

Abstract
Although the effects of high intensity interval training (HIIT) on health and sports performance are well documented, the effects of this training type on mucosal immune function remain unclear. The aim of this study was to assess the impact of an acute HIIT session on salivary immune and endocrine marker levels (immunoglobulin A (sIgA), alpha amylase (sAA), cortisol (C), and testosterone (T)) in male and female endurance athletes. Twenty subjects (ten males and ten females) underwent ten bouts of treadmill running using a 4 min:2 min work:rest ratio at ~90% of peak oxygen uptake (VO2peak). Saliva samples were collected 5 min before and 20 min post-exercise. During work intervals, female participants had a higher HR than male participants (+4.0 ± 5%; p = 0.008). Rating of perceived exertion (RPE) increased throughout the duration of the HIIT session in both males and females (main time effect: p < 0.001), but was higher in males than females (+17 ± 4%; time x gender main effect: p < 0.001). Lactate concentrations were similar in both males and females. Exercise increased the concentration of salivary IgA (males: +24 ± 6%, p = 0.004; females: +27 ± 3%, p = 0.03), salivary alpha-amylase (males: +44 ± 22%, p = 0.036; females: +71 ± 26%, p = 0.026) and salivary cortisol (males: +41 ± 24%, p = 0.015; females: +55 ± 24%, p = 0.005). Testosterone levels and the Testosterone/Cortisol ratio remained stable in both males and females. These findings suggest that the physiological stress produced by a HIIT session does not affect immune function and does not disturb the anabolic/catabolic balance.
Key points.
This study is the first to examine the immune and endocrine responses in well-trained subjects after a single bout of HIIT and to evaluate the influence of the gender on those responses.
After acute session of HIIT, the catabolic/anabolic balance was conserved, though cortisol levels increased in both gender, testosterone levels remained unchanged after HIIT exercise.
Interestingly, one session of HIIT induced a protective immune response since salivary IgA and sAA concentrations increased in both men and women.
HIIT session did not cause immune risk and the anabolic/catabolic balance was preserved.
However, further investigation is warranted to exclude a delayed response in the hours or days following HIIT.
Key words: IgA, alpha amylase, cortisol, testosterone, HIIT
Introduction
High intensity interval training (HIIT) has been recognized as an alternative to classic continuous endurance training, bringing about similar or even greater performance and health benefits (Gibala et al., 2006). It is characterized by short, repeated bouts of high intensity efforts, separated by recovery periods (Gibala et al., 2012). The main physiological changes produced by HIIT include improved substrate utilization (Perry et al., 2008), increased maximal oxygen uptake, improved cardiac and endothelial function (Little et al., 2011; Tjønna et al., 2013), and acute metabolic stress and hormonal responses (Wahl et al., 2013). However, it remains unresolved whether the training load of several HIIT sessions within a short period of time compromises the mucosal immune function.
Exercise causes a constant physiological and psychological stress in elite athletes. Ninety-five percent of infectious pathogens enter through the mucosa of the upper respiratory tract (Neville et al., 2008; Spence et al., 2007), ultimately reducing training effects and athletic performance (Pyne et al., 1998; Gleeson et al., 2001). One of the main players involved in immune system regulation is immunoglobulin A (IgA), being the first line of defense and an indicator of mucosal immune system (Neville et al., 2008). Previous studies have reported reductions in IgA levels following strenuous and repetitive exercise, which might be mediated by training volume and intensity (Trochimiak and Hübner-Woźniak, 2012). The decreased levels in this marker of immune function could lead to the so-called “open window”, during which athletes are more susceptible to upper airway infections (Kakanis et al., 2010). Decreases in salivary IgA concentrations have been reported after both acute and chronic exercise as well as after strenuous and high-volume exercise (Nieman et al., 2002). For instance, IgA concentrations were reduced by 30% after three Wingate tests (MacKinnon and Jenkins, 1993) and by ~50% immediately post-marathon race (Nieman et al., 2006). A 75% decrease in IgA has also been shown after a soccer match in elite male soccer players (Peñailillo et al., 2015).
Salivary alpha amylase (sAA) has been described as the most sensitive stress response marker due to exertion as it is directly produced in saliva (Papacosta and Nassis, 2011; Rohleder et al., 2009). Acute increases in sAA levels have been reported following strenuous activities such as short progressive tests to exhaustion (Allgrove et al., 2008; de Oliveira et al., 2010), and rowing (Kivlighan and Granger, 2006). The increase in sAA levels has been proposed to counteract the reductions in IgA levels, as well as the immune depression commonly observed following strenuous activities (Gatti and De Palo, 2011).
Exercise has been proposed to influence the regulation of testosterone and cortisol levels (Doan et al., 2007; Gatti and De Palo, 2011). Short bouts of endurance exercise tend to increase testosterone levels in both females (Consitt et al., 2002; Cumming et al., 1987; Nindl et al., 2001) and males (Hayes et al., 2015). Elevated circulating cortisol levels have been reported after intense intermittent or continuous endurance exercise in males (Kraemer et al., 1999; Sari-Sarraf et al., 2006) and females (Consitt et al., 2002). Gender differences in cortisol and testosterone levels have been reported in volleyball tournaments, which seem mainly associated to the intensity of the efforts during the matches (Peñailillo et al., 2018).
Although the effects of diverse exercise types on the endocrine and immune responses have been reported, there is still a paucity of data on the responses after a HIIT session and whether these responses differ between males and females. Therefore, besides the well documented effects of HIIT training on health and sport performance, the prophylactic role of this type of training needs to be investigated, considering possible gender differences. The aim of this study was to assess the effect of an acute HIIT session on endocrine- and mucosal immune function of male and female endurance athletes. To this end, endocrine and immune responses were monitored through the changes in salivary testosterone, cortisol, IgA and sAA concentrations after a HIIT session. We hypothesized that one HIIT session would induce a decreased immune response and favour catabolic processes through a decrease in the Testosterone/Cortisol ratio in the early recovery period in both males and females
Methods
Participants
Subjects’ characteristics are presented in Table 1. Ten male and ten female long distance national level runners volunteered to participate. The inclusion criteria included: aged between 18 - 40 years, participating in ≥ five training sessions/week, > 4 years of systematic long distance running training, national competition experience, peak oxygen uptake (VO2peak) ≥ 50ml/kg/min for males and ≥ 40ml/kg/min for females, and no recent musculoskeletal injuries (continuous training in the 6-month period before intervention), cardiovascular or infectious diseases. Female participants were evaluated in the follicular phase of their menstrual cycle to minimize potential effects of estrogen on muscle stress caused by exercise (Enns et al., 2007). The study conformed to the Code of Ethics of the World Medical Association (Declaration of Helsinki) and was approved by the University’s Ethics committee.
Table 1.
Subjects’ characteristics. Data are means ± SD.
| Females (n=10) | Males (n=10) | |
|---|---|---|
| Age (years) | 25.8 ± 6.2 | 21.9 ± 0.8 |
| Height (m) | 1.62 ± 0.07 | 1.75 ± 0.02 * |
| Weight (kg) | 55.7 ± 5.9 | 67. 8 ± 1.8 * |
| BMI (kg/m2) | 21.3 ± 1.6 | 22.4 ± 0.6 |
| FM (%) | 12.9 ± 1.3 | 10.3 ± 0.2 * |
| VO2Peak (ml/kg/min) | 45.9 ± 3.5 | 55.4 ± 2.9 * |
BMI: Body mass index, FM: Percent fat mass, VO2 peak: peak oxygen consumption.
* p < 0.05.
Body composition and VO2peak measurements
Body composition was assessed by body mass index and body fat percentage as estimated from the sum of six skin folds (Slimguide Caliper) (Legaz Arrese et al., 2006). VO2max was measured using an incremental running protocol on a treadmill (h/p/cosmos pulsar® 3p, Germany), during which gas exchange was assessed using a breath-by-breath gas analyser (Ergocard, Medisoft, Belgium). The incremental running protocol was started at 11km/h for male and 10km/h for female participants. The intensity was increased by 1km/h every 2min, with a fixed slope of 1.5%. VO2max criteria were: 1) Plateau in VO2 despite increase in workload, 2) Respiratory exchange ratio (RER) ≥ 1.10, and 3) Maximal heart rate expected for age (220 bpm - age). Tests were terminated when two of these three criteria were met (Castro-Sepulveda et al., 2019).
Intervention
The participants attended the laboratory to perform an acute HIIT 5-7 days after the VO2peak test. They were instructed to refrain from any intense physical activity, dietary supplementation and pharmacological intake in the 48h prior to the intervention. Furthermore, they were not prohibited from consuming tobacco, alcohol and caffeine in the 12h prior to the HIIT session. A standardized diet with a high carbohydrate (125g) and protein content (21g) was provided for breakfast and lunch on the day of the intervention. The HIIT session was performed after two hours of fasting, between 3:00pm and 6:00pm, to minimize hormonal fluctuations. The session consisted of ten, 4-min running intervals at an intensity that elicited 90% of VO2peak, which corresponded to a speed of 15.9 ± 6.8 km/h for male and 14.6 ± 4.7 km/h for female participants. Each interval was separated by two min of rest. The protocol included a 3-min warm-up and a 3-min cool-down at 45% of VO2peak at an average speed of 7.1 ± 0.4km/h for male and 7.8 ± 0.4 km/h for female participants. During the rest periods, the participants were instructed to remain on the side of the treadmill and be prepared to resume exercise on the treadmill 30s before the next interval. Participants were supervised by the same examiner, who monitored their heart rate (HR) to ensure that the exercise was performed at the prescribed intensity. The coefficient of variation (CV) for the present study was 5.3% for HR. The rate of perceived exertion (RPE) was recorded after completing each interval. Participants were asked to rate their perceived exertion on a Borg 6-20 scale (Moreira et al., 2009). The CV for the present study was 20.9% for RPE. Blood lactate levels were assessed immediately after exercise, using a Lactate Pro 2 analyser (Arkray KDK, Japan) on a capillary blood sample and the CV for lactate levels was 52.6%.
Saliva collection
Saliva samples were collected 5 min before (PRE-) and 20 min after (POST-) exercise as detailed in (Peñailillo et al., 2015).
Saliva Analysis
Enzyme-linked immunosorbent assays (ELISA) were used to analyze cortisol, testosterone, sAA and IgA concentrations according to the manufacturer’s protocol (Salimetrics, USA). All the analyses were performed in duplicate. Furthermore, testosterone to cortisol ratio (T/C) was calculated. The CV for the present study was 2.1% for cortisol, 3.2% for testosterone, 3.2% for IgA and 5.5% for sAA.
Statistical Analysis
Data are presented as mean and standard deviation (mean ± SD) in the text and tables. Data for figures are presented as mean and standard error of the mean (mean ± SEM). To determine the distribution of the data a Shapiro-Wilk test was performed prior to statistical model selection. After confirming normality, a two-way repeated measures analysis of variance (ANOVA) was used for the assessment of time, gender and interaction (time x gender) on HR, RPE and lactate variables. When a significant interaction effect was found, a Fisher’s LSD test was used for pairwise comparisons. Paired sample t-tests were used to analyze differences between 5 min before (PRE-) and 20 min after (POST-) exercise values of IgA, sAA, cortisol, testosterone and T/C ratio values in males, females, and males and females combined. Statistical significance was set at 0.05. All statistical analysis was completed with SPSS 21.0 (SPSS Inc., Chicago, IL, USA).
Results
Heart rate, RPE and lactate levels
Figure 1A shows the changes in mean HR (as percentage of HRmax) during the active intervals. HR was on average 5.0 ± 0.0% higher in females than males (main gender effect; p = 0.008). HR increased gradually throughout the course of the HIIT session in both males and females (main time effect; p < 0.001). No interaction effect was found for HR during the intervals (time x gender: p = 0.97). HR during the recovery intervals increased gradually when progressing throughout the HIIT session in both males and females (main time effect: p < 0.001, Figure 1B). HR during recovery was similar between males and females (main gender effect: p = 0.68 and interaction effect: p = 0.25, Figure 1B). RPE increased with the repetition of intervals in both males (33 ± 10%) and females (16 ± 5%) (main time effect: p < 0.001). However, there was a difference in RPE scores between males and females over the time-course of the HIIT session (time x gender effect: p < 0.001, Figure 1C). Blood lactate levels at the end of the HIIT session were similar in male and female participants (5.9 ± 0.8mmol/L and 5.1 ± 1.0 mmol/L, respectively) as shown in Figure 1D.
Figure 1.
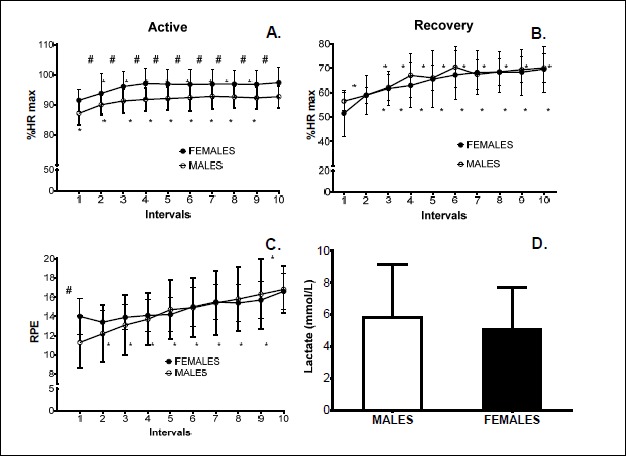
Heart rate during active intervals (A), heart rate during recovery intervals (B), RPE after completing each interval (C), post-exercise lactate levels (D). Values are expressed as means ± SEM (n=10 in each group). # p<0.05 between males and females, * p<0.05 compared to the first interval.
IgA and alpha-amylase levels
Resting sIgA levels of male and female participants were similar (p = 0.34). Likewise, a similar increase in sIgA levels was observed in both males (24 ± 6% p = 0.004, Figure 2A) and females (27 ± 3% p = 0.03, Figure 2B) after acute HIIT protocol compared to their respective 5 min pre-exercise values. An increase of 25 ± 4% across all participants in sIgA levels was observed after acute exercise (PRE: 138 ± 14ug/ml, POST: 184 ± 16ug/ml; p < 0.001, Figure 2C).
Figure 2.

Salivary IgA levels in males (A), females (B) and all participants(C). Salivary alpha-amylase in males (D), females (E) and all participants (F). 5 min before (PRE) and 20 min after (POST) exercise. Values are expressed as means ± SEM (n=10 in each group for A, B, D and E; n=20 in each group for C and F). *p<0.05, **p<0.01, ***p<0.001 between 5 min before and 20 min post-exercise.
Resting sAA levels were ~1.5 times higher in male than female participants (p = 0.02). sAA levels increased by 44 ± 22% in male (p = 0.036, Figure 2D) and by 71 ± 26% in female participants (p = 0.026, Figure 2E) compared to their respective 5 min pre-exercise values. Salivary alpha-amylase levels across all participants increased by 59 ± 17% 20 min after exercise (PRE: 117 ± 15U/ml, POST: 284 ± 61U/ml; p = 0.007, Figure 2F).
Cortisol and testosterone levels and T/C ratio
Resting salivary cortisol levels were similar in male and female participants (p = 0.18). Salivary cortisol levels increased by 48 ± 17% across all participants 20 min after acute exercise (p < 0.0001), with no differences observed between male and female participants (Table 2). Cortisol levels increased by 41 ± 24% in male (p = 0.015) and by 55 ± 24% in female participants (p = 0.005) when compared to the 5 min pre-exercise values. Resting salivary testosterone concentrations were ~ three times higher in males than females (p = 0.002). Testosterone was unchanged 20 min after HIIT in both males (p = 0.087) and females (p = 0.078). Resting T/C ratio was 32 ± 20% higher in males than females (p = 0.005).
Table 2.
5 min pre- and 20 min post- exercise salivary cortisol, testosterone levels and T/C ratio in males and females combined (all participants), and males and females individually. Data are means ± SD.
| All participants | Males | Females | ||
|---|---|---|---|---|
| Cortisol (nmol/L) | PRE | 9.7 ± 1.9 | 10.3 ± 1.7 | 9.0 ± 1.9 |
| POST | 18.6 ± 7.4 | 17.3 ± 6.9 | 19.9 ± 8.1 | |
| p-value | <0.001 | 0.002 | 0.005 | |
| Testosterone (nmol/L) | PRE | 3.2 ± 2.6 | 4.8 ± 2.6 | 1.6 ± 1.5 |
| POST | 3.4 ± 2.5 | 5.1 ± 2.3 | 1.6 ± 1.0 | |
| p-value | 0.60 | 0.14 | 0.52 | |
| T/C ratio | PRE | 0.31 ± 0.24 | 0.45 ± 0.23 | 0.17 ± 0.15 |
| POST | 0.23 ± 0.21 | 0.35 ± 0.23 | 0.11 ± 0.15 | |
| p-value | 0.25 | 0.09 | 0.22 | |
Discussion
The main findings of this study were that 20 min after completing a HIIT session, sIgA, alpha-amylase, and cortisol levels were increased to a similar extent in both males and females, whilst testosterone and the T/C ratio remained stable. This suggests that the physiological stress produced by this HIIT session does not reduce immune function. Moreover, the anabolic/catabolic balance was preserved 20 min after an acute HIIT session. Therefore, we reject our hypothesis that one session of HIIT results in a decreased immune response and favours catabolic processes in both males and females.
Our HIIT protocol elicited higher average HR values in the female than the male participants across the active intervals. This was probably due to a greater strain on the females’ cardiovascular system (Laurent et al., 2014). Like (Wheatley et al., 2014), we found higher %HRmax and %VO2peak in females than males when exercising at the same relative intensity. During the recovery intervals, the HR of both males and females gradually increased with the number of active intervals completed and tended to remain high relative to the first interval. Furthermore, females reported greater perceived exertion after the first active interval than males. However, after normalizing the RPE obtained with HRmax in each interval no difference between males and females was found (data not shown). This is in concordance with a previous study using relative physical units of work such as velocity (Robertson et al., 2000). Similarly, we found no difference in %HRmax in the recovery intervals between males and females. Previous studies have found no differences in resting heart rate between males and females (Ryan et al., 1994; Pavlik et al., 1999). However, we accept that not having assessed resting HR and resting lactate levels to be a limitation to our study.
Decreases in salivary IgA concentrations have been reported after both acute and chronic exercise, and in intermittent as well as continuous exercise. For instance, IgA concentrations were reduced by 30% after three Wingate tests (MacKinnon and Jenkins, 1993) and by ~50% immediately post-marathon race (Nieman et al., 2006). A 75% decrease in IgA has also been reported after a soccer match in elite male soccer players (Peñailillo et al., 2015). However, others have found sIgA levels to be unaffected after a maximal incremental intensity front crawl exercise in both males and females (Morgado et al., 2014) and after a cycling HIIT session in males (Walsh et al., 1999). Here, we found increased sIgA levels in response to a running HIIT session in both males and females after HIIT. This contrasted with previous results indicating that strenuous endurance exercise leads to reductions in IgA within 24 hours (Trochimiak and Hübner-Woźniak, 2012), a period known as the “open window” during which athletes are more susceptible to upper respiratory infections (Neville et al., 2006). Nonetheless, IgA levels and secretion rates have been found to be increased immediately after an incremental cycling test to exhaustion in male subjects (Allgrove et al., 2008). Similarly, IgA concentrations increased three-fold in males after cycling at 80% of VO2max to exhaustion (Blannin et al., 1998). Short high intensity exercise could result in increased sIgA due to sympathetic stimulation, which increases IgA mobilization into saliva (Allgrove et al., 2008). Furthermore, increased sympathetic nervous activity constricts the salivary glands (Li and Gleeson., 2005), which in conjunction with dehydration during exercise (Walsh et al., 2004), may affect the saliva flow rate (Perez-Luco et al., 2019) and stress hormone regulation, including cortisol (Castro-Sepulveda et al., 2018). Thus, we accept that not having -measuremed the saliva flow rate was a limitation of this study. Therefore, the increased sIgA levels found after completion of our HIIT protocol suggest that this HIIT protocol did not induce negatively impact immune function.
Similar to a previous study, the current study found greater baseline levels of sAA in males than females (Carr et al., 2016). This may reflect heightened tonic arousal in men or greater anticipatory anxiety related to the exercise session. Salivary alpha-amylase concentrations increased 20 min after the HIIT session in both males and females, reflecting the sympathetic response to the physical stress induced by this kind of exercise. Our findings are in contrast with a recent report by Kilian et al. (2016), in which a single bout of HIIT produced higher sAA concentrations than high volume endurance training, but failed to reach significance over time or between groups. The authors suggest that their protocol (4 x 4min intervals at 90-95% peak power output, separated by 3min rest) was not sufficient to increase sympathetic activity (Kilian et al., 2016). The acute concentration of sAA was found to be linearly correlated with both intensity and duration (Rosa et al., 2014). Thus, the duration of our protocol with more repetitions and shorter recovery times may explain the increase in sAA after HIIT. The increased sAA levels that have been recorded after elite swimming (Diaz et al., 2012) and taekwondo (Chiodo et al., 2011) championships, have been suggested to be due to both physical and physiological stress associated with competition (Diaz et al., 2012). As these strenuous events are very energy demanding, the sAA levels may be increased in order to accelerate the hydrolysis of starch to glucose and maltose (Kivlighan and Granger, 2006). Beyond this role in energy provision, sAA could modulate mucosal immunity, since it inhibits the adherence and growth of microbial agents (Papacosta and Nassis, 2011). In addition to the high IgA levels found in response to our HIIT protocol, the increments in sAA levels may enhance immunity and reduce the risk of acute infection. Thus, we suggest that our HIIT protocol may induce a protective rather than a negative immune response.
Cortisol play an important role in response to stress, in skeletal muscle recovery, and is involved in the activation of the hypothalamic-pituitary-adrenocortical axis (Hackney and Walz, 2013). Salivary cortisol levels have been reported to increase in relation to the intensity and duration of continuous endurance exercise in males (Jacks et al., 2002) as well as high intensity short duration endurance exercise in females (Consitt et al., 2002). Furthermore, increased cortisol levels have also been reported during competition, including after a triathlon race in middle-aged males (Hayes et al., 2015) and after a 10-mile race in females (Consitt et al., 2002). Our results are in line with these previous studies, as cortisol levels were increased in both males and females (Kraemer et al., 1999; Consitt et al., 2002). Given that cortisol is a well-recognized physiological stress marker, this indicates that the exercise protocol implemented in our study was sufficiently stressful.
Unexpectedly, salivary testosterone levels were unaffected by our HIIT protocol in both males and females. Previously, short bouts of intensive endurance exercise has been reported to increase plasma free testosterone levels in trained subjects (Hackney et al., 2012). As salivary levels have been shown to reflect plasma free testosterone (Gatti and De Palo, 2011), we hypothesized that salivary testosterone would increase after the HIIT session in the present study. However, similarly to cortisol, both the intensity and the duration of the stimulus affect the testosterone response (Consitt et al., 2002). Given that the duration of the exercise protocol in our study, i.e. 60min, was longer than that used by Hackney et al (2012), i.e.45min,, it is likely that the intensity of the intervals is more decisive in the regulation of testosterone levels. Indeed, the intensity of the active intervals corresponded to 100-110% of VO2peak for 90s vs. 90% for 4min in our study. Thus, the intensity of our protocol may not have been sufficient to modify salivary testosterone concentrations. Furthermore, the lower resting and exercise-induced testosterone levels that have been reported as a result of training (Consitt et al., 2002) may have dampened the testosterone response in our participants who were national level endurance athletes . Therefore, it is possible that either the intensity of the exercise or the training background of our participants, or both may have resulted in the testosterone levels being unaffected by the HIIT session.
The tendencies towards a reduced T/C ratio 20 min after exercise in both males and females was therefore mainly due to the increased cortisol concentrations. The acute effect on the T/C ratio following the HIIT session may have been influenced by the intensity, duration and the timing of measurement. In the present study, testosterone and cortisol levels were only assessed 20 min after completing the HIIT session. Hence, possible changes in the T/C ratio across time, driven either by cortisol or testosterone responses cannot be discarded.
Conclusion
This study is the first to examine the immune and endocrine responses in endurance athletes 20 min after a single bout of HIIT and to evaluate whether gender affects these responses. We found that both males and females have increased salivary IgA, alpha-amylase and cortisol levels, whilst testosterone and the T/C ratio remained unaffected 20 min after the HIIT session. Together, this suggests that the physiological stress produced by a HIIT session does not reduce immune function and maintains the anabolic/catabolic balance 20 min after exercise. These findings may be of practical importance to athletes with autoimmune disorders who could use this HIIT protocol to reduce the risk of developing a flare-up during training. However, further investigation is warranted to exclude a delayed response in the hours or days following HIIT.
Acknowledgements
This project was funded by the Chilean National Science and Technology Fund, FONDECYT N° 11150576. The authors would like to thank Prof. Martin Gibala (McMaster University) for his helpful suggestions and proofreading of the manuscript. The experiments comply with the current laws of the country in which they were performed. The authors have no conflict of interest to declare.
Biographies

Camila MONJE
Employment
Graduate student, Universidad Finis Terrae
Degree
M.Sc.
Research interests
Clinical exercise physiology
E-mail: cmonjes@uft.edu
Isabel RADA
Employment
Research Assistant, Universidad Finis Terrae
Degree
M.Sc. PhD Student
Research interests
Clinical exercise physiology
E-mail: isabel.rada92@gmail.com

Mauricio CASTRO-SEPULVEDA
Employment
Research Assistant. Universidad Finis Terrae
Degree
Ph.D. Student
Research interests
Skeletal muscle physiology
E-mail: mcastro@uft.cl

Luis PEÑAILILLO
Employment
Professor (Assistant) of exercise and sport science. Universidad Finis Terrae
Degree
Ph.D.
Research interests
Exercise physiology and resistance /strength training
E-mail: lpenaililllo@uft.cl
Louise DELDICQUE
Employment
Professor in exercise physiology. Université catholique de Louvain.
Degree
Ph.D.
Research interests
Endurance physiology and nutrition
E-mail: louise.deldicque@uft.cl

Hermann ZBINDEN-FONCEA
Employment
Professor (Associate) of exercise physiology and sport science. Universidad Finis Terrae
Degree
Ph.D.
Research interests
Exercise physiology, chronic diseases and exercise
E-mail: hzbinden@uft.cl
References
- Allgrove J. E., Gomes E., Hough J., Gleeson M. (2008) Effects of exercise intensity on salivary antimicrobial proteins and markers of stress in active men. Journal of Sports Sciences 26(6), 653-661. [DOI] [PubMed] [Google Scholar]
- Blannin A. K., Robson P. J., Walsh N. P., Clark A. M., Glennon L., Gleeson M. (1998) The effect of exercising to exhaustion at different intensities on saliva immunoglobulin A, protein and electrolyte secretion. International Journal of Sports Medicine 19(8), 547-552. [DOI] [PubMed] [Google Scholar]
- Carr A.R., Scully A., Webb M., Felmingham K.L. (2016) Gender differences in salivary alpha-amylase and attentional bias towards negative facial expressions following acute stress induction. Cognition and Emotion 30(2), 315-324. [DOI] [PubMed] [Google Scholar]
- Castro-Sepulveda M., Ramirez-Campillo R., Abad-Colil F., Monje C., Peñailillo L., Cancino J., Zbinden-Foncea H. (2018) Basal Mild Dehydration Increase Salivary Cortisol After a Friendly Match in Young Elite Soccer Players. Frontiers in Physiology 26(9),1347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castro-Sepulveda M., Cancino J., Fernández-Verdejo R., Pérez-Luco C., Jannas-Vela S., Ramirez-Campillo R., Del Coso J., Zbinden-Foncea H. (2019) Basal Serum Cortisol and Testosterone/Cortisol Ratio Are Related to Rate of Na+ Lost During Exercise in Elite Soccer Players. International Journal of Sport Nutrition and Exercise Metabolism 17, 1-6. [DOI] [PubMed] [Google Scholar]
- Chiodo S., Tessitore A., Cortis C., Cibelli G., Lupo C., Ammendolia A., De Rosas M., Capranica L. (2011) Stress-related hormonal and psychological changes to official youth Taekwondo competitions. Scandinavian Journal of Medicine and Science in Sports 21(1), 111-119. [DOI] [PubMed] [Google Scholar]
- Consitt L. A., Copeland J. L., Tremblay M. S. (2002) Endogenous anabolic hormone responses to endurance versus resistance exercise and training in women. Sports Medicine 32(1), 1-22. [DOI] [PubMed] [Google Scholar]
- Cumming D. C., Wall S. R., Galbraith M. A., Belcastro A. N. (1987) Reproductive hormone responses to resistance exercise. Medicine and Science in Sports and Exercise 19(3), 234-238. [PubMed] [Google Scholar]
- de Oliveira V. N., Bessa A., Lamounier R. P., de Santana M. G., de Mello M. T., Espindola F. S. (2010) Changes in the salivary biomarkers induced by an effort test. International Journal of Sports Medicine 31(6), 377-381. [DOI] [PubMed] [Google Scholar]
- Diaz M. M., Bocanegra O. L., Teixeira R. R., Soares S. S., Espindola F. S. (2012) Response of salivary markers of autonomic activity to elite competition. International Journal of Sports Medicine 33(9), 763-768. [DOI] [PubMed] [Google Scholar]
- Doan B. K., Newton R. U., Kraemer W. J., Kwon Y. H., Scheet T. P. (2007) Salivary cortisol, testosterone, and T/C ratio responses during a 36-hole golf competition. International Journal Sports Medicine 28(6), 470-479. [DOI] [PubMed] [Google Scholar]
- Enns D.L., Tiidus P.M. (2007) Estrogen influences satellite cell activation and proliferation following downhill running in rats. Journal of Applied Physiology (1985) 104(2):347-53. [DOI] [PubMed] [Google Scholar]
- Fahlman M.M., Engels H.J. (2005) Mucosal IgA and URTI in American college football players: a year longitudinal study. Medicine and Science in Sports and Exercise 37, 374-80. [DOI] [PubMed] [Google Scholar]
- Gatti R., De Palo E. F. (2011) An update: salivary hormones and physical exercise. Scandinavian Journal of Medicine and Science in Sports 21(2), 157-169. [DOI] [PubMed] [Google Scholar]
- Gibala M. J., Little J. P., Macdonald M. J., Hawley J. A. (2012) Physiological adaptations to low-volume, high-intensity interval training in health and disease. The Journal of Physiology 590(Pt 5), 1077-1084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibala M. J., Little J. P., van Essen M., Wilkin G. P., Burgomaster K. A., Safdar A., Raha S., Tarnopolsky M. A. (2006) Short-term sprint interval versus traditional endurance training: similar initial adaptations in human skeletal muscle and exercise performance. The journal of Physiology 575(Pt 3), 901-911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gleeson M., Lancaster G.I., Bishop N.C. (2001). Nutritional strategies to minimise exercise-induced immunosuppression in athletes. Canadian Journal of Applied Physiology 26(Suppl), S23-35. [DOI] [PubMed] [Google Scholar]
- Hackney A. C., Hosick K. P., Myer A., Rubin D. A., Battaglini C. L. (2012) Testosterone responses to intensive interval versus steady-state endurance exercise. Journal of Endocrinological Investigation 35(11), 947-950. [DOI] [PubMed] [Google Scholar]
- Hackney A.C., Walz E.A. (2013) Hormonal adaptation and the stress of exercise training: the role of glucocorticoids. Trends in Sport Science 20(4), 165-171 [PMC free article] [PubMed] [Google Scholar]
- Hayes L. D., Grace F. M., Baker J. S., Sculthorpe N. (2015) Exercise-induced responses in salivary testosterone, cortisol, and their ratios in men: a meta-analysis. Sports Medicine 45(5), 713-726. [DOI] [PubMed] [Google Scholar]
- Jacks D. E., Sowash J., Anning J., McGloughlin T., Andres F. (2002) Effect of exercise at three exercise intensities on salivary cortisol. The Journal of Strength and Conditioning Research 16(2), 286-289. [PubMed] [Google Scholar]
- Kakanis M. W., Peake J., Brenu E. W., Simmonds M., Gray B., Hooper S. L., Marshall-Gradisnik S. M. (2010) The open window of susceptibility to infection after acute exercise in healthy young male elite athletes. Exercise Immunology Review 16, 119-137. [PubMed] [Google Scholar]
- Kilian Y., Engel F., Wahl P., Achtzehn S., Sperlich B., Mester J. (2016) Markers of biological stress in response to a single session of high-intensity interval training and high-volume training in young athletes. European Journal of Applied Physiology 116(11-12), 2177-2186. [DOI] [PubMed] [Google Scholar]
- Kivlighan K. T., Granger D. A. (2006) Salivary alpha-amylase response to competition: relation to gender, previous experience, and attitudes. Psychoneuroendocrinology 31(6), 703-714. [DOI] [PubMed] [Google Scholar]
- Kraemer W.J., Fleck S.J., Maresh C.M., Ratamess N.A., Gordon S.E., Goetz K.L., Harman E.A., Frykman P.N., Volek J.S., Mazzetti S.A., Fry A.C., Marchitelli L.J., Patton JF. (1999) Acute hormonal responses to a single bout of heavy resistance exercise in trained power lifters and untrained men. Canadian Journal of Applied Physiology 24(6), 524-537. [DOI] [PubMed] [Google Scholar]
- Laurent C. M., Vervaecke L. S., Kutz M. R., Green J. M. (2014) Sex-specific responses to self-paced, high-intensity interval training with variable recovery periods. The Journal of Strength and Conditioning Research 28(4), 920-927. [DOI] [PubMed] [Google Scholar]
- Legaz Arrese A., Munguía Izquierdo D., Serveto Galindo J. R. (2006) Physiological measures associated with marathon running performance in high-level male and female homogeneous groups. International Journal of Sports Medicine 27(4), 289-295. [DOI] [PubMed] [Google Scholar]
- Li T. L., Gleeson M. (2005) The effects of carbohydrate supplementation during the second of two prolonged cycling bouts on immunoendocrine responses. European Journal of Applied Physiology 95(5-6), 391-399. [DOI] [PubMed] [Google Scholar]
- Little J. P., Gillen J. B., Percival M. E., Safdar A., Tarnopolsky M. A., Punthakee Z., Jung M.E., Gibala M. J. (2011) Low-volume high-intensity interval training reduces hyperglycemia and increases muscle mitochondrial capacity in patients with type 2 diabetes. Journal of Applied Physiology (1985) 111(6), 1554-1560. [DOI] [PubMed] [Google Scholar]
- MacKinnon L. T., Jenkins D. G. (1993) Decreased salivary immunoglobulins after intense interval exercise before and after training. Medicine and Science in Sports and Exercise 25(6), 678-683. [PubMed] [Google Scholar]
- Moreira A., Arsati F., de Oliveira Lima Arsati, Y. B., da Silva D. A., de Araújo V. C. (2009) Salivary cortisol in top-level professional soccer players. European Journal of Applied Physiology 106(1), 25-30. [DOI] [PubMed] [Google Scholar]
- Morgado J. P., Monteiro C. P., Matias C. N., Alves F., Pessoa P., Reis J., Martins F., Seixas T., Laires M. J. (2014) Sex-based effects on immune changes induced by a maximal incremental exercise test in well-trained swimmers. Journal of Sports Science and Medicine 13(3), 708-714. [PMC free article] [PubMed] [Google Scholar]
- Neville V. J., Molloy J., Brooks J. H., Speedy D. B., Atkinson G. (2006) Epidemiology of injuries and illnesses in America's Cup yacht racing. British Journal of Sports Medicine 40(4), 304-311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neville V., Gleeson M., Folland J.P. (2008) Salivary IgA as a risk factor for upper respiratory infection in elite professional athletes. Medicine and Science in Sports and Exercise 40, 1228-1236. [DOI] [PubMed] [Google Scholar]
- Nieman D. C., Henson D. A., Dumke C. L., Lind R. H., Shooter L. R., Gross S. J. (2006) Relationship between salivary IgA secretion and upper respiratory tract infection following a 160-km race. The Journal of Sports Medicine and Physical Fitness 46(1), 158-162. [PubMed] [Google Scholar]
- Nieman D.C., Henson D.A., Fagoaga O.R., Utter A.C., Vinci D.M., Davis J.M., Nehlsen-Cannarella S.L. (2002). Change in salivary IgA following a competitive marathon race. International Journal of Sports Medicine 23, 69-75. [DOI] [PubMed] [Google Scholar]
- Nindl B. C., Kraemer W. J., Gotshalk L. A., Marx J. O., Volek J. S., Bush F. A., Hakkinen K., Newton R.U., Fleck S. J. (2001) Testosterone responses after resistance exercise in women: influence of regional fat distribution. International Journal of Sport Nutrition and Exercise Metabolism 11(4), 451-465. [DOI] [PubMed] [Google Scholar]
- Papacosta E., Nassis G. P. (2011) Saliva as a tool for monitoring steroid, peptide and immune markers in sport and exercise science. Journal of Science and Medicine in Sport 14(5), 424-434. [DOI] [PubMed] [Google Scholar]
- Pavlik G., Olexó Z., Bánhegyi A., Sidó Z., Frenkl R. (1999) Gender differences in the echocardiographic characteristics of the athletic heart. Acta Physiologica Hungarica 86(3-4), 273-278. [PubMed] [Google Scholar]
- Pérez-Luco C., Díaz-Castro F., Jorquera C., Troncoso R., Zbinden-Foncea H., Johannsen N.M., Castro-Sepulveda M. (2019) Fluid Restriction Decreases Solid Food Consumption Post-Exercise. Nutrients 11(6), pii: E1209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perry C. G., Heigenhauser G. J., Bonen A., Spriet L. L. (2008) High-intensity aerobic interval training increases fat and carbohydrate metabolic capacities in human skeletal muscle. Applied Physiology Nutrition and Metabolism 33(6), 1112-1123. [DOI] [PubMed] [Google Scholar]
- Peñailillo L.E., Escanilla F.A., Jury E.R., Castro-Sepulveda M.A., Deldicque L., Zbinden-Foncea H.P. (2018). Differences in salivary hormones and perception of exertion in elite women and men volleyball players during tournament. Journal of Sports Medicine and Physical Fitness 58, 1688-1694. [DOI] [PubMed] [Google Scholar]
- Peñailillo L., Maya L., Niño G., Torres H., Zbinden-Foncea H. (2015) Salivary hormones and IgA in relation to physical performance in football. Journal of Sports Science 33(20), 2080-2087. [DOI] [PubMed] [Google Scholar]
- Pyne D.B., Gleeson M. (1998). Effects of intensive exercise training on immunity in athletes. International Journal of Sports Medicine 19(Suppl 3), S183-191; discussion S191-184. [DOI] [PubMed] [Google Scholar]
- Ryan S.M., Goldberger A.L., Pincus S.M., Mietus J., Lipsitz LA. (1994) Gender- and age-related differences in heart rate dynamics: are women more complex than men? Journal American College of Cardiology 24(7), 1700-1707. [DOI] [PubMed] [Google Scholar]
- Robertson R. J., Moyna N. M., Sward K. L., Millich N. B., Goss F. L., Thompson P. D. (2000) Gender comparison of RPE at absolute and relative physiological criteria. Medicine and Science in Sports and Exercise 32(12), 2120-2129. [DOI] [PubMed] [Google Scholar]
- Rohleder N., Nater U. M. (2009) Determinants of salivary alpha-amylase in humans and methodological considerations. Psychoneuroendocrinology 34(4), 469-485. [DOI] [PubMed] [Google Scholar]
- Rosa L., Teixeira A., Lira F., Tufik S., Mello M., Santos R. (2014) Moderate acute exercise (70% VO2 peak) induces TGF-β, α-amylase and IgA in saliva during recovery. Oral Diseases 20(2), 186-190. [DOI] [PubMed] [Google Scholar]
- Sari-Sarraf V., Reilly T., Doran D. A. (2006) Salivary IgA response to intermittent and continuous exercise. International Journal of Sports Medicine 27(11), 849-855. [DOI] [PubMed] [Google Scholar]
- Spence L., Brown W.J., Pyne D.B., Nissen M.D., Sloots T.P., McCormack J.G., Locke A.S., Fricker P.A. (2007). Incidence, etiology, and symptomatology of upper respiratory illness in elite athletes. Medicine and Science in Sports and Exercise 39, 577-586. [DOI] [PubMed] [Google Scholar]
- Tjønna A. E., Leinan I. M., Bartnes A. T., Jenssen B. M., Gibala M. J., Winett R. A., Wisløff U. (2013) Low- and high-volume of intensive endurance training significantly improves maximal oxygen uptake after 10-weeks of training in healthy men. Plos One 8(5), e65382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trochimiak T., Hübner-Woźniak E. (2012) Effect of exercise on the level of immunoglobulin a in saliva. Biology of Sport 29(4), 255-261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wahl P., Mathes S., Köhler K., Achtzehn S., Bloch W., Mester J. (2013) Acute metabolic, hormonal, and psychological responses to different endurance training protocols. Hormone and Metabolic Research 45(11), 827-833. [DOI] [PubMed] [Google Scholar]
- Walsh N. P., Blannin A. K., Clark A. M., Cook L., Robson P. J., Gleeson M. (1999) The effects of high-intensity intermittent exercise on saliva IgA, total protein and alpha-amylase. Journal of Sports Science 17(2), 129-134. [DOI] [PubMed] [Google Scholar]
- Walsh N. P., Laing S. J., Oliver S. J., Montague J. C., Walters R., Bilzon J. L. (2004) Saliva parameters as potential indices of hydration status during acute dehydration. Medicine and Science in Sports and Exercise 36(9), 1535-1542. [DOI] [PubMed] [Google Scholar]
- Wheatley C. M., Snyder E. M., Johnson B. D., Olson T. P. (2014) Sex differences in cardiovascular function during submaximal exercise in humans. SpringerPlus 3, 445. [DOI] [PMC free article] [PubMed] [Google Scholar]