

Abstract
Purpose. A new strain of H1N1 influenza, also known as swine flu was confirmed in the UK in May 2009 and has spread to over 100 countries around the world causing the World Health Organization to declare a global flu pandemic. The primary objectives of this review are to identify the key demographic and attitudinal determinants of three types of protective behaviour during a pandemic: preventive, avoidant, and management of illness behaviours, in order to describe conceptual frameworks in which to better understand these behaviours and to inform future communications and interventions in the current outbreak of swine flu and subsequent influenza pandemics.
Methods. Web of Science and PubMed databases were searched for references to papers on severe acute respiratory syndrome, avian influenza/flu, H5N1, swine influenza/flu, H1N1, and pandemics. Forward searching of the identified references was also carried out. In addition, references were gleaned from an expert panel of the Behaviour and Communications sub‐group of the UK Scientific Pandemic Influenza Advisory Group. Papers were included if they reported associations between demographic factors, attitudes, and a behavioural measure (reported, intended, or actual behaviour).
Results. Twenty‐six papers were identified that met the study inclusion criteria. The studies were of variable quality and most lacked an explicit theoretical framework. Most were cross‐sectional in design and therefore not predictive over time. The research shows that there are demographic differences in behaviour: being older, female and more educated, or non‐White, is associated with a higher chance of adopting the behaviours. There is evidence that greater levels of perceived susceptibility to and perceived severity of the diseases and greater belief in the effectiveness of recommended behaviours to protect against the disease are important predictors of behaviour. There is also evidence that greater levels of state anxiety and greater trust in authorities are associated with behaviour.
Conclusions. The findings from this review can be broadly explained by theories of health behaviour. However, theoretically driven prospective studies are required to further clarify the relationship between demographic factors, attitudes, and behaviour. The findings suggest that intervention studies and communication strategies should focus on particular demographic groups and on raising levels of perceived threat of the pandemic disease and belief in the effectiveness of measures designed to protect against it.
In the face of an outbreak of pandemic influenza, it is important to understand factors that influence how people behave in order to decrease the likelihood of infection, transmission, and disease severity. This understanding can inform communication strategies aimed at minimizing the impact and spread of the disease. The aim of this review is to place empirical research findings within conceptual frameworks which can facilitate the synthesis of these findings and their application to policy and practice. The diseases covered in this review are included due to their pandemic or potential pandemic status. They are all respiratory type diseases.
Severe acute respiratory syndrome (SARS) is a respiratory disease caused by the SARS coronavirus. A near pandemic occurred between November 2002 and July 2003, where the disease spread from China to 37 countries around the world. Avian influenza refers to the highly pathogenic influenza A (HPAI) virus subtype H5N1 virus that is of concern globally as a potential pandemic threat. Since the first H5N1 outbreak occurred in 1997, there have been an increasing number of HPAI H5N1 bird‐to‐human transmissions leading to clinically severe and fatal human infections. A new strain of H1N1 influenza, also known as swine flu was confirmed in the UK in May 2009 and has spread to over 100 countries around the world causing the World Health Organization to declare a global flu pandemic. Such diseases have far reaching effects due to their ease of transmission and they can lead to both health and economic costs due to absenteeism and reduced or changed commercial activity.
Protective behaviours carried out in response to an influenza pandemic can be broadly classified into three types: preventive, avoidant, and management of disease behaviours. Preventive behaviours include hygiene behaviours (such as hand washing, coughing or sneezing into a hand or tissue, cleaning surfaces); mask wearing and uptake of vaccinations. Avoidant behaviours include avoiding crowds, public transport, and work and compliance with quarantine restrictions. Management of disease behaviours include taking antiviral medication, seeking help from a professional and use of telephone or Internet help lines. Some of these behaviours are the responsibility of the individual to carry out whereas others are decreed by law (e.g., quarantine laws in Singapore during the 2003 SARS outbreak).
Method
Search strategy
Web of Science and PubMed databases were searched for references to papers on SARS, avian influenza/flu, H5N1, swine influenza/flu, H1N1, and pandemics since 2002. Forward searching of the identified references was also carried out. In addition, references were obtained from an expert panel of the Behaviour and Communications sub‐group of the UK Scientific Pandemic Influenza Advisory Group.
Screening
Titles and abstracts were screened against the inclusion criteria.
Eligibility criteria
The eligibility criteria for inclusion in this study were:
-
1
Population: general population (excluding patient groups, healthcare workers).
-
2
Behaviour: preventive, avoidant, or management of pandemic disease behaviours. Studies about avian influenza risk which focus solely on the handling of chickens or food consumption are not included, as they are less relevant to the hygiene and avoidance behaviour for protection against other pandemic influenzas. Studies of uptake of influenza vaccinations were excluded if they were not carried out in the context of a pandemic outbreak.
-
3
Psychological variables and demographic characteristics had to be included and associations between these and behaviours (reported, intended, or actual behaviour) reported.
-
4
Date: published after 2002 (when SARS emerged as a pandemic).
-
5
Language: published in the English language.
Analysis plan
The analysis began with three broad categories of behaviour which are relevant during a pandemic in terms of the protection which they confer on an individual or society – i.e., preventive, avoidant, or management of disease behaviours. For each identified study the behaviours investigated were classified into one of these categories. Following this, the attitudinal and demographic factors which were assessed in each study were recorded. Finally, associations between these factors and each category of behaviour were examined. This analysis formed the basis of the three conceptual maps (detailed in 1, 2, 3).
Figure 1.

Factors associated with carrying out preventive behaviours.
Figure 2.

Factors associated with carrying out avoidant behaviours.
Figure 3.

Factors associated with carrying out management of disease behaviours.
Results
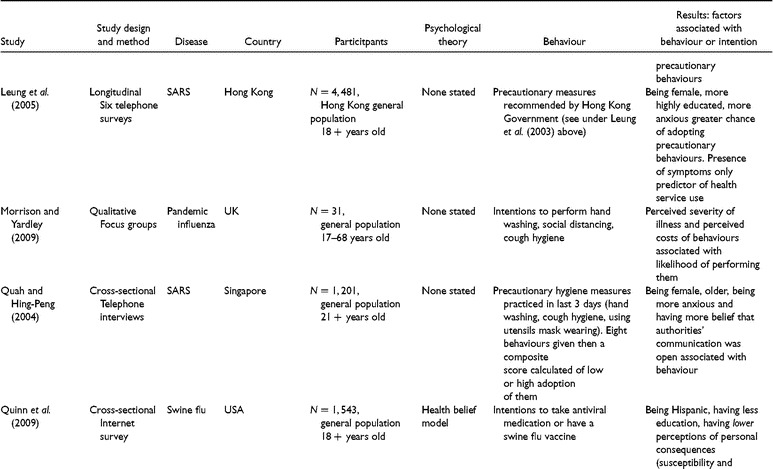
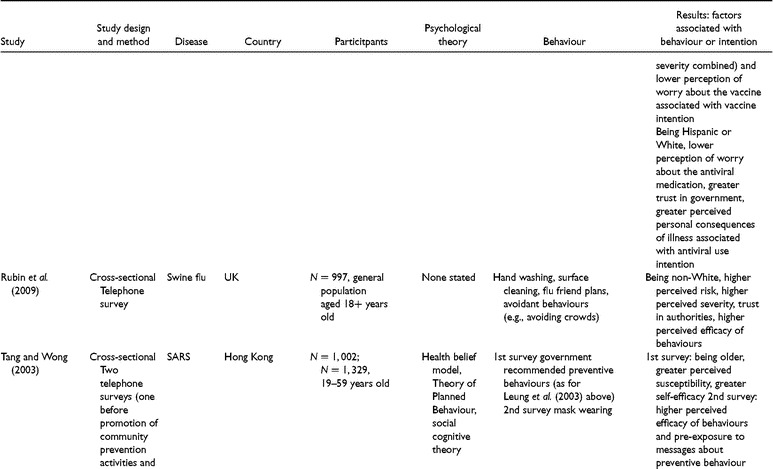
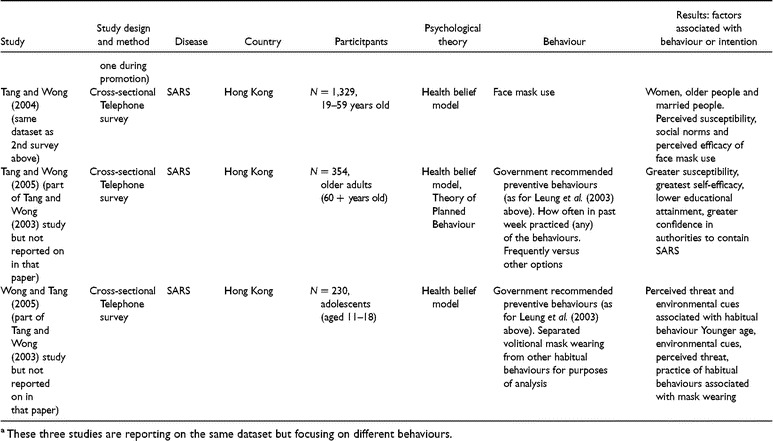
Twenty‐six papers met the inclusion criteria; comprising twenty different studies (see Table 1). The studies were heterogeneous, being carried out in different countries with differing populations. Most of the research was carried out in the middle of an outbreak; however, six studies focused on intentions to behave in the event of an outbreak. The results from these studies were similar and are therefore reported together in this review. The studies were of variable quality. Few were based on an explicit theoretical framework (N=3). Nearly, all (N=24) were cross‐sectional in design. Few studies examined the mediating role of attitudes and beliefs in the relationship between demographic factors and behaviour (N=3). Most studies concentrated on factors associated with carrying out preventive behaviours (N=22) rather than avoidant (N=13) or management of disease behaviours (N=10). 1,
Table 1.
Summary of studies included in review

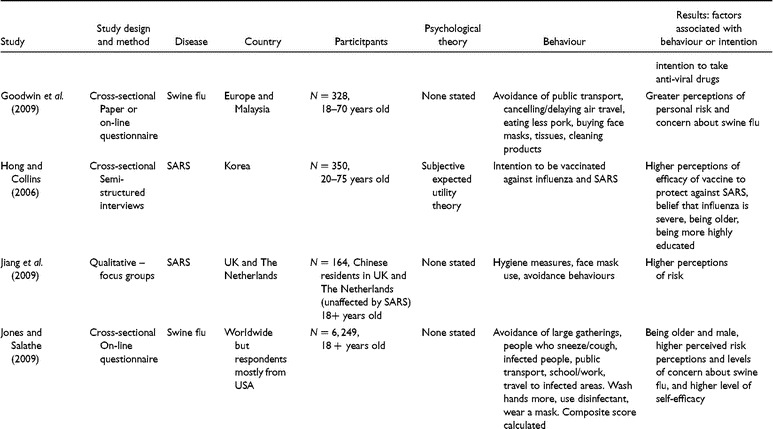


This review investigates the influence of demographic and psychological variables on protective behaviours that are key to reducing the spread and impact of pandemic influenza. Figures 1–3 illustrate these associations.
The association between demographic factors and protective behaviours
Age
Cross‐sectional studies carried out in Singapore and Hong Kong examining the influence of age on behaviours to protect against SARS have found that older people are more likely to adopt precautionary behaviours (Lau, Yang, Tsui, & Kim, 2003; Leung et al., 2003, 2004, 2005; Quah & Hin‐Peng, 2004; Tang & Wong, 2003, 2004). The behaviours included hand washing, respiratory hygiene, mask wearing, using utensils, and washing after touching contaminated surfaces. An Internet survey carried out during the beginning of the H1N1 swine flu outbreak found that older age was associated with more frequent hand washing (Jones & Salathe, 2009). Older people are more likely to say they intend to be vaccinated against influenza during an outbreak of SARS (Hong & Collins, 2006). Older people have also been found to be more likely to report that they would take self‐protective behaviours in the event of an outbreak of avian influenza (Lau, Kim, Tsui, & Griffiths, 2007a) or an influenza pandemic in the future (Barr et al., 2008). Research by Barr et al. (2008) may explain the association between older age and behaviour in that they found that older people feel more susceptible to being affected by a possible influenza pandemic. In the context of the threat of the 2009 swine flu pandemic, the pattern of results for age was different, with people aged 18–24 more likely to follow recommended behaviours (hand washing more, cleaning surfaces more, and having plans for a flu friend 2, ) than older people (Rubin, Amlôt, Page, & Wessely, 2009). A cross‐sectional study of adolescents in Hong Kong during the SARS outbreak found that younger adolescents were more likely to report mask wearing (Wong & Tang, 2005).
In contrast, a cross‐sectional study in The Netherlands (where no cases of SARS had been found) did not find any association between age and carrying out precautionary behaviour (Brug et al., 2004). Three studies carried out in the Australia, Hong Kong, and the USA found no influence of age on intentions to have a vaccination or actual uptake of the vaccination (Eastwood et al., 2009; Lau, Kim, Tsui, & Griffiths, 2008; Quinn, Kumar, Freimuth, Kidwell, & Musa, 2009).
Older people were more likely to avoid public places during the SARS outbreak (Lau et al., 2003) and to report that they would avoid crowds in the event of an avian flu outbreak (Lau et al., 2007a). An Internet survey carried out at the beginning of the swine flu outbreak also found that older age was associated with more avoidant behaviours, such as avoiding large gatherings, infected people, and public transport (Jones & Salathe, 2009). In contrast studies with cross border and air travellers in Hong Kong found no association between age and avoidance behaviour (Lau, Yang, Tsui, & Pang, 2004; Lau, Yang, Tsui, Pang, & Kim, 2004). Similarly, an Australian study found no association between age and intentions to comply with quarantine (Eastwood et al., 2009).
The pattern of findings for age is not straightforward. Whilst the balance of evidence shows that increasing age is associated with a greater chance of carrying out behaviours, some results are inconclusive.
Gender
Cross‐sectional studies carried out in Hong Kong and Singapore have found that women are more likely than men to adopt precautionary behaviours to protect against SARS (Lau et al., 2003; Lau, Yang, Tsui, & Pang, 2004; Leung et al., 2003, 2004; Quah & Hin‐Peng, 2004; Tang & Wong, 2004) including hand washing, respiratory hygiene, mask wearing, using utensils, and washing after touching contaminated surfaces. This result was also found in a longitudinal study carried out in Hong Kong (Leung et al., 2005). In the UK, women were also more likely than men to follow recommended behaviours in the face of a swine flu pandemic (hand washing more, cleaning surfaces more, and having plans for a flu friend; Rubin et al., 2009). In addition, an Internet survey found that women were more likely than men to report increased hand‐washing at the beginning of the swine flu pandemic (Jones & Salathe, 2009). This association between gender and behaviour may be because women have been found to perceive themselves as more susceptible, for example to SARS, than men do (Brug et al., 2004). In contrast, there were no gender differences found in one Australian study for intentions to wear a mask (Barr et al., 2008) or actual face mask use in studies carried out in The Netherlands and Hong Kong (Brug et al., 2004; Tang & Wong, 2004; Wong & Tang, 2005). In addition, no gender differences were found in intentions to be vaccinated (Hong & Collins, 2006; Quinn et al., 2009).
Women were found, in an Australian cross‐sectional study, which asked about intentions in the event of a future pandemic, to be more likely than men to report that they would comply with home quarantine restrictions (Eastwood et al., 2009). An Internet survey carried out with mainly American respondents at the beginning of the swine flu outbreak found that women were more likely than men to carry out avoidant behaviours (Jones & Salathe, 2009). However, in contrast, in the UK women were no more likely than men to avoid crowds and public places (Rubin et al., 2009).
The pattern of results here shows that when there is a significant difference women are consistently more likely than men to carry out the behaviours. However, a proportion of studies do not find any gender differences.
Ethnicity
Few studies have examined the association between ethnicity and behaviour during a pandemic. This may be due to the study samples being homogenous ethnically, ethnicity being poorly recorded, or the question being seen as not important. A UK study found that participants from non‐White ethnic backgrounds were more likely than White participants to take protective action and to adopt avoidant behaviours (e.g., avoiding large crowds or public transport; Rubin et al., 2009). A cross‐sectional study in the USA found that Hispanic respondents were more likely than Black or White respondents to say they would have a vaccine for swine flu and additionally Hispanic and White respondents were more likely than Black respondents to say that they would take an antiviral drug (Quinn et al., 2009). An Australian cross‐sectional study found that those individuals who spoke a language other than English in the home were less likely to say they would wear a mask, be vaccinated or quarantined in the event of an outbreak of pandemic flu (Barr et al., 2008). In contrast, a study carried out in Singapore (Quah & Hin‐Peng, 2004) found no association between ethnicity and precautionary behaviour. There is insufficient evidence to draw any firm conclusions about associations between ethnicity and pandemic‐related behaviours.
Educational level/working status
Cross‐sectional studies carried out in Hong Kong have found that those with more education are more likely to adopt precautionary behaviours to protect against SARS (Leung et al., 2003, 2004, 2005; Tang & Wong, 2004) and avian influenza (Lau et al., 2007a). The behaviours included hand washing, respiratory hygiene, mask wearing, using utensils, and washing after touching contaminated surfaces. Research in Australia found that more highly educated people reported a greater intention to wear a face mask in the event of pandemic influenza (Barr et al., 2008). More highly educated people in Australia in the event of pandemic influenza and in Korea during a SARS outbreak have been found to report that they intend to be vaccinated against influenza (Barr et al., 2008; Hong & Collins, 2006).
In contrast, in Hong Kong a cross‐sectional study of older adults found that those with lower educational attainment were more likely to carry out protective behaviours (Tang & Wong, 2005). In addition, in the USA a cross‐sectional study found that less educated people were more likely to say that they would be willing to be vaccinated against swine flu (Quinn et al., 2009).
However, other studies carried out in Hong Kong and The Netherlands found no association between educational level and reported mask wearing or hand‐washing (Lau, Yang, Tsui, & Pang, 2004; Lau, Yang, Tsui, Pang, & Kim, 2004; Tang & Wong, 2003).
The relationship between educational level and avoidant behaviour is not clear. Some research in the UK during the swine flu pandemic has found that people who were not working, poorer or who had no educational qualifications were more likely to adopt avoidant behaviours (e.g., avoiding large crowds or public transport; Rubin et al., 2009), whereas other studies carried out in Hong Kong have found that more educated people were more likely to avoid public places during the SARS outbreak (Lau et al., 2003; Leung et al., 2003). In addition, two studies in Hong Kong with cross border and air travellers found no association between educational level and avoiding crowds (Lau, Yang, Tsui, & Pang, 2004; Lau, Yang, Tsui, Pang, & Kim, 2004). In Australia, a cross‐sectional study of intention to comply with quarantine restrictions in the event of pandemic influenza found that more highly educated people were more likely to report intended compliance (Barr et al., 2008). Also in Australia it has been found that individuals who are employed but not able to work from home are less likely to report intended compliance with quarantine restrictions (Eastwood et al., 2009).
On the whole then, more educated people are likely to take protective and avoidant behaviour, but some results are inconclusive.
Marital status
The influence of marital status is not examined in many studies. However, one cross‐sectional study in Hong Kong found married people to be more likely to wear face masks to protect themselves against SARS (Tang & Wong, 2004) and another, also carried out in Hong Kong, found that married people were more likely to report that they would comply with quarantine policies in the event of an outbreak of avian influenza (Lau et al., 2007a).
In contrast, other studies have found no influence of marital status on reported mask wearing or hand washing and other precautionary behaviours (Lau, Yang, Tsui, & Pang, 2004; Lau, Yang, Tsui, Pang, & Kim, 2004; Lau et al., 2008; Leung et al., 2003, 2004) or vaccination uptake (Lau et al., 2008). The association between marital status and behaviour is therefore inconclusive.
Psychological factors associated with carrying out the behaviours
Perceived susceptibility to the disease
Associations between perceptions of risk and carrying out preventive behaviours have been found in studies conducted in the UK, Hong Kong, Korea, Australia, and The Netherlands. The following types of assessment were classified as representing perceptions of susceptibility: concern about developing disease, worry about developing disease, estimates of risk, likelihood of developing disease, and chances of disease. Some studies in addition to assessing personal perceived susceptibility also include an assessment of the association between perceived susceptibility of an individual's family to developing the disease and behaviour (e.g., Lau, Kim, Tsui, & Griffiths, 2007b). Associations between greater perceived risk and likelihood of hand washing (Brug et al., 2004; Jones & Salathe, 2009; Lau et al., 2003; Rubin et al., 2009; Tang & Wong, 2003); good personal hygiene (Tang & Wong, 2005; Wong & Tang, 2005) disinfecting the home (Lau et al., 2003; Rubin et al., 2009; Wong & Tang, 2005) mask wearing (Lau, Yang, Tsui, & Pang, 2004; Lau, Yang, Tsui, Pang, & Kim, 2004; Tang & Wong, 2003; Wong & Tang, 2005); building up body immunity with diet and exercise (Tang & Wong, 2005; Wong & Tang, 2005); being vaccinated (Barr et al., 2008) and adopting other precautionary behaviours to protect against SARS including hand washing, respiratory hygiene, mask wearing, using utensils, and washing after touching contaminated surfaces (Barr et al., 2008; Leung et al., 2003, 2004) have been found. In contrast, no relationship was found between perceived susceptibility to avian flu and hand washing in one study (Lau et al., 2007b) and between perceived likelihood of contracting SARS and carrying out precautionary behaviour (Leung et al., 2005; Quah & Hin‐Peng, 2004).
Greater perceived susceptibility to developing SARS is associated with avoidant behaviour. For example, avoiding public places, restaurants, shops, public events, and avoiding people who had travelled to countries with high incidence of SARS (Blendon, Benson, DesRoches, Raleigh, & Taylor‐Clark, 2004; Brug et al., 2004; Lau, Yang, Tsui, & Pang, 2004; Lau et al., 2003). In Australia, a cross‐sectional study found that individuals with greater perceptions of the risk of pandemic influenza were more likely to report an intention to comply with quarantine restrictions (Barr et al., 2008). In the UK, a relationship was found between a greater perceived susceptibility to swine flu and avoiding public places (Rubin et al., 2009) and in Canada, between a greater perceived risk of contracting or spreading SARS and higher compliance with quarantine restrictions (Cava, Fay, Beanlands, McCay, & Wignall, 2005). A cross‐sectional study carried out in Europe and Malaysia in the early weeks of the swine flu pandemic found that those individuals who perceived themselves to be at risk of developing swine flu were more likely to say that they had reduced their use of public transport, or cancelled or delayed their air travel plans (Goodwin, Haque, Neto, & Myers, 2009). Similarly, an Internet survey carried out at the beginning of the swine flu outbreak found that those with higher perceptions of their risk of developing swine flu were more likely to have carried out avoidant behaviours (Jones & Salathe, 2009). A qualitative study carried out in the UK and The Netherlands with Chinese residents found that perceptions of susceptibility were associated with their use of avoidance behaviours during the outbreak of SARS in China (despite their not being in an at risk country; Jiang et al., 2009).
Those individuals in the USA and Canada who perceived themselves to be more susceptible to SARS were found to be more likely to have consulted a health professional or a website for information than those who perceived themselves to be less susceptible (Blendon et al., 2004).
Perceived severity of disease
Constructs of perceived severity as assessed in the studies included the chances of dying from the disease and its infectivity. In the UK, a cross‐sectional study showed that those who felt that swine flu was more severe were more likely to report carrying out hand washing, disinfecting, and arranging a flu friend behaviours (Rubin et al., 2009). Travellers between Hong Kong and mainland China who thought that SARS was fatal were more likely to wear masks (Lau, Yang, Tsui, & Pang, 2004; Lau, Yang, Tsui, Pang, & Kim, 2004) and those who believed that SARS was under control were found to be less likely to wear a mask (Lau et al., 2003). A belief that avian flu might be worse than SARS was found to be associated with influenza vaccination uptake and mask wearing in Hong Kong (Lau et al., 2008). A belief that influenza was severe in terms of being extremely risky was found to be related to intentions to be vaccinated (Hong & Collins, 2006). A qualitative UK study found that participants agreed that if something was very serious then they would implement all the infection control recommendations, if it was a matter of life and death (Morrison & Yardley, 2009).
However, other studies did not find a relationship between the likelihood of surviving SARS on the adoption of precautionary behaviours amongst Hong Kong residents (Leung et al., 2003, 2005; Tang & Wong, 2004) or of the likelihood of wearing face masks (Tang & Wong, 2004).
A belief that avian flu would have high fatality rates and have a greater impact on individuals than SARS was associated with more avoidance behaviours (not going out, keeping children off school, avoiding crowds, avoiding hospitals, and travelling) in cross‐sectional studies carried out in Hong Kong (Lau, Yang, Tsui, & Pang, 2004; Lau et al., 2007a). A relationship has been found between avoidant behaviours (such as avoiding large crowds and public transport) and a higher perceived severity of swine flu (Rubin et al., 2009).
Perceived efficacy of behaviour
Perceived efficacy of behaviour was assessed in the studies by how far the respondents felt that the behaviour would protect them from disease. In a UK study, an association has been found between the perceived efficacy of preventive behaviours (hand washing, making flu friend plans, cleaning surfaces) in protecting against swine flu and reports of having carried these out (Rubin et al., 2009).
Studies amongst Hong Kong residents, cross border travellers and air travellers have found a relationship between the perceived efficacy of mask wearing to protect against SARS and a greater likelihood of carrying out this behaviour (Lau, Yang, Tsui, & Pang, 2004; Lau, Yang, Tsui, Pang, & Kim, 2004; Lau et al., 2003; Tang & Wong, 2003). A relationship has also been found between efficacy of face mask use and reported intentions to wear one in the event of an avian influenza pandemic (Lau et al., 2007a).
Other research carried out in Hong Kong has found a relationship between perceived efficacy of disinfecting the home and frequent hand washing in protecting against SARS and the carrying out of these behaviours (Lau et al., 2003). In addition, other research has found a relationship between the efficacy of hand washing and the reported likelihood that people would do this if avian influenza occurred (Lau et al., 2007a). Regarding influenza vaccination, two studies have shown a relationship between a belief that influenza vaccination would protect against avian flu and uptake of vaccination (Lau et al., 2008) and a belief that influenza vaccination would protect against SARS and uptake of vaccination (Hong & Collins, 2006).
In contrast, a cross‐sectional study of older adults in Hong Kong did not find any association between the perceived efficacy of precautionary behaviours and having carried these out (Tang & Wong, 2005).
A relationship has been found in the UK between the perceived efficacy of avoidant behaviours in protecting against swine flu and individuals reporting having carried them out (Rubin et al., 2009). An association has been found in Hong Kong between a belief that avoiding public places was effective in protecting against SARS and doing this (Lau, Yang, Tsui, & Pang, 2004; Lau et al., 2003) and a belief that face mask wearing is efficacious and compliance with quarantine (Lau et al., 2007a).
Perceived costs of behaviours
The influence of the perceived barriers to behaviours on carrying them out has not been examined in many studies. This may be due to an assumption that the recommended preventive behaviours are fairly easy to carry out. This construct was assessed by examining practical barriers to behaviour such as it being time consuming and also fear of side effects of vaccines and medication. In a UK qualitative study, it was found that people thought there would be barriers to carrying out recommended behaviours, such as there not being anywhere to dispose of tissues, or that they would forget to wash their hands, or lack of space to keep away from other people and that these barriers might influence how likely they would be to carry out the behaviours in the event of a pandemic (Morrison & Yardley, 2009).
A cross‐sectional study carried out in the USA found that those people who were more worried about the side effects and safety of a vaccine or antiviral medication were less likely to say they would be willing to have the vaccine or take the medication (Quinn et al., 2009). A relationship has been found in an Australian study between fear of the side effects of anti‐viral medication and the reported likelihood of compliance with the treatment regime (Eastwood et al., 2009).
In contrast, perceptions of barriers to carrying out precautionary behaviour during the SARS outbreak, such as it being time consuming, was not found to be associated with behaviour by two studies (Tang & Wong, 2004, 2005).
Perceived self‐efficacy
Perceived self‐efficacy was assessed in the studies by asking respondents to indicate the degree with which they felt they were capable of carrying out the behaviours required. Cross‐sectional studies carried out in Hong Kong with adults, older adults, and adolescents found that a greater perceived self‐efficacy to carry out precautionary behaviours and to wear masks was associated with undertaking these behaviours (Tang & Wong, 2003, 2004, 2005). In contrast, a study carried out with adolescents in Hong Kong found no association between perceived self‐efficacy and their having carried out precautionary behaviours (Wong & Tang, 2005).
An Internet survey carried out with mainly American respondents found that those who had greater confidence in their ability to avoid infection were more likely to have carried out avoidant behaviour to reduce their risk of developing swine flu (Jones & Salathe, 2009).
Social norms
Social pressure (in terms of what people think is expected of them by authority and family) has been shown to be associated with mask wearing during the outbreak of SARS (Tang & Wong, 2004), and of other recommended behaviours (good personal hygiene, keeping home clean, and building up body immunity) amongst adolescents (Wong & Tang, 2005). A qualitative Canadian study found an association between social pressure to comply with quarantine and carrying out this behaviour (Cava et al., 2005).
Cues to action
Cues to action incorporated both internal cues (such as bodily symptoms) and also external cues (such as mass media campaigns). It has been found in studies carried out in Hong Kong that individuals who had experienced symptoms that could be an indication of infection with SARS were more likely to adopt precautionary behaviours (e.g., hand washing, respiratory hygiene, etc.; Leung et al., 2003). A longitudinal study carried out in Hong Kong found that presence of symptoms was the best predictor of health service use (Leung et al., 2005).
State anxiety
Studies carried out in Hong Kong and Singapore have found that individuals with higher levels of general anxiety (as measured by the State‐Trait Anxiety Inventory; Spielberger, Edwards, Lushene, Montuori, & Platzek, 1973) are more likely to adopt recommended precautionary behaviours to protect against SARS such as hand washing, cough hygiene, mask wearing, using utensils, and washing after touching contaminated surfaces (Leung et al., 2003, 2004; Quah & Hin‐Peng, 2004). The finding that higher anxiety is associated with a greater chance of uptake of precautionary behaviours was also observed in a longitudinal study carried out in Hong Kong (Leung et al., 2005).
Perceptions about communications from authority
It has been found that those individuals in Singapore who believed that the authorities were open with their communication were more likely to carry out precautionary behaviours. These included covering the mouth with bare hand when sneezing or coughing, washing hands after sneezing, coughing, or clearing nose; using soap or liquid hand‐wash when washing hands; wearing a mask; using serving utensils for shared food; taking preventive measures when touching objects; washing hands after touching objects (Quah & Hin‐Peng, 2004). In addition, those with greater trust in authorities to contain the spread of SARS and swine flu were more likely to adopt precautionary behaviours (Tang & Wong, 2005) and avoidant behaviours (Rubin et al., 2009) and accept antiviral medication (Quinn et al., 2009). A Canadian qualitative study found that inconsistent information from authorities lead to individuals questioning the credibility of the information available and this affected their compliance with quarantine (Cava et al., 2005).
Knowledge
Cross‐sectional studies in Hong Kong and Australia have found that greater knowledge about how SARS is transmitted is associated with greater adoption of precautionary behaviours (Leung et al., 2004) and that a greater knowledge of the meaning of a pandemic is associated with intentions to comply with quarantine restrictions (Eastwood et al., 2009). Misconceptions and lack of knowledge can also be important. For example, a study in Hong Kong found that a belief that there was sustained spread by human to human contact of avian flu in the last 12 months (a misconception) was associated with precautionary behaviour (eating less poultry, taking/stocking Tamiflu, getting vaccinated) and misconceptions about mode of transmission of avian flu was associated with avoidance of hospitals (Lau, Tsui, & Kim, 2006).
However, a longitudinal study found that level of knowledge of SARS was not consistently or strongly associated with future uptake of precautionary behaviour (Leung et al., 2005). Additionally, a study carried out in The Netherlands found no association between knowledge of SARS and behaviour (Brug et al., 2004).
Discussion
This review was carried out in order to identify the key demographic and psychological variables associated with protective behaviour during a pandemic and to place these within conceptual frameworks. The aim was to inform future communication strategies to encourage behaviour which would reduce the spread and impact of disease. Since there are likely to be cultural and societal differences in responses to a pandemic, we can draw some broad conclusions from the evidence identified, but applicability is likely to vary across country.
Direct associations between demographic factors and preventive and avoidant behaviours are shown by this review. There are no direct links between demographic factors and management of disease behaviours. Consistent results have been found for the influence of gender on preventive and avoidant behaviour, with women being more likely to carry out preventive and avoidant behaviours. The pattern for age generally shows that older people are more likely to carry out behaviours, with the exception of one study examining behaviours during the swine flu outbreak, and one which included only adolescents in a SARS outbreak where the younger participants were more likely to carry out behaviours. In general, more educated people are more likely to adopt preventive and avoidant behaviours, although three studies found that less educated people were more likely to adopt the behaviours. There is some evidence that these observed associations may be mediated by differing attitudes, for example, higher levels of perceived susceptibility to disease amongst women may explain why there is an observed link between being female and being more likely to comply with quarantine restrictions, wear a mask, and perform hygiene behaviours. Gender has been found to be related to risk judgments in other areas than pandemic disease. For example, Flynn, Slovic, and Mertz (1994) found that of 25 hazards (e.g., the risk posed by nuclear power plants) women consistently judged risk to be higher than men.
An aim of this review was to describe conceptual frameworks in which to better understand predictors of protective behaviours in the face of a pandemic flu threat. Theories of behaviour such as the health belief model (HBM), theory of planned behaviour (TPB), and protective motivation theory (PMT) provide explanatory models of how people react to a threat to their health and may help to make sense of the observed pattern of findings. These theories are briefly outlined below.
The HBM has been applied in a number of contexts including use of preventive screening, obtaining immunizations, compliance with medical regimens, and response to illness symptoms (see Sheeran & Abraham, 1996, for a review; Harrison, Mullen, & Green, 1992, for a meta‐analysis). The HBM includes assessments of perceived susceptibility to, and severity of, a disease; and perceived benefits and perceived costs of a preventive health action and also cues to action.
The TPB, an expansion of the theory of reasoned action which was devised by Fishbein and Ajzen (1975) to explain social behaviour, has been widely applied to a variety of behaviours – both health and non‐health related (see Conner & Sparks, 1996, for a review and meta‐analyses by Godin & Kok, 1996 and Sheppard, Hartwick, & Warshaw, 1988). The TPB postulates that the proximal determinant of a behaviour is an intention to perform it. In turn, intentions are determined by three constructs: attitude towards the behaviour, subjective norm, and perceived behavioural control (PBC). Attitude towards the behaviour refers to the person's overall evaluation of the behaviour, which may be positive or negative. Subjective norms involve perceptions of how other people think the individual should behave in relation to the particular behaviour in question and also how these other people themselves behave. PBC aims to take account of differences in abilities, skills, access to resources, confidence, etc. between individuals.
PMT (Rogers, 1975, 1983) was originally developed to understand the basis of fear appeals in health promotion. Protection motivation (a behavioural intention to perform a maladaptive or adaptive behaviour) is postulated to be determined by two processes: threat and coping appraisals. Threat appraisal involves a consideration of the severity of the health threat and a perception of personal vulnerability to it. Coping appraisal involves a consideration of whether or not the health action is an effective means of alleviating the threat (i.e., response efficacy), and also a consideration by the individual of whether they will be able to carry out the health action (i.e., their perceived self‐efficacy). PMT suggests that threat appraisal will generate an intention to act whereas coping appraisal will determine the type of action. This can be adaptive (i.e., in line with recommended behaviour) or maladaptive (i.e., against the recommendations). Rogers suggests that protection motivation is a linear function of the belief that the threat is severe, high personal vulnerability, a belief that one can perform the coping response and that the response is effective. It is a negative linear function of the reinforcements associated with the maladaptive response and of the response costs.
There is evidence from this review that perceiving oneself to be more susceptible to SARS, avian flu, swine flu, or pandemic influenza is associated with undertaking preventive, avoidant, and management of disease behaviours to protect oneself. The literature on risk perception (Adams, 1995) has established that public concerns about risk are higher with novel threats and when individuals do not feel in control of the risk, both factors relevant to an influenza pandemic. There is also evidence from this review that perceiving the disease to be more severe is associated with taking preventive and avoidant behaviours. Both these findings can be explained by reference to the proposed relationship between attitudes and behaviour as described by the HBM and PMT which highlight the importance of perceptions of threat in determining behaviour. The review finds that having more confidence in the efficacy of the preventive and avoidant behaviours is associated with a greater likelihood of taking action. The HBM, PMT, and TPB all highlight the influence of attitudes towards the behaviour in determining a behavioural response and provide a framework to understand this finding.
A criticism of the above theories of behaviour is that they do not explain behaviours that are emotionally rather than cognitively and rationally driven as they do not adequately take into account emotional factors in decision making (Joffe, 1996). In this review, four studies found that a higher level of general anxiety was related to a greater chance of carrying out preventive and avoidant protective behaviours. The common sense model of illness developed by Leventhal, Meyer, and Nerenz (1980) is a ‘parallel processing model’ whereby individuals simultaneously make cognitive and emotional representations of an illness. When faced with a new threat, individuals build a mental model of the threat in order to make sense of and manage the problem. The representation involves beliefs about the cause, consequences (in terms of the impact the disease would have), identity, time line, and controllability of the illness (Petrie & Weinman, 1997, 2006). A parallel emotional reaction interacts with this mental model and drives coping strategies and health behaviours relating to that threat. A meta‐analysis including 45 studies examined the relationship between illness representations and coping and illness outcomes. This demonstrated how the relationships between these concepts were consistent with those predicted by the model and that the model predicted a variety of health behaviours (Hagger & Orbell, 2003).
Other models incorporating emotional influences and automatic processing are the two system model of social behaviour which posits that behaviour is determined by both reasoned and impulsive processes (see Strack & Deutsch, 2004) and PRIME theory of motivation (see West, 2006). The two system model suggests that social behaviour is controlled by two interacting systems one generating behavioural decisions that are based on knowledge about facts and values, and the other driving behaviour through automatic associative links (akin to classical and operant conditioning). PRIME theory posits that behavioural responses are driven by the greatest ‘wants and needs’ at the time; the latter arises from anticipated relief from anxiety. This and/or identity as someone who follows particular rules, interacts with triggers to action (e.g., symptoms, advice from government) to cause behaviour. It is possible to interpret the findings for the role of anxiety in this review with these theories.
A further finding that cannot be readily explained in terms of perceptions of threat or perceived efficacy of behaviour but can be interpreted in the light of the above theories is that having a high level of trust in authorities and satisfaction with the communications received about the disease is associated with compliance with preventive, avoidant, and management behaviours. Research has shown that trust is a key emotion which has been found to be relevant in risk‐related behaviour (Slovic, 1999). Levels of trust and satisfaction with communication are particularly important in a pandemic situation in that the authorities are responsible for providing information about the course of the outbreak and also for developing treatments and vaccinations. Lack of trust can therefore have very detrimental effects in terms of controlling the disease. Trust is important because it affects how likely it is that risk assessments from authorities are deemed to be credible and this belief in turn can influence behaviour. A lack of trust in authorities is likely to affect how people process and interpret health messages and risk communication advice, to increase concerns and to interfere with the way that the risk messages are interpreted and acted on (Petts, Horlick‐Jones, & Murdock, 2001; Vaughan & Tinker, 2009). Issues of trust can be especially important in situations which are uncertain, such as how the course of a pandemic will develop. Slovic (1999) points out that trust is fragile and difficult to maintain, being easily broken because negative events which can destroy trust are more noticeable than positive events.
Previous research has highlighted the importance of communication in preventing disease. Openness of government communication and acknowledging uncertainty is important for fostering trust (e.g., Wray et al., 2008). Reviews by Lee (2008), Menon (2006), and Menon and Goh (2004) examined why Singapore fared so well during the SARS crisis, whereas Hong Kong did not and concluded that transparency in communications was key. The Singapore Government's success was partly due to their ability to build confidence and trust in the community and their transparent approach to communications. This was associated with compliance with the recommendations (e.g., quarantine) and reduced spread of SARS. In contrast, the Hong Kong Government lost public trust due to its handling of the event. In particular, the government said that there was nothing to worry about and failed to implement containment measures when cases were already occurring in Hong Kong. People were given inconsistent advice about precautionary measures and insufficient information about the spread of the disease. Some research suggests that the public are more likely to take appropriate action and accept the recommended treatment plan if they have been involved in the decision‐making process (e.g., focus groups, patient forums; Holmes, 2008; Tam, Sciberras, Mullington, & King, 2005). Such involvement can influence the level of trust that the public has in government and institutions (Holmes, 2008; Tam et al., 2005).
Limitations
This review is not exhaustive and caution needs to be exercised when generalizing from the findings of these studies. The majority of the studies were carried out in Asia and therefore one should be circumspect when generalizing to Western populations. A few studies report parts of the same dataset thus reducing the actual number of studies, time periods, and situations in which the findings are observed.
Some studies use multiple behaviours as the outcome measures, often combining a number of different behaviours into one scale, precluding the possibility of determining which psychological and demographic variables predict which particular behaviours. Predictors may differ across behaviour, e.g., whether it is routine/habitual (such as hand washing) or requires a conscious decision (e.g., mask wearing). Also, behaviours differ in their frequency (such as disinfecting homes compared with having a vaccination); some are cued by circumstance and novel (e.g., quarantine) whereas others are a stepping up of existing behaviour (e.g., more frequent hand washing). Some are decreed by law, some are personal choice. Such differences make the directing of interventions and communication strategies harder.
The majority of the studies in this review were cross‐sectional in design and therefore not able to infer causality. In addition, measurement of the psychological constructs included in the studies was heterogeneous. For example, a recent review of studies examining risk perception in a pandemic (Leppin & Aro, 2009) showed that this construct was assessed in many different ways, with some studies emphasizing emotional aspects of the construct (e.g., concern, worry) and others assessing risk in a more cognitive way (e.g., perceived susceptibility, likelihood of developing disease). Some research suggests that measurement of risk by including aspects of feelings as well as cognitive judgment improves the prediction of behaviour (Weinstein et al., 2007).
The studies included in this review relied on self‐reports of behaviour (or examined reported intentions), with the majority assessing this using telephone surveys. This method is open to reporting bias, in particular to behave in a socially desirable way and therefore there may have been over‐reporting of behaviour. There is research evidence that self‐report of hand‐washing practices has poor validity (e.g., Curtis, Danquah, & Aunger, 2009; Curtis et al., 1993). Studies examining intentions in the face of a future pandemic have the limitation of the ‘intention–behaviour gap’ where reported intentions may not in fact translate into behaviour in the event of an actual pandemic (Orbell & Sheeran, 1998).
Despite these limitations, the findings are broadly consistent across diseases and, for preventive and avoidant behaviours, across behaviours. They form a good basis for informing communication and behaviour change strategies, and for research informed by the recent influenza pandemic.
Implications for future research, interventions, and communication strategies
The demographic findings from this review suggest that interventions designed to increase protective behaviour during a pandemic should be adapted for specific groups of individuals, i.e., men, younger people, and the less well educated. Further research is required to clarify the influence of these demographic factors on behaviour. Theories of behaviour suggest that their influence is mediated by differing attitudes. Further research analysing these possible mediators would enable communication strategies to target relevant attitudes. For example, a recent intervention study designed to increase hand washing found gender differences: men tended to be motivated more by messages highlighting the disgust of not washing ones hands, whereas women were more influenced by ‘knowledge activation’ – which involved being reminded of what they know already about the advantages of hand washing (Judah et al., 2009).
Future research should focus on prospective, theory‐driven studies of predictors of particular behaviours. If attitudes were assessed using reliable measures developed from psychological theory before an outbreak it would be possible to see if these attitudes predicted subsequent behaviour during a pandemic. In addition, it is important to carry out behavioural research during a pandemic where actual behaviour can be measured. This should include a variety of designs, including observational and experimental, and types of data, both quantitative and qualitative. Findings from such studies would add to the literature in that more confident conclusions could be drawn about influences on behaviour. The results from these types of studies could then be used to develop targeted interventions to encourage appropriate protective behavioural responses during a pandemic. For example, the finding that perceiving oneself to be more susceptible to the illness is associated with engaging in protective behaviours highlights the need to focus on perceptions of risk in communications. A certain level of perceived susceptibility is required to get people to take action. Communications designed to highlight perceptions of risk should also be combined with advice as to how the perceived threat can be lessened. For example, by emphasizing that risk can be reduced by carrying out the recommended protective actions and providing information about the efficacy of such measures in reducing risk. However, recent work has shown the conceptual and empirical limitations of social cognition models in informing behaviour change interventions (e.g., Sniehotta, 2009). Studies ‘testing’ social cognition models are usually observational, non‐experimental studies, limiting the possibility of drawing causal inferences. For example, assumptions should not be made about the direction of causality (i.e., that attitudes cause behaviour and not the other way around) or about the stability of any observed relationship over time (see Sutton, 2002).
Whilst attitudes and beliefs are important, we need to also consider issues of respect, authority, and social relations (e.g., Hobson‐West, 2003). Effective communication during a pandemic will be vital for controlling the spread of disease. This should be open and transparent in order to build trust and confidence in the authorities. For example, one way of maintaining trust is to communicate the uncertainty which is associated with an emerging pandemic (see Holmes, 2008).
This review has brought together research evidence for the key demographic and attitudinal determinants of behaviour which are key for controlling the spread of pandemic disease, and described conceptual frameworks in which to better understand these behaviours. In sum, the review shows that there are demographic differences in behaviour: being older, female and more educated, or non‐White, is associated with a higher chance of adopting the behaviours. There is evidence that greater levels of perceived susceptibility to and perceived severity of the diseases and greater belief in the effectiveness of recommended behaviours to protect against the disease are also important predictors of behaviour. There is also evidence that greater levels of state anxiety and greater trust in authorities are associated with behaviour. The findings from this review can be broadly explained by theories of health behaviour. However, theoretically driven prospective studies are required to further clarify the relationship between demographic factors, attitudes, and behaviour. The findings suggest that intervention studies should focus on particular demographic groups and on raising levels of perceived threat of the pandemic disease and belief in the effectiveness of measures designed to protect against it. Communication strategies should maximize levels of trust amongst the public by being open and transparent in order to maintain the credibility of the information provided. Carrying out this work now will be invaluable in preparing for future pandemics.
Acknowledgements
The authors would like to thank the editor, two anonymous reviewers, Dr Peter Harris (Sheffield University), and Dr James Rubin (Kings College London) for their helpful comments on earlier drafts of this paper. In addition, the authors thank the Behaviour and Communications sub‐group of the UK Scientific Pandemic Influenza Advisory Group for supplying relevant references.
Footnotes
1These add up to more than 26 as some studies examined more than one type of behaviour.
2During the outbreak of swine flu the UK Government recommended that individuals identify someone in their social network who could collect antiviral medication for them in the event of their contracting swine flu. This person is referred to as a ‘Flu Friend’.
References
- Adams, J. Risk London UCL Press; 1995. [Google Scholar]
- Barr, M. , Raphael, B. , Taylor, M. , Stevens, G. , Jorm, L. , Giffin, M. , Lujic, S. Pandemic influenza in Australia: Using telephone surveys to measure perceptions of threat and willingness to comply Infectious Diseases 8 117–130 doi:10.1186/1471‐2334‐8‐117 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blendon, R. J. , Benson, J. M. , DesRoches, C. M. , Raleigh, E. , Taylor‐Clark, K. The public's response to severe acute respiratory syndrome in Toronto and the United States Clinical Infectious Diseases 38 7 925–931 2004. [DOI] [PubMed] [Google Scholar]
- Brug, J. Aro, A. R. , Oenema, A. , de Zwart, , O. , Richardus, J. H. , Bishop, G. D. SARS risk perception, knowledge, precautions, and information sources, The Netherlands Emerging Infectious Disease 10 8 1486–1489 doi:10.1007/s12529‐008‐9000‐x 2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cava, M. A. , Fay, K. E. , Beanlands, H. J. , McCay, E. A. , Wignall, R. Risk perception and compliance with quarantine during the SARS outbreak Journal of Nursing Scholarship 37 4 343–347 2005. [DOI] [PubMed] [Google Scholar]
- Conner, M. , Sparks, P. The theory of planned behaviour and health behaviours Conner M., Norman P. Predicting health behaviour 121–162 Buckingham Open University Press; 1996. [Google Scholar]
- Curtis, V. , Cousens, S. , Mertens, T. , Traore, E. , Kanki, B. , Diallo, I. Structured observations of hygiene in Burkina Faso, validity, variability and utility Bulletin of the World Health Organisation 71 23–32 1993. [PMC free article] [PubMed] [Google Scholar]
- Curtis, V. , Danquah, L. O. , Aunger, R. V. Planned, motivated and habitual hygiene behaviour: An eleven country review Health Education Research 24 4 655–673 doi:10.1093/her/cyp002 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eastwood, K. , Durrheim, D. , Francis, J. L. , d'Espaignet, E. Tursan , Duncan, S. , Islam, F. , Speare, R. Knowledge about pandemic influenza and compliance with containment measures among Australians Bulletin World Health Organisation 87 588–594 doi:10.2471/BLT.08.060772 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fishbein, M. , Ajzen, I. Belief, attitude, intention and behaviour: An introduction to theory and research Reading, MA Addison‐Wesley; 1975. [Google Scholar]
- Flynn, J. , Slovic, P. , Mertz, C. K. Gender, race and perception of environmental health risks Risk Analysis 14 6 1101–1108 1994. [DOI] [PubMed] [Google Scholar]
- Godin, G. , Kok, G. The theory of planned behavior: A review of its applications to health‐related behaviors American Journal of Health Promotion 11 2 87–98 1996. [DOI] [PubMed] [Google Scholar]
- Goodwin, R. , Haque, S. , Neto, F. , & Myers, L. B. (2009). Initial psychological responses to influenza A, H1N1 (‘swine flu’). BMC Infectious Diseases, 9(1), 166. doi:10.1186/1471‐2334‐9‐166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagger, M. , Orbell, S. A meta analytic review of the common‐sense model of illness representations Psychology and Health 18 141–184 doi:10.1080/088704403100081321 2003. [Google Scholar]
- Harrison, J. A. , Mullen, P. D. , Green, L. W. A meta‐analysis of studies of the health belief model with adults Health Education Research: Theory and Practice 7 1 107–116 1992. [DOI] [PubMed] [Google Scholar]
- Hobson‐West, P. Understanding vaccine resistance: Moving beyond risk Health, Risk and Society 5 273–283 doi:10.1080/13698570310001606978 2003. [Google Scholar]
- Holmes, B. J. Communicating about emerging infectious disease: The importance of research Health Risk and Society 10 4 349–360 doi:10.1080/13698570802166431 2008. [Google Scholar]
- Hong, S. , Collins, A. Societal response to familiar versus unfamiliar risk: Comparisons of influenza and SARS in Korea Risk Analysis 26 5 1247–1257 doi:10.1111/j.1539‐6924.2006.00812.x 2006. [DOI] [PubMed] [Google Scholar]
- Jiang, X. Elam, G. , Yuen, C. , Voeten, H. , de Zwart, , O. , Veldhuijzen, I. , Brug, J. The perceived threat of SARS and its impact on precautionary actions and adverse consequences: A qualitative study among Chinese communities in the United Kingdom and The Netherlands International Journal of Behavioral Medicine 16 58–67 doi:10.1007/s12529‐008‐9005‐5 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joffe, H. AIDS research and prevention: A social representational approach British Journal of Medical Psychology 69 3 169–190 1996. [DOI] [PubMed] [Google Scholar]
- Jones, J. H. , & Salathe, M. (2009). Early assessment of anxiety and behavioural response to novel swine‐origin influenza A(H1N1). PLoS One, 4(12), e:8032. doi:10.1371/journal.pone.0008032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Judah, G. , Aunger, R. , Schmidt, W. P. , Michie, S. , Granger, S. , Curtis, V. Experimental pre‐testing of hand‐washing interventions in a natural setting American Journal of Public Health 99 S2 405–411 doi:10.2105/AJPH.2009.164160 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lau, J. T. F. , Kim, J. H. , Tsui, H. Y. , Griffiths, S. Anticipated and current preventive behaviours in response to an anticipated human‐to‐human H5N1 epidemic in the Hong Kong Chinese general population BMC Infectious Diseases 7 18 18–29 doi:10.1186/1471‐2334‐7‐18 2007a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lau, J. T. F. , Kim, J. H. , Tsui, H. Y. , Griffiths, S. Perceptions related to human avian influenza and their associations with anticipated psychological and behavioural responses at the onset of outbreak in the Hong Kong Chinese general population American Journal of Infection Control 35 38–49 doi:10.1016/j.ajic.2006.07.010 2007b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lau, J. T. F. , Kim, J. H. , Tsui, H. Y. , Griffiths, S. Perceptions related to bird‐to‐human avian influenza, influenza vaccination, and use of face mask Infection 36 5 434–443 doi:10.1007/s15010‐008‐7277‐Y 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lau, J. T. F. , Tsui, H. Y. , Kim, J. H. Perceptions about status and modes of H5N1 transmission and associations with immediate behavioural responses in the Hong Kong general population Preventive Medicine 43 5 406–410 doi:10.1016/j.ypmed.2006.06.007 2006. [DOI] [PubMed] [Google Scholar]
- Lau, J. T. F. , Yang, X. , Tsui, H. Y. , Kim, J. H. Monitoring community responses to the SARS epidemic in Hong Kong: From day 10 to day 62 Journal of Epidemiology and Community Health 57 864–870 doi:10.1136/jech.57.11.864 2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lau, J. T. , Yang, X. , Tsui, H. Y. , Pang, E. SARS related preventive and risk behaviours practised by Hong Kong–mainland China cross border travellers during the outbreak of the SARS epidemic in Hong Kong Journal of Epidemiology and Community Health 58 12 988–996 doi:10.1136/jech.2003.017483 2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lau, J. T. , Yang, X. , Tsui, H. Y. , Pang, E. , Kim, J. H. SARS preventive and risk behaviours of Hong Kong air travellers Epidemiology and Infection 132 727–736 doi:10.1017/S0950268804002225 2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, K. How the Hong Kong Government lost the public trust in SARS: Insights for government communication in a health crisis Public Relations Review 35 1 74–76 doi:10.1016/j.pubrev.2008.06.003 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leppin, A. , Aro, A. R. Risk perceptions related to SARS and avian influenza: Theoretical foundations of current empirical research International Journal of Behavioral Medicine 16 7–29 doi:10.1007/s12529‐008‐9002‐8 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung, G. M. , Ho, L. M. , Chan, S. K. K. , Ho, S. Y. , Bacon‐Shone, J. , Choy, R. , Fielding, R. (2005). Longitudinal assessment of community psycho‐behavioural responses during and after the 2003 outbreak of severe acute respiratory syndrome in Hong Kong. Clinical Infectious Diseases, 40, 1713–1720. [DOI] [PubMed] [Google Scholar]
- Leung, G. M. , Lam, T. H. , Ho, L. M. , Ho, S. Y. , Chan, B. H. Y. , Wong, I. O. L. , Hedley, A. J. The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong Journal of Epidemiology and Community Health 57 857–863 doi:10.1136/jech.57.11.857 2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung, G. M. , Quah, S. , Ho, L. M. , Ho, S. Y. , Hedley, A. J. , Lee, H. P. , Lam, T. H. A tale of two cities: Community psychobehavioral surveillance in Hong Kong and Singapore during the severe acute respiratory syndrome epidemic Infection Control and Hospital Epidemiology 25 12 1033–1041 2004. [DOI] [PubMed] [Google Scholar]
- Leventhal, H. , Meyer, D. , Nerenz, D. The common sense model of illness danger Rachman S. Medical psychology 2 7–30 New York Pergamon; 1980. [Google Scholar]
- Menon, K. U. SARS revisited: Managing outbreaks with communications Annals of the Academy of Medicine, Singapore 35 361–367 2006. [PubMed] [Google Scholar]
- Menon, K. U. , Goh, K. T. Transparency and trust: Risk communications and the Singapore experience in managing SARS Journal of Communication Management 9 4 375–383 2004. [Google Scholar]
- Morrison, L. G. , Yardley, L. What infection control measures will people carry out to reduce transmission of pandemic influenza? A focus group study BMC Public Health 9 258–269 doi:10.1186/1471‐2458‐9‐258 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orbell, S. , Sheeran, P. Inclined abstainers: A problem for predicting health‐related behaviour British Journal of Social Psychology 37 2 151–165 1998. [DOI] [PubMed] [Google Scholar]
- Petrie, K. J. , Weinman, J. Perceptions of health and illness: Current research and applications Amsterdam Harwood; 1997. [Google Scholar]
- Petrie, K. J. , Weinman, J. Why illness perceptions matter Clinical Medicine 6 6 536–539 2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petts, J. , Horlick‐Jones, T. , & Murdock, G. (2001). Social amplification of risk: The media and the public. Contract Research Report 329/2001. Sudbury: HSE Books. [Google Scholar]
- Quah, S. R. , Hin‐Peng, L. Crisis prevention and management during SARS outbreak, Singapore Emerging Infectious Disease 10 364–368 2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quinn, S. C. , Kumar, S. , Freimuth, V. S. , Kidwell, K. , & Musa, D. (2009). Public willingness to take a vaccine or drug under emergency use authorization during the 2009 H1N1 pandemic. Biosecurity and Bioterrorism: Biodefense Strategy, Practice, and Science, 7(3), 275–290. doi:10.1089 = bsp.2009.0041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers, R. W. A protection motivation theory of fear appeals and attitude change Journal of Psychology 91 93–114 1975. [DOI] [PubMed] [Google Scholar]
- Rogers, R. W. Cognitive and physiological processes in attitude change: A revised theory of protection motivation Cacioppo J., Petty R. Social psychophysiology 153–176 New York Guildford Press; 1983. [Google Scholar]
- Rubin, G. J. , Amlôt, R. , Page, L. , Wessely, S. Public perceptions, anxiety and behavioural change in relation to the swine flu outbreak: A cross‐sectional telephone survey British Medical Journal 339 b2651 doi:10.1136/bmj.b2651 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheeran, P. , Abraham, C. The health belief model Conner M., Norman P. Predicting health behaviour 23–61 Buckingham Open University Press; 1996. [Google Scholar]
- Sheppard, B. H. , Hartwick, J. , Warshaw, P. R. The theory of reasoned action: A meta‐analysis of past research with recommendations for modifications and future research Journal of Consumer Research 15 325–343 1988. [Google Scholar]
- Slovic, P. Trust, emotion, sex, politics and science: Surveying the risk‐assessment battlefield Risk Analysis 19 4 689–701 1999. [DOI] [PubMed] [Google Scholar]
- Sniehotta, F. Towards a theory of intentional behaviour change: Plans, planning and self‐regulation British Journal of Health Psychology 14 261–273 doi:10.1348/135910708X389042 2009. [DOI] [PubMed] [Google Scholar]
- Spielberger, C. , Edwards, C. , Lushene, R. , Montuori, J. , Platzek, D. Preliminary test manual for the State‐Trait Anxiety Inventory for children Palo Alto, CA Consulting Psychologists Press; 1973. [Google Scholar]
- Strack, F. , Deutsch, R. Reflective and impulsive determinants of social behaviour Personality and Social Psychology Review 8 3 220–247 doi:10.1207/s15327957pspr0803_1 2004. [DOI] [PubMed] [Google Scholar]
- Sutton, S. Testing attitude–behaviour theories using non‐experimental data: An examination of some hidden assumptions European Review of Social Psychology 13 293–323 doi:10.1080/10463280240000019 2002. [Google Scholar]
- Tam, T. , Sciberras, J. , Mullington, B. , King, A. Fortune favours the prepared mind Canadian Journal of Public Health 96 406–408 2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tang, C. S. K. , Wong, C. Y. An outbreak of the severe acute respiratory syndrome: Predictors of health behaviours and effect of community prevention measures in Hong Kong, China American Journal of Public Health 93 11 1887–1888 2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tang, C. S. K. , Wong, C. Y. Factors influencing the wearing of facemasks to prevent the severe acute respiratory syndrome among Chinese in Hong Kong Preventive Medicine 39 1187–1193 doi:10.1016/j.ypmed.2004.04.032 2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tang, C. S. K. , Wong, C. Y. Psychosocial factors influencing the practice of preventive behaviours against the severe acute respirator syndrome among older Chinese in Hong Kong Journal of Aging Health 17 490–506 doi:10.1177/0898264305277966 2005. [DOI] [PubMed] [Google Scholar]
- Vaughan, E. , Tinker, T. Effective health risk communication about pandemic influenza for vulnerable populations American Journal of Public Health 99 2 324–332 doi:10.2105/AJPH.2009.162537 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weinstein, N. D. , Kwitel, A. , McCaul, K. , Magnan, R. E. , Gerrard, M. , Gibbons, F. X. Risk perceptions: Assessment and relationship to influenza vaccination Health Psychology 26 2 146–151 doi:10.1037/0278‐6133.26.2.146 2007. [DOI] [PubMed] [Google Scholar]
- West, R. Theory of addiction Oxford Blackwell Publishing; 2006. [Google Scholar]
- Wong, C. Y. , Tang, C. S. K. Practice of habitual and volitional health behaviours to prevent severe acute respiratory syndrome among Chinese adolescents in Hong Kong Journal of Adolescent Health 36 3 193–200 doi:10.1016/j.jadohealth.2004.02.024 2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wray, R. , Becker, S. M. , Henderson, N. , Glik, D. , Jupka, K. , Middleton, S. , Mitchell, E. W. (2008). Communication with the public about emerging health threats: Lessons from the Pre‐Event Message Development Project. American Journal of Public Health, 98(12), 2214–2222. doi:10.2105/AJPH.2006.107102. [DOI] [PMC free article] [PubMed] [Google Scholar]