

Abstract
Background
Recent studies have shown that oral administration of probiotics may improve the immune imbalance caused by dysbiosis of the gut microbiome in atopic dermatitis (AD). This study aimed to investigate the clinical and immunological effects of Lactobacillus pentosus in children with mild to moderate AD.
Methods
Children aged 2–13 years with AD were randomized to receive either 1.0 × 1010 colony-forming units of L. pentosus or placebo, daily, for 12 weeks. The clinical severity of AD and transepidermal water loss were evaluated. Blood eosinophil counts, serum total immunoglobulin E (IgE), and cytokine levels were measured. The diversity and composition of the gut microbiota were also analyzed.
Results
Eighty-two children were recruited, and 41 were assigned to the probiotics intervention group. The mean scoring of atopic dermatitis (SCORAD) indices at baseline were 30.4 and 34.3 for the probiotics and placebo groups, respectively. At week 12, the mean indices were 23.6 and 23.1 for the probiotics and placebo groups, respectively. Clinical severity decreased significantly over time in both groups, with no significant difference between the two groups. In both groups, there were no significant differences in cytokine levels, microbial diversity, or the relative abundance of the gut microbiota at week 12 compared with the corresponding baseline values. The mean subjective scores of SCORAD indices after intervention for the probiotics group were significantly lower than those for the placebo group in IgE sensitized AD (P = 0.019).
Conclusion
Our results show improved symptoms in the probiotics and placebo groups, and we could not find additional effects of L. pentosus in AD. However, the mean subjective scores of SCORAD indices for the probiotics group are significantly improved compared with those for the placebo group in allergen-sensitized AD.
Keywords: Atopic Dermatitis, Probiotics, Lactobacillus pentosus, Microbiome
Graphical Abstract
INTRODUCTION
Atopic dermatitis (AD) is a chronic, recurrent, inflammatory skin disease characterized by extreme itching and dryness,1 affecting 10%–20% of children worldwide.2 This disease exhibits chronic progression from childhood and has been recognized as a refractory disease that is difficult to treat despite long-term therapy. Complex associations between genetic, environmental, and immunological factors induce the development of AD,3 and cellular immune dysregulation in AD results in a Th cell (Th1/Th2) imbalance, shifted toward Th2 cell differentiation. Given the complexity of the immune pathways that lead to AD, selective anti-inflammatory or immunomodulatory agents may be less effective. Thus, it is important to restore balance in immune pathways through fundamental immune regulation.
An imbalance of the gut microbiome may be associated with AD.4 Low microbial diversity in the gut microbiota in the first month of life has been associated with subsequent incidence of AD.5,6 Several studies have attempted oral administration of probiotics to alter gut microbiome imbalances, eventually restoring the immune balance and improving the symptoms of AD.7 Some studies have shown that probiotics are effective in controlling AD, but others have concluded that probiotics administration does not improve AD symptoms.
Lactobacillus pentosus derived from Kimchi is an effective modulator of the immune response.8 In house dust mite-sensitized AD mice, it increases the induction of regulatory B10 cells to produce IL-10.9 Lactobacillus plantarum, of the same genus as L. pentosus, was also shown to be effective in the treatment of AD in children.10
In this study, we investigated the clinical and immunological effects of L. pentosus in children with mild to moderate AD and aimed to observe the microbial diversity and composition of the gut microbiota. Additionally, we investigated whether probiotics administration is effective in subgroups with specific characteristics.
METHODS
Study subjects
One hundred and twenty-four subjects with mild to moderate AD (2–13 years old) were recruited from the Department of Pediatrics, Korea University Anam Hospital between January and September 2017. All subjects were diagnosed with AD by a pediatric allergist, according to the diagnostic criteria developed by Hanifin and Rajka,11 and the clinical severity was determined using the scoring of atopic dermatitis (SCORAD) index.12 Subjects with mild to moderate AD (SCORAD 20–50) were included. The exclusion criteria were as follows: 1) having additional systemic diseases, such as skin disease, immunodeficiency, or autoimmune disease; 2) treatment with systemic antibiotics, corticosteroids, antifungal agents, or immunosuppressants associated with AD within 4 weeks of screening; 3) treatment with medicines such as antihistamines, herbal medicines, or health functional foods for AD within 4 weeks of screening; 4) treatment with phototherapy within 4 weeks of screening; and 5) intent to participate in other studies during this clinical study.
Study design
This study was designed as a double-blinded, placebo-controlled, randomized study. Subjects were randomized to receive either live probiotics, specifically L. pentosus (1.0×1010 colony-forming units), or placebo twice a day for 12 weeks (Fig. 1). The probiotics and placebos were identical in color, taste, smell, packing, and manner of administration. All formulations were dispensed by a technician, with the investigator and subjects blinded to the identity of the intervention. Compliance was assessed from the weight of residual powder.
Fig. 1. Double-blinded, placebo-controlled, randomized study design.

L. pentosus = Lactobacillus pentosus, SCORAD = scoring of atopic dermatitis, TEWL = transepidermal water loss, IgE = immunoglobulin E.
Throughout the intervention period, the subjects were strictly prohibited from using corticosteroids, antibiotics, antihistamines, and other probiotics; only topical fluticasone propionate was allowed for severe flare-ups or itching. All subjects received an equal amount of skin emollients, and the weight of the tube containing topical steroids was quantitatively measured at each visit.
Assessment of clinical severity of AD
The primary outcome was the change in severity of AD between baseline and week 12. The clinical severity of AD was evaluated at consecutive visits (by the SCORAD index). The SCORAD index combines objective and subjective scores, including the evaluation of pruritus and insomnia on a visual analog scale. The range of the SCORAD index is between 0 and 80. Subjects were divided into three groups: mild (< 25), moderate (25–50), or severe (> 50). Subjects with a SCORAD index of < 20 or > 50 were excluded from this study.
Transepidermal water loss (TEWL) was assessed noninvasively with a Tewameter® TM 300 (Courage+Khazaka, Köln, Germany) under standardized environmental conditions (indoor temperature of 22°C–26°C, relative humidity of 40%–60%, a ≥ 10-minute adaptation period, and exposed area of skin with clothes uncovered) using a standardized protocol,13 at baseline and at weeks 6 and 12. TEWL was measured on both forearms. The secondary outcome was the amount of topical steroid used, assessed by weighing the tubes.
Blood eosinophil counts and serum immunoglobulin E (IgE) levels
Blood samples were collected at baseline and at week 12. The number of peripheral blood eosinophils was measured using a Sysmex XE-2100 automated hematological analyzer (Sysmex, Kobe, Japan). The levels of total serum IgE and specific IgE antibodies against food allergens (egg white and soybean) and inhalant allergens (Dermatophagoides farinae) were determined using a fluorescence enzyme immunoassay (UniCAP, Phadia AB, Uppsala, Sweden). IgE sensitized AD was defined as blood specific IgE levels of > 0.7 kU/L.
Measurement of cytokine levels
Serum levels of IL-4, IL-5, IL-10, IL-13, and IFN-γ were measured using ELISA kits (R&D Systems, Minneapolis, MN, USA), whereas serum levels of IL-6, IL-17, and TGF-β were measured using a multiplex immunoassay based on Luminex technology (R&D Systems). The detection limits for IL-4, IL-5, IL-10, IL-13, and IFN-γ were 0.25, 3.9, 0.78, 125, and 15.6 pg/mL, respectively, and the maximum detection levels were 16, 150, 50, 4,000, and 1,000 pg/mL, respectively. The detection limits/maximum detection levels for IL-6, IL-17, and TGF-β were 0.95/2.53 pg/mL, 33.3/3,900 pg/mL, and 10,370/24,300 pg/mL, respectively.
Analysis of gut microbiome
specimen collection
Fecal samples from the subjects were collected in OMNIgene-GUT tubes (DNA Genotek, Ontario, Canada) as per the manufacturer's instructions and were stored at ambient temperature until they were processed.
DNA extraction
Metagenomic DNA was extracted from the fecal samples using the QIAamp DNA Stool Mini Kit (Qiagen, Hilden, Germany) with additional pre-processing steps. Briefly, the fecal samples (250 μL) stored in the OMNIgene-GUT tubes were transferred into 2 mL tubes containing 0.3 g of sterile 0.1 mm zirconia beads and 1.2 mL lysis buffer. After homogenization via vortexing, the samples were heated at 95°C for 15 minutes. Using a Qiagen TissueLyser II (Qiagen), the samples were bead beaten for 1 minute at 30 Hz, left on ice for 5 minutes, and then bead beaten for an additional minute. After centrifugation, the supernatant solution (1.2 mL) was reacted with an InhibitEX tablet and then centrifuged, after which 350 μL of the supernatant was transferred to a new tube. The subsequent DNA extraction steps were performed using a QIAcube (Qiagen). The extracted DNA samples were stored at −20°C until use.
16S rRNA gene sequencing and sequence analysis
For gut microbiome analysis, 16S rRNA gene sequencing was performed for the fecal samples at baseline and at weeks 12 and 14. Amplicon library preparation targeting the V3-V4 region of the 16S rRNA gene was performed according to the Illumina protocol for 16S Metagenomic Sequencing Library Preparation (Part # 15044223 Rev. B, Illumina, San Diego, CA, USA). Sequencing was performed on the MiSeq platform using the 2 × 300-bp MiSeq Reagent Kit v3. Raw sequence reads were processed for quality filtering and merging of read pairs, and subsequent analysis steps were performed using QIIME version 1.9.0 software.14 The sequences were clustered into operational taxonomic units (OTUs) based on 97% identity with pick_open_reference_otus.py. The α-diversity (observed species, Chao 1, phylogenetic diversity) and β-diversity (Bray-Curtis, weighted UniFrac, unweighted UniFrac distances) were calculated using core_diversity_analyses.py.
Statistical analysis
Comparison of mean values for continuous variables between the two groups was performed using t-tests, and the outcome values are represented as means ± standard deviations (SDs). Blood eosinophil counts and total serum IgE levels did not follow normal distributions, and therefore, are represented as natural log values of the means ± SDs. Comparison of frequencies between the two groups was performed using χ2 tests. The analysis method for efficacy assessment variables was performed using analysis of covariance, which takes baseline characteristics (covariates, variables that are observed prior to probiotics administration that may affect primary efficacy assessment variables) into consideration. Statistical analysis was performed using IBM SPSS Statistics version 22.0 (IBM Corp., Armonk, NY, USA), and outcomes with a P value of < 0.05 were considered statistically significant.
Statistical analysis of bacterial abundance
Statistical analysis of bacterial abundance at each visit and in each group was performed at the genus level for microbes detected in ≥ 40% of the samples. Comparison of bacterial abundances at different visits (baseline vs. week 12; baseline vs. week 14; and week 12 vs. 14) within each group (probiotics vs. placebo) was performed using the Wilcoxon signed rank test. The log2 fold change was obtained by adding 0.00001 to the bacterial relative abundance of each sample and calculating the log2 ratio at week 12 or week 14 against the baseline. The difference in fold change between the probiotics and placebo groups was analyzed using the Wilcoxon rank sum test.
Ethics statement
Written informed consent was obtained from the parents of each subject. This study protocol was approved by the Institutional Review Board (IRB) of the Korea University Anam Hospital (IRB No. 2016-0371).
RESULTS
Subject characteristics
One hundred and twenty-four AD subjects were screened for eligibility. The following 29 subjects were excluded: 5 subjects with severe AD, 19 with loss of symptoms prior to probiotics administration, 3 with recent use of topical steroids, and 2 that were lost to follow-up. The remaining 95 subjects were randomly assigned and equally distributed between the two groups. However, there were 13 additional drop-outs who withdrew from the study; these included those who took antibiotics, discontinued the visits, or could not complete the study due to violation of study protocol. The remaining 82 subjects were finally recruited, resulting in 41 subjects in each group (Fig. 2). The proportion of male subjects was higher in the probiotics group than in the placebo group (P = 0.004). The mean age was 4.8 ± 2.3 years in the probiotics group and 5.4 ± 3.0 years in the placebo group (P = 0.305). However, there were no other significant differences between the two groups in baseline demographics (Table 1).
Fig. 2. Flowchart of the study.

SCORAD = scoring of atopic dermatitis.
Table 1. Demographics of subjects.
| Variables | Probiotics (n = 41) | Placebo (n = 41) | P value | |
|---|---|---|---|---|
| Age, yr | 4.8 ± 2.3 | 5.4 ± 3.0 | 0.305 | |
| Sex, male | 25 (61) | 12 (29) | 0.004 | |
| Duration of illness, mon | 37.5 ± 21.5 | 46.6 ± 30.6 | 0.124 | |
| Cesarean section | 10 (24) | 14 (34) | 0.332 | |
| Family history of allergy | 33 (81) | 30 (73) | 0.432 | |
| Environmental tobacco smoke | 17 (41) | 19 (46) | 0.656 | |
| Bathing ≥ 1/day | 12 (29) | 15 (37) | 0.467 | |
| Soaping ≥ 1/day | 7 (17) | 11 (27) | 0.143 | |
| TEWL, g/m2/hr | 30.3 ± 17.0 | 27.7 ± 11.9 | 0.428 | |
| SCORAD | 30.4 ± 8.6 | 34.3 ± 8.3 | 0.040 | |
| Objective | 17.1 ± 8.8 | 21.0 ± 8.0 | 0.074 | |
| Subjective | 13.27 ± 2.61 | 13.34 ± 2.56 | 0.898 | |
| Log eosinophils, /µL | 5.7 ± 0.7 | 5.9 ± 0.6 | 0.275 | |
| Log total IgE, kU/L | 4.7 ± 1.5 | 4.5 ± 1.2 | 0.150 | |
| Sensitization to allergens | ||||
| Egg white | 4 (9.8) | 2 (4.9) | 0.466 | |
| Soybean | 11 (26.9) | 6 (14.6) | 0.172 | |
| Dermatophagoides farinae | 17 (43.9) | 18 (43.9) | 0.857 | |
Data are expressed as mean ± standard deviation or number (%).
TEWL = transepidermal water loss, SCORAD = scoring of atopic dermatitis, IgE = immunoglobulin E.
Changes in the clinical severity of AD
The mean SCORAD indices at baseline were 30.4 ± 8.6 for the probiotics group and 34.3 ± 8.3 for the placebo group. The mean SCORAD indices were significantly lower in the probiotics group than in the placebo group (P = 0.040). We also analyzed the mean objective and subjective scores of SCORAD indices separately. The mean objective and subjective scores of SCORAD indices were not significantly different between the probiotics and placebo groups (P = 0.074 and P = 0.898) (Table 1).
Comparing the mean SCORAD indices at baseline to those at week 12, the probiotics group exhibited a reduction from 30.4 ± 8.6 to 23.6 ± 11.0 (P < 0.001), and the placebo group exhibited a reduction from 34.3 ± 8.3 to 23.1 ± 9.7 (P < 0.001). The mean objective and subjective scores of SCORAD indices were not significantly different between the probiotics and placebo groups (P = 0.328 and P = 0.869) (Table 2).
Table 2. Clinical parameters in the two groups at baseline and at week 12.
| Variables | Probiotics (n = 41) | Placebo (n = 41) | P valuea | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Week 12 | P value | Baseline | Week 12 | P value | |||
| SCORAD | 30.4 ± 8.6 | 23.6 ± 11.0 | < 0.001 | 34.3 ± 8.3 | 23.1 ± 9.7 | < 0.001 | 0.254 | |
| Objective | 17.1 ± 8.8 | 12.3 ± 9.9 | < 0.001 | 21.0 ± 8.0 | 11.8 ± 8.2 | < 0.001 | 0.328 | |
| Subjective | 13.27 ± 2.61 | 11.32 ± 3.67 | < 0.001 | 13.34 ± 2.56 | 11.24 ± 3.56 | < 0.001 | 0.869 | |
| TEWL, g/m2/hr | 30.3 ± 17.0 | 28.1 ± 11.3 | 0.444 | 27.7 ± 11.9 | 25.1 ± 9.1 | 0.265 | 0.233 | |
| Log total IgE, kU/L | 4.7 ± 1.5 | 4.9 ± 1.5 | 0.122 | 4.5 ± 2.0 | 4.7 ± 1.2 | 0.044 | 0.563 | |
| Log eosinophils, /µL | 5.7 ± 0.7 | 5.8 ± 0.8 | 0.241 | 5.9 ± 0.6 | 5.8 ± 0.7 | 0.777 | 0.470 | |
Data are expressed as means ± standard deviation.
TEWL = transepidermal water loss, SCORAD = scoring of atopic dermatitis, IgE = immunoglobulin E.
aCompared between groups; P value by analysis of covariance adjusted by baseline.
Both the probiotics and placebo groups exhibited significant improvements in the severity of AD, but no additional effect was observed for the probiotics group compared with the placebo group. The mean TEWL values at baseline were 30.3 ± 17.0 g/m2/hr for the probiotics group and 27.7 ± 11.9 g/m2/hr for the placebo group (P = 0.428) (Table 1). Similarly, the mean TEWL values at week 12 were 28.1 ± 11.3 g/m2/hr for the probiotics group and 25.1 ± 9.1 g/m2/hr for the placebo group (P = 0.233) (Table 2).
Changes in blood eosinophil counts, total serum IgE, and specific IgE
At baseline, there was no significant difference in the logarithmic mean concentration of total IgE between the two groups, with values of 4.7 ± 1.5 IU/mL in the probiotics group and 4.5 ± 2.0 IU/mL in the placebo group (P = 0.150). Similarly, the logarithmic mean blood eosinophil count at baseline was not significantly different, with 5.7 ± 0.7 cells/μL in the probiotics group and 5.9 ± 0.6 cells/μL in the placebo group (P = 0.275) (Table 1). The same pattern was observed at week 12; the logarithmic mean concentration of total IgE was 4.9 ± 1.5 IU/mL in the probiotics group and 4.7 ± 1.2 IU/mL in the placebo group (P = 0.563). The logarithmic mean blood eosinophil count was 5.8 ± 0.8/µL in the probiotics group and 5.8 ± 0.7/µL in the placebo group (P = 0.470) (Table 2). Among the 41 subjects in each group, 23 (56%) from the probiotics group and 26 (63%) from the placebo group were positive for specific IgE.
Changes in serum cytokine levels
The serum levels of IL-4, IL-5, IL-6, IL-10, IL-13, IL-17, IFN-γ, and TGF-β were measured at baseline. There were no significant differences between the two groups (Table 3). In addition, the cytokine levels at week 12 compared with the baseline within each group were not statistically significant (Table 4).
Table 3. Baseline cytokine levels in the two groups.
| Cytokine, pg/mL | Probiotics (n = 41) | Placebo (n = 41) | P value |
|---|---|---|---|
| IL-4 | 0.29 ± 0.26 | 0.26 ± 0.07 | 0.479 |
| IL-5 | 3.90 ± 0.00 | 3.90 ± 0.00 | 1.000 |
| IL-6 | 0.66 ± 0.92 | 0.61 ± 1.70 | 0.863 |
| IL-10 | 0.95 ± 0.39 | 1.45 ± 2.23 | 0.810 |
| IL-13 | 129.00 ± 24.60 | 125.20 ± 1.40 | 0.336 |
| IL-17 | 0.43 ± 1.35 | 0.27 ± 0.76 | 0.505 |
| IFN-γ | 16.30 ± 4.20 | 15.60 ± 0.00 | 0.279 |
| TGF-β | 166,434 ± 36,403 | 179,179 ± 36,227 | 0.118 |
Data are expressed as means ± standard deviation.
IL = interleukin, IFN-γ = interferon-gamma, TGF-β = transforming growth factor-beta.
Table 4. Cytokine levels in the two groups at baseline and at week 12.
| Cytokine, pg/mL | Probiotics (n = 41) | Placebo (n = 41) | P value | ||
|---|---|---|---|---|---|
| Baseline | Week 12 | Baseline | Week 12 | ||
| IL-4 | 0.29 ± 0.26 | 0.25 ± 0.00 | 0.26 ± 0.07 | 0.25 ± 0.00 | - |
| IL-5 | 3.90 ± 0.00 | 4.24 ± 1.19 | 3.90 ± 0.00 | 3.90 ± 0.00 | 0.075 |
| IL-6 | 0.66 ± 0.92 | 0.84 ± 1.65 | 0.61 ± 1.70 | 0.72 ± 0.92 | 0.740 |
| IL-10 | 0.95 ± 0.39 | 1.24 ± 1.62 | 1.45 ± 2.23 | 1.59 ± 2.21 | 0.369 |
| IL-13 | 128.96 ± 24.57 | 138.86 ± 71.34 | 125.22 ± 1.40 | 125.55 ± 3.52 | 0.303 |
| IL-17 | 0.43 ± 1.35 | 0.49 ± 0.75 | 0.27 ± 0.76 | 0.38 ± 0.96 | 0.600 |
| IFN-γ | 16.32 ± 4.18 | 18.58 ± 12.24 | 15.60 ± 0.00 | 15.88 ± 1.29 | 0.366 |
| TGF-β | 166,434 ± 36,403 | 153,283 ± 41,393 | 179,179 ± 36,227 | 159,816 ± 34,250 | 0.750 |
Data are expressed as means ± standard deviation.
IL = interleukin, IFN-γ = interferon-gamma, TGF-β = transforming growth factor-beta.
Compared between groups; P value by analysis of covariance adjusted by baseline.
Gut microbiome analysis
Diversity of gut microbiota
The gut microbiomes of 76 subjects whose 16S sequence data were available for all the fecal samples at baseline and at weeks 12 and 14 were analyzed. First, the microbial α-diversity measured by the Chao 1 index was analyzed. No significant difference was observed in the Chao 1 index of the probiotics group compared with that of the placebo group at each visit (Fig. 3A). Next, the Bray-Curtis distances between different visits (baseline vs. week 12; baseline vs. week 14; and week 12 vs. 14) within each group (probiotics group vs. placebo group), respectively, were calculated. However, there was no significant difference in β-diversity, indicating similar degrees of overall compositional change between the probiotics and placebo groups (Fig. 3B).
Fig. 3. Changes in gut microbial diversity in the two groups. (A) The α-diversity, measured by Chao 1 index. (B) The β-diversity, measured by Bray-Curtis distance. Each bar indicates the distance between different visits (baseline vs. week 12, baseline vs. week 14, and week 12 vs. week 14) within each group (probiotics vs. placebo).

Microbiota characteristics
The relative abundance of the dominant taxa was analyzed at the phylum and genus levels (Fig. 4). At the phylum level, Bacteroidetes, Firmicutes, Proteobacteria, Actinobacteria, Verrucomicrobia, Fusobacteria, Cyanobacteria, and Tenericutes were detected in both the probiotics and placebo groups at baseline. Bacteroidetes was the most dominant microbe with an abundance of 45%–52%, followed by Firmicutes (36%–40%). At baseline, there was no statistically significant difference between the two groups at the phylum level (Fig. 4A). At the genus level, Bacteroides, Faecalibacterium, Prevotella, unclassified Ruminococcaceae, unclassified Clostridiales, and Sutterella were detected in both the probiotics and placebo groups at baseline, with Bacteroides being the most dominant microbe at 45%–46% abundance. Throughout the 12-week period, the relative abundance of Faecalibacterium and Prevotella (at the genus level) increased in both the probiotics and placebo groups, while that of unclassified Ruminococcaceae, unclassified Clostridiales, Sutterella, and unclassified Lachnospiraceae decreased in both groups (Fig. 4B).
Fig. 4. Relative abundance of dominant bacteria in gut microbiota in the two groups. (A) Phyla and (B) Genera levels.

Use of topical steroids
A total of 42 subjects whose AD symptoms were not managed, including 18 (44%) from the probiotics group and 24 (59%) from the placebo group, were given equal amounts of topical steroids. After the intervention period, the number of subjects whose symptoms were not managed was 10 (24%) in the probiotics group and 19 (46%) in the placebo group.
The mean weight of fluticasone propionate remaining in the tubes was 1.66 ± 3.29 g in the probiotics group and 2.99 ± 4.13 g in the placebo group at baseline (P = 0.111). When comparing the total weight of steroids used, there was no significant difference between the two groups (7.23 ± 6.22 g vs. 9.84 ± 9.37 g, respectively; P = 0.314) (data not shown).
Subgroup: allergic sensitization, age, and AD severity
Stratification of subjects by allergic sensitization, age, and AD severity indicated differences in changes in the SCORAD indices (Table 5).
Table 5. Changes in SCORAD indices of the probiotics and placebo groups with subgroup for allergic sensitization, age, and AD severity.
| Subgroups | Probiotics | Placebo | P value | ||
|---|---|---|---|---|---|
| IgE | |||||
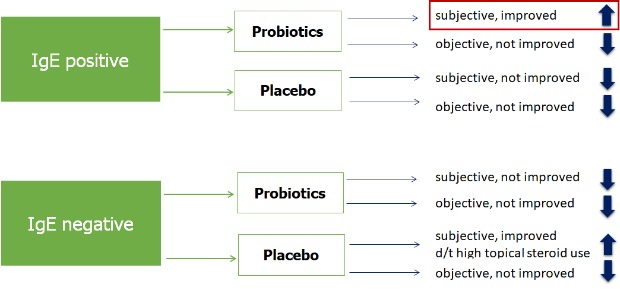
| Sensitized (n = 43) | |||||
| Objective | 5.6 ± 9.8 | 3.8 ± 8.0 | 0.724 | ||
| Subjective | 2.7 ± 3.6 | 0.9 ± 3.0 | 0.019 | ||
| Non-sensitized (n = 39) | |||||
| Objective | 7.8 ± 6.8 | 10.4 ± 0.9 | 0.148 | ||
| Subjective | 0.9 ± 3.0 | 3.4 ± 3.3 | 0.013 | ||
| Age | |||||
| ≤ 6 yr (n = 59) | |||||
| Objective | 6.1 ± 9.3 | 8.0 ± 8.5 | 0.752 | ||
| Subjective | 2.7 ± 3.7 | 1.6 ± 2.9 | 0.131 | ||
| > 6 yr (n = 23) | |||||
| Objective | 2.2 ± 10.4 | 7.8 ± 9.0 | 0.288 | ||
| Subjective | 1.4 ± 3.5 | 2.4 ± 3.1 | 0.659 | ||
| AD severity | |||||
| Mild (n = 26) | |||||
| Objective | 2.7 ± 5.1 | 2.8 ± 5.4 | 0.910 | ||
| Subjective | 1.6 ± 4.2 | 1.8 ± 2.7 | 0.989 | ||
| Moderate (n = 56) | |||||
| Objective | 7.1 ± 11.4 | 9.3 ± 8.8 | 0.918 | ||
| Subjective | 3.0 ± 3.2 | 1.9 ± 3.1 | 0.222 | ||
Data are expressed as means ± standard deviation.
SCORAD = scoring of atopic dermatitis, AD = atopic dermatitis, IgE = immunoglobulin E.
Compared between groups; P value by analysis of covariance adjusted by baseline.
In IgE sensitized AD, the mean SCORAD indices were 32.0 ± 9.4 and 35.5 ± 8.5 for the probiotics and placebo groups, respectively, at baseline (P = 0.222). However, the mean subjective scores of SCORAD indices at week 12 for the probiotics group were 10.4 ± 3.4, which was significantly lower than that at baseline (P = 0.001). Moreover, the mean subjective scores of SCORAD indices at week 12 for the probiotics group were significantly lower than that for the placebo group in IgE sensitized AD (P = 0.019) (Table 5). In contrast, it was lower in the placebo group than in the probiotics group in non-sensitized AD. The proportion of subjects who used topical steroids in the placebo group (64%) was approximately double than that in the probiotics group (29%), with the difference being significant (P = 0.034) (data not shown). However, there were no significant difference in changes in the SCORAD indices by age group between the probiotics and placebo groups. Similarly, the SCORAD indices by AD severity subgroups did not show any significant differences between the two groups (Table 5). There were no significant differences in α-diversity, β-diversity, and microbiota relative abundances between the probiotics and placebo groups among those with specific IgE sensitized AD (data not shown).
DISCUSSION
This was a double-blinded, placebo-controlled, randomized study to investigate the clinical and immunological effects of L. pentosus in children with mild to moderate AD. The following are the main findings: 1) clinical improvements were observed regardless of probiotics administration; 2) oral administration of L. pentosus did not alter serum cytokine levels; 3) the diversity of the gut microbiome was not significantly changed by probiotics administration; and 4) the mean subjective scores of SCORAD indices at week 12 for the probiotics group were significantly lower than those for the placebo group with IgE sensitized AD.
The neonatal immune system is shifted towards a Th2 response, and exposure to various common allergens after birth results in the maturation of Th1, Th2, Th17, and Treg cells.15 The gut microbiota plays an important role in mucosal immune system signaling, and gut dysbiosis alters immune regulation and precedes allergic diseases.16,17 Alteration of the gut microbiota by probiotics administration is expected to be an effective means of preventing AD from occurring. However, the therapeutic effects on AD have been inconclusive.18,19,20
L. pentosus, the main colonizer of the human intestines, is an anaerobic, non-sporulating, gram-positive bacterium extracted from fermented foods.21,22 L. pentosus functions in the production of mucosal IgA,23 and leads to increased levels of IL-10 and Foxp3+, which are involved in balancing the Th1/Th2 ratio, as well as suppressing IL-4.8,9 In house dust mite-sensitized AD mice, L. pentosus also reduced IL-4 and induced splenic regulatory B10 cells to produce IL-10.9
However, in this study, no statistically significant differences were observed in clinical severity, cytokine levels, microbial diversity, or the relative abundance of the gut microbiota between the probiotics and placebo groups. Factors that could have influenced these results are as follows. First, a single strain of L. pentosus was investigated in this study. In a previous study,7 a single strain showed clinical improvement in 7 out of 12 cases (58%), and mixed strains showed improvement in 8 out of 9 cases (89%). Previous meta-analyses on the effects of probiotics have also found that mixed strains improved the SCORAD index better than single strains.18,20,24,25 We studied a single strain in this analysis, but clinical severity decreased significantly over time in both groups, with no significant difference in the strength of this effect. Further research is needed to determine the synergistic effects of mixed strains of bacteria in modulating the gut microbiota and immune system. Second, the mean age in this study was older than that of patients in previous studies.26,27 The human intestinal microbiota evolves with age and stabilizes after 3 years of life.28 At birth, the gastrointestinal tract of the newborn is sterile, and the developing microflora in the early postnatal period is involved in the activation of innate and adaptive immunity.29 The infant microbiota structure is highly unstable and has low diversity compared to that of the adult.30,31 In this study, the mean age was over 3 years, and the duration of the disease was longer than that of studies conducted in infants. Thus, it is possible that the immune system is still under development in infants and that immunologic modulation by probiotics is less likely in children than in infants. Third, although a 12-week period is sufficient for assessing treatment efficacy, it may have been too short to induce alterations in the gut microbiota. A study on the prevention of AD showed a high diversity of the microbiota after 3 months of probiotics administration.32 A recent study identified an inverse relationship between SCORAD index and probiotics administration, indicating that probiotics administration influences the composition of the gut microbiota and functional changes.33
To the best of our knowledge, this is the first study to assess improvements in clinical severity and alterations in the gut microbiome in AD treatment in children. However, we found no significant difference in microbial diversity or relative abundance. Further investigation will be needed for longer periods of administration of L. pentosus.
Consistent with our results, many randomized clinical trials that have examined the effects of probiotics on AD did not find a positive effect in the entire study population.26,34,35,36,37,38 In several of these studies, however, the SCORAD index in IgE sensitized AD was significantly improved in the probiotics group.26,34,35,36 In our study, L. pentosus had a positive effect on the improvement of subjective symptoms only in IgE sensitized AD, and such improvement in IgE sensitized AD was lower in the placebo group than in the probiotics group. It is difficult to determine that the clinical significance was only based on the differences in the subjective scores of the SCORAD index between the two groups after probiotics administration. Further large-scale study is needed to find a clinical significance of probiotics in AD. These results suggest that the effects of probiotics may differ depending on the IgE sensitization of each subject. In the future, probiotics may be helpful in relieving symptoms when administered to subjects with IgE sensitized AD.
There are, however, several limitations to be considered. First, the potential effects of the additional intake of other fermented foods could not be excluded in this study. Although we provided instructions to minimize contamination from the intake of other probiotics, we could not completely prevent subjects from consuming fermented foods that contain various probiotics. In the future, more detailed instructions should be provided to reduce the dietary intake of probiotics. Second, the mean SCORAD indices at baseline were higher in the placebo group than in the probiotics group despite randomization; however, these were corrected for in the statistical analyses. Third, the mean subjective SCORAD indices were lower in the placebo group than in the probiotics group in non-sensitized AD. This is probably related to the difference in the proportion of subjects who used topical steroids and the amount of topical steroids used. In our study, the proportion of subjects who used topical steroids in the placebo group was higher than that in the probiotics group, with the difference being significant and the amount of topical steroids used for the placebo group being higher than that of the probiotics group in non-sensitized AD (data not shown). Fourth, in this study, allergen tests on two food allergens and one inhalant allergen were performed. The number of allergens was not enough to define allergen-sensitized AD. The results with subgroup for sensitization to each allergen were added, but there were no differences significantly (Supplementary Table 1). Finally, in the present study, we used the single dose of L. pentosus. It would have been better if our study was conducted to assess the dose-response relationship between our probiotics and AD severity. However, dose-response relationships of probiotics in terms of prevention or treatment of AD has not been reported yet. One animal study conducted with various doses of probiotics revealed that there is dose-response relationship between the probiotics and AD severity.39
In conclusion, subjective symptoms indicate that the degree of itching and the itch are caused by chemical mediators secreted by various inflammatory cells. Although there was no statistically significant change in cytokine levels in this study, the subjective symptoms of the IgE sensitized subgroup were improved. Therefore, it is believed that L. pentosus may be effective in allergen-sensitized AD and probiotics administration might be helpful in relieving symptoms in allergen-sensitized AD.
ACKNOWLEDGMENTS
The authors thank the field workers and other staff who supported in the data collection, and all the parents and children who participated in this study.
Footnotes
Funding: This study was supported by Main Research Program (E0170400-01) of the Korea Food Research Institute (KFRI) funded by the Ministry of Science and ICT, by Environmental Health Center for Childhood Asthma funded by the Ministry of Environment, Korea, by Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Science, Korea (NRF-2018R1A6A3A11049961, NRF-2019R1F1A1041169).
Disclosure: The authors have no potential conflicts of interest to disclose.
- Conceptualization: Yoo Y.
- Data curation: Lee SY, Shin HS.
- Formal analysis: Lee SY, Ahn SH, Lim MY, Nam YD.
- Investigation: Ahn SH.
- Writing - original draft: Ahn SH.
- Writing - review & editing: Ahn SH, Yoon W, Yoo Y.
SUPPLEMENTARY MATERIAL
Changes in SCORAD indices of the probiotics and placebo groups with subgroup for sensitization to each allergen
References
- 1.Leung DY, Boguniewicz M, Howell MD, Nomura I, Hamid QA. New insights into atopic dermatitis. J Clin Invest. 2004;113(5):651–657. doi: 10.1172/JCI21060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Schneider L, Tilles S, Lio P, Boguniewicz M, Beck L, LeBovidge J, et al. Atopic dermatitis: a practice parameter update 2012. J Allergy Clin Immunol. 2013;131(2):295–299.e1. doi: 10.1016/j.jaci.2012.12.672. [DOI] [PubMed] [Google Scholar]
- 3.Thomsen SF. Atopic dermatitis: natural history, diagnosis, and treatment. ISRN Allergy. 2014;2014:354250. doi: 10.1155/2014/354250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lee SY, Lee E, Park YM, Hong SJ. Microbiome in the gut-skin axis in atopic dermatitis. Allergy Asthma Immunol Res. 2018;10(4):354–362. doi: 10.4168/aair.2018.10.4.354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Abrahamsson TR, Jakobsson HE, Andersson AF, Björkstén B, Engstrand L, Jenmalm MC. Low diversity of the gut microbiota in infants with atopic eczema. J Allergy Clin Immunol. 2012;129(2):434–440. doi: 10.1016/j.jaci.2011.10.025. [DOI] [PubMed] [Google Scholar]
- 6.Song H, Yoo Y, Hwang J, Na YC, Kim HS. Faecalibacterium prausnitzii subspecies-level dysbiosis in the human gut microbiome underlying atopic dermatitis. J Allergy Clin Immunol. 2016;137(3):852–860. doi: 10.1016/j.jaci.2015.08.021. [DOI] [PubMed] [Google Scholar]
- 7.Rather IA, Bajpai VK, Kumar S, Lim J, Paek WK, Park YH. Probiotics and atopic dermatitis: an overview. Front Microbiol. 2016;7:507. doi: 10.3389/fmicb.2016.00507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nonaka Y, Izumo T, Izumi F, Maekawa T, Shibata H, Nakano A, et al. Antiallergic effects of Lactobacillus pentosus strain S-PT84 mediated by modulation of Th1/Th2 immunobalance and induction of IL-10 production. Int Arch Allergy Immunol. 2008;145(3):249–257. doi: 10.1159/000109294. [DOI] [PubMed] [Google Scholar]
- 9.Bae MJ, Kim HK, Lim S, Lee SY, Shin HS, Kim JE, et al. Lactobacillus pentosus KF340 alleviates house dust mite-induced murine atopic dermatitis via the secretion of IL-10-producing splenic B10 cells. J Funct Foods. 2016;26:258–267. [Google Scholar]
- 10.Kim J, Lee BS, Kim B, Na I, Lee J, Lee JY, et al. Identification of atopic dermatitis phenotypes with good responses to probiotics (Lactobacillus plantarum CJLP133) in children. Benef Microbes. 2017;8(5):755–761. doi: 10.3920/BM2017.0034. [DOI] [PubMed] [Google Scholar]
- 11.Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol (Stockh) 1980;60(92):S44–7. [Google Scholar]
- 12.Stadler JF. Severity scoring of atopic dermatitis: the SCORAD index. Consensus Report of the European Task Force on Atopic Dermatitis. Dermatology. 1993;186(1):23–31. doi: 10.1159/000247298. [DOI] [PubMed] [Google Scholar]
- 13.Garcia Bartels N, Scheufele R, Prosch F, Schink T, Proquitté H, Wauer RR, et al. Effect of standardized skin care regimens on neonatal skin barrier function in different body areas. Pediatr Dermatol. 2010;27(1):1–8. doi: 10.1111/j.1525-1470.2009.01068.x. [DOI] [PubMed] [Google Scholar]
- 14.Caporaso JG, Kuczynski J, Stombaugh J, Bittinger K, Bushman FD, Costello EK, et al. QIIME allows analysis of high-throughput community sequencing data. Nat Methods. 2010;7(5):335–336. doi: 10.1038/nmeth.f.303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ji GE. Probiotics in primary prevention of atopic dermatitis. Forum Nutr. 2009;61:117–128. doi: 10.1159/000212744. [DOI] [PubMed] [Google Scholar]
- 16.Wang IJ, Wang JY. Children with atopic dermatitis show clinical improvement after Lactobacillus exposure. Clin Exp Allergy. 2015;45(4):779–787. doi: 10.1111/cea.12489. [DOI] [PubMed] [Google Scholar]
- 17.Niccoli AA, Artesi AL, Candio F, Ceccarelli S, Cozzali R, Ferraro L, et al. Preliminary results on clinical effects of probiotic Lactobacillus salivarius LS01 in children affected by atopic dermatitis. J Clin Gastroenterol. 2014;48(Suppl 1):S34–S36. doi: 10.1097/MCG.0000000000000233. [DOI] [PubMed] [Google Scholar]
- 18.Kim SO, Ah YM, Yu YM, Choi KH, Shin WG, Lee JY. Effects of probiotics for the treatment of atopic dermatitis: a meta-analysis of randomized controlled trials. Ann Allergy Asthma Immunol. 2014;113(2):217–226. doi: 10.1016/j.anai.2014.05.021. [DOI] [PubMed] [Google Scholar]
- 19.Boyle RJ, Bath-Hextall FJ, Leonardi-Bee J, Murrell DF, Tang ML. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;8(4):CD006135. doi: 10.1002/14651858.CD006135.pub2. [DOI] [PubMed] [Google Scholar]
- 20.Huang R, Ning H, Shen M, Li J, Zhang J, Chen X. Probiotics for the treatment of atopic dermatitis in children: a systematic review and meta-analysis of randomized controlled trials. Front Cell Infect Microbiol. 2017;7:392. doi: 10.3389/fcimb.2017.00392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shimosato T, Tomida K, Otani H. Effect of Lactobacillus pentosus ONRIC b0240 on intestinal IgA production in mice fed differing levels of protein. J Agric Food Chem. 2011;59(6):2646–2651. doi: 10.1021/jf104240d. [DOI] [PubMed] [Google Scholar]
- 22.Shimizu K, Sato H, Suga Y, Yamahira S, Toba M, Hamuro K, et al. The effects of Lactobacillus pentosus strain b240 and appropriate physical training on salivary secretory IgA levels in elderly adults with low physical fitness: a randomized, double-blind, placebo-controlled trial. J Clin Biochem Nutr. 2014;54(1):61–66. doi: 10.3164/jcbn.13-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kotani Y, Kunisawa J, Suzuki Y, Sato I, Saito T, Toba M, et al. Role of Lactobacillus pentosus Strain b240 and the Toll-like receptor 2 axis in Peyer's patch dendritic cell-mediated immunoglobulin A enhancement. PLoS One. 2014;9(3):e91857. doi: 10.1371/journal.pone.0091857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chang YS, Trivedi MK, Jha A, Lin YF, Dimaano L, García-Romero MT. Synbiotics for prevention and treatment of atopic dermatitis: a meta-analysis of randomized clinical trials. JAMA Pediatr. 2016;170(3):236–242. doi: 10.1001/jamapediatrics.2015.3943. [DOI] [PubMed] [Google Scholar]
- 25.Dang D, Zhou W, Lun ZJ, Mu X, Wang DX, Wu H. Meta-analysis of probiotics and/or prebiotics for the prevention of eczema. J Int Med Res. 2013;41(5):1426–1436. doi: 10.1177/0300060513493692. [DOI] [PubMed] [Google Scholar]
- 26.Rosenfeldt V, Benfeldt E, Nielsen SD, Michaelsen KF, Jeppesen DL, Valerius NH, et al. Effect of probiotic Lactobacillus strains in children with atopic dermatitis. J Allergy Clin Immunol. 2003;111(2):389–395. doi: 10.1067/mai.2003.389. [DOI] [PubMed] [Google Scholar]
- 27.Gerasimov SV, Vasjuta VV, Myhovych OO, Bondarchuk LI. Probiotic supplement reduces atopic dermatitis in preschool children: a randomized, double-blind, placebo-controlled, clinical trial. Am J Clin Dermatol. 2010;11(5):351–361. doi: 10.2165/11531420-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 28.Gensollen T, Blumberg RS. Correlation between early-life regulation of the immune system by microbiota and allergy development. J Allergy Clin Immunol. 2017;139(4):1084–1091. doi: 10.1016/j.jaci.2017.02.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Meneghin F, Fabiano V, Mameli C, Zuccotti GV. Probiotics and atopic dermatitis in children. Pharmaceuticals (Basel) 2012;5(7):727–744. doi: 10.3390/ph5070727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Arrieta MC, Stiemsma LT, Amenyogbe N, Brown EM, Finlay B. The intestinal microbiome in early life: health and disease. Front Immunol. 2014;5:427. doi: 10.3389/fimmu.2014.00427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Claesson MJ, Cusack S, O'Sullivan O, Greene-Diniz R, de Weerd H, Flannery E, et al. Composition, variability, and temporal stability of the intestinal microbiota of the elderly. Proc Natl Acad Sci U S A. 2011;108(Suppl 1):4586–4591. doi: 10.1073/pnas.1000097107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Nylund L, Nermes M, Isolauri E, Salminen S, de Vos WM, Satokari R. Severity of atopic disease inversely correlates with intestinal microbiota diversity and butyrate-producing bacteria. Allergy. 2015;70(2):241–244. doi: 10.1111/all.12549. [DOI] [PubMed] [Google Scholar]
- 33.Fang Z, Lu W, Zhao J, Zhang H, Qian L, Wang Q, et al. Probiotics modulate the gut microbiota composition and immune responses in patients with atopic dermatitis: a pilot study. Eur J Nutr. 2019 doi: 10.1007/s00394-019-02061-x. [DOI] [PubMed] [Google Scholar]
- 34.Sistek D, Kelly R, Wickens K, Stanley T, Fitzharris P, Crane J. Is the effect of probiotics on atopic dermatitis confined to food sensitized children? Clin Exp Allergy. 2006;36(5):629–633. doi: 10.1111/j.1365-2222.2006.02485.x. [DOI] [PubMed] [Google Scholar]
- 35.Viljanen M, Savilahti E, Haahtela T, Juntunen-Backman K, Korpela R, Poussa T, et al. Probiotics in the treatment of atopic eczema/dermatitis syndrome in infants: a double-blind placebo-controlled trial. Allergy. 2005;60(4):494–500. doi: 10.1111/j.1398-9995.2004.00514.x. [DOI] [PubMed] [Google Scholar]
- 36.van der Aa LB, Heymans HS, van Aalderen WM, Sillevis Smitt JH, Knol J, Ben Amor K, et al. Effect of a new synbiotic mixture on atopic dermatitis in infants: a randomized-controlled trial. Clin Exp Allergy. 2010;40(5):795–804. doi: 10.1111/j.1365-2222.2010.03465.x. [DOI] [PubMed] [Google Scholar]
- 37.Grüber C, Wendt M, Sulser C, Lau S, Kulig M, Wahn U, et al. Randomized, placebo-controlled trial of Lactobacillus rhamnosus GG as treatment of atopic dermatitis in infancy. Allergy. 2007;62(11):1270–1276. doi: 10.1111/j.1398-9995.2007.01543.x. [DOI] [PubMed] [Google Scholar]
- 38.Fölster-Holst R, Müller F, Schnopp N, Abeck D, Kreiselmaier I, Lenz T, et al. Prospective, randomized controlled trial on Lactobacillus rhamnosus in infants with moderate to severe atopic dermatitis. Br J Dermatol. 2006;155(6):1256–1261. doi: 10.1111/j.1365-2133.2006.07558.x. [DOI] [PubMed] [Google Scholar]
- 39.Won TJ, Kim B, Lee Y, Bang JS, Oh ES, Yoo JS, et al. Therapeutic potential of Lactobacillus plantarum CJLP133 for house-dust mite-induced dermatitis in NC/Nga mice. Cell Immunol. 2012;277(1-2):49–57. doi: 10.1016/j.cellimm.2012.05.013. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Changes in SCORAD indices of the probiotics and placebo groups with subgroup for sensitization to each allergen