

Background:
The Functional Movement Screen (FMSTM) is a nonspecific movement pattern assessment while the Landing Error Scoring System (LESS) is a screen for movement patterns associated with lower extremity injury. The purpose of this study was to determine if the LESS and FMSTM are correlated or if they can be used as complementary assessments of preseason injury risk for anterior cruciate ligament injury.
Methods:
FMSTM and LESS were used to conduct a cohort study of 126 male National Collegiate Athletic Association Division IA football players. One hundred and eleven players met the criteria for inclusion during data review. At risk and not at risk LESS scores of players and FMSTM exercise score status were compared using Welch’s t-test. Associations between FMSTM composites and LESS scores were evaluated using linear regression.
Results:
The average LESS score was 5.51±1.34, and the average composite FMSTM score was 11.77±2.13 (max=15). A poor FMSTM squat score (≤1 or asymmetry present) was associated with a higher LESS score (P<0.001). No other FMSTM individual exercise score was associated with an at-risk LESS score (P>0.05). Composite FMSTM score was loosely associated with the LESS score (R-squared=0.0677, P=0.006). Prior history of an ACL injury and player position were not associated with LESS score on multivariate regression (P>0.05).
Conclusions:
The LESS and FMSTM are not well correlated and may serve as complementary assessments for preseason injury risk.
Level of Evidence:
Level III.
Key Words: screening, injury prevention, FMS, LESS, ACL
INTRODUCTION
Anterior cruciate ligament (ACL) injuries frequently occur both by contact and noncontact mechanisms during cutting, jumping, and pivoting sports.1 ACL injuries lead to significant surgical expense and time away from play.2 Furthermore, ACL injury is associated with a long-term increased risk of knee osteoarthritis.3 Data from the National Football League (NFL) Combine show that 7.8% of participants had a history of ACL tear.4 An analysis of the National Collegiate Athletic Association (NCAA) Injury Surveillance System reported an ACL-injury rate of 8.06 per 10,000 football athlete-exposures during competition.5 Given the costs and incidence of ACL injury, there is considerable interest in identifying at-risk athletes.
The Functional Movement Screen (FMSTM; Functional Movement Systems, Inc., Virginia) is a fundamental movement pattern screening tool commonly used as an approach to assist with injury prevention and performance prediction.6–8 Several studies have found the FMSTM to be both repeatable and reproducible among minimally trained and highly trained raters, with intraclass correlation (ICC) values as high as 0.98, although this varied by individual FMS task.9–13 A low FMS score has been associated with an increased risk of nonspecific athletic injury across a number of high-level competitive sports.8,14–16 In studies of professional American football players, Kiesel et al. reported that a preseason FMSTM score less than 14 or at least one asymmetry were associated with increased likelihood of serious injury, defined as an injury reserve status and time loss of 3 wk during the season.16,17
The Landing Error Scoring System (LESS) is a clinical assessment tool used to identify athletes at risk for ACL tear and has been validated by three-dimensional lower extremity kinematic and kinetic analysis.18,19 The LESS has been found to have strong intrarater and interrater reliability even between expert and novice raters, with an ICC from 0.72 to 0.84.2,18 A number of studies have used the LESS as a tool to assess improvement in movement patterns associated with injury-prevention training programs.7,20
The LESS and FMSTM are screening tools used to identify high-risk movement patterns. Effective injury prevention requires identification of modifiable risk factors.18,21 Strength and conditioning programs are increasingly using the FMSTM as an injury risk screening tool16 and it is commonly used in NCAA football programs. While the FMSTM has been shown to assess general sports-related injury risk, there is currently no evidence that it can be used to screen for specific injury risks. Identification of specific injury risks allows targeted injury risk reduction intervention. The LESS has been validated for screening of movement patterns related to ACL injury. Our institution previously used only the FMSTM as an injury screen and previously piloted LESS testing for one season. We hypothesized that the LESS would be a useful supplement to the FMSTM to screen for risky movement patterns associated with ACL injury in NCAA Division I football athletes.
MATERIALS AND METHODS
Ethical Review and Study Design
Institutional Review Board approval (approval no. 33510) was obtained for a retrospective review of all football athletes undergoing LESS and FMSTM testing from August, 2013 to June, 2014. Informed consent was obtained from all participants prior to testing.
Participant Inclusion
One hundred and twenty six NCAA Division IA football athletes at a single institution underwent a combination of LESS and FMSTM testing. Subjects were subsequently excluded if either FMS or LESS testing was not performed due to any reason or if video files from the LESS testing were missing or corrupt. No post-hoc power analysis was performed as all eligible players’ data were included in the study.
Data Collected
Given the logistical and coaching demands of high-level competitive athletics, a cohort study following players throughout the season was performed. The following variables were collected: average subject LESS score across raters, modified FMSTM score, FMSTM squat score, FMSTM hurdle-step score, FMSTM in-line lunge score, FMSTM leg raise score, FMSTM trunk stability score, player position, LESS testing date, and prior subject history of ACL injury. Although there is no exact definition, player position was categorized as “skill” (wide receiver, running back, quarterback, kicker, punter, defensive back) or “strength” (lineman, linebacker, tight end) for purposes of this analysis. The modified FMSTM score did not include FMSTM shoulder mobility score and FMSTM push-up score because these do not involve the lower extremities and have not been shown to affect lower extremity biomechanics. Therefore, the modified FMSTM score had a maximum of 15 points. An individual exercise FMSTM score was considered “poor” if the score was less than 1 or if an asymmetry was present. A score was otherwise considered “acceptable.” LESS scores were averaged over three trials and across all three raters and had a maximum of 17 points. A higher LESS score indicated more errors in landing pattern.
FMSTM Protocol
The FMSTM composed of seven tasks used to assess overall functional movement: deep squat, hurdle step, in-line lunge, shoulder mobility, active straight leg raise, trunk stability-pushup, and rotary stability. Each task is scored from 0 to 3, with a maximal total score of 21. A score of 3 indicates a subject performed the task precisely as described, 2 indicates evidence of compensation, and 1 indicates that the task could not be performed according to the standardized testing criteria. A score of 0 indicates pain associated with the task.6,7
At our institution, the FMSTM is conducted annually by football strength and conditioning coaches at the beginning of training camp of each respective season. No changes were made to FMSTM protocols already in place at our institution. All coaches were certified in FMSTM testing. One coach evaluated each player. Scores for each assessment were immediately recorded, and a cumulative score was later tallied. Players were excluded from testing if they participated in another NCAA sport coinciding with the start of football training camp or for injuries that warranted medical restrictions as determined by a team physician.
LESS Protocol
Due to time constraints by team athletics staff for this study, players were divided into two groups by a random number generator. LESS data were collected from one group before the start of the football season and the other group at the end of the season. LESS data were recorded using two standard video cameras (ZR960 MiniDV Camcorder, Canon Inc., Japan; PV-GS500 3CCD MiniDV Camcorder, Panasonic, Japan), positioned to capture frontal and sagittal views of the subject, and collected through a commercially available motion analysis software (Siliconcoach, The Tarn Group Ltd, New Zealand). Athletes were asked to perform three successful trials of a double-legged drop-jump-landing-rebound task. Athletes were instructed to jump vertically and horizontally off a 30-cm high box towards a marked target measured 50% body height horizontal distance from the box, followed immediately by a jump to achieve maximal vertical height (Figure 1). Three athletic trainers received training on scoring LESS videos, following existing guidelines.19 Each video was replayed and scored by at least three trained reviewers. Intertester reliability testing was performed (average score ICC [2, k]=0.76).
FIGURE 1.

Demonstration of a double leg vertical drop-jump-landing-rebound task as part of the Landing Error Scoring System (LESS).
Statistical Analyses
Welch’s two-sample t-tests were used to examine if players with “acceptable” FMSTM scores (yes vs. no) differed on LESS scores for each individual FMSTM task. Welch’s two-sample t-tests were used to test for correlations between player position, LESS testing date, or prior subject history of ACL injury, and FMSTM or LESS score. Sensitivity and specificity of individual FMSTM tasks and at-risk LESS score (>6) were calculated using point estimates with a 95% confidence interval.
Univariate linear regression and multiple regression were used to examine associations between the modified FMSTM scores and LESS scores. The multiple regression included player position, LESS testing date, prior subject history of ACL injury. Alpha=0.05 was used for all statistical tests. Statistical tests were conducted using R software.22
RESULTS
One hundred and eleven subjects met the criteria for final inclusion in this study. Forty-six players were tested post-season, 61 were considered “strength” players, and eight had a prior history of ACL injury. The average LESS score was 5.51±1.34, and the average modified FMSTM score was 11.77±2.13 (Table 1). No ACL injuries occurred during the study period.
TABLE 1.
Variables recorded

There was an association between poor FMSTM squat score and higher LESS score (t=−5.41, P<0.001). The average LESS score for poor FMSTM squat score was 7.17 compared to 5.35 for acceptable FMSTM squat score. A poor FMSTM squat score has a 98% specificity and 24% sensitivity for LESS >6. Significant differences in LESS scores were not found between groups defined by FMSTM hurdle-step score status (t=−1.35, P=0.19), FMSTM in-line lunge score status (t=0.91, P=0.38), FMSTM leg raise score status (t=-0.99, P=0.33), or FMSTM trunk stability score status (t=−0.52, P=0.61). Compared to players without a history of ACL injury, players with a prior history of ACL injury were not more likely to have a lower modified FMSTM score (P=0.89) or higher LESS score (P=0.22).
In the univariate regression, there is an inverse linear relationship between modified FMSTM score and LESS score (coefficient=−0.16, r2=0.068, P<0.001) (Figure 2). In the multiple regression, the modified FMSTM score was still inversely associated with LESS score (coefficient=-1.66, r2=0.14, P=0.017) in a model with a history of ACL injury (P=0.60) and player position (P=0.82).
FIGURE 2.
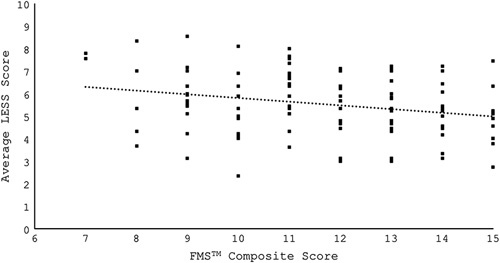
Univariate regression of LESS score against modified FMSTM score (Coefficient=−0.16416, R-squared=0).
DISCUSSION
The prevalence of knee injury in college football is high.4,5 Bradley et al.23 reported that 54% of participants at the 2005 NFL Combine had a history of knee injury, and 10% of participants had a history of ACL injury, with most requiring surgical reconstruction.3 In addition to the medical costs involved after ACL injury, Brophy et al.4 noted that a prior history of ACL injury was correlated with a decreased likelihood of playing in the NFL. Once at the NFL level, only 63 percent of players returned to play after ACL injury with a cost of 10.8 mo of lost playing time after ACL reconstruction.24 The ability to risk-stratify players for potential intervention is paramount.
Our study uses LESS as a measure of risky movement patterns associated with ACL injury in elite college football players. Although we found a statistically significant inverse relationship between LESS score and modified FMSTM score, the correlation may not be useful in clinical practice to stratify risk, as the difference in predicted LESS score from the highest and lowest FMSTM scores is small. Furthermore, there is a large amount of variance in the LESS score at any given modified FMSTM score, which is poorly explained by the linear relationship (r2=0.14). Kraus et al.25 suggest that FMSTM is better evaluated by each sub-item in order to determine modifiable injury risk and athletic performance. Of the individual FMSTM exercises, as defined by this study, only a poor FMSTM squat exercise was associated with higher LESS score. The average LESS score for athletes who performed poorly on the FMSTM squat was 7.17 compared to 5.35 for athletes who were not considered at risk. Padua et al.19 suggested that LESS scores greater than 6 be considered high risk, while LESS scores greater than 5 but less than or equal to 6 be considered moderate risk. However, we found that FMSTM squat is a specific (98.6%) but not sensitive (23.7%) test for LESS >6. Based on these results, we believe that the FMSTM is not an adequate screening tool for ACL injury risk.
The mechanism of ACL injury has been well studied. The most common mechanism of noncontact ACL injury involves a significant dynamic valgus rotational force directed over a fixed-planted foot.1 Biomechanical risk factors for ACL injury include decreased relative hamstring strength (to quadriceps), decreased core strength and proprioception, low trunk, hip and knee flexion angles, and increased dynamic knee valgus during cutting and jump-landing exercises. Both the FMSTM and the LESS assess for risky dynamic movement patterns. Compared to the FMSTM, the LESS involves a faster and higher-impact movement. We believe that this difference is a key factor that makes the LESS more suited to assess movement patterns associated with ACL injury risk.
The LESS is designed to be conducted in less than 5 min and has been well correlated to ACL injury-specific risky movement patterns by three-dimensional biomechanical analysis.19 However, there is conflicting evidence regarding the use of the LESS as a predictor of actual ACL injury. In a case-control study of over 5000 varsity high school and college athletes, Smith et al.21 found no relationship between LESS score and ACL injury. However, Padua et al. conducted a cohort study of over 800 elite youth-soccer athletes and found an association between high LESS score and ACL injury.18
There are several limitations inherent in our study. The LESS test has not been widely validated in collegiate football players, nor is it necessarily an appropriate screen for contact-related ACL injury that occurs in football more often than many other sports and may occur by many different mechanisms.26 Furthermore, due to constraints imposed by team staff, we were not able to control FMSTM administration protocols, and LESS data were collected at different times during the football season. We did not find a statistical difference in LESS scores collected pre-season and post-season, although one might expect higher LESS scores collected post-season given injuries and fatigue sustained over the course of the season. While this is an acknowledged methodologic weakness of the study, given the study population of high-performing NCAA Division IA football players and no effect of testing time on multiple regression, we believe that our results provide a meaningful contribution to clinical practice. Further study may better refine optimal and efficient screening tools for ACL injury risk, thereby improving risk assessment and increasing adoption of the screening tool by training staff.
CONCLUSIONS
This study did not find a strong correlation between the FMSTM and LESS. The LESS is a validated screening tool for the evaluation of movement patterns associated with ACL injury risk. We do not believe that the FMSTM adequately screens for movement patterns associated with ACL injury, and that the LESS may be a useful supplement in assessing such risky movement patterns. Identification of at-risk players will allow athletic staff and coaches to implement targeted movement pattern modification and injury prevention interventions.
Footnotes
Financial Disclosure: Dr. Dragoo discloses a financial relationship outside this work with DePuy/Mitek, Linvatec, Ossur, Smith and Nephew, Zimmer Biomet, Moximed. The other authors have no disclosures. The authors report no conflicts of interest in regard to this study.
REFERENCES
- 1.Alentorn-Geli E, Myer GD, Silvers HJ, et al. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surgery Sport Traumatol Arthrosc. 2009; 17:705–729. [DOI] [PubMed] [Google Scholar]
- 2.Myklebust G, Bahr R. Return to play guidelines after anterior cruciate ligament surgery. Br J Sports Med. 2005; 39:127–131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lohmander L, Englund P, Dahl L, et al. The long-term consequence of anterior cruciate ligament and meniscus injuries. Am J Sports Med. 2007; 35:1756–1769. [DOI] [PubMed] [Google Scholar]
- 4.Brophy R, Barnes R, Rodeo S, et al. Prevalence of musculoskeletal disorders at the NFL combine - Trends from 1987 to 2000. Med Sci Sports Exerc. 2007; 39:22–27. [DOI] [PubMed] [Google Scholar]
- 5.Dragoo J, Braun H, Durham J, et al. Incidence and risk factors for injuries to the anterior cruciate ligament in National Collegiate Athletic Association Football. Am J Sport Med. 2012; 40:990–995. [DOI] [PubMed] [Google Scholar]
- 6.Cook G, Burton L, Hoogenboom B. Pre-participation screening: the use of fundamental movements as an assessment of function - part 1. N Am J Sport Phys Ther. 2006; 9:396–409. [PMC free article] [PubMed] [Google Scholar]
- 7.Cook G, Burton L, Hoogenboom B. Pre-participation screening: the use of fundamental movements as an assessment of function - part 2. N Am J Sports Phys Ther. 2006; 9:549–563. [PMC free article] [PubMed] [Google Scholar]
- 8.DiStefano L, Padua D, DiStefano M, et al. Influence of age, sex, technique, and exercise program on movement patterns after an anterior cruciate ligament injury prevention program in youth soccer players. Am J Sports Med. 2009; 37:495–505. [DOI] [PubMed] [Google Scholar]
- 9.Leeder J, Horsley IG, Herrington LC. The inter-rater reliability of the functional movement screen within an athletic population using untrained raters. J Strength Cond Res. 2013; 30:2591–2599. [DOI] [PubMed] [Google Scholar]
- 10.Gribble P, Brigle J, Pietrosimone B, et al. Intrarater reliability of the functional movement screenTM. J Strength Cond Res. 2013; 27:978–981. [DOI] [PubMed] [Google Scholar]
- 11.Gulgin H, Hoogenboom B. The functional movement screen (FMS): an inter-rater reliability study between raters of varied experience. Int J Sports Phys Ther. 2014; 9:14–20. [PMC free article] [PubMed] [Google Scholar]
- 12.Parenteau-G E, Gaudreault N, Chambers S, et al. Functional movement screen test: A reliable screening test for young elite ice hockey players. Phys Ther Sport. 2014; 15:169–175. [DOI] [PubMed] [Google Scholar]
- 13.Smith C, Chimera N, Wright N, et al. Interrater and intrarater reliability of the functional movement screen. J Strength Cond Res. 2013; 27:982–987. [DOI] [PubMed] [Google Scholar]
- 14.Chorba R, Chorba D, Bouillon L, et al. Use of a functional movement screening tool to determine injury risk in female collegiate athletes. N Am J Sports Phys Ther. 2010; 5:47–54. [PMC free article] [PubMed] [Google Scholar]
- 15.Irick E. NCAA sports sponsorship and participation rates report; 2014.
- 16.Kiesel K, Plisky P, Voight M. Can serious injury in professional football be predicted by a preseason functional movement screen? N Am J Sports Phys Ther. 2007; 2:147–158. [PMC free article] [PubMed] [Google Scholar]
- 17.Kiesel K, Butler R, Plisky P. Prediction of injury by limited and asymmetrical fundamental movement patterns in American football players. J Sport Rehabil. 2014; 23:88–94. [DOI] [PubMed] [Google Scholar]
- 18.Padua D, DiStefano L, Beutler A, et al. The Landing Error Scoring System as a screening tool for an anterior cruciate ligament injury–prevention program in elite-youth soccer athletes. J Athl Train. 2015; 50:589–595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Padua D, Boling M, Distefano L, et al. Reliability of the landing error scoring system-real time, a clinical assessment tool of jump-landing biomechanics. J Sport Rehabil. 2011; 20:145–156. [DOI] [PubMed] [Google Scholar]
- 20.Onate J, Cortes N, Welch C, et al. Expert versus novice interrater reliability and criterion validity of the landing error scoring system. J Sport Rehabil. 2010; 19:41–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Smith HC, Johnson RJ, Shultz SJ, et al. A prospective rvaluation of the Landing Error Scoring System (LESS) as a screening tool for anterior cruciate ligament injury risk. Am J Sports Med. 2012; 40:521–526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.R Core Team R: A language and environment for statistical computing; 2015.
- 23.Bradley J, Honkamp NJ, Jost P, et al. Incidence and variance of knee injuries in elite college football players. Am J Orthop. 2008; 37:310–314. [PubMed] [Google Scholar]
- 24.Shah V, Andrews J, Fleisig G, et al. Return to play after anterior cruciate ligament reconstruction in National Football League athletes. Am J Sports Med. 2010; 38:2233–2239. [DOI] [PubMed] [Google Scholar]
- 25.Kraus K, Sch Tz E, Taylor W, et al. Efficacy of the functional movement screen: a review. J Strength Cond Res. 2014; 28:3571–3584. [DOI] [PubMed] [Google Scholar]
- 26.Bradley J, Klimkiewicz J, Rytel M, et al. Anterior cruciate ligament injuries in the National Football League: Epidemiology and current treatment trends among team physicians. Arthroscopy. 2002; 18:502–509. [DOI] [PubMed] [Google Scholar]