

Abstract
Background
One Health is receiving attention for arbovirus infection prevention and control and for defining national “intersectoral” priorities. Increasing awareness of intersectoral priorities through multisectorial risk assessments (MRA) is promising, where data are not systematically shared between sectors. Towards this aim, the MediLabSecure project organized three MRA exercises (hereby called exercises): one on West Nile virus, one on Crimean–Congo haemorrhagic fever, and one on Rift Valley fever, assessing the added value of this approach.
Methods
The exercises relied on RA methodologies of international organisations. Country representatives of the human and animal virology, medical entomology, and public health sectors (hereby called “sectors”) involved in the surveillance of vector-borne diseases participated in the exercises. Background documentation was provided before each exercise, and a guide was developed for the facilitators. All three exercises included technical and methodological presentations and a guided RA directed at bringing into play the different sectors involved. To assess the added value of the approach, each participant was asked to rank the level of perceived benefit of the multisectoral collaboration for each “risk question” included in the exercises.
Results
In total, 195 participants from 19 non-EU countries in the Mediterranean and Black Sea regions took part in the exercises. The participants assessed the multisectoral approach as valuable in analysing comprehensively the situation by having access to information and knowledge provided by each of the sectors involved. Sharing of information and discussion facilitated reaching a consensus on the level of risk in each country.
Conclusions
Increasing awareness of intersectoral priorities, including cross-border ones, through MRA is relevant to reduce gaps due to unavailability of shared data and information. Given that six out of the ten threats to global health listed by WHO are occurring at the human-animal-environmental interfaces, comprehensive regional RA with a One Health approach made by national authorities can be a relevant added value for the global health security.
1. Introduction
Integrated surveillance is considered a promising working strategy [1–4] to enhance early warning of emerging infections such as arboviral diseases. In addition to providing early signals, integrated surveillance by systematically integrating multiple sources of surveillance data in a timely manner (indicator- and event-based surveillance, case-based surveillance, vector surveillance, and virus and environmental data and information) could contribute more effectively to accurate risk assessments (RA) [5]. Unfortunately, very few countries worldwide [6–8], and in the Mediterranean Region [9,10], have managed to collect and analyse surveillance data across sectors related to arbovirus transmission, and even fewer have interoperable databases. Ultimately, this limits early warning and risk assessment capacity with impact on the prevention and control of arbovirus infections. This is in line with the recognised challenges of sharing data and information, although the evidence for the public health benefits of sharing is growing with well-documented instances of an improved outcome as a result of sharing surveillance data [11–16]. Efficient data sharing also prompted an early response to the emergence of the H7N9 influenza virus in humans in China [14]; conversely, reluctance to share can hinder or slow down the response and global outbreaks have shown that inadequate surveillance and response capacity in a single country can endanger national populations and the public health security of the entire world [13]. One relevant issue is how to enhance trust within and between countries, considering that trust facilitates the sharing of data and information. Trust-building measures can take the form of face-to-face meetings, regular regional workshops, desktop exercises, joint outbreak investigations, and networking activities. These promote the sense of working towards a common goal [11].
To this aim, working with a multisectoral and transdisciplinary approach, often mentioned as a One Health approach, can help to mediate different assumptions and views and to fill knowledge gaps [17–20].
Focusing specifically on those threats which occur at the animal-human-ecosystem interfaces, several international organisations, including the World Health Organization (WHO), Food and Agriculture Organization of the United Nations (FAO), World Organisation for Animal Health (OIE), and World Bank, have recognised the critical role of multisectoral risk assessment (MRA) (multisectoral risk assessment (MRA): assessment with the concomitant participation of all the relevant sectors involved in the surveillance of a given arbovirus infection) to enhancing cross-sectoral collaboration and improving data collection and data-sharing from different sectors [21–24].
In fact, for health threats that are either emerging or existing at the interface, including food safety issues, neither the technical data nor other information important to conduct a comprehensive assessment nor the appropriate breadth of technical expertise and experience are routinely available within a single agency or sector [22].
In the dimension of capacity building and training, risk assessment exercises implemented with a multisectorial approach can foster data and information sharing across sectors reducing information gaps, highlight experiences and contributions across countries, develop the concept of a national/regional “cross-sectoral” risk assessment outcome, and guide prioritisation of actions and allocation of funds also taking into account the cross-border dimension.
In fact, regional public health threats are often presenting common characteristics such as the need of joint prevention and response activities, common coordination, and comprehensive lessons learned analysis across the actors involved, especially at borders (see the cases of Crimean–Congo haemorrhagic fever cluster in 2008 at the borders between Greece and Bulgaria [25] and in 2009 between Georgia and Turkey [26]).
These characteristics can be easily integrated in the framework of MRA.
Towards this aim, we organized three MRA exercises: one on West Nile virus (WNV) infection, one on Crimean–Congo haemorrhagic fever (CCHF), and one on Rift Valley fever (RVF) in the framework of the MediLabSecure (MLS) project [27].
The aim of these exercises was not only to formulate more reliable risk assessments but also to promote a process leading to a homogenous understanding of risk across different sectors in a given country, and across neighbouring countries, using a structured strategy of assessment. This article describes their implementation and discusses the added value of the adopted multisectoral approach.
2. Materials and Methods
The MLS project started in 2014 and aims at consolidating a regional network of public health institutions and laboratories, belonging to 19 non-European Union (EU) countries (Albania, Algeria, Armenia, Bosnia and Herzegovina, Egypt, Georgia, Jordan, Kosovo, Lebanon, Libya, Moldova, Montenegro, Morocco, Palestine, Former Yugoslav Republic of Macedonia, Serbia, Tunisia, Turkey, and Ukraine), for the control of zoonotic emerging viruses. It represents a cluster for awareness, risk assessment, surveillance, monitoring, and control of relevant emerging diseases, with special focus on arbovirus infections.
In this context, we designed three MRA exercises in coordination with the MLS working group and the subject-matter experts of the European Centre for Disease Prevention and Control (ECDC) and of the Italian Animal Health Institute “Istituto Zooprofilattico Sperimentale dell'Abruzzo e del Molise (IZSAM).”
For the development of the three MRA exercises, we relied on the following existing RA methodology and guidance documents: the ECDC “WNV risk assessment tool” [28], the ECDC “operational guidance on rapid risk assessment (RRA) methodology” [29], and the Food and Agriculture Organization of the United Nations (FAO) methodology of “The RVF in Niger: Risk Assessment” [30]. All mentioned tools and guidance documents were developed by subject-matter experts, had been piloted in other contexts, and were in line with the pathogens and methodological priorities identified by the MLS countries.
We invited country representatives of the human virology, animal virology, medical entomology, and public health sectors (hereby called “sectors”) involved in the surveillance of vector-borne diseases to participate in the three MRA exercises. Background documentation (including selected references) was sent by e-mail to participants one week before each exercise. An exercise implementation guide was also developed and sent to the facilitators together with the background documentation. The participants were asked to send national epidemiological data on the concerned pathogens that were then shared with all participants. At the start of each exercise session, participants were provided with a participant's guide.
All three exercises developed in three phases, the first always consisted in technical and methodological presentations by subject-matter experts. The second and third phases differed as shown in Table 1.
Table 1.
Overview of the three multisectoral risk assessment exercises conducted, Source: [31].
| Exercise (place and date) | Participant countries from MediLabSecure network | Objectives | Methodology | Guidance documents |
|---|---|---|---|---|
| West Nile virus exercise (Paris, December 2015) | Albania, Algeria, Armenia, Bosnia and Herzegovina, Egypt, Georgia, Jordan, Kosovo, Lebanon, Libya, Moldova, Montenegro, Morocco, Palestine, former Yugoslav Republic of Macedonia (FYROM), Serbia, Tunisia, Turkey, and Ukraine | (i) Describe risk level assessment between sectors and countries (ii) Assess the cross-sectoral collaboration during the initial phase of the MediLabSecure project (iii) Make participants aware of the ECDC tool (iv) Provide indications for the next MRA exercises |
(1) Map the assessment of WNV risk across four sectors (human and animal virology, medical entomology, and public health) by country and by regions (2) Conduct a SWOT analysis to assess strengths, weaknesses, opportunities, and threats in relation to the surveillance systems in place at national level, to support the risk assessment (3) Compile an evaluation questionnaire on exercise satisfaction |
ECDC “West Nile virus risk assessment tool” [28] |
|
| ||||
| Crimean–Congo haemorrhagic fever exercise (Belgrade, November 2016) | Albania, Armenia, Bosnia and Herzegovina, Former Yugoslav Republic of Macedonia (FYROM), Georgia, Kosovo, Moldova Montenegro, Serbia, Turkey, and Ukraine | (i) Enhance knowledge and capacity on MRA (ii) Encourage multisectoral collaboration and exchange, also among neighbouring countries and assess the related added value (iii)Provide consensus on a single national level of risk across all the sectors (iv) Make participants aware of ECDC RRA guidance and FAO RA methodology (v) Make participants aware of ECDC RRA guidance and FAO RA methodology |
(1) Table0top exercise on multisector risk assessment with four sectors (human and animal virology, medical entomology, and public health) by country and by regions (2) Questionnaire on the value of multisector approach (3) Evaluation questionnaire on exercise satisfaction |
ECDC “operational guidance on rapid risk assessment methodology” [29] FAO “RVF in Niger risk assessment” [30] |
Additional details on the developed exercises, background documents, and guidance for facilitators and participants are available in the MRA exercise reports [32–34].
The added value of the multisectoral approach during the CCHF and the RVF assessments was collected by asking each participant to rank (high, medium, or low) the level of perceived benefit of the multisectoral collaboration when answering each “risk question” included in the exercises.
Pre- and posttest questionnaires, designed to assess if the MRA had increased the participant's knowledge, were prepared and submitted for the CCHF (Annex 5 of [33]) and RVF (Annex 6 of [34]) exercises. We deemed that, considering the aim of the exercises, it would have been particularly important to assess knowledge of participants on key parameters on which to rely on for the assessment, notably, surveillance data, source, and type of information and disease/infection risk factors.
Participants were also asked to compile an exercise evaluation form (Annex 6 of [34]) at the end of each exercise to provide MediLabSecure project with feedback on the quality and the pertinence of the training sessions.
2.1. The WNV Exercise
All the 19 countries involved in the MLS network took part in the exercise (Table 1). The participants were divided in smaller groups by country according to regional proximity.
Each participant was asked to identify the risk area typology that was mostly representative of his/her country on the basis of the six risk area types defined by ECDC for WNV transmission (Figure 1).
Figure 1.
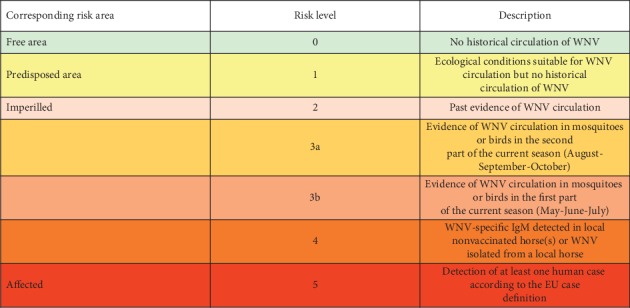
Seasonal risk levels of WNV transmission to humans with the corresponding risk area and the indicators used to define the level (source ECDC), Source: [28].
Subsequently, the participants discussed the reasons for their identified risk area in groups, considering both national and cross-border factors. They were allowed to modify their risk area after the discussion. Then, the participants discussed in country groups the level of risk with regard to national surveillance system characteristics using the SWOT [35] analysis framework (strengths, weaknesses, opportunities, and threats analysis) guided by the ECDC tool [28]. The final risk area typology and the main aspects that had emerged from all the national SWOT analyses were presented and discussed in plenary with all other groups [31].
2.2. The CCHF Exercise
CCHF MRA was implemented with the countries of the Balkans and Black Sea Region of MLS (Table 1) that considered this disease as a priority for the area. The exercise was developed by adapting the information table for rapid risk assessment and the risk-ranking algorithm of the ECDC operational guidance on rapid risk assessment methodology (Annex 2 and 3 in [33]) to rate the potential of CCHF virus transmission in each participating country integrating the views of the different sectors. The assessment was done in two steps: first, the participants assessed the risk in small groups of neighbouring countries on the basis of the information delivered with the technical presentations, available national data, and the background document sent in advance; second, an assessment was made by each country over the different sectors. Each country provided the multisectoral added value to the rapporteur for plenary audience restitution.
2.3. The RVF Exercise
The RVF exercise was implemented with the countries of North Africa and the Middle East Region of MLS (Table 1) which considered RVF a priority for the area. The RVF exercise was developed by adapting the risk questions of the FAO RVF in Niger Risk assessment (Annex 3 in [34]) to identify the risk of RVF virus infection introduction, spread and/or persistence in each participating country. As for the CCHF exercise, the participants were divided in small groups of neighbouring countries to discuss the regional situation with the colleagues of the other sectors in the group.
For the last phase, the group was divided by country with all sectors represented because the expected outcome was the level of risk by country. Each country provided the multisectoral added value to the rapporteur for plenary audience restitution.
3. Results
A total of 159 participants from the 19 non-EU countries of the MLS network took part in the three exercises: 73 participants in the WNV, 42 in the CCHF, and 44 in the RVF exercise.
3.1. The WNV Exercise
The WNV exercise highlighted a high heterogeneity in assessing the level of risk across the involved sectors. The sharing of information and discussion between sectors and neighbouring countries reduced intersectoral variability towards a single level of risk in each country.
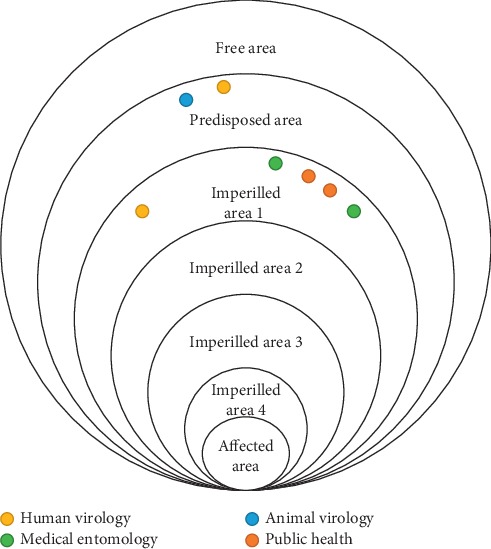
Each participant was provided with dots coloured as per his/her sector (i.e., yellow for human virology, blue for animal virology, green for medical entomology, and red for public health), and these dots were used to mark the identified risk area on a wall poster.
As an example, we report here the outcomes of two groups. In Figure 2, country 1 assessed risk level 5 (affected risk area), country 2, risk level 2 (imperilled risk area), and country 3, risk level 1 (predisposed risk area) with final good agreement between different sectors within country. In Figure 3, countries 1 and 2 assessed risk level as 1 and 2, respectively, without final agreement between different sectors in one country.
Figure 2.

Perceived risk of West Nile virus using the ECDC risk assessment tool. Risk areas identified by three countries with consensus between sectors.
Figure 3.
Perceived risk of West Nile virus using the ECDC risk assessment tool. Risk areas identified by two countries with less consensus between sectors.
The SWOT analysis underlined the critical role of integrated surveillance systems, laboratory capacity, and intersectoral collaboration for reliable risk assessments of arbovirus infections. The implementation of the first MRA exercise on WNV highlighted the need for enhancing the collaboration between sectors to reduce heterogeneity in risk assessment and for analysing the added value of a multisectoral approach.
3.2. The CCHF Exercise
3.2.1. Knowledge and Capacity
The results of the pre- and posttests completed by thirty-five (83%) participants of CCHF exercise showed that the exercise led to improvements in the capacity to determine risk factors and to identify sources of reliable information to assess the risk. For example, with reference to the question of the test “Would CCHF be an unusual or unexpected threat in your country?”10 out of 35 (29%) of the respondents replied “yes” in the pretest, while in the posttest, all the respondents (35) replied “no” to this question. This suggests that the discussion between countries and the assessment exercise helped to identify possible risk factors also at cross-border or regional level (i.e., knowledge that neighbouring countries host the pathogen).
Regarding documentation for risk assessment, we reported in Table 2 the documents mentioned by the participants to assess the level of risk for CCHF in their country.
Table 2.
Number of participants of the CCHF exercise who identified useful documents for RA, by type of document.
| Type of document | Pretest | Posttest | ||
|---|---|---|---|---|
| N participants | Percentage | N participants | Percentage | |
| No documents mentioned | 9 | 25 | 2 | 6 |
| Guidance, law decrees, plans | 22 | 63 | 17 | 49 |
| Guidance, law decrees, plans, scientific articles, unpublished documents, studies | 2 | 6 | 14 | 39 |
| Scientific articles | 2 | 6 | 2 | 6 |
| Total responders | 35 | 100 | 35 | 100 |
3.2.2. The Added Value of the Multisectoral Approach
The added value of the concomitant participation of several sectors to the RA for each risk question of the exercise is reported in Figure 4. These specific aspects related to the added value of the exercise were considered particularly relevant by the project's stakeholders and therefore reported in the MediLabSecure Strategic Document [31] for further developments.
Figure 4.
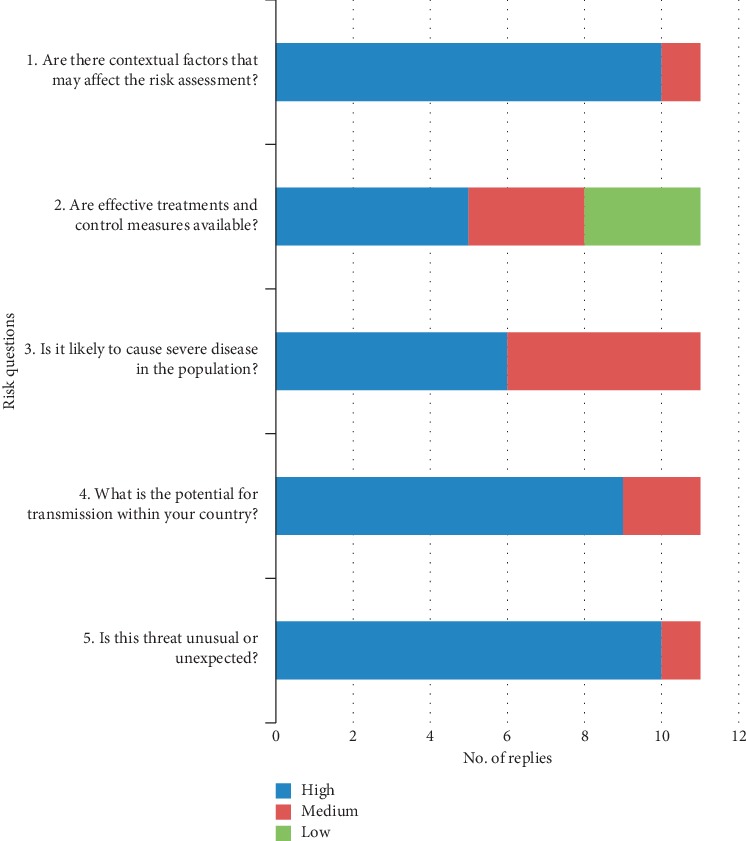
Added value of the multisectoral approach as assessed by participants to the CCHF exercise (11 countries).
The multisectoral approach was assessed as particularly valuable in “setting the scene” and in analysing comprehensively the situation having access to information and knowledge provided by each of the sectors involved in the exercise (see the added value for risk questions 1 and 5 in Figure 4 and data analysis in additional file 1).
3.3. The RVF Exercise
3.3.1. Knowledge and Capacity
The results of the pre- and posttests, completed by twenty-one (48%) participants of the RVF exercise, showed that the exercises led to improvements in the capacity to determine risk factors. Although the participants were all able to identify several relevant risk factors, some specific risks were only identified in the posttest. Among them “animal movements” included by 11 (52%) and 10 (48%), as relevant risk of spread of the virus in endemic and new areas, respectively, “social and economic instability” included by six (29%) both as relevant risk of endemic and new areas, and “climate changes” included by eight (38%) and seven (33%) as relevant risk of endemic and new areas, respectively. In relation to “list kind of documents to rely on to assess the level of risk for RVF in your country,” in total, 18 (88%) and 19 (90%) of participants were able to mention kind of documents useful for RA of RVF in their countries in pre- and posttest, respectively.
3.4. The Added Value of the Multisectoral Approach
The country perception of the added value of the multisectoral approach is reported in Figure 5. Also, for this exercise, the multisectoral approach was particularly valuable in “setting the scene” and in analysing comprehensively the situation having access to wide range of information and knowledge provided by each of the sectors involved in the exercise (see the added value for risk questions 3, 4, and 6 in Figure 5 and data analysis in additional file 1). As for CCHF and also for RVF, the aspects related to the added value of the exercise were considered particularly relevant by the project's stakeholders and therefore reported in the MediLabSecure Strategic Document [31].
Figure 5.
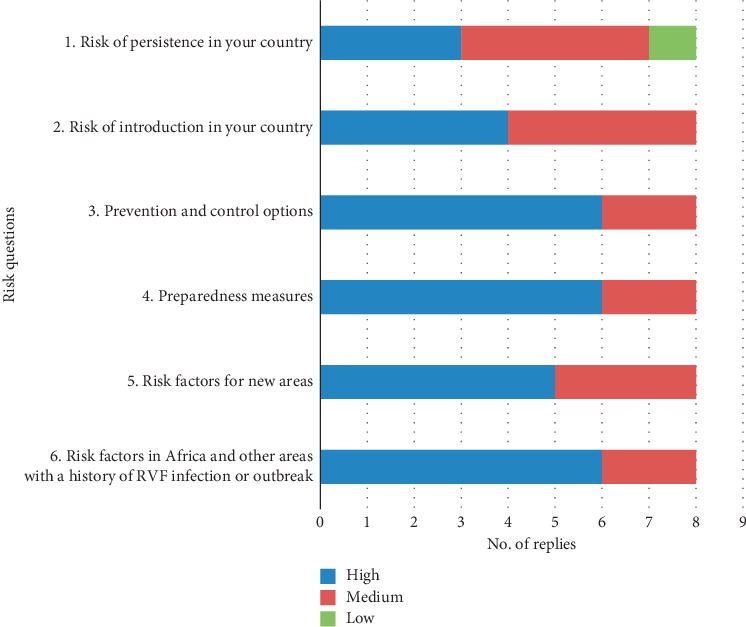
Added value of the multisectoral approach as assessed by participants to the RVF exercise (8 countries).
3.5. Results of the Evaluation of Three Exercises
Response rates to the evaluation questionnaire were 90% (66/73), 88% (37/42), and 68% (30/44) for WNV, CCHF, and RVF exercises, respectively.
Overall, 92% (WNV), 94% (CCHF), and 83% (RVF) of respondents found the exercise satisfactory. Ninety percent or more of respondents for each exercise found the discussion between sectors useful to identify the level of risk.
Almost all respondents reported that the objectives of the exercises were clearly communicated (99% for the WNV MRA exercise, 89% for the CCHF MRA, and 83% for the RFV MRS), while agreement on the appropriateness of the time allotted for the exercises was 92% for both WNV and CCHF and just 54% for the RVF exercise (see data analysis in additional file 1).
4. Discussion
As reported, the main aims of these exercises were to increase knowledge on MRA and raise awareness of multisectoral collaboration for conducting risk assessment of arbovirus infection with a One Health approach in the Mediterranean region. Using available tools and guidance documents allowed to avoid duplications and to refer to existing recognized published guidance.
Also, using different guidance documents helped to identify methods needed to facilitate risk assessments. For example, the WNV and CCHF exercises seem to have been facilitated by the concomitant presence of “risk questions” and algorithms in the method that guide in a stepwise manner the participants towards the final assessment. The RVF exercise instead relied only on “risk questions” to guide the participants. Replying to those questions might be difficult for people not familiar with RA methodologies and/or without access to relevant information and data. This has probably generated the perception of lack of adequate time allotted for the RVF exercise, and it is also in line with the best practice identified for a joint risk assessment by WHO-OIE-FAO [21]: “at least one member of the Joint Risk Assessment (JRA) Technical Team should have experience in risk assessment to guide the process and advise on the JRA methodology.”
Considering that different sectors may rightfully assess the risk differently, this approach has the advantage of enabling actors in each sector to recognize this variability and the reasons behind it. This awareness is a first step towards the identification of national intersectoral priorities in terms of surveillance and response that, in turn, can guide a OneHealth approach to resource allocation. In fact, MRA can facilitate prioritization of zoonosis in line with other proposed integrated approaches [19, 21, 36] and, in addition, allow joint evaluation of the risk of a specific zoonosis and prepare for a coordinated integrated response.
The pre- and posttests implemented during the exercises have highlighted that many participants did not perceive the relevance and need of recent published and unpublished documents (including those from neighbourhood countries) to support risk assessments. The exercises helped in understanding the relevance of different sources of information and data for RAs. However, it has to be noted that, in order to save time during the implementation, the ISS team searched and analysed in advance the available relevant documentation and synthetized the outcomes of the research in background documents distributed to participants. Data review was therefore not fully simulated. The identification of relevant sources of information by each of the sectors involved in the assessment and their sharing is the first step of the RA, and it should be considered among the relevant outcomes of intersectoral collaboration.
As highlighted by the WNV exercise, the multisectoral collaboration helped in the identification of the level of risk, and with the CCHF and RVF exercises, we explored at what stage of the RA this collaboration was more beneficial. Our findings suggest that the strategic added value of the multisectoral approach lies in its ability to create a common base of comprehensive and critical information, filing knowledge gaps, and to reduce uncertainty in risk assessment. This, in turn, facilitates the achievement of consensus on the comprehensive level of risk for the country taking into account the perspective of all sectors involved. The concomitant participation to the assessment of other countries of the region has also contributed to the identification of possible cross-border risk factors and to the assessment of a “regional” risk level. Similar outcomes were reported following the 2003 International Workshop [37] on the possibility, benefits, and obstacles of integration of ecological and health risk assessments based on the WHO “framework for integrated assessment of human health and ecological risks” [38]. Improved assessment quality, efficiency, and predictive capability were considered to be principal benefits of integration of risk assessments. Unfortunately, some of the obstacles to the acceptance and implementation of this approach, identified at the time, such as disciplinary and organizational barriers between disciplines, are still present. The workshop's recommendations, such as harmonization of exposure characterization, surveillance methods and models, and development of methods to facilitate comparison of risks, are still being addressed [21, 31, 39] underlying both the relevance and the complexity of the issue.
5. Conclusions
Increasing awareness of intersectoral priorities, including cross-border ones, through MRA is a new frontier which can support early warning capacities. This approach is relevant to reduce gaps due to unavailability of shared data and information, and it can also promote the use of multiple sources of information across sectors and facilitate consensus on operational arrangements for the RA, e.g., as recommended by the World Health Organisation (WHO) in the Western Pacific Regional Action Plan for Dengue Prevention and Control [5]. Given that six out of the ten threats to global health listed by WHO [40] are issues occurring at the human, animal, and environmental interface, the implementation of comprehensive regional assessments with a One Health approach made by national authorities using similar frameworks is promising in terms of the potential added value for the global health security agenda. This justifies further efforts in fine-tuning methodological approaches and addressing implementation challenges.
Acknowledgments
The authors acknowledge the active participation of the members of MediLabSecure network to the MRA exercises. The MediLabSecure project was supported by the European Commission (DEVCO: IFS/21010/23/_194 & IFS/2018/402-247). The funding body was not involved in the design of the study, in collection, analysis, and interpretation of data, and in writing the manuscript.
Abbreviations
- CCHF:
Crimean–Congo haemorrhagic fever
- ECDC:
European Centre for Disease Prevention and Control
- EU:
European Union
- FAO:
Food and Agriculture Organization of the United Nations
- IZSAM:
Istituto Zooprofilattico Sperimentale dell'Abruzzo e del Molise
- MLS:
MediLabSecure project
- MRA:
Multisectoral risk assessment
- RA:
Risk assessment
- RRA:
Rapid risk assessment
- RVF:
Rift Valley fever
- SWOT analysis:
Strengths, weaknesses, opportunities, and threats analysis
- WHO:
World Health Organisation
- WNV:
West Nile virus.
Data Availability
The data generated or analysed during this study, including documentation and tools prepared for the exercises, are available in the references reported in this published article (refer to [32–34]) and its supplementary information files. Pre-test and post-test forms filled in by participants are in hard copies available from the corresponding author and can be provided on reasonable request making the copies anonymous.
Ethical Approval
The implementation of the exercises reported in this manuscript did not need formal ethical approval and informed consent and complies with national guidelines as per the code of ethics of Istituto Superiore di Sanità https://www.iss.it/wp-content/uploads/2017/12/CE_Codice_di_etica_2015_01_13.pdf
Conflicts of Interest
The authors declare that they have no competing interests.
Authors' Contributions
MGD developed and implemented the exercises and wrote the manuscript; FR supported the development of the exercises, the implementation of WNV exercise, and the drafting of the manuscript; WVB and LM supported the development and the implementation of the WNV exercises and critically revised the manuscript; TM and TD supported the development and the implementation of the CCHF exercise and critically revised the manuscript; BS and PC supported the development and the implementation of the RVF exercise and critically revised the manuscript; SD supported the development and the implementation of all the three exercises and critically revised the manuscript; the persons of the MediLabSecure Working Group collaborated in the exercise development and implementation. All authors reviewed and approved the final manuscript.
Supplementary Materials
Additional file 1: file format: excel; title of data: data analysis of the evaluation of the exercises and the added value of multisectoral approach. Description of data: replies of the participants to the questions related to the evaluation of the exercises and perceived participants' added value of the multisectoral approach.
References
- 1.Stärk K. D. C., Arroyo Kuribreña M., Dauphin G., et al. One health surveillance—more than a buzz word? Preventive Veterinary Medicine. 2015;120(1):124–130. doi: 10.1016/j.prevetmed.2015.01.019. [DOI] [PubMed] [Google Scholar]
- 2.Bordier M., Uea-Anuwongd T., Binotb A., Hendrikxg P., Goutardb F. Characteristics of one health surveillance systems: a systematic literature review. Preventive Veterinary Medicine. 2018;158 doi: 10.1016/j.prevetmed.2018.10.005. [DOI] [PubMed] [Google Scholar]
- 3.Babo Martins S., Rushton J., Stärk K. D. Economics of zoonoses surveillance in a “one health” context: an assessment of campylobacter surveillance in Switzerland. Epidemiology and Infection. 2018;145:1148–1158. doi: 10.1017/s0950268816003320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Riccardo F., Monaco F., Bella A., et al. An early start of west Nile virus seasonal transmission: the added value of one heath surveillance in detecting early circulation and triggering timely response in Italy, june to july 2018. Eurosurveillance. 2018;23(32) doi: 10.2807/1560-7917.es.2018.23.32.1800427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.WHO. Western Pacific Regional Action Plan for Dengue Prevention and Control. Geneva, Switzerland: WHO; 2016. [Google Scholar]
- 6.Vrbova L., Stephen C., Kasman N., et al. Systematic review of surveillance systems for emerging zoonoses. Transboundary and Emerging Diseases. 2010;57(3):154–161. doi: 10.1111/j.1865-1682.2010.01100.x. [DOI] [PubMed] [Google Scholar]
- 7.Halliday J., Cleaveland S., Auty H., et al. London, UK: Department for International Development; 2011. Surveillance and monitoring of zoonoses: report for the department for international development. Project Report. [Google Scholar]
- 8.Wendt A. Kreienbrock L and campe a zoonotic disease surveillance—inventory of systems integrating human and animal disease. Zoonoses and Public Health. 2015;62:61–74. doi: 10.1111/zph.12120. [DOI] [PubMed] [Google Scholar]
- 9.Dente M. G., Riccardo F., Nacca G, et al. Declich s on behal of the medilabsecure network strenghtening integrated surveillance for arboviruses in the mediterranean and Black sea regions in the framework of the one health approach quaderni della società Italiana di medicina tropicale e salute globale N. 2016;1 http://www.simetweb.eu/Page/WebObjects/PageSimet.woa/wa/displayPage?name=Pubblic499azioni. [Google Scholar]
- 10.Dente M. G., Riccardo F., Bolici F., et al. Implementation of the one health approach to fight arbovirus infections in the mediterranean and Black sea region: assessing integrated surveillance in Serbia, Tunisia and Georgia. Zoonoses and Public Health. 2019;66(3):276–287. doi: 10.1111/zph.12562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chatham House. Jussi Sane and Michael Edelstein Overcoming Barriers to Data Sharing in Public Health: A Global Perspective: Centre on Global Health Security. London, UK: Chatham House; 2015. [Google Scholar]
- 12.Edelstein M., Lee L. M., Herten-Crabb A., Heymann D. L., Harper D. R. Strengthening global public health surveillance through data and benefit sharing. Emerging Infectious Diseases. 2018;24(7):1324–1330. doi: 10.3201/eid2407.151830. [DOI] [Google Scholar]
- 13.Heymann D. L., Rodier G. Global surveillance, national surveillance, and SARS. Emerging Infectious Diseases. 2004;10(2):173–175. doi: 10.3201/eid1002.031038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.WHO. Strengthening the WHO global influenza surveillance network (GISN). Proceedings of the Report of the 3rd Meeting with National Influenza Centres (NICs); December 2010; Hammamet, Tunisia. http://www.who.int/influenza/gisrs_laboratory/GISN_Meeting_Report_apr2011.pdf. [Google Scholar]
- 15.Vong S., O’Leary M., Feng Z. Early response to the emergence of influenza A(H7N9) virus in humans in China: the central role of prompt information sharing and public communication. Bulletin of the World Health Organization. 2014;92(4):303–308. doi: 10.2471/blt.13.125989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kahn L. H. Confronting zoonoses, linking human and veterinary medicine. Emerging Infectious Diseases. 2006;12(4):556–561. doi: 10.3201/eid1204.050956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Marcotty T., Thys E., Conrad P., et al. Intersectoral collaboration between the medical and veterinary professions in low-resource societies: the role of research and training institutions. Comparative Immunology, Microbiology and Infectious Diseases. 2013;36(3):233–239. doi: 10.1016/j.cimid.2012.10.009. [DOI] [PubMed] [Google Scholar]
- 18.Conrad P. A., Meek L. A., Dumit J. Operationalizing a one health approach to global health challenges. Comparative Immunology, Microbiology and Infectious Diseases. 2013;36(3):211–216. doi: 10.1016/j.cimid.2013.03.006. [DOI] [PubMed] [Google Scholar]
- 19.The World Bank Agriculture and Rural Development Health. Washington, DC, USA: The World Bank Agriculture and Rural Development Health; 2010. Nutrition and population people, pathogens, and our planet. Report No. 50833-GLB. [Google Scholar]
- 20.Landford J., Nunn M. J. Good governance in “one health” approaches. Revue Scientifique et Technique de l’OIE. 2012;31(2):561–575. doi: 10.20506/rst.31.2.2133. [DOI] [PubMed] [Google Scholar]
- 21.World Organisation for Animal Health. Taking a Multisectoral, One Health Approach: A Tripartite Guide to Addressing Zoonotic Diseases in Countries: World Health Organization (WHO): Food and Agriculture Organization of the United Nations (FAO) and World Organisation for Animal Health. Paris, France: World Organisation for Animal Health; 2019. [Google Scholar]
- 22.Berthe F. C. J., Bouley T., Karesh W. B., et al. Operational Framework for Strengthening Human, Animal and Environmental Public Health Systems at Their Interface. Washington, DC, USA: World Bank; 2018. [Google Scholar]
- 23.Forcella S., Tantawy N., Yilma J., et al. The development of a four-way linking framework in Egypt: an example of the FAO, OIE and WHO joint activities to facilitate national risk assessment. Veterinaria Italiana. 2015;51(1):45–50. doi: 10.12834/VetIt.220.680.1. [DOI] [PubMed] [Google Scholar]
- 24.Mackenzie J. S., McKinnon M., Jeggo M. Confronting Emerging Zoonoses. Berlin, Germany: Springer; 2014. One health: from concept to practice. [DOI] [Google Scholar]
- 25.Maltezou H. C., Andonova L., Andraghetti R, et al. Crimean-Congo hemorrhagic fever in Europe: current situation calls for preparedness. Eurosurveillance. 2010;15(10) [PubMed] [Google Scholar]
- 26.Kuchuloria T., Endeladze M., Tsertsvadze T., et al. Viral hemorrhagic fever cases in the country of Georgia: acute febrile illness surveillance study results. The American Journal of Tropical Medicine and Hygiene. 2014;91(2):246–248. doi: 10.4269/ajtmh.13-0460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. MediLabSecure Project, http://medilabsecure.com/project.html, 2018.
- 28.European Centre for Disease Prevention and Control. West Nile Virus Risk Assessment Tool Stockholm. Solna Municipality, Sweden: European Centre for Disease Prevention and Control; 2013. https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/west-nile-virus-risk-assessment-tool.pdf. [Google Scholar]
- 29.European Centre for Disease Prevention and Control. Operational Guidance on Rapid Risk Assessment Methodology. Stockholm, Sweden: European Centre for Disease Prevention and Control; 2011. https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/1108_TED_Risk_Assessment_Methodology_Guidance.pdf. [Google Scholar]
- 30.Food and Agriculture Organization of the United Nations (FAO of the UN) Rift Valley Fever in Niger: Risk Assessment: FAO Animal Health Risk Analysis—Assessment, Issue No. 1. Rome, Italy: Food and Agriculture Organization; 2017. [Google Scholar]
- 31.Dente M. G., Ranghiasci A., Nacca G., Declich S. Integrated Surveillance and Risk Assessment for Arbovirus Infections: Recommendations for Enhancing One Health in the Mediterranean Region: MediLabSecure Strategic Document. Rome, Italy: Istituto Superiore di Sanità; 2018. [Google Scholar]
- 32.Grazia Dente M., Declich S., Riccardo F. The West Nile Risk Assessment Exercise. Paris, France: 2015. http://www.medilabsecure.com/documents/site/wnv_risk_assessment_exercise_2015_report.pdf. [Google Scholar]
- 33.Grazia Dente M., Declich S., Riccardo F. The Crimean Congo Risk Assessment Exercise. Belgrade, Serbia: 2016. http://www.medilabsecure.com/documents/site/cchf_risk_assessment_exercise_2016_report_completo.pdf. [Google Scholar]
- 34.Grazia Dente M., Declich S. The Rift Valley Fever Risk Assessment Exercise. Tunis, Tunisia: 2017. http://www.medilabsecure.com/documents/site/rvf_risk_assessment_exercise_2017_report_completo.pdf. [Google Scholar]
- 35.Van Wijngaarden J. D. H., Scholten G. R. M., van Wijk K. P. Strategic analysis for health care organizations: the suitability of the SWOT-analysis. The International Journal of Health Planning and Management. 2010;27(1):34–49. doi: 10.1002/hpm.1032. [DOI] [PubMed] [Google Scholar]
- 36.Rist C. L., Arriola C. S., Rubin C. Prioritizing zoonoses: a proposed one health tool for collaborative decision-making. PLoS One. 2014;9(10) doi: 10.1371/journal.pone.0109986.e109986 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Munns W. R., Suter G. W., II, Damstra T., Kroes R., Reiter L. W., Marafante E. Integrated risk assessment—results from an international workshop. Human and Ecological Risk Assessment: An International Journal. 2003;9(1):379–386. doi: 10.1080/713609870. [DOI] [Google Scholar]
- 38.WHO. Geneva, Swizertland: WHO; 2001. Integrated risk assessment. report prepared for the WHO/UNEP/ILO international programme on chemical safety. Technical Reort WHO/IPCS/IRA/01/12. [Google Scholar]
- 39.Jourdain F., Samy A. M., Hamidi A., et al. Towards harmonisation of entomological surveillance in the Mediterranean area. PLOS Neglected Tropical Diseases. 2019;13(6) doi: 10.1371/journal.pntd.0007314.e0007314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.WHO. WHO 10 Threats to Global Health in 2018. Geneva, Switzerland: WHO; 2018. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: file format: excel; title of data: data analysis of the evaluation of the exercises and the added value of multisectoral approach. Description of data: replies of the participants to the questions related to the evaluation of the exercises and perceived participants' added value of the multisectoral approach.
Data Availability Statement
The data generated or analysed during this study, including documentation and tools prepared for the exercises, are available in the references reported in this published article (refer to [32–34]) and its supplementary information files. Pre-test and post-test forms filled in by participants are in hard copies available from the corresponding author and can be provided on reasonable request making the copies anonymous.