

Abstract
This study examined disruptions in caregiving, as well as the association of these disruptions, with cognitive, behavioral, and social outcomes at age 12 in a sample of 136 Romanian children who were abandoned to institutions as infants and who experienced a range of subsequent types of care. Children were found to experience significantly more caregiving disruptions (CGD) earlier in life than later in childhood. More frequent CGD predicted increases in externalizing and internalizing behavior problems at age 12. Results are discussed in terms of the association between CGD and the long-term development of children who have experienced institutional rearing.
The importance of a stable and nurturing caregiving environment on child development has been well documented, as this type of environment allows for the development of secure, supportive relationships with primary caregivers and other significant adults (Cassidy, Kirsh, Scolton, & Parke, 1996). In addition, a stable family environment allows for continuity in peer relationships and networks as well as the school setting, thereby setting the stage for more optimal social and cognitive development. For children living in nonparental care arrangements, there is often great instability in the caregiving environment. This instability can include moves from placement to placement, including to a foster family or extended biological family, or reunification with the mother. Whether temporary or permanent, instability often brings with it many negative consequences to the child (see Harden, 2004, for a review). When a child changes caregiving placement, this not only involves changes in the caregiving environment but can also include termination of a caregiving relationship. It is therefore important to determine those factors that lead to caregiving disruptions (CGD), in order to decrease or eliminate the potential negative effects to a child’s development.
A consistent finding in the child maltreatment literature is that disruptions or changes in placements for children living in foster care correlate with negative outcomes, particularly in terms of increases in behavioral problems (Newton, Litrownik, & Landsverk, 2000; Rubin, O’Reilly, Luan, & Localio, 2007) and decreases in academic performance (Zima et al., 2000). Few studies, however, have collected data prospectively, have taken into account children’s behavior before placement in a new home, and been able to disentangle this early behavior from outcome behaviors of interest (Newton et al., 2000; Rubin, O’Reilly, Luan, & Localio, 2007). Researchers have also relied on information on CGD captured during a distinct period (e.g., Connell et al., 2006; James, Landsverk, & Slymen, 2004) as opposed to considering all disruptions occurring from birth or first entry into the care system.
In this study, we sought to examine the nature of CGD experienced by children who had been placed in institutional care early in life and subsequently experienced a range of care arrangements across childhood, sometimes including foster care or care by extended kin or reinstitutionalization after reunification with family. Data were collected on children’s CGD from infancy to age 12. We were interested in examining characteristics of the child that may influence the frequency of CGD, including physical, cognitive, and behavioral characteristics. We were also interested in examining the associations between these disruptions and outcomes across multiple domains of development. We expected particular characteristics of the child, including internalizing and externalizing behaviors, to lead to an increase in the number of CGD. Furthermore, we expected frequent CGD to have a negative impact on child outcomes across multiple domains, including cognitive, behavioral, and social.
Researchers have identified a variety of factors that influence the number of placement disruptions experienced by children (see Oosterman, Schuengel, Slot, Bullens, & Doreleijers, 2007, for a review), including those factors related to the child and the environment. Age and gender are two such factors, with older children found to experience more placement changes than younger children (Barber, Delfabbro, & Cooper, 2001; Chamberlain et al., 2006; Connell et al., 2006; Pardeck, 1984; Smith, Stormshak, Chamberlain, & Bridges-Whaley, 2001; Wulczyn, Kogan, & Harden, 2003). This is due, in part, to the increased frequency of behavioral problems seen in older children. Findings about the effects of gender, however, are mixed (Connell et al., 2006; Palmer, 1996; Smith et al., 2001). Emotional and behavior problems are consistently related to more frequent placement disruptions (Barber et al., 2001; Barth et al., 2007; James, 2004; Newton et al., 2000; Palmer, 1996; Pardeck, 1984). In this study, we sought to extend this work by examining factors that may predict disruptions for children who experienced a variety of caregiving arrangements, measured from birth to late childhood.
Researchers have also studied the impact of changes in care, finding associations with poor outcomes in multiple domains across childhood and adolescence (Newton et al., 2000; Pardeck, 1984). Children living in foster care often face a high degree of uncertainty as they sometimes move from foster family to foster family before being reunited with their biological family or being permanently adopted (Fisher & Kim, 2007). These changes can have a negative impact on early attachment relationships, often negating the positive effects of attachment security formed early on in development (Stovall & Dozier, 1998). Frequent placement changes also predict greater internalizing and externalizing behavior (Newton et al., 2000; Rubin et al., 2007), decreased academic performance (Zima et al., 2000) and more frequent use of mental health services (Rubin et al., 2004). In this study, we sought to extend previous work on CGD in order to determine whether children who had previously experienced institutional care also experienced negative outcomes as a consequence of multiple caregiving changes.
This study is part of a comprehensive, longitudinal examination of the development of children who experienced severe psychosocial deprivation in early infancy during care in large, impersonal institutional facilities. The aim of the larger study was to determine the effects of a foster care intervention across various domains of development. In order to do this, a foster care program was created in Bucharest, Romania, the community from which all participants were drawn. Infants and young children living in institutions were recruited, and half of them were assigned to live with foster families, while the remaining half continued to live as usual, within institutions. The study maintained a noninterference policy, in that although children were initially assigned to one of two groups at the outset of the study, they were free to change placements across the course of the study. Such changes included being adopted, being reunited with their biological family, and changing institutions or areas within an institution. In addition, once the children reached 54 months of age, the Romanian government created a foster care program of their own, and foster families who had been a part of the study were incorporated into this program. Therefore, it was possible for children to be transferred to different foster families after 54 months of age based on decisions made by the government.
By the time children in the study entered middle childhood, many had experienced multiple changes in caregiver and caregiving environment. This was due, in part, to the fact that many children were living in institutions not because they were orphaned but because their families had abandoned them. As they got older, many children reunited with their families, and in some cases, subsequently returned to institutional care. Others were moved to different institutions or placed in foster care. It became important to examine the nature of the CGD experienced by each child in our sample, including the timing, duration, and frequency. In addition, we wanted to examine potential predictors of CGD, including demographic characteristics and children’s behavioral issues. In this study, we define CGD as those moves from a caregiving environment (and thus a change in caregiver) that were intended to be permanent. Therefore, extended hospital stays or visits home to family members were not included in the disruptions variable. This definition is similar to that used by Wulczyn et al. (2003) in their examination of placement disruptions in multiple samples, including one of over 4,000 children placed in foster care before their first birthday. Definitions of placement instability and CGD vary widely across studies (Connell et al., 2006). We chose the current definition in order to provide a child-centered and conservative estimate of the association of disruptions with outcomes of interest at age 12. Guided by previous research, our hypotheses were as follows: (a) Children’s age would positively predict CGD, with older children (at age of placement into first foster care home [FCG]) experiencing more disruptions than younger children; (b) Children with higher ratings of behavioral issues would experience a greater number of disruptions. We made no predictions with respect to gender, given the fact that previous literature has found mixed results, nor cognitive abilities given the lack of existing previous literature for this predictor, as well as the unique nature of the institutionalized sample.
We were also interested in examining the relations between experiencing CGD across childhood, and behaviors and skills when children were 12 years of age. We expected multiple changes in caregiver and the caregiving environment to have a negative impact on children’s social and emotional development. Children who moved placements frequently may not have the opportunity to form an attachment relationship with a caregiver and reap the rewards of that supportive relationship. Children who did have such an opportunity but then later experienced disruptions may have suffered the consequences of loss of that important relationship. In both cases, the foundation of later social and emotional development, the attachment relationship, would be negatively impacted, thereby increasing the chances of increased internalizing and externalizing problems, as well as social skills deficits later on. Frequent changes in caregiver could have also meant changes in location, making it difficult for children in our sample to form friendships and become members of a peer group in any one setting. In turn, their chances to learn and practice social skills would have been limited or interrupted. These changes are likely accompanied by emotional stress associated with moving from one living situation to another, having to adapt to a new home, family, and school. Therefore, we expected that a greater number of CGD also would be significantly related to lower ratings of social competence and skills.
Finally, we expected frequent CGD to negatively affect cognitive skills in late childhood. Few studies have examined the impact of CGD on cognitive outcomes. Zima et al. (2000), for example, found academic skills delays to be related to placement in multiple foster homes, but their sample included a broad age range of children (6–12 years), making it difficult to understand the impact of CGD on different stages of cognitive development. Kira, Somers, Lewandowski, and Chiodo (2012) more recently examined IQ scores in relation to disruptions to attachment relationships in a sample of African American adolescents living in foster care. They found that frequent changes in caregiver was negatively related to working memory subscale scores on the Wechsler Intelligence Scale for Children, 4th ed. (WISC–IV). In this study, we expected that changes in caregiver may have also meant changes in schools and teachers for many children, and inconsistent school attendance, which are likely accompanied by increased stress, making it difficult for children to adapt to and focus in school. This reasoning is in line with research by Zorc et al. (2013) who found significant relations between placement instability and both school absenteeism and school changes. We therefore expected frequent CGD to be associated with compromised learning and cognitive development, manifesting as lower IQ scores at age 12.
Method
Participants
The participants included 136 children recruited from six major institutions in Bucharest, Romania in April of 2001 to participate in a longitudinal study examining the effects of foster care intervention. An initial sample of 187 children completed a battery of initial pediatric and neurological assessments, which resulted in 51 children being excluded based on medical reasons including genetic syndromes (including Down syndrome), microcephaly, obvious signs of Fetal alcohol syndrome, and other neurological, motor, and sensory abnormalities. The remaining sample of 136 children ranged in age from 5 to 31 months at the time of baseline assessment and had spent at least half of their lives in institutional care. Following baseline assessment, the 136 institutionalized children were randomly assigned to either the care as usual group (CAUG; continue living in their current institution) or were placed in a FCG as part of the intervention designed for the larger study. Sixty-eight children (33 males and 35 females) were randomly assigned to the CAUG, and 68 (34 males and 34 females) were randomly assigned to the FCG. In this study, the total institutionalized sample (CAUG + FCG), when considered as a whole, was labeled the everinstitutionalized group (EIG).
Measures
Demographic Information
Age in days at first placement into an institution (M = 78.97, SD = 122.75, range = 0–532) and, for children randomly assigned to foster care intervention, age in days at first placement into foster care (M = 697.22, SD = 218.46, range = 207–1,004).
Behavior Problems
Primary caregivers were asked to complete the Infant-Toddler Social and Emotional Assessment (ITSEA; Carter, Briggs-Gowan, Jones, & Little, 2003) when children were 30 months of age. The ITSEA assesses four domains of functioning related to social-emotional development, including internalizing behaviors and externalizing behaviors, and yields standardized scores which were used in the present analyses as both predictors of CGD as well as control variables in the prediction of outcomes at age 12. The ITSEA has been found to be a reliable and valid measure of infants’ and toddlers’ behavior problems (Briggs-Gowan & Carter, 1998). As reported by Carter and her colleagues (Briggs Gowan & Carter, 2007; Carter & Briggs-Gowan, 2006; Carter et al., 2003), the ITSEA subscales and domains have established acceptable internal consistency (Cronbach’s alphas from .59 to .90, MN = .75) as well as test–retest reliability (intraclass correlation coefficients = .69–.90).
The Diagnostic Interview Schedule for Children (4th ed.; DISC–IV, Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000), a diagnostic instrument that assesses 34 psychiatric diagnoses of children and adolescents, was administered to all caregivers by a trained interviewer. The DISC was administered in order to obtain scores for multiple behavior problems, including internalizing and externalizing behaviors, both of which were used as outcome variables at age 12 in the present analyses. Previous research has found the DISC to be a reliable and valid instrument for assessing common psychiatric disorder symptoms in children and adolescents (Schwab-Stone et al., 1993; Shaffer et al., 1993).
Social Relatedness
Primary caregivers were also asked to report on children’s interactions with others using the ITSEA (Carter et al., 2003) when children were 30 months of age. Responses to these items yielded a score for social relatedness that was used in the present analyses as both a predictor of CGD as well as a control variable in the prediction of social outcomes at age 12.
Friendship Quality
Children were asked to report on the level of friendship quality experienced in a current close friendship using the Friendship Quality Questionnaire (FQQ; Parker & Asher, 1993). The FQQ uses 40 items to assess six dimensions of friendship quality: validation and caring, conflict resolution, conflict and betrayal, help and guidance, companionship and recreation, and intimate exchange. All of the dimensions except conflict and betrayal were significantly and highly intercorrelated (all rs > .36, all ps > .001) and therefore were averaged to form an overall score of friendship quality for each participant to be used in the present analyses. The total friendship quality variable created for the purpose of this study yielded very good internal reliability (α = .91).
Peer Relations
Parents were asked to report on their children’s experiences interacting with peers at age 12 using the MacArthur Health and Behavior Questionnaire (HBQ; Boyce et al., 2002; Essex et al., 2002). The HBQ is a validated tool used to assess behavioral and emotional functioning of children ranging in age from 4 to 18 years old. The HBQ Global Peer Relations composite was used as an index of children’s social competence. The composite is created by averaging scores from two subscales: Peer Acceptance/Rejection (eight items) and Bullied (five items). The HBQ Global Peer Relations composite score yielded very good internal reliability (α = .93).
Social Skills
Teachers were asked to report on children’s social functioning at age 12 using the Social Skills subscale of the Social Skills Rating System (SSRS; Gresham & Elliot, 1990). The Social Skills subscale includes 40 items relating to the participants’ cooperation, assertion, self-control, and other positive social behaviors utilized in social situations. Previous research (Bracken, Keith, & Walker, 1998; Gresham & Elliot, 1990) has shown the SSRS to be a valid and reliable measures of social skills and behaviors. In this study, a composite score of Social Skills was created by averaging children’s scores across the relevant subscale items. The Social Skills composite score yielded good internal reliability (α = .89).
IQ
IQ was assessed when children were 42 months of age using the Bayley Scales of Infant Development (Bayley, 1993; see Nelson et al., 2007, for details of administration), and again at 12 years of age using the fourth version of the WISC–IV (Wechsler, 2003; see Almas, Degnan, Nelson, Zeanah, & Fox, 2016, for details of administration). The Bayley yields an overall score, labeled the developmental quotient (DQ), which was used in the present analyses. The WISC–IV includes 10 subtests to assess intellectual functioning across multiple domains, yielding composite scores for verbal comprehension, perceptual reasoning, working memory, and processing speed. In addition, a full-scale IQ scale is calculated based on the scores from the 10 subtests. Each of the four subscale composite scores as well as full-scale IQ scores was used in the present analyses. All of the IQ assessments were conducted by trained and reliable Romanian psychologists and supervised by clinicians in the United States.
CGD From Early Infancy to Age 12
Participants experienced a variety of caregiving and location changes from birth to 12 years of age. Caregivers and locations included: maternal centers, placement in an institution, hospitals, a new pavil ion or area within the same institution, a foster care family, reunification with biological parents, a biological family member, a member of extended kin, or a new family through adoption. For this study, information on children’s caregiving and location changes was collected from various sources including: (a) Records from the time of initial institutionalization; (b) Staff records maintained throughout the course of the study; and (c) Interviews with study personnel.
At the time of institutionalization, if the institutional caregivers and the representatives from the National Authority for Child Protection of Bucharest knew the birth parents of the child, the parents were questioned about any caregiving changes prior to institutionalization. If the child was abandoned with no way of contacting their biological families despite extensive attempts by the authorities and social workers in the sector, then information on caregiving and location changes prior to institutionalization could not be gathered. Typically, children in this circumstance were abandoned at birth; therefore, no information on their caregiving experiences were unknown.
After abandonment and during periods of institutionalization, the National Authority for Child Protection monitored all disruptions experienced by each child, including hospitalizations, visits with biological or extended family, pavilion changes, and changes between institutions. After randomization, Research Assistants monitored the children of the FCG placed in MacArthur foster care families in the system organized by the BEIP during the first 6 months of placement. A Representative of the BEIP communicated weekly with MacArthur foster parents to gather information about any changes in health, behavior, or disruptions. After the first 6 months, Research Assistants conducted monthly in-home visits where they collected similar information about the children’s status. These home visits continued until the child was 54 months of age. For children in the CAUG, Research Assistants communicated with the Directors of Institutions and Residential Apartments, as well as the Head of Placement Centers and other staff of the foster care department under the Child Protection branch of government, in order to gather information and track the children’s placements into various care arrangements.
After 54 months of age, the MacArthur foster families became employees of the National Authority for Child Protection and the MacArthur foster care program transitioned to Government Foster Care. To update information about children’s caregiving and location changes after 54 months, the Research Assistants of the BEIP would contact the National Authority for Child Protection or, with permission of National Authority for Child Protection, the foster parents directly. If a child were reintegrated with their biological family, Research Assistants contacted their primary caregivers in their biological family. If children were living in institutions, Research Assistants contacted a variety of individuals, including the caregivers in the institutions, the case manager for each child (social worker) or their psychologist.
If children in the CAUG were moved from an institution to government foster care, information about caregiving and location changes were also tracked by and obtained from the National Author ity for Child Protection for each sector. Research Assistants were able to contact the National Authority for Child Protection to ask for permission to contact the government foster parents of the child and, if permission were granted, the Research Assistants were able to obtain information during in-person interviews or over the phone with the government foster family about the disruptions the child experienced.
Coding of Disruptions in Caregiving. Each time a child experienced a change in caregiver, this change was coded into one of nine categories: (a) institution; (b) maternal center; (c) hospital; (d) MacArthur foster care; (e) Government foster care; (f) adopted; (g) family placement (unpaid, nonrelative family); (h) biological family; (i) biological extended family. The date of each change was also recorded. Using this information, a CGD variable was created. CGD were defined as any move from a caregiving placement that was originally intended to be permanent. Many of the children in our sample were not institutionalized because they were orphaned. The biological families of some of the children maintained contact with them if the children were in nonmaternal/biological family care. Frequent and reoccurring visits with biological family were not coded as CGD, and neither were hospital stays. The number of CGD for each child from birth to age 12 was summed to create a Total CGD variable for each child. CGD were further coded by length of time in each placement, resulting in three categories: 0–7 days, 7–30 days, and 30+ days. The frequency of disruptions occurring of varying durations was calculated by summing the total number from birth to age 12.
Results
Characteristics of CGD
Frequency of Disruptions
Children in the EIG experienced a minimum of 1 and a maximum of 9 CGD between birth and 12 years of age (M = 3.37, SD = 1.57). A summary of the frequency of disruptions can be found in Table 1. Children in the CAUG and FCG groups experienced a similar number of disruptions during this time period (CAUG M = 3.63, SD = 1.81; FCG M = 3.11, SD = 1.23; t = 1.96, ns).
Table 1.
Frequency of Caregiving Disruptions From Birth to 12 Years of Age
| Number of disruptions | FCG (n = 68) | CAUG (n = 68) | Total (n = 134) |
|---|---|---|---|
| n | n | n | |
| 1 | 3 | — | 3 |
| 2 | 19 | 23 | 42 |
| 3 | 25 | 18 | 43 |
| 4 | 11 | 10 | 21 |
| 5 | 3 | 6 | 9 |
| 6 | 5 | 5 | 10 |
| 7 | — | 3 | 3 |
| 8 | — | 1 | 1 |
| 9 | — | 2 | 2 |
| M (SD) | 3.11 (1.23) | 3.63 (1.81) | 3.37 (1.57) |
Note. FCG = foster care group; CAUG = care as usual group.
The number of disruptions experienced before and after the first assessment point of the study (when children were 30 months of age) was examined. For all children (EIG), the mean number of CGD experienced before 30 months of age (M = 2.01, SD = 0.87) was significantly higher than the mean number of disruptions experienced after (M = 1.36, SD = 1.36; t = 4.61, p < .001). The mean number of disruptions experienced before 30 months of age was significantly higher for children in the FCG than the CAUG, (FCG M = 2.24, SD = 0.79; CAUG M = 1.81, SD = 0.91, t = [C0]2.96, p = .004). The mean number of disruptions experienced after 30 months of age was significantly higher for children in the CAUG (M = 1.95, SD = 1.52) than children in the FCG (M = 0.89, SD = 1.12; t = 4.21, p < .001). A summary of the mean number of disruptions, by group, can be found in Table 2.
Table 2.
Descriptive Statistics for Frequency of CGD From Birth to 12 Years of Age
| Variable | FCG (n = 68) M (SD) |
CAUG (n = 68) M (SD) |
Total (n = 136) M (SD) |
|---|---|---|---|
| CGD Birth—12 years | 3.11 (1.23) | 3.63 (1.81) | 337 (1.57) |
| CGD Birth—30 months | 2.24 (0.79) | 1.81 (0.91) | 2.01 (0.87) |
| CGD 30 months—12 years | 0.89 (1.12) | 1.95 (1.52) | 1.36 (1.36) |
Note. FCG = foster care group; CAUG = care as usual group; CGD = caregiving disruptions.
The frequency of caregiving arrangements of varying durations (< 7 days, 7–30 days, and over 30 days) was also examined for the EIG. Children most often remained in a particular caregiving arrangement for over 30 days, compared to the other two duration categories. We also examined the differences in the frequency of disruptions of these three durations for the CAUG and FCG participants. There were no significant differences between the frequency of CGD across all three duration categories for children in the CAUG and FCG (< 7 days, t = 0.49, ns; between 7 and 30 days, t = 1.05, ns; over 30 days, t = 1.81, ns).
Type of Disrupted Placement
After random assignment was complete, the number of times children disrupted from five main categories of caregiving placements was calculated for the EIG as well as separately for the CAUG and FCG. These categories included institutional care, MacArthur foster care, government foster care, biological family care (including care by parents as well as relatives), and adopted family. These data show that children in the CAUG disrupted from institutional care more often than other types of care, and more often than children in the FCG. These data are summarized in Table 3.
Table 3.
Number of Caregiving Disruptions by Type of Placement From Birth to 12 Years of Age
| Type of placement | FCG (n = 68) n (%) |
CAUG (n = 68) n (%) |
Total (n = 136) n (%) |
|---|---|---|---|
| Institution | 50 (45) | 52 (53) | 102 (48) |
| MacArthur foster care | 27 (24) | — | — |
| Government foster care | 2 (2) | 10 (10) | 12 (6) |
| Family care | 31 (28) | 36 (36) | 67 (32) |
| Adoption | 1 (1) | 1 (1) | 2 (1) |
| Total | 111 (100) | 99 (100) | 210 (100) |
Note. FCG = foster care group; CAUG = care as usual group.
Visualization of CGD
Using the statistical package R (R Development Core Team, 2013), code was created to visually depict CGD experienced by each child from birth to age 12 (Tueller, 2013). Included in the graphs is the type of placement, the length of each placement, and the timing of each disruption (Figure 1). General trends in CGD are clearly depicted. The plot shows the initial caregiving location of all participants as with their immediate family or a health care facility where abandonment at birth occurred, before transitioning to institutional care. Over time, distinct variations in the CGD experienced in our sample are evident. Half of the children in our sample were randomly assigned to FCG at, on average, 23 months of age. Many of these children spent the majority of their time with these same families, although some disrupted and moved to new caregiving arrangements. The second figure (Figure 2) depicts the individual experiences of four children in our sample. This figure highlights the variability in the number of CGD experienced by children in our sample.
Figure 1.
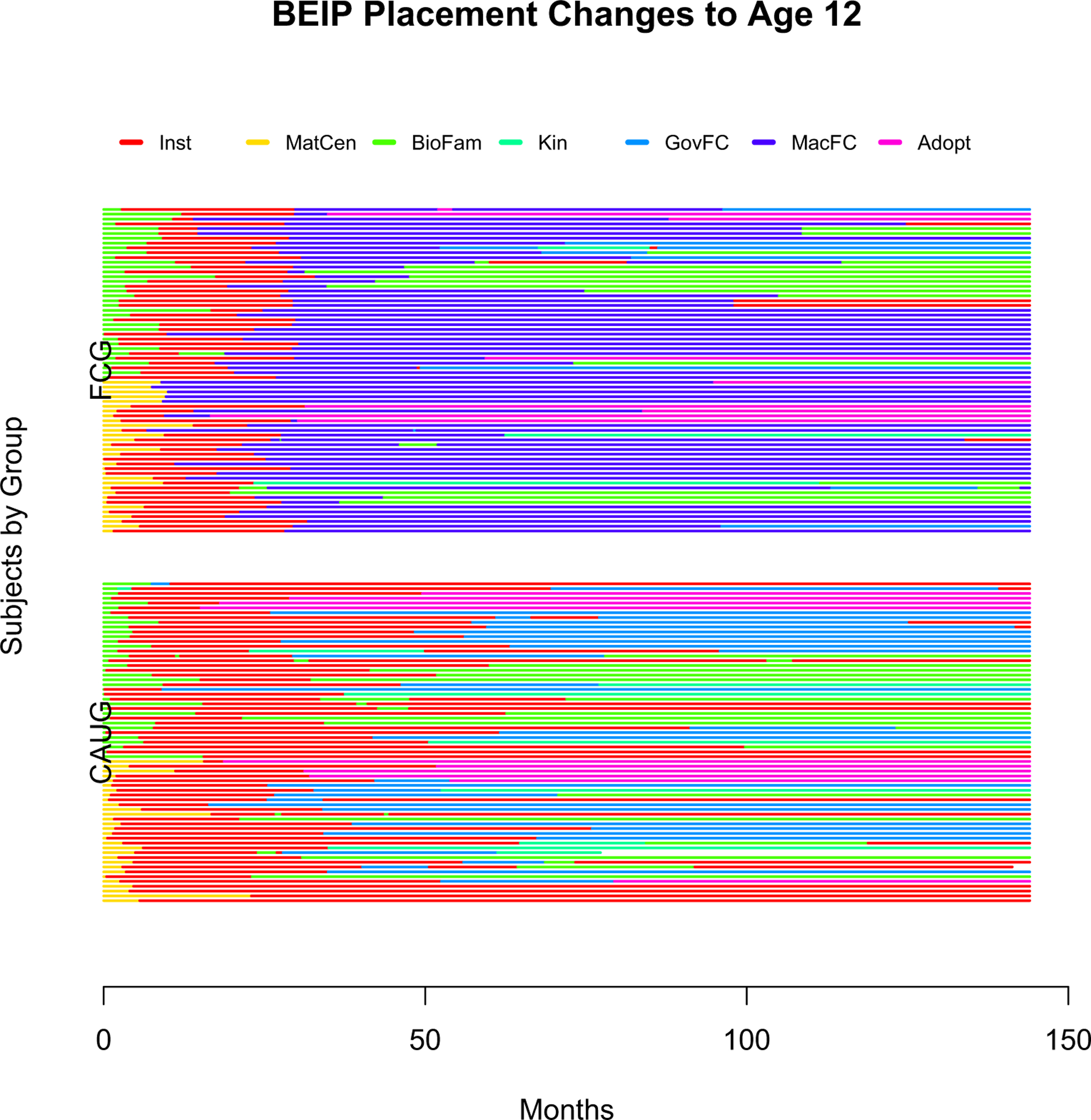
Line plots illustrating caregiving disruptions experienced by children from birth to 12 years of age, separated by randomization group.
Figure 2.
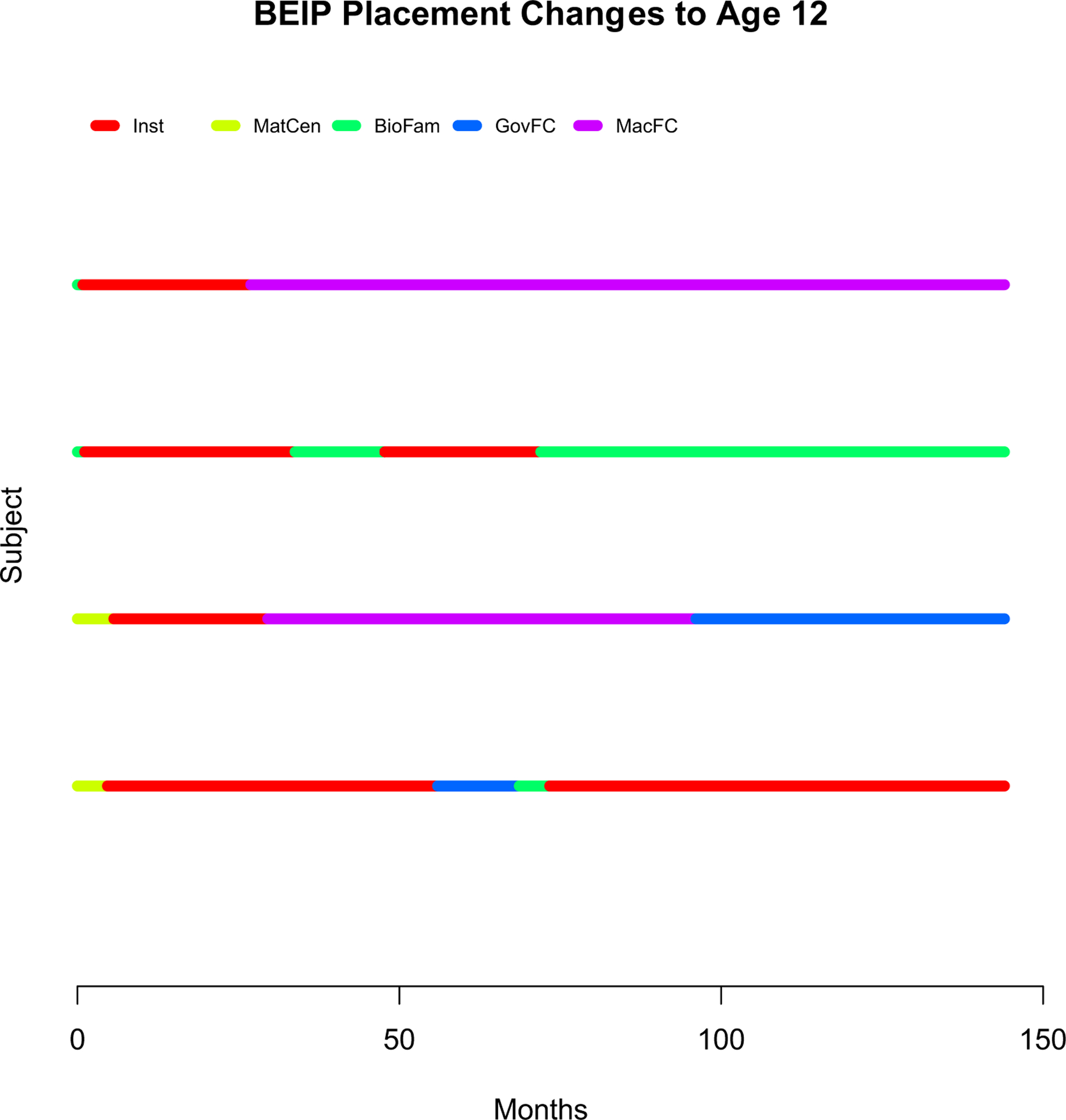
Line Plot illustrating caregiving disruptions experienced by four individual children from birth to 12 years of age.
Predictors of CGD
Demographic Variables
The total number of disruptions was compared for girls and boy using an independent samples t-test, which revealed no significant differences in the total number of disruptions experienced (t = −1.04, ns). Age at placement into institutional care did not significantly predict CGD. For those children who were randomly assigned to receive foster care intervention at the beginning of the study, older age at foster care placement significantly predicted more frequent CGD (r = .27, p = .03).
Behavior Problems
The correlations between caregiver-rated externalizing and internalizing behavior problems at 30 months of age and the number of CGD between 30 months and 12 years of age were examined. No significant relations emerged between either externalizing behavior (r = [C0].10, ns) or internalizing behavior (r = .13, ns) and CGD.
IQ
The correlation between DQ at 30 months of age and the number of CGD between 30 months and 12 years of age was examined. No significant relations emerged (r = −.03, ns).
Social Relatedness
The correlation between caregiver-rated social relatedness at 30 months of age and the number of CGD between 30 months and 12 years of age was examined. No significant relations emerged (r = −.08, ns).
Attachment Security
The correlation between attachment security at 42 months of age and the number of CGD between 42 months and 12 years of age was examined. No significant relations emerged (r = −.10, ns).
Relations Between CGD and Outcomes at Age 12
A series of linear regression analyses was conducted to examine the impact influence of CGD on outcome variables at 12 years of age. Bootstrapping regression models were used as a more robust method of analysis that would be less affected by the non-normal distributions of some of the variables. In all models, gender and group were entered first as covariates, followed by CGD from birth to 30 months as well as the relevant control variable at 30 or 42 months of age, followed by CGD as the predictor. Group and gender variables were only included in the final models if they were significant. A group (FCG or CAUG) by CGD interaction term was also included initially in all models, but did not emerge as a significant predictor in any model and therefore was not included in any final model. A gender by CGD interaction term was also included initially in all models, and was included in final models where significant. Results are presented with bias corrected and accelerated 95% confidence intervals (BCa 95% CI). Five thousand bootstrap samples were drawn for every regression model. Effect sizes (f2) are also reported for each regression model.
Cognitive Outcomes
A linear regression analysis was conducted to examine the influence of CGD on IQ at 12 years of age. DQ at 30 months of age was entered as the control variable, followed by CGD from 30 months to 12 years of age as the predictor. In the model predicting full-scale IQ, CGD predicted full-scale IQ at the trend level, over and above DQ, with more frequent CGD predicting lower scores at 12 years of age (R2 change = .03, b = −2.22, BCa 95% CI [−4.76, −0.04], t = [C0]1.85, p = .06, f2 = .11).
Behavioral Outcomes
Linear regression analyses were conducted to examine the influence of CGD on internalizing and externalizing behaviors at 12 years of age. In each model, the relevant ITSEA Subscale at 30 months of age (Internalizing or Externalizing) was entered as the control variable, followed by CGD from 30 months to 12 years of age as the predictor. In the model predicting internalizing behavior, CGD after 30 months emerged as a significant predictor, over and above internalizing behavior at 30 months, with more frequent disruptions predicting greater internalizing behavior at age 12 (R2 change = .05, b = 0.27, BCa 95% CI [0.05, 0.54], t = 2.35, p = .02, f2 = .07). In the model predicting externalizing behavior, externalizing behavior at 30 months of age significantly predicted higher scores at age 12 (R2 change = .10, b = 5.42, BCa 95% CI [1.48, 8.86], t = 3.34, p = .001, f2 = .11). CGD also emerged as a significant predictor, over and above externalizing behavior at 30 months, with more frequent disruptions predicting greater externalizing behavior at age 12 (R2 change = .06, b = 1.22, BCa 95% CI [0.43, 2.55], t = 2.62, p = .01, f2 = .19).
Social Outcomes
Linear regression analyses were conducted to examine the influence of CGD on social behaviors at 12 years of age. ITSEA Social Relatedness at 30 months was entered as the control variable, followed by CGD from 30 months to 12 years of age as the predictor. In the model predicting friendship quality (FQQ), only gender emerged as a significant predictor, with girls reporting higher quality friendships than boys (b = [C0]0.30, 95% BCa CI [− 0.56, − 0.03], t = −2.24, p = .03). In the model predicting parent-rated Global Peer Relations (HBQ) there were no significant predictors. In the model predicting teacher-rated Social Skills (SSRS) there were also no significant predictors.
Discussion
This study provides a systematic examination of the characteristics of CGD as well as the predictors and effects of these disruptions on children’s cognitive, behavioral, and social competence. It is, to our knowledge, the only study to examine disruptions across such a large time period (toddlerhood to late childhood). CGD are not experiences unique to institutionalized children, or those in the BEIP, but instead are experiences faced by many children within the foster care system and those who are separated from their biological families and living in alternative care.
Researchers have noted the variability in the categorization of caregiving changes or disruptions (James et al., 2004) in both the research literature as well as across welfare and government systems used to track this type of information. In this study, we considered only those changes to the caregiving environment that were intended to be permanent. We did so in part to use a more conservative estimate of the caregiving experiences of children in our sample when examining the potential effects of these on developmental outcomes. We also considered the fact that temporary moves or changes (e.g., an extended summer visit with a relative, a hospitalization) may be less detrimental to a child’s well-being than disruptions that were unexpected for the child. Other researchers have used strategies that include only considering moves starting at four or more, in order to avoid considering temporary moves in their analyses (e.g., Barth et al., 2007), but we felt that this type of approach may underestimate the effects of frequent CGD.
Our study is somewhat unique in that we were able to consider all disruptions experienced by the children in our sample from birth to age 12 (current assessment), as opposed to considering only those within a particular sampling period, as was done in many of the studies in this research area (e.g., Con nell et al., 2006; James et al., 2004). We found a broad range in the number of CGD experienced by children, ranging from 1 to 9, with about 66% of children in our sample experiencing three or more disruptions. We found that the majority of disruptions occurred during early childhood. When examining the length of placements, we found that children most often spent more than 30 days in any given placement. When compared to children in other samples, the present rates of disruption are somewhat higher, with the mean number of disruptions experienced by children in our sample being 3.37, while others report rates of < 1. Wulczyn et al. (2003), as one example, report an average of 0.697 moves per child in foster care in their sample of 14–18 year olds, with even lower rates for children who start off in group care settings. One likely reason for the high rates of disruption found in our sample may be the fact that the Romanian government began the process of creating a foster system during our study, closing down many institutions, and leading to changes in the care of many children. This is reflected in the higher rate of disruptions found after the first assessment point in our study (30 months of age) for children in the CAUG versus children in the FCG. This group difference may also reflect the stable nature of the foster families who children were assigned to as part of the study. Figures 1 and 2 provide a visual representation of the variability in number and length of disruptions experienced by children in our sample, as well as the timing of each disruption. These figures are similar to the Placement History Charts used by Kim, Pears, and Fisher (2012) to illustrate and summarize the placement changes experienced by children in the children in the American foster care system.
In this study, we found no relations between cognitive, behavioral, or attachment factors assessed during early childhood and the frequency of CGD, suggesting that these variables could not explain the number of disruptions. These results are consistent with those found by Holtan, Jandegard, Thornblad, and Vis (2013) in a sample of children in care in Norway. Our results, however, contrast those found with North American, British and Dutch samples where often researchers find lower IQ and both internalizing and externalizing behavior problems predict more frequent disruptions (James et al., 2004; Leathers, 2006; Strijker, Knorth, & KnotDickscheit, 2008; van Rooij, Maaskant, Weijers, Weijers, & Hermanns, 2015). It seems to be the case that, as least in the present context, characteristics of the children assessed early in life may not be the driving force behind the tendency to change care arrangements later on. Instead, one possibility is that characteristics of the system influence the stability of caregiving arrangements for these children. This idea is in line with the work of James (2004), who found that almost three quarters of placement changes for U.S. foster children were due to administrative or policy reasons, including lack of funding or closure of a foster home. In addition, James found that stressors or events occurring within the foster family, including house moves and family member deaths, precipitated placement disruptions. Similar factors may have influenced placement changes in the present sample. It is also possible that cognitive, behavioral or attachment factors assessed at later ages may evidence a stronger relation with CGD. In line with previous research on foster care (e.g., Connell et al., 2006), we found that older age of placement into a foster home (for children in the FCG) was a significant predictor of more frequent placement disruptions, while gender was not.
When examining the relations between CGD and children’s characteristics and behaviors at age 12, we found evidence of the negative influence of CGD on children’s behavior problems. When controlling for levels of internalizing and externalizing behavior when children were 30 months of age, experiencing a greater number of CGD over time significantly predicted both higher internalizing and higher externalizing symptoms at age 12. These results are consistent with those reported on North American samples showing evidence of increased behavioral problems, after controlling for initial levels of behavior, in children who experienced frequent CGD (Lewis, Dozier, Ackerman, & Sepulveda-Kozakowski, 2007; Rubin et al., 2007). Although the size of the effects we report are small, they are similar in size to those reported by others (e.g., Lewis et al., 2007). The present findings are important in part because few studies in this area have taken into account baseline child behavior problems when considering the influence of caregiving changes on later behavioral outcomes. Although Rubin et al. (2007) provide one exception, they examined the behavior of children during a short period (18 months) and the ages of children in their sample varied greatly (from infancy to adolescence). The present findings are the first, of our knowledge, to provide a more rigorous examination of behavioral outcomes in late childhood related to CGD.
We failed to find a significant relation between frequent CGD and IQ at age 12. This finding is inconsistent with previous research by Zima et al. (2000) who found a relation between the number of changes in foster homes and academic skills delays in their sample of U.S. children aged 6–12 years. It is possible that the instability resulting from frequent CGD may have a more negative impact on the development of learning skills and achievements specific to the school setting (e.g., repeating a grade, delays in math skills), as opposed to overall IQ scores. Each time a child changes placement, the disruption to their day-to-day lives, as well as the stress that likely accompanies the loss of a previous home and caregiver, and adaptation to a new home and caregiver and even school, likely impacts the child’s success at school in multiple ways. Further research is needed to understand how and in what way these negative effects occur.
We did not find evidence of relations between CGD and social outcomes however, across measures of friendship quality (self-report), global peer relations (parent report) and social skills (teacher report). Other researchers who have examined social competence and social skills (e.g., Zima et al., 2000) also have failed to find an association with multiple foster care placements. It is possible that frequent disruptions to the caregiving environment bring both positive and negative consequences within the social domain, in which case the positive and negative effects may cancel each other out. On the positive side, it is possible that changes in caregiver (and in some cases, caregiving family and even school) provide children with the opportunity to strengthen their social skills by learning to adapt to new people and social settings, provide more frequent opportunities to practice initiation and relationship-building skills, as well as more opportunities to receive feedback from which to learn and improve their skills. On the negative side, children who had to move to a new location as a consequence of a disruptions would likely experience strains on their friendships or even friendship termination, as well as loss of a stable peer group. These experiences might result in fewer intimate, supportive relationships, higher feelings of loneliness and stress, and fewer opportunities to practice more complex social skills. Further research is needed in order to examine these possible outcomes.
It is important to note some limitations of this study, including the fact that effect sizes were small and, due to the correlational nature of the design, conclusions about causality are limited. However, the inclusion of early levels of each variable of interest as control variables added strength to our conclusions around outcomes at age 12. Nonetheless, it is likely that other factors that we did not control for played a role in the development of the outcomes we assessed. Also important to note is the fact that we did not take into account whether each disruption in care led to a positive or negative change in the caregiving environment in our coding. In other words, because our design involved assessments at certain ages rather than following each disruption, we did not assess whether the change was to a better or worse caregiving environment than the previous care setting, nor did we assess the characteristics of the caregiver and his or her relationship with the child. We assumed that a disruption in care itself would be stressful and possibly a negative experience for a child, recognizing that some aspects of changes in caregiving arrangements could be positive (e.g., higher quality caregiver). However, it would be valuable for future studies to examine the nature of each placement context, including setting and caregiver, to determine the impact of caregiving changes on the child. It is possible that for some children, being reunited with their biological mother or family is a positive experience while, for others, it is not. Disruptions may result from a confluence of factors, which could include characteristics of the caregiver, the child, both or either of their previous experiences with care, or the setting. The examination of such detailed aspects of nonparental caregiving experiences, although valuable, is not available in our data. Nevertheless, this is a 10-year long examination of CGD in a very high-risk sample who experienced abandonment followed by deprivation. It also includes a careful examination of factors that preceded and followed the disruptions.
Overall, this study provides important insight into the negative effects of CGD on the development of children across multiple domains. We found that more frequent CGD significantly predicted behavior problems at age 12, after controlling for levels of behavior during early childhood. Because we found no evidence that the disruptions were driven by child characteristics, these results highlight the need for greater stability in the care system supporting previously institutionalized and currently institutionalized children in Romania and beyond. Indeed, the results underscore the importance of preventing the negative consequences that disruptions to the caregiver–child relationship and change in caregiving environment have on children’s behavioral and cognitive development.
Contributor Information
Alisa N. Almas, University of British Columbia
Margaret R. Woodbury, University of Maryland
Charles H. Zeanah, Tulane University School of Medicine
Leanna J. Papp, University of Michigan
Charles A. Nelson, Children’s Hospital Boston and Harvard Graduate School of Education and Harvard Center on the Developing Child
Nathan A. Fox, University of Maryland
References
- Almas AN, Degnan KA, Nelson CA, Zeanah C,& Fox NA (2016). IQ at age 12 following a history of institutional care: Findings from the Bucharest Early Intervention Project. Developmental Psychology, 52, 1858–1866. 10.1037/dev0000167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barber JG, Delfabbro PH, & Cooper LL (2001). The predictors of unsuccessful transition to foster care. Journal of Child Psychology and Psychiatry, 42, 785–790. 10.1111/1469-7610.00775 [DOI] [PubMed] [Google Scholar]
- Barth RP, Lloyd C, Green RL, James S, Leslie LK, & Landsverk J (2007). Predictors of placement moves among children with and without emotional and behavioral disorders. Journal of Emotional and Behavioral Disorders, 14, 46–55. 10.1177/10634266070150010501 [DOI] [Google Scholar]
- Bayley N (1993). Bayley Scales of Infant Development: Manual (2nd ed.). San Antonio, TX: Psychological Corporation. [Google Scholar]
- Boyce WT, Essex MJ, Goldstein LH, Armstrong JM, Kraemer HC, & Kupfer DJ (2002). The confluence of mental, physical, social, and academic difficulties in middle childhood. I: Exploring the “headwaters” of early life morbidities. Journal of the American Academy of Child & Adolescent Psychiatry, 41, 580–587. 10.1097/00004583-200205000-00016 [DOI] [PubMed] [Google Scholar]
- Bracken BA, Keith LK, & Walker KC (1998). Assessment of preschool behavior and social-emotional functioning: A review of thirteen third-party instruments. Journal of Psychoeducational Assessment, 16, 153–169. 10.1177/073428299801600204 [DOI] [Google Scholar]
- Briggs Gowan M, & Carter AS (2007). Applying the Infant-Toddler Social & Emotional Assessment (ITSEA) and Brief-ITSEA in early intervention. Infant Mental Health Journal, 28, 564–583. 10.1002/(ISSN)1097-0355 [DOI] [PubMed] [Google Scholar]
- Briggs-Gowan M, & Carter AS (1998). Preliminary acceptability and psychometrics of the Infant-Toddler Social and Emotional Assessment (ITSEA): A new adult-report questionnaire. Infant Mental Health Journal, 19, 422–445. [DOI] [Google Scholar]
- Carter AS, & Briggs-Gowan MJ (2006). Manual for the Infant-Toddler Social & Emotional Assessment (ITSEA)—Version 2. San Antonio, TX: Psychological Corporation, Harcourt Press. [Google Scholar]
- Carter AS, Briggs-Gowan MJ, Jones SM, & Little TD (2003). The Infant-Toddler Social and Emotional Assessment (ITSEA): Factor structure, reliability, and validity. Journal of Abnormal Child Psychology, 31, 495–514. 10.1023/A:1025449031360 [DOI] [PubMed] [Google Scholar]
- Cassidy J, Kirsh S, Scolton K, & Parke RD (1996). Attachment and representations of peer relationships. Developmental Psychology, 32, 892–904. 10.1037/0012-1649.32.5.892 [DOI] [Google Scholar]
- Chamberlain P, Price JM, Reid JB, Landsverk J, Fisher PA, & Stoolmiller M (2006). Who disrupts from placement in foster and kinship care? Child Abuse & Neglect, 30, 409–424. 10.1016/j.chiabu.2005.11.004 [DOI] [PubMed] [Google Scholar]
- Connell CM, Vanderploeg JJ, Flaspohler P, Katz KH, Saunders L, & Tebes JK (2006). Changes in placement among children in foster care: A longitudinal study of child and care influence. Social Service Review, 80, 398–418. 10.1086/505554 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Essex MJ, Boyce WT, Goldstein LH, Armstrong JM, Kraemer HC, & Kupfer DJ (2002). The confluence of mental, physical, social, and academic difficulties in middle childhood. II: Developing the MacArthur Health and Behavior Questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 41, 588–603. 10.1097/00004583-200205000-00017 [DOI] [PubMed] [Google Scholar]
- Fisher PA, & Kim HK (2007). Intervention effects on foster preschoolers’ attachment-related behaviors from a randomized trial. Prevention Science, 8, 161–170. 10.1007/s11121-007-0066-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gresham F, & Elliot S (1990). Social Skills Rating System manual. Minneapolis, MN: Pearson. [Google Scholar]
- Harden BJ (2004). Safety and stability for foster children: A developmental perspective. The Future of Children, 14, 30–47. 10.2307/1602753 [DOI] [PubMed] [Google Scholar]
- Holtan A, Jandegard BH, Thornblad R, & Vis SA(2013). Placement disruption in long-term kinship and nonkinship foster care. Children and Youth Services Review, 35, 1087–1094. 10.1016/j.childyouth.2013.04.022 [DOI] [Google Scholar]
- James S (2004). Why do foster care placements disrupt?An investigation of reasons for placement change in foster care. The Social Service Review, 78, 601–627. 10.1086/424546 [DOI] [Google Scholar]
- James S, Landsverk J, & Slymen DJ (2004). Placement movement in out-of-home care: Patterns and predictors. Children and Youth Services Review, 26, 185–206. 10.1016/j.childyouth.2004.01.008 [DOI] [Google Scholar]
- Kim HK, Pears KC, & Fisher PA (2012). The Placement History Chart: A tool for understanding the longitudinal pattern of foster children’s placement. Children and Youth Services, 34, 1459–1464. 10.1016/j.childyouth.2012.03.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kira IA, Somers C, Lewandowski L, & Chiodo L(2012). Attachment disruptions, IQ, and PTSD in African American adolescents: A traumatology perspective. Journal of Aggression, Maltreatment & Trauma, 21, 665–690. 10.1080/10926771.2012.698377 [DOI] [Google Scholar]
- Leathers SJ (2006). Placement disruption and negative placement outcomes among adolescents in long-term foster care: The role of behavior problems. Child Abuse & Neglect, 30, 307–324. 10.1016/j.chiabu.2005.09.003 [DOI] [PubMed] [Google Scholar]
- Lewis EE, Dozier M, Ackerman J, & Sepulveda-Kozakowski S (2007). The effect of placement instability on adopted chidlren’s inhibitory control abilities and oppositional behavior. Developmental Psychology, 43, 1415–1427. 10.1037/0012-1649.43.6.1415 [DOI] [PubMed] [Google Scholar]
- Nelson CA, Zeanah CH, Fox NA, Marshall PJ, Smyke AT, & Guthrie D (2007). Cognitive recovery in socially deprived young children: The Bucharest Early Intervention Project. Science, 318, 1937–1940. 10.1126/science.1143921 [DOI] [PubMed] [Google Scholar]
- Newton RR, Litrownik AJ, & Landsverk JA (2000). Children and youth in foster care: Disentangling the relationship between problem behaviors and number of placements. Child Abuse & Neglect, 24, 1363–1374. 10.1016/S0145-2134(00)00189-7 [DOI] [PubMed] [Google Scholar]
- Oosterman M, Schuengel C, Slot NW, Bullens RAR, & Doreleijers TAH (2007). Disruptions in foster care: A review and meta-analysis. Children and Youth Services Review, 29, 53–76. 10.1016/j.childyouth.2006.07.003 [DOI] [Google Scholar]
- Palmer SE (1996). Placement stability and inclusive practice in foster care: An empirical study. Children and Youth Services Review, 18, 589–601. 10.1016/0190-7409(96)00025-4 [DOI] [Google Scholar]
- Pardeck JT (1984). Multiple placement of children in foster family care: An empirical analysis. Social Work, 29, 506–509. 10.1093/sw/29.6.506 [DOI] [Google Scholar]
- Parker JG, & Asher SR (1993). Friendship quality in middle childhood: Links with peer group acceptance and feelings of loneliness and social dissatisfaction. Developmental Psychology, 29, 611–621. 10.1037/0012-1649.29.4.611 [DOI] [Google Scholar]
- R Development Core Team. (2013). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing. [Google Scholar]
- Rubin DM, Alessandrini EA, Feudtner C, Mandell DS, Localio AR, & Hadley T (2004). Placement stability and mental health costs for children in foster care. Pediatrics, 113, 1336–1341. 10.1542/peds.113.5.1336 [DOI] [PubMed] [Google Scholar]
- Rubin A, O’Reilly A, Luan X, & Localio A (2007). The impact of placement stability on behavioral well-being for children in foster care. Pediatrics, 119, 336–344. 10.1542/peds.2006-1995 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwab-Stone M, Fisher P, Piacentini J, Shaffer D, Davies M, & Briggs M (1993). The Diagnostic Interview Schedule for Children–Revised version (DISC–R):II. Test–retest reliability. Journal of the American Academy of Child & Adolescent Psychiatry, 32, 651–700. 10.1097/00004583-199305000-00024 [DOI] [PubMed] [Google Scholar]
- Shaffer D, Fisher P, Lucas CP, Dulcan MK, & Schwab-Stone ME (2000). NIMH Diagnostic Interview Schedule for Children, version IV (NIMH DISC–IV): Description, differences from previous versions, and reliability of some common diagnoses. Journal of the American Academy of Child & Adolescent Psychiatry, 39, 28–38. 10.1097/00004583-200001000-00014 [DOI] [PubMed] [Google Scholar]
- Shaffer D, Schwab-Stone M, Fisher P, Cohen P, Piacentini J, Davies M, … Regier D (1993). The Diagnostic Interview Schedule for Children–Revised version (DISC–R): I. Preparation, field testing, interrater reliability, and acceptability. Journal of the American Academy of Child & Adolescent Psychiatry, 32, 643–650. 10.1097/00004583-199305000-00023 [DOI] [PubMed] [Google Scholar]
- Smith DK, Stormshak E, Chamberlain P, & Bridges-Whaley R (2001). Placement disruption in treatment foster care. Journal of Emotional and Behavioral Disorders, 9, 200–205. 10.1177/106342660100900306 [DOI] [Google Scholar]
- Stovall KC, & Dozier M (1998). Infants in foster care: An attachment theory perspective. Adoption Quarterly, 2, 55–88. 10.1300/J145v02n01_05 [DOI] [Google Scholar]
- Strijker J, Knorth EJ, & Knot-Dickscheit J (2008). Placement history of foster children: A study of placement history and outcomes in long-term family foster care. Child Welfare, 87, 107–124. [PubMed] [Google Scholar]
- Tueller S (2013). longCatEDA: Package for plotting categorical longitudinal and time-series data (R package, version0.1). Retrieved from http://cran.rproject.org/web/packages/longCatEDA/index.html
- van Rooij F, Maaskant A, Weijers I, Weijers D, & Hermanns J (2015). Planned and unplanned terminations of foster care placements in the Netherlands: Relationships with characteristics of foster children and foster placements. Children and Youth Services Review, 53, 130–136. 10.1016/j.childyouth.2015.03.022 [DOI] [Google Scholar]
- Wechsler D (2003). WISC–IV technical and interpretive manual. San Antonio, TX: Psychological Corporation. [Google Scholar]
- Wulczyn F, Kogan J, & Harden BJ (2003). Placement stability and movement trajectories. Social Services Review, 77, 212–236. 10.1086/373906 [DOI] [Google Scholar]
- Zima BT, Bussin R, Freeman S, Yang X, Belin TR, & Forness SR (2000). Behavior problems, academic skills delays and school failure among school-aged children in foster care: Their relationship to placement characteristics. Journal of Child and Family Studies, 9, 87–103. 10.1023/A:1009415800475 [DOI] [Google Scholar]
- Zorc CS, O’Reilly ALR, Matone M, Long J, Watts CL, & Rubin D (2013). The relationship of placement experience to school absenteeism and changing schools in young, school-aged children in foster care. Child Youth Services Review, 35, 826–833. 10.1016/j.childyouth.2013.02.006 [DOI] [PMC free article] [PubMed] [Google Scholar]