

As of this writing, the growing coronavirus disease 2019 (COVID-19) pandemic has suspended international travel, has injected instability in global financial markets, and has led to widespread school and business closures. There are increased calls for social distancing, avoidance of unnecessary physical contacts/interactions, and even mandatory isolation in some countries. These restrictions are leading hospitals and healthcare systems to suspend elective procedures and limit staff interactions with patients to essential personnel only.
The currently reported overall case fatality rate of COVID-19 is 2.3% in the general population, and is higher (14.8%) in patients >80 years of age.1 Further, patients with COVID-19 requiring hospitalization suffer a number of cardiovascular complications including arrhythmias (16.7% of patients)2 and heart failure (23% of patients),3 raising the risk for acute ischemic stroke (AIS). Indeed, cerebrovascular complications have been reported in 5% to 6% of patients with severe COVID-19.4,5 In this context, emergent delivery of endovascular therapy (EVT) requires careful planning and deliberation with special attention to patient selection, resource utilization, and the safety of healthcare providers.
With the goal of minimizing the negative impact of COVID-19 on acute stroke patients and healthcare providers, we assembled a multidisciplinary working group to develop consensus-based recommendations and an algorithm for evaluation and treatment of acute stroke patients eligible for EVT during the COVID-19 pandemic. The role of intravenous thrombolysis is not addressed here because EVT presents unique challenges compared with intravenous drug administration.
Three populations of potential thrombectomy patients are highlighted: (1) emergency department (ED) patients with stroke and suspected COVID-19, (2) admitted patients with COVID-19 who develop stroke, and (3) patients with stroke who present to a hospital with constrained resources due to COVID-19. Recommendations are discussed and a clinical algorithm is proposed with anticipated decision points of care. This algorithm takes into account the American Heart Association/American Stroke Association (AHA/ASA) EVT guidelines, the safety of patients and staff, the predictors of mortality in patients with COVID-19, and the appropriate utilization of scarce resources.
Our working group concluded that diagnosis with COVID-19 is not necessarily a contraindication to EVT for stroke. However, particular care must be taken when preparing patients with COVID-19 for EVT to ensure staff safety. In addition, it may be reasonable during these times of extreme resource limitation to modify current EVT protocols including patient selection and post-EVT care, and to avoid EVT in unstable, severely critically ill patients with COVID-19.
Methods
Setting
Our Comprehensive Stroke Center is a large, urban, tertiary care academic medical center performing >200 thrombectomies a year. The center also serves as the only Level I Trauma Center in the region and as a safety net hospital for underserved persons in the community. In response to the pandemic, the ED established a respiratory ED with tents deployed outside the ED where patients with respiratory symptoms are evaluated separately from the general ED population, many in their private vehicles. For acute stroke, the principles of facilitated triage including direct-to-computed tomography (CT), emergent stroke team contact, and emergent initiation of EVT in eligible patients continue to be prioritized.
Process
As governmental and institutional responses to the pandemic escalated, we assembled a multidisciplinary team of providers to establish local processes for the care of EVT patients while minimizing the exposure of emergent stroke providers and staff to coronavirus.
The assembled team involved experts along the spectrum of care for this patient population, including Prehospital Emergency Medical Services (Drs Richards and Knight), Emergency Medicine (Drs Bonomo, Knight, Richards, and Adeoye), Radiology (Dr Vagal), Vascular Neurology (Drs Bonomo, Knight, Richards, Adeoye, Shirani, Khatri, Kleindorfer, Broderick, and Grossman), Neurointerventional Surgery (Drs Shirani, Prestigiacomo, and Grossman), Neurological Surgery (Dr Prestigiacomo), Anesthesiology (Dr Bertsch), Neurocritical Care (Drs Smith, Bonomo, Knight, and Adeoye), Pulmonary/Critical Care (Dr Ramser), Infectious Disease (Dr Fichtenbaum), and Medical Ethics (Drs Housholder and Bonomo). Meetings were conducted via remote video interaction. A preliminary proposal was developed by 2 of the co-authors (Drs Smith and Grossman) using the best available published data by performing Pubmed search between March 13 and 16 with the terms COVID-19 and China or Italy in conjunction with stroke, cerebrovascular disease, heart failure, symptom onset, mortality, and recovery. Due to the urgent nature of these recommendations we included non peer-reviewed sources sent to the authors via social media and email from our colleagues in the above listed specialties. Centers for Disease Control and Prevention (CDC) and World Health Organization guidance provided a framework for discussion. All co-authors contributed to the consensus-based recommendations and algorithm based on their area of expertise.
Results and Recommendations
Given that COVID-19 case fatality rates are currently near 2.3% and given the expectation that most patients with mild to moderate symptoms will recover,1 it is the consensus of our working group that diagnosis with COVID-19 does not represent an absolute contraindication to EVT for AIS. Upon further assessing the nuanced impact of COVID-19 on patient eligibility for EVT, 3 patient populations were highlighted: (1) ED patients with stroke and suspected or unknown exposure to COVID-19, (2) admitted patients with COVID-19 who develop stroke, and (3) patients with stroke who present to a hospital with constrained resources due to COVID-19.
Recommendations for ED Patients Presenting With Stroke and Suspected or Unknown Exposure to COVID-19
Screening
Descriptive studies from China indicate that the most common presenting symptoms of COVID-19 are fever (43% of patients),6 cough (59%–82% of patients), and dyspnea with respiratory rate >24 breaths per minute (29%–31% of patients).2,7,8 Up to 83% to 94% of patients experienced subjective fever/chills.7 In addition, some neurological symptoms, such as anosmia or ageusia, have been noted as presenting symptoms.9 We, therefore, recommend that, on arrival to the ED, vital signs of patients with symptoms of acute stroke be screened for fever >38 C and tachypnea. Using the CDC COVID-19 Case Report Form as a guide,10 acute stroke patients should be assessed for a history of subjective fever, chills, myalgias, rhinorrhea, sore throat, cough, shortness of breath, nausea/vomiting, headache, abdominal pain, or diarrhea within the past 7 days. Finally, patients should be asked for any exposure to anyone with known or suspected COVID-19 disease in the past 14 days. This screening process is outlined in Figure 1. One of the major challenges of patients with stroke, compared with other patients presenting to the ED, is that they may not be able to communicate due to aphasia or changes in the level of consciousness. Patients who cannot provide screening information should be assumed to potentially have COVID-19 and managed accordingly.
Figure 1.
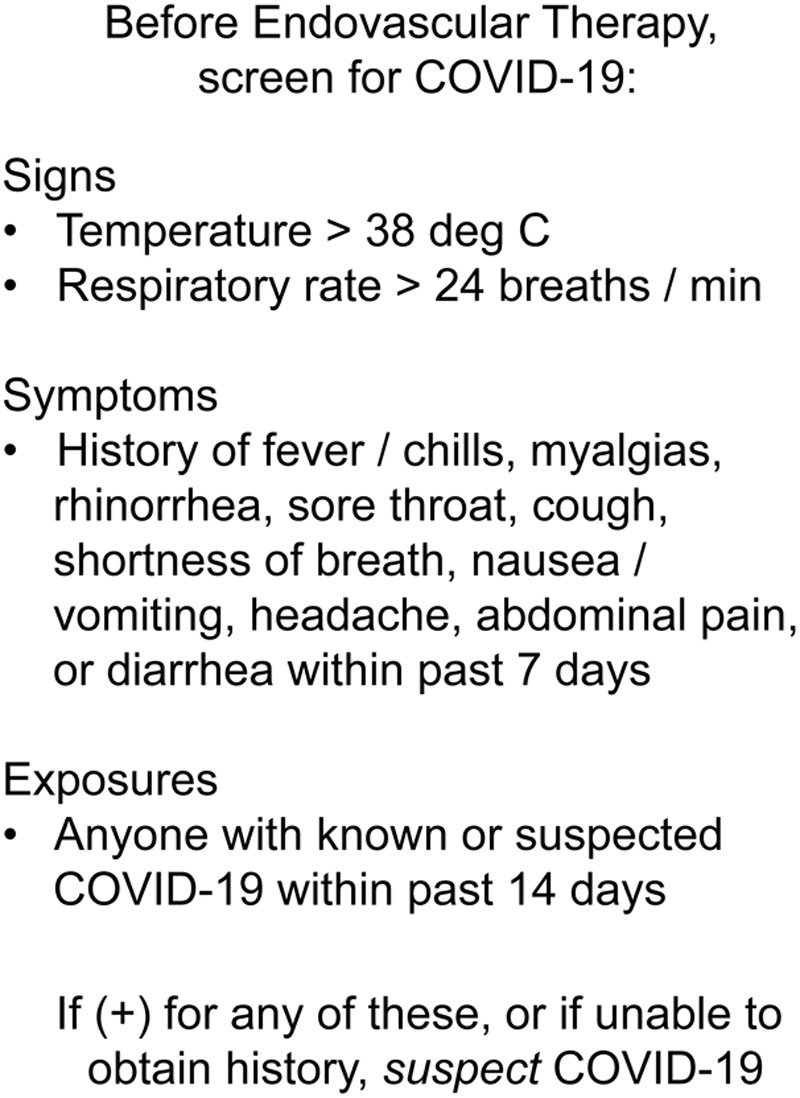
Recommendations for screening patients for coronavirus disease 2019 (COVID-19) before endovascular therapy (EVT), adapted from the Centers for Disease Control and Prevention (CDC’s) human infection with 2019 novel coronavirus person under investigation (PUI) and case report form.10
Anecdotally, there have been reports of patients with stroke who screen negative for COVID-19 ultimately being diagnosed as COVID positive based initially on findings in lung apices on their stroke CT angiogram. Although providers may be tempted to include a CT of the chest along with acute stroke imaging, the American College of Radiology does not currently recommend using chest CT as a screening tool or first line test for suspected COVID-19. The chest imaging findings are nonspecific and overlap with other infections such as influenza.11 It is also important to note that depending on the air exchange rate in the CT scanner room, the scanner may be temporarily unavailable for subsequent patients after imaging a patient under investigation or COVID positive patient. Radiology departments must have protocols and procedures in place for expedited decontamination based on CDC guidelines,12 or even (as in our ED) a dedicated scanner for persons under investigation (PUIs) and COVID positive patients.
Airway Management
If all of the above outlined screening conditions are confirmed to be negative (by patient or caregiver history), a patient with acute stroke may proceed for EVT according to local protocols. In light of the median 5 to 6 day incubation period during which a patient is infectious but may remain asymptomatic,13 we advise that even patients who screen negative should wear a surgical mask throughout the procedure.
Patients with any of these signs, symptoms or known exposures, or for whom data are unknown, should be treated as suspected of having COVID-19 (frequently termed a PUI) and should carefully be evaluated by a member of the stroke/neurointerventional team and an experienced airway specialist. The decision whether to intubate a suspected patient with COVID-19 for EVT must balance the patient’s need for airway protection, the risk to staff performing the intubation, the risk to interventional radiology (IR) staff managing an extubated patient who may require aerosol generating procedures, the current ventilator capacity of the hospital system, and the potential success of EVT. In this section, we elaborate on the nuances of these risks and ways to mitigate them.
With limited staff, positive pressure airflow rooms, and a potential shortage of N95 masks, IR suites may be ill-equipped to handle aerosolizing procedures such as intubation/extubation, high flow nasal cannula, or suctioning in patients with suspected or confirmed COVID-19. For this reason, we recommend that patients with suspected or confirmed COVID-19 who require intubation undergo elective endotracheal intubation in a negative airflow room by an experienced airway specialist using local institutional precautions and backed by CDC Guidelines for infection control12 before arrival to the IR suite. Unless the need for a secure airway is emergent, intubation should occur after a patient receives acute stroke imaging and is deemed to be a candidate for EVT to avoid unnecessary use of resources. While preprocedural intubation will delay door-to-groin time compared with conscious sedation, retrospective studies are conflicting as to whether this translates into worse functional outcomes.14,15 As the AHA recommends, “it is reasonable to select an anesthetic technique during EVT for AIS on the basis of individualized assessment of patient risk factors, technical performance of the procedure, and other clinical characteristics.”16 To mitigate potential worsening of stroke symptoms due to hypotension, we recommend using an intubation strategy that preserves cerebral perfusion pressure using either etomidate or ketamine,17 with near continuous monitoring of blood pressure. If hypotension does occur, we recommend early use of sympathomimetics and a fluid-conservative resuscitation strategy in accordance with Critical Care Medicine COVID-19 Surviving Sepsis Guidelines.18 Preoxygenation, apneic oxygenation during intubation, avoidance of bag mask ventilation, rapid sequence intubation facilitated by neuromuscular blockade, and use of video laryngoscopy are also recommended to further limit exposure to secretions and optimize first pass success rate.
Once electively intubated, we recommend patient transport to the IR suite using transport ventilators with exhaust port viral/bacterial filters. The patient should remain on the transport ventilator for the duration of the procedure to avoid breaking the ventilator circuit while outside of a negative pressure room. If transport ventilators are unavailable, bag valve manual ventilation may be used with 2 viral filters (one between the ET tube and bag, and another between the bag and PEEP valve). Upon arrival to the IR suite, the endotracheal tube should be clamped with forceps on expiration before being placed on a ventilator or anesthesia machine that has appropriate exhaust port viral filters. If inline ET tube suctioning is to be performed, we again recommend a viral filter on the suctioning exhaust. Consumable ventilator and bag valve mask equipment ought to be preserved for use again postprocedure in management of that patient. Train-of-four monitoring should be considered during the procedure to facilitate optimal paralysis and prevent coughing or aerosolization. Before leaving the IR suite, the patient’s ET tube should again be clamped before being transferred onto an exhaust filtered transport ventilator or manual ventilation with 2 viral filters. Once admitted to the ICU, neuromuscular blockade should be reversed and the patient should be extubated as soon as deemed safe to minimize use of scarce resources.
Optimally, all providers caring for patients with suspected COVID-19 would be provided with N95 masks or equivalent respirators. However, if N95 masks are limited, by following the above precautions and minimizing aerosolizing procedures in the IR suite, EVT for intubated patients can continue with nonsterile staff using modified CDC-recommended personal protective equipment (PPE) for COVID-19 which consists of handwashing, surgical mask, hair covering, eye protection, nonsterile contact gown and gloves.12 N95 masks are not superior to standard face masks for preventing spread of severe acute respiratory syndrome, influenza-like illness or other respiratory viral infections during routine patient care19 and should be reserved for personnel performing aerosolizing procedures if supplies are limited. Sterile operators should continue to follow sterile technique with handwashing, surgical mask and cap, eye protection, and sterile gown/gloves. Following the procedure, all staff should remove their PPE in the presence of a trained observer to limit accidental contamination.20
For patients with suspected or confirmed COVID-19 infection who do not require intubation before the procedure, we recommend using the contact and droplet precautions outlined above, with the addition of placing a surgical mask over the patient to be worn at all times. PPE for staff, including N95 masks or other respirators for airborne precautions should be immediately available in the IR suite. If supplies are limited, however, they should only be used if a patient unexpectedly develops a need for aerosolizing procedures during EVT (high flow nasal cannula, nebulizer treatment, suctioning, or intubation). The above recommendations are summarized in Figure 2.
Figure 2.
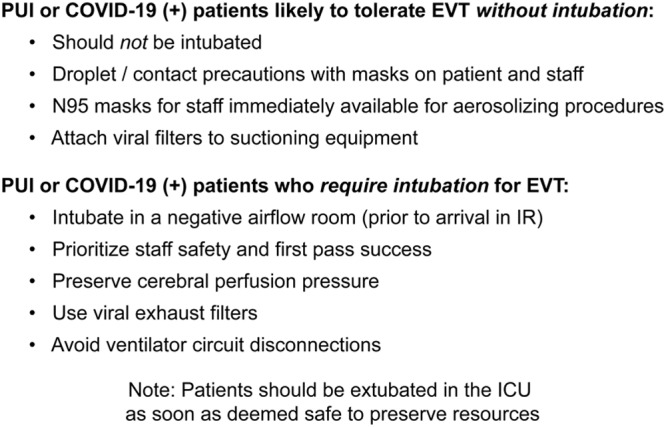
Recommendations for airway management in patients with suspected or confirmed coronavirus disease 2019 (COVID-19) undergoing endovascular therapy (EVT). IR indicates interventional radiology; and PUI, person under investigation.
Recommendations for Patients Admitted With COVID-19 Who Develop Stroke
With the high number of cardiovascular complications found in patients admitted to ICUs for COVID-19 including arrhythmias (16.7% of patients)2 and heart failure (23% of patients),3 we may anticipate a higher than usual rate of inpatient strokes in this new patient population.4 We summarize recommendations for the evaluation and management of these patients in Figure 3. Specifically, we recommend that patients who are admitted to the standard floor (medical/surgical) level of care with confirmed or suspected infection undergo a baseline neurological assessment in addition to their routine nursing and vital sign assessments. Treating physicians should be aware of the increased risk of neurological complications and monitor for these changes. To minimize the duration of nurse/patient encounters, we suggest the rapidly administered Cincinnati Prehospital Stroke Scale which consists of asking a patient to (1) smile, assessing for facial drop; (2) hold both arms up for 10 seconds, assessing for weakness; and (3) repeat a simple phrase, assessing for language dysfunction. The Cincinnati Prehospital Stroke Scale has 81% sensitivity for stroke detection.21 A positive screen should trigger activation of a provider experienced in evaluating stroke patients and, if AIS is strongly suspected, a stat CT head and CT angiogram of the head and neck should be obtained concurrently. Given the risk to staff of transporting a COVID+ patient to the CT scanner, in-person or telemedicine screening by an experienced provider before imaging may be a net benefit despite any delay in care it may impose. Patients should wear a surgical mask at all times and staff in the IR suite should use PPE as described above to avoid exposure. After CT and CT angiogram are performed, IV thrombolytic therapy can be started as appropriate and EVT algorithm can be initiated as above for patients with large vessel occlusions. If a patient is deemed a candidate for EVT, we again recommend careful risk-assessment with respect to airway management by a member of the stroke/neurointerventional team and an experienced airway specialist, as outlined above and in Figure 2.
Figure 3.
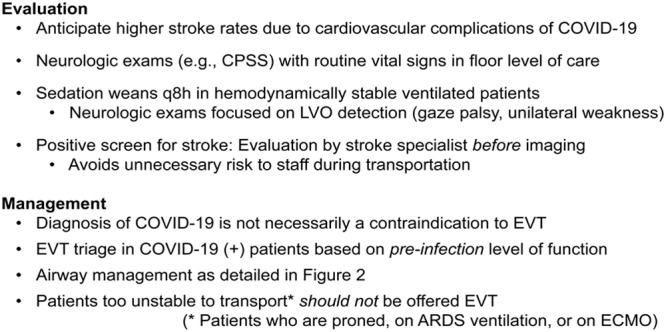
Recommendations for evaluation and management of coronavirus disease 2019 (COVID-19) positive patients who develop stroke. ARDS indicates acute respiratory distress syndrome; CPSS, Cincinnati Prehospital Stroke Scale; ECMO, extracorporeal membrane oxygenation; EVT, endovascular therapy; and LVO, large vessel occlusion.
In hemodynamically stable patients undergoing routine mechanical ventilation, we recommend weaning of sedation every 8 hours to assess for sensitive signs of large vessel occlusion (gaze deviation and focal weakness as determined in these patients by applying bilateral nail bed pressure).22 Again, a positive screen should trigger activation of stroke pathways and evaluation before imaging to minimize infection risk to staff. In these patients, CT perfusion is likely to be indicated for consideration of extended window thrombectomy at >6 hours from last known well (given q8h evaluations). We recommend that consideration for EVT be based on the patient’s preinfection level of functioning rather than their current infected functional status.
In more critically ill patients with COVID-19, the decision is more challenging whether to intervene or even to investigate with imaging when stroke is suspected. A diagnosis of acute respiratory distress syndrome within Chinese cohorts was associated with 50% to 90% in-hospital mortality.8,23 Similarly, whereas extracorporeal membrane oxygenation remains an option for treating critically ill patients with COVID-19, a large retrospective study from China including >1000 hospitalized patients reports only 5 patients who received extracorporeal membrane oxygenation, none of whom survived to hospital discharge.6 As always, patient decisions must remain individualized, but with such high mortality, it is ethically permissible to forego EVT for most of these patients, as the exposure risk from transporting them to the CT scanner and then IR suite for EVT is unlikely to change their ultimate outcome. The ethical principle of distributive justice requires that scarce medical resources be allocated in ways that are both equitable and appropriate. The increased risks to staff and other patients are inequitable, and the low chance of success may make the procedure inappropriate in times of increased scarcity.
In general practice, patients undergoing prone positioning, requiring neuromuscular blockade, or other advanced ventilator management strategies for acute respiratory distress syndrome are often too critically ill to transport for procedures outside of the ICU. Similarly, the technical limitations of transporting a patient on extracorporeal membrane oxygenation to the CT scanner and then the IR suite in a timely manner are likely to preclude effective reperfusion therapy. Therefore, we recommend that most COVID-19 patients in whom these therapeutic strategies are employed not be considered for EVT. As more knowledge emerges about outcome predictors in critically ill patients with COVID-19, we may be able to better triage those critically ill patients whose suspected strokes should be investigated and intervened upon.
Recommendations for Patients Who Develop Stroke and Present to a Hospital Whose Resources Are Constrained by Patients With COVID-19
This third patient group highlights the scenario in which a healthcare system may be too overwhelmed to consider performing thrombectomies, even for patients not suspected of having COVID-19. Several stroke centers in Italy have been moved or even closed to assist patients with serious infectious and respiratory problems.24 Until and unless this occurs, current local protocols for management of patients with AIS should remain in effect. To help systems mitigate overload and avoid this scenario, we provide 4 recommendations (Figure 4).
Figure 4.
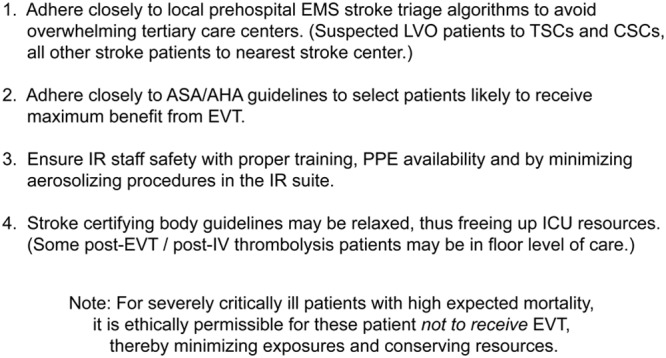
Recommendations to mitigate overload in stroke systems of care during the coronavirus disease 2019 (COVID-19) pandemic. AHA indicates American Heart Association; ASA, American Stroke Association; CSC, comprehensive stroke center; EVT, endovascular therapy; IR, interventional radiology; LVO, large vessel occlusion; PPE, personal protective equipment; and TSC, thrombectomy-ready stroke center.
First, prehospital systems of care should include prehospital stroke severity screening by emergency medical services providers, with patients screening positive for severe stroke transported preferentially to a more distant Comprehensive Stroke Center or thrombectomy-capable stroke center. Patients with suspected stroke, but without abnormal stroke severity screening (and therefore unlikely to receive EVT), should be transported to the closest stroke center. Improving the availability of advanced imaging including magnetic resonance and CT perfusion can help triage patients who may not require transfer to higher levels of care. These strategies can help mitigate capacity concerns at Comprehensive Stroke Centers and thrombectomy-capable stroke centers while helping to ensure timely and appropriate stroke care.
Our second recommendation pertains to careful selection of EVT candidates. Over the past 5 years, there has been a trend toward patient-specific expansion of indications for EVT to a broader population who do not meet definitive (Class I, Level of Evidence A) AHA/ASA guidelines, that is, patients with modified Rankin Scale score >2, Alberta Stroke Program Early CT Score <6, distal M2 occlusions, and larger ischemic cores. While current and future research will likely lead to the expansion of indications for EVT, during the current pandemic it may be reasonable to reserve EVT for patients in whom the largest benefit can be obtained according to AHA/ASA guidelines as hospital resources become scarce. In all cases, decisions must remain patient-specific and will need to reflect the local institutional processes, decision-making, and available resources at a given point in time.
Third, every effort must be made to protect the physicians, nurses and technicians working within the IR suite (and throughout the hospital) from high-risk exposure to COVID-19. All patients should be masked, and those with limited medical history or testing should be assumed to be COVID-19 suspects. With this vigilant stance, by ensuring proper training and PPE availability, and by minimizing aerosolizing procedures in the IR suite, we can help ensure staff safety and increase the likelihood that these highly trained teams remain operational.
Finally, as ICU beds are increasingly occupied with patients with COVID-19, the stroke center accreditation body guidelines for the care of post-EVT and post-thrombolysis patients should be reassessed. For a limited time during the pandemic it may be reasonable to admit these patients to floor level of care following uncomplicated procedures with excellent reperfusion on imaging, to forgo q1h neurological exams after the initial 2 hours, and to relax other post-EVT measures to free resources for more critically ill populations.
Discussion: Ethical Perspective
In routine clinical care within developed healthcare systems, medical ethics is patient-centered. Resources are allocated to patients with greatest need, with an expectation that there will be sufficient resources available for all patients. Rationing of truly scarce resources, such as transplantable organs, have well-established procedures to ensure fair distribution. In typical circumstances, resources to pursue EVT are not particularly scarce and, therefore, decisions ethically adhere to well-established guidelines and the preferences and values of the individual patient. During a public health emergency, such as the current COVID-19 pandemic, EVT may become an intervention that must ethically be considered in competition with other uses of scarce medical resources. During such crises, health care leaders have additional ethical duties to balance the needs of individuals with the needs of the community. Berlinger et al25 recently identified 4 core ethical duties that should guide health care leaders during this public health emergency: the duties to care, to plan, to safeguard and to guide.
The duty to care that underlies patient-centered ethics is never abandoned; however, the duty to protect the community may take on greater significance for determining which medical treatments are prioritized. As the risks to the community increase, the resources that would ordinarily be allocated to intensive procedures such as EVT may be ethically redirected towards other higher need activities within the community. In times of public health emergencies, health care leaders have additional ethical duties, which these proposed EVT recommendations seek to address.
The duty to plan requires health care leaders to identify foreseeable ethical challenges before they occur. Managing uncertainty preemptively may help decrease anxiety and moral distress among all members of the care team.
The duty to safeguard requires health care leaders to protect and support all members of the care team and vulnerable populations. This EVT guidance makes specific recommendations for the timing and location of high-risk procedures, such as intubation, to decrease risk to health care workers and other patients.
The duty to guide identifies that public health emergencies will evolve over time such that guidance will be needed throughout the emergency. Within the duty to guide, Berlinger et al25 identify both contingency levels of care and crisis standards of care. These recommendations include contingency planning such that as resources change there will be increasingly stringent allocation of scarce resources, including EVT. These recommendations are offered within an ethical framework that difficult decisions will be made by health care leaders. Preemptive considerations of how and to whom to offer EVT that balance the needs and risk of all patients, the community and the care team will allow for ethically sound decisions to be in place as the current public health emergency escalates.
Conclusions
Our multidisciplinary working group recommends that the majority of patients with suspected or confirmed COVID-19 suffering from AIS with large vessel occlusions should be considered for EVT based on preinfection level of functioning and in accordance with 2019 AHA/ASA guidelines. A simplified decision algorithm is available in Figure 5. Due to limitations imposed by positive pressure in most IR suites and by the limited supply of PPE, individuals with confirmed, suspected, or unknown status of COVID-19 who require general anesthesia for the procedure should undergo elective endotracheal intubation after confirmation of large vessel occlusion but before arrival in the IR suite to minimize risk of viral spread. Patients who do not require general anesthesia should proceed to the IR suite with a surgical mask in place and with standard contact/droplet precautions, but with N95 masks immediately available should the need for aerosolizing procedures arise. Due to high rates of cardiovascular complications with potentially higher than expected stroke risk, patients admitted with confirmed or suspected COVID-19 should be monitored for neurological changes and q8h sedation weans should be performed for mechanically ventilated patients when possible. Patients with suspected stroke should be evaluated by experienced providers before imaging, to minimize infectious risk during transportation. It is reasonable to withhold EVT from most patients with COVID-19 undergoing advanced ventilator management for acute respiratory distress syndrome or extracorporeal membrane oxygenation due to high mortality. To preserve hospital resources during this crisis, patient populations most likely to benefit from thrombectomy, as outlined in AHA/ASA guidelines, should be prioritized for EVT. For a limited time, many of these patients may be admitted to a floor level of care postprocedure to preserve ICU capacity for more critically ill patients.
Figure 5.
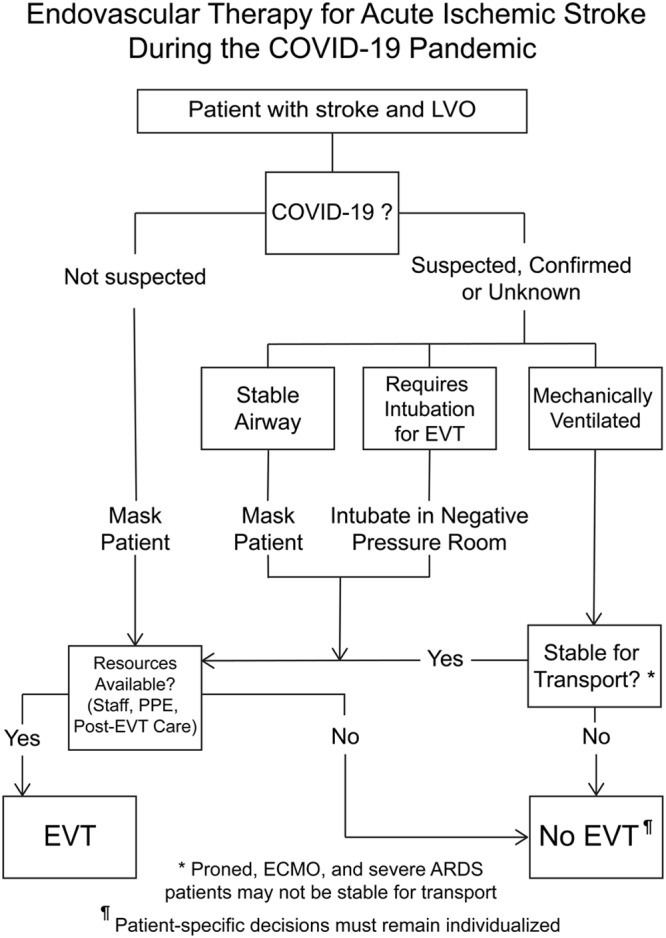
A proposed algorithm for endovascular therapy in acute ischemic stroke during the coronavirus disease 2019 (COVID-19) pandemic. ARDS indicates acute respiratory distress syndrome; ECMO, extra corporeal membrane oxygenation; EVT, endovascular therapy; LVO, large vessel occlusion; and PPE, personal protective equipment.
These recommendations from our institution are intended as a guide to decision-making regarding EVT therapy during the COVID-19 pandemic. In developing their own process, each institution must respond to specific institutional challenges, including availability of resources and staff, which may dramatically change over a short time period. Adapting an existing and evolving workflow requires input, coordination, and engagement across hospital units and disciplines, and we think a multidisciplinary approach that is proactive rather than reactionary will best serve patients with AIS during the COVID-19 pandemic.
Author’s Note
After submission of this article, several professional societies have come forth with recommendations regarding specific aspects of care in the management of patients with AIS requiring EVT during the COVID pandemic. The guidance of these societies is generally consistent with the multidisciplinary recommendations and algorithm proposed above and is referenced here for the benefit of readers.26–28
Acknowledgments
We appreciate the many healthcare providers at our institution and across the world who have shared insights and best practices in the published literature and online in real-time during the fight against coronavirus disease 2019 (COVID-19). Most of them, colleagues and friends, will place themselves in harm’s way, and we are grateful for their sacrifice.
Disclosures
Dr Bonomo reports Genentech—Speaker’s Bureau; Portola—Speaker’s Bureau. Dr Knight IV reports Genentech—Speaker’s Bureau; BD, Inc—Speaker’s Bureau. Dr Prestigiacomo reports consulting work with Stryker, Aesculap, and Cerenovus; member of the Board of the International Brain Research Foundation. Dr Richards reports travel reimbursement from the American Heart Association, from the Illinois EMT Association, and from ACEP; grants from AHRQ, all outside the submitted work. Dr Adeoye reports research grants from the National Institutes of Health (NIH)/National Institute of Neurological Disorders and Stroke (NINDS); Founder, Equity and Patent Holder, Sense Diagnostics, Inc. Dr Vagal reports research grants from NIH and American College of Radiology; Imaging Core Lab, Cerenovus. Dr Fichtenbaum reports Gilead Sciences,ViiV Healthcare, Janssen Inc, Kowa Pharmaceuticals America, Amgen, Merck Inc, Clinical Care Options Speaker’s Bureau, Abbvie Inc. Research Grants from Cytodyn, NIH/NIAID and NHLBI. Dr Housholder reports Clinical Trials Investigator for Leo Pharma, Acetelion and US World Meds; employed at Cincinnati Veterans Administration Medical Center. Dr Khatri reports Department has received funds for her research efforts from Cerenovus (grant MPI), Nervive (grant CoI), Lumosa (consultant, DSMB), and Bayer (National PI). Dr Broderick reports consulting work with Genentech, Dr Grossman reports Genentech—Speakers Bureau. The other authors report no conflicts.
Footnotes
Guest Editor for this article was Emmanuel Touzé, PhD.
References
- 1.Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323:1239–1242. doi: 10.1001/jama.2020.2648. doi: 10.1001/jama.2020.2648. [DOI] [PubMed] [Google Scholar]
- 2.Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323:1061–1069. doi: 10.1001/jama.2020.1585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China [published online March 3, 2020]. Intensive Care Med. doi: 10.1007/s00134-020-05991-x. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7080116/pdf/134_2020_Article_5991.pdf. doi: 10.1007/s00134-020-05991-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mao L, Wang M, Chen S, He Q, Chang J, Hong C, et al. Neurological manifestations of hospitalized patients with COVID-19 in Wuhan, China: a retrospective case series study [published online February 25, 2020]. MedRxiv. https://jamanetwork.com/journals/jamaneurology/fullarticle/2764549. doi: 10.1101/2020.02.22.20026500. [Google Scholar]
- 5.Li Y, Wang M, Zhou Y, Chang J, Xian Y, Mao L, et al. Acute cerebrovascular disease following COVID-19: a single center, retrospective, observational study [published online March 13, 2020]. Lancet. doi: 10.1136/svn-2020-000431. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3550025. doi: 10.2139/ssrn.3550025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Guan WJ, Ni ZY, Hu Y, Lian WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China [published online February 28, 2020]. N Engl J Med. doi: 10.1056/NEJMoa2002032. https://www.nejm.org/doi/pdf/10.1056/NEJMoa2002032. doi: 10.1056/NEJMoa2002032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395:507–513. doi: 10.1016/S0140-6736(20)30211-7. doi: 10.1016/S0140-6736(20)30211-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–1062. doi: 10.1016/S0140-6736(20)30566-3. doi: 10.1016/S0140-6736(20)30566-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Giacomelli A, Pezzati L, Conti F, Bernacchia D, Siano M, Oreni L, et al. Self-reported olfactory and taste disorders in SARS-CoV-2 patients: a cross-sectional study [published online March 26, 2020]. Clin Infect Dis. doi: 10.1093/cid/ciaa330. https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa330/5811989. doi: 10.1093/cid/ciaa330/5811989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Human infection with 2019 novel coronavirus person under investigation (PUI) and case report form. Center for Disease Control. https://www.cdc.gov/coronavirus/2019-ncov/downloads/pui-form.pdf. Accessed April 1, 2020.
- 11.ACR recommendations for the use of chest radiography and computed tomography (CT) for suspected COVID-19 infections. American College of Radiology Position Statements. https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recommendations-for-Chest-Radiography-and-CT-for-Suspected-COVID19-Infection. Accessed March 17, 2020.
- 12.Interim infection prevention and control recommendations for patients with suspected or confirmed coronavirus disease 2019 (COVID-19) in healthcare settings. Center for Disease Control. https://www.cdc.gov/coronavirus/2019-ncov/infection-control/control-recommendations.html. Accessed April 1, 2020.
- 13.Lauer SA, Grantz KH, Bi Q, Jones FK, Zhen Q, Meredith HR, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application [published online March 10, 2020]. Ann Intern Med. doi: 10.7326/M20-0504. https://annals.org/aim/fullarticle/2762808/incubation-period-coronavirus-disease-2019-covid-19-from-publicly-reported. doi: 10.7326/M20-0504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Vukasinovic I, Darcourt J, Guenego A, Michelozzi C, Januel AC, Bonneville F, et al. Toulouse Stroke Group. “Real life” impact of anesthesia strategy for mechanical thrombectomy on the delay, recanalization and outcome in acute ischemic stroke patients. J Neuroradiol. 2019;46:238–242. doi: 10.1016/j.neurad.2018.09.005. doi: 10.1016/j.neurad.2018.09.005. [DOI] [PubMed] [Google Scholar]
- 15.Powers CJ, Dornbos D, 3rd, Mlynash M, Gulati D, Torbey M, Nimjee SM, et al. Thrombectomy with conscious sedation compared with general anesthesia: a DEFUSE 3 analysis. AJNR Am J Neuroradiol. 2019;40:1001–1005. doi: 10.3174/ajnr.A6059. doi: 10.3174/ajnr.A6059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:e344–e418. doi: 10.1161/STR.0000000000000211. doi: 10.1161/STR.0000000000000211. [DOI] [PubMed] [Google Scholar]
- 17.Jabre P, Combes X, Lapostolle F, Dhaouadi M, Ricard-Hibon A, Vivien B, et al. KETASED Collaborative Study Group. Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial. Lancet. 2009;374:293–300. doi: 10.1016/S0140-6736(09)60949-1. doi: 10.1016/S0140-6736(09)60949-1. [DOI] [PubMed] [Google Scholar]
- 18.Alhazzani W, Moller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving sepsis campaign: Guidelines on the management of critically ill adults with coronavirus disease 2019 (COVID-19) [published online March 28, 2020]. Crit Care Med. doi: 10.1097/CCM.0000000000004363. https://www.sccm.org/getattachment/Disaster/SSC-COVID19-Critical-Care-Guidelines.pdf. doi: 10.1007/s00134-020-06022-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Offeddu V, Yung CF, Low MSF, Tam CC. Effectiveness of masks and respirators against respiratory infections in healthcare workers: a systematic review and meta-analysis. Clin Infect Dis. 2017;65:1934–1942. doi: 10.1093/cid/cix681. doi: 10.1093/cid/cix681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Grandbastien B, Parneix P, Berthelot P French High Council for Public Health; French Society for Hospital Hygiene. Putting on and removing personal protective equipment. N Engl J Med. 2015;372:2464. doi: 10.1056/NEJMc1504851. doi: 10.1056/NEJMc1504851. [DOI] [PubMed] [Google Scholar]
- 21.Maddali A, Razack FA, Cattamanchi S, Ramakrishnan TV. Validation of the cincinnati prehospital stroke scale. J Emerg Trauma Shock. 2018;11:111–114. doi: 10.4103/JETS.JETS_8_17. doi: 10.4103/JETS.JETS_8_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Beume LA, Hieber M, Kaller CP, Nitschke K, Bardutzky J, Urbach H, et al. Large vessel occlusion in acute stroke. Stroke. 2018;49:2323–2329. doi: 10.1161/STROKEAHA.118.022253. doi: 10.1161/STROKEAHA.118.022253. [DOI] [PubMed] [Google Scholar]
- 23.Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China [published online March 13, 2020]. JAMA Intern Med. doi: 10.1001/jamainternmed.2020.0994. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2763184. doi: 10.1001/jamainternmed.2020.0994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Stroke care during the COVID-19 pandemic. European Stroke Organization. https://eso-stroke.org/eso/stroke-care-during-covid-19-pandemic/. Accessed March 18, 2020.
- 25.Berlinger N, Wynia M, Powell T, Hester M, Milliken A, Fabi R, et al. Ethical framework for health care institutions responding to novel coronavirus SARS-CoV-2 (COVID-19) [published online March 16, 2020]. The Hastings Center. https://www.thehastingscenter.org/ethicalframeworkcovid19/. [Google Scholar]
- 26.Fraser JF, Arthur A, Chen M, Levitt M, Mocco J, Albuquerque F, et al. Society of neuroInterventional surgery recommendations for the care of emergent neurointerventional patients in the setting of COVID-19 [published online April 15, 2020]. J Neurointerv Surg. doi: 10.1136/neurintsurg-2020-016098. https://jnis.bmj.com/content/early/2020/04/15/neurintsurg-2020-016098.long. doi: 10.1136/neurintsurg-2020-016098. [DOI] [PubMed] [Google Scholar]
- 27.Sharma D, Rasmussen M, Han R, Whalin M, Davis M, Kofke A, et al. Anesthetic management of endovascular treatment of acute ischemic stroke during COVID-19 pandemic: consensus statement from Society for Neuroscience in Anesthesiology & Critical Care (SNACC) [published online April 8, 2020]. J Neurosurg Anesthesiol. doi: 10.1097/ANA.0000000000000688. https://journals.lww.com/jnsa/Abstract/9000/Anesthetic_Management_of_Endovascular_Treatment_of.99076.aspx. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lyden P AHA/ASA Stroke Council Leadership. Temporary emergency guidance to US stroke centers during the COVID-19 pandemic [published online April 1, 2020]. Stroke. https://www.ahajournals.org/doi/pdf/10.1161/STROKEAHA.120.030023. doi: 10.1161/STROKEAHA.120.030023. [Google Scholar]