

Abstract
Background:
Trauma, a major public health concern in remote highlands of Nepal, has led to considerable morbidity and mortality. The study elucidates the pattern and characteristics of trauma at the only tertiary care hospital in the Karnali province, Nepal.
Materials and Methods:
Case records of all injured patients who presented to the emergency department from January to December 2018 were analyzed for demographic data, types of injuries, body parts injured, the outcome of the treatment, and distribution of injuries with respect to age and sex.
Results:
A total of 460 injured patients (age: 26.5 ± 19.67 years, range: 0.5–84) were studied consisting of 282 (61.3%) males and 178 (38.7%) females, with a male-to-female ratio being 1.58:1 (P = 0.001). Unintentional injuries were the predominant form of trauma (n = 383, 84.1%), with fall (n = 194, 42.2%), road traffic crashes (RTC) (n = 161, 35%), and physical assaults (n = 73, 15.9%) being the top three leading causes in order. Fall injury and RTC were most prevalent in children, accounting 12.8% (59) and 9.3% (43) of the total injuries, respectively. The physical assaults were predominant (n = 23, 5%) in adults (20–29 years). Male patients significantly outnumbered females for all types of injuries. Soft tissue followed by head and extremities was the most common site of injuries.
Conclusion:
Trauma in Karnali is a predominantly early age male occurrence, with fall injury being the leading etiological factor, followed by injuries due to RTC and physical assaults. Soft tissue, head, and extremities were the major sites of injuries. Reducing fall injuries, RTC, and physical assaults will likely reduce mortality and morbidity due to trauma in this province.
Keywords: Fall injury, Karnali, Nepal, physical assaults, road traffic crashes
INTRODUCTION
Any trauma is a bodily lesion at the organic level that results from acute exposure to different forms of energy (mechanical, thermal, electrical, chemical, or radiant) in amounts that exceed physiologic tolerance threshold. In some cases (like drowning, strangulation, or freezing), the injury results from an insufficiency of a vital element. The causes of injuries can be either intentional or unintentional. Road traffic crashes (RTC), burns, fall, drowning, and most of the poisonings are classified as unintentional, whereas injuries due to physical assaults and self-inflicted violence are classified as intentional injuries.[1]
The WHO highlights that more than 5 million people die each year as a result of injuries, which accounts for 9% of the world's deaths which is nearly 1.7 times the number of fatalities due to HIV/AIDS, tuberculosis, and malaria combined. Furthermore, tens of millions of people suffer nonfatal injuries that require treatment.[2] The WHO further indicates that 90% of the world's death from injuries occur in low- and middle-income countries. In the Asia-Pacific region, about 2.7 million deaths occurred due to injuries in 2002 (7000 deaths daily) that was 52% of worldwide injury deaths. The injury burden in the same year was about 92.5 million disability-adjusted life years lost that is 51% of the global total.[2]
Injuries, violence, and disabilities are major public health problems in Nepal.[3] As per estimates of morbidity and mortality for 1998–1999, injury contributed 9% to total mortality and was the third leading cause in the country.[4]
Karnali, one of the seven federal provinces, the country's most deceived region both by geography and development, occupies the higher mountainous land of north and mid-hills of Nepal and inhabits 1,570,418 people.[5] In terms of life expectancy and adult literacy, Karnali has an average value of 63.64 years and 42.99%, compared to the national average of 68.80 years and 59.57%, respectively.[6] Illiteracy, trying physical environments, recent urbanization with the access of new road networks extending into far-flung remote villages, low socioeconomic status, and family conflicts are the primary factors for the higher incidence of fall injuries, RTC, and physical assaults in this province.[4] The prevailing burden of injuries in this part of the nation has not yet been scientifically presented.
Trauma care in Nepal is at its start. There is a lack of strict evidence regarding the incidence of injury. Unavailability of data on trauma is one of the most important impediments to trauma management in Nepal, especially in backward and remote regions like Karnali. Trauma has been recognized to be preventable over the past few decades, and methods for the scientific study of injury prevention have been established.[1] However, the development of effective trauma prevention measures depends on reliable and detailed information on the characteristics and pattern of injury. Thus, the aim of this study is to elucidate the pattern and characteristics of trauma at teaching hospital of Karnali Academy of Health Sciences (KAHS), Karnali, Nepal.
MATERIALS AND METHODS
Study design and setting
This is retrospective cross-sectional study of patients of all age groups and gender who presented to the emergency department of KAHS teaching hospital, Jumla, Karnali province, Nepal, from January to December 2018.
We retrieved medical records of the patients presented to the emergency department; the medical record files were reviewed, and the sociodemographic information, presenting complaints, diagnosis, and outcome of management of patients were extracted. The patients with missing medical record files, uncompleted clinical information, and not diagnosed were excluded from the study. The institutional research and ethical committee approved the study.
KAHS, established in 2011 by an act of parliament of Nepal in Jumla (at altitude of 2514 m), is the only hospital to provide tertiary health-care facilities to all the districts of Karnali province (the Western region of Nepal). There is no trauma center in the province. The Karnali is the most poverty-stricken mountainous, remote province of Nepal with ten districts – the province extends up to the elevation of 6717 m from the mean sea level.[7]
Study population
The case records of all patients seen with injuries at the emergency department during the study period were retrieved. Demographic data, types of injuries sustained, causes, and circumstances of injuries, as well as the outcome of treatment were extracted from the case files and entered onto a computerized questionnaire. The patients with missing medical record files, uncompleted vital clinical information, and patients with unidentified causes of injuries were excluded from the study.
Statistical analysis
A total of 460 cases were entered into the EpiData. The data from the EpiData were imported to SPSS version 20 (Statistical Package for Social Science, Inc., Chicago, USA) for analysis. Descriptive statistics were used to display single variable, mean and standard deviation were used for continuous variables, and proportions were used for categorical variables. Chi-square test for goodness of fit was used to show the significant distribution and P < 0.05 was considered statistically significant.
RESULTS
Demographic data
A total of 460 patients attending the emergency department were included in the study. There were 282 (61.3%) males and 178 (38.7%) females with a male-to-female ratio of 1.58:1 (P < 0.001). The average age of the patients was 26.5 ± 19.67 years, ranging from 6 months to 84 years with a median age of 22 years. The majority of the patients were below 10 years of age, accounting for 23.9% (110) of total and least (7.6%) were of 50s. The sex distribution of patients with respect to age groups is presented in Figure 1.
Figure 1.

Sex distribution of patients with respect to age groups
Types of injuries and injury distribution with age
Unintentional injuries were the predominant form of trauma (n = 383, 84.1%) in the study population [Figure 2]. Considering the causes of trauma, the most common was fall injury (n = 194, 42.2%), followed by RTC (n = 161, 35%), physical assault (n = 73, 15.9%), burn (n = 11, 2.4%), dog bite (n = 8, 1.7%), snakebite (n = 2, 0.4%), cut injury (n = 10, 2.2%), and drowning (n = 1, 0.2%).
Figure 2.

Causes of injuries
The distribution of etiologies of injury with respect to age groups is illustrated in Table 1 and Figure 3. The causes of injuries disproportionately distributed with the age groups. Fall injury, RTC, and physical assaults were the predominant forms of trauma in each group of age. Fall injury and RTC were most common in the participants below 10 years of age, accounting for 12.8% (59) and 9.3% (43), respectively, of the total injuries in the study population. The number of injuries, however, declined with increasing age. The physical assaults were predominant (n = 23, 5%) among adults (20–29 years) and were less likely in younger and older participants.
Table 1.
Distribution of injuries with respect to age group
| Age of patients (years) | Fall injury | RTA | Physical assault | Burn | Dog bite | Snakebite | Cut injury | Drowning | Total |
|---|---|---|---|---|---|---|---|---|---|
| Below 10 | 59 | 43 | 3 | 4 | 1 | 0 | 0 | 0 | 110 |
| 10-19 | 41 | 31 | 16 | 3 | 1 | 1 | 1 | 0 | 94 |
| 20-29 | 21 | 31 | 23 | 1 | 3 | 1 | 3 | 1 | 84 |
| 30-39 | 22 | 19 | 15 | 2 | 0 | 0 | 2 | 0 | 60 |
| 40-49 | 16 | 13 | 6 | 0 | 0 | 0 | 2 | 0 | 37 |
| 50-59 | 10 | 16 | 7 | 1 | 1 | 0 | 0 | 0 | 35 |
| 60 and above | 25 | 8 | 3 | 0 | 2 | 0 | 2 | 0 | 40 |
| Total | 194 | 161 | 73 | 11 | 8 | 2 | 10 | 1 | 460 |
RTA: Road traffic accident
Figure 3.

Distribution of injuries with respect to age groups
Injury distribution with sex
Table 2 and Figure 4 illustrate the distribution of trauma with respect to sex. The proportions of fall injury in male (n = 282) and female (n = 178) were 42.9% (confidence interval [CI]: 37.12%–48.67%) and 41% (CI: 33.77%–48.22%), respectively. Similarly, the proportions of physical assault in male and female were 16.3% (CI: 11.98%–20.6%) and 15.2% (CI: 10.8%–19.59%). The sex distribution of patients in fall injury (P = 0.001), RTC (P = 0.033), and physical assault (P = 0.026) was significant.
Table 2.
Distribution of injury with respect to sex
| Type of injuries | Sex | Total | |
|---|---|---|---|
| Male | Female | ||
| Fall injury | 121 | 73 | 194 |
| RTA | 94 | 67 | 161 |
| Physical assault | 46 | 27 | 73 |
| Burn | 6 | 5 | 11 |
| Dog bite | 6 | 2 | 8 |
| Snakebite | 1 | 1 | 2 |
| Cut injury | 7 | 3 | 10 |
| Drowning | 1 | 0 | 1 |
| Total | 282 | 178 | 460 |
RTA: Road traffic accident
Figure 4.
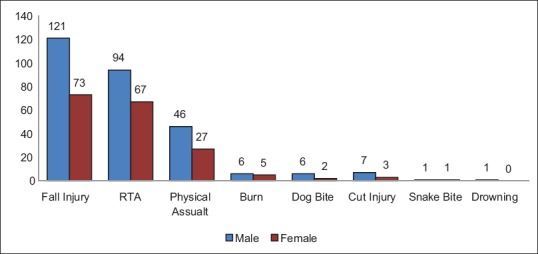
Distribution of injury with respect to sex
Body parts injured
Considering all the cases of injuries, majority was soft-tissue injury (n = 182, 39.60%). Injury of the extremities (n = 134, 29.1%) and head (n = 113, 24.6%) were most common after soft-tissue injury. The other body regions injured are presented in Figure 5.
Figure 5.
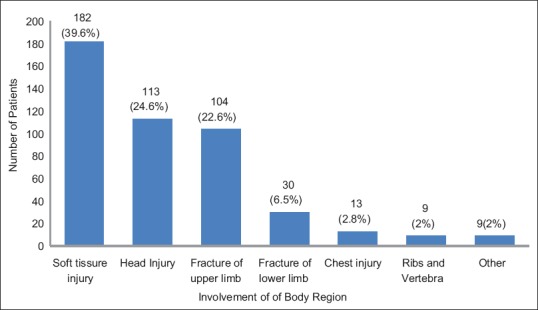
Involvement of body region
Outcome
The outcome of the injured patients is illustrated in Figure 6. Majority of the patients were discharged from the emergency ward (n = 266, 57.8%) after required treatment, whereas very few (n = 30, 6.5%) were kept for observation. One-fourth of the patients (n = 118, 25.7%) were admitted to the indoor patient department. The average hospital stay was 5.56 ± 5.7 h, ranging from 1 to 48 h.
Figure 6.
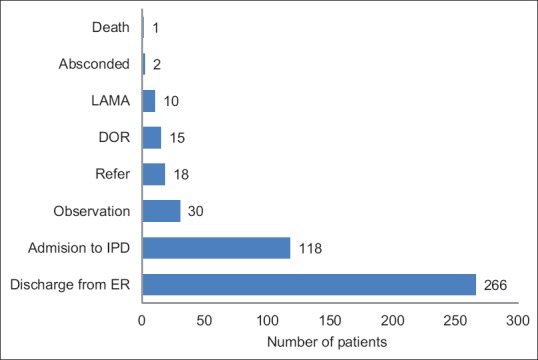
Outcome of patients visiting to emergency department
DISCUSSION
Unintentional injuries were the predominant form of trauma among the people of Karnali that accounted for the 84.1% of total injury-related cases. A similar study in Nigeria has also reported unintentional injuries as the chief form of trauma with 83.6% of total injuries.[8] Our finding is further supported by the report of Nepal health research council; still, the percentage attributed to unintentional injuries was slightly higher in our study population. The discrepancy may be due to the council report produced largely based on the data from the major urban tertiary care hospitals of the country.[4]
The present study showed fall as the leading cause of injury among the people of Karnali; this is ascribed to the precipitous high mountains and hills in the province that provides residence and land for agriculture. The people's compulsion of working for their livelihood in such topography highly predisposes them to fall and subsequent injuries. Our finding contradicts other studies that reported road traffic injuries as a major cause of trauma and disability.[8,9,10] In this study, road traffic injuries were the second most common form of trauma after fall injuries, despite the fact that the region has far less number of motor vehicles and road access to the villages. Karnali, one of the most remote and isolated regions in Nepal, is reachable only by foot or small aircrafts. Surprisingly, RTC is the second most common cause that contributed 35% of total injuries; this can be due to very poor enforcement of traffic safety regulations. However, supporting the other studies, the lowlands of Nepal have shown RTC as the major leading cause of death and disabilities.[4]
Our results showed physical assaults, an intentional injury, as the third most common cause of trauma. Illiteracy, alcohol and drug abuse, poor prosecution of security services, and poor access to health services in the province may have increased the rate of trauma due to assaults. The WHO, in support of this, has suggested that illiteracy and heavy alcohol consumption are strongly linked to violent behavior.[11]
Considering all forms of injuries, the burden of trauma in this study population is mostly borne by young males, a finding which aligns to other studies.[8,12] The injured patients in our study population were mostly below 10 years of age, which constituted almost one-fourth of the total. The injuries gradually declined with the age and least were recorded at 40–49 years but were recorded slightly higher after the age of 60 years. In each age group, majority cases were due to fall, followed by RTC and physical assault; the highest injuries due to these were recorded in the age group below 10 years. The incidences of physical assaults were more prevalent at the ages of 20s and 30s. Several studies have revealed the age group of 15–44 years as the most susceptible group to different forms of trauma.[4,13,14] This age group actually involves in risk-taking activities and is more exposed to the elements being the main revenue earners in families, which may have made them more susceptible. The group represents the active and productive segment of the society and may lead to serious economic loss; thus, the proper preventive measures should be taken particularly targeting boys in their formative years. This study also has shaded light on the different etiologies of injury with the increasing age.
Regarding the body regions involvement, soft-tissue injury was widely present in our patients comprising 40% of all the injuries. This contradicts the finding of Elachi et al.[8] as they have reported extremities the most commonly injured body region. Another study in Southern Iran, however, has stated that head and neck are the most frequent sites for trauma.[15] In our study population, after soft tissue, head was the major site of trauma and was followed by extremities. Considering the outcome of injured patients, more than half of the patients were treated and discharged without permanent disabilities, few were referred, one died, and interestingly two absconded from the ward.
This study has characterized the trauma injuries in the country's most remote and backward high-altitude province. The study has primarily focused on the prevalence, causes of injuries, distribution of injuries with age and sex, affected body parts, and outcome of the patients. The findings of this study may have underestimated the real prevalence of injures as only the emergency patients were considered for the study. Many victims because of remoteness of the region and dearth of transportation facilities do not visit the hospital.
CONCLUSION
Unintentional injuries were the most predominant form of trauma in Karnali, with the fall injury being the leading cause. RTC were the second prominent cause, and physical assault, an intentional injury, was the third most common cause. The burden of trauma was mostly borne by early age group (<10 years) male population. The incidence of physical assaults was more during their 20s and 30s. Soft tissue and head were the most common sites of injuries in our study population.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Krug EG, Sharma GK, Lozano R. The global burden of injuries. Am J Public Health. 2000;90:523–6. doi: 10.2105/ajph.90.4.523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.World Health Organization. Injuries and Violence:the Facts. World Health Organization; 2014. [Last accessed on 2018 Oct 28]. Available from: http://www.who.int/violence_injury_prevention/media/news/2015/Injury_violence_facts_2014/en/ [Google Scholar]
- 3.Mishra B, Sinha Mishra ND, Sukhla S, Sinha A. Epidemiological study of road traffic accident cases from Western Nepal. Indian J Community Med. 2010;35:115–21. doi: 10.4103/0970-0218.62568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nepal Health Research Council. Epidemiological Study on Injury and Violence in Nepal. Nepal Health Research Council; 2009. [Last accessed on 2018 Dec 11]. Available from: http://nhrc.gov.np/wp-content/uploads/2017/02/Injury-and-Violence.pdf . [Google Scholar]
- 5.Central Bureau of Statistics. Population and Housing Census. Central Bureau of Statistics; 2011. [Last accessed on 2018 Oct 31]. Available from: https://unstats.un.org/unsd/demographic-social/census/documents/Nepal/Nepal-Census-2011-Vol1.pdf . [Google Scholar]
- 6.Government of Nepal, UNDP. Nepal Human Development Report. 2014. [Last accessed on 2018 Oct 28]. Available from: http://www.hdr.undp.org/sites/default/files/nepal_nhdr_2014-final.pdf .
- 7.Karnali Academy of Health Sciences. Home Page, Introduction. Karnali Academy of Health Sciences. 2011. [Last accessed on 2019 Jan 05]. Available from: http://kahs.edu.np .
- 8.Elachi IC, Yongu WT, Odoyoh OO, Mue DD, Ogwuche EI, Ahachi CN. An epidemiological study of the burden of trauma in Makurdi, Nigeria. Int J Crit Illn Inj Sci. 2015;5:99–102. doi: 10.4103/2229-5151.158404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chalya PL, Dass RM, Mchembe MD, Mbelenge N, Ngayomela IH, Chandika AB, et al. Citywide trauma experience in Mwanza, Tanzania:A need for urgent intervention. J Trauma Manag Outcomes. 2013;7:9. doi: 10.1186/1752-2897-7-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Demyttenaere SV, Nansamba C, Nganwa A, Mutto M, Lett R, Razek T. Injury in Kampala, Uganda:6 years later. Can J Surg. 2009;52:E146–50. [PMC free article] [PubMed] [Google Scholar]
- 11.World Health Organization. Youth Violence and Alcohol. World Health Organization; 2006. [Last accessed on 2018 Oct 31]. Available from: http://www.who.int/violence_injury_prevention/violence/world_report/factsheets/fs_youth.pdf . [Google Scholar]
- 12.Swarnkar M, Singh PK, Dwivedi S. Pattern of trauma in central India:An epidemiological study with special reference to mode of injury. Internet J Epidemiol. 2009;9:1–7. [Google Scholar]
- 13.Moshiro C, Heuch I, Astrøm AN, Setel P, Hemed Y, Kvåle G. Injury morbidity in an urban and a rural area in Tanzania:An epidemiological survey. BMC Public Health. 2005;5:11. doi: 10.1186/1471-2458-5-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Oliver Bañuls A, Civera Clemente P. Epidemiologic study of accidents attended in a non-hospital emergency service. Aten Primaria. 1998;21:522–6. [PubMed] [Google Scholar]
- 15.Abbasi HR, Mousavi SM, Taheri Akerdi A, Niakan MH, Bolandparvaz S, Paydar S. Pattern of traumatic injuries and injury severity score in a major trauma center in Shiraz, Southern Iran. Bull Emerg Trauma. 2013;1:81–5. [PMC free article] [PubMed] [Google Scholar]