

Abstract
The recent outbreak of COVID-19, which continues to ravage communities with high death tolls and untold psychosocial and catastrophic economic consequences, is a vivid reminder of nature's capacity to defy contemporary healthcare. The pandemic calls for rapid mobilization of every potential clinical tool, including phototherapy—one of the most effective treatments used to reduce the impact of the 1918 “Spanish influenza” pandemic. This paper cites several studies showing that phototherapy has immense potential to reduce the impact of coronavirus diseases, and offers suggested ways that the healthcare industry can integrate modern light technologies in the fight against COVID-19 and other infections. The evidence shows that violet/blue (400–470 nm) light is antimicrobial against numerous bacteria, and that it accounts for Niels Ryberg Finsen's Nobel-winning treatment of tuberculosis. Further evidence shows that blue light inactivates several viruses, including the common flu coronavirus, and that in experimental animals, red and near infrared light reduce respiratory disorders, similar to those complications associated with coronavirus infection. Moreover, in patients, red light has been shown to alleviate chronic obstructive lung disease and bronchial asthma. These findings call for urgent efforts to further explore the clinical value of light, and not wait for another pandemic to serve as a reminder. The ubiquity of inexpensive light emitting lasers and light emitting diodes (LEDs), makes it relatively easy to develop safe low-cost light-based devices with the potential to reduce infections, sanitize equipment, hospital facilities, emergency care vehicles, homes, and the general environment as pilot studies have shown.
Keywords: COVID-19, Coronaviruses, Photobiomodulation, Antiviral, Pulsed blue light, Red or near infrared light
1. Introduction
In 1918, the world was gripped with panic and apprehension as one of the most devastating pandemics ever recorded in human history, the H1N1 influenza virus, killed millions of people across the globe [1,2]. Dubbed “Spanish influenza”, the disease spread quickly, ravaging the world at a time that there were no antibiotics and medicine—as a field—was essentially infantile in its development. Without the benefit of modern technology, data keeping was poor, making it difficult to have accurate mortality and morbidity figures; but even then, estimates suggest that the flu killed 1% to 3% of its victims, with the mortality rate reaching 10% in some communities [[1], [2], [3]]. While a 1991 report [3] put the death toll in the range of 24.7–39.3 million, and related morbidity estimates between 25% and 90%, recent publications suggest that 50–100 million died as a result of the pandemic [1,4].
Since 1918, the world has experienced more outbreaks of pandemic diseases. The 1957 H2N2 “Asian influenza” pandemic claimed more than two million lives; the 1968 H3N2 “Hong Kong influenza” virus killed one million worldwide. More recently, the Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) pandemic of 2002 claimed 774 lives, and the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) of 2012 resulted in about 300,000 deaths [[1], [2], [3],5,6]. While the declining morbidity and mortality rate of each successive pandemic may be attributed to modern medicine, early diagnosis, ready availability of effective antibiotics to address secondary bacterial infections, the availability of artificial respirators to support life, and acute awareness of preventive measures gained from past pandemics, the threat of a severe devastating disease of global concern remains high.
The ongoing pandemic of novel coronavirus (SARS-CoV-2) COVID-19, serves as a vivid reminder that nature is unpredictable; no one knows what disease epidemic might emerge and defy available clinical armamentaria. With over 2.97 million confirmed cases and more than 260,000 deaths worldwide within a mere four months (as of Sunday, April 26, 2020), the world has—once again—become gripped with untold fear and panic as the number of those sick or dying continues to climb by the minute [6]. Further raising the level of fear are the portentous economic consequences, which has risen to hitherto unimaginable heights and continues to worsen. That some of the world's largest economies—the US, China, Germany, France, Britain, Italy, Spain South Korea and Switzerland—rank among the worst hit countries, cast a dark shadow on the future of the world as we know it. These developments call for immediate mobilization of every available tool to fight the disease. A frantic search for effective treatments is underway to stem the pandemic and give hope to billions quarantined—willingly or unwillingly—worldwide. However, the world continues to race against time given the rate of spread and the long period usually required to develop effective vaccines.
Whereas some of the important lessons learned from past pandemics, such as social distancing, the use of facemasks and the search for new vaccines, have been marshalled to mitigate the pandemic, records indicate that, phototherapy, one of the most effective tools used to minimize the impact of the 1918 pandemic and other disease epidemics [[7], [8], [9]] has been overlooked. This paper suggests that phototherapy, a seemingly forgotten treatment for bacterial and viral infections, has immense potential to reduce the impact of COVID-19 pandemic and similar coronavirus infections, particularly in view of recent developments in the field. Further, it reviews contemporary evidence for this assertion, and offers suggested ways that modern healthcare may integrate readily available inexpensive light technologies in its stash of clinical tools for patients with COVID-19 and other infections.
2. Disease Epidemics, Pandemics and Phototherapy
In 1918, governments and the medical establishment frantically sought every means to fight the H1N1 flu pandemic, but the results were mixed. Available reports clearly show that sunlight was effective in reducing flu-related mortality and morbidity, and person-to-person infection [[7], [8], [9]]. Patients with severe infections exposed to sunlight therapy outdoors recovered better than those treated indoors, and the treatment prevented death among patients and infections among the healthcare workers [[8], [9], [10]].
Like the 1918 pandemic, most of those succumbing to COVID-19 pandemic today die from disease-related complications, such as pulmonary inflammation/edema, pneumonia and acute respiratory disorder syndrome (ARDS). In the case of the 1918 flu, overcrowding in poorly lit and poorly ventilated enclosures raised associated risks of infection, a major reason that the City of Boston was badly hit by the flu until exposure to sunlight was introduced [[7], [8], [9], [10]]. By one anonymous editorial account [9], the Massachusetts State Health Department found sunlight therapy to be “the most valuable factor in reducing mortality,” decreasing fatality of hospitalized patients from 40% to 13%, boosting flu immunity among physicians and nurses, and overall, besting the outcome of vaccines, which, then, were in their early stages of development [[6], [7], [8], [9]]. The benefit of exposure to the healing rays of the sun was so obvious that it became a common form of treatment against tuberculosis—another respiratory disorder, as well as wound infections, psoriasis, acne vulgaris, rickettsia, depression, jaundice, and a host of other diseases [[10], [11], [12], [13], [14], [15], [16], [17], [18], [19]]. Indeed, records indicate that across North America, many healthcare facilities built sunrooms to which patients were wheeled for sun therapy, then known as heliotherapy [11]. Written accounts of the successes of heliotherapy abound, and as the treatment became popular, it was adapted to include treatment with various lamps [[15], [16], [17], [18], [19]].
None of the foregoing should come as a surprise, because less than 25 years before the 1918 pandemic, a Danish physician, Niels Ryberg Finsen, had developed a light source that was successful in curing patients with skin tuberculosis (lupus vulgaris) and other ailments [20,21]. Between 1896 and 1901, he treated as many as 804 patients with skin tuberculosis and similar microbial infections at his Medical Light Institute, achieving 83% cure rate [20,21,22]. The Finsen lamp became widely popular and was adopted in most of Europe and North America, earning Finsen the Nobel Prize in 1903. Finsen himself acknowledged the healing power of sunlight but erroneously assumed that his lamp took advantage of the UV spectrum of radiation. It is quite conceivable that his pioneering work spurred many in the healthcare industry to use sunlight to treat victims of the 1918 influenza pandemic and beyond. To date, studies continue to extol the susceptibility of viruses to rays emanating from the sun [11,16].
3. From Heliotherapy to Photobiomodulation
While it is obvious that Finsen pioneered the scientific documentation of the bactericidal effect of light, the use of light to treat a variety of diseases predates him. Perhaps the earliest record of sunlight as medical treatment dates back to the time of Egyptian Pharaohs—more than 5000 BCE—as evidenced by images, archeological findings and artifacts [[23], [24], [25], [26]]. A popular ancient Egyptian image clearly shows a family exposing themselves to the healing rays of the sun (Fig. 1 ). Veneration of the sun and acknowledgement of its healing power remains a cultural practice in most of Africa, and early records indicate that the Egyptians treated chronic ulcers successfully by exposing them to sunlight [23,24]. Furthermore, sunbathing was a common practice, not just in ancient Egypt, Babylonia and Mesopotamia, but ancient Greece and Rome [[23], [24], [25], [26]].
Fig. 1.
An image showing Akhenaten, Nefertiti and three children exposing themselves and a house plant to the healing rays of sunlight. The religious symbols in the image suggest that the Ancient Egyptians venerated and worshipped the sun.
Adapted from: https://www.sciencephoto.com/media/1005027/view/egyptian-pharaoh-akhenaten-and-nefertiti.
The Greeks and the Romans clearly recognized the healing power of the sun. They built solariums and sunbaths, and the Greeks even used them to enhance the strength of athletes preparing for the Olympic Games by exposing them to several months of sunlight treatment. The word, heliotherapy, actually derives from the Greek name for their sun god, “Helios”; heliotherapy meaning sunlight therapy [[23], [24], [25], [26]]. Furthermore, Ayurvedic medical records show that as far back and 1400 BCE; Hindus used the combination of sunlight and photosensitive herbs, such as furocoumarins, to treat vitiligo and other conditions—a combined treatment, which many refer to today as photodynamic therapy [27]. Moreover, records indicate that heliotherapy was a cardinal method used in early Daoism, which Lingyan Tzu-Ming introduced in China during the first century CE [28]. In summary, evidence from many parts of the world clearly show that communities worldwide used heliotherapy to treat a variety of diseases. In those days, the inimical effects of UV were unknown before UV was discovered in 1801 [11].
The discovery of UV transformed the practice of heliotherapy into clinical phototherapy as the antimicrobial effects of UV became evident during the second half of the 19th century. As early as 1877, studies showed that UV killed anthrax bacilli [11], and by 1890, it was determined that it played a role in rachitis, rickettsia and peritoneal tuberculosis [11,16,29]. By this time, lamps generating light from quartz, mercury vapor and other sources were built and used to treat acne, psoriasis, syphilis, leprosy, and pellagra, among others [11,17,25]. Three years later, Finsen began to use filtered sunlight to treat lupus vulgaris and through careful documentation published his Nobel-winning work, in 1901. The use of lamps and other artificial light sources to treat skin diseases continued well into the second half of the 20th century, but was quickly overtaken by easy availability of potent antibiotics, which became popular for their quick results and ease of use [11,25].
The development of lasers in the late 50s and the early 60s, and the subsequent evolution of light emitting diodes transformed phototherapy; it gave rise to laser therapy or light therapy, which in turn evolved into photobiomodulation as a variety of light emitting technologies were devised. Today, photobiomodulation, which takes advantage of the photochemical effects of low power lasers, LEDs and other monochromatic sources of light to treat various diseases and ailments, has evolved scientifically, allowing evidence-based practice. This development now enables clinicians and others to exploit the specific effect of each wavelength or spectrum of light for treatment purposes. Detailed below are several studies, which show that we do not need UV to eradicate bacteria, viruses and other pathogens, and that relatively safer wavelengths adjacent to UV, such as violet or blue light, are antimicrobial against microorganisms. Furthermore, evidence shows that red and near infrared light have immense therapeutic value as well, and may be effective in treating a range of ailments, including the respiratory complications of coronavirus disease.
4. Photobiomodulation
Advances in light technology and steady development of photobiomodulation through research and continual adaptation to evolving technologies have enabled science to uncover the beneficial effects of several spectra of light—in particular, violet/blue light, red light and near infrared light. We now know that light in the blue 400–470 nm range is antimicrobial against numerous bacteria [[23], [24], [25], [26], [27], [28], [29], [30], [31], [32], [33], [34], [35], [36], [37], [38], [39], [40], [41], [42], [43], [44], [45]] and has the potential to mitigate opportunistic bacterial infections associated with COVID-19 and other coronavirus infections. Furthermore, as detailed below, laboratory experiments show that red and near infrared light, with wavelengths approximately in the range of 600–700 nm and 700–1000 nm respectively, have the potential to reduce lung inflammation and fibrosis, and hence acute respiratory disorder syndrome, a major cause of death in every coronavirus pandemic, including the prevailing COVID-19 pandemic. Therefore, as a part of the ongoing effort to mobilize every clinical tool with the potential to alleviate the disease and minimize its spread, these recent studies offer compelling reasons to explore the potential effects of various spectra of light in reducing secondary bacterial infections associated with the disease, and the possibility of suppressing COVID-19 and other viral infections.
5. Antimicrobial Blue Light
Recent studies demonstrate that various wavelengths in the blue spectrum are antimicrobial against the deadly methicillin-resistant Staphylococcus aureus (MRSA) [31,32,35,45], Escherichia coli [38,40], Helicobacter pylori [39], Listeria monocytogenes [40], Pseudomonas aeruginosa [38], Salmonella [37], Acinetobacter baumannii [41], Aggregatibacter actinomycetemcomitans [46], Propionibacterium acnes [[34], [35], [36],47], Neisseria gonorrhoeae [[48], [49], [50]], Porphyromonas gingivalis [[51], [52], [53]], Fusobacterium nucleatum [51], and others [42,50,[54], [55], [56], [57], [58]]. An analysis of the Nobel-winning work of Finsen, supports these blue light studies, because it shows that the Finsen Lamp, used to heal many with tuberculosis infection, did not produce UV as Finsen believed; rather, it produces light in the violet/blue range [59] (Fig. 2 ).
Fig. 2.
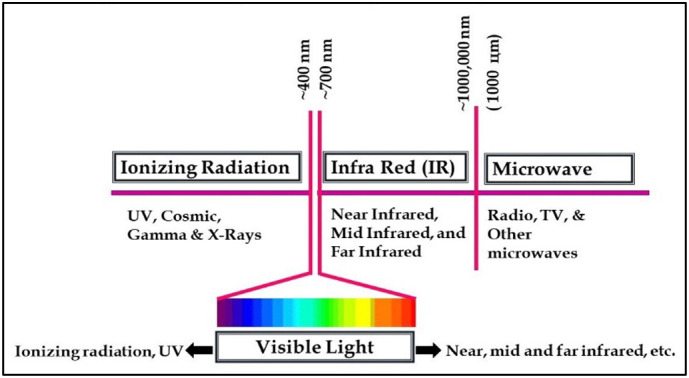
A simple illustration of the light spectrum.
Indeed, the Finsen Lamp could not have emitted UV because the type of glass used to construct its lenses does not transmit UV. Thus, when Møller et al. measured the radiation transmitted through the Finsen lens systems, and the absorption of the stain solution filters in the lamps relative to the lamp's effect on Mycobacterium tuberculosis, they found that the lens and filters absorbed UV wavelengths below 340 nm [59]. Moreover, the methylene blue solution used to absorb the heat generated by the system also blocked the transmission of wavelengths below 340 nm, as well as light in the 550–700 nm range; thus, allowing predominant transmission of light in the UV-A and violet/blue range [59]. Furthermore, the fluorescence of M. tuberculosis shows the presence of endogenous porphyrins, known to absorb blue light and engender the production of reactive oxygen species and bacterial suppression, not UV absorption [39,[46], [47], [48],[60], [61], [62], [63], [64], [65], [66], [67], [68], [69], [70], [71], [72], [73], [74], [75], [76], [77], [78], [79]].
This clearly explains Finsen's success in treating tuberculosis, implying that unbeknownst to the world, the 1903 Nobel Prize was awarded to Finsen for demonstrating the antimicrobial effect of violet/blue light. The only logical explanation of Finsen's success is that endogenous porphyrins in tuberculosis bacteria absorbed the violet/blue light predominantly transmitted through his lamp system; the absorption triggered downstream production of reactive oxygen species, thus killing the bacteria and curing his patients of tuberculosis, not UV light absorption as the Nobel laureate assumed.
Just as an analysis of Finsen's lamp makes it clear that its effect was due to violet/blue light and not UV, so a thought analysis of the radiation from the sun renders vivid the fact that the bactericidal effect of sunlight, often ascribed to UV, can be attributed to the immense amount of blue light reaching the earth from the sun. Atmospheric ozone substantially absorbs solar UV rays, allowing transmission of violet/blue light to the surface of the earth. Indeed, the peak transmission at the surface of the earth is in the blue region, and together with violet light, is 10 times more than the amount of UV reaching the surface of the earth [80]. Given the absorption of violet blue light by most microbes and the resulting bactericidal effect, it seems reasonable to attribute a good proportion of the sun's environmental sanitization power to the violet blue spectrum of radiation, and not UV as many assert.
Modern technology now makes flexible printed micro-LEDs readily available, making it relatively easy to develop therapeutic tools with the potential to reduce bacterial and potentially viral infections. In relation to COVID-19, some relatively easy targets are the nasal and oral cavities, and the upper respiratory tract, particularly as the nasal passage is an acclaimed point of entry of the virus into the human body [81]. Antimicrobial blue light may serve another useful purpose in reducing the COVID-19 pandemic; it could be used effectively to sanitize equipment, tools, hospital facilities, emergency care vehicles, homes, and the general environment as pilot studies have shown [[54], [55], [56]].
Recent works now show that there may be as many as four mechanisms underlying the antimicrobial effect of blue light. The first and most well-grounded of which is that blue light triggers endogenous bacterial chromophores such as porphyrins, flavins, NADH and other photosensitive receptors to produce reactive oxygen species, which in adequate amount results in cell death [39,[46], [47], [48], [49], [50],[64], [65], [66], [67], [68], [69], [70], [71], [72], [73], [74], [75], [76], [77], [78], [79]]. Indeed, porphyrins with absorption peaks in the 405 to 470 nm range have been identified in microbial cells [39,[46], [47], [48], [49], [50],[64], [65], [66], [67], [68], [69], [70], [71], [72], [73], [74], [75], [76], [77], [78], [79]]. In three recent papers [[34], [35], [36]], we took advantage of this theory by timing in vitro irradiation of P. acnes and MRSA to coincide with periods of abundant endogenous porphyrins and hence elicit maximal bacterial suppression. The outcome was impressive. The dominant chromophores in P. acnes and MRSA emit red light with peak emission between 612 and 660 nm when excited with blue/violet light [36,46,47,64]. Thus, by monitoring the fluorescence—red glow—emitted by both bacteria, we were able to correlate bacterial kill rate with quantitated amounts of remnant bacterial colonies. Not only did it show bacterial suppression, it revealed that their red fluorescence diminished as bacterial colonies were depleted and vice versa [36], further affirming the theory that porphyrins play a major role in antimicrobial blue light treatment.
The second mechanism, which is continuing to gain traction, is that irradiation with blue light alters bacterial cell membrane integrity with a consequent decrease in membrane polarization and rapid alteration of cellular functions [64]. Our recent electron microscopic study affirms this finding. It shows that even at a sub-lethal dose level, treatment with pulsed blue 450 nm light disrupts the structural architecture of MRSA cell membrane and its internal organelles. The third and fourth mechanisms of action, deserving further investigation and affirmation are that blue light alters A-DNA [82], and upregulates prophage genes to promote bacteria kill [83].
These findings clearly explain Finsen's remarkable achievement in healing many patients with tuberculosis, and suggests that similar successes could be attained in reducing secondary bacterial infections associated with coronavirus infections—the common flu, SARS, MERS, COVID-19, etc. It would be highly beneficial to patients with coronavirus disease if their loads of opportunistic bacterial infection could be reduced with blue light; such treatment—when fully developed—will give their immune systems a better chance of overcoming the deadly disease.
6. Photobiomodulation and Acute Pulmonary Disorder
Emerging data show that light in the red and near infrared light spectra can reduce lung inflammation, lung fibrosis, pneumonia, acute respiratory disorders, and other severe complications of coronavirus infections. This is an encouraging development since the experience of those at the frontline of the COVID-19 outbreak in Wuhan, China clearly show that acute respiratory disorder was the major cause of death [84]. Moreover, lack of effective antiviral drugs against COVID-19 remains a serious concern, making it unlikely that such life-threatening complications may be resolved with medication in the short run. Early reports on the Wuhan COVID-19 outbreak show that commonly used antiviral drugs, such as neuraminidase inhibitors (oseltamivir, peramivir, zanamivir and others), acyclovir, the corticosteroid—methylprednisolone, and ribavirin were ineffectual in treating the disease [81,84].
There are indications that Acute Respiratory Distress Syndrome (ARDS) a critical complication of COVID-19 infection [81,84], often characterized by airway edema, pulmonary inflammation, and lung fibrosis, could be ameliorated with photobiomodulation, as evidenced by early results in laboratory animals [[85], [86], [87]]. For example, following induction of pulmonary inflammation in rats, de Lima et al. [85] showed that irradiation of the skin over the inflamed bronchus with a single dose of 1.3 J cm−2 of continuous wave (CW) red 650 nm laser administered 1 h after induction of inflammation, inhibited pulmonary edema and downregulated several measures of inflammation. The treatment reduced activation and influx of neutrophils, damage to endothelial cytoskeleton, and the amount of TNF-α, and IL-1β in the lung and bronchoalveolar lavage fluid.
In a similar study, Brochetti et al. [86] induced pulmonary fibrosis in mice, and then treated the animals with red 660 ± 20 nm light (5 J cm−2 radiant exposure and 33 mW cm−2 irradiance) daily for eight days, beginning from day 14. They found that the treatment reduced collagen production and the number of inflammatory cells in the alveoli, decreased interstitial thickening, and static as well as dynamic pulmonary elasticity. Further, cultures of pneumocytes and fibroblasts obtained from the animals showed downregulation of pro-inflammatory cells and collagen deposits in the lungs [86]. Another study of the same murine model showed that infrared 780 nm light reduced inflammation and collagen deposits in the lungs of mice, downregulated pro-inflammatory cytokines, and upregulated the secretion of IL-10 from fibroblasts and pneumocytes. Moreover, it significantly reduced total lung TGFβ [87]. Taken together, these early results suggest that red and near infrared light have the potential to reduce some of the critical complications of coronavirus infections, i.e., pulmonary inflammation and lung fibrosis. The preliminary nature of these results and the need for improved experimental methods and data reporting should not diminish their significance; rather it should draw attention to another spectrum of light that may be beneficial in the ongoing fight against coronavirus diseases, which continues to challenge healthcare systems worldwide.
In the race against the anticipated devastation of COVID-19, clinicians have deployed chloroquine and hydroxychloroquine—two analogue medications commonly used to treat malaria but rarely used for coronavirus disease—to mitigate the disease, even though their mechanisms of action against viral infections remains poorly understood [84,[88], [89], [90]]. The rapid spread of COVID-19 and its clear capacity to kill on a massive scale obviously justify deployment of treatments that seem to work, even though their underlying mechanisms are not clear. Thus, given the potential capacity of red and near infrared light to reduce the life-threatening respiratory complications of COVID-19, it goes without saying that every effort should be made to advance the work so that an effective therapy can be fashioned from the body of research work achieved to date. It will be a wise investment to urgently investigate these initial results clinically, and not wait for another deadly coronavirus pandemic to remind us of the inherent potential of light as a therapeutic tool. The urgency of this call is heightened by recent clinical results, which indicate that patients with chronic obstructive lung disease and others with bronchial asthma and allergy improved significantly following treatment with light [91,92].
Even more striking are reports showing that certain wavelengths of light inactivate viruses. Light has been shown to inactivate baculoviruses [93] and prolonged exposure to blue light in the 420–430 nm range inactivates leukemia virus [94]. One may argue that baculoviruses are confined to invertebrates and are not known to replicate in humans; but the fact that COVID-19 traversed species barrier to humans [84] is a cause to worry. One or more of the 76 species of baculoviruses could mutate to survive and replicate in human hosts, more so because shrimps consumed by humans and mosquitoes that suck human blood are among their 600 or more invertebrate hosts. These prospects make urgent the need to intensify efforts to test the effect of blue light on common viruses, including COVID-19. Further, that light in the visible spectrum constitutes the basis for photodynamic treatment of plasma to inactivate several viruses, including herpes simplex and human immunodeficiency virus (HIV) [[95], [96], [97]], offers strong reason to suggest that blue light—particularly pulsed blue light, which recent reports have shown to be 40 to 100 times more potent than continuous wave blue light [[33], [34], [35]]—has great potential to inactivate coronaviruses.
Already, fresh off the press is an early report that the common cold virus—a coronavirus—is inactivated by light [98]. In this recent study, broad spectrum light—mimicking sunlight—was tested on aerosolized influenza virus at 20% and 70% relative humidity, while the decay constant and half-life of the virus were measured as indices of survival. The results showed that relative humidity had no effect. The simulated sunlight alone significantly inactivated the virus, resulting in 0.29 ± 0.09 min−1 decay constant and a half-live of approximately 2.4 min compared to non-irradiated controls, which had 0.02 ± 0.06 min−1 decay constant and 31.1 min half-life. The resulting 93% increase in decay constant and the concomitant 92.3% decline in half-life due to light is impressive. This recent development buttresses the suggestion that blue light, in particular, pulsed blue light, which recent reports have shown to be 40 to 100 times more potent than the commonly available continuous wave blue light [[34], [35], [36]], has great potential to inactivate COVID-19 and other coronaviruses, in addition to suppressing related opportunistic bacterial infections. This recent finding further elevates the urgency to explore the potential of blue light as an antiviral agent. When convincing clinical results prove that blue light is antiviral, in addition to being antibiotic against coronavirus opportunistic bacteria, it would be a revolutionary paradigm shift, considering the ubiquity of low cost blue light emitting devices and the low risk involved in terms of safety. Moreover, the potential to disinfect equipment, the environment and spaces difficult to sanitize with common disinfectants, is huge.
Declaration of Competing Interest
The authors certify that this manuscript is an original work and that besides presentation at conferences and related abstract publication, it has not been submitted or published, in whole or in part, in any other medium and is not under consideration for publication in any other journal. Furthermore, we the authors are liable for its content and for having contributed to the conception, design and implementation of the work, data analysis and data interpretation, and for having participated in writing and reviewing the text, as well as approving the final version submitted. Likewise, we accept the introduction of changes to the content, if necessary subsequent to review, and of changes to the style of the manuscript by the journal's editorial staff. We also declare that conflict of interest does not exist.
Acknowledgments
Acknowledgement
We thank Dr. Aldo Brugnera of University of São Paulo, São Paulo, Brazil for his correspondence with Dr. Chukuka S. Enwemeka, which inspired this paper, Drs. Terrence L. Baker, University of Maryland, Baltimore, MD and J. Chris Castel, Carewear Corporation, Reno, NV for their encouragement, and Dr. Jack Greiner, Schepens Eye Research Institute of Massachusetts Eye and Ear, Department of Ophtalmology, Harvard Medical School, Boston, MA for his editorial review and feedback on the paper.
References
- 1.Morens D.M., Fauci A.S. The 1918 influenza pandemic: insights for the 21st century. J. Infect. Dis. 2007;195:1018–1028. doi: 10.1086/511989. [DOI] [PubMed] [Google Scholar]
- 2.Johnson N.P., Mueller J. Updating the accounts: global mortality of the 1918–1920 “Spanish” influenza pandemic. Bull. Hist. Med. 2002;76:105–115. doi: 10.1353/bhm.2002.0022. [DOI] [PubMed] [Google Scholar]
- 3.Patterson K.D., Pyle G.F. The geography of mortality of the 1918 influenza pandemic. Bull. Hist. Med. 1991;65:4–21. [PubMed] [Google Scholar]
- 4.Jester B.J., Uyeki T.M., Patel A., Koonin L., Jernigan D.B. 100 years of medical countermeasures and pandemic influenza preparedness. Am. J. Public Health. 2018;108:1469–1472. doi: 10.2105/AJPH.2018.304586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Centers for Disease Control . January 13, 2004. Basic information about SARS; pp. 1–2. [Google Scholar]
- 6.Johns Hopkins University School of Medicine Coronavirus Resource Center https://coronavirus.jhu.edu/map.html accessed on April 26, 2020.
- 7.Hobday R. Coronavirus and the Sun: a lesson from the 1918 influenza pandemic. https://medium.com/@ra.hobday/coronavirus-and-the-sun-a-lesson-from-the-1918-influenza-pandemic-509151dc8065
- 8.Hobday R.A., Cason J.W. The open-air treatment of pandemic influenza. Am. J. Public Health. 2009;99:S236–S242. doi: 10.2105/AJPH.2008.134627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Editorial: weapons against influenza. Am. J. Public Health. 1918;10:787–788. doi: 10.2105/ajph.8.10.787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Brooks W.A. The open air treatment of influenza. Am. J. Public Health (N Y) 1918;8:746–750. doi: 10.2105/ajph.8.10.746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Roelandts R. The history of phototherapy: Something new under the sun? J. Am. Acad. Dermatol. 2002;46:926–930. doi: 10.1067/mjd.2002.121354. [DOI] [PubMed] [Google Scholar]
- 12.Hobday R.A., Dancer S.J. Roles of sunlight and natural ventilation for controlling infection: historical and current perspectives. J. Hosp. Infect. 2013;84:271–282. doi: 10.1016/j.jhin.2013.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hobday R.A. Sunlight therapy and solar architecture. Med. Hist. 1997;41:455–472. doi: 10.1017/s0025727300063043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Beauchemin K.M., Hays P. Sunny rooms expedite recovery from severe and refractory depressions. J. Affect. Disord. 1996;40:49–51. doi: 10.1016/0165-0327(96)00040-7. [DOI] [PubMed] [Google Scholar]
- 15.Benedetti F., Colombo C., Barbini B., Campori E., Smeraldi E. Morning sunlight reduces length of hospitalization in bipolar depression. J. Affect. Disord. 2001;62:221–223. doi: 10.1016/s0165-0327(00)00149-x. [DOI] [PubMed] [Google Scholar]
- 16.Alpert J.S. Sunshine: Clinical friend or foe. Am. J. Med. 2010;123:291–292. doi: 10.1016/j.amjmed.2009.05.033. [DOI] [PubMed] [Google Scholar]
- 17.Hammond R. Heliotherapy (of Rollier) as an adjunct in the treatment of bone disease. J. Bone Joint Surg. Am. 1913;S2–11:269–275. [Google Scholar]
- 18.Semmlman E., Lauharanta J., Reunanen A., Jansen C.T., Jyrkinen-Pakkasvirta T., Kallio M., Luoma J., Aromaa A., Waal J. Effect of heliotherapy on skin and joint symptoms in psoriasis: a 6-month follow-up study. Br. J. Dermatol. 1993;128:172–177. doi: 10.1111/j.1365-2133.1993.tb15147.x. [DOI] [PubMed] [Google Scholar]
- 19.Giryes H., Sukenik S., Haley S. Clearing of psoriatic erythroderma following heliotherapy in the Dead Sea area. J. Eur. Acad. Dermatol. Veneriol. 1995;5:44–46. [Google Scholar]
- 20.Alpert M.R., Ostheimer K.G. The evolution of current medical and popular attitudes toward ultraviolet light exposure: part 2. J. Am. Acad. Dermatol. 2003;48:909–918. doi: 10.1067/mjd.2003.272. [DOI] [PubMed] [Google Scholar]
- 21.Gøtzsche P.C. Niels Finsen’s treatment for lupus vulgaris. J. R. Soc. Med. 2011;104:41–42. doi: 10.1258/jrsm.2010.10k066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Grzybowski A., Pietrzak K. From patient to discoverer—Niels Ryberg Finsen (1860–1904)—the founder of phototherapy in dermatology. Clin. Dermatol. 2012;30:451–455. doi: 10.1016/j.clindermatol.2011.11.019. [DOI] [PubMed] [Google Scholar]
- 23.Editors Encyclopaedia Britannica: Sun Worship https://www.britannica.com/topic/sun-worship Updated March 19, 2020.
- 24.Solar Deities https://en.wikipedia.org/wiki/Solar_deity Available at. accessed March 31, 2020.
- 25.Alpert J.S. Jeremiah Metzger and the era of heliotherapy. Trans. Am. Clin. Climatol. Assoc. 2015;126:123–191. [PMC free article] [PubMed] [Google Scholar]
- 26.Mcdonagh A.F. Phototherapy: from ancient Egypt to the new millennium. J. Perinatol. 2001;21:S7–S12. doi: 10.1038/sj.jp.7210625. [DOI] [PubMed] [Google Scholar]
- 27.Fitzpatrick T.B., Pathak M.A. Historical aspects of methoxsalen and other furocoumarins. J. Invest. Dermatol. 1959;31:229–331. [PubMed] [Google Scholar]
- 28.Needham J., Gwei-Djen L. Science and civilization in China, Vol 5, Part 5. Cambridge: Cambridge University Press. 1983:12181–12184. [Google Scholar]
- 29.Palm T.A. The Practitioner; October–November, 1890. The Geographical Distribution and Aetiology of Rickets. [Google Scholar]
- 30.Enwemeka C.S. Antimicrobial blue light: an emerging alternative to antibiotics. Photomed. Laser Surg. 2013;31:509–511. doi: 10.1089/pho.2013.9871. [DOI] [PubMed] [Google Scholar]
- 31.Enwemeka C.S., Williams D., Enwemeka S.K., Hollosi S., Yens D. 470 nm blue Light kills methicillin-resistant Staphylococcus aureus (MRSA) in vitro. Photomed. Laser Surg. 2009;27:221–226. doi: 10.1089/pho.2008.2413. [DOI] [PubMed] [Google Scholar]
- 32.Enwemeka C.S., Williams D., Hollosi S., Yens D., Enwemeka S.K. Visible 405 nm SLD photo-destroys methicillin-resistant Staphylococcus aureus (MRSA) in vitro. Lasers Surg. Med. 2008;40:734–737. doi: 10.1002/lsm.20724. [DOI] [PubMed] [Google Scholar]
- 33.Enwemeka C.S., Williams D., Hollosi S., Yens D. Blue light photo-destroys methicillin- resistant Staphylococcus aureus (MRSA) in vitro. In: Waynant R., Tata D., editors. Lecture Notes in Electrical Engineering. Vol. 12. Springer Publishers; New York: 2008. pp. 33–37. [Google Scholar]
- 34.Masson-Meyers D.S., Bumah V.V., Castel C., Castel D., Enwemeka C.S. Pulsed 450 nm blue light significantly inactivates Propionibacterium acnes more than continuous wave blue light. J. Photochem. Photobiol. B. 2020;202:111719. doi: 10.1016/j.jphotobiol.2019.111719. [DOI] [PubMed] [Google Scholar]
- 35.Bumah V.V., Masson-Meyers D.S., Enwemeka C.S. Pulsed 450 nm blue light suppresses MRSA and Propionibacterium acnes in planktonic cultures and bacterial biofilms. J. Photochem. Photobiol. B. 2020;202:111702. doi: 10.1016/j.jphotobiol.2019.111702. [DOI] [PubMed] [Google Scholar]
- 36.Bumah V.V., Masson-Meyers D.S., Tong W., Castel C., Enwemeka C.S. Optimizing the bactericidal effect of pulsed blue light on Propionibacterium acnes - a correlative fluorescence spectroscopy study. Photochem. Photobiol. B. 2020;2020:111701. doi: 10.1016/j.jphotobiol.2019.111701. [DOI] [PubMed] [Google Scholar]
- 37.Bumah V.V., Masson-Meyers D.S., Enwemeka C.S. Blue 470 nm light suppresses the growth of Salmonella enterica and Methicillin-resistant Staphylococcus aureus (MRSA) in vitro. Lasers Surg. Med. 2015;47:595–601. doi: 10.1002/lsm.22385. [DOI] [PubMed] [Google Scholar]
- 38.De Sous N.T.A., Santos M.F., Gomes R.C., Brandino H.E., Martinez R., de Jesus Guirro R.R. Blue laser inhibits bacterial growth of Staphylococcus aureus, Escherichia coli, Pseudomonas aeruginosa. Photomed. Laser Surg. 2015;33:278–282. doi: 10.1089/pho.2014.3854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hamblin M.R., Viveiros J., Yang C., Ahmadi A., Ganz R.A., Tolkoff M.J. Helicobacter pylori accumulates photoactive porphyrins and is killed by visible light. Antimicrob. Agents Chemother. 2005;49:2822–2827. doi: 10.1128/AAC.49.7.2822-2827.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.McKenzie K., Maclean M., Timoshkin I.V., MacGregor S.J., Anderson J.G. Enhanced inactivation of Escherichia coli and Listeria monocytogenes by exposure to 405 nm light under sub-lethal temperature, salt and acid stress conditions. Int. J. Food Microbiol. 2013;170:91–98. doi: 10.1016/j.ijfoodmicro.2013.10.016. [DOI] [PubMed] [Google Scholar]
- 41.Mussi M.A., Gaddy J.A., Cabruja M., Arivett B.A., Viale A.M., Rasia R., Actis L.A. The opportunistic human pathogen Acinetobacter baumannii senses and responds to light. J. Bacteriol. 2010;192(24):6336–6345. doi: 10.1128/JB.00917-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Maclean M., MacGregor S.J., Anderson J.G., Woolsey G. High-intensity narrow-spectrum light inactivation and wavelength sensitivity of Staphylococcus aureus. FEMS Microbiol. Lett. 2008;285:227–232. doi: 10.1111/j.1574-6968.2008.01233.x. [DOI] [PubMed] [Google Scholar]
- 43.Maclean M., MacGregor S.J., Anderson J.G., Woolsey G. Inactivation of bacterial pathogens following exposure to light from a 405 nanometer light-emitting diode array. Appl. Environ. Microbiol. 2009;75:1932–1937. doi: 10.1128/AEM.01892-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Dai T., Tegos G.P., Zhiyentayev T., Mylonakis E., Hamblin M.R. Photodynamic therapy for methicillin-resistant Staphylococcus aureus infection in a mouse skin abrasion model. Lasers Surg. Med. 2010;42:1–14. doi: 10.1002/lsm.20887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Dai T., Gupta A., Huang Y.Y., Yin R., Murray C.K., Vrahas M.S., Sherwood M.E., Tegos G.P., Hamblin M.R. Blue light rescues mice from potentially fatal pseudomonas aeruginosa burn infection: efficacy, safety, and mechanism of action. Antimicrob. Agents Chemother. 2013;57:1238–1245. doi: 10.1128/AAC.01652-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Cieplik F., Spath A., Leibl C., Gollmer A., Regensburger J., Tabenski L., Hiller K.A., Maisch T., Schmalz G. Blue light kills Aggregatibacter actinomycetemcomitans due to its endogenous photosensitizers. Clin. Oral Investig. 2014;18:1763–1769. doi: 10.1007/s00784-013-1151-8. [DOI] [PubMed] [Google Scholar]
- 47.Ashkenazi H., Malik Z., Harth Y., Nitzan Y. Eradication of Propionibacterium acnes by its endogenic porphyrins after illumination with high intensity blue light. FEMS Immunol. Med. Microbiol. 2003;35:17–24. doi: 10.1111/j.1574-695X.2003.tb00644.x. [DOI] [PubMed] [Google Scholar]
- 48.Wang Y., Ferrer-Espada R., Baglo Y., Gu Y., Dai T. Antimicrobial blue light inactivation of Neisseria gonorrhoeae: roles of wavelength, endogenous photosensitizer, oxygen, and reactive oxygen species. Lasers Surg. Med. 2019;51:815–823. doi: 10.1002/lsm.23104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Wang Y., Ferrer-Espada R., Gu Y., Dai T. Antimicrobial blue light: An alternative therapeutic for multidrug-resistant gonococcal infections? MOJ Sol. Photoenergy Syst. 2017;1(2):00009. doi: 10.15406/mojsp.2017.01.00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Wang Y., Ferrer-Espada R., Baglo Y., Goh X.S., Held K.D., Grad Y.H., Gu Y., Gelfand J.A., Dai T. Photoinactivation of Neisseria gonorrhoeae: A paradigm-changing approach for combating antibiotic-resistant gonococcal infection. J. Infect. Dis. 2019;220:873–881. doi: 10.1093/infdis/jiz018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Feuerstein O., Persman N., Weiss E.I. Phototoxic effect of visible light on Porphyromonas gingivalis and Fusobacterium nucleatum, an in vitro study. Photochem. Photobiol. 2004;80:412–415. doi: 10.1562/0031-8655(2004)080<0412:PEOVLO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 52.Yoshida A., Sasaki H., Toyama T., Araki M., Fujioka J., Tsukiyama K., Hamada N., Yoshino F. Antimicrobial effect of blue light using Porphyromonas gingivalis pigment. Sci. Rep. 2017;7:5225. doi: 10.1038/s41598-017-05706-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Song H.W., Lee J.K., Um H.S., Chang B.S., Lee S.Y., Lee M.K. Phototoxic effect of blue light on the planktonic and biofilm state of anaerobic periodontal pathogens. J. Periodontal. Implant Sci. 2013;43:72–78. doi: 10.5051/jpis.2013.43.2.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Maclean M., Booth M.G., Anderson J.G., MacGregor S.J., Woolsey G.A., Coia J.E., Hamilton K., Gettinby G. Continuous decontamination of an intensive care isolation room during patient occupancy using 405 nm light technology. J. Infect. Prev. 2013;14:176–181. [Google Scholar]
- 55.Maclean M., Macgregor S.J., Anderson J.G., Woolsey G.A., Coia J.E., Hamilton K., Taggart I., Watson S.B., Gettinby G. Environmental decontamination of a hospital isolation room using high-intensity narrow-spectrum light. J. Hosp. Infect. 2010;76:247–251. doi: 10.1016/j.jhin.2010.07.010. [DOI] [PubMed] [Google Scholar]
- 56.Maclean M., Anderson J.G., MacGregor S.J., White T., Atreya C.D. A new proof of concept in bacterial reduction: antimicrobial action of violet-blue light (405 nm) in ex vivo stored plasma. J. Blood Transf. 2016:1–11. doi: 10.1155/2016/2920514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Halstead F.D., Ahmed Z., Bishop J.R.B., Oppenheim B.A. The potential of visible blue light (405 nm) as a novel decontamination strategy for carbapenemase-producing enterobacteriaceae (CPE) Antimicrob. Resist. Infect. Control. 2019;8:14. doi: 10.1186/s13756-019-0470-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Halstead F.D., Thwaite J.E., Burt R., Laws T.R., Raguse M., Moeller R., Weber M.A., Oppenheim B.A. Antibacterial activity of blue light against nosocomial wound pathogens growing Planktonically and as mature biofilms. Appl. Environ. Microbiol. 2016;82:4006–4016. doi: 10.1128/AEM.00756-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Møller K.I., Kongshoj B., Philipsen P.A., Thomsen V.O., Wulf H.C. How Finsen’s light cured lupus vulgaris. Photodermatol. Photoimmunol. Photomed. 2005;21:118–124. doi: 10.1111/j.1600-0781.2005.00159.x. [DOI] [PubMed] [Google Scholar]
- 60.Shany-Kdoshim S., Polak D., Houri-Haddad Y., Feuerstein O. Killing mechanism of bacteria within multi-species biofilm by blue light. J. Oral Microbiol. 2019;11:1–10. doi: 10.1080/20002297.2019.1628577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Wang Y., Wang Y., Wang Y., Murray C.K., Hamblin H.R., Hooper D.C., Dai T. Antimicrobial blue light inactivation of pathogenic microbes: state of the art. Drug Resist. Updat. 2017;33–35:1–22. doi: 10.1016/j.drup.2017.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Aboualizadeh E., Bumah V.V., Masson-Meyers D.S., Eells J.T., Hirschmugl C.J., Enwemeka C.S. Infrared microspectroscopy study: understanding the antimicrobial activity of selected disinfectants against methicillin-resistant Staphylococcus aureus (MRSA) PLoS One. 2017;12(10) doi: 10.1371/journal.pone.0186375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Schmid J., Hoenes K., Vatter P., Hessling M. Antimicrobial effect of visible light—photoinactivation of Legionella rubrilucens by irradiation at 450, 470, and 620 nm. Antibiotics. 2019;8(4):187. doi: 10.3390/antibiotics8040187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Biener G., Masson-Meyers D., Bumah V., Hussey G., Stoneman M., Enwemeka C.S., Raicu V. Blue/violet laser inactivates methicillin-resistant Staphylococcus aureus by altering its transmembrane potential. J. Photochem. Photobiol. B. 2017;170:118–124. doi: 10.1016/j.jphotobiol.2017.04.002. [DOI] [PubMed] [Google Scholar]
- 65.Szundi I., Liao G.L., Einarsdottir O. Near-infrared time-resolved optical absorption studies of the reaction of fully reduced cytochrome c oxidase with dioxygen. Biochem. 2001;40:2332–2339. doi: 10.1021/bi002220v. [DOI] [PubMed] [Google Scholar]
- 66.Karu T.I., Kolyakov S.F. Exact action spectra for cellular responses relevant to phototherapy. Photomed. Laser Surg. 2005;23:355–361. doi: 10.1089/pho.2005.23.355. [DOI] [PubMed] [Google Scholar]
- 67.Passarella S., Casamassima E., Molinari S., Pastore D., Quagliariello E., Catalano I.M., Cingolani A. Increase of proton electrochemical potential and ATP synthesis in rat liver mitochondria irradiated in vitro by helium-neon laser. FEBS Lett. 1984;175:95–99. doi: 10.1016/0014-5793(84)80577-3. [DOI] [PubMed] [Google Scholar]
- 68.Greco M., Guida G., Perlino E., Marra E., Quagliariello E. Increase in RNA and protein synthesis by mitochondria irradiated with helium-neon laser. Biochem. Biophys. Res. Commun. 1989;163:1428–1434. doi: 10.1016/0006-291x(89)91138-8. [DOI] [PubMed] [Google Scholar]
- 69.Pastore D., Greco M., Petragallo V.A., Passarella S. Increase in <--H+/e- ratio of the cytochrome c oxidase reaction in mitochondria irradiated with helium-neon laser. Biochem. Mol. Biol. Int. 1994;34:817–826. [PubMed] [Google Scholar]
- 70.Yu W., Naim J.O., McGowan M., Ippolito K., Lanzafame R.J. Photomodulation of oxidative metabolism and electron chain enzymes in rat liver mitochondria. Photochem. Photobiol. 1997;66:866–871. doi: 10.1111/j.1751-1097.1997.tb03239.x. [DOI] [PubMed] [Google Scholar]
- 71.Callaghan G.A., Riordan C., Gilmore W.S., McIntyre I.A., Allen J.M., Hannigan B.M. Reactive oxygen species inducible by low-intensity laser irradiation alter DNA synthesis in the haemopoietic cell line U937. Lasers Surg. Med. 1996;19:201–206. doi: 10.1002/(SICI)1096-9101(1996)19:2<201::AID-LSM12>3.0.CO;2-9. [DOI] [PubMed] [Google Scholar]
- 72.Grossman N., Schneid N., Reuveni H., Halevy S., Lubart R. 780 nm low power diode laser irradiation stimulates proliferation of keratinocyte cultures: involvement of reactive oxygen species. Lasers Surg. Med. 1998;22:212–218. doi: 10.1002/(sici)1096-9101(1998)22:4<212::aid-lsm5>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 73.Lavi R., Shainberg A., Friedmann H., Shneyvays V., Rickover O., Eichler M., Kaplan D., Lubart R. Low energy visible light induces reactive oxygen species generation and stimulates an increase of intracellular calcium concentration in cardiac cells. J. Biol. Chem. 2003;278:40917–40922. doi: 10.1074/jbc.M303034200. [DOI] [PubMed] [Google Scholar]
- 74.Lubart R., Eichler M., Lavi R., Friedman H., Shainberg A. Low-energy laser irradiation promotes cellular redox activity. Photomed. Laser Surg. 2005;23:3–9. doi: 10.1089/pho.2005.23.3. [DOI] [PubMed] [Google Scholar]
- 75.Eichler M., Lavi R., Shainberg A., Lubart R. Flavins are source of visible-light-induced free radical formation in cells. Lasers Surg. Med. 2005;37:314–319. doi: 10.1002/lsm.20239. [DOI] [PubMed] [Google Scholar]
- 76.Lubart R., Lavi R., Friedmann H., Rochkind S. Photochemistry and photobiology of light absorption by living cells. Photomed. Laser Surg. 2006;24:179–185. doi: 10.1089/pho.2006.24.179. [DOI] [PubMed] [Google Scholar]
- 77.Eichler M., Lavi R., Friedmann H., Shainberg A., Lubart R. Red light-induced redox reactions in cells observed with TEMPO. Photomed. Laser Surg. 2007;25:170–174. doi: 10.1089/pho.2007.2046. [DOI] [PubMed] [Google Scholar]
- 78.Zhang J., Xing D., Gao X. Low-power laser irradiation activates Src tyrosine kinase through reactive oxygen species-mediated signaling pathway. J. Cell. Physiol. 2008;217:518–528. doi: 10.1002/jcp.21529. [DOI] [PubMed] [Google Scholar]
- 79.Wu S., Xing D., Gao X., Chen W.R. High fluence low-power laser irradiation induces mitochondrial permeability transition mediated by reactive oxygen species. J. Cell. Physiol. 2009;218:603–611. doi: 10.1002/jcp.21636. [DOI] [PubMed] [Google Scholar]
- 80.Hockberger P.E. The discovery of the damaging effect of sunlight on bacteria. J. Photochem. Photobiol. B. 2000;58:185–191. doi: 10.1016/s1011-1344(00)00121-4. [DOI] [PubMed] [Google Scholar]
- 81.Lai C.C., Shih T.P., Ko W.C., Tang H.J., Hsueh P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19), The epidemic and the challenges. Int. J. Antimicrob. Agents. 2020;55:105924. doi: 10.1016/j.ijantimicag.2020.105924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Bumah V.V., Aboualizadeh E., Masson-Meyers D., Eells J., Enwemeka C.S., Hirschmugl C. Resistance of B-DNA to blue light induced damage in methicillin-resistant Staphylococcus aureus. J. Photochem. Photobiol. B. 2017;167:150–157. doi: 10.1016/j.jphotobiol.2016.12.030. [DOI] [PubMed] [Google Scholar]
- 83.Pang P., Wang N., Wang C., Yao Y., Fu X., Yu W., Cai R., Yao M. 460 nm visible light irradiation eradicates MRSA via inducing prophage activation. J. Photochem. Photobiol. B. 2017;166:311–322. doi: 10.1016/j.jphotobiol.2016.12.001. [DOI] [PubMed] [Google Scholar]
- 84.Guo Y.R., Cao Q.D., Hong Z.S., Tan Y.Y., Chen S.D., Jin H.J., Tan K.S., Wang D.Y., Yan Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status. Mil. Med. Res. 2020;7(11):1–10. doi: 10.1186/s40779-020-00240-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.de Lima F.M., Villaverde A.B., Salgado M.A., Castro-Faria-Neto H.C., Munin E., Albertini R., Aimbire F. Low intensity laser therapy (LILT) in vivo acts on the neutrophils recruitment and chemokines/cytokines levels in a model of acute pulmonary inflammation induced by aerosol of lipopolysaccharide from Escherichia coli in rat. J. Photochem. Photobiol. B. 2010;101:271–278. doi: 10.1016/j.jphotobiol.2010.07.012. [DOI] [PubMed] [Google Scholar]
- 86.Brochetti R.A., Leal M.P., Rodrgues R., da Palma P.K., de Oliveira L.V.F., Horliana A.C.R.T., Damazo A.S., de Oliveira A.P.L., Paula Vieira R., Lino-Dos-Santos-Franco A. Photobiomodulation therapy improves both inflammatory and fibrotic parameters in experimental model of lung fibrosis in mice. Lasers Med. Sci. 2017;32:1825–1834. doi: 10.1007/s10103-017-2281-z. [DOI] [PubMed] [Google Scholar]
- 87.de Brito A.A., da Silveira E.C., Rigonato-Liveira N.C., Soares S.S., Brandao-Rangel M.A.R., Soares C.R., Santos T.G., Alves C.E., Herculano K.Z., Vieira R.P., Lino-dos-Santos-Franco A., Albertini R., Aimbire F., de Oliveira A.P. Low-level laser therapy attenuates lung inflammation and airway remodeling in a murine model of idiopathic pulmonary fibrosis, Relevance to cytokines secretion from lung structural cells. J. Photochem. Photobiol. B. 2020;203:111731. doi: 10.1016/j.jphotobiol.2019.111731. [DOI] [PubMed] [Google Scholar]
- 88.Aguiar A.C.C., Murce E., Cortopassi W.A., Pimentel A.S., Almeida M., Barros D.C.S., Guedes J.S., Meneghetti M.R., Krettli A.U. Chloroquine analogs as antimalarial candidates with potent in vitro and in vivo activity. Int. J. Parasitol. Drug Resist. 2018;8:459–464. doi: 10.1016/j.ijpddr.2018.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Savarino A., Boelaert J.R., Cassone A., Majori G., Cauda R. Effects of chloroquine on viral infections: an old drug against today's diseases? Lancet Infect. Dis. 2003;3:722–727. doi: 10.1016/S1473-3099(03)00806-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Vincent M.J., Bergeron E., Benjannet S., Erickson B.R., Rollin P.E., Ksiazek T.G., Seidah N.G., Nichol S.T. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol. J. 2005;2:69. doi: 10.1186/1743-422X-2-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Askenova I.Z., Burduli N.M. Pathogenetic effects of low-intensity laser therapy for chronic obstructive pulmonary disease. Ter. Arkh. 2015;88:32–35. doi: 10.17116/terarkh201688332-35. [DOI] [PubMed] [Google Scholar]
- 92.Yusupalieva M.M., Savtchenko V.M. The effectiveness of combined laser therapy for the treatment of the patients presenting with bronchial asthma and concomitant allergic rhinitis. Vopr. Kurortol. Fizioter. Lech. Fiz. Kult. 2017;94:14–18. doi: 10.17116/kurort201794414-18. [DOI] [PubMed] [Google Scholar]
- 93.Jarvis D.L., Garcia A., Jr. Long-term stability of baculoviruses stored under various conditions. BioTechniques. 1994;16:508–513. [PubMed] [Google Scholar]
- 94.Richardson T.B., Porter C.D. Inactivation of murine leukaemia virus by exposure to visible light. Virology. 2005;341:321–329. doi: 10.1016/j.virol.2005.07.025. [DOI] [PubMed] [Google Scholar]
- 95.Muller-Breitkreutz K., Mohr H., Briviba K., Sies H. Inactivation of viruses by chemically and photchemically generated singlet molecular oxygen. J. Photochem. Photobiol. B. 1995;30(1):63–70. doi: 10.1016/1011-1344(95)07150-z. [DOI] [PubMed] [Google Scholar]
- 96.Bachmann B., Knuver-Hopf J., Lambrecht B., Mohr H. Target structures for HIV-1 inactivation by methylene blue and light. J. Med. Virol. 1995;47:172–178. doi: 10.1002/jmv.1890470211. [DOI] [PubMed] [Google Scholar]
- 97.Wagner S.J. Virus inactivation in blood components by photoactive phenothiazine dyes. Transfus. Med. Rev. 2002;16:61–66. doi: 10.1053/tmrv.2002.29405. [DOI] [PubMed] [Google Scholar]
- 98.Schuit M., Gardner S., Wood S., Bower K., Williams G., Freeburger D., Dabisch P. The influence of simulated sunlight on the inactivation of influenza virus in aerosols. J. Infect. Dis. 2020;221:372–378. doi: 10.1093/infdis/jiz582. [DOI] [PubMed] [Google Scholar]