

Abstract
Perna, FM, Coa, K, Troiano, RP, Lawman, HG, Wang, C-Y, Li, Y, Moser, RP, Ciccolo, JT, Comstock, BA, and Kraemer, WJ. Muscular grip strength estimates of the U.S. population from the National Health and Nutrition Examination Survey 2011–12. J Strength Cond Res 30(3): 867–874, 2016—The purposes of this study were to use the National Health and Nutrition Examination Study (2011–12) data to determine nationally representative combined handgrip strength ranges and percentile information by sex and age group, examine trends in strength across age by sex, and to determine the relative proportion of children and adults falling into established health benefit zones (HBZ). Results indicate that mean strength was greater among men than women and increased linearly for children and in a quadratic fashion among adults for both sexes. Grip strength peaked in the 30- to 39-year age group for both men (216.4 lbs) and women (136.5 lbs) with subsequent age groups showing gradual decline, p < 0.0001. Relative and absolute increases in grip strength were greater for men than for women, but relative decrease from peak strength was less among women than men. Although absolute strength was greater among men than women, HBZ data indicated that a higher percentage of men than women overall and at each age group fell into the needs improvement zone, with differences particularly pronounced during adolescence and older adulthood. These data provide the first nationally representative population estimates of combined handgrip strength and percentile information from childhood through senescence and suggest consideration of HBZ information in conjunction with grip strength to improve surveillance data interpretation and intervention planning.
Keywords: NHANES, fitness, youth, adults
Introduction
The Physical Activity Guidelines for Americans (2008) recommend adults to complete muscle strengthening activities 2 or more days a week in conjunction with general recommendations to obtain at least 150 min·wk−1 of moderate-intensity or 75 min·wk−1 of vigorous-intensity aerobic physical activity or an equivalent combination of moderate and vigorous aerobic activity (34). Similar guidelines exist for school-aged children (e.g., at least 60 min·d−1 aerobic activity with at least 3 days of vigorous activity and muscle and bone strengthening activity 3 d·wk−1). Indeed, recent studies with children and adults indicate the relative importance of muscular fitness, and its independence from aerobic fitness, to impart health benefits. Children’s muscular fitness is associated with overall health, bone health, and self-esteem and inversely associated with metabolic and cardiovascular disease biomarkers (31). Among older adults, benefits of musular fitness include lower relative risk of all-cause and cancer-specific mortality and lower relative risk of conditions that may underpin the association between muscular strength and all-cause mortality (13,23,28). For example, after controlling for body fat, central obesity, physical activity, and muscle mass, strength (as measured by handgrip dynamometer) was independently inversely associated with metabolic syndrome and accounted for 14% of population-attributable risk in adults 35–81 years old (1). Moreover, estimates suggest that modest increases in strength (approximately 17%) would result in a 14–24% decrease in metabolic syndrome. A large prospective cohort study reported similar relative risks between quadriceps and handgrip strength with all-cause mortality (23). These studies indicate that strength improvements may be important for public health and grip strength is a suitable and viable strength measure. Furthermore, the frequency and duration of exercise needed to attain and maintain adequate muscular strength are less than that required to achieve a similar degree of gain in aerobic fitness. Aerobic fitness and strength are also complementary in that improvements in muscular strength may also enhance aerobic fitness and performance, both of which may be beneficial for behavioral compliance (1,3,11).
Despite growing evidence of the benefits of attaining and maintaining adequate muscular strength, there has been no ongoing nationally representative assessment of muscular strength across age and sex in the United States. The 1999–2002 cycles of the National Health and Nutrition Examination Survey (NHANES) included lower-body (quadriceps) isokinetic strength (dynamometer) measurement, but assessment was limited to a subsample of older adults and has since been discontinued because of subject burden and cost (18,25). Handgrip dynamometer assessment was recently included in NHANES, and grip strength data are available in the 2011–12 data release.
Several publications have provided reference values for handgrip strength among healthy non-U.S. children and adults (2,6,24). Grip strength by body weight status among U.S. youth was recently reported, but findings were limited to mean values for boys and girls aged 6–15 years and did not provide percentile information for children (10). Recent data on changes in grip strength from fourth to fifth grades showed small increases for the girls but not for the boys from year to year (12). Normative grip strength estimates have also been reported for Canadian men and women across age groups, and additionally, grip strength cut points corresponding to health benefit zones (HBZs) have been established (4,5,33). Health benefit zones are intended to characterize the relative health and physical performance benefits and risks associated with an individuals’ sex- and age-specific grip strength. Information is lacking regarding the relative percentages of the U.S. population by age and sex falling into established HBZs (i.e., needs improvement to excellent) (4,5). Normative grip strength data across childhood and adulthood and estimates of the population by HBZ may be useful for physical education programming for youth and may inform physical activity intervention for both children and adults. The purposes of this study were to determine nationally representative estimates of combined handgrip strength by sex and age group, examine differences in strength across age and sex, and to determine the relative proportion of U.S. children and adults falling into established HBZs (4,5).
Methods
Experimental Approach to the Problem
The 2011–12 cycle of NHANES included a representative sample of the U.S. civilian noninstitutionalized population selected with a complex multistage probability design. To increase precision for population subgroups, respondents who were Hispanic, non-Hispanic black, non-Hispanic Asian, non-Hispanic white persons 80 years and older, and non-Hispanic white persons who were at or below 130% of the federal poverty level were oversampled. The survey design includes an in-person home interview and visit to a Mobile Examination Center (MEC). At the MEC, medical, physiological, and laboratory measures were collected. The National Center for Health Statistics Research Ethics Review Board approved the protocol, and informed consent (adults) or assent (children) was obtained for all participants. The overall survey response rate for the 2011–12 MEC sample was 69.5%. Additional NHANES design and protocol details are available elsewhere (7, http://wwwn.cdc.gov/nchs/nhanes/search/nhanes11_12).
Experimental Procedures
Grip Strength.
The NHANES Muscle Strength and Procedural Manual contains the complete grip strength testing protocol. Briefly, the Takei Digital Grip Strength Dynamometer, Model T.K.K.5401, was used for all assessments, and participants’ maximal contraction on each hand (over 3 trials separated by 60 seconds and alternating hands) was summed to yield the final combined handgrip strength value (kilograms converted to pounds). All personnel were trained in testing and calibration procedures, and a calibration log was maintained. The device handle was adjusted to accommodate participants’ hand size such that the index finger of each hand was at 90° flexion between proximal and middle phalangeal joint. A technician demonstrated proper form consisting of placing feet hip width apart and holding the dynamometer away from the body and in line with the forearm at thigh level so that it did not touch the body and the arm was fully extended and emphasized a quick and hard squeeze of the handle. The participant was then instructed in one practice trial, using submaximal effort, to ensure understanding of proper procedure. Before testing, participants were queried regarding physical limitations rendering them unable to complete the procedure with both hands in a standing position. Participants who could complete the test with only one hand or who needed to be seated were accommodated but excluded from these analyses.
Health Benefit Zones.
Five HBZs (needs improvement, fair, good, very good, and excellent) have been established that correspond to combined handgrip strength for men and women by age groups 15–69 years (4,5). Health benefit zones reflect the combination of quintiles derived from 1988 Campbell Survey on Well-Being in Canada and estimated benefit associated with achieving the specified grip strength relative to sex and age (4). Criteria underpinning specific HBZ cut points were not provided. Generally, increased health risks are reportedly associated with musculoskeletal strength in the “needs improvement” zone, both risks and benefits for scores in the “fair” zone, benefits in the “good” zone, and considerable and optimal benefits for grip strength in the “very good” and “excellent” zones, respectively. For example, grip strength <21 kg has been associated with an eightfold risk of developing muscular disability among older adults, and poor grip strength has been associated with adverse weight gain among women and mortality among men (4,17,20). Movement from the first 2 zones into the good zone is associated with the improvement in self-reported health status, such as increased mobility and unrestricted participation in occupational tasks, whereas movement to the latter 2 zones is associated with recreation and sport participation (4,5). Historical information related to Canadian population grip strength estimates and HBZ can be found at www.statcan.gc.ca.
Statistical Analyses
Data from participants aged 6 years and older as of the testing date were grouped as follows (6–8, 9–11, 12–15, 16–19 years and beginning at 20 years in 10-year age bands through 69 years and 70+ years thereafter). Participants were included in the analyses if they completed testing with both hands in the appropriate standing position and met all other strength testing inclusion criteria (n = 3,497 men, n = 3,400 women). Preliminary analyses determined that there were no significant demographic differences between participants included and those excluded for taking the test with one hand (n = 111) or not completing testing for some other reason (n = 644), (p = 0.8 for men and 0.11 for women). For both men and women, individuals aged 70 years and older were more likely to be excluded from analysis because of completing testing in seated position (n = 172, p < 0.01).
For men and women by age group, cutoffs for grip strength quintiles were calculated with standard error estimates and the resulting distributions were examined for skewness and kurtosis and deemed to have no significant departures from normality. Similarly, the resulting population quintile estimates and coefficient of variation (CV) for each age and sex grouping were examined and deemed stable (i.e., CV < 30%). Because strength may vary greatly at younger ages as children grow and develop, the nonparametric double-kernel method of Li et al. (19) was used to generate smoothed percentile curves of grip strength by single years for boys and girls aged 6–19 years. By incorporating survey weights in the curve estimation and the bandwidth selections, this approach is a modification of the method described by Yu et al. (35) and is applicable to population survey data, such as NHANES. In the curve estimation, grip strength is smoothed separately along the age axis and also the grip strength axis using kernel smoothing and local linear weighting in the age axis direction. During bandwidth selections, a bandwidth for the conditional mean is selected first and then modified to obtain the automatic bandwidths for the age axis according to the percentiles being estimated. A median correction is conducted to reduce smoothing bias and a bandwidth rescaling procedure to make the bandwidth selection scale invariant (19,35). QuntlSmoother (26) was applied to generate the smoothed percentiles. This statistical software package in language R estimates percentile smoothers for bivariate data with varying sample weights using the double-kernel method with median correction.
Regression with linear and quadratic terms was used to test for strength differences by age group and sex and to test for their interaction. Participants were also classified into 5 previously established HBZs by age and sex (4,5). Because distinguishing people in the needs improvement zone is particularly important (33), logistic regression tested for relative differences in percentages of participants within the needs improvement category in comparison with the other categories by age group, sex, and their interaction. Given that HBZs have only been established for people aged 15–69 years, health zone analyses were restricted to these age groups. All analyses were conducted with SAS callable SUDAAN and incorporated the sample weights. Standard errors were estimated with Taylor series linearization to incorporate the sample design.
Results
As can be seen in Table 1 and Figures 1A, B, mean strength was greater among men than in women, increased in a quadratic fashion for both (p < 0.0001 for both), and peaked in the 30- to 39-year age group in both men (216.4 lbs) and women (136.5 lbs) with subsequent age groups showing gradual decline (p < 0.0001). Relative decline in grip strength after peak was initially slightly steeper among men than in women aged 40–49 years, p ≤ 0.05, but became comparable after 50 years and older. Mean strength was 2.6, 9.6, 14.8, and 30.4% less for women aged 40–49, 50–59, 60– 69, and 70+ years, respectively, as compared with women aged 30–39 years (all comparisons significant at p ≤ 0.05). Among men, strength was 4.5, 10.3, 16.0, and 28.9% less for ages 40–49, 50–59, 60–69, and 70+ years, respectively, compared with men aged 30–39 years (all comparisons significant at p ≤ 0.05).
Table 1.
Mean, standard error (SE), and percentile distribution of grip strength (pound) in U.S. children and adults by sex and age group, 2011–12.*
| Sex | Age group (y) | n | Mean (SE) | 20th (SE) | 40th (SE) | 50th (SE) | 60th (SE) | 80th (SE) |
|---|---|---|---|---|---|---|---|---|
| Males | 6–8 | 332 | 55.1 (1.1) | 43.9 (0.8) | 49.2 (1.4) | 53.2 (1.4) | 56.41 (1.7) | 67.6 (1.6) |
| 9–11 | 282 | 82.3 (1.3) | 65.8 (1.8) | 76.8 (1.5) | 81.0 (1.3) | 84.0 (1.2) | 95.3 (2.5) | |
| 12–15 | 303 | 138.2 (3.6) | 99.2 (3.4) | 124.2 (6.1) | 138.9 (5.0) | 147.1 (3.9) | 170.9 (3.6) | |
| 16–19 | 290 | 187.7 (3.0) | 163.9 (3.5) | 180.3 (3.4) | 187.9 (3.3) | 194.3 (3.2) | 209.7 (2.4) | |
| 20–29 | 454 | 210.2 (2.7) | 178.2 (4.1) | 200.4 (3.1) | 208.1 (2.4) | 218.0 (3.9) | 241.4 (3.9) | |
| 30–39 | 411 | 216.4 (1.8) | 184.7 (2.5) | 209.5 (2.1) | 216.1 (1.8) | 224.6 (3.0) | 245.3 (3.1) | |
| 40–49 | 378 | 206.7 (2.7) | 180.0 (2.5) | 198.2 (3.1) | 207.6 (2.9) | 212.4 (3.1) | 234.4 (3.3) | |
| 50–59 | 372 | 194.0 (4.2) | 161.9 (5.9) | 188.1 (3.7) | 195.0 (3.5) | 203.3 (3.6) | 220.2 (4.7) | |
| 60–69 | 373 | 181.7 (4.2) | 152.2 (5.6) | 176.5 (5.1) | 184.9 (3.6) | 191.6 (2.8) | 206.0 (5.2) | |
| 70 and above | 302 | 153.9 (1.8) | 128.7 (3.4) | 146.0 (2.7) | 155.5 (2.2) | 162.1 (2.8) | 178.1 (2.8) | |
| Females | 6–8 | 281 | 50.4 (0.9) | 39.9 (1.0) | 45.6 (1.0) | 48.6 (1.1) | 51.4 (0.9) | 59.7 (1.4) |
| 9–11 | 301 | 78.2 (1.2) | 61.9 (1.4) | 71.5 (1.6) | 75.8 (1.1) | 81.0 (1.5) | 93.9 (2.0) | |
| 12–15 | 292 | 112.2 (1.8) | 95.7 (1.4) | 105.1 (2.1) | 109.3 (1.7) | 114.2 (2.9) | 128.5 (3.1) | |
| 16–19 | 285 | 124.7 (2.2) | 107.8 (2.5) | 117.5 (2.4) | 122.5 (2.2) | 126.6 (2.3) | 141.7 (4.9) | |
| 20–29 | 412 | 131.8 (1.1) | 112.7 (1.2) | 125.9 (1.3) | 130.3 (1.2) | 135.8 (1.1) | 148.4 (1.1) | |
| 30–39 | 382 | 136.5 (1.4) | 117.9 (1.5) | 128.8 (2.1) | 135.8 (1.7) | 139.6 (1.5) | 154.2 (1.9) | |
| 40–49 | 392 | 132.9 (1.4) | 114.5 (2.2) | 125.2 (1.8) | 132.9 (1.5) | 138.1 (2.0) | 154.1 (2.6) | |
| 50–59 | 401 | 123.4 (1.5) | 106.9 (2.0) | 117.7 (1.8) | 121.5 (2.0) | 128.0 (2.4) | 141.7 (2.2) | |
| 60–69 | 354 | 116.3 (1.3) | 100.3 (2.6) | 114.0 (1.8) | 117.1 (1.3) | 119.7 (1.5) | 131.2 (1.9) | |
| 70 and above | 300 | 95.0 (1.4) | 76.7 (1.8) | 88.4 (1.7) | 93.0 (1.9) | 100.2 (2.4) | 113.7 (1.5) |
Maximal contraction on each hand (over 3 trials each) was summed to yield combined grip strength (pound) used to identify the age- and sex-appropriate quintile and median. Source: National Health and Nutrition Examination Survey.
Figure 1.

Quartile distribution of grip strength (pound) in men (A) and women (B) by age.
Among children 6–19 years old, mean grip strength was greater among boys than in girls (p < 0.0001). Although mean grip strengths of both boys and girls were significantly higher at progressive age groups, the rate of increase with age was significantly greater among boys (p < 0.0001, Table 1 and Figures 1A, B). Mean strength among 16- to 19-year-old boys was over 240% greater than that of 6- to 8-year-old boys, and peak strength was attained in men aged 30–39 years and was over 292% greater than the grip strength of boys aged 6–8 years. In contrast, among girls, mean strength of 16- to 19-year-old girls was over 147% greater than girls aged 6–8 years, with peak strength attained in women aged 30–39 years being 171% greater than grip strength of girls aged 6–8 years. Single-year grip strength percentile estimates have utility for physical education purposes among children. Because physical maturation is more variable across chronological age in childhood than in adulthood and data smoothing captures important data patterns while minimizing error from single data points in smaller sample sizes, smoothed quartile estimates are provided in Table 2 (see Figures 2 and 3 for single-year smoothed curves).
Table 2.
Mean grip strength and smoothed quartile distribution (pound) in U.S. children by sex and single-year age, 2011–12.*
| Gender | Age | n | Mean | SEM | 25th percentile | 50th percentile | 75th percentile |
|---|---|---|---|---|---|---|---|
| Males | 6 | 107 | 46.9 | 1.1 | 38.6 | 44.6 | 51.5 |
| 7 | 111 | 54.9 | 1.7 | 42.5 | 50.2 | 58.9 | |
| 8 | 114 | 62.2 | 1.6 | 48.6 | 57.9 | 67.9 | |
| 9 | 102 | 71.6 | 1.5 | 57.5 | 67.6 | 78.1 | |
| 10 | 94 | 82.6 | 2.0 | 66.3 | 76.6 | 88.3 | |
| 11 | 86 | 93.9 | 2.8 | 75.9 | 86.7 | 100.7 | |
| 12 | 64 | 104.2 | 3.6 | 85.2 | 97.7 | 114.4 | |
| 13 | 88 | 130.5 | 4.3 | 96.7 | 113.2 | 133.2 | |
| 14 | 82 | 151.4 | 5.0 | 123.5 | 143.5 | 165.8 | |
| 15 | 69 | 166.8 | 3.8 | 138.8 | 159.5 | 181.9 | |
| 16 | 82 | 182.2 | 4.8 | 153.6 | 175.0 | 196.6 | |
| 17 | 67 | 182.8 | 2.7 | 164.5 | 183.9 | 203.9 | |
| 18 | 60 | 194.0 | 3.4 | 169.9 | 186.5 | 206.0 | |
| 19 | 81 | 191.0 | 4.4 | 170.1 | 187.4 | 207.5 | |
| Females | 6 | 95 | 44.1 | 0.8 | 34.8 | 40.7 | 46.2 |
| 7 | 95 | 47.9 | 1.4 | 38.9 | 45.3 | 51.8 | |
| 8 | 91 | 58.5 | 1.5 | 46.1 | 52.8 | 59.8 | |
| 9 | 105 | 64.7 | 0.9 | 54.3 | 61.3 | 68.4 | |
| 10 | 83 | 78.6 | 2.3 | 62.7 | 70.9 | 79.1 | |
| 11 | 113 | 90.7 | 1.5 | 73.5 | 83.4 | 94.1 | |
| 12 | 78 | 107.7 | 3.3 | 84.9 | 96.2 | 110.0 | |
| 13 | 84 | 106.0 | 3.1 | 92.6 | 104.0 | 117.6 | |
| 14 | 65 | 117.3 | 3.6 | 97.1 | 108.4 | 121.2 | |
| 15 | 65 | 119.1 | 2.8 | 102.2 | 113. | 126.6 | |
| 16 | 81 | 115.9 | 2.5 | 106.9 | 118.5 | 129.8 | |
| 17 | 70 | 128.4 | 4.0 | 108.4 | 121.1 | 133.6 | |
| 18 | 55 | 121.9 | 2.6 | 109.0 | 123.0 | 140.3 | |
| 19 | 79 | 132.9 | 3.2 | 114.4 | 126.3 | 142.7 |
Values (pound) represent the maximal grip strength achieved for each hand over 3 trials, combined for the left and right hand. Source: National Health and Nutrition Examination Survey. Smoothed quartile estimates are provided rather than quintiles because of sample size. Standard errors cannot be calculated for smoothed quartile estimates.
Figure 2.
Smoothed grip strength estimates of boys by age, 2011–12.
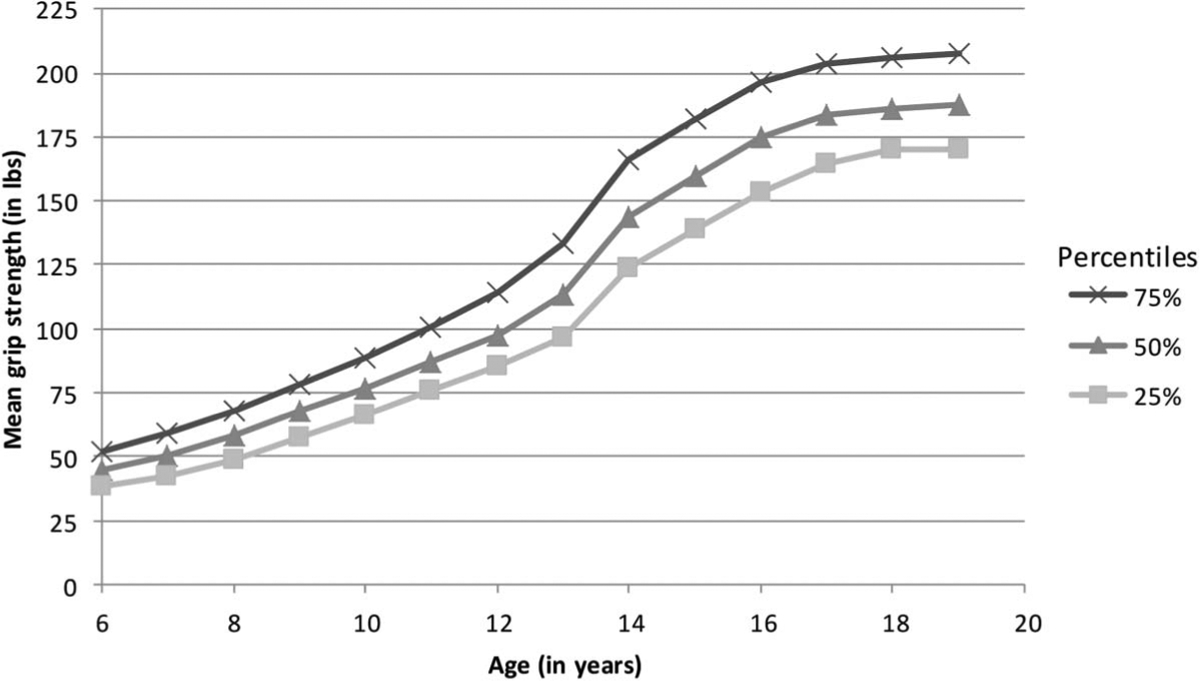
Figure 3.

Smoothed grip strength estimates of girls by age 2011–12.
Health Benefit Zones
For youth aged 15–19 years, significantly more boys (37.2%) than girls (20.3%) were in the needs improvement category and more girls (12.1%) than boys (5.3%) were in the excellent category, p < 0.002 (Figure 4). Overall, among adults aged 20–69 years, significantly more men (21.7%) than women (14.3%) were in the needs improvement category, p < 0.003. Compared with women of similar age, men aged 30–39 years (odds ratio [OR] = 1.66, 95% confidence interval [CI] = 1.10–2.50), 50–59 years (OR = 2.26, 95% CI = 1.05–4.86), and 60–69 years (OR = 3.78, 95% CI = 2.31–6.19) had significantly higher odds of being in the needs improvement category. Within sex, the odds of women being classified in the needs improvement category was significantly lower among women aged 30–39 years (OR = 0.56, 95% CI = 0.35–0.89), 40–49 years (OR = 0.60, 95% CI = 0.37–0.95), 50–59 years (OR = 0.46, 95% CI = 0.22–0.95), and 60–69 years (OR = 0.32, 95% CI = 0.18–0.56) compared with 20- to 29-year-old women. Among men, the odds of being classified in the needs improvement category was significantly lower among men aged 40–49 years compared with 20- to 29-year-old men (OR = 0.56, 95% CI = 0.34–0.91).
Figure 4.

Percentage of U.S. men (A) and women (B) by grip strength health benefit zone (HBZ), 2011–12.
More women (24.1%) than men (15.1%) were in the excellent category, p < 0.001. Compared with women of similar age, men aged 60–69 years (OR = 0.18, 95% CI = 0.08–0.39) had a lower odds of being in the excellent category. Within sex, the odds of being classified as excellent was significantly higher among women aged 40–49 years (OR = 1.87, 95% CI = 1.11–3.14), 50–59 years (OR = 2.57, 95% CI = 1.63–4.06), and 60–69 years (OR = 4.95, 95% CI = 3.10–7.90) compared with 20- to 29-year-old women. Among men, there were no significant differences in being classified as excellent across age groups.
Discussion
These data provide the first U.S. population estimates of grip strength, a marker of overall strength and future health risk, for children through senescence. These data also provide the first estimates of the proportion of the U.S. noninstitutionalized population falling into various HBZs on the basis of grip strength. Together, these data may inform surveillance data interpretation and intervention programming aimed at improving physical education and physical activity.
Consistent with other studies, grip strength was greater among men than women and mean strength increased with successive age groups into middle adulthood for both sex (2,5,6,24,30,33). For both men and women, average strength peaked in the 30- to 39-year decade. These data are similar to other reports estimating young adulthood as time of peak strength, but other reports more frequently identify the 20- to 29-year decade as the period of peak strength (30).
Our data also indicate sex differences in both the rates of increase and decrease of grip strength to and from peak, respectively. Consistent with other studies, absolute grip strength and the ascent of strength from childhood to young adulthood were greater among men than women (10,30,33). There were also age and sex differences in HBZ categories. Beginning at 15–19 years, the percentage of men and women in the needs improvement category steadily decreased with each increasing age group. However, age group–associated increase in mean grip strength was not necessarily associated with improvement in HBZ category. For example, among 15- to 19-year olds, the percentage of boys with grip strength in the needs improvement category was exceedingly high (37%), higher than has been reported for Canadians, and higher than similarly aged U.S. girls (20.3%) who were on par with their Canadian counterparts (33). Correspondingly, there were less than half as many teen boys (5.3%) in the excellent zone compared with similarly aged girls (12.1%). Excellent strength is considered important for competitive sports, an important pursuit of many teens, and has possible implications for military service readiness (11,14). Therefore, even as favorable changes in HBZ from adolescence to young adulthood seem to occur for both men and women in terms of percentage in either the needs improvement or excellent strength zone, a high frequency of teens, particularly boys, with poor strength may be of concern.
Although men and women end up with similar percent loss from peak grip strength, men aged 40–49 years had a significantly greater loss in absolute strength from peak strength as compared with women. Health benefit zone data support and extend this observation. From 40 years onward, a significantly higher percentage of men than women at corresponding ages was in the needs improvement category. The percentage of men in the needs improvement category increased steadily with age, and the percentage in the excellent grip strength category remained relatively unchanged with age. In contrast, the percentage of women aged 40 years or older in the needs improvement category was low, remained relatively steady, and was accompanied by increasing percentages of women in the excellent grip strength category with increasing age. These findings are consistent with reports indicating that women lose upper extremity strength at a lower rate than lower extremity strength, whereas men evidence parallel decline in upper and lower-body strengths (16). However, it is possible that women with poor lower-body strength have relatively good grip strength, but generally, good grip strength is associated with less disability as adults age (22,23,29).
Our study is limited in several respects. Grip strength is a proxy measure of overall muscular strength, and some outcomes (e.g., mobility) may be more closely related to leg strength or muscular endurance. We also reported absolute grip strength values, but adjustment for body size and composition (relative grip strength) has been suggested, particularly in samples of younger adults (1,32). However, using absolute grip strength values facilitates normative comparisons, and absolute values have been correlated with leg strength, muscular endurance, and with indexes of general health, disability, and mortality (27,29). Because cardiorespiratory fitness assessment did not occur in this iteration NHANES, we were also unable to compare muscular and cardiorespiratory fitness across participants. The use of grip strength–related HBZ is also a relatively new metric. Although HBZs are used in other national surveillance efforts and to facilitate exercise prescription and counseling, the research underpinning the various HBZ cut points is evolving, and specific health outcomes may be associated with different cut points, fewer categories, or both (4,5,30,33). However, the use of HBZ is also a strength of the current study and provides the first available data of its kind in the U.S. population. Grip strength protocol differences should be considered in comparing and interpreting population estimates because protocols vary in terms of position, use of both vs. single dominant hand, and number of trials that may affect results. For example, standing position has been used in many normative studies (5,8–10), whereas seated position has been used in some studies and has been recommended for frail populations (15,21). Lastly, as with all cross-sectional studies, the design limits the degree to which causal and age-related inferences can be drawn.
Practical Applications
In summary, our grip strength findings are similar to other studies that report sex differences and quadratic age-related trends in absolute strength. Our study extends previous reports concerning the U.S. population by inclusion of respondent data from childhood through senescence, provision of single-year percentile estimates for children, and inclusion of HBZ metrics, which in conjunction with grip strength information may aid surveillance data interpretation and intervention planning. Such data can be used by physical education teachers, athletic trainers, physical therapists, coaches, and fitness professionals to place grip strength fitness scores into context with a large-scale normative database.
Footnotes
The opinions in this article are those of the authors and do not represent the NIH, CDC, or U.S. Government.
References
- 1.Atlantis E, Martin SA, Haren MT, Taylor AW, and Wittert GA; Members of the Florey Adelaide Male Ageing Study. Inverse1. associations between muscle mass, strength, and the metabolic syndrome. Metabolism 58: 1013–1022, 2009. [DOI] [PubMed] [Google Scholar]
- 2.Budziareck MB, Pureza Duarte RR, and Barbosa-Silva MC. Reference values and determinants for handgrip strength in healthy subjects. Clin Nutr 27: 357–362, 2008. [DOI] [PubMed] [Google Scholar]
- 3.Cadore EL, Pinto RS, Bottaro M, and Izquierdo M Strength and endurance training prescription in healthy and frail elderly. Aging Dis 5: 183–195, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Canadian Society for Exercise Physiology. Canadian Physical Activity, Fitness And Lifestyle Approach: CSEP—Health And Fitness Program’s Health-Related Appraisal And Counselling Strategy. Ottawa, ON: Canadian Society for Exercise Physiology, 2004. [Google Scholar]
- 5.Canadian Society for Exercise Physiology. Canadian Society for Exercise Physiology-physical Activity Training for Health (CSEP-path). Ottawa, ON: Canadian Society for Exercise Physiology, 2013. pp. 210. [Google Scholar]
- 6.Catley MJ and Tomkinson GR. Normative health-related fitness values for children: Analysis of 85347 test results on 9–17-year-old Australians since 1985. Br J Sports Med 47: 98–108, 2013. [DOI] [PubMed] [Google Scholar]
- 7.Centers for Disease Control and Prevention. National Health and Nutrition Examination Surveys: NHANES; 2011. –2012, 2012. [Google Scholar]
- 8.Craig CL, Shields M, Leblanc AG, and Tremblay MS. Trends in aerobic fitness among Canadians, 1981 to 2007–2009. Appl Physiol Nutr Metab 37: 511–519, 2012. [DOI] [PubMed] [Google Scholar]
- 9.Dodds RM, Syddall HE, Cooper R, Benzeval M, Deary IJ, Dennison EM, Der G, Gale CR, Inskip HM, Jagger C, Kirkwood TB, Lawlor DA, Robinson SM, Starr JM, Steptoe A, Tilling K, Kuh D, Cooper C, and Sayer AA. Grip strength across the life course: Normative data from twelve British studies. PLoS One 9: e113637, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ervin RB, Fryar CD, Wang CY, Miller IM, and Ogden CL. Strength and body weight in US children and adolescents. Pediatrics 134: e782–e789, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Faigenbaum AD, Lloyd RS, and Myer GD. Youth resistance training: Past practices, new perspectives, and future directions. Pediatr Exerc Sci 25: 591–604, 2013. [DOI] [PubMed] [Google Scholar]
- 12.Flanagan SD, Dunn-Lewis C, Hatfield DL, Distefano LJ, Fragala MS, Shoap M, Gotwald M, Trail J, Gomez AL, Volek JS, Cortis C, Comstock BA, Hooper DR, Szivak TK, Looney DP, DuPont WH, McDermott DM, Gaudiose MC, and Kraemer WJ. Developmental differences between boys and girls result in sex-specific physical fitness changes from fourth to fifth grade. J Strength Cond Res 29: 175–180, 2015. [DOI] [PubMed] [Google Scholar]
- 13.Gale CR, Martyn CN, Cooper C, and Sayer AA. Grip strength, body composition, and mortality. Int J Epidemiol 36: 228–235, 2007. [DOI] [PubMed] [Google Scholar]
- 14.Heinrich KM, Spencer V, Fehl N, and Poston WS. Mission essential fitness: Comparison of functional circuit training to traditional Army physical training for active duty military. Mil Med 177: 1125–1130, 2012. [DOI] [PubMed] [Google Scholar]
- 15.Hillman TE, Nunes QM, Hornby ST, Stanga Z, Neal KR, Rowlands BJ, Allison SP, and Lobo DN. A practical posture for hand grip dynamometry in the clinical setting. Clin Nutr 24: 224– 228, 2005. [DOI] [PubMed] [Google Scholar]
- 16.Hughes VA, Frontera WR, Wood M, Evans WJ, Dallal GE, Roubenoff R, and Fiatarone Singh MA. Longitudinal muscle strength changes in older adults: Influence of muscle mass, physical activity, and health. J Gerontol A Biol Sci Med Sci 56: B209–B217, 2001. [DOI] [PubMed] [Google Scholar]
- 17.Katzmarzyk PT and Craig CL. Musculoskeletal fitness and risk of mortality. Med Sci Sports Exerc 34: 740–744, 2002. [DOI] [PubMed] [Google Scholar]
- 18.Kuo HK, Leveille SG, Yen CJ, Chai HM, Chang CH, Yeh YC, Yu YH, and Bean JF. Exploring how peak leg power and usual gait speed are linked to late-life disability: Data from the national health and nutrition examination survey (NHANES), 1999–2002. Am J Phys Med Rehabil 85: 650–658, 2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Li Y, Graubard BI, and Korn EL. Application of nonparametric quantile regression to body mass index percentile curves from survey data. Stat Med 29: 558–572, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mason C, Brien SE, Craig CL, Gauvin L, and Katzmarzyk PT. Musculoskeletal fitness and weight gain in Canada. Med Sci Sports Exerc 39: 38–43, 2007. [DOI] [PubMed] [Google Scholar]
- 21.Massy-Westropp NM, Gill TK, Taylor AW, Bohannon RW, and Hill CL. Hand grip strength: Age and gender stratified normative data in a population-based study. BMC Res Notes 4: 127, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Newman AB, Haggerty CL, Goodpaster B, Harris T, Kritchevsky S, Nevitt M, Miles TP, and Visser M; Health Aging Body Composition Research Group. Strength and muscle quality in a well-functioning cohort of older adults: The health, aging and body composition study. J Am Geriatr Soc 51: 323–330, 2003. [DOI] [PubMed] [Google Scholar]
- 23.Newman AB, Kupelian V, Visser M, Simonsick EM, Goodpaster BH, Kritchevsky SB, Tylavsky FA, Rubin SM, and Harris TB. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J Gerontol A Biol Sci Med Sci 61: 72–77, 2006. [DOI] [PubMed] [Google Scholar]
- 24.Omar MT, Alghadir A, and Al Baker S Norms for hand grip strength in children aged 6–12 years in Saudi Arabia. Dev Neurorehabil 18: 1–6, 2014. [DOI] [PubMed] [Google Scholar]
- 25.Ostchega Y, Dillon CF, Lindle R, Carroll M, and Hurley BF. Isokinetic leg muscle strength in older americans and its relationship to a standardized walk test: Data from the national health and nutrition examination survey 1999–2000. J Am Geriatr Soc 52: 977– 982, 2004. [DOI] [PubMed] [Google Scholar]
- 26.Package R QuntlSmoother [online], 2010. Available at: https://umd.app.box.com/s/urg7hmkf6d1fqoq1waau/1/1373505528/12247656316/1. Accessed February 26, 2015. [Google Scholar]
- 27.Roberts HC, Denison HJ, Martin HJ, Patel HP, Syddall H, Cooper C, and Sayer AA. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 40: 423–429, 2011. [DOI] [PubMed] [Google Scholar]
- 28.Ruiz JR, Sui X, Lobelo F, Lee DC, Morrow JR Jr, Jackson AW, Hebert JR, Matthews CE, Sjostrom M, and Blair SN. Muscular strength and adiposity as predictors of adulthood cancer mortality in men. Cancer epidemiology, biomarkers & prevention. Cancer Epidemiol Biomarkers Prev 18: 1468–1476, 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sallinen J, Stenholm S, Rantanen T, Heliovaara M, Sainio P, and Koskinen S Hand-grip strength cut points to screen older persons at risk for mobility limitation. J Am Geriatr Soc 58: 1721–1726, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Shields M, Tremblay MS, Laviolette M, Craig CL, Janssen I, and Connor Gorber S Fitness of Canadian adults: Results from the 2007–2009 Canadian health measures survey. Health Rep 21: 21–35, 2010. [PubMed] [Google Scholar]
- 31.Smith JJ, Eather N, Morgan PJ, Plotnikoff RC, Faigenbaum AD, and Lubans DR. The health benefits of muscular fitness for children and adolescents: A systematic review and meta-analysis. Sports Med 44: 1209–1223, 2014. [DOI] [PubMed] [Google Scholar]
- 32.Stenholm S, Sallinen J, Koster A, Rantanen T, Sainio P, Heliovaara M, and Koskinen S Association between obesity history and hand grip strength in older adults–exploring the roles of inflammation and insulin resistance as mediating factors. J Gerontol A Biol Sci Med Sci 66: 341–348, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Tremblay MS, Shields M, Laviolette M, Craig CL, Janssen I, and Connor Gorber S Fitness of Canadian children and youth: Results from the 2007–2009 Canadian health measures survey. Health Rep 21: 7–20, 2010. [PubMed] [Google Scholar]
- 34.United States. Department of health and Human services. In: 2008 physical Activity Guidelines for Americans Be Active, Healthy, and Happy! In ODPHP publication no U0036. Washington, DC: U.S. Dept. of Health and Human Services, 2008. [Google Scholar]
- 35.Yu Y, Graubard BI, and Korn EL. Local linear quantile regression. J Am Stat Assoc 93: 228–237, 1998. [Google Scholar]