. 2020;25:1058–1109. doi: 10.2741/4847. [DOI] [PubMed] [Google Scholar]
- Iswariya G.T., Paital B., Padma P.R., Nirmaladevi R. microRNAs: epigenetic players in cancer and aging. Front. Biosci. Scholar Ed. 2019;11:29–55. doi: 10.2741/S524. [DOI] [PubMed] [Google Scholar]
- Jin Y.H., Cai L., Cheng Z.S., Cheng H., Deng T., Fan Y.P., Fang C., Huang D., Huang L.Q., Huang Q., Han Y., Hu B., Hu F., Li B.H., Li Y.R., Liang K., Lin L.K., Luo L.S., Ma J., Ma L.L., Peng Z.Y., Pan Y.B., Pan Z.Y., Ren X.Q., Sun H.M., Wang Y., Wang Y.Y., Weng H., Wei C.J., Wu D.F., Xia J., Xiong Y., Xu H.B., Yao X.M., Yuan Y.F., Ye T.S., Zhang X.C., Zhang Y.W., Zhang Y.G., Zhang H.M., Zhao Y., Zhao M.J., Zi H., Zeng X.T., Wang Y.Y., Wang X.H., Zhongnan Hospital of Wuhan University Novel Coronavirus Management and Research Team, Evidence-Based Medicine Chapter of China International Exchange and Promotive Association for Medical and Health Care (CPAM) A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version) Mil. Med. Res. 2020;7(1):4. doi: 10.1186/s40779-020-0233-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ko W.C., Rolain J.M., Lee N.Y., Chen P.L., Huang C.T., Lee P.I., Hsueh P.R. Arguments in favor of remdesivir for treating SARS-CoV-2 infections. Int. J. Antimicrob. Agents. 2020:105933. doi: 10.1016/j.ijantimicag.2020.105933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumar A. Coronavirus: WHO lauds Modi government's social outreach during lockdown. 2020. https://www.indiatoday.in/india/story/who-coronavirus-lockdown-india-economic-stimulus-package-1662392-2020-04-02 (retrieved on 11.04.2020)
- Kumar R., Pal R. India achieves WHO recommended doctor population ratio: a call for paradigm shift in public health discourse! J. Family Med. Prim. Care. 2018;7(5):841–844. doi: 10.4103/jfmpc.jfmpc_218_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lai M.M.C., Perlman S., Anderson L.J. Coronaviridae. In: Knipe D.M., Howley P.M., editors. Fields Virology. Lippincott Williams & Wilkins; Philadelphia, PA: 2007. pp. 1305–1335. [Google Scholar]
- Li R., Pei S., Chen B., Song Y., Zhang T., Yang W., Shaman J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2) Science. 2020 doi: 10.1126/science.abb3221. pii: eabb3221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li X., Geng M., Peng Y., Meng L., Lu S. Molecular immune pathogenesis and diagnosis of COVID-19. J. Pharmaceutic. Anal. 2020 doi: 10.1016/j.jpha.2020.03.0011235. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu X., Wang X.J. Potential inhibitors for 2019-nCoV coronavirus M protease from clinically proven medicines. J. Genet. Genomics. 2020;47(2):119–121. doi: 10.1016/j.jgg.2020.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Livemint What Google tells us about lockdown impact in India's biggest cities. 2020. https://www.livemint.com/news/india/what-google-tells-us-about-lockdown-impact-in-india-s-biggest-cities-11585634729068.html
- Livemint How to help the most vulnerable during the COVID-19 lockdown. 2020. https://www.livemint.com/mint-lounge/features/how-to-help-the-most-vulnerable-during-the-COVID-19-lockdown-11585631303316.html (retrieved on 11.04.2020)
- Loutfy M.R., Blatt L.M., Siminovitch K.A., Ward S., Wolff B., Lho H., Pham D.H., Deif H., LaMere E.A., Chang M., Kain K.C., Farcas G.A., Ferguson P., Latchford M., Levy G., Dennis J.W., Lai E.K., Fish E.N. Interferon Alfacon-1 plus corticosteroids in severe acute respiratory syndrome: a preliminary study. J. Am. Med. Assoc. 2003;290(24):3222–3228. doi: 10.1001/jama.290.24.3222. [DOI] [PubMed] [Google Scholar]
- Lu G., Liu D. SARS-like virus in the Middle East: a truly bat-related coronavirus causing human diseases. Protein Cell. 2012;3:803–805. doi: 10.1007/s13238-012-2811-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackay I.M., Arden K.E. MERS coronavirus: diagnostics, epidemiology and transmission. Virol. J. 2015;12:222. doi: 10.1186/s12985-015-0439-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malik M. No curfew like lockdown, PM Imran Khan insists. 2020. https://nation.com.pk/23-Mar-2020/no-curfew-like-lockdown-pm-imran-khan-insists (retrieved on 11.04.2020)
- Mishra P., Paital B., Jena S., Samanta L., Kumar S., Chainy G.B.N., Swain S. Possible activation of NRF2 by vitamin E/curcumin against altered thyroid hormone induced oxidative stress via NFĸB/AKT/mTOR/KEAP1 signaling in rat heart. Sci. Rep. 2019;9(1):7408. doi: 10.1038/s41598-019-43320-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- N.I.H . NIH News Release; 2020. NIH Clinical Trial of Investigational Vaccine for COVID-19 Begins.https://www.nih.gov/news-events/news-releases/nih-clinical-trial-investigational-vaccine-covid-19-begins (retrieved on 12.04.2020) [Google Scholar]
- Naidoo D., Schembri A., Cohen M. The health impact of residential retreats: a systematic review. BMC Complement. Altern. Med. 2018;18(1):8. doi: 10.1186/s12906-017-2078-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Noronha G. World bank approves $1 billion aid to India to fight COVID-19. 2020. https://economictimes.indiatimes.com/news/politics-and-nation/world-bank-approves-1-billion-aid-to-india-to-fight-COVID-19/articleshow/74959070.cms
- P.T.I. India Today COVID-19: Odisha govt to provide Rs 3,000 to 65,000 vendors amid lockdown. 2020. https://www.indiatoday.in/india/story/COVID-19-odisha-govt-to-provide-rs-3-000-to-65-000-vendors-amid-lockdown-1660855-2020-03-29 (retrieved on 11.04.2020)
- P.T.I. India Today Coronavirus: 120 Indians from Iran to reach Jaisalmer today, to be quarantined at Army facility. 2020. https://www.indiatoday.in/india/story/coronavirus-120-indians-from-iran-to-reach-jaisalmer-today-to-be-quarantined-at-army-facility-1654999-2020-03-13 (retrieved on 11.04.2020)
- Paital B., Kumar S., Farmer R., Tripathy N.K., Chainy G.B.N. In silico prediction of 3D structure of superoxide dismutase of Scylla serrata and its binding properties with inhibitors. Interdiscip. Sci. Comput. Life Sci. 2013;5:69–76. doi: 10.1007/s12539-013-0150-4. [DOI] [PubMed] [Google Scholar]
- Paital B., Hati A.K., Naik K.N., Mishra A.K., Nanda L.K., Chainy G.B.N. Re: Editorial comment on constitutional, organopathic and combined homeopathic treatment of begin prostatic hypertrophy: a clinical trial: S. A. Kaplan J Urol 2013; 190: 1818–1819. J. Urol. 2014;193:1–2. doi: 10.1016/j.juro.2014.04.088. [DOI] [PubMed] [Google Scholar]
- Paital B., Panda S.K., Hati A.K., Mohanty B., Mohapatra M.K., Kanungo S., Chainy G.B.N. Longevity of animals under reactive oxygen species stress and disease susceptibility due to global warming. World J. Biol. Chem. 2016;7(1):110–127. doi: 10.4331/wjbc.v7.i1.110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paital B., Hati A.K., Nayak C., Mishra A.K., Nanda L.K. Combined effects of constitutional and organopathic homeopathic medicines for better improvement of benign prostatic hyperplasia cases. Int. J. Clin. Med. Imag. 2017;4(7):1–2. doi: 10.4172/2376-0249.1000574. [DOI] [Google Scholar]
- Paital B., Guru D., Mohapatra P., Panda B., Parida N., Rath S., Kumar V., Saxena P.S., Srivastava A. Ecotoxic impact assessment of graphene oxide on lipid peroxidation at mitochondrial level and redox modulation in fresh water fish Anabas testudineus. Chemosphere. 2019;224:796–804. doi: 10.1016/j.chemosphere.2019.02.156. [DOI] [PubMed] [Google Scholar]
- Panda A. Odisha government's free meal scheme turns into community feast amid coronavirus lockdown. 2020. https://www.newindianexpress.com/states/odisha/2020/apr/03/odisha-governments-free-meal-scheme-turns-into-community-feast-amid-coronavirus-lockdown-2125144.html (retrieved on 11.04.2020)
- Peiris J.S., Chu C.M., Cheng V.C., Chan K.S., Hung I.F., Poon L.L., Law K.I., Tang B.S., Hon T.Y., Chan C.S., Chan K.H., Ng J.S., Zheng B.J., Ng W.L., Lai R.W., Guan Y., Yuen K.Y., HKU/UCH SARS Study Group Clinical progression and viral load in a community outbreak of coronavirus-associated SARS pneumonia: a prospective study. Lancet. 2003;361(9371):1767–1772. doi: 10.1016/s0140-6736(03)13412-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raja M., Nayak C., Paital B., Rath P., Moorthy K., Raj S., Hati A.K. Randomized trial on weight and lipid profile of obese by formulation from Garcina cambogia. Med. Sci. 2020;24(103):1000–1009. [Google Scholar]
- Rasheed Z., Allahoum R., Siddiqui U. Trump extends US social distancing until April 30: live updates. 2020. https://www.aljazeera.com/news/2020/03/trump-weighs-coronavirus-lockdown-york-live-updates-200328234401911.html
- Roth D.B. V(D)J recombination: mechanism, errors, and Fidelity. Microbiol Spectr. 2014;2(6) doi: 10.1128/microbiolspec.MDNA3-0041-2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Science News COVID-19 coronavirus epidemic has a natural origin. 2020. https://www.sciencedaily.com/releases/2020/03/200317175442.htm (retrieved on 10.04.2020)
- Scripps Research Institute COVID-19 coronavirus epidemic has a natural origin. Coronavirus illustration (stock image) 2020. https://stock.adobe.com (retrieved on 12.04.2020)
- Sharma S. Lockdown in India was early, far-sighted and courageous': WHO envoy. 2020. https://www.hindustantimes.com/india-news/lockdown-in-india-was-early-this-was-far-sighted-courageous-move-who-special-envoy-on-COVID-19/story-wNdCkNVOqV5gCN8Du9jJ3N.html
- She J., Jiang J., Ye L., Hu L., Bai C., Song Y. 2019 novel coronavirus of pneumonia in Wuhan, China: emerging attack and management strategies. Clin. Transl. Med. 2020;9(1):19. doi: 10.1186/s40169-020-00271-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shereen M.A., Khan S., Kazmi A., Bashir N., Siddique R. COVID-19 infection: origin, transmission, and characteristics of human coronaviruses. J. Adv. Res. 2020;24:91–98. doi: 10.1016/j.jare.2020.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith T., Bushek J., Prosser T. COVID-19 drug therapy – potential options, clinical drug information|clinical solutions. 2020. https://www.elsevier.com/__data/assets/pdf_file/0007/988648/COVID-19-Drug-Therapy_Mar-2020.pdf
- Suffian M. COVID-19 crisis: Odisha businessman feeds starving families of migrant workers returning to UP, Bihar. 2020. https://www.indiatoday.in/india/story/coronavirus-odisha-businessman-food-starving-families-migrant-workers-1661934-2020-03-31 (retrieved on 10.04.2020)
- T.E.T Centre gives Rs 11,092 crores to states from disaster management fund. 2020. https://economictimes.indiatimes.com/news/politics-and-nation/centre-gives-rs-11092-crores-to-states-from-disaster-management-fund/articleshow/74970730.cms?from=mdr (retrieved on 10.04.2020)
- T.G.I Bangladesh declares 10 days of holiday to curb coronavirus spread, the tele graph India. 2020. https://www.telegraphindia.com/world/bangladesh-declares-10-days-of-holiday-to-curb-coronavirus-spread/cid/1758388
- The Morning Last train to leave at 4 p.m. from Colombo. 2020. http://www.themorning.lk/last-train-to-leave-at-4-p-m-from-colombo/?fbclid=IwAR3f9iua2z2gHYrr0j1FMAxXwx8zFZShnARSLKpIitazrJpDS4qyhL55lWs (retrieved on 10.04.2020)
- Tripathi R. Strictly enforce lockdown: Centre to states. 2020. https://economictimes.indiatimes.com/news/politics-and-nation/strictly-enforce-lockdown-centre-to-states/articleshow/74784848.cms?from=mdr (retrieved on 10.04.2020)
- Vellingiri B., Jayaramayya K., Iyer Narayanasamy A., Govindasamy V., Giridharan B., Ganesan S., Venugopal A., Venkatesan D., Ganesan H., Rajagopalan K., Rahman P.K.S.M., Cho S.G., Kumar N.S., Subramaniam M.D. COVID-19: a promising cure for the global panic. Sci. Total Environ. 2020;725:138277. doi: 10.1016/j.scitotenv.2020.138277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- W.H.O World Health Organization. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected. 2020. https://www.who.int/publicationsdetail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected
- W.H.O Report of the WHO-China joint mission on coronavirus disease 2019 (COVID-19) 2020. https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-COVID-19-final-report.pdf
- W.H.O Rolling updates on coronavirus disease (COVID-19) 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (retrieved on 10.04.2020)
- Wang M., Cao R., Zhang L., Yang X., Liu J., Xu M., Shi Z., Hu Z., Zhong W., Xiao G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020;30:269–271. doi: 10.1038/s41422-020-0282-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang Q., Zhang Y., Wu L., Niu S., Song C., Zhang Z., Lu G., Qia C., Hu Y., Yuen N.Y., Wang O., Zhou H., Yan J., Qi J. Structural and functional basis of SARS-CoV-2 entry by using human ACE2. Cell. 2020 doi: 10.1016/j.cell.2020.03.0452020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wit E., Feldmann F., Cronin J., Jordan R., Okumura A., Thomas T., Scott D., Cihlar T., Feldmann H. Prophylactic and therapeutic remdesivir (GS-5734) treatment in the rhesus macaque model of MERS-CoV infection. Proc. Natl. Acad. Sci. U. S. A. 2020;117(12):6771–6776. doi: 10.1073/pnas.1922083117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woo P.C., Lau S.K., Lam C.S., Lai K.K., Huang Y., Lee P., Luk G.S., Dyrting K.C., Chan K.H., Yuen K.Y. Comparative analysis of complete genome sequences of three avian coronaviruses reveals a novel group 3c coronavirus. J. Virol. 2009;83:908–917. doi: 10.1128/JVI.01977-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Bank Hospital beds (per 1,000 people) 2020. https://data.worldbank.org/indicator/sh.med.beds.zs (retrieved on 10.04.2020)
- Wright R. The world's largest coronavirus lockdown is having a dramatic impact on pollution in India. 2020. https://edition.cnn.com/2020/03/31/asia/coronavirus-lockdown-impact-pollution-india-intl-hnk/index.html (retrieved on 10.04.2020)
- Xu X., Han M., LI T. 2020. Effect Treatment of Severe COVID-19 Patients With Tocilizumab. (ChinaXiv.20200300026.v1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yao T.T., Qian J.D., Zhu W.Y., Wang Y., Wang G.Q. A systematic review of lopinavir therapy for SARS coronavirus and MERS coronavirus-a possible reference for coronavirus disease-19 treatment option. J. Med. Virol. 2020 doi: 10.1002/jmv.25729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yao X., Ye F., Zhang M., Cui C., Huang B., Niu P., Liu X., Zhao L., Dong E., Song C., Zhan S., Lu R., Li H., Tan W., Liu D. In vitro antiviral activity and projection of optimized dosing design of hydroxychloroquine for the treatment of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Clin. Infect. Dis. 2020:ciaa237. doi: 10.1093/cid/ciaa237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu P., Hu B., Shi Z.L., Cui J. Geographical structure of bat SARS-related coronaviruses. Infect. Genet. Evol. 2019;69:224–229. doi: 10.1016/j.meegid.2019.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zaveri K. Unhealthy lifestyle and Indian ethnicity tied to hypertension. 2019. https://www.forbesindia.com/article/doctors-voice/unhealthy-lifesstyle-and-indian-ethnicity-tied-to-hypertension/55909/1
- Zhong R., Mozur P., Tame T.Y.T. The New Yorks Times; 2020. Coronavirus, Mao-style Social Control Blankets China.https://www.nytimes.com/2020/02/15/business/china-coronavirus-lockdown.html (retrieved on 10.04.2020) [Google Scholar]
- Zhou F., Yu T., Du R., Fan G., Liu Y., Liu Z., Xiang J., Wang Y., Song B., Gu X., Guan L., Wei Y., Li H., Wu X., Xu J., Tu S., Zhang Y., Chen H., Cao B. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi: 10.1016/S0140-6736(20)30566-3. 1038. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Inter nation social lockdown versus medical care against COVID-19, a mild environmental insight with special reference to India Biswaranjan Paital1,*, Kabita Das2, Sarat Kumar Parida31Redox Regulation Laboratory, Department of Zoology, Odisha University of Agriculture and Technology, College of Basic Science and Humanities, Bhubaneswar-751003, India, 2Post Graduate Department of Philosophy, Utkal University, VaniVihar, Bhubaneswar, India, 3Department of Nephrology, Srirama Chandra Bhanja Medical College and Hospital, Mangalabag, Cuttack, Odisha, India.