

Abstract
Objective:
To provide contemporary estimates of internists’ perceptions of adverse effects associated with proton pump inhibitors (PPIs) and self-reported clinical use.
Methods:
We invited 799 internists, including specialists and post-graduate trainees, to complete an online survey. Topics included perceptions of PPI adverse effects (AEs) and effectiveness for upper gastrointestinal bleeding (UGIB) prevention, changes in prescribing, and management recommendations for patients using PPIs for gastroesophageal reflux disease (GERD) or UGIB prevention. For the high-risk UGIB prevention scenario, we used logistic regression to identify factors associated with appropriate PPI continuation.
Results:
Among 437 respondents (55% response rate), 10% were trainees and 72% specialized in general medicine. 70% were somewhat/very concerned about PPI AEs and 76% had somewhat/very much changed their prescribing. A majority believed PPIs increase the risk for 6 of 12 AEs queried. 52% perceived PPIs to be somewhat/very effective for UGIB prevention. In a GERD scenario in which PPI can be safely discontinued, 86% appropriately recommended PPI discontinuation. However, in a high-risk UGIB prevention scenario in which long-term PPI use is recommended, 79% inappropriately recommended discontinuation. In this latter scenario, perceived effectiveness for bleeding prevention was strongly associated with continuing PPI (OR 7.68, p<0.001 for moderately; OR 17.3, p<.001 for very effective). Other covariates, including concern about PPI AEs, had no significant association.
Conclusions:
Most internists believe PPIs cause multiple AEs and recommend discontinuation even in patients at high risk for UGIB. Future interventions should focus on ensuring that PPIs are prescribed appropriately according to individual risks and benefits.
Keywords: Gastroprotection, Gastrointestinal bleeding, Adverse effects, Proton pump inhibitor, Survey
Introduction
Proton pump inhibitors (PPIs) are one of the most commonly used drug classes in the United States (1) but are often used at higher doses and longer than necessary for gastroesophageal reflux disease (GERD) (2–6). The appropriate use of these potent acid-reducing medications has become a topic of growing interest in recent years due to case-control and cohort studies linking PPIs to numerous clinical conditions, including bone fractures (7), C. difficile infection (8), pneumonia (9), and various vitamin and mineral deficiencies (10). However, the clinical significance of many of these studies is unclear since data are mostly lacking to support a definite causal link in most cases (11), and a recent randomized trial of pantoprazole found that they were associated with an increased risk for enteric infection only (12).
To address overuse of PPIs, in 2012 the American Board of Internal Medicine’s Choosing Wisely Campaign included conditional recommendations for dose-reduction or discontinuation of PPIs in some patients with GERD (13). The following year, a survey of internists found that rather than recommending stopping PPIs when used for GERD, they more often inappropriately recommended stopping PPIs when used for the prevention of upper gastrointestinal bleeding (UGIB) (14). The results of this survey highlighted the need to carefully consider a patient’s medical history, symptoms, and concurrent medications before deprescribing. Failure to do so can be perilous: For those patients at increased risk of UGIB, discontinuation can lead to bleeding events, with potential long-term morbidity and mortality, particularly in older adults with comorbid illness (15–17). Indeed, PPI gastroprotection is recommended for patients at high risk for UGIB (18,19).
Since the prior survey, decision-making around the use of PPIs has become even more complex. PPIs have been linked to other serious conditions, including chronic kidney disease (20), dementia (21), and excess risk of death (22), and additional guidance supporting PPI deprescribing has been published (23). In the setting of a dynamic evidence base, little is known about how healthcare providers now perceive the adverse effects (AEs) associated with PPIs, or if they are appropriately changing their prescribing, and deprescribing, practices as a result. To gain greater insight into physicians’ current perceptions of PPI AEs, as well as their benefits for preventing UGIB, and how these perceptions are associated with PPI prescribing behavior, we conducted an online national survey of physician members of the American College of Physicians (ACP).
Methods
Study population
Together with the ACP, we conducted an Internet-based national survey of internal medicine physicians, including residents and fellows, in general practice or any medical subspecialty. Participants were drawn from the Internal Medicine Insider research panel maintained by the ACP Research Center (24). The panel includes 1,730 ACP members who have volunteered to participate in periodic surveys, and it is representative of the larger ACP by member class (e.g., trainee vs. fellow vs. master). The panel excludes medical students, affiliate members (non-physicians), honorary fellows, and non-U.S. members. Since its inception in 2011, it has been regularly adjusted to also represent ACP membership across multiple demographics. We invited 799 physicians to participate after excluding panel members who had previously reported that they were retired, not currently working in the medical field, or spending <25% of time in direct patient care.
Questionnaire Development and Content
We developed a 34-item multiple-choice survey with input from the Center for Bioethics and Social Sciences in Medicine at the University of Michigan, which includes faculty with expertise in risk communication and decision making (BZF). The survey contained questions about general familiarity with and concern about possible PPI AEs, and awareness of and beliefs about whether PPIs in fact increase the risk for any of 12 conditions that have been associated with PPIs. For possible AEs they were aware of, participants were asked which ones they worry most about when prescribing PPIs. We also asked how often patients using PPIs bring up concerns about AEs and how often the physicians personally discuss the risks and benefits of PPIs before prescribing them. In addition, we asked the extent to which physicians had changed their PPI prescribing habits as result of studies on AEs.
Next, we presented participants with four separate common clinical scenarios all featuring a 70-year old female patient who uses omeprazole 20 mg daily and has recently been diagnosed with osteopenia, which would increase her risk for bone fracture, a condition that has associated with PPIs (Supplement 1) (7). The scenarios varied in the degree of the patient’s UGIB risk (minimal [history of GERD], low [low-dose aspirin], moderate [low-dose aspirin and warfarin], and high [prior PUD and low-dose aspirin]). Following each scenario, we queried how the participant would manage the patient’s PPI with the following response options: (1) Continue the omeprazole; (2) Stop the omeprazole; and (3) Stop the omeprazole and also start an H2-blocker, such as ranitidine (Zantac). The order in which the scenarios were presented to participants was randomized. Following the high-risk UGIB prevention scenario, participants were asked how effective they believed omeprazole is at reducing the risk of UGIB in that case on a Likert-type scale (response options: not at all, slightly, moderately, very). Our estimates of UGIB risk for each scenario, of which the survey participants were not informed, are based on prior risk estimates (25,26). For the low-, medium-, and high-risk UGIB scenarios presented in the survey, the annual risks of UGIB are estimated to be 0.5% per year, 1.5% per year, and 2.7% per year without PPI. Recent recommendations on appropriate PPI discontinuation would support PPI discontinuation in the GERD scenario (23), while recommendations on use of PPI gastroprotection support its use in the moderate-risk and high-risk GI bleed scenarios but not the low-risk scenario (18,19).
Finally, we asked about basic demographic, professional, and practice characteristics, familiarity with guidelines on appropriate use of PPIs, and availability of decision support to help with appropriate continuation or discontinuation of PPIs. Practice characteristics were not obtained for residents or fellows.
The full survey can be found in Supplement 2.
Survey distribution
The first email invitation was sent on June 11, 2018. Three additional reminder emails were sent to non-responders before the survey was closed on June 26, 2018. Each participant who completed the survey was given participation points that could be redeemed for a $10 Amazon gift card.
Analysis
For categorical variables, we calculated descriptive statistics, including frequencies and percentages. In calculating the frequency of awareness of and beliefs about AEs, we combined the categories osteoporosis/osteopenia with bone fracture under the heading “bone loss or fracture.”
We then conducted an exploratory multivariable analysis to evaluate independent predictors of continuing PPI in the high-risk UGIB prevention scenario. We selected this scenario because it had the strongest indication for PPI continuation and a high proportion of participants choosing to deviate from that strategy. The dichotomous outcome was defined as PPI continuation vs. (stopping PPI or switching to an H2-blocker) (“PPI discontinuation”) since H2-blockers are likely inferior to PPIs for the purposes of UGIB prevention and are not recommended for this purpose (27). For predictors, we included concern about PPI AEs, perceived PPI effectiveness for preventing UGIB, age, gender, trainee status, number of patients seen per week, familiarity with guidelines on PPI use for prevention of UGIB, and availability of decision support for appropriate PPI use. Concern about PPI AEs and perceived effectiveness of PPIs for UGIB prevention were both analyzed as four-level indicator variables with “not at all” as the base category. Because of the presence of complete separation of one of the predictors (PPI effectiveness) by the outcome variable, which precluded maximum likelihood estimation of the model, we merged two levels of the scale for PPI effectiveness (not at all effective, and slightly effective) into a single level for the regression. Logistic regression was used first to assess the bivariate relationship between the predictor variables and management of the clinical scenario, as well as for the final multivariable model. We hypothesized that concern about AEs and perceived effectiveness for bleeding prevention would respectively be negatively and positively associated with recommending PPI continuation. In this model, four cases had missing data on age and were excluded.
This study was approved as exempt research by the IRB at the University of Michigan Medical School. We used Stata version 15.0 for all analyses.
Role of funding source
This project was supported by NIDDK K23 118179–01A1 (JEK) and VA SDR I01 HX002693–01 (YXY, LL, SDS). The funding source had no role in the study’s design, conduct, or reporting.
Results
Sample characteristics
The response rate was 55% (440 responses out of 799 invitations). Twenty-two participants who had previously reported to the ACP that they spent >25% time on patient care (and were therefore invited to participate), reported in this survey spending <25% time on patient care. These participants were included in the analysis, but we excluded three respondents because they reported not seeing any patients, for a final sample size of 437. Our sample was predominantly male (64%) with a mean age of 48 years (SD 12; Table 1). Ten percent were trainees, 87% were board certified, and 72% specialized in general internal medicine. Only 1% were gastroenterologists. Seventy-seven percent of respondents saw outpatients in clinic. The largest share of participants was part of either a group practice (29%) or academic practice (28%). Most participants reported familiarity with guidance on appropriate use of PPIs to prevent UGIB (67%), while 22% had decision support available to help with appropriate continuation or discontinuation of PPIs.
Table 1.
Participant characteristics
| Gender | |
| Female | 143 (32.7%) |
| Male | 280 (64.1%) |
| Decline to answer | 14 (3.2%) |
| Age (years; mean +/− SD) | 48 +/− 12 |
| Training level | |
| Residency | 30 (6.9%) |
| Fellowship | 15 (3.4%) |
| Non-trainee physician | 392 (89.7%) |
| Specialty | |
| Trainee | 45 (10.3%) |
| Internal medicine | 314 (71.8%) |
| Gastroenterology | 6 (1.4%) |
| Cardiology | 8 (1.83%) |
| Other | 64 (14.6%) |
| Year of residency completion | |
| Trainee | 45 (10.3%) |
| 1960–69 | 2 (0.5% |
| 1970–79 | 17 (3.9%) |
| 1980–89 | 83 (19.0%) |
| 1990–99 | 98 (22.4%) |
| 2000–09 | 103 (23.6%) |
| 2010–2018 | 89 (20.4%) |
| Board certified | |
| Trainee | 45 (10.3%) |
| Yes | 380 (87.0%) |
| No | 12 (2.8%) |
| See outpatients in clinic | |
| Yes | 337 (77.1%) |
| No | 100 (22.9%) |
| Patients seen per week | |
| 1–25 | 77 (17.6%) |
| 26–50 | 120 (27.5%) |
| 51–75 | 114 (26.1%) |
| 76–100 | 88 (20.1%) |
| >100 | 38 (8.7%) |
| Patients seen per week on PPI | |
| None | 2 (0.5%) |
| 1–25 | 329 (75.3%) |
| 26–50 | 88 (20.1%) |
| 51–75 | 14 (3.2%) |
| 76–100 | 1 (0.2%) |
| >100 | 3 (0.7%) |
| Percent patient care | |
| <25% | 22 (5.0%) |
| 25–49% | 47 (10.8%) |
| 50–74% | 73 (16.7%) |
| 75–100% | 295 (67.5%) |
| Practice type | |
| Solo | 48 (11.0%) |
| Group | 125 (28.6%) |
| Academic | 121 (27.7%) |
| VA | 19 (4.4%) |
| Military/government | 9 (2.1%) |
| Hospital employed – integrated health system | 42 (9.6%) |
| Hospital employed – private practice model | 73 (16.7%) |
| Familiar with guidelines on appropriate use of PPIs to prevent upper GI bleeding | |
| Yes | 294 (67.3%) |
| No | 143 (32.7) |
| Decision support available to help with appropriate continuation or discontinuation of PPIs | |
| Yes | 97 (22.2%) |
| No | 340 (77.8%) |
VA = Veterans Affairs.
Perceptions and experience with PPIs
Most participants reported being somewhat or very (93%) familiar with published data on PPI AEs, 70% were somewhat or very concerned about AEs when prescribing PPIs, and 76% had somewhat or very much changed their prescribing practices for PPIs (Table 2).
Table 2.
Perceptions of and beliefs about PPI adverse effects and changes in prescribing habits. PPI= proton pump inhibitor.
| Not at all | Slightly | Somewhat | Very much | |
|---|---|---|---|---|
| Familiar with published data on PPI adverse effects | 1 (0.2%) | 30 (6.9%) | 269 (61.6%) | 137 (31.4%) |
| Concerned about adverse effects when prescribing PPIs | 15 (3.4%) | 118 (27.0%) | 208 (47.6%) | 96 (22.0) |
| Have changed PPI prescribing habits as a result of studies on adverse effects* | 30 (6.9%) | 75 (17.2%) | 224 (51.3%) | 107 (24.5%) |
Participants with no familiarity of published data on PPI adverse effects were not prompted with this question (n=1)
Eighty-one percent of participants reported sometimes or often discussing the risks/benefits of PPIs before prescribing them, while fewer (42%) reported patients sometimes or often bringing up concerns about AEs.
Concern about specific adverse effects
Among the 12 conditions associated with PPIs that we asked respondents to consider, the greatest proportion reported being aware of bone loss or fracture (96%), C. difficile infection (93%), and pneumonia (90%). For the others, rates of awareness were: B12 deficiency 82%, chronic kidney disease 72%, vitamin D deficiency 70%, acute interstitial nephritis 70%, gastric cancer 68%, dementia 68%, death 63%, heart attack 61%, and stroke 58%. Participants endorsed believing that PPIs increase the risk for a mean of 5.2 (SD 2.5) different conditions, most often bone loss or fracture (88%), C difficile infection (82%), and pneumonia (70%; Figure 1). Ninety-seven percent endorsed believing that PPIs increase the risk for at least one condition. Relatively few respondents believed that PPIs increase the risk of death (14%), heart attack (11%), or stroke (7%). For these three conditions, there were the greatest differences between rates of awareness and belief that PPIs are a cause, roughly 50% for all three. For chronic kidney disease, 43% believed that PPIs increase the risk. When prescribing PPIs, the conditions for which the highest proportion of participants expressed the most concern were C. difficile infection (28%) and bone loss or fracture (25%).
Figure 1.
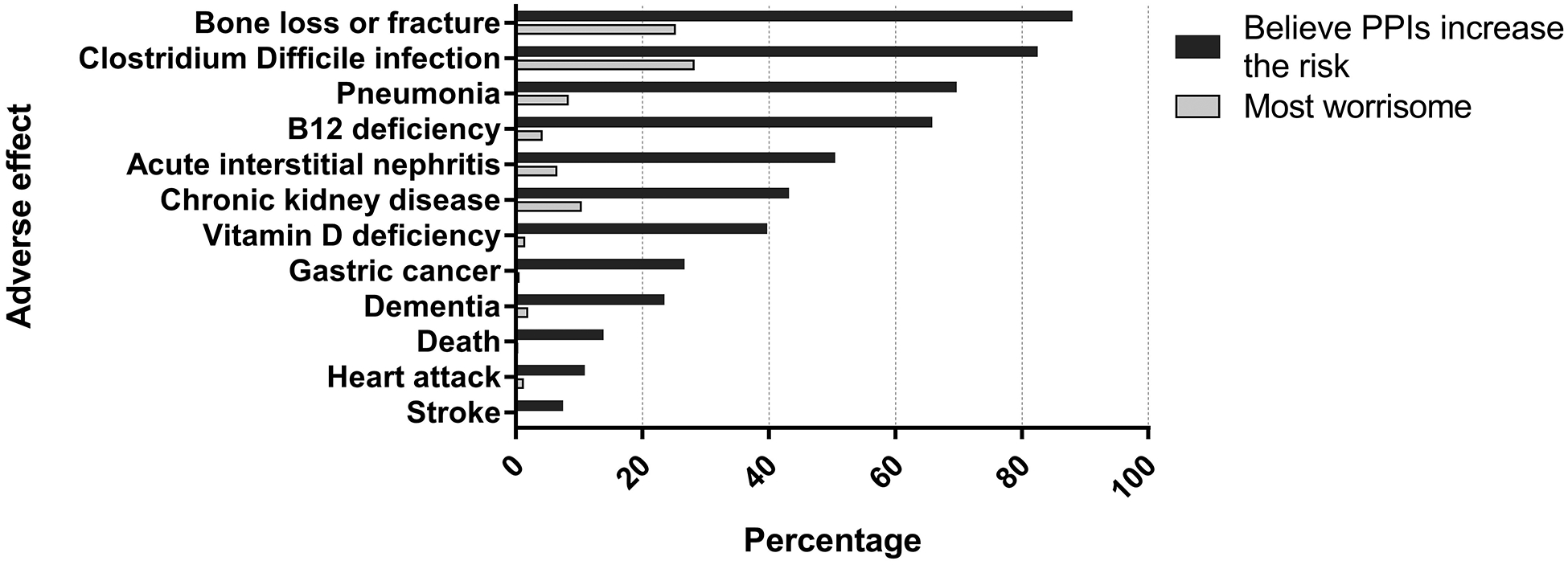
Participants’ beliefs about whether PPIs increase the risk for any of 12 specific adverse effects, and perception of the most worrisome adverse effect. Twelve respondents did not believe PPIs increased the risk for any adverse effects, and 34 participants who believed PPIs caused at least one adverse effect answered “none of the above” when asked which adverse effect was most worrisome.
Management of the patient scenarios and perceived effectiveness of PPIs for UGIB prevention
The majority (67%) of participants recommended stopping the PPI with or without an H2 blocker in all four of the clinical scenarios (Figure 2). The rate of PPI continuation in the GERD scenario was 14%, and in the low-, moderate-, and high-risk UGIB prevention scenarios, 9%, 14%, and 21% respectively. For the GERD scenario, the most common recommendation was to switch the PPI to an H2 blocker. In contrast, for all three of the scenarios for which the PPI indication was prevention of UGIB, the most common management decision was to discontinue the PPI without starting an H2 blocker, followed by switching to an H2 blocker, with the smallest proportion electing to continue the PPI. In the high-risk scenario, 48% recommended stopping the PPI without starting an H2 blocker, and 31% recommended switching to an H2 blocker. In that same scenario, PPIs were perceived to be not effective for UGIB prevention by 13%, slightly effective by 35%, moderately effective by 40%, and very effective by 12%.
Figure 2.
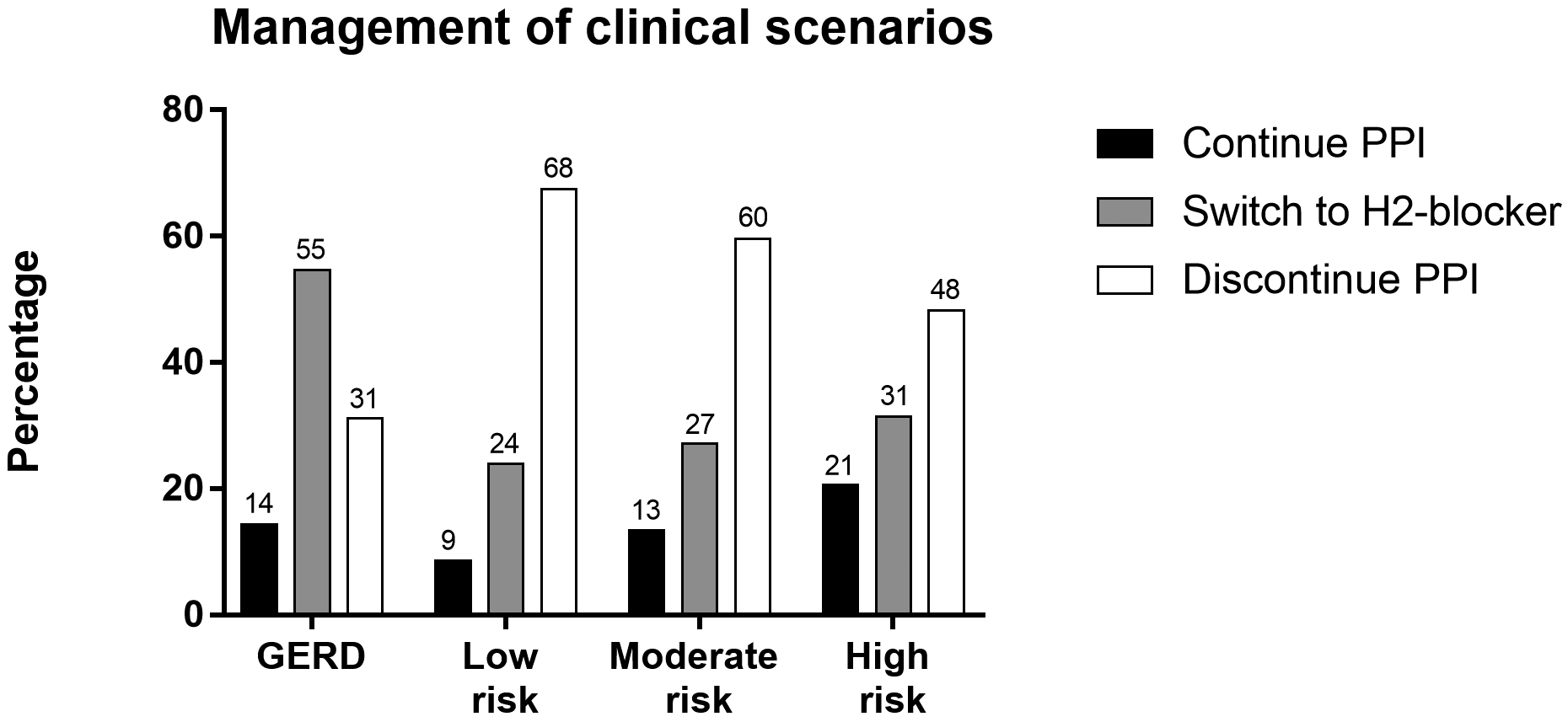
Recommendations for management of proton pump inhibitor in clinical scenarios by indication, including varying levels of upper gastrointestinal bleeding risk. Management options presented to survey participants were continue PPI, switch PPI to H2-blocker, or stop PPI. See Supplement 1 for scenario descriptions. GERD = gastroesophageal reflux disease. PPI= proton pump inhibitor.
Predictors of PPI continuation in high-risk GI bleed scenario
In the multivariable analysis, perceived effectiveness of PPI for preventing UGIB was strongly positively associated with PPI continuation in a dose-dependent fashion. Among participants reporting that PPIs were not at all or slightly effective for preventing UGIB, only 5% recommended PPI continuation (Table 3). For participants who perceived PPIs to be moderately effective (versus not at all or slightly effective), the odds of continuation were increased by 7.68 times (95% CI [3.77, 15.6]; p<0.001), and for participants who perceived PPIs to be very effective, the odds of PPI continuation were increased 17.3 times (95% CI [7.35, 40.8]; p<0.001). Concern about PPI AEs did not have a significant association with PPI continuation, nor did age, gender, trainee status, patient volume, availability of decision support for appropriate PPI use, or familiarity with guidelines.
Table 3.
Multivariable regression model for management of high-risk upper gastrointestinal bleed prevention scenario. Outcome variable was continuation of proton pump inhibitor (vs. discontinuation with or without starting H2 blocker), such that an odds ratio >1 indicates a higher odds of PPI continuation. N=433 for the multivariable regression; data for age were missing for four participants. Age was analyzed in the multivariable model as a continuous variable.
| n (%) discontinuing PPI (N=344) | n (%) continuing PPI (N=89) | Unadjusted OR (95% CI) | Multivariable OR (95% CI) | p-value | |
|---|---|---|---|---|---|
| Age (years) | |||||
| 20–39 | 94 (27.3%) | 35 (39.3%) | |||
| 40–59 | 167 (48.6%) | 35 (39.3%) | |||
| 60–79 | 83 (24.1%) | 18 (20.2%) | |||
| >80 | 0 (0%) | 1 (1.1%) | 0.987 (0.968, 1.01) | 0.999 (0.975, 1.02) | 0.95 |
| Male | 228 (66.28%) | 63 (70.8%) | 1 (reference) | 1 (reference) | |
| Female | 116 (33.72%) | 26 (29.2%) | 0.811 (0.488, 1.35) | 0.714 (0.400,1.28) | 0.26 |
| Non-trainee | 314 (91.3%) | 74 (83.2%) | 1 (reference) | 1 (reference) | |
| Trainee | 30 (8.7%) | 15 (16.8%) | 2.12 (1.09, 4.14) | 2.58 (0.956, 6.98) | 0.06 |
| Patients seen per week | |||||
| 1–25 | |||||
| 26–50 | 59 (17.2) | 17 (19.1) | 1 (reference) | 1 (Reference) | - |
| 51–75 | 100 (29.1) | 19 (21.4) | 0.659 (0.318, 1.37) | 0.928 (0.389, 2.22) | 0.87 |
| 76–100 | 91 (26.5) | 22 (24.7) | 0.839 (0.411, 1.71) | 1.11 (0.468, 2.64) | 0.81 |
| >100 | 62 (18.0) | 25 (28.1) | 1.40 (0.687, 2.85) | 1.87 (0.765, 4.57) | 0.17 |
| 32 (9.3) | 6 (6.74) | 0.651 (0.233, 1.81) | 0.642 (0.186, 2.21) | 0.48 | |
| Decision support for PPI use | |||||
| Yes | 70 (20.4%) | 26 (29.2%) | 1 (reference) | 1 (reference) | |
| No | 274 (79.6%) | 63 (70.8%) | 0.619 (0.365, 1.05) | 1.62 (0.847, 3.11) | 0.14 |
| Familiar with guidelines on PPI use for bleeding prevention | |||||
| Yes | |||||
| No | 222 (64.5) | 69 (77.5) | 1 (reference) | 1 (reference) | |
| 122 (35.5) | 20 (22.5) | 0.527 (0.306, 0.909) | 1.63 (0.878, 3.02) | 0.12 | |
| Concern about PPI adverse effects | |||||
| Not at all | 10 (2.9%) | 5 (5.6%) | 1 (Reference) | 1 (Reference) | |
| Slightly | 86 (25.0%) | 31 (34.8%) | 0.721 (0.228, 2.28) | 0.748 (0.186, 3.00) | 0.68 |
| Somewhat | 166 (48.3%) | 40 (44.9%) | 0.482 (0.156, 1.49) | 0.499 (0.128, 1.95) | 0.32 |
| Very | 82 (23.8%) | 13 (14.6%) | 0.317 (0.934, 1.08) | 0.243 (0.0565, 1.04) | 0.06 |
| Perceived effectiveness of PPI for preventing upper GI bleeding | |||||
| Not at all or slightly | 193 (56.1%) | 11 (12.4%) | 1 (Reference) | 1 (Reference) | - |
| Moderately | 122 (35.5%) | 53 (59.6%) | 7.62 (3.83, 15.2) | 7.68 (3.77, 15.6) | <0.001 |
| Very | 29 (8.4%) | 25 (28.1%) | 15.1 (6.73, 34.0) | 17.3 (7.35, 40.8) | <0.001 |
Discussion
In this survey of internists in the United States, we found that a majority of participants are concerned about AEs from PPIs and report having changed their PPI prescribing practices as a result. While conclusive evidence is lacking to prove that PPIs actually cause many of the conditions with which they have been associated, our survey has for the first time found that nearly all respondents believe that PPIs increase the risk for one or more AEs (on average 5–6), and most respondents are concerned about PPI AEs when prescribing these drugs. Our findings also shed light on how current PPI prescribing, and deprescribing, practices may affect the use of PPIs for GERD, as well as for prevention of UGIB. In response to common clinical scenarios, most participants recommended stopping a PPI used for GERD (in a case where doing so is appropriate) but also recommended stopping when used for prevention of UGIB (in a case where doing so is appropriate). Only 21% of participants recommended PPI continuation in the latter scneario. These findings demonstrate that internists have received the message that PPIs may be harmful and should be used more restrictively. At the same time, they also raise concerns that efforts to decrease PPI use may have the unintended consequence of exacerbating underuse of PPIs for prevention of UGIB, which has been a persistent problem (28–30).
Our results provide additional insight into the reasons for underuse of PPIs for UGIB prevention. Levels of concern about PPI AEs were not significantly associated with recommending PPI continuation when used for high-risk UGIB prevention. However, perceived effectiveness of PPIs for prevention of bleeding was strongly associated with appropriate PPI continuation in this setting, with participants who believed PPIs were moderately effective having 7.7 times the odds of PPI continuation, and for the those who believed they were very effective, 17.3 times the odds in our adjusted model. Taken together, these findings suggest that the default management option for PPIs is discontinuation, regardless of indication, but that an understanding of the benefits for UGIB prevention can motivate appropriate PPI continuation in this context.
While prior studies have documented inappropriate prescribing of PPIs in the outpatient setting, few have examined the appropriateness of PPI deprescribing, which has been widely recommended (23,31). In 2013, we conducted a similar scenario-based survey of ACP members to investigate recommendations for management of PPIs, prior to more recent articles on conditions associated with PPIs. The scenarios for high-risk UGIB prevention and GERD were nearly identical the survey reported here, but there were slight differences in the response options: In the earlier the survey, no option for switching to H2 blocker was given. In the 2013 survey, 62% of participants recommended stopping PPI in the high-risk UGIB prevention scenario, and 32% recommended stopping in the GERD scenario, compared to 79% and 86%, respectively, in the survey reported here. In the last 5 years, internists have thus become more restrictive in their use of PPIs for GERD, in keeping with recent recommendations, but also have become more guideline-discrepant in their use of PPIs for gastroprotection, allowing for methodologic differences in the two surveys. Prior studies have shown that patients, for their part, are also concerned about PPI AEs. A 2017 survey of adults with GERD in the United States found that 79% had some degree of concern about AEs (32). Furthermore, 39% of patients had tried stopping their PPI, most without involving their health care providers, and patients who were high risk for UGIB were no less likely to have tried stopping, underscoring the need for clinicians to be vigilant about this issue.
This study has several implications for clinicians. It is imperative to evaluate the risk of upper GI complications when deprescribing is considered, and to understand the role of PPIs for prevention of acid peptic diseases. A meta-analysis of randomized controlled trials demonstrated that PPIs reduce the risk of ulcer bleeds by 79% (27). Accordingly, guidelines support the use of gastroprotection with PPIs (but not H2 blockers) for patients with any two of the following risk factors: thienopyridines, UGIB history (non-variceal) or ulcer history, NSAIDs, anticoagulants, and aspirin; a useful acronym is TUNA2 (18,19,33–36). PPIs are also recommended for certain other high risk groups, including a patients over 65-years-old using NSAIDs (see supplement 3). Some GERD patients are also not appropriate for PPI deprescribing, including those with a history of reflux esophagitis, especially LA grade C or D, or peptic stricture (37). Long-term PPI may also be appropriate for patients with non-erosive reflux esophagitis and symptom recurrence off PPI. As clinicians make these decisions, they should be cognizant of the lack of data supporting a causal relationship between PPIs and many of conditions with which they have been associated. In most cases, the strength of association is weak and can potentially be explained by residual confounding (i.e., at baseline, patients who are prescribed PPIs tend to be sicker than others). The best evidence of a causal link exists for enteric infections, hypomagnesemia, and fundic gland polyps (11). Most convincingly, safety outcomes were prospectively evaluated as part of a recently reported randomized controlled trial of PPI gastroprotection, the strongest possible design to answer this question (12). Over 53,152 person-years of follow up, PPIs were associated with an increased risk for enteric infections only. This study provides evidence that PPIs used for even a few years have little detectable risk, although risks from longer term use could not be evaluated.
For researchers, it will be important to evaluate for unintended consequences of PPI deprescribing (e.g., stopping in the wrong patients, UGIB events). Moreover, new tools are needed to proactively prescribe PPIs to high-risk patients. Several multi-component interventions aimed at reducing high-risk prescribing of NSAIDs and antiplatelet drugs, which included efforts to increase appropriate use of PPI gastroprotection, have proven successful in European countries (38–40), including one which showed a reduction in hospitalizations for GI ulcers and bleeding (38). The intervention strategies included clinician education, informatics tools, feedback on high-risk prescribing, and incentive payments. Point-of-care clinical decision support tools, which roughly one-fifth of respondents report currently having for PPIs, are one potentially appealing intervention strategy that have been shown to improve prescribing of other recommended medications in a prior meta-analysis (41). However, it will be critical to consider the impact on clinician satisfaction and work efficiency given the prevalence of PPI use. Validated point-of-care risk stratification tools are also needed to better characterize individual patients’ UGIB risk.
Our study has a number of strengths. The participants were drawn from a national sample of internists, and our response rate was relatively high. In addition, survey questions were developed in collaboration with experts in survey development and risk communication. Despite these strengths, the study has a number of limitations. First, the survey was administered in 2018, and thus participants’ responses do not reflect the most recent data on PPI AEs (12,42). Second, participants’ management recommendations in clinical scenarios are likely to reflect what they believe to be optimal management strategies but may differ from real-world clinical management; however, the scenarios were designed to be as realistic as possible. Third, the order of the questions in the survey, with questions probing perceptions of AEs preceding the scenarios, may have influenced participants’ responses. Fourth, members of the ACP may not be representative of the broader population of U.S. internists, although rates of board certification are nearly equivalent (43). Finally, because the large majority of participants were general internists, our findings cannot be generalized to medical subspecialists.
In conclusion, we found that most internists believe PPIs have multiple serious AEs and report changing their prescribing practices as a result. Furthermore, they most often recommend PPI discontinuation for patients regardless of whether prescribed for GERD or high-risk UGIB prevention, when stopping is inappropriate. These findings raise concerns that efforts to reduce the use of PPIs could have unintended consequences, such as UGIB. Educational efforts around the use of PPIs should place greater emphasis on appropriate use of PPIs, including the strong evidence base in support of PPIs for the prevention of UGIB. Finally, it is time to develop and disseminate clinically nuanced, user-centered interventions that cannot only facilitate PPI stopping in appropriate candidates, but also PPI initiation in patients at high risk for UGIB, to ensure that decisions around PPI use accurately reflect the true risks and benefits.
Supplementary Material
Study Highlights.
What is known:
Proton pump inhibitor use have been linked with numerous serious clinical conditions, which have been hypothesized to represent adverse effects.
It is not known how clinicians perceive the adverse effects of PPIs or how they may be changing their prescribing.
Currently, the FDA has approved the use of PPIs for the treatment of erosive esophagitis, gastric hypersecretion, gastroesophageal reflux disease, Helicobacter pylori infection and gastric and duodenal ulcers. However, professional guidelines recommend the prophylactic use of PPIs for bleeding prevention in select patients at an increased risk of bleeding.
What is new:
Internists believe PPIs cause on average 5–6 different adverse effects and report changing their prescribing.
Most internists recommend stopping PPIs whether used for reflux or prevention of upper gastrointestinal bleeding in a patient at high risk, when stopping is inappropriate.
Perceived effectiveness of PPIs for bleeding prevention was strongly associated with appropriate continuation when used for prevention of upper gastrointestinal bleeding.
Acknowledgments
Conflict of Interest Disclosure: Sameer D. Saini, MD, MS served as a technical consultant for FMS inc. No other disclosures were reported.
Grant Support: This project was supported by NIDDK K23 118179-01A1 (JEK) and VA SDR I01 HX002693-01 (YXY, LL, SDS). The funding source had no role in the study’s design, conduct, or reporting. The contents do not represent the views of the U.S. Department of Veterans Affairs or the U.S. Government.
Abbreviations:
- AEs
Adverse Effects
- ACP
American College of Physicians
- CI
Confidence Interval
- GERD
Gastroesophageal Reflux Disease
- IRB
Institutional Review Board
- NIDDK
National Institute of Diabetes and Digestive and Kidney Diseases
- OR
Odds Ratio
- PPIs
Proton Pump Inhibitors
- UGIB
Upper Gastrointestinal Bleeding
- VA SDR
Veterans Affairs Service Directed Research
Footnotes
Disclosures: Sameer D. Saini, MD, MS served as a technical consultant for FMS inc.
Guarantor of the Article: Jacob E. Kurlander accepts official responsibility for the overall conduct of this study and publication of this manuscript.
References
- 1.List of Top 50 Prescription Drugs Filled in the US [Internet]. RetailMeNot Rx Saver. 2016. [cited 2018 Dec 18]. Available from: https://www.lowestmed.com/top-50-prescription-drugs-filled/
- 2.Gawron AJ, Pandolfino JE, Miskevics S, Lavela SL. Proton pump inhibitor prescriptions and subsequent use in US veterans diagnosed with gastroesophageal reflux disease. J Gen Intern Med. 2013. July;28(7):930–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Heidelbaugh JJ, Goldberg KL, Inadomi JM. Magnitude and economic effect of overuse of antisecretory therapy in the ambulatory care setting. Am J Manag Care. 2010. September;16(9):e228–234. [PubMed] [Google Scholar]
- 4.Metaxas ES, Bain KT. Review of Proton Pump Inhibitor Overuse in the US Veteran Population. J Pharm Technol. 2015. August 1;31(4):167–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Glew CM, Rentler RJ. Use of proton pump inhibitors and other acid suppressive medications in newly admitted nursing facility patients. J Am Med Dir Assoc. 2007. November;8(9):607–9. [DOI] [PubMed] [Google Scholar]
- 6.Mafi JN, May FP, Kahn KL, Chong M, Corona E, Yang L, et al. Low-Value Proton Pump Inhibitor Prescriptions Among Older Adults at a Large Academic Health System. J Am Geriatr Soc [Internet]. [cited 2019 Sep 12];0(0). Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/jgs.16117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zhou B, Huang Y, Li H, Sun W, Liu J. Proton-pump inhibitors and risk of fractures: an update meta-analysis. Osteoporos Int. 2016. January 1;27(1):339–47. [DOI] [PubMed] [Google Scholar]
- 8.Janarthanan S, Ditah I, Adler DG, Ehrinpreis MN. Clostridium difficile-Associated Diarrhea and Proton Pump Inhibitor Therapy: A Meta-Analysis. Am J Gastroenterol. 2012. July;107(7):1001–10. [DOI] [PubMed] [Google Scholar]
- 9.Sarkar M, Hennessy S, Yang Y-X. Proton-pump inhibitor use and the risk for community-acquired pneumonia. Ann Intern Med. 2008. September 16;149(6):391–8. [DOI] [PubMed] [Google Scholar]
- 10.Hoorn EJ, van der Hoek J, de Man RA, Kuipers EJ, Bolwerk C, Zietse R. A Case Series of Proton Pump Inhibitor–Induced Hypomagnesemia. Am J Kidney Dis. 2010. July;56(1):112–6. [DOI] [PubMed] [Google Scholar]
- 11.Vaezi MF, Yang Y-X, Howden CW. Complications of Proton Pump Inhibitor Therapy. Gastroenterology. 2017. May 18;153(1):35–48. [DOI] [PubMed] [Google Scholar]
- 12.Moayyedi P, Eikelboom JW, Bosch J, Connolly SJ, Dyal L, Shestakovska O, et al. Safety of Proton Pump Inhibitors Based on a Large, Multi-year, Randomized Trial of Patients Receiving Rivaroxaban or Aspirin. Gastroenterology [Internet]. 2019. May 29 [cited 2019 Jul 16];0(0). Available from: https://www.gastrojournal.org/article/S0016-5085(19)40974-8/abstract [DOI] [PubMed] [Google Scholar]
- 13.Treating Heartburn and GERD | Choosing Wisely [Internet]. [cited 2018 Aug 25]. Available from: http://www.choosingwisely.org/patient-resources/treating-heartburn-and-gerd/
- 14.Kurlander JE, Kolbe M, Scheiman JM, Weissman A, Piette JD, Rubenstein JH, et al. The Right Idea for the Wrong Patient: Results of a National Survey on Stopping PPIs. Clin Gastroenterol Hepatol. 2017;15(9):1475–6. [DOI] [PubMed] [Google Scholar]
- 15.Li L, Geraghty OC, Mehta Z, Rothwell PM, Oxford Vascular Study. Age-specific risks, severity, time course, and outcome of bleeding on long-term antiplatelet treatment after vascular events: a population-based cohort study. Lancet. 2017. 29;390(10093):490–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Abraham NS, Noseworthy PA, Inselman J, Herrin J, Yao X, Sangaralingham LR, et al. Risk of Gastrointestinal Bleeding Increases With Combinations of Antithrombotic Agents and Patient Age. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2019. May 18; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Platt KD, Saini SD, Kurlander JE. Selecting the Appropriate Patients for Proton Pump Inhibitor Discontinuation: A Teachable Moment. JAMA Intern Med [Internet]. 2019. July 1 [cited 2019 Jul 2]; Available from: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2737324 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bhatt DL, Scheiman J, Abraham NS, Antman EM, Chan FKL, Furberg CD, et al. ACCF/ACG/AHA 2008 Expert Consensus Document on Reducing the Gastrointestinal Risks of Antiplatelet Therapy and NSAID Use A Report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Circulation. 2008. October 28;118(18):1894–909. [DOI] [PubMed] [Google Scholar]
- 19.Abraham NS, Hlatky MA, Antman EM, Bhatt DL, Bjorkman DJ, Clark CB, et al. ACCF/ACG/AHA 2010 Expert Consensus Document on the Concomitant Use of Proton Pump Inhibitors and Thienopyridines: A Focused Update of the ACCF/ACG/AHA 2008 Expert Consensus Document on Reducing the Gastrointestinal Risks of Antiplatelet Therapy and NSAID Use. Am J Gastroenterol. 2010. December;105(12):2533–49. [DOI] [PubMed] [Google Scholar]
- 20.Lazarus B, Chen Y, Wilson FP, Sang Y, Chang AR, Coresh J, et al. Proton pump inhibitor use and the risk of chronic kidney disease. JAMA Intern Med [Internet]. 2016. [cited 2016 Dec 12];176(2). Available from: http://archinte.jamanetwork.com/article.aspx?articleid=2481157&version=meter+at+null&module=meter-Links&pgtype=Blogs&contentId=&mediaId=%25%25ADID%25%25&referrer=&priority=true&action=click&contentCollection=meter-links-click [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gomm W, von Holt K, Thomé F, Broich K, Maier W, Fink A, et al. Association of proton pump inhibitors with risk of dementia: a pharmacoepidemiological claims data analysis. JAMA Neurol. 2016;73(4):410–416. [DOI] [PubMed] [Google Scholar]
- 22.Xie Y, Bowe B, Li T, Xian H, Yan Y, Al-Aly Z. Risk of death among users of Proton Pump Inhibitors: a longitudinal observational cohort study of United States veterans. BMJ Open. 2017. July 1;7(6):e015735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Farrell B, Pottie K, Thompson W, Boghossian T, Pizzola L, Rashid FJ, et al. Deprescribing proton pump inhibitors: Evidence-based clinical practice guideline. Can Fam Physician. 2017. May 1;63(5):354–64. [PMC free article] [PubMed] [Google Scholar]
- 24.Internal Medicine Insider Research Panel. [Internet] [cited 2016 Nov 14]. Available from: https://iminsider.org/
- 25.Lanas A, Polo-Tomás M, Casado-Arroyo R. The aspirin cardiovascular/gastrointestinal risk calculator - a tool to aid clinicians in practice. Aliment Pharmacol Ther. 2013. April 1;37(7):738–48. [DOI] [PubMed] [Google Scholar]
- 26.Rodríguez LAG, Lin KJ, Hernández-Díaz S, Johansson S. Risk of Upper Gastrointestinal Bleeding With Low-Dose Acetylsalicylic Acid Alone and in Combination With Clopidogrel and Other MedicationsClinical Perspective. Circulation. 2011. March 15;123(10):1108–15. [DOI] [PubMed] [Google Scholar]
- 27.Scally B, Emberson JR, Spata E, Reith C, Davies K, Halls H, et al. Effects of gastroprotectant drugs for the prevention and treatment of peptic ulcer disease and its complications: a meta-analysis of randomised trials. Lancet Gastroenterol Hepatol. 2018. April 1;3(4):231–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Medlock S, Eslami S, Askari M, Taherzadeh Z, Opondo D, de Rooij SE, et al. Co-prescription of Gastroprotective Agents and Their Efficacy in Elderly Patients Taking Nonsteroidal Anti-inflammatory Drugs: A Systematic Review of Observational Studies. Clin Gastroenterol Hepatol. 2013. October;11(10):1259–1269.e10. [DOI] [PubMed] [Google Scholar]
- 29.Abraham NS, El–Serag HB, Johnson ML, Hartman C, Richardson P, Ray WA, et al. National Adherence to Evidence-Based Guidelines for the Prescription of Nonsteroidal Anti-Inflammatory Drugs. Gastroenterology. 2005. October;129(4):1171–8. [DOI] [PubMed] [Google Scholar]
- 30.Kurlander JE, Gu X, Scheiman JM, Haymart B, Kline-Rogers E, Saini SD, et al. Missed opportunities to prevent upper GI hemorrhage: The experience of the Michigan Anticoagulation Quality Improvement Initiative. Vasc Med. 2019. April 1;24(2):153–5. [DOI] [PubMed] [Google Scholar]
- 31.Schoenfeld AJ, Grady D. Adverse Effects Associated With Proton Pump Inhibitors. JAMA Intern Med. 2016. February 1;176(2):172–4. [DOI] [PubMed] [Google Scholar]
- 32.Kurlander JE, Kennedy JK, Rubenstein JH, Richardson CR, Krein SL, De Vries R, et al. Patientsʼ Perceptions of Proton Pump Inhibitor Risks and Attempts at Discontinuation: A National Survey. Am J Gastroenterol. 2019. February;114(2):244–9. [DOI] [PubMed] [Google Scholar]
- 33.Freedberg DE, Kim LS, Yang Y-X. The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology. 2017. March;152(4):706–15. [DOI] [PubMed] [Google Scholar]
- 34.Barkun AN, Almadi M, Kuipers EJ, Laine L, Sung J, Tse F, et al. Management of Nonvariceal Upper Gastrointestinal Bleeding: Guideline Recommendations From the International Consensus Group. Ann Intern Med [Internet]. 2019. October 22 [cited 2019 Nov 22]; Available from: https://annals.org/aim/fullarticle/2753604/management-nonvariceal-upper-gastrointestinal-bleeding-guideline-recommendations-from-international-consensus [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Valgimigli M, Bueno H, Byrne RA, Collet J-P, Costa F, Jeppsson A, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTSThe Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2018. January 14;39(3):213–60. [DOI] [PubMed] [Google Scholar]
- 36.Lanza FL, Chan FKL, Quigley EMM. Guidelines for Prevention of NSAID-Related Ulcer Complications. Am J Gastroenterol. 2009. March;104(3):728–38. [DOI] [PubMed] [Google Scholar]
- 37.Targownik L Discontinuing Long-Term PPI Therapy: Why, With Whom, and How? Am J Gastroenterol. 2018. April;113(4):519–28. [DOI] [PubMed] [Google Scholar]
- 38.Dreischulte T, Donnan P, Grant A, Hapca A, McCowan C, Guthrie B. Safer Prescribing--A Trial of Education, Informatics, and Financial Incentives. N Engl J Med. 2016. March 17;374(11):1053–64. [DOI] [PubMed] [Google Scholar]
- 39.Avery AJ, Rodgers S, Cantrill JA, Armstrong S, Cresswell K, Eden M, et al. A pharmacist-led information technology intervention for medication errors (PINCER): a multicentre, cluster randomised, controlled trial and cost-effectiveness analysis. The Lancet. 2012. April 7;379(9823):1310–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Guthrie B, Donnan PT, Murphy DJ, Makubate B, Dreischulte T. Bad apples or spoiled barrels? Multilevel modelling analysis of variation in high-risk prescribing in Scotland between general practitioners and between the practices they work in. BMJ Open. 2015. November 1;5(11):e008270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Bright TJ, Wong A, Dhurjati R, Bristow E, Bastian L, Coeytaux RR, et al. Effect of Clinical Decision-Support Systems: A Systematic Review. Ann Intern Med. 2012. July 3;157(1):29. [DOI] [PubMed] [Google Scholar]
- 42.Xie Y, Bowe B, Yan Y, Xian H, Li T, Al-Aly Z. Estimates of all cause mortality and cause specific mortality associated with proton pump inhibitors among US veterans: cohort study. BMJ. 2019. 29;365:l1580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Lipner RS, Young A, Chaudhry HJ, Duhigg LM, Papadakis MA. Specialty Certification Status, Performance Ratings, and Disciplinary Actions of Internal Medicine Residents. Acad Med. 2016. March;91(3):376. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.