

Abstract
Background:
Eliminating racial/ethnic disparities in physical activity remains a challenge in the United States. South Asian immigrants in the United States have particularly low physical activity levels, and evidence suggests that social context may be important. This study examined associations between personal social networks and moderate to vigorous leisure-time physical activity (MVPA) among South Asians in the United States.
Methods:
We used cross-sectional data (2014–2017) from 689 South Asians (aged 43–85 y) who participated in the Mediators of Atherosclerosis in South Asians Living in America study. Self-reported physical activity and egocentric network data were collected from participants about their network members. Regression models were used to determine associations between social network characteristics and participants’ MVPA.
Results:
Participants were on average 59 years old (SD = 9) and reported 1335 metabolic equivalent minutes per week of MVPA (interquartile range = 735, 2212). Having network members who exercised or who were exercise partners associated with increased MVPA in men (β coefficient = 241 MET min/wk [95% confidence interval, 63 to 419] and β = 520 MET min/wk [95% confidence interval, 322 to 718], respectively). For women, the association was only significant if the exercise partner was a spouse.
Conclusion:
Physical activity interventions utilizing network members as exercise partners may have potential in South Asians but must consider gender differences.
Keywords: Asian American, social support, gender, exercise
Regular physical activity is one of the most important actions individuals can take to improve their health, and promotion of regular physical activity is a national public health priority.1
Only 50% of American adults get the recommended amount of physical activity, and racial/ethnic minorities may be at even greater risk for physical inactivity.1 Despite efforts to improve the physical activity of all Americans, there is evidence that current strategies focused on increasing physical activity may not be reaching minority populations.2 A key gap is that most interventions focus on individual-level change and do not consider the social context in which physical activity is encouraged or constrained3,4 or how interpersonal relationships could motivate physical activity.5 To address these gaps and improve the effectiveness of physical activity promotion efforts, an important area of inquiry is to determine how and to what extent social relationships influence physical activity in high-risk minority populations.
One particularly high-risk and understudied group is South Asians (individuals from India, Pakistan, Bangladesh, Sri Lanka, and Nepal). People of South Asian descent are one of the fastest growing segments of the US population, with current population estimates approaching 5 million residents of South Asian origin.6 South Asians have an elevated risk for coronary heart disease and diabetes mellitus7 compared with non-Hispanic whites and most other Asian groups. A well-documented, modifiable contributor to South Asians’ increased cardiovascular and diabetes risk is low physical activity.8,9 Studies indicate that South Asians are some of the least physically active adults in the United States.9,10 The majority of South Asians in the United States are immigrants,11 and studies of South Asian migrants in different countries suggest that there may be important social and cultural influences on this group’s motivation for physical activity.12,13
For many South Asians, the usual framing of exercise, in terms of individual self-efficacy and benefit, may be mismatched to community values that emphasize family and community relationships and considering the needs of others before one’s own.14,15 For example, a study in the United Kingdom found that participating in physical activity with friends and family was an important motivator for South Asians.9 Social influence theories suggest that interpersonal relationships primarily influence physical activity through peer modeling, imitation, and social learning.16 In our prior qualitative work, South Asian women described a lack of role models which reduced motivation and self-efficacy for physical activity. Established social and cultural norms are another mechanism of social influence, and in our prior work, South Asian women were less likely to participate in intentional physical activity or exercise because it was perceived as a “Western behavior” by their families and community.17 Clearly, family, friends, and community influence physical activity through multiple pathways, including establishing social norms and values, role modeling, and the provision of social support.18–20
Family and peers’ social support for physical activity enhances motivation and planning for physical activity in adolescents.21 Social support is potentially modifiable and may also be salient for South Asian adults, who in general, are collectively oriented and define themselves in terms of their interconnectedness and relationships with family and community.22,23 Thus, when faced with a need for behavior change, a collective approach to addressing the behavior that involves family, friends, or community may be particularly effective.24
The goal of this study was to examine the association between South Asians’ personal social networks and moderate to vigorous leisure-time physical activity (MVPA) levels, using cross-sectional data from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) cohort study.25 This study extends current literature by specifically examining how physical activity behaviors of personal network members associate with South Asians’ physical activity, if differences exist between men and women in how social networks influence activity, and generating new knowledge to inform evidence-based health promotion interventions for racial/ethnic minority communities.
Methods
Study Population
The MASALA study is a community-based cohort of South Asians without known cardiovascular disease at baseline, who are being prospectively followed for development of clinical cardiovascular disease.25 Study participants were recruited for the baseline exam between October 2010 and March 2013 from the San Francisco Bay Area through the University of California, San Francisco and the greater Chicago Area through Northwestern University. Briefly, to be eligible, participants had to (1) self-identify as South Asian; (2) be between 40 and 84 years and (3) have the ability to speak and/or read English, Hindi, or Urdu. The study excluded those who had a physician-diagnosed heart attack, stroke or transient ischemic attack, heart failure, angina, use of nitroglycerin, a history of cardiovascular disease procedures or any surgery on the heart or arteries, current atrial fibrillation, or in active treatment for cancer. Details regarding the MASALA study cohort’s baseline exam and methods have been published previously.25
From 2014 to 2017, all surviving MASALA study participants were reenrolled for a second study visit (Figure 1), where social network characteristics were measured using a standard egocentric approach that examined the network members (alters) reported by the respondent (ego). The visit included a 2-hour interview about the ego’s personal social network; survey measures of ego’s physical activity and diet; and physical exam measurements (blood pressure, height, and weight).26 The data collection for the social networks study did not include any blood draws or imaging procedures, and most visits were conducted in convenient community locations or in the participant’s home.
Figure 1 —
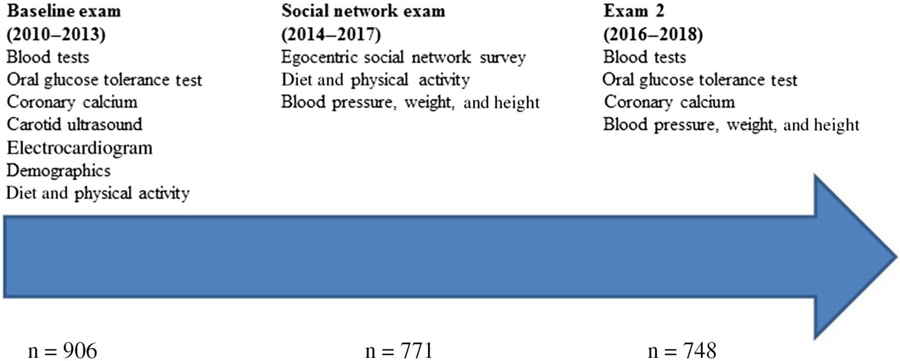
MASALA study exams and measures. MASALA indicates Mediators of Atherosclerosis in South Asians Living in America.
Participants were administered a social networks questionnaire adapted from the National Social Life, Health, and Aging Project’s social networks module.27 The MASALA study social network module was designed as a one-time interview to elicit information on the egos’ personal social network. The surveys were administered in-person in English, Hindi, or Urdu. The design and methods of the MASALA social networks ancillary study have been published previously.26 In brief, interviewers asked each participant (ego) the following question, “Looking back over the last 12 months, who are the people you talk with most often about things that are important to you?” This question has been shown to elicit personal network members (alters) who have potential to exert social influences on the ego. Egos could list up to 10 network members. If the ego listed more than 5 network members, additional information was only collected on the first 5 alters using name interpreter questions. Name interpreter questions are used to characterize the type of relationships (eg, spouse or significant other, friend); sociodemographic characteristics (eg, age, country of birth); strength of relationship (emotional closeness, frequency of contact); functions (eg, social support); and health behaviors of alters.26 There were 103 questions in the social network module, and 15 were specifically related to ego’s perceptions of alters’ exercise behaviors and attitudes. Limiting the name interpreter questions to the first 5 alters is an established approach used to reduce participant burden and interview time.28 The study protocol and procedures were approved by institutional review boards at Northwestern University and University of California, San Francisco, and all study participants signed informed consent.
Measures
The main exposures of interest were alters’ exercise behaviors; this information was collected from egos during the social networks ancillary study (Figure 1). Egos were asked to report on each alter’s exercise behaviors, if they ever exercised with the alter, and if so, how frequently the ego and alter exercised together. Egos were asked, “In the last 12 months, how often did [alter name] exercise?” Next, they were asked, “In the last 12 months, how often did you and [alter name] exercise together.”25 The ego was asked to respond with the time frame options of: “daily or almost daily (≥5 ×/week),” “weekly,” “monthly,” “few times a year (1–11),” “never,” and “don’t know.”25 Alters were categorized as nonexercisers if the ego reported that the alter did not exercise; 2.5% (n = 74/2934 named alters) were categorized as don’t know, which was grouped with missing data (0.2%). Alters who did any exercise were categorized as “exercising alters,” and alters who exercised with the ego were categorized as “exercise partners.” Among the 2553 alters who the egos said they exercise with, there was no one with “don’t know/missing” for “how often?”
The focus of this study was on physical activity, defined as nonessential activities of daily living, such as walking for exercise, dancing, sports, and swimming.29 The primary outcome was the ego’s self-reported MVPA over the past 6 months. Physical activity was self-reported and measured with the validated Cross-Cultural Activity Participation Study.30 MVPA was defined as activity that required at least 3 metabolic equivalents (METs). In contrast, 1 MET is the energy consumed while sitting quietly.29 Egos’ MVPA levels were calculated as MET minutes per week and were examined in relation to both ego and alter characteristics. Data on physical activity were collected at the social networks ancillary study visit. Both the main exposure and outcome were from the social network ancillary study visit (Figure 1), and we did not examine physical activity data from the baseline MASALA study visit because those data were collected 3 years prior to the social network ancillary study visit.
Information on egos’ age, gender, education, income, marital status, and traditional cultural beliefs were collected at the baseline study visit (2010–2013) as previously described25 and were included as covariates in regression models. We also included self-rated health, which was measured at the social networks visit by asking egos to rate their health on a continuous scale of 1 to 10, with 1 being poor health and 10 being excellent health. Study site (San Francisco or Chicago) was also included as a covariate.
Statistical Analysis
We calculated descriptive statistics for all variables of interest, including participant (ego) characteristics and MVPA level; social network characteristics (eg, network size, density31); and alters’ characteristics and exercise behaviors. We conducted bivariate analyses to examine the associations between ego MVPA and these characteristics using Pearson correlation coefficient for continuous exposures, t tests for binary variables, and analysis of variance for categorical variables. Informed by bivariate results, we conducted multivariable linear regression. Data analysis was conducted in 2018.
We utilized a linear regression model in which we regressed the outcome, ego MVPA (in MET minutes per week), on number of exercise partners, number of exercising alters, total number of alters, and covariates. By leaving the variable “number of nonexercising alters” out of the regression model, we are able to examine the effect of substituting an exercise partner or an exercising alter in place of a nonexercising alter while holding constant the total number of alters. We fit a partially adjusted model using study site and network size as covariates and a fully adjusted model using site, ego age, education, income, marital status, level of traditional South Asian cultural beliefs, and self-rated health as covariates. Initial analyses revealed important gender differences, and all analyses were stratified by gender. (Thus, there are 2 partially adjusted models and 2 fully adjusted models.)
Additional post hoc analyses were completed to explore potential explanations for gender differences in the association between social network characteristics and MVPA. We conducted descriptive analyses of alters who were exercise partners, exercising alters, and alters who did not exercise, stratified by ego gender. We examined the type of relationship (eg, spouse, friend); closeness of relationship; alter age and education; difference in age between ego and alter, alter gender (whether it was the same as ego); and coresident status. We then ran additional regression models where exercise partners were decomposed as spouse exercise partners and nonspouse exercise partners. All analyses were limited to the MASALA study participants who completed the social network module and who self-reported any level of MVPA greater than 0 MET minute per week (n = 689, 89% of total 771 participants). Of the 82 participants excluded from the study, 81 participants (10.5% of total 771 participants) reported MVPA equal to 0 MET minute per week and 1 participant (0.1% of total 771 participants) had a missing MVPA variable in data collection.
Results
Overall, the egos’ average age was 59 years (SD = 9), and 44% were female. The majority of egos were married (89%), had high education and income levels, and high self-reported health (Table 1). Among male egos, the median MVPA level was 1361 MET minutes per week (interquartile range = 735, 2318), and for female egos, median MVPA was 1267 MET minutes per week (interquartile range = 735, 2145). The overall average social network size was 4.3 alters (SD = 1.1). South Asian social networks were dense, and a majority of network members (71%) were kin.
Table 1.
Participant (Ego) and Social Network Characteristics in the MASALA Study Sample (2014–2017)
| Male (n = 384) |
Female (n = 305) |
Overall (n = 689) |
|
|---|---|---|---|
| Characteristics | Mean (SD) | Mean (SD) | Mean (SD) |
| Age, y | 60.2 (9.7) | 58.0 (8.6) | 59.2 (9.3) |
| Study site: northwestern, n (%) | 169 (44.7) | 102 (34.7) | 271 (40.3) |
| Married/cohabitating, n (%) | 357 (94.4) | 244 (83.0) | 601 (89.4) |
| Education category, n (%) | |||
| ≤High school | 13 (3.4) | 20 (6.8) | 33 (4.9) |
| <Bachelor’s degree | 15 (4.0) | 15 (5.1) | 30 (4.5) |
| Bachelor’s degree | 88 (23.3) | 90 (30.6) | 178 (26.5) |
| >Bachelor’s degree | 262 (69.3) | 169 (57.5) | 431 (64.1) |
| Income category,a n (%) | |||
| <$40k | 33 (8.8) | 29 (9.8) | 62 (9.2) |
| $40–75k | 53 (14.1) | 31 (10.5) | 84 (12.5) |
| $75–100k | 30 (8.0) | 35 (11.9) | 65 (9.7) |
| >100k | 260 (69.1) | 200 (67.8) | 460 (68.6) |
| BMI,b kg/m2 | 26.3 (3.8) | 26.6 (4.4) | 26.4 (4.1) |
| Self-reported healthc (1 = low to 10 = high) | 7.9 (1.4) | 7.8 (1.4) | 7.9 (1.4) |
| Self-reported exercise, median (interquartile range), MET min/wk | 1361 (735, 2318) | 1267 (735, 2145) | 1358 (735, 2220) |
| Sum of cultural tradition measures (0 = traditional to 28 = nontraditional) | 14.2 (6.1) | 14.5 (6.1) | 14.3 (6.1) |
| Social network characteristics | |||
| Network size | 4.2 (1.1) | 4.3 (1.1) | 4.3 (1.1) |
| Proportion kin | 0.71 (0.29) | 0.72 (0.28) | 0.71 (0.28) |
| Proportion female | 0.48 (0.24) | 0.64 (0.24) | 0.55 (0.25) |
| Density | 0.79 (0.26) | 0.78 (0.27) | 0.78 (0.27) |
| Proportion South Asian | 0.87 (0.25) | 0.90 (0.21) | 0.88 (0.23) |
Abbreviations: BMI, body mass index; MASALA, Mediators of Atherosclerosis in South Asians Living in America; MET, metabolic equivalent.
n: male = 376, female = 295, and overall = 671.
n: male = 381, female = 302, and overall = 683.
n: male = 384, female = 303, and overall = 687.
Among male egos, there were differences in effect sizes depending on whether the alter was an “exercising alter” or an “exercise partner” (Table 2). Replacing a nonexercising alter in a male ego’s network with an alter who is an exercise partner increased the ego’s MVPA by 520 MET minutes per week (95% confidence interval [CI], 322 to 718). Among male egos, replacing a nonexercising alter in the network with an exercising alter (who is not an exercise partner) increased MVPA by 241 MET minutes per week (95% CI, 63 to 419). Results for women were not significant (Table 2).
Table 2.
Association of Alter Exercise With Egos’ Moderate to Vigorous Physical Activity (in MET Minutes per Week) in the MASALA Study
| Parameter | Male |
Female |
||
|---|---|---|---|---|
| Estimate | 95% confidence interval | Estimate | 95% confidence interval | |
| Intercept | 1213 | 558 to 1867 | 1214 | 506 to 1923 |
| Number of alters who are exercise partners | 520* | 322 to 718 | 166 | −41 to 373 |
| Number of exercising alters | 241* | 63 to 419 | 71 | −136 to 279 |
Abbreviations: MASALA, Mediators of Atherosclerosis in South Asians Living in America; MET, metabolic equivalent. Note: Model controls for the following covariates: ego age, study site, education, marital status, income, cultural beliefs, self-rated health, and network size.
P < .01.
Additional analyses were completed to explore potential explanations for why having exercising alters or exercise partners in the social network led to a significant increase in MVPA for South Asian men but not for women. When examining alters’ characteristics, a notable finding was that 44% of exercise partners for South Asian men were their spouses, compared with 28% for South Asian women (Supplemental Table 1 [available online]). In regression models, where exercise partners were decomposed to spouse and nonspouse exercise partners (Table 3), we found additional gender differences in associations with MVPA. Among male egos, a significant increase in MVPA was observed if the exercise partner was not a spouse (596 MET min/wk; 95% CI, 374 to 818), whereas for female egos, a significant increase in MVPA was only found when a nonexercising alter in their network was replaced with an exercise partner who was a spouse (429 MET min/wk; 95% CI, 66 to 791). The association of a nonspouse exercise partners or exercising alters with MVPA was not significant for South Asian women (Table 3).
Table 3.
Association of Spouse/Nonspouse Exercise Partner With Egos’ Moderate to Vigorous Physical Activity (in MET Minutes per Week) in the MASALA Study
| Parameter | Male |
Female |
||
|---|---|---|---|---|
| Estimate | 95% confidence interval | Estimate | 95% confidence interval | |
| Intercept | 1311 | 650 to 1972 | 1120 | 406 to 1834 |
| Number of alters who are nonspouse exercise partners | 596** | 374 to 818 | 123 | −89 to 336 |
| Spouse exercise partner | 315 | −22 to 653 | 429* | 66 to 791 |
| Number of exercising alters | 256** | 78 to 435 | 71 | −135 to 277 |
Abbreviations: MASALA, Mediators of Atherosclerosis in South Asians Living in America; MET, metabolic equivalent. Note: Model controls for the following covariates: ego age, study site, education, marital status, income, cultural beliefs, self-rated health, and network size.
P < .05.
P < .01.
Discussion
This study yielded several important insights about social networks and physical activity among South Asian men and women. We found that having social network members who exercised was associated with large increases in MVPA among South Asian men; this effect was present when an alter exercised without the ego and was even larger if the alter was an exercise partner. In addition, there were key gender differences in the association between social networks and physical activity. For South Asian men, having an exercise partner who was not a spouse was associated with the greatest increases in MVPA. Notably, the opposite was true for South Asian women. A significant increase in South Asian women’s MVPA was only observed if the exercise partner was a spouse, suggesting that the type of relationship is an important consideration when trying to design interventions to increase physical activity. Our results provide empirical evidence of links between interpersonal social environment and physical activity among South Asians in the United States.
Although there is a large and growing literature about online social networks and physical activity, fewer studies exist on personal social networks and physical activity in adults. Others have found that selected social network characteristics, such as number of individuals in the network, frequency of contact, and network homogeneity, are positively associated with energy expenditure and exercise adherence.32,33 Our study extended beyond prior literature on network characteristics (eg, network size, density) to examine if the exercise behaviors of network members were associated with MVPA levels, as well as the importance of potential gender differences and spousal influences. Two recent studies have also found evidence of exercise contagion in social networks. Similar to our study’s findings, the Greenville Healthy Neighborhoods Project, which was predominantly African Americans, found that having a higher percentage of physically active network members was associated with higher odds of meeting physical activity guidelines.34 A second study using fitness tracker data from a million people in a global social network of runners found that exercise was socially contagious.35 Importantly, exercise contagiousness varied by the gender relationships between friends; both men and women influenced men, while only women influenced women. In our study, the type of relationship also mattered, but for South Asian women, the spouse was the most influential exercise partner, and gender did not seem to matter.
One potential mechanism that might explain our findings is that social networks can influence physical activity through the provision of social support. A recent study found that perceived social support from friends and family for physical activity was associated with MVPA in young women in Australia.5 Results from previous studies and the Australian study found that support from family or friends—such as encouragement or co-participation—was associated with an increase in physical activity partly because levels of self-efficacy also increase. In those studies, self-efficacy appeared to partly mediate the relationship between social support and physical activity. In our study, having an exercising alter in the network was associated with more MVPA in South Asian men, and this effect was much larger if the alter was an exercise partner. An exercise partner can provide instrumental and emotional support, which can help increase self-efficacy through the direct experience of exercising together, positive feedback, and role modeling. In addition, having an exercise partner can increase the enjoyment associated with exercise because of positive social interactions.36 Further research is needed to understand the mediators through which the social network exerts its influence on physical activity in South Asians.
The gender differences we found in the association between network characteristics and MVPA are intriguing and deserve further exploration. Among South Asian women, having a spouse as an exercise partner in the social network was positively associated with MVPA, and there was no significant association if the exercise partner was not a spouse. In a study of non-Hispanic black and white older adults in the United States, spousal physical activity levels were found to be important determinants for physical activity in older men and women.37 One possible explanation for why a spouse exercise partner was significant for South Asian women may be that spouses can provide more consistent, tangible support compared with an exercise partner who is not a spouse. In addition, prior studies have found significant cultural and social barriers to physical activity among South Asian women.38 South Asian women are typically less physically active than South Asian men or non-Hispanic white women due to “cultural norms, such as religious modesty or avoidance of mixed-sex activity, and fear of going out alone.”39 There is an expectation that South Asian women should prioritize domestic and family responsibilities over physical activity. If a spouse is an exercise partner, then he or she may be willing to share family responsibilities and can also help shift cultural or social norms that are barriers to exercise. For South Asian men, the effects of having an exercising alter and having a nonspouse exercise partner on MVPA were stronger than having a spouse exercise partner. It is possible that for men, social networks influenced physical activity through different mediators than for women. For example, South Asian men who observed their network members exercising may view MVPA as a social norm and adopt more positive attitudes or beliefs about physical activity. Other studies have also reported that gender modified the effects of social networks on physical activity,40 and additional research is needed to delineate the reasons underlying these gender differences.
Limitations
The results of this study should be examined in the context of a few limitations. First, this was a cross-sectional study that examines associations from one time point. The analysis does not provide information pertaining to the direction of association nor on changes in social networks and physical activity over time. Without longitudinal data, it is impossible to disentangle direct social influence by network members or participant self-selection into a network with people who have similar activity levels. The MASALA study is a prospective cohort study, and physical activity data collection at future study visits will allow for longitudinal analyses on social networks and physical activity. Second, all data were self-reported by respondents (typical of egocentric analysis) and, thus, are susceptible to projection bias.41 If study respondents accurately report on their perceptions of network members’ behavior, this could be even more important than the network members’ actual behavior; others have shown that perceptions are as important for influencing people’s health behaviors as the actual behaviors of the observed network members.42 To some extent, individuals justify their actions by believing that others support and encourage those actions.43
We adapted the self-reported social network measures from other national studies,27 but these measures have not been validated in multiethnic samples. Third, the MASALA study participants were largely middle-aged, first-generation immigrants from India, with high socioeconomic status from 2 US locations. These results may not be generalizable to all South Asians living in the United States. However, we have previously reported the similarity of the MASALA population to the US Census 2010 South Asian data.25 Additional work is needed to confirm if our results are similar in South Asians with lower socioeconomic status and among those born in the United States.
Conclusion
These results demonstrate that personal social networks are associated with physical activity in South Asians. The findings also highlight the need to understand which social network members are most influential for physical activity and how that may differ for men and women. For South Asian men, having exercise role models or exercise companions may be promising avenues for intervention. In South Asian women, having a spouse who is an exercise companion may be a more effective lever for physical activity behavior change. Our results support the idea that leveraging social networks and interpersonal processes may enhance the effectiveness of physical activity interventions in South Asians.
Supplementary Material
Acknowledgments
The authors would like to thank the MASALA study participants and study staff for their dedicated participation. The MASALA social networks study is registered as NCT02268513 at clinicaltrials.gov without an analysis plan. This study was funded by the National Heart, Lung, and Blood Institute: 1R01HL120725 (Principal Investigator [PI]: N.R.K.), R01-HL-093009 (PI: A.M.K.). Drs N.R.K., J.S., J.A.S., and A.M.K. were supported by 1R01HL120725. Drs N.R.K. and A.M.K. were supported by R01-HL-093009. The study sponsor had any role in study design; collection, analysis, and interpretation of data; writing the report; and the decision to submit the report for publication. The MASALA social networks data and surveys can be made available to other researchers at https://www.masalastudy.org/. N.R.K. conceived and designed the study, supervised data collection and analysis, and assisted with writing the manuscript; M.S.T. participated in data interpretation and drafted the manuscript; J.S. directed and supervised analyses; J.A.S. helped with study design and provided critical input on analyses and manuscript revisions; A.M.K. provided critical input and revisions on manuscript; A.J.C. and N.L. conducted analyses and provided input on the manuscript; S.S.D. assisted with data collection and assisted with drafting the manuscript. This paper was presented at the American Heart Association EPI/Lifestyle 2018 Scientific Sessions on March 22, 2018. At the start of the survey, participants provided written informed consent. There are no personally identifying details, images, or videos included in this manuscript. The study was approved by Institutional Review Board Office at Northwestern University and University of California, San Francisco. Participants all consented to participate in this study.
Footnotes
None of the authors have any competing interests to declare.
Contributor Information
Mitali S. Thanawala, School of Medicine, University of Missouri-Kansas City, Kansas City, MO, USA. Division of General Internal Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA.
Juned Siddique, Department of Preventive Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA..
John A. Schneider, Department of Medicine and Public Health Sciences and the Chicago Center for HIV Elimination, The University of Chicago, Chicago, IL, USA.
Alka M. Kanaya, Department of Medicine, University of California, San Francisco, USA.
Andrew J. Cooper, Division of General Internal Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA.
Swapna S. Dave, Division of General Internal Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA.
Nicola Lancki, Division of General Internal Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA..
Namratha R. Kandula, Division of General Internal Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA. Department of Preventive Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA.
References
- 1.US Department of Health and Human Services. Step it up! The surgeon general’s call to action to promote walking and walkable communities. 2015. https://www.surgeongeneral.gov/library/calls/walking-and-walkable-communities/call-to-action-walking-and-walkable-communites.pdf. Accessed October 1, 2019. [PubMed]
- 2.Hasson RE, Brown DR, Dorn J, et al. Achieving equity in physical activity participation: ACSM experience and next steps. Med Sci Sports Exerc 2017;49:848–858. PubMed ID: 27870795 doi: 10.1249/MSS.0000000000001161 [DOI] [PubMed] [Google Scholar]
- 3.Garcia LMT, Diez Roux AV, Martins ACR, Yang Y, Florindo AA. Development of a dynamic framework to explain population patterns of leisure-time physical activity through agent-based modeling. Int J Behav Nutr Phys Act 2017;14:111 PubMed ID: 28830527 doi: 10.1186/s12966-017-0553-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sawyer A, Ucci M, Jones R, Smith L, Fisher A. Simultaneous evaluation of physical and social environmental correlates of physical activity in adults: a systematic review. SSM Population Health. 2017;3:506–515. PubMed ID: 29349241 doi: 10.1016/j.ssmph.2017.05.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Darlow SD, Xu X. The influence of close others’ exercise habits and perceived social support on exercise. Psychol Sport Exerc 2011;12: 575–578. doi: 10.1016/j.psychsport.2011.04.004 [DOI] [Google Scholar]
- 6.Bureau USC. American Community Survey Demographic and Housing Estimates 2016 American Community Survey 1-Year Estimates. 2016.
- 7.Joshi P, Islam S, Pais P, et al. Risk factors for early myocardial infarction in South Asians compared with individuals in other countries. JAMA 2007;297:286–294. PubMed ID: 17227980 doi: 10.1001/jama.297.3.286 [DOI] [PubMed] [Google Scholar]
- 8.Kandula N, Ahmed M, Dodani S, et al. Cardiovascular disease & cancer risk among South Asians: impact of sociocultural influences on lifestyle and behavior. J Immigr Minor Health. 2019;21(suppl 1): 15–25. doi: 10.1007/s10903-017-0578-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jepson R, Harris FM, Bowes A, Robertson R, Avan G, Sheikh A. Physical activity in South Asians: an in-depth qualitative study to explore motivations and facilitators. PLoS One. 2012;7:e45333 PubMed ID: 23071511 doi: 10.1371/journal.pone.0045333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rackow P, Scholz U, Hornung R. Received social support and exercising: an intervention study to test the enabling hypothesis. Br J Health Psychol 2015;20:763–776. PubMed ID: 25854295 doi: 10.1111/bjhp.12139 [DOI] [PubMed] [Google Scholar]
- 11.South Asian Americans Leading Together. A demographic snapshot of South Asians in the United States. 2012. http://saalt.org/wp-content/uploads/2012/09/Demographic-Snapshot-Asian-American-Foundation-2012.pdf. Accessed September 18, 2018.
- 12.Daniel M, Wilbur J, Fogg LF, Miller AM. Correlates of lifestyle: physical activity among South Asian Indian immigrants. J Community Health Nurs. 2013;30:185–200. PubMed ID: 24219639 doi: 10.1080/07370016.2013.838482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bhatnagar P, Shaw A, Foster C. Generational differences in the physical activity of UK South Asians: a systematic review. Int J Behav Nutr Phys Act 2015;12:96 PubMed ID: 26187626 doi: 10.1186/s12966-015-0255-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jayaprakash M, Puri-Taneja A, Kandula NR, Bharucha H, Kumar S, Dave SS. Qualitative process evaluation of a community-based culturally tailored lifestyle intervention for underserved South Asians. Health Promot Pract 2016;17(6):802–813. PubMed ID: 27225217 doi: 10.1177/1524839916650165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Morrison Z, Douglas A, Bhopal R, Sheikh A, Trial I. Understanding experiences of participating in a weight loss lifestyle intervention trial: a qualitative evaluation of South Asians at high risk of diabetes. BMJ Open 2014;4:e004736 PubMed ID: 24951108 doi: 10.1136/bmjopen-2013-004736 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bandura A Social Learning Theory Englewood Cliffs, NJ: Prentice Hall; 1977. [Google Scholar]
- 17.Dave SS, Craft LL, Mehta P, Naval S, Kumar S, Kandula NR. Life stage influences on U.S. South Asian women’s physical activity. Am J Health Promot. 2015;29:e100–e108. PubMed ID: 24717067 doi: 10.4278/ajhp.130415-QUAL-175 [DOI] [PubMed] [Google Scholar]
- 18.Sani F, Madhok V, Norbury M, Dugard P, Wakefield JRH. Greater number of group identifications is associated with healthier behaviour: evidence from a Scottish community sample. Br J Health Psychol 2015;20:466–481. PubMed ID: 25270579 doi: 10.1111/bjhp.12119 [DOI] [PubMed] [Google Scholar]
- 19.Wilson PM, Rodgers WM. The relationship between perceived autonomy support, exercise regulations and behavioral intentions in women. Psychol Sport Exerc 2004;5:229–242. doi: 10.1016/S1469-0292(03)00003-7 [DOI] [Google Scholar]
- 20.Vissenberg C, Nierkens V, van Valkengoed I, et al. The impact of a social network based intervention on self-management behaviours among patients with type 2 diabetes living in socioeconomically deprived neighbourhoods: a mixed methods approach. Scand J Public Health. 2017;45:569–583. PubMed ID: 28707567 doi: 10.1177/1403494817701565 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Li K, Iannotti RJ, Haynie DL, Perlus JG, Simons-Morton BG. Motivation and planning as mediators of the relation between social support and physical activity among U.S. adolescents: a nationally representative study. Int J Behav Nutr Phys Act. 2014;11:42 PubMed ID: 24656181 doi: 10.1186/1479-5868-11-42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pollard TM, Carlin LE, Bhopal R, Unwin N, White M, Fischbacher C. Social networks and coronary heart disease risk factors in South Asians and Europeans in the UK. Ethn Health. 2003;8:263–275. PubMed ID: 14577999 doi: 10.1080/1355785032000136452 [DOI] [PubMed] [Google Scholar]
- 23.Bhattacharya G The Indian Diaspora in transnational context: social relations and cultural identities of immigrants to New York City. J Intercult Stud 2008;29:65–80. doi: 10.1080/07256860701759949 [DOI] [Google Scholar]
- 24.Pilisuk M Kinship, social networks, social support and health. Soc Sci Med 1978;12:273–280. [DOI] [PubMed] [Google Scholar]
- 25.Kanaya AM, Kandula N, Herrington D, et al. Mediators of Atherosclerosis in South Asians Living in America (MASALA) study: objectives, methods, and cohort description. Clin Cardiol 2013;36: 713–720. PubMed ID: 24194499 doi: 10.1002/clc.22219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kandula NR, Cooper AJ, Schneider JA, et al. Personal social networks and organizational affiliation of South Asians in the United States. BMC Public Health. 2018;18:218 PubMed ID: 29402246 doi: 10.1186/s12889-018-5128-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cornwell B, Schumm LP, Laumann EO, Graber J. Social networks in the NSHAP study: rationale, measurement, and preliminary findings. J Gerontol B Psychol 2009;64:I47–I55. doi: 10.1093/geronb/gbp042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Marsden PV. Network data and measurement. Annu Rev Sociol 1990;16:435–463. doi: 10.1146/annurev.so.16.080190.002251 [DOI] [Google Scholar]
- 29.WHO. What is Moderate-intensity and Vigorous-intensity Physical Activity? Global Strategy on Diet, Physical Activity and Health. 2018. https://www.who.int/dietphysicalactivity/physical_activity_intensity/en/. Accessed October 1, 2019. [Google Scholar]
- 30.Ainsworth BE, Irwin ML, Addy CL, Whitt MC, Stolarczyk LM. Moderate physical activity patterns of minority women: the cross-cultural activity participation study. J Womens Health Gend Based Med 1999;8:805–813. PubMed ID: 10495261 doi: 10.1089/152460999319129 [DOI] [PubMed] [Google Scholar]
- 31.Cornwell B Network bridging potential in later life: life-course experiences and social network position. J Aging Health. 2009;21:129–154. PubMed ID: 19144972 doi: 10.1177/0898264308328649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kim BH, Wallington SF, Makambi KH, Adams-Campbell LL. Social networks and physical activity behaviors among cancer survivors: data from the 2005 Health Information National Trends Survey. J Health Commun 2015;20:656–662. PubMed ID: 25978562 doi: 10.1080/10810730.2015.1018576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mötteli S, Dohle S. Egocentric social network correlates of physical activity [published online ahead of print January 6, 2017]. J Sport Health Sci 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Child S, Kaczynski AT, Moore S. Meeting physical activity guidelines: the role of personal networks among residents of low-income communities. Am J Prev Med 2017;53:385–391. PubMed ID: 28601404 doi: 10.1016/j.amepre.2017.04.007 [DOI] [PubMed] [Google Scholar]
- 35.Aral S, Nicolaides C. Exercise contagion in a global social network. Nat Commun 2017;8:14753 PubMed ID: 28418379 doi: 10.1038/ncomms14753 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Middelweerd A, Te Velde SJ, Abbott G, Timperio A, Brug J, Ball K. Do intrapersonal factors mediate the association of social support with physical activity in young women living in socioeconomically disadvantaged neighbourhoods? A longitudinal mediation analysis. PLoS One. 2017;12:e0173231 PubMed ID: 28301538 doi: 10.1371/journal.pone.0173231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Pettee KK, Brach JS, Kriska AM, et al. Influence of marital status on physical activity levels among older adults. Med Sci Sports Exerc 2006;38:541–546. PubMed ID: 16540843 doi: 10.1249/01.mss.0000191346.95244.f7 [DOI] [PubMed] [Google Scholar]
- 38.Babakus WS, Thompson JL. Physical activity among South Asian women: a systematic, mixed-methods review. Int J Behav Nutr Phys Act. 2012;9:150 PubMed ID: 23256686 doi: 10.1186/1479-5868-9-150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sriskantharajah J, Kai J. Promoting physical activity among South Asian women with coronary heart disease and diabetes: what might help? Fam Pract 2007;24:71–76. PubMed ID: 17179137 doi: 10.1093/fampra/cml066 [DOI] [PubMed] [Google Scholar]
- 40.Bot SD, Mackenbach JD, Nijpels G, Lakerveld J. Association between social network characteristics and lifestyle behaviours in adults at risk of diabetes and cardiovascular disease. PLoS One. 2016; 11:e0165041 PubMed ID: 27798709 doi: 10.1371/journal.pone.0165041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Henry DB, Kobus K, Schoeny ME. Accuracy and bias in adolescents’ perceptions of friends’ substance use. Psychol Addict Behav 2011; 25:80–89. PubMed ID: 21244119 doi: 10.1037/a0021874 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Valente TW, Watkins SC, Jato MN, van der Straten A, Tsitsol LP. Social network associations with contraceptive use among Cameroonian women in voluntary associations. Soc Sci Med 1997;45:677–687. PubMed ID: 9226791 doi: 10.1016/S0277-9536(96)00385-1 [DOI] [PubMed] [Google Scholar]
- 43.Valente TW. Social Networks and Health: Models, Methods, and Applications. New York, NY: Oxford University Press; 2010. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.