

INTRODUCTION
Research suggests that pain is capable of undermining self-regulatory processing with negative implications for adjustment [19, 21, 29]. For example, pain has been shown to interfere with many of the valued tasks of daily living, including the pursuit of personal goals [1, 2, 22, 40]. However, as additional research is warranted to examine mediation of the direct relationship between pain intensity and progress toward goal attainment. For example, increases in pain intensity can lead to more pain interference with goal pursuit, which in turn, can undermine goal progress. Thus, the present study examined whether pain interference with afternoon goal pursuit mediates the association between morning pain intensity and evening work goal progress.
Exploring potential moderators of the pathway from pain intensity to goal progress may help to further clarify how the pain experience is differentially regulated, as individual differences in pain attitudes and beliefs are known to influence the functioning of chronic pain patients [32, 47]. Two possible attitudinal moderators are particularly relevant to pain and goal-related action: pain acceptance, characterized by a willingness to experience pain while pursuing goals [35], and pain catastrophizing, a maladaptive style of thinking characterized by magnification, helplessness, and rumination about the pain experience [43]. Individuals with greater pain acceptance tend to display higher levels of functioning, improved worked status, and less reported pain and anxiety [30, 31, 32, 36]. By contrast, catastrophizing contributes to higher levels of pain and psychological distress, and to functional disabilities [45, 23, 47]. These between-person differences have also been found to moderate within-person relationships in the context of chronic pain. Pain acceptance moderates the relations between daily pain intensity and fearful thinking [10], and between negative affect and pain severity [24]. Similarly, individuals high in trait levels of pain catastrophizing reveal greater daily increases in state catastrophizing in response to increases in pain intensity [41]. However, to our knowledge, no studies have examined how these two individual difference factors impact the day-to-day relationship between changes in pain intensity and pain interference with work goal pursuit.
Finally, we note that the process of self-regulation can be influenced by an individual’s affective state [19]. Negative affect has been shown, under certain circumstances, to inhibit the pursuit of meaningful goals, whereas positive affect can serve an appetitive, reward-seeking function that enhances goal directedness [7, 8, 11, 15, 16]. Therefore, examining how affect influences daily goal pursuit and progress among individuals with chronic pain would expand our nascent understanding of the motivational dynamics of pain.
Figure 1 depicts the model tested in the present study. It was hypothesized that: (1) the within-person relationship between morning pain intensity and evening goal progress will be mediated by afternoon pain’s interference with work goal pursuit; (2) the within-person, positive relationship between morning pain intensity and its interference with work goal pursuit in the afternoon will decrease as pain catastrophizing decreases and as pain acceptance increases; and (3) morning positive affect will decrease and morning negative affect will increase pain’s interference with work goal pursuit in the afternoon.
Fig. 1.
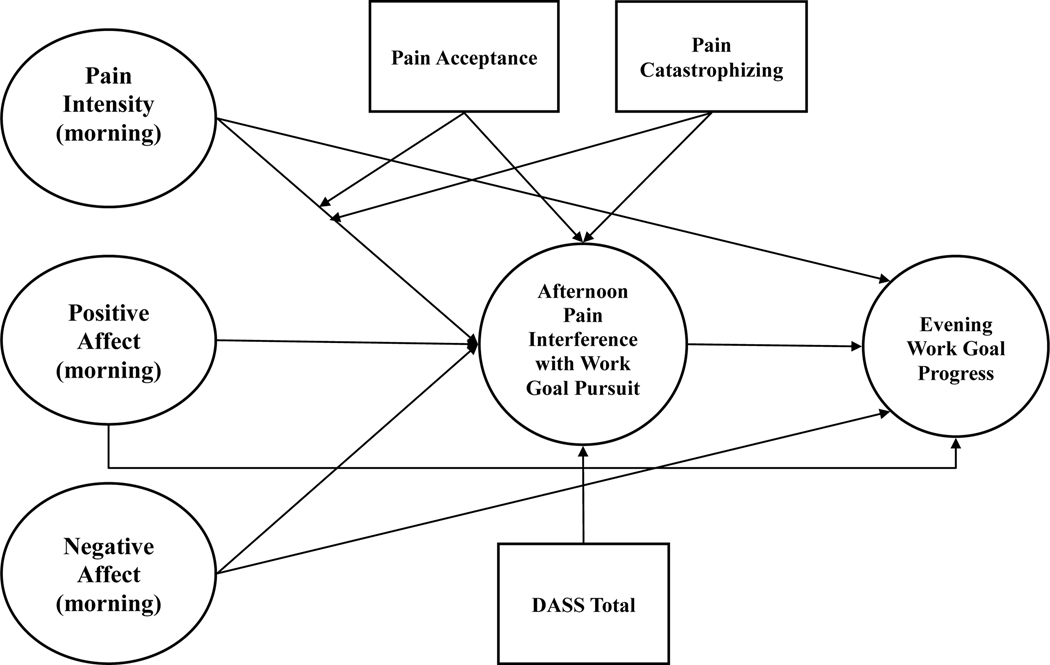
Hypothetical model
Note. Variables with circular shape are level-1 (day-level) variables and variables with rectangular shape are level-2 (person-level) variables.
METHOD
Participants
The current sample was recruited by a survey research organization in Phoenix, Arizona. Residents living within approximately 20 miles of the research facility in the Phoenix metropolitan area received phone calls generated by a random-digit dialing process. Telephone interviewers screened the residents who answered the phone calls based on a script developed by the experimenters. To participate in the study, residents had to: (1) be at least 25 years old but less than 70 years old (these minimum and maximum ages were selected based upon the ages included in the national norms of the Profile of Chronic Pain, which was used to determine study eligibility), (2) have experienced physical pain for the past six months almost every day, (3) be able to read English at a minimum third grade level, (4) not be color blind because participants had to complete executive function measures including the Wisconsin Card Sorting Test and the Stroop Test which used color stimulus materials, (5) work either at a paid full-time or part-time job during the day, (6) report not using illegal substances (e.g., marijuana, LSD, heroin, cocaine, etc) in the past 12 months, and (7) be able to complete the diary by phone call three times a day for 21 days. In addition to the phone screening, those selected participants were screened using a self-report, 4-item chronic pain severity questionnaire from the Profile of Chronic Pain (PCP) Screen. Cut off scores for inclusion in the present study were determined separately by age and sex based upon the Ruehlman et al. [39] norms.
Of the 318 adults deemed eligible to participate, 155 (48.7 percent) declined. The remaining 163 eligible participants who agreed to participate were scheduled for a laboratory appointment. Sixteen participants (9.8 percent) never showed up to any scheduled appointments (even after attempts at re-scheduling). Among the 147 subjects who arrived for their initial assessments, 16 (10.9 percent) were found to be ineligible for one of the following reasons: (a) not currently working, (b) unable to articulate an important work goal, or (c) not able to complete phone-based diaries 3 times a day for 21 days. Hence, the final sample for the current study consists of 131 participants.
To examine the potential for bias in the final sample, individuals who declined to participate, those who did not appear for their initial assessment, those who were disqualified, and those who participated were compared. For the continuous variables, one-way ANOVAs were used and for categorical variables, chi-square tests were used. The ANOVA and chi-square tests showed that the difference in participant status (final participants of the current study, decliners, no shows, and those ineligible) were not statistically significant (p > .05) for age, chronic pain severity, gender, race (Hispanic versus Non-Hispanic), ethnicity (White versus other single ethnicities combined, versus two or more ethnicities), and zip code (Phoenix versus Mesa versus Tempe). These findings support the representativeness of the final sample included in the present study.
Procedure
All procedures for recruitment and data collection received prior approval from the Institutional Review Board at Arizona State University. Also, written informed consent was obtained from the participants before the start of the research. Participants were paid separately for two different types of data: (a) $45 for participating in a 150 minute lab visit (initial lab appointment); and (b) up to $155 if almost all diaries across 21 days were completed.
During the first part of the lab visit, participants were asked to provide lists of important work- and lifestyle goals. Work- and lifestyle goals were respectively defined as follows: (a) “a personally valued outcome toward which effort is consistently directed while you are on the job”; (b) “things that make your life better such as goals for physical health, mental health, social relationships, intellectual pursuits, hobbies, recreation, spirituality, or community service”. Criteria for listing important work- and lifestyle goals were that each goal had to be: (a) highly valued, (b) realistically obtainable, (c) concrete and measurable, and (d) pursued almost every day for the next 21 days. From the lists they generated, participants were asked to select a single work goal and a single lifestyle goal that were most important to them. Because the present report focuses on work goal pursuit, only work goals are included for analysis.
During the second part of the lab visit, participants completed questionnaires that assessed demographics, personality, pain experiences, and goal behaviors.
During the third part of the lab visit, participants’ executive functions were assessed using four tasks: (1) a Verbal Fluency Task; (2) an Operation Span Task; (3) the Wisconsin Card Sorting Test; and (4) the Stroop Test. The tasks were administered to the participants in a random order to eliminate the possibility of order effects. The results of these executive function tasks, however, were not used in the present research paper.
During the final part of the lab visit, participants also received a thorough explanation of the special features of the interactive voice response (IVR) system used for the collection of the diary data. For example, participants were told that they would receive a 5-minute phone call via the IVR system three times a day for 21 consecutive days, for a total of 63 calls. If participants missed a call, they were asked to call back during the fixed time window to complete the diary. After the explanation, participants undertook a mandatory face-to-face training session on how to complete IVR system based diary. Research staff explained the required time windows for placing the morning call (6:00 to 10:00 AM), afternoon (noon to 4:00 PM), and evening calls (7:00 to 11:00 PM). Some of the questions required participants to respond about their current feelings (pain and affect), whereas other questions necessitated recalling what transpired since the previous telephone call (interference with goal pursuit and goal progress). Thus, the data bearing on interference with work goal pursuit can be thought of as occurring in the late morning or early afternoon, and the data on work goal progress can be thought of as occurring during the late afternoon or early evening.
During the practice session, participants took part in an automated interview answering practice questions via the telephone number pad. Participants were also shown the scripts for diary interview which contains all the questions for each time of the day. The practice session continued until participants indicated that they were confident in using the IVR system. At the end of the lab visit, participants were provided with an information packet which contained detailed instructions for completing the IVR system-based diary calls, a copy of the script used for the diary assessment, and a card with the IVR phone number, details about the log-in procedure, and the participant’s work- and lifestyle goals.
IVR Technology
The IVR technology, hosted by the University of Connecticut Health Center, provided a combination of telephone service with computer-administered questionnaires. The system was interfaced with local area network stations for data input, storage, and backup. The procedure for IVR data collection was as follows: (1) participants received a phone call from the IVR system with a toll-free call-back number, (2) participants entered their identification number, and (3) by pressing numbers on the keypad of their telephones (0 to 9), participants could answer the computer-administered diary questions.
The IVR activities of the participants were monitored by the research staff. When a participant missed several calls in a row, a staff member initiated a friendly reminder call. A short note of appreciation was sent by mail to participants who completed the first 14 days of the 21-day diary procedure. Across all occasions, participants completed an average of 89.5% of the phone calls.
Chronic Pain Severity Screen
To recruit a sample of persons with chronic pain, the Profile of Chronic Pain (PCP) Screen Severity Scale was administered twice—once during the telephone interview and again during the lab visit. Approximately 7 days elapsed between the two assessments. The PCP-Screen Severity Scale consists of four questions [39]: (1) “Over the past 6 months, how often did you have this pain?”, with response options ranging from 0 (never) to 6 (daily), (2) “What was your AVERAGE level of pain on days when you had pain during the past six months, where zero means very little pain and nine means unbearable pain?” (3) “How often during the PAST 6 MONTHS have you had at least one hour’s worth of pain that hinders you from accomplishing your daily tasks?”, with response options ranging from 0 (never) to 6 (daily), and (4) “What was the GREATEST amount of pain you have had over the PAST 6 MONTHS, where zero means very little pain and nine means unbearable pain?” The test-retest correlation for the PCP-Screen Severity scores was .68. The mean of the PCP screen was 22.33 (SD = 4.28) at the first administration and 21.98 (SD = 3.89) at the second administration. The mean pain severity scores did not differ over time, t(129) = 1.19, p > .05.The internal consistency reliability, as indexed by Cronbach’s α, for the PCP-Screen Severity subscale was .69.
Demographics
Sixty-one percent of the final sample of 131 participants was 61% female. The mean age of the participants was 49.49 years old (SD = 11.99). Eighty percent of the sample consisted of Caucasians, with 4% African American, 2% Native American, 2% Asian, 7% mixed race, and 5% other). As an additional index of ethnicity, 18% of the sample labeled themselves as Hispanic. The sample also varied in marital status (53% were married, 23% were single, 18% were divorced, 3% were widowed, and 3% were not married but living together). The majority of the participants were working full-time (74%). Education backgrounds also varied (48.5% had some college or had earned an Associate’s degree, 15.9% had a Bachelor’s degree, 28.8% had a graduate or professional school degree, and the remaining 6.8% had a high school diploma or less). Although the current sample was not clinic referred, 49% of the participants reported seeing health care professionals for their pain problems.
Measures
Goal Content
Participants reported diverse work goals. Overall, work goals tended to be either task-oriented or interpersonally-oriented. Examples of task-oriented work goals include: “Create 4 new training modules for team members”, and “Prepare instructor materials for fall semester and spend at least 3 hours per day doing this.” Examples of interpersonally-oriented work goals include: “Demonstrate respectful tone when dealing with co-workers”, and “Manage emotional reactions when speaking on phone with other hospital personnel about patient medications.” Owing to their content heterogeneity, they were not further sub-categorized.
Daily Diary Measures
Pain Intensity:
Participants answered the following question about morning pain intensity: “If a zero means no pain, and nine means pain as bad as it could be, on a scale from 0–9, what is your level of pain right now?” Although it was not analyzed for the present study, pain intensity was measured in the afternoon and in the evening as well.
Positive Affect:
Morning positive affect was measured with four items: alert and enthusiastic (from the PANAS; [48]) as well as happy and relaxed. Participants were asked to rate the intensity of each positive affect felt over the past 30 minutes using a scale ranging from 0 (not at all) to 9 (extremely). A morning positive affect score was calculated as the average ratings of the four items.
Negative Affect:
Negative affect was also assessed with four items: nervous and upset, from the PANAS, and angry and fearful. Participants were asked to rate the intensity of each negative affect that they felt over the past 30 minutes using a scale ranging from 0 (not at all) to 9 (extremely). A morning negative affect score was calculated as the average ratings of the four items.
Note that afternoon and evening positive and negative affect were assessed, but not included in the present analyses.
Pain Interference with Work Goal Pursuit:
To measure perceived pain interference with work goals in the afternoon, participants were asked to rate how much their pain interfered with their ability to effectively pursue their work goal using a scale ranging from 0 (not at all) to 9 (extremely). Note that before participants were asked to rate pain interference they first responded to another item, called “Goal Pursuit”, that asked whether or not they had pursued their work goal in the afternoon. Only participants who said that they had pursued their work goal in the afternoon rated pain interference. For the entire sample, the percent of days that work goals were pursued in the afternoon was 45.2 percent. Further, full-time and part-time employees did not differ in the percentage of days they did not pursed their work goals in the afternoon [t(2433) = 1.65, p = .10].
Work Goal Progress:
Perceived work goal progress was measured in the evening diary by the following question: “How much progress have you made on your work goal today since the last time we talked with you?” Participants indicated their evening work goal progress using a scale that ranged from 0 (none at all) to 9 (quite a lot). Although the measure is labeled evening goal progress, the rating reflects activity occurring between the late afternoon and early evening hours (as noted in the Procedure section above). In addition, before participants were asked to rate their evening progress, they first responded to another item, called “Goal Pursuit”, that inquired into whether they in fact pursued their work goal since the last reporting interval. Only participants who said that they had pursued their goal rated their goal progress.
Individual Differences
Pain Acceptance:
Pain acceptance was measured by the 20-item self-report Chronic Pain Acceptance Questionnaire (CPAQ;[35]). The CPAQ uses a Likert scale ranging from 0 (Never) to 6 (Always), and is comprised of two reliable and valid subscales. The activity engagement subscale consists of 11 items gauging how much one pursues life activities while experiencing pain (e.g., “I lead a full life even though I have chronic pain”). The other subscale, pain willingness, consists of 9 items that assess the extent to which an individual is willing to experience pain without trying to control it (e.g., “I need to concentrate on getting rid of my pain” [reversed scored]). A higher total score represents higher pain acceptance. Cronbach’s alpha for the CPAQ was .88.
Pain Catastrophizing:
Pain catastrophizing was assessed using the Pain Catastrophizing Scale (PCS; [42]) that consists of 13 items rated on 5-point Likert scales ranging from 0 (not at all) to 4 (all the time). The PCS is made up of three subscales: Rumination, Magnification, and Helplessness. Examples of items for each subscale are: “I keep thinking about how badly I want the pain to stop” (Rumination); “I become afraid that the pain may get worse” (Magnification); and “There is nothing I can do to reduce the intensity of the pain” (Helplessness).The total score of the PCS can range from 0 to 52, with higher PCS scores indicating greater pain catastrophizing. Cronbach’s alpha for the total score of PCS in the present study was .90.
Depression, Anxiety and Stress:
Depression, anxiety and stress were measured using the Depression Anxiety Stress Scales (DASS; [26]). Each item is rated on a 4-point Likert scale ranging from 0 (Never) to 3 (Almost Always). Examples of items for each subscale are: “I couldn’t seem to experience any positive feeling at all” (Depression); “I experienced trembling (e.g., in the hands)” (Anxiety); and “I tend to over-react to situations” (Stress). All three subscales have been shown to have excellent reliability as well as convergent and discriminant validity [9]. The range of possible scores for each subscale extends from 0 to 21. The original DASS consisted of 42 items, but a shortened 21-item shortened version was administered in the current study. This version has a more interpretable factor structure and smaller inter-factor correlations than the original 42-item DASS [4]. The Cronbach’s alphas for depression, anxiety and stress subscales were .89, .79, and .84, respectively. Because the DASS subscales were highly correlated, the total mean score was used in the present study.
Within- and Between-Person Variability in Daily Diary Measures
Before constructing the proposed multilevel models, unconditional models which do not include any predictors were estimated for the continuous outcomes. This process was employed because it provides important information on how the variation in ratings is partitioned into within- and between-person variability. Results showed that the intraclass correlations (ICCs) for all the day-level variables ranged between .44 and .54. For example, 54% of the variation in pain interference with work goal pursuit and 47% of the variation in work goal progress was explained by the between-person differences. Table 1 presents the within- and between-person variability in the daily diary measures used in the present study. Because the statistical outcomes suggested that there was substantial variation at both the within- and between-person levels of the data hierarchy, it seemed appropriate to estimate the models at both levels of the predictors.
Table 1.
Descriptive statistics, intercorrelations, and ICC for Within-Person Variables,
| Variable | M | SD | ICC | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Level-1 Variables | |||||||||||
| 1 | Morning Pain Intensity | 3.54 | 2.20 | 0.54 | — | −.18** | .11** | .19** | −.01 | ||
| 2 | Morning Positive Affect | 5.05 | 1.94 | 0.64 | −.21* | — | −.31** | −.13** | .01 | ||
| 3 | Morning Negative Affect | 1.15 | 1.66 | 0.44 | .19* | −.22* | — | .03 | −0.00 | ||
| 4 | Afternoon Pain Interference with Work Goal | 2.09 | 2.44 | 0.54 | .62** | −.24* | .13 | — | −.07* | ||
| 5 | Evening Work Goal Progress | 6.14 | 2.44 | 0.47 | −.05 | .36** | .02 | .02 | — | ||
| Level-2 Variables | |||||||||||
| 6 | Pain Acceptance | 3.69 | 0.81 | −.22* | .24** | −.20* | −.49** | −.04 | — | ||
| 7 | Pain Catastrophizing | 1.76 | 0.67 | .21* | −.22** | .28* | .42** | −.01 | −.61** | — | |
| 8 | DASS total score | 0.68 | 0.49 | .30** | −.32** | .55* | .33** | −.01 | −.38** | .54** |
Note. Upper-diagonal shows correlations among day-level (level-1) variables that are person-mean centered. Lower-diagonal shows correlations between person-level variables and day-level variables that are averaged across the 21-days.
p < .05
p < .01
Centering
Both level-1 and level-2 predictors were centered for two reasons. First, in the case of level-1 variables, it was expected that daily score values would depend on other scores of the same cluster (i.e., person). For example, the interpretation of any daily pain score (e.g., a rating 4 out of 9) depends on the overall mean of a participant’s daily pain ratings (that is, a score of 4 is low if the person mean is 8, but is high if the person mean is 2). Thus, person-mean centering was used for level-1 predictors. In the case of level-2 variables, grand-mean centering was used because the interpretation of score values does not depend on other scores of the same cluster (i.e., it reflects trait-like variation). Second, by centering the level 1 and level 2 predictors, the relationship between them becomes orthogonal. To be specific, the level-1 predictors were centered at the person means [13] by subtracting each individual’s average rating for a variable from the daily rating. In the case of level-2 predictors that were grand mean centered, each individual’s rating was subtracted from the mean of all the individuals. Employing this strategy, the person mean centered level-1 variables are uncorrelated with grand mean centered level-2 variables. Hence, we can assess the unique influence of a variable at each level. This centering strategy was used for all models.
Overview of Multilevel Models
A random intercept multilevel model for afternoon pain interference with work goal pursuit as the outcome was tested. This model includes the alpha path of a simple mediation model in which morning pain intensity influence evening work goal progress through afternoon pain interference with work goal pursuit. The model was estimated first by including level-1, then level-2 predictors, and then cross-level interaction terms. The equation for this model is as follows:
| (1) |
Note. APIWGP = Afternoon Pain Interference with Work Goal Pursuit, Pain = Morning Pain, PA = Morning Positive Affect, NA = Morning Negative Affect, Accept = Pain Acceptance, Catastro = Pain Catastrophizing, DASS = Depression, Anxiety and Stress Total Score
In this model, is the outcome score at day i for person j. The intercept () quantifies the expected value (conditional mean) of afternoon pain interference with work goal pursuit for days where persons are at their average of the level-1 variables and at the grand mean of level-2 variables. is the coefficient for the within-person morning pain predictor with average pain acceptance, pain catastrophizing, and the DASS total score. is the coefficient for the morning positive affect predictor with average pain acceptance, pain catastrophizing, and the DASS total score. is the coefficient for the morning negative affect predictor at the average pain acceptance, pain catastrophizing, and the DASS total score. is the coefficient of the between-person pain acceptance predictor for someone at their own pain mean and at the grand mean of pain catastrophizing. is the coefficient of the pain catastrophizing predictor for someone at their own pain mean and at the grand mean of pain acceptance. is the regression coefficient of the DASS (Depression, Anxiety, Stress) control variable. is the coefficient of the cross-level interaction between the within-person morning pain rating and between-person pain acceptance. is the coefficient of the cross-level interaction between within-person morning pain and between-person pain catastrophizing. Finally, is a random intercept that captures between-person variation in the outcome means, and is the level-1 residual. We also investigated whether the influence of the level-1 predictors varied across persons. To do so, we estimated the model in Equation 1 three times, each time adding a random slope for one of the predictors. Likelihood ratio tests from restricted maximum likelihood estimation revealed that daily morning pain ratings, χ2(2) = 21.712, p < .001 and morning negative affect scores, χ2(2)= 11.810, p < .01, required a random slope (i.e., the association between afternoon pain interference with work goal pursuit and morning pain varied across persons). and are the random slopes for the level-1 predictors.
Next, turning to evening work goal progress as the outcome predicted by the beta and alpha prime paths in a mediation model, a series of level-1 and level-2 predictors were entered to the model. The model is given in Equation 2.
| (2) |
Note. EWGP = Evening Work Goal Progress, APIWGP = Afternoon Pain Interference with Work Goal Pursuit
In this model, is the conditional mean of the evening work-goal progress ratings for days where persons are at the average of the level-1 variables and at the grand mean of the level-2 variables. is the coefficient for the within-person afternoon pain interference with work goal pursuit predictor, with average pain acceptance, pain catastrophizing, and the DASS total score. is the coefficient for the within-person morning pain predictor with average pain acceptance, pain catastrophizing, and the DASS total score. is the coefficient for the morning positive affect predictor with average pain acceptance, pain catastrophizing, and the DASS total score, is the coefficient for the morning negative affect predictor with average pain acceptance, pain catastrophizing, and the DASS total score, is the coefficient of the between-person pain acceptance predictor for someone at their own means for pain, positive affect, and negative affect. is the coefficient of the pain catastrophizing predictor for someone at their own means for pain, positive affect, and negative affect. is the coefficient of the DASS control variable. is a random intercept that captures the between-person variation in the outcome means, and is the level-1 residual.
Likelihood ratio tests from restricted maximum likelihood estimation revealed that daily morning pain ratings, χ2(2) = 8.310, p < .05, and morning positive affect scores, χ2(2) = 18.882, p < .001, required a random slope, indicating that the association between morning pain intensity and evening work goal progress, and the association between morning negative affect and evening work goal progress varied across people. These random slopes are denoted by and , respectively.
Assessment of Mediation
To address research questions regarding the possible mediating effects of pain interference with work goal pursuit on the within-person relationship between morning pain intensity and affect and evening goal progress, PRODCLIN (distribution of the PRODuct Confidence Limits for Indirect Effects; [28]) software was used. MacKinnon and his colleagues have demonstrated through simulation studies that asymmetric confidence limits for the distribution of the product (which are used in PRODCLIN) provide higher statistical power and more adequately controls Type I error rates than do the symmetric confidence limits for the distribution of the product [27, 28]. The observed values for α, ß, the standard error of α, the standard error of ß, the correlation between α and ß, and the Type 1 error rate are entered in the program which calculates the 95% confidence interval for the mediated effect. Following PRODCLIN’s result, the significance of the mediating effect can be determined if zero was not included in the upper and lower limits of the 95% confidence interval.
RESULTS
Data Analysis
Multilevel Modeling (i.e., Hierarchical Linear Modeling) was used to examine the hypothesized model described above. Mplus version 7 [37] with TYPE = TWOLEVEL command was used to estimate a series of multilevel models. In addition, through Mplus alpha and beta path correlations were computed.
Preliminary Analysis
Means and standard deviations were calculated for each of the day-level (Level-1) measures throughout the 21-day period for each participant and for the person-level measures (Level-2). The summary of these findings is depicted in Table 1. The inter correlations among the day-level variables as well as person-level and outcome variables were also calculated. Results of these correlations are presented in Table 1. Most of the inter correlation between the daily measures were significant except that only positive affect was significantly correlated with evening goal progress. As low-to-moderate correlations were obtained between all variables, it appears that the possibility of multicollinearity is mitigated in the multivariate analyses using a set of level-1 predictors. The inter correlations between the level-2 variables indicated that pain acceptance was moderately correlated with pain catastrophizing. The DASS total mean score was also found to be moderately correlated with both pain catastrophizing and acceptance.
Modeling Afternoon Pain Interference with Work-Goal Pursuit
Table 2 gives the parameter estimates, standard errors, and t tests from the analysis of pain interference with work goal pursuit (i.e., the alpha path of the mediation model). Compared to the unconditional model which does not include any predictors, the level-1 predictors reduced the within-person variance from 2.58 to 2.11 (an 18.2% reduction). The results also show a significant positive coefficient for morning pain intensity, such that when a participant experienced greater than usual morning pain intensity, he or she reported more afternoon pain interference with work goal pursuit (p < .001) over and above morning positive and negative affect. On the other hand, morning positive affect was found to be a significant negative within-person predictor (p < .05), suggesting that on days with greater than average positive affect in the morning, people reported less pain interference with work goal pursuit in the afternoon.
Table 2.
MLM Parameter Estimates from the Pain Interference with Work Goal Pursuit Analysis (X→M)
| Parameter | Est. | SE | t | p |
|---|---|---|---|---|
| Intercept | 1.932 | 0.138 | 14.033 | < .001 |
| Pain Intensity (Level-1) | 0.156 | 0.040 | 3.885 | < .001 |
| Positive Affect (Level-1) | −0.149 | 0.044 | −3.377 | < .01 |
| Negative Affect (Level-1) | −0.039 | 0.050 | −0.776 | .438 |
| Pain Acceptance (Level-2) | −0.838 | 0.216 | −3.877 | < .001 |
| Pain Catastrophizing (Level-2) | 0.417 | 0.288 | 1.451 | .147 |
| DASS total (Level-2) | 0.387 | 0.336 | 1.150 | .250 |
| Pain Intensity x Pain Acceptance | −0.149 | 0.064 | −2.322 | < .05 |
| Pain Intensity x Pain Catastrophizing | −0.073 | 0.071 | −1.029 | .303 |
| Intercept Variance | 2.107 | 0.138 | ||
| Pain Intensity Slope Variance | 0.045 | 0.019 | ||
| Negative Affect Slope Variance | 0.050 | 0.026 | ||
| Residual Variance | 2.107 | 0.302 | ||
| Intercept-Slope (Pain) Covariance | 0.074 | 0.059 | ||
| Intercept-Slope (Negative Affect) Covariance | −0.025 | 0.069 |
Note. Wald tests are invalid for variance estimates and are omitted from the table.
The level-2 predictors reduced the between-person variance from 3.04 to 2.11 (a 30.6% reduction). Only pain acceptance was a significant negative level-2 predictor (p < .001), meaning that, after controlling for pain catastrophizing and the DASS total mean score, participants with higher pain acceptance ratings were less likely to report daily pain interference with work goal pursuit in the afternoon. A significant cross-level interaction was found between pain acceptance and morning pain intensity. Pain acceptance moderated the within-person relation between morning pain intensity and afternoon pain interference with work goal pursuit (p < .05) while controlling for pain catastrophizing and the DASS total score. To aid in the interpretation of the moderation effect and to provide a means of clarifying how the relationship between morning pain intensity and afternoon pain interference with work goal pursuit tends to change across levels of pain acceptance, a simple slope analysis, as suggested by Aiken and West [3], was conducted (see Figure 2). A significant positive association between morning pain and afternoon pain’s interference with work goal pursuit emerged when the pain acceptance level was at its mean and one standard deviation below the mean. However, the association was not significant when pain acceptance was at one standard deviation above the mean.
Fig. 2.

Slopes and intercepts portraying the effects of pain acceptance (−1 SD, mean, +1 SD) on the within-person relations between person-centered pain intensity and afternoon pain’s interference with work goal pursuit.
Note. When the ratings of pain acceptance are one standard deviation above the grand mean, ß = 0.067, S.E. = 0.061, p = 0.28. When the ratings of pain acceptance are at the grand mean, ß = 0.156, S.E. = 0.037, p < 0.01. When the ratings of pain acceptance are one standard deviation below the grand mean, ß = 0.250, S.E. = 0.056, p < 0.01.
Contrary to our expectation, pain catastrophizing did not exert a significant main effect to afternoon pain interference with work goal pursuit (p = .147), and the cross-level interaction effect was not significant (p = .303). One of the potential reasons for these null effects is the variance shared between pain catastrophizing and pain acceptance and the DASS total scores. In order to examine whether these null effects are due to these covariates, a post-hoc analysis was conducted excluding these covariates from the model. With the exclusion of these covariates, pain catastrophizing was found to have a significant main effect on the afternoon pain interference with work goal pursuit (B = 1.190, SE = 0.221, p < .001). However, the cross-level interaction between morning pain intensity and afternoon pain interference with work goal pursuit remained non-significant (B = 0.036, SE = 0.059, p = 0.55).
Modeling Evening Work Goal Progress
The parameter estimates, standard errors, and t tests for the baseline model of work goal progress as an outcome are presented in Table 3. Compared to the unconditional model, the level-1 predictors reduced the within-person variance from 3.20 to 2.56 (a 20% reduction), and the level-2 predictors reduced the between-person variance from 2.87 to 2.63 (a 0.7% reduction). Consistent with our expectation, there was a significant negative level-1 coefficient for afternoon pain interference with work goal pursuit. This result implies that when a participant experienced greater than usual pain interference with work goal pursuit in the afternoon, he or she reported a decrease in work goal progress in the evening (p < .01) over and above morning pain and morning positive and negative affect. None of the other level-1 nor any of the level-2 predictors were statistically significant.
Table 3.
MLM Parameter Estimates from the Work Goal Progress Analysis(M→Y controlling for X)
| Parameter | Est. | SE | t | P |
|---|---|---|---|---|
| Intercept | 6.087 | 0.168 | 36.297 | < .001 |
| Pain Interference with Work Goal Pursuit (Level-1) | −0.093 | 0.035 | −2.632 | < .01 |
| Pain Intensity (Level-1) | −0.006 | 0.067 | −0.094 | .925 |
| Positive Affect (Level-1) | 0.036 | 0.084 | 0.432 | .666 |
| Negative Affect (Level-1) | 0.043 | 0.077 | 0.557 | .578 |
| Pain Acceptance (Level-2) | −0.211 | 0.266 | −0.795 | .426 |
| Pain Catastrophizing (Level-2) | −0.202 | 0.334 | −0.605 | .545 |
| DASS total (Level-2) | −0.037 | 0.403 | −0.091 | .928 |
| Intercept Variance | 2.626 | 0.347 | ||
| Pain Intensity Slope Variance | 0.049 | 0.050 | ||
| Positive Affect Slope Variance | 0.154 | 0.099 | ||
| Residual Variance | 2.556 | 0.261 | ||
| Intercept-Slope (Pain) Covariance | −0.037 | 0.111 | ||
| Intercept-Slope (Positive Affect) Covariance | −0.249 | 0.118 |
Note. Wald tests are invalid for variance estimates and are omitted from the table.
Although afternoon pain interference with work goal pursuit was significantly associated with the evening work goal progress, controlling for morning pain intensity, one can still raise the question of whether evening work goal progress is influenced by “afternoon” pain intensity rather than pain interference. Thus, a post-hoc analysis was conducted and it was found that even when “afternoon” pain intensity was controlled in the model, the afternoon pain interference with work goal pursuit still significantly predicted evening work goal pursuit (B = −0.084, SE = 0.038, p < .05). In other words, we can assume that a significant decrease in evening work goal progress is not merely due to morning or afternoon pain intensity, but to one’s perceived pain interference with work goal pursuit.
Results of the Mediation Analyses
In order to evaluate the significance of the mediation effect, the procedure suggested by Mackinnon and colleagues [27, 28] was followed by using PRODCLIN software. It can be concluded that a significant indirect effect exists if zero is not included in the 95% confidence interval.
First, we tested whether morning pain intensity exerts an indirect effect on goal progress in the evening via afternoon pain interference with goal pursuit. The correlation between α and ß was computed and entered into the PRODCLIN software. The estimate of the αß correlation was −0.009. Given our finding that pain acceptance was a statistically significant moderator between morning pain ratings and afternoon pain interference with work goal pursuit, conditional indirect effects were then tested to determine whether the mediated effects differed across levels of pain acceptance. The results showed that when the level of pain acceptance was at its grand mean or one standard deviation below the grand mean, the within-person association between morning pain intensity and evening work goal progress was significantly mediated by afternoon pain interference with work goal pursuit ([95% CI] −0.02904, −0.00329 and [95% CI] −0.04600, −0.00540, respectively). However, the within-person relationship between morning pain intensity and evening work goal progress was not significantly mediated by pain interference with work goal pursuit in the afternoon when pain acceptance was at one standard deviation above the grand mean ([95% CI] −0.02108, 0.00487).
Second, we examined whether morning positive and negative affect exerted indirect effects on evening goal progress. The estimate of the αß correlation was 0.008 and −0.012, respectively. According to the PRODCLIN result, pain interference with work goal pursuit significantly mediated the relationship between morning positive affect and evening goal progress ([95% CI] 0.00271, 0.02918); but not the relation between morning negative affect and evening goal progress ([95% CI] −0.00578, 0.01505).
DISCUSSION
Although chronic pain has been shown to adversely impact cognitive processing, instrumental and communicative behaviors, and various indices of adjustment and well-being, its effects on motivation have, until recently, been relatively under-investigated. The present study demonstrated the subtle influence that pain exerts on work motivation in the form of interference with goal pursuit and goal progress. Figure 3 visually summarizes the findings. The subtlety is illustrated first by the indirect path from pain intensity to work goal progress as mediated by pain’s perceived interference with work goal pursuit, even after controlling for affective states. A second manifestation of subtle motivational processes is revealed by the finding that the mediational effect just noted was itself moderated by pain acceptance. In addition, the fact that positive affect was negatively related to pain’s interference with goal pursuit controlling for morning pain intensity suggests that it may protect individuals with chronic pain against daily pain interference with goal pursuit. In these ways, the motivational face of chronic pain in daily life is becoming clearer.
Fig. 3.

Summary of the present findings
Note. The dashed lines represent non-significant paths. DASS Total = DASS Total Score (Level-2 covariate) * p < .05, ** p < .01, *** p < .001
Previous findings suggest several possible mechanisms that might begin to explain pain’s disruptive effects on goal pursuit. First, although not unequivocally demonstrated, pain may, under certain circumstance, compromise executive functioning [12, 17]. Pain can also disrupt goal pursuit by biasing the individual’s attentional focus toward pain-related goals thereby undercutting the pursuit other important personal objectives [46]. Finally, pain is often catastrophically misinterpreted, thus activating pain-related fear, anxiety, and avoidance [25, 35]. However, not all individuals experience pain’s interference with goal pursuit to the same extent because interference is likely to depend upon pain attitudes. Experimental studies have shown that higher levels of catastrophizing predict greater pain interference during acute pain inductions, but that persons high in pain acceptance are less likely to experience pain interference [38]. Our findings reveal similar patterns, albeit in an extra-laboratory context.
The results of the present study partially supported our hypotheses in that only pain acceptance emerged as a statistically significant cross-level moderator of the within-person relationship between morning pain intensity and pain’s interference with afternoon work goal pursuit. Why did catastrophizing fail to emerge as a moderator? Perhaps, instead of focusing on trait pain catastrophizing, we should have focused on state pain catastrophizing. In other words, the within-person relationship between pain intensity and pain’s interference with goal pursuit may be contingent upon whether increases in pain intensity are accompanied by increases in catastrophic thoughts about pain involving rumination, magnification, and hopelessness. By using cognitive resources, in-the-moment catastrophic thinking could amplify the disrupting influence of fluctuations in pain intensity on the pursuit of work goals. Hence, we recommend that future studies examine the moderating role of both state and trait pain catastrophizing.
Speculating on why pain acceptance acted as a moderator, we note that acceptance implies more than simply ignoring or distracting one’s attention away from pain. Rather, it involves decreasing unnecessary rumination about pain avoidance and pain control while pursing valuable goals even in the presence of pain [35]. Thus, individuals with high levels of pain acceptance may not be as readily interrupted by pain flares during the course of their daily work-goal pursuits.
Affect is known to influence higher level cognition including the processing and interpretation of information, reasoning, and judgment [5]. Positive affect in particular has been recognized as a potential source of resilience among individuals with chronic pain [51]. The present study found preliminary but nonetheless useful evidence of the role played by positive affect in the reduction of pain’s interruptive effects on goal pursuit among persons with chronic pain. During times when our study participants experienced more than usual positive affect in the morning, they were less likely to experience pain-related interference with the pursuit of important work goals (an effect that holds even morning negative affect and pain intensity are controlled). This finding extends previous research on the relation between positive affect and a construct called primary control striving, the motivation to invest time and effort to overcome obstacles [20]. In two longitudinal studies, Haase, Poulin, and Heckhausen [18] showed that positive affect can lead participants to believe that they have more control over the attainment of their goals (i.e., career and educational goals), which, in turn, significantly elevated their motivation to invest further time and effort toward achieving these goals. Participants also appeared more likely to overcome obstacles in the pursuit of their goals. Although in the present study we did not measure the primary control strivings of our sample, a conceptual bridge can nonetheless be erected suggesting that the experience of increased positive affect may elevate primary control striving, which, in turn, may down-regulate pain’s deleterious effects on work goal pursuit.
Contrary to our expectations, morning negative affect was not significantly associated with pain interference with work goal pursuit and work goal progress. One potential explanation for these null findings may be linked to the level of negative affect reported by our participants. Although the negative affect scale ranged from 0 to 9, the mean and standard deviation for morning negative affect in the present study was 1.15 and 1.66, respectively. Even individuals two standard deviations above the mean on the morning negative affect scale (4.5) are located only at the scale’s midpoint. Therefore, the low level of daily negative affect may have contributed to its small association with goal pursuit processes after controlling for pain intensity and positive affect. Another possible explanation for this null finding is that negative affect can have facilitative as well as detrimental effects on self-regulatory processes. For instance, findings of a study by Forgas [14] suggest that moderate levels of negative affect are associated with a decrease in judgmental errors and an improvement in memory and motivation. Controlled experiments can perhaps shed additional light on the complex associations between negative affect and goal pursuit.
Limitations
Methodological limitations of the present study also need to be acknowledged. First, readers should be cautious in generalizing the results because the sample recruited for the present study consisted of non-clinically-referred individuals with chronic pain. Second, the results are based solely on the self-report measures assessed in the daily diary. Although diary data can mitigate problems associated with recall bias [44], depending solely on diary-obtained self-reports might lead to erroneous conclusions. To reliably assess a person’s progress on work-related goals, self-reports should be supplemented by peer and/or supervisor ratings of progress.
Implications for Future Studies
Despite its limitations, the current study provides some stepping stones for future research. First, in order to generalize the present findings, replication is called for using clinical samples of working adults with diverse pain conditions. Second, the co-occurrence of work-related and non-work- goals might be particularly relevant for individuals with chronic pain. Although pain-related goals (e.g., controlling pain and avoiding situations that may cause pain) are among the most highly sought after outcomes, the pursuit of such goals can impede the pursuit of other important personal objectives [46]. Understanding the relations between pain-related and other important personal goals in a within-day analytic framework may prove to be invaluable in treatment planning for persons with chronic pain. In addition, further investigations are required examining the mitigating effect of pain acceptance on the positive relationship between pain intensity and pain interference with work goal pursuit. A psychological intervention particularly relevant in this regard is Acceptance-Commitment Therapy (ACT) [6, 34, 49], a method that has been found to enhance psychosocial and physical functioning among individuals with chronic pain [33, 49, 50]. Thus, testing the present model in a randomized controlled ACT intervention with working adults, employing diary methods and multiple observers of varied goal activities (its pursuit, progress, interference, revision, and the like) could be a particularly productive research direction. Finally, as goals do not achieve themselves, future research on the role of personal goal striving and chronic pain should include measures of self-regulatory skills and competencies, both as stable level-2 (between- person) and as time- and context-varying level-1 (within-person) factors.
Acknowledgements
This research was supported in part by the National Institute of Nursing Research grant 5-R21NRO10752–02. We are especially indebted to Dr. Barbara Huff for her assistance in the conduct of this research and Mirna Hodzic Mun for her comments on a revision of this paper. This study has been presented at the 26th Association for Psychological Science Annual Convention, San Francisco, California in 2014.
Footnotes
Conflict of Interest
Paul Karoly is co-developer of Profile of Chronic Pain: Screen (PCP: S) an instrument used in the present research.
References
- [1].Affleck G, Tennen H, Urrows S, Higgins P, Abeles M, Hall C, Karoly P, Newton C. Fibromyalgia and women’s pursuit of personal goals: a daily process analysis. Health Psychol 1998; 17: 40–7. [DOI] [PubMed] [Google Scholar]
- [2].Affleck G, Tennen H, Zautra A, Urrows S, Abeles M, Karoly P. Women’s pursuit of personal goals in daily life with fibromyalgia: A value-expectancy analysis. J Consult Clin Psych 2001; 69:587–96. [DOI] [PubMed] [Google Scholar]
- [3].Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Newbury Park: Sage, 1991. [Google Scholar]
- [4].Antony MM, Bieling PT, Cox BJ, Enns MW, Swinson RP. Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychol Assessment 1998; 10: 176–81. [Google Scholar]
- [5].Blanchette I, Richards A. The influence of affect on higher level cognition: A review of research on interpretation, judgment, decision making and reasoning. Cogn Emot 2010; 24: 561–95. [Google Scholar]
- [6].Buhrman M, Skoglund A, Husell J, Bergström K, Gordh T, Hursti T, Bendelin N, Furmark T, Andersson G. Guided internet-delivered acceptance and commitment therapy for chronic pain patients: A randomized controlled trial. Behav Res Ther 2013; 51(6): 307–15. [DOI] [PubMed] [Google Scholar]
- [7].Carver CS., Lawrence JW, Scheier MF. A control-process perspective on the origins of affect In: Martin LL, Abraham T, editors. Striving and feeling: Interactions among goals, affect, and self-regulation, Mahwah, NJ: Erlbaum; 1996; pp. 10–51. [Google Scholar]
- [8].Carver CS, Scheier MF. Origins and functions of positive and negative affect: A control process view. Psychol Rev 1990; 97: 19–35. [Google Scholar]
- [9].Crawford JR, Henry JD. The Depression anxiety stress scales (DASS):Normative data and latent structure in a large non-clinical sample. Brit J Clin Psychol 2003; 42: 111–31. [DOI] [PubMed] [Google Scholar]
- [10].Crombez G, Viane I, Eccleston C, Devulder J, Goubert L. Attention to pain and fear of pain in patients with chronic pain. J Behav Med 2013; 36:371–8. [DOI] [PubMed] [Google Scholar]
- [11].Custers R, Aarts H. Positive affect as implicit motivator: On the non-conscious operation of behavioral goals. J Pers Soc Psychol 2005; 89:129–42. [DOI] [PubMed] [Google Scholar]
- [12].Eccleston C Chronic pain and distraction: An experimental investigation into the role of sustained and shifting attention in the processing of chronic persistent pain. Behav Res Ther 1995; 33: 391–405. [DOI] [PubMed] [Google Scholar]
- [13].Enders CK, Tofighi D. Centering predictor variables in cross-sectional multilevel models: a new look at an old issue. Psychol Methods2007; 12: 121–138. [DOI] [PubMed] [Google Scholar]
- [14].Forgas JP. Don’t worry, be sad! On the cognitive, motivational, and interpersonal benefits of negative mood. Curr Directions in Psychol Sci 2013; 22:225–32. [Google Scholar]
- [15].Fredrickson BL. What good are positive emotions? Review of General Psychology1998; 2: 300–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Gray JA. Personality dimensions and emotion systems In: Ekman P, Davidson J, editors. The nature of emotion: Fundamental questions. New York: Oxford University Press; 1994. pp. 329–331. [Google Scholar]
- [17].Grisart JM, Plaghki LH. Impaired selective attention in chronic pain patients. Eur J Pain1999; 3: 325–33. [DOI] [PubMed] [Google Scholar]
- [18].Haase CM, Poulin MJ, Heckhausen J. Happiness as a motivator: positive affect predicts primary control striving for career and educational goals. Pers Soc Psychol Bull 2012; 38:1093–104. [DOI] [PubMed] [Google Scholar]
- [19].Hamilton NA, Karoly P, Kitzman H. Self-regulation and chronic pain: The role of emotion. Cog Therapy Res 2004; 28(5): 559–76. [Google Scholar]
- [20].Heckhausen J, Wrosch C, Schulz R. A motivational theory of life-span development. Psychol Rev 2010; 117(1): 32–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Karoly P, Ruehlman LS. The motivational implications of pain: Chronicity, psychological distress, and work goal construal in a national sample of adults. Health Psychol 1996; 15: 383–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Karoly P, Ruehlman LS. Psychosocial aspects of pain-related life task interference: An exploratory analysis in a general population sample. Pain Med 2007; 8(7): 563–72. [DOI] [PubMed] [Google Scholar]
- [23].Keefe FJ, Brown GK, Wallston KA, Caldwell DS.Coping with rheumatoid arthritis pain: catastrophizing as a maladaptive strategy. Pain 1989; 37: 51–6. [DOI] [PubMed] [Google Scholar]
- [24].Kratz AL, Davis MC, Zautra AJ. Pain acceptance moderates the relation between pain and negative affect in female osteoarthritis and fibromyalgia patients. Ann Behav Med 2007; 33: 291–301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Leeuw M, Goossens MEJB, Linton SJ, Crombez G, Boersma K,Vlaeyen JWS.The fear6avoidancemodel of musculoskeletal pain: current state of scientific evidence. J Behav Med 2007; 30:77–94. [DOI] [PubMed] [Google Scholar]
- [26].Lovibond SH, Lovibond PF. Manual for the depression anxiety stress scales (2nd ed). Sydney: Psychology Foundation, 2002. [Google Scholar]
- [27].MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods 2002; 7: 83–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivar Behav Res 2004; 39: 99–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Maes S, Karoly P. (2005). Self-regulation assessment and intervention in physical health and illness: A review. Appl Psychol 54: 267–299. [Google Scholar]
- [30].McCracken LM. Learning to live with the pain: acceptance of pain predicts adjustment in persons with chronic pain. Pain 1998; 74: 21–7. [DOI] [PubMed] [Google Scholar]
- [31].McCracken LM, Eccleston C. Coping or acceptance: what to do about chronic pain? Pain 2003; 105(1–2), 197–204. [DOI] [PubMed] [Google Scholar]
- [32].McCracken LM, Eccleston CA. Prospective study of acceptance of pain and patient functioning with chronic pain. Pain 2005, 118: 164–9. [DOI] [PubMed] [Google Scholar]
- [33].McCracken LM, Gutiérrez-Martínez O. Processes of change in psychological flexibility in an interdisciplinary group-based treatment for chronic pain based on Acceptance and Commitment Therapy. Behav Res Ther 2011; 49: 267–74. [DOI] [PubMed] [Google Scholar]
- [34].McCracken LM, Jones R. Treatment for chronic pain for adults in the seventh and eighth decades of life: A preliminary study of acceptance and commitment therapy (ACT). Pain Med 2012; 13: 861–7. [DOI] [PubMed] [Google Scholar]
- [35].McCracken LM, Vowles KE, Eccleston, C. Acceptance of chronic pain: Component analysis and a revised assessment method. Pain 2004; 107: 159–66. [DOI] [PubMed] [Google Scholar]
- [36].McCracken LM, Vowles KE. Acceptance of chronic pain. Curr Pain and Headache Rep 2006; 10: 90–4. [DOI] [PubMed] [Google Scholar]
- [37].Muthén LK, Muthén BO. Mplus user’s guide. 7th ed Los Angeles, CA: Muthen & Muthen, 2012. [Google Scholar]
- [38].Richardson EJ, Ness TJ, Doleys DM, Baños JH, Cianfrini L, Richards JS. Catastrophizing, acceptance, and interference: Laboratory findings, subjective report, and pain willingness as a moderator. Health Psychology 2010; 29: 299–306. [DOI] [PubMed] [Google Scholar]
- [39].Ruehlman LS, Karoly P, Newton C, Aiken LS. The development and preliminary validation of a brief measure of chronic pain impact for use in the general population. Pain 2005; 113: 1–10. [DOI] [PubMed] [Google Scholar]
- [40].Ruehlman LS, Karoly P, Taylor A. Perceptions of chronic pain’s interference with sexual functioning: The role of gender, treatment status, and psychosocial factors. Sex Disabil 2008; 26(3): 123–36. [Google Scholar]
- [41].Sturgeon JA, Zautra AJ. State and trait pain catastrophizing and emotional health in rheumatoid arthritis. Ann Behav Med 2013; 45: 69–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Sullivan MJL, Bishop SR, PivikJ. The pain catastrophizing scale: development and validation. Psychol Assessment 1995; 7: 524–32. [Google Scholar]
- [43].Sullivan MJL, Thorn B, Haythornthwaite JA, Keefe F, Martin M, Bradley LA, Lefebvre JC. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 2001; 17: 52–64. [DOI] [PubMed] [Google Scholar]
- [44].Tennen H, Affleck G. Daily processes in coping with chronic pain: Methods and analytic strategies In:Zeidner M, Endler N, editors. Handbook of Coping: Theory, Research, and Applications, New York: Wiley & Son,; 1996, pp. 151–177. [Google Scholar]
- [45].Turner JA, Jensen MP, Warms CA, Cardenas DD. Catastrophizing is associated with pain intensity, psychological distress, and pain-related disability among individuals with chronic pain after spinal cord injury. Pain 2002; 98: 127–34. [DOI] [PubMed] [Google Scholar]
- [46].Van Damme S, Legrain V, Vogt J, Crombez G. Keeping pain in mind: A motivational account of attention to pain. Neurosci Biobehav Rev 2010; 34: 204–13. [DOI] [PubMed] [Google Scholar]
- [47].Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain 2000; 85: 317–32. [DOI] [PubMed] [Google Scholar]
- [48].Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J Pers Soc Psychol 1988; 4(6): 1063–70. [DOI] [PubMed] [Google Scholar]
- [49].Wetherell JL, Afari N, Rutledge T, Sorrell JT, Stoddard JA, Petkus AJ, Solomon BC, Lehman DH, Liu L, Lang AJ, Atkinson JH.A randomized, controlled trial of acceptance and commitment therapy and cognitive-behavioral therapy for chronic pain. Pain 2011; 152(9): 2098–107. [DOI] [PubMed] [Google Scholar]
- [50].Wicksell RK, Ahlqvist J, Bring A, Melin L, Olsson GL. Can exposure and acceptance strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (WAD)? A randomized controlled trial. Cog Behav Ther 2008; 37: 169–82. [DOI] [PubMed] [Google Scholar]
- [51].Zautra AJ, Johnson LM, Davis MC. Positive affect as a source of resilience for Women in chronic pain. J Consult Clin Psychol 2005;73(2): 212–20. [DOI] [PMC free article] [PubMed] [Google Scholar]