

Abstract
This study reviews the performance of a community‐based nutrition programme in preventing and treating wasting without complications among children under age three in urban informal settlements of India. Implemented by a non‐profit organization, with national (Integrated Child Development Services [ICDS]) and city‐level (Municipal Corporation of Greater Mumbai [MCGM]) government partners, the programme screened 7,759 children between May 2014 and April 2015. During this period, the programme admitted 705 moderately wasted and 189 severely wasted children into the treatment group and 6,820 not wasted children into the prevention group. Both prevention and treatment groups received growth monitoring, referrals to public health facilities, and home‐based counselling (if <6 months) by community health workers. Treatment groups received additional home‐based counselling and access to medical screenings. Severely wasted children also received access to ready‐to‐use therapeutic food. The study assessed default rates, wasting status, and average weight gain 3 months after admission. Factors associated with growth faltering in the prevention group were explored using logistic regression.
Default rates for the severely wasted, moderately wasted, and prevention group were 12.7%, 20.4%, and 22.1%, respectively. Recovery rate was 42.4% for the severely wasted and 61.3% for the moderately wasted. For the moderately wasted, mean weight gain was 2.1 g/kg/day, 95% confidence interval (CI) [1.6, 2.6], and 4.5 g/kg/day for the severely wasted, 95% CI [3.1, 5.9]. Among prevention group children, 3.6% faltered into wasting—3.2% into moderate and 0.4% into severe. The paper gives insights into ways in which ICDS and MCGM can successfully integrate large‐scale community‐based acute malnutrition programming.
Key messages.
Prevention and treatment of wasting can successfully be integrated into existing public health infrastructure in urban India, where high population density provides an opportunity to monitor large numbers of wasted children.
Coverage and recovery outcomes could be improved through greater engagement of the community and better communication strategies on the health risks of moderate wasting and the preventative benefits of routine growth monitoring, timely vaccinations, and appropriate treatment of illnesses.
1. INTRODUCTION
Approximately 50 million children under age five worldwide suffer from acute malnutrition, or wasting (low weight‐for‐height; UNICEF/WHO/World Bank, 2016)—India suffers from the highest burden of wasted children (Ahmed et al., 2014; Black et al., 2008). Recent estimates indicate that 21% of Indian children under age five are wasted, and 7.5% are severely wasted (International Institute for Population Sciences, 2016a). Wasting is associated with increased risk of repeated infections and mortality (Black et al., 2008); malnourished children suffer from impaired early childhood development, thus limiting their cognitive potential (Berkman, Lescano, Gilman, Lopez, & Black, 2002; Grantham‐McGregor et al., 2007).
India's urban population grew from 222 million in 1990 to 410 million in 2014; by 2050, 50% of India's population is expected to reside in urban areas (United Nations, 2014). In urban Maharashtra, acute malnutrition rates are worse than the national average—24.9% of children under age five are wasted, and 9.5% are severely wasted (International Institute for Population Sciences, 2016b). Rapid urbanization in Mumbai has led to a subsequent increase in informal settlements (Gandhi, 2012) that carry health risks caused by lack of clean water, sanitation, and nutritious food. Children face specific nutritional disadvantages due to recurrent diarrhoea, poor breastfeeding practices, and consumption of unhealthy street foods (Ezeh et al., 2016). Complementary feeding practices in informal settlements of Mumbai are poor; a study of feeding practices found that only 13% of children 6–23 months of age met the criteria for minimum dietary diversity, and 5% had a minimally acceptable diet. Sixty‐three percent of infants (6–11 months of age) had consumed sugary snacks in the preceding 24 hr (Bentley et al., 2015).
In 1975, the Government of India (GOI) launched the Integrated Child Development Services (ICDS) mandated to ensure appropriate growth and development of all children. ICDS works at the community level to cover all children under age six and pregnant and nursing mothers. ICDS provides services through a community health centre or Anganwadi centre. These Anganwadi centres are staffed with community health workers (CHWs) called Anganwadi workers (AWWs) who provides supplementary nutrition, nonformal pre‐school services, nutrition and health education, mobilization for immunizations, and referral services. Each Anganwadi centre covers a population of approximately 1,000 and is staffed with one AWW and one assistant.
Evaluations of ICDS have indicated weak implementation (Lokshin, Das Gupta, Gragnolati, & Ivaschenko, 2005)—a 2011 interministerial plan to restructure ICDS called for a focus on children under three and community‐based prevention and care of severely undernourished children with stronger health referral linkages (Planning Commission, 2011). Despite the availability of public child health services at the municipal level through secondary and tertiary hospitals, outreach and referrals at the community level by ICDS have been ineffective (Kumar & Banerjee, 2015).
ICDS continues to target children who are underweight (low weight‐for‐age), whereas wasting is considered a more useful indicator of malnourishment in a child (Black et al., 2008). Experts have called for ICDS to integrate a strategy for outpatient community‐based therapeutic care and prevention of acute malnutrition without complications (Avula, Kadiyala, Singh, & Menon, 2013; Dalwai et al., 2013); there is less consensus on how community‐based approaches for reducing acute malnutrition can be integrated into ICDS (Dasgupta, Yumnam, & Ahuja, 2015). Community‐based Management of Acute Malnutrition (CMAM) is one proven design for treatment of severely wasted children (Bhutta et al., 2013; Collins et al., 2006; USAID, 2017), which has been recommended for integration with public health systems (Park et al., 2012); however, the literature on the effectiveness of CMAM in the Indian context is limited (Dasgupta, Sinha, & Yumnam, 2014), especially so in urban India.
The Society for Nutrition, Education and Health Action (SNEHA), a Mumbai‐based non‐profit, aimed to build a child nutrition programme for care and prevention of acute malnutrition in partnership with ICDS and the Municipal Corporation of Greater Mumbai (MCGM) in urban informal settlements of Mumbai. With MCGM, SNEHA partnered with their Nutritional Rehabilitation and Research Centre (NRRC) at Lokmanya Tilak Municipal General Hospital. Expanding the scope of typical CMAM programmes, the child nutrition programme focused on prevention as well as identification and treatment of children who are wasted. A quasi‐experimental programme evaluation of the same child nutrition programme indicated lower wasting prevalence in intervention areas at endline (More et al., 2018).
The purpose of this study is to review the performance of the child nutrition programme to provide greater insight into how a comprehensive community‐based approach to address acute malnutrition can be integrated with public health systems in urban India. We examine a cohort of children from admission through their first 3 months of participation in the child nutrition programme. Previously published methodologies were reviewed for this study (Aguayo et al., 2013; Akparibo, Harris, Blank, Campbell, & Holdsworth, 2017) to evaluate (a) key programme outcomes of default rates, wasting status, and average weight gain against standards recommended internationally for Outpatient Therapeutic Programme CMAM reporting (Save the Children, 2015) and (b) factors associated with growth faltering among children who were admitted as not wasted using logistic regression models.
2. METHODS
2.1. The child nutrition programme
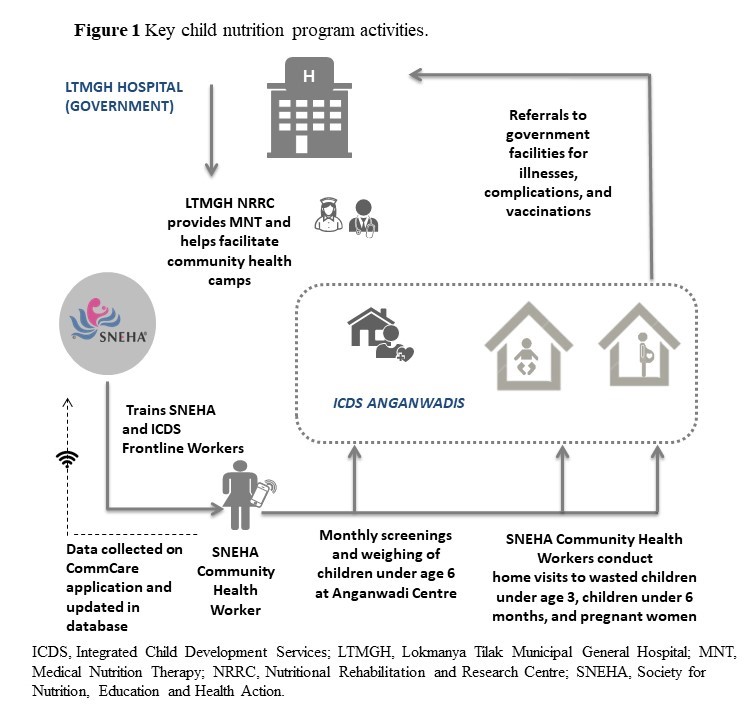
In collaboration with ICDS and MCGM, SNEHA led the implementation of the child nutrition programme from December 2011 through March 2016 in Dharavi, one of South Asia's largest informal settlements. Covering 300 Anganwadi centres, a population of approximately 300,000, the child nutrition programme incorporated both prevention and treatment mechanisms to address wasting. The treatment component for children with severe wasting was adapted from international and national facility‐based management guidelines recommended by the World Health Organization (WHO) and GOI (Government of India Ministry of Health and Family Welfare, 2011; WHO, 2013b). While AWWs cover all children under age six, SNEHA staffed additional CHWs to focus on children under age three. Each SNEHA CHW covered three Anganwadi centre cluster areas, typically monitoring a total of 150–180 children under age three.
Figure S1 presents an overview of key child nutrition programme activities.
SNEHA CHWs and AWWs worked together to continuously identify households in the Anganwadi centre service area and screen all children under age three for wasting. At the time of screening, SNEHA CHWs collected basic socioeconomic information for the household and referred children with complications (including bipedal oedema, convulsions, severe diarrhoea, high fever, persistent vomiting, tuberculosis, and HIV) to the MCGM NRRC for additional treatment. Children with uncomplicated moderate or severe wasting were admitted and categorized into a treatment group for additional programme activities. Children not wasted at screening continued to be monitored through the prevention activities of the programme.
2.1.1. Prevention activities
All children (prevention and treatment groups) were monitored monthly for wasting at the Anganwadi centre as a part of routine ICDS monthly growth monitoring activities. SNEHA CHWs monitored all immunization records and gave appropriate referrals to government health facilities and local vaccination campaigns. Caregivers of all children under the age of 6 months also received monthly home visits by SNEHA CHWs for counselling focused on appropriate breastfeeding and complementary feeding practices.
Community awareness activities, including women's groups and motivational events, were regularly held at the Anganwadi centres. Motivational events included activities such as celebrations for children who had recovered from wasting and remained not wasted for at least 6 months, Ushtavan celebrations for the introduction of complementary feeding, Godbharai or baby shower celebrations for pregnant women, and Khana Khazana events to demonstrate nutritional recipes to caregivers. CHWs also held rallies called Mata Melavas or Mothers Gathering for caregivers to participate in health and nutrition games and movie screenings at the community level.
On‐going training on maternal and child health topics and Appreciative Inquiry workshops were conducted with SNEHA CHWs and AWWs to build their capacity in conducting anthropometry and to ensure consistent and appropriate communication during home visits. Appreciative Inquiry is a participatory methodology frequently used by SNEHA in their work with public health systems. The process aims to encourage positive changes by valuing existing possibilities, capabilities, and assets (Moore & Charvat, 2007). SNEHA and ICDS supervisory staff regularly held monthly planning meetings to facilitate coordination of activities, review data, and discuss specific cases of wasted children that were either not improving or had caregivers that were reluctant to participate in programme activities.
2.1.2. Treatment for moderately and severely wasted children
All caregivers of children in the severely or moderately wasted treatment groups received additional home visits by SNEHA CHWs for counselling. Home visits were done on a weekly basis for both treatment groups; however, severely wasted children were typically visited more often during the first 2 weeks after admission to encourage participation in programme activities. Caregivers of moderately and severely wasted children were encouraged to bring their children to SNEHA community‐based health camps for a medical screening. Doctors at the health camps confirmed wasting status, prescribed antibiotics if required, and referred children to appropriate public health facilities.
SNEHA CHWs referred all severely wasted children to the NRRC and accompanied caregivers to the NRRC if required. At the NRRC or the SNEHA community health camps, eligible severely wasted children underwent appetite tests for Medical Nutrition Therapy (MNT) supplements that are provided by the NRRC. MNT is a locally produced nutrient dense lipid‐based paste given in prepackaged cups to children over six months that are severely wasted, do not suffer from medical complications, and have passed an appetite test. Lokmanya Tilak Municipal General Hospital, Indian Institute of Technology Bombay, and Toddler Food Partners (USA) developed the composition and production processes (Shah, Jadhav, Manglani, Fernandes, & Surve, 2015). Doctors typically prescribed children 1–2 cups daily as a supplement to their regular diet over an 8‐week treatment period.
SNEHA CHWs provided regular doorstep delivery of the MNT cups, free of cost, to children. Although supply and cost of MNT to the caregivers were not issues, the key challenge was timely confirmation of the severe wasting diagnosis by a doctor at the SNEHA health camp or NRRC. MNT could not be prescribed without examination by a paediatric doctor and often caregivers did not want to travel to the NRRC or found the timing of the health camp to be inconvenient. SNEHA could staff one paediatrician for the programme; in any given area, there was one health camp per month. Once a prescription was given, SNEHA CHWs found monitoring compliance with consumption also to be a challenge; despite cups being delivered, SNEHA CHWs were not certain the wasted child was in fact consuming the cups according to protocol.
2.2. Data collection and analysis
SNEHA CHWs collected surveillance data on pregnant women and children under age three using Android smartphones and the CommCare mobile application designed for CHWs. CHWs collected longitudinal data records, including anthropometric data, on the mobile application. The application facilitated accurate categorization of children based on their wasting status through a built‐in nutrition calculator (Chanani et al., 2016).
SNEHA CHWs assessed wasting using weight for height or length anthropometric measurements and children were categorized based on the WHO 2006 simplified weight‐for‐height or length field tables (WHO, 2016). SNEHA CHWs calculated child age by entering the date of birth in the smartphone; the CommCare application was programmed to provide an age estimate based on the date of screening, and the CHW confirmed the age with the caregiver. Moderate wasting is defined for children with weight‐for‐height or length z‐scores (WHZ) lower than two standard deviations (SDs) below the median WHO growth standards and equal to or above three SDs below the median; severely wasted children have WHZ scores lower than three SD below the median WHO growth standards. Mid‐Upper Arm Circumference was not used as an additional criterion.
The study evaluated programme surveillance data collected by SNEHA CHWs electronically from a purposively selected period between May 1, 2014, and April 30, 2015, by when programme processes had been well established. The study includes all children under age three admitted into the child nutrition programme in five administrative areas of Dharavi, covering a population of 150,000.
Table 1 provides detailed definitions of status categories. All children were continuously monitored by SNEHA and ICDS, so the typical “Re‐admission,” “Non‐Recovery,” “Moved‐out,” and “Relapse” categories for CMAM programmes do not apply. The child nutrition programme did not formally discharge children; thus, we examined the children's status 3 months after being admitted into the child nutrition programme. The standard Outpatient Therapeutic Programme recommendation for an average length of stay of 45–60 days was adjusted to 3 months for the study because children were weighed monthly at the Anganwadi centre on specific days of the month. Depending on what day of the month a child was admitted into the child nutrition programme, the child might not have attended their first follow‐up growth monitoring session until the next month.
Table 1.
Categories for children enrolled in the community‐based child nutrition programme
| Category | Definition |
|---|---|
| Admit | Child under 3 years of age without complications who was screened with anthropometry and background information collected. |
| Monitored | Post admission, the child attended at least one follow‐up growth monitoring session within 3 months. |
| Defaulter | Post admission, the child did not receive any growth monitoring follow‐up within 3 months. |
| Recovered | Three months post admission, a wasted child is no longer wasted. |
| Improved | Three months post admission, a severely wasted child became moderately wasted. |
| Thriving | Three months post admission, a child admitted as not wasted continued to remain not wasted. |
| Non‐response | Three months post admission, a severely wasted child stayed severely wasted or a moderately wasted child stayed moderately wasted. |
| Faltering | Three months post admission, a moderately wasted children became severely wasted or a child admitted as not wasted became wasted. |
| Exits | Children who left the programme within 3 months of admission. This includes deaths, migration, and becoming over 3 years of age (ineligible). |
2.2.1. Statistical analysis
Surveillance data were downloaded from the CommCare server in Excel and imported into STATA version 12 (StataCorp LP, College Station, TX) for analysis. Children excluded from the analysis include those who were: older than 3 years of age at the time of screening; marked by SNEHA CHWs as an “incorrect” entry; without valid geographic information; given an incorrect wasting status based on their anthropometric information; or screened with WHZ scores out of range by WHO standards (−5 SD to +5 SD). Children with implausible weight gains and losses were excluded from the average weight gain analysis.
The study assessed wasting status and average weight gain of the child by their third month post admission. Over the 3‐month period, the mean gram weight gain per kilogram of body mass per day (g/kg/day) is calculated for all children included in the analysis. The calculation uses the total individual weight gained since admission, based on the last measurement taken during the 3‐month period. The study also reviewed the mean number of days since admission from the date of the last measurement used in the weight gain calculation. Multilevel logistic regression analysis explored factors associated with children in the prevention group faltering into wasting status, adjusting for clustering at the Anganwadi centre level. A child screened as not wasted was coded as 1 if she faltered by the end of the 3‐month period into severe or moderate wasting. Children who remained not wasted were coded as 0. Independent variables included all the socioeconomic information collected at the time of admission.
2.2.2. Ethical approval
Data presented are part of programme implementation where participation by mothers and children was voluntary. Use of the intervention data for a study on programme impact and effectiveness was approved by the Institutional Ethics Committee at Bandra Holy Family Medical Research Society, Mumbai.
3. RESULTS
Between May 2014 and April 2015, 7,759 children were identified and screened. Cases removed from the analysis include 10 children older than 3 years of age at the time of screening, 163 children marked by the CHW as an “incorrect” data entry case or for not having valid geographic information, 291 children screened incorrectly on their wasting status, and 31 children with implausible WHZ scores.
3.1. Characteristics of children screened into the child nutrition programme
Table 2 describes the characteristics of children screened into the child nutrition programme. Nearly half of the children in the prevention group who were screened as not wasted were female, whereas approximately 43% of the severely wasted in the treatment group were female. Over 20% of children screened were below 6 months of age in both groups. Severely wasted children experienced higher rates of illness (25%) at the time of screening as compared with children who were not wasted (8%). Close to half of the children in both prevention and treatment group were residing in joint families, and over 90% of mothers reported that they do not work for income. Thirty‐five percent of severely wasted children were firstborns as compared with 44% of the children in the prevention group. Children in the treatment group (severe and moderately wasted) have higher poverty likelihoods according to the Progress out of Poverty Index. The mean likelihoods indicate that 79% of severely wasted children were likely to be living in households below the $2.16 per day PPP poverty line as compared with 75% of the children who were not wasted.
Table 2.
Characteristics of children screened into prevention and treatment group
| Prevention: Not wasted | Treatment: Wasted | ||
|---|---|---|---|
| Moderate | Severe | ||
| Screened N | 6,849 | 715 | 195 |
| n (%) | n (%) | n (%) | |
| Female | 3,372 (49.2) | 315 (44.1) | 84 (43.1) |
| Age (months) | |||
| 0 to 5 | 1,665 (24.3) | 147 (20.6) | 46 (23.6) |
| 6 to 11 | 1,365 (19.9) | 149 (20.8) | 33 (16.9) |
| 12 to 23 | 2,245 (32.8) | 282 (39.4) | 74 (37.9) |
| 24 to 36 | 1,574 (23.0) | 137 (19.2) | 42 (21.5) |
| Experiencing illness (at admission) | 527 (7.7) | 134 (18.7) | 49 (25.1) |
| Diarrhoea | 138 (2.0) | 41 (5.7) | 13 (6.7) |
| Fever | 247 (3.6) | 64 (9.0) | 22 (11.3) |
| Cough | 100 (1.5) | 18 (2.5) | 7 (3.6) |
| Lives in joint family | 3,400 (49.6) | 346 (48.4) | 86 (44.1) |
| Mother not working | 6,484 (94.7) | 679 (95.0) | 182 (93.3) |
| Household owns home | 3,732 (54.5) | 372 (52.0) | 96 (49.2) |
| Birth order: First child | 2,877 (43.9) | 261 (38.2) | 63 (34.8) |
| Progress out of poverty index poverty likelihoods below $2.16/day/PPP line | |||
| % mean likelihood | 74.6 | 78.2 | 79.4 |
Note. For birth order, total sample falls to 7,412; for the Progress out of Poverty index, the sample falls to 7,735.
3.2. Status of children 3 months after admission into the child nutrition programme
Figure S2 presents a flow diagram of the study cohort.
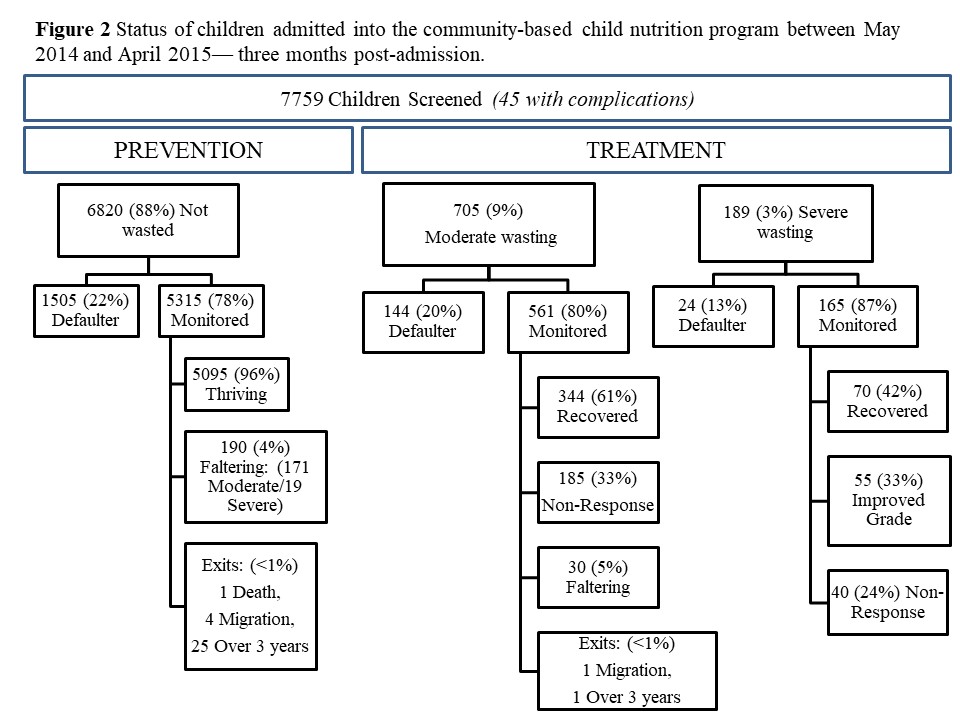
SNEHA CHWs identified 45 (0.6%) of the 7,759 screened children as having one or more complications. Table 3 presents the status of children 3 months after admission. Among the 6,820 children admitted into the prevention group, 5,315 (78%) were monitored within 3 months of admission. In the treatment group, 561 (80%) of the 705 children admitted as moderately wasted were monitored, and 165 (87%) of the 189 severely wasted children were monitored after screening. Overall, a total of 32 monitored children exited the intervention during this 3‐month period; one was due to death.
Table 3.
Status of children admitted into the community‐based child nutrition programme—Three months post admission
| Prevention: Not wasted | Treatment: Wasted | ||
|---|---|---|---|
| Moderate | Severe | ||
| Total admitted | 6820 | 705 | 189 |
| n (%) | n (%) | n (%) | |
| Defaulters | 1,505 (22.1) | 144 (20.4) | 24 (12.7) |
| Monitored | 5,315 (77.9) | 561 (79.6) | 165 (87.3) |
| Recovered | — | 344 (61.3) | 70 (42.4) |
| Improved | — | — | 55 (33.3) |
| Thriving | 5,095 (95.9) | — | — |
| Non‐response | — | 185 (33.0) | 40 (24.2) |
| Faltering (moderate) | 171 (3.2) | — | — |
| Faltering (severe) | 19 (0.4) | 30 (5.3) | — |
| Exits | 30 (0.6) | 2 (0.4) | 0 (0.0) |
In the prevention group, 1,505 (22%) of children were categorized as Defaulters for not attending any growth monitoring sessions within 3 months of their admission. In the treatment groups, 144 (20%) of moderately wasted children defaulted and severely wasted children experienced the lowest default rate of 13% (24 of 189 children). No severely wasted child exited during the three‐month period. Among those in the prevention and moderately wasted treatment group who exited, the primary reason was turning over 3 years of age. Although they were no longer monitored by SNEHA CHWs, they continued to be monitored by ICDS.
Three hundred forty‐four (61%) of the 561 monitored moderately wasted children and 70 (42%) of the 165 monitored severely wasted children recovered to not wasted within 3 months. Fifty‐five (33%) of the monitored severely wasted children had not yet fully recovered but had improved to moderate status. One hundred eighty‐five (33%) of the monitored moderately wasted children and 40 (24%) of the monitored severely wasted children were not yet responding to the intervention within 3 months. Over this period, 190 (4%) children in the prevention group faltered into wasting, and 30 (5%) moderately wasted children became severely wasted.
Table 4 summarizes the mean admission age, mean days since admission, and mean weight gain for monitored children. The mean age at the time of admission is approximately the same around 14–15 months of age for children in both prevention and treatment groups. The mean number of days between admission and the last growth monitoring follow‐up during the 3‐month period is also similar for all categories at approximately 70–71 days. Children in the prevention group screened as not wasted gained an average of 1.9 g/kg/day, 95% confidence interval (CI) [1.8, 2.0] since their last measurement taken during the 3‐month period. In the treatment groups, moderately wasted children gained an average of 2.1 g/kg/day, 95% CI [1.6, 2.6], and severely wasted children gained an average of 4.5 g/kg/day, 95% CI [3.1, 5.9].
Table 4.
Mean admission age, mean weight gain, and mean days since admission for monitored children—Three months post admission
| N | Mean admission age (months) | Mean days since admission | Mean weight gain (g/kg/day) | |
|---|---|---|---|---|
| (95% CI) | (95% CI) | (95% CI) | ||
| Prevention: | ||||
| Not wasted | 5,269 | 14.6 (14.3–14.9) | 70.4 (69.8–71.0) | 1.9 (1.8–2.0) |
| Treatment: Wasted | ||||
| Moderate | 557 | 14.6 (13.9–15.4) | 71.4 (69.8–73.0) | 2.1 (1.6–2.6) |
| Severe | 163 | 14.8 (13.4–16.3) | 71.2 (68.2–74.3) | 4.5 (3.1–5.9) |
Note. g/kg/day gram weight gain per kilogram of body mass per day.
Another standard measure of recovery for weight gain in CMAM programmes is the percentage of severely wasted children who gain at least 15% of their admission weight. For the 163 severely wasted children whose weight gain was analysed, 50.3% (not shown in tables) gained at least 15% of their admission weight within 3 months.
3.3. Factors associated with growth faltering into wasting
Table 5 presents the regression analysis examining characteristics among prevention group children associated with faltering into wasting (severe or moderate). Results indicated that girls (adjusted odds ratio = 0.67, 95% CI [0.49, 0.91]) had lower odds of faltering as compared with boys. Older children were more likely to falter (adjusted odds ratio = 1.12, 95% CI [1.09, 1.16]). As expected, a higher admission screening weight was associated with lower odds of faltering (adjusted odds ratio = 0.58, 95% CI [0.50, 0.66].
Table 5.
Factors associated with faltering into wasting for children in the prevention group—Three months post admission
| Faltering |
Crude odds ratio (95% CI) |
Adjusted odds ratio (95% CI) |
||
|---|---|---|---|---|
|
No (N = 5,125) n (%) |
Yes (N = 190) n (%) |
|||
| Female | 2,542 (49.6) | 87 (45.8) | 0.85 (0.64, 1.14) | 0.67 (0.49, 0.91)* |
| Age (months) | 14.6 (14.2, 15.1) | 14.6 (13.0, 16.3) | 1.00 (0.98, 1.01) | 1.12 (1.09, 1.16)** |
| Illness (at admission) | 325 (6.3) | 14 (7.4) | 1.22 (0.69, 2.14) | 1.24 (0.69, 2.22) |
| Lives in joint family | 2,575 (50.2) | 99 (52.1) | 1.09 (0.81, 1.46) | 1.18 (0.83, 1.67) |
| Mother not working | 4,852 (94.7) | 183 (96.3) | 1.50 (0.69, 3.24) | 1.40 (0.63, 3.10) |
| Household owns home | 2,861 (55.8) | 104 (54.7) | 0.95 (0.71, 1.28) | 0.89 (0.63, 1.27) |
| Birth order | ||||
| First child | 2,185 (44.4) | 78 (42.9) | 1 | 1 |
| Second child | 1,622 (33.0) | 60 (33.0) | 1.03 (0.73, 1.46) | 0.89 (0.62, 1.28) |
| Third child | 666 (13.5) | 22 (12.1) | 0.93 (0.57, 1.52) | 0.77 (0.46, 1.30) |
| Fourth or higher | 443 (9.0) | 22 (12.1) | 1.39 (0.85, 2.28) | 1.05 (0.60, 1.84) |
| Admission weight (kg) | 8.2 (8.1, 8.3) | 7.4 (7.1, 7.8) | 0.89 (0.84, 0.94) | 0.58 (0.50, 0.66)** |
| PPI: % mean likelihood below the $2.16/day/PPP line | 74.3 (73.2, 75.5) | 77.2 (74.6, 79.8) | 2.80 (1.08, 7.22) | 1.87 (0.61, 5.75) |
Note. For age, admission weight and Progress out of Poverty Index (PPI), means are presented with 95% confidence intervals (CIs). Illnesses documented at admission include diarrhoea, cough, fever, and vomiting. Adjusted model sample falls to 5,081 due to missing birth order data that was added after revising the screening format.
P ≤ 0.05.
P ≤ 0.001.
4. DISCUSSION
This paper reviews the performance of a community‐based nutrition programme implemented collaboratively by a non‐profit organization, with national and city‐level government partners in informal settlements of Mumbai, India. Findings suggest that wasted children, as compared with children who were not wasted, are more likely to be male, belong to the 12–23 months age group, not be a firstborn child, be experiencing an illness, and come from a poorer household. Although many CMAM programmes exclude children below 6 months of age, approximately 24% of severely wasted children in this cohort were below 6 months. These estimates reinforce the importance of early intervention, as recommended by the WHO (World Health Organization, 2013a), to prevent acute malnutrition among children.
4.1. Default rates and effective coverage
Default rates were over 15% for the children admitted as moderately wasted or not wasted, indicating a need for reducing attrition in the prevention and the moderately wasted treatment components of the programme. SNEHA CHWs' focus on ensuring timely treatment of severely wasted children may have affected the participation of children who were moderately wasted or in the prevention group. A qualitative study of high default rates in a rural CMAM programme in Bihar, India, determined that more effort was needed to create an understanding of malnutrition as a disease at the community level and to empower caregivers to adopt proactive care‐seeking behaviours concerning malnutrition prevention and treatment (Burtscher & Burza, 2015). The study found that better communication strategies should incorporate local perceptions and beliefs regarding malnutrition, along with a more contextual understanding of what it means to be a healthy child. Processes for ensuring participation of all children in the child nutrition programme could have improved through better communication to caregivers regarding the health risks of moderate wasting and the preventative benefits of routine growth monitoring, appropriate complementary feeding practices, timely vaccinations, and treatment of illnesses. Caregivers would have benefited from an understanding that all children, and not just the severely wasted, were at risk of poor growth and cognitive development without the appropriate introduction of solids, a more diverse diet, and less displaced consumption through nutrient poor snack foods.
The migratory nature of the community also affects attrition. Programmes working in urban informal settlements face difficulty in tracking the movement of families within the city and back and forth to their natal villages. Additionally, given the instability of informal settlements, some Anganwadi boundaries shifted or areas were demolished. The child nutrition programme had systems in place to follow‐up with children that had moved within the intervention area, but temporary and permanent movement remained a challenge for on‐going surveillance activities. SNEHA CHWs have indicated that a substantial number of defaulters had likely migrated within and outside the intervention areas.
4.2. Prevention of wasting
This child nutrition programme expands the scope of typical CMAM programmes by focusing on the prevention of wasting for all children. Only 190 (3.6%) of the monitored children in the prevention group faltered during the 3‐month period from admission, with 171 of the 190 falling into moderate wasting. In these informal settlements, environmental factors beyond the scope of the programme such as poor quality of water, lack of access to sanitation, open sewers, and overcrowding contribute to the persistence of malnutrition in children (Pörtner & Su, 2018). An incidence rate of 3.2% for moderate wasting and 0.4% for severe wasting among the prevention group suggests the prevention component of the child nutrition programme was effective.
Given that the primary activity for the prevention group was the monthly growth monitoring at the Anganwadi centre, the child nutrition programme could have further strengthened the prevention component by ensuring that the growth monitoring activity was more systematically coupled with age‐specific health and nutritional counselling from the SNEHA CHWs and AWWs. Caregivers should not perceive growth monitoring as an activity primarily for the screening of wasting but also as a point of interaction for getting information on breastfeeding, complementary feeding, immunizations, and illness management (Ashworth, Shrimpton, & Jamil, 2008). A review of effective information, education, communication interventions to improve complementary feeding practices indicates that using multiple and existing workers to counsel caregivers is feasible and improves coverage and impact (Aguayo, 2017). Studies in other urban contexts, where commercial foods are ubiquitous, have highlighted that caregivers struggle with children's demand and preferences for snack foods (Pries et al., 2017). The child nutrition programme held cooking workshops to teach caregivers how to make nutritious home‐cooked foods using local ingredients; AWWs provided take‐home rations for all children in the community. These were additional opportunities for CHWs and AWWs to discuss complementary feeding challenges and provide advice on how to include fresh and nutrient‐rich foods in the diets of children who were not wasted.
The factors associated with the incidence of wasting among the children in the prevention group indicate vulnerabilities among boys and older children in this context. The findings for boys are consistent with a review of risk factors for children living in urban informal settlements (Goudet, Griffiths, Bogin, & Madise, 2017), which found that in most studies, male children were more malnourished than females. A review of national surveys in South Asia noted the systematically higher prevalence of wasting among boys in India since the mid‐1990s (Harding, Aguayo, & Webb, 2018). In a 2014 survey of the 10 most populous cities of India, boys had a greater prevalence of wasting in every city (Naandi Foundation, 2014). At the same time, a demographic review also indicated the possibility that wasting among girls in Indian urban informal settlements could be underestimated due to son preference selection and the substantial number of missing girls (Pörtner & Su, 2018).
4.3. Treatment of wasted children
4.3.1. Severe wasting
The performance of this cohort, when compared with Sphere minimum standards (Save the Children, 2015) for the management of severe acute malnutrition, is mostly positive. For severely wasted children, the default rate (12.7%) met the international standard (<15%) and the average weight gain (4.5 g/kg/day) for severely wasted children also met the standard for outpatient care (>4 g/kg/day). By the end of 3 months, approximately 42% of the severely wasted children were not experiencing any wasting. Over 50% of the severely wasted children gained at least 15% of their admission weight within 3 months (not shown in tables). Although this percentage is less than the Sphere standard (>75%), the appropriateness of the 15% weight gain criteria is under scrutiny (V. Aguayo, Badgaiyan, & Singh, 2014).
Other facility and community‐based nutrition programmes in India have had similarly low performance in recovery rates (Aguayo et al., 2013; V. M. Aguayo et al., 2014; Burza et al., 2015; Prasad & Sinha, 2015; Singh et al., 2014). In the only Indian multicentre randomized trial evaluating the efficacy of ready‐to‐use therapeutic food (RUTF) for community‐based treatment of uncomplicated severe acute malnutrition, recovery rates were below 41% at 8 weeks of treatment; after extending to 16 weeks, over 40% of children had not yet recovered (Bhandari et al., 2016).
4.3.2. Moderate wasting
The recovery rate of moderately malnourished children was also below the Sphere benchmark, and 5% of the moderately malnourished worsened into severe wasting. The reason for lower recovery outcomes could be the greater programmatic focus on the severely wasted treatment group and perhaps a lack of more aggressive strategies to improve recovery rates of moderately malnourished children, such as the provision of RUTF. However, the evidence on RUTF for moderately wasted children is neither clear nor inclusive for South Asia with respect to recovery or preventing deterioration into acute malnutrition (Kennedy, Branca, Webb, Bhutta, & Brown, 2015).
4.4. Strengthening community engagement to improve prevention and treatment
The programme evaluation of the child nutrition programme found that the reduction in the prevalence of wasting was due in large part to the constant presence and intensive support of the SNEHA CHWs (More et al., 2018). The reliance on SNEHA CHWs highlights the programmatic gap in developing community‐level demand for ICDS and NRRC services. Recommendations for addressing community engagement in CMAM programmes include peer counselling to ensure relevancy and credibility of information, on‐going sharing of results with the community for participatory solutions, the inclusion of key community‐level influencers, and participation of volunteers in community screening (Blanárová, Rogers, Magen, & Woodhead, 2016).
4.5. Next phase of the programme and integration with Mahila Arogya Samitis
In April 2016, SNEHA, ICDS, and MCGM formalized the partnership with a Memorandum of Understanding to form the Mumbai Child Health and Nutrition Committee and began a process of handover to sustain the overall reduction in wasting achieved by the programme. The longer term sustainability strategy is to shift direct implementation of programme activities done by SNEHA CHWs to both ICDS and the community. The goal of the next iteration of the programme is to strengthen ICDS capacity to effectively deliver services while also building community ownership over activities to prevent and treat child malnutrition.
SNEHA will provide technical support to ICDS in strengthening the following core activities: (a) registration of pregnant woman for institutional delivery in their first or second trimester, (b) pregnant woman accessing antenatal care in her first trimester, (c) growth monitoring of children under 6 years of age, (d) distribution of take‐home rations, (e) complete immunizations of children, (f) counselling on infant and young child feeding practices, and (g) appropriate referrals to public health facilities for management of illnesses. SNEHA's capacity building efforts with ICDS have included workshops to jointly articulate a vision and build a plan of action, participatory learning and action exercises, and training on relevant health and nutrition topics. Using an Appreciative Inquiry approach, SNEHA will provide on‐going monitoring, feedback, and assistance to ICDS (at all levels) to deliver the above core activities.
To foster community ownership, SNEHA is recruiting community volunteers who can assist and monitor community‐based activities including identification of beneficiaries (children and pregnant women), mobilization of community members to access services offered by ICDS and MCGM, resource mobilization to conduct community‐level awareness events, making referrals, conducting home visits, and accompanying community members to hospitals as and when needed. Community volunteers will be trained along with ICDS staff on health and nutrition topics to enable them better to assist AWWs in tracking and encouraging children to attend the growth monitoring sessions and other community activities. The implementation team has initiated the process of shortlisting community volunteers—three to five volunteers including female, male, and youth volunteers per Anganwadi centre; thus far, the child nutrition programme has recruited over 600 individuals.
All activities fall within the services currently mandated by the public health systems, thus minimizing the need for external funding. Building community ownership is in line with key policy principles of decentralized decision‐making prescribed in the most recent National Health Policy of India, which promotes community participation in health planning (Government of India. Ministry of Health and Family Welfare, 2017). Subsequently, SNEHA expects the community volunteers to convert to or join with existing Mahila Arogya Samitis (MAS), which are community‐based women's groups that serve as local institutions for health planning and action. MAS is a state‐level programme being implemented to strengthen community processes in urban areas under the National Urban Health Mission. MAS groups are expected to support government CHWs (for both ICDS and National Urban Health Mission), by generating community awareness and facilitating linkages to maternal, newborn, child health and nutrition services; water, sanitation, and hygiene services; adolescent health issues, and noncommunicable diseases (Government of India. Ministry of Health and Family Welfare, 2014).
4.6. Limitations
For the multivariable regression model, due to the nature of surveillance data, the child nutrition programme had to prioritize timely screening of all children. Thus, the number of independent variables available to include in the adjusted model is limited. A key limitation in understanding the effectiveness of the prevention component is a lack of comparison data on what incidence of wasting would have been without the programme. Another limitation of the study is our weak understanding of compliance with the MNT component of the programme and the challenges faced by both programme staff and caregivers in feeding severely wasted children the RUTF supplements. Intervention data indicates that both provision and consumption of MNT was poor. Nutrient‐rich therapeutic food has been proven to improve the recovery of severely wasted children. Our study lacked information on to what extent poor compliance was affected by availability, quality, or perceptions of the product.
5. CONCLUSIONS
To the best of our knowledge, the child nutrition programme has been the only large‐scale community‐based nutrition programme working in partnership with ICDS and a municipal corporation to identify, treat, and prevent wasting in urban informal settlements of India. Although the child nutrition programme was implemented by a non‐profit organization, a key strength was that at each step an attempt was made to strengthen and work in collaboration with the public health systems. The child nutrition programme also demonstrated how the dense nature of urban informal settlements is an opportunity for ICDS to explore innovative approaches to reduce acute malnutrition; AWWs can monitor large numbers of vulnerable children that reside a short distance from the Anganwadi centre. A community‐based approach for addressing acute malnutrition through ICDS infrastructure in urban India is viable. But to promote better coverage and recovery outcomes further efforts are required to build community awareness, ownership, and participation in activities for both prevention and treatment.
CONFLICTS OF INTEREST
All authors are employed by SNEHA. No authors have received grants, speakers fees, etc., from any commercial body within the past 2 years.
CONTRIBUTIONS
SC and AJ designed research, including development of overall research plan, and study oversight. SC analysed data and drafted manuscript. AJ, SP, NSM provided critical review and commentary to revisions of manuscript. AW and NSM led programme implementation. AF conceptualized the overall design and objectives of the intervention. AJ had primary responsibility for final content of manuscript. All authors read and approved the final manuscript.
Supporting information
Figure S1. Key child nutrition program activities
{kind=link}
Figure S2. Status of children admitted into the community‐based child nutrition program between May 2014 and April 2015‐three months post‐admission
{kind=link}
ACKNOWLEDGEMENTS
We thank the families and caregivers in Dharavi who made this study possible through their participation in the SNEHA child nutrition programme. We thank all the programme coordinators, programme officers, and FWs CHWs for data collection and supervision of programme operations. We are thankful to Archana Bagra, Vanessa D'souza, Priya Agrawal, Wasundhara Joshi, Devika Deshmukh, Evelet Sequeira, Vishal Kapoor, and members of the SNEHA Research Group. We thank the implementation funders. Finally, we thank the Integrated Child Development Services Scheme staff and The Municipal Corporation of Greater Mumbai for their partnership.
Chanani S, Waingankar A, Shah More N, Pantvaidya S, Fernandez A, Jayaraman A. Effectiveness of NGO‐government partnership to prevent and treat child wasting in urban India. Matern Child Nutr. 2019;15(S1):e12706 10.1111/mcn.12706
Clinical Trial Registry number: Retrospectively registered; ISRCTN62834195
Footnotes
Bipedal oedema is swelling in both foot and legs due to accumulation of fluids resulting from severe acute malnutrition.
Bubble levels (manufactured by Freemans Measures Pvt. Ltd.) were used to verify flat weighing locations. Children under 2 years lay or sat on an electronic baby weighing scale (manufactured by Nitiraj Engineers Pvt. Ltd.), and their lengths were measured on an infantometer (manufactured by Meditrin Instruments Pvt. Ltd.). Children over 2 years were weighed on an adult weighing scale, and heights were taken using measuring tapes with accuracy up to 0.1 cm.
The Progress out of Poverty Index is an India‐specific poverty tool that utilizes 10 questions about household characteristics (e.g., father's education and occupation) and assets to estimate the likelihood that the household is living above or below international poverty lines—this study utilizes the 2008 India scorecard.
REFERENCES
- Aguayo, V. , Badgaiyan, N. , & Singh, K. (2014). How do the new WHO discharge criteria for the treatment of severe acute malnutrition affect the performance of therapeutic feeding programmes? New evidence from India. European Journal of Clinical Nutrition, 69(10), 509–513. 10.1038/ejcn.2014.197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aguayo, V. M. (2017). Complementary feeding practices for infants and young children in South Asia. A review of evidence for action post‐2015. Maternal & Child Nutrition, 13 Suppl 2 10.1111/mcn.12439 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aguayo, V. M. , Agarwal, V. , Agnani, M. , Das Agrawal, D. , Bhambhal, S. , Rawat, A. K. , … Singh, K. (2013). Integrated program achieves good survival but moderate recovery rates among children with severe acute malnutrition in India. American Journal of Clinical Nutrition, 98(5), 1335–1342. 10.3945/ajcn.112.054080 [DOI] [PubMed] [Google Scholar]
- Aguayo, V. M. , Jacob, S. , Badgaiyan, N. , Chandra, P. , Kumar, A. , & Singh, K. (2014). Providing care for children with severe acute malnutrition in India: New evidence from Jharkhand. Public Health Nutrition, 17(1), 206–211. 10.1017/S1368980012004788 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahmed, T. , Hossain, M. , Mahfuz, M. , Choudhury, N. , Hossain, M. M. , Bhandari, N. , … Bhutta, Z. (2014). Severe acute malnutrition in Asia. Food and Nutrition Bulletin, 35(2), S14–S26. 10.1177/15648265140352S103 [DOI] [PubMed] [Google Scholar]
- Akparibo, R. , Harris, J. , Blank, L. , Campbell, M. J. , & Holdsworth, M. (2017). Severe acute malnutrition in children aged under 5 years can be successfully managed in a non‐emergency routine community healthcare setting in Ghana. Maternal & Child Nutrition, 13, e12417 10.1111/mcn.12417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashworth, A. , Shrimpton, R. , & Jamil, K. (2008). Growth monitoring and promotion: Review of evidence of impact. Maternal & Child Nutrition, 4(Suppl 1), 86–117. 10.1111/j.1740-8709.2007.00125.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Avula, R. , Kadiyala, S. , Singh, K. , & Menon, P. (2013). The operational evidence base for delivering direct nutrition interventions in India: A desk review. IFPRI ‐ Discussion Papers, (1299), vii + 60 pp.
- Bentley, A. , Das, S. , Alcock, G. , Shah More, N. , Pantvaidya, S. , & Osrin, D. (2015). Malnutrition and infant and young child feeding in informal settlements in Mumbai, India: Findings from a census. Food Science & Nutrition, 3(3), 257–271. 10.1002/fsn3.214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkman, D. S. , Lescano, A. G. , Gilman, R. H. , Lopez, S. L. , & Black, M. M. (2002). Effects of stunting, diarrhoeal disease, and parasitic infection during infancy on cognition in late childhood: A follow‐up study. Lancet, 359(9306), 564–571. 10.1016/S0140-6736(02)07744-9 [DOI] [PubMed] [Google Scholar]
- Bhandari, N. , Mohan, S. B. , Bose, A. , Iyengar, S. D. , Taneja, S. , Mazumder, S. , … Bahl, R. (2016). Efficacy of three feeding regimens for home‐based management of children with uncomplicated severe acute malnutrition: A randomised trial in India. BMJ Global Health, 1(4), e000144 10.1136/bmjgh-2016-000144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhutta, Z. A. , Das, J. K. , Rizvi, A. , Gaffey, M. F. , Walker, N. , Horton, S. , … Black, R. E. (2013). Evidence‐based interventions for improvement of maternal and child nutrition: What can be done and at what cost? The Lancet, 382(9890), 452–477. 10.1016/S0140-6736(13)60996-4 [DOI] [PubMed] [Google Scholar]
- Black, R. E. , Allen, L. H. , Bhutta, Z. A. , Caulfield, L. E. , de Onis, M. , Ezzati, M. , … Rivera, J. (2008). Maternal and child undernutrition: Global and regional exposures and health consequences. The Lancet. 10.1016/S0140-6736(07)61690-0, 371, 243–260. [DOI] [PubMed] [Google Scholar]
- Blanárová, L. , Rogers, E. , Magen, C. , & Woodhead, S. (2016). Taking severe acute malnutrition treatment back to the community: Practical experiences from nutrition coverage surveys. Frontiers in Public Health 10.3389/fpubh.2016.00198, 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burtscher, D. , & Burza, S. (2015). Health‐seeking behaviour and community perceptions of childhood undernutrition and a community management of acute malnutrition (CMAM) programme in rural Bihar, India: A qualitative study. Public Health Nutrition 10.1017/S1368980015000440, 18, 3234–3243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burza, S. , Mahajan, R. , Marino, E. , Sunyoto, T. , Shandilya, C. , Tabrez, M. , … Mishra, K. N. (2015). Community‐based management of severe acute malnutrition in India: New evidence from Bihar. The American Journal of Clinical Nutrition, 101(4), 847–859. 10.3945/ajcn.114.093294 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chanani, S. , Wacksman, J. , Deshmukh, D. , Pantvaidya, S. , Fernandez, A. , & Jayaraman, A. (2016). M‐Health for improving screening accuracy of acute malnutrition in a Community‐Based Management of Acute Malnutrition program in Mumbai informal settlements. Food and Nutrition Bulletin, 37(4), 504–516. 10.1177/0379572116657241 [DOI] [PubMed] [Google Scholar]
- Collins, S. , Sadler, K. , Dent, N. , Khara, T. , Guerrero, S. , Myatt, M. , … Walsh, A. (2006). Key issues in the success of community‐based management of severe malnutrition. Food and Nutrition Bulletin, 27(SUPPL.3), S49–S82. 10.1177/15648265060273S304 [DOI] [PubMed] [Google Scholar]
- Dalwai, S. , Choudhury, P. , Bavdekar, S. B. , Dalal, R. , Kapil, U. , Dubey, A. , … Sachdev, H. (2013). Consensus statement of the Indian Academy of Pediatrics on integrated management of severe acute malnutrition. Indian Pediatrics, 50(4), 399–404. 10.1007/s13312-013-0111-3 [DOI] [PubMed] [Google Scholar]
- Dasgupta, R. , Sinha, D. , & Yumnam, V. (2014). Programmatic response to malnutrition in India: Room for more than one elephant? Indian Pediatrics, 51(11), 863–868. 10.1007/s13312-014-0518-5 [DOI] [PubMed] [Google Scholar]
- Dasgupta, R. , Yumnam, V. , & Ahuja, S. (2015). Making CMAM relevant in India: The letter and the spirit. American Journal of Clinical Nutrition. 10.3945/ajcn.115.116228, 102, 1297–1298. [DOI] [PubMed] [Google Scholar]
- Ezeh, A. , Oyebode, O. , Satterthwaite, D. , Chen, Y. , Ndugwa, R. , Sartori, J. , … Lilford, R. J. (2016). The history, geography, and sociology of slums and the health problems of people who live in slums. The Lancet, 6736(16), 1–12. 10.1016/S0140-6736(16)31650-6 [DOI] [PubMed] [Google Scholar]
- Gandhi, S. (2012). Economics of affordable housing in Indian cities: The case of Mumbai. Environment and Urbanization ASIA, 3(1), 221–235. 10.1177/097542531200300112 [DOI] [Google Scholar]
- Goudet, S. , Griffiths, P. , Bogin, B. , & Madise, N. (2017). Interventions to tackle malnutrition and its risk factors in children living in slums: A scoping review. Annals of Human Biology, 44(1), 1–10. 10.1080/03014460.2016.1205660 [DOI] [PubMed] [Google Scholar]
- Government of India Ministry of Health and Family Welfare . (2011). Operational guidelines on facility based management of children with severe acute malnutrition.
- Government of India. Ministry of Health and Family Welfare . (2014). Guidelines for ASHA and Mahila Arogya Samiti in the Urban Context. New Delhi. Retrieved from http://cghealth.nic.in/ehealth/2016/NUHMDOC/guidelines-for-mas-and-uasha.pdf
- Government of India. Ministry of Health and Family Welfare . (2017). National Health Policy. New Delhi. Retrieved from http://cdsco.nic.in/writereaddata/National-Health-Policy.pdf
- Grantham‐McGregor, S. , Cheung, Y. B. , Cueto, S. , Glewwe, P. , Richter, L. , & Strupp, B. (2007). Developmental potential in the first 5 years for children in developing countries. Lancet. 10.1016/S0140-6736(07)60032-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harding, K. L. , Aguayo, V. M. , & Webb, P. (2018). Factors associated with wasting among children under five years old in South Asia: Implications for action. PLoS One, 13(7), e0198749 10.1371/journal.pone.0198749 [DOI] [PMC free article] [PubMed] [Google Scholar]
- International Institute for Population Sciences (2016a). National Family Health Survey‐4 India Fact Sheet 2015‐2016. Retrieved January 1, 2017, from http://rchiips.org/NFHS/factsheet_NFHS-4.shtml
- International Institute for Population Sciences (2016b). National Family Health Survey‐4 Maharashtra State Fact Sheet 2015‐2016. Mumbai. Retrieved from http://rchiips.org/NFHS/factsheet_NFHS-4.shtml
- Kennedy, E. , Branca, F. , Webb, P. , Bhutta, Z. , & Brown, R. (2015). Setting the scene: An overview of issues related to policies and programs for moderate and severe acute malnutrition. Food and Nutrition Bulletin, 36(1_suppl1), S9–S14. 10.1177/15648265150361S102 [DOI] [PubMed] [Google Scholar]
- Kumar, S. , & Banerjee, S. (2015). Integrated Child Development Services (ICDS) programme in the context of urban poor and slum dwellers in India: Exploring challenges and opportunities. Indian Journal of Public Administration, 61(1), 94–113. 10.1177/0019556120150107 [DOI] [Google Scholar]
- Lokshin, M. , Das Gupta, M. , Gragnolati, M. , & Ivaschenko, O. (2005). Improving child nutrition? The integrated child development services in India. Development and Change, 36(4), 613–640. 10.1111/j.0012-155X.2005.00427.x [DOI] [Google Scholar]
- Moore, S. M. , & Charvat, J. (2007). Promoting health behavior change using appreciative inquiry: moving from deficit models to affirmation models of care. Family & Community Health, 30(1 Suppl), S64–S74. 10.1097/00003727-200701001-00009 [DOI] [PubMed] [Google Scholar]
- More, N. S. , Waingankar, A. , Ramani, S. , Chanani, S. , D'Souza, V. , Pantvaidya, S. , & Jayaraman, A. (2018). Community‐Based Management of Acute Malnutrition to reduce wasting in urban informal settlements of Mumbai, India: A mixed‐methods evaluation. Global Health: Science and Practice. (Forthcoming), Forthcoming [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naandi Foundation . (2014). Urban HUNGaMA (Hunger and Malnutrition) Survey (2014th ed.). Hyderabad. Retrieved from http://www.naandi.org/wp-content/uploads/Urban-HUNGAMA-Final-Report-1.pdf
- Park, S.‐E. , Kim, S. , Ouma, C. , Loha, M. , Wierzba, T. F. , & Beck, N. S. (2012). Community management of acute malnutrition in the developing world. Pediatric Gastroenterology, Hepatology & Nutrition, 15(4), 210–219. 10.5223/pghn.2012.15.4.210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Planning Commission, G. of I . (2011). Report of the Inter‐Ministerial Group on ICDS Restructuring. New Delhi. Retrieved from http://planningcommission.nic.in/reports/genrep/rep_icds2704.pdf
- Pörtner, C. C. , & Su, Y. (2018). Differences in child health across rural, urban, and slum areas: Evidence from India. Demography, 55(1), 223–247. 10.1007/s13524-017-0634-7 [DOI] [PubMed] [Google Scholar]
- Prasad, V. , & Sinha, D. (2015). Potentials, experiences and outcomes of a comprehensive community based programme to address malnutrition in tribal India. International Journal of Child Health and Nutrition, 4, 151–162. 10.6000/1929-4247.2015.04.03.4 [DOI] [Google Scholar]
- Pries, A. M. , Huffman, S. L. , Champeny, M. , Adhikary, I. , Benjamin, M. , Coly, A. N. , … Zehner, E. (2017). Consumption of commercially produced snack foods and sugar‐sweetened beverages during the complementary feeding period in four African and Asian urban contexts. Maternal & Child Nutrition, 13(Suppl 2). 10.1111/mcn.12412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Save the Children . (2015). Standardised indicators and categories for better CMAM reporting. London: Save the Children. [Google Scholar]
- Shah, N. , Jadhav, A. , Manglani, M. , Fernandes, L. , & Surve, A. (2015). Indigenous production of ready‐to‐use therapeutic food to address severe acute malnutrition in Indian children. International Journal of Scientific and Research Publication, 5, 287–294. [Google Scholar]
- Singh, K. , Badgaiyan, N. , Ranjan, A. , Dixit, H. O. , Kaushik, A. , Kushwaha, K. P. , & Aguayo, V. M. (2014). Management of children with severe acute malnutrition: Experience of nutrition rehabilitation centers in Uttar Pradesh, India. Indian Pediatrics, 51(1), 21–25. 10.1007/s13312-014-0328-9 [DOI] [PubMed] [Google Scholar]
- UNICEF/WHO/World Bank . (2016). Levels and trends in child malnutrition. UNICEF‐WHO‐World Bank Joint Child Malnutrition Estimates, 2016(accessed 12 October 2016), 1–8. 10.1016/S0266-6138(96)90067-4 [DOI]
- United Nations . (2014). World Urbanization Prospects: The 2014 Revision, Highlights (ST/ESA/SER.A/352). New York, United. 10.4054/DemRes.2005.12.9 [DOI]
- USAID . (2017). Community‐based management of acute malnutrition: Technical guidance brief. Retrieved from https://www.usaid.gov/sites/default/files/documents/1864/CMAM-technical-guidance-brief-508-revFeb2017.pdf
- World Health Organization . (2013a). Essential Nutrition Actions- Improving maternal, newborn, infant and young child health and nutrition. Geneva: WHO; https://doi.org/NBK258736 [bookaccession] [PubMed] [Google Scholar]
- World Health Organization (2013b). Guideline: Updates on the management of severe acute malnutrition in infants and children. Geneva: WHO; 10.1007/s13398-014-0173-7.2 [DOI] [PubMed] [Google Scholar]
- World Health Organization . (2016). The WHO Child Growth Standards. Retrieved from http://www.who.int/childgrowth/standards/en/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Key child nutrition program activities
Figure S2. Status of children admitted into the community‐based child nutrition program between May 2014 and April 2015‐three months post‐admission