

Abstract
Objectives
This study aimed to investigate associations between occupational physical activity patterns (physical work demands linked to job title) and leisure time physical activity (assessed by questionnaire) with cardiorespiratory fitness (assessed by exercise test) among men and women in the German working population.
Design
Population-based cross-sectional study.
Setting
Two-stage cluster-randomised general population sample selected from population registries of 180 nationally distributed sample points. Information was collected from 2008 to 2011.
Participants
1296 women and 1199 men aged 18–64 from the resident working population.
Outcome measure
Estimated low maximal oxygen consumption (), defined as first and second sex-specific quintile, assessed by a standardised, submaximal cycle ergometer test.
Results
Low estimated was strongly linked to low leisure time physical activity, but not occupational physical activity. The association of domain-specific physical activity patterns with low varied by sex: women doing no leisure time physical activity with high occupational physical activity levels were more likely to have low (OR 6.54; 95% CI 2.98 to 14.3) compared with women with ≥2 hours of leisure time physical activity and high occupational physical activity. Men with no leisure time physical activity and low occupational physical activity had the highest odds of low (OR 4.37; 95% CI 2.02 to 9.47).
Conclusion
There was a strong association between patterns of leisure time and occupational physical activity and cardiorespiratory fitness within the adult working population in Germany. Women doing no leisure time physical activity were likely to have poor cardiorespiratory fitness, especially if they worked in physically demanding jobs. However, further investigation is needed to understand the relationships between activity and fitness in different domains. Current guidelines do not distinguish between activity during work and leisure time, so specifying leisure time recommendations by occupational physical activity level should be considered.
Keywords: cardiorespiratory fitness, adults, physical activity, physical fitness, occupational physical activity
Strengths and limitations of this study.
This is among the first studies to examine the association between leisure time and occupational physical activity patterns and cardiorespiratory fitness in Germany.
We used a large nationally representative population-based sample of the resident adult working population, to allow our findings to be generalised.
Leisure time physical activity was assessed by self-reports, which may be prone to recall and social desirability bias.
Background
Physical activity is crucial for health and the unfavourable effects of an increasingly sedentary lifestyle are acknowledged as a major public health challenge.1 2 Physical activity is defined as all bodily movement produced by skeletal muscles that require energy expenditure.3 It has a positive influence on physical and mental health and contributes to the prevention of non-communicable diseases and premature mortality.1 It can also take different forms and happen in different domains of individual daily routines and life courses. For example, people may participate in sports during their leisure time (leisure time physical activity) or be active at work (occupational physical activity). To date, physical activity in any form and setting has been considered beneficial and recent recommendations do not distinguish between domains. The current WHO guideline recommends at least 150 min of moderate intensity aerobic physical activity per week, stating that “[…] Physical activity includes leisure time physical activity, transportation (eg, walking or cycling), occupational (ie, work), household chores, play, games, sports or planned exercise, in the context of daily, family, and community activities”.(3, p8)
Manual and physically demanding occupations have been declining for decades, but occupational physical activity still accounts for a large part of many people’s daily activity.4 The beneficial effects of leisure time physical activity are well established, but the effect of occupational physical activity is inconclusive. Studies in the past often argued that occupational physical activity should also be considered to improve health,5 but recent studies suggest that it is not health enhancing and may even have the opposite effect.6 7 As a possible explanation for this ‘health paradox’, the domain-specific effects of physical activity on cardiorespiratory fitness have come to attention.8 9 Defined as the ability of circulatory, respiratory and muscular systems to supply oxygen during prolonged physical exercise,3 cardiorespiratory fitness can be enhanced by regular endurance exercise10 and is a strong predictor of adverse health outcomes.11 It has been argued that occupational physical activity rarely has the adequate intensity, duration and volume to increase cardiorespiratory fitness.8 9 12 13
However, research on the association between different activity domains and cardiorespiratory fitness in Germany is limited. In particular, the interplay between different domains has not yet been analysed for cardiorespiratory fitness. This study therefore aimed to investigate the associations between leisure time and occupational physical activity with cardiorespiratory fitness among the German working population. Furthermore, in addition to the direct effects of the domain-specific physical activity, their interactional effects on cardiorespiratory fitness are investigated. The analyses were stratified by sex because men and women may vary in their exposure to physical demands at work,14 type of occupations15 and response to physical activity.16
Methods
Study design
We used data from the nationwide cross-sectional German Health Interview and Examination Survey for Adults (Studie zur Gesundheit Erwachsener in Deutschland; DEGS1). DEGS1 is part of the Federal Health Monitoring System administered by the Robert Koch Institute.17 In detail, the study design is described elsewhere.18 Briefly, the study is based on a two-stage cluster randomised sampling procedure. First, 180 sample points were sampled from a list of German communities stratified to represent the regional distribution. Second, within these units, adult individuals were randomly drawn from local population registries stratified by 10-year age groups. The response rate was 42%. A total of 5262 participants aged 18–64 years took part in the physical measurements component from November 2008 to December 2011. Of these, 3110 individuals were test qualified for the exercise test (figure 1).
Figure 1.
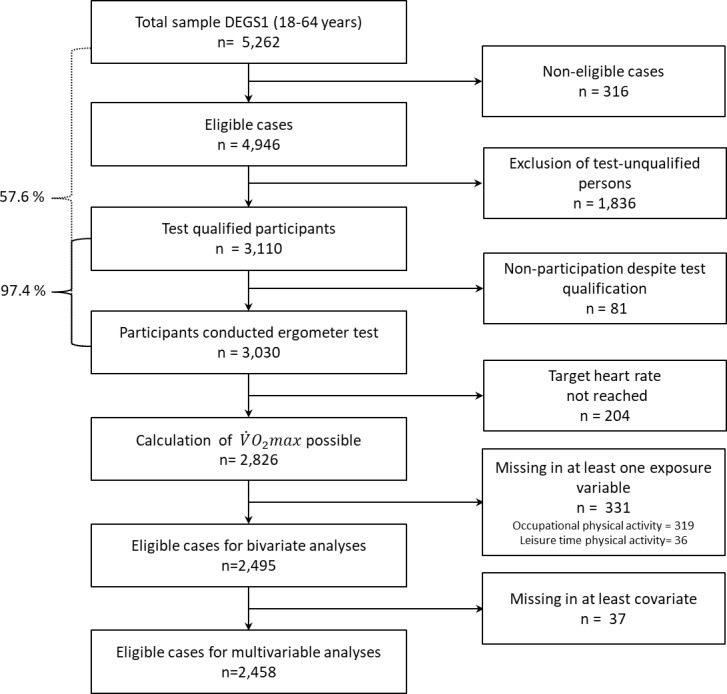
Flow diagram of participants. DEGS1, German National Health Interview and Examination Survey for Adults; , maximal oxygen consumption
Overall, 3030 participants completed the exercise test (participation rate 97.4%). was estimated for all participants reaching at least 75% of the age-predicted maximum heart rate (HRmax). In total, 204 participants terminated the test before reaching this heart rate, so could be calculated for 2826 participants. Further cases were excluded from this analysis because of missing physical activity data. Overall, valid information on and occupational and leisure time physical activity was available for 1296 women and 1199 men. Table 1 shows demographic, anthropometric and health behaviour variables from this representative sample of the adult working population of Germany. Women made up 48.0% of the sample, and the mean age of the participants was 39.6 years (range 18–64 years). The unweighted and weighted percentages did not differ substantially, although weighting led to a slightly smaller proportion of participants in the older age groups and a smaller proportion in the high socioeconomic status group.
Table 1.
Characteristics of study participants in German Health Interview and Examination Survey for Adults
| Men | Women | Total | |||||||
| n | %* | %† | n | %* | %† | n | %* | %† | |
| Low | 494 | 41.2 | 41.2 | 546 | 42.1 | 40.5 | 1040 | 41.7 | 40.9 |
| Intermediate/high | 705 | 58.8 | 58.8 | 750 | 57.9 | 59.5 | 1455 | 58.3 | 59.1 |
| Missing | 0 | 0.0 | – | 0 | 0.0 | – | 0 | 0.0 | – |
| LTPA | |||||||||
| No | 297 | 24.8 | 24.9 | 309 | 23.8 | 24.7 | 606 | 24.3 | 24.8 |
| <2 hours | 492 | 41.0 | 39.8 | 647 | 49.9 | 49.9 | 1139 | 45.7 | 44.7 |
| ≥2 hours | 410 | 34.2 | 35.3 | 340 | 26.2 | 25.3 | 750 | 30.1 | 30.5 |
| Missing | 0 | 0.0 | – | 0 | 0.0 | – | 0 | 0.0 | – |
| OPA | |||||||||
| Low | 750 | 62.6 | 59.7 | 895 | 69.1 | 67.0 | 1645 | 65.9 | 63.2 |
| High | 449 | 37.4 | 40.3 | 401 | 30.9 | 33.0 | 850 | 34.1 | 36.8 |
| Missing | 0 | 0.0 | – | 0 | 0.0 | – | 0 | 0.0 | – |
| Age | |||||||||
| 18–24 Years | 137 | 11.4 | 11.3 | 138 | 10.6 | 11.8 | 275 | 11.0 | 11.5 |
| 25–34 Years | 277 | 23.1 | 26.4 | 250 | 19.3 | 22.5 | 527 | 21.1 | 24.5 |
| 35–44 Years | 287 | 23.9 | 26.8 | 338 | 26.1 | 27.7 | 625 | 25.1 | 27.2 |
| 45–54 Years | 308 | 25.7 | 23.2 | 369 | 28.5 | 25.8 | 677 | 27.1 | 24.5 |
| 55–64 Years | 190 | 15.8 | 12.3 | 201 | 15.5 | 12.3 | 391 | 15.7 | 12.3 |
| Missing | 0 | 0.0 | – | 0 | 0.0 | – | 0 | 0.0 | – |
| Waist circumference | |||||||||
| Normal | 719 | 60.0 | 61.7 | 702 | 54.2 | 57.0 | 1421 | 57.0 | 59.4 |
| Increased | 256 | 21.4 | 20.1 | 289 | 22.3 | 22.5 | 545 | 21.8 | 21.3 |
| Strongly increased | 224 | 18.7 | 18.2 | 303 | 23.4 | 20.5 | 527 | 21.1 | 19.3 |
| Missing | 0 | 0.0 | – | 2 | 0.2 | – | 2 | 0.1 | – |
| Body mass index | |||||||||
| Underweight | 9 | 0.8 | 0.8 | 32 | 2.5 | 2.8 | 41 | 1.6 | 1.8 |
| Normal weight | 467 | 38.9 | 37.7 | 748 | 57.7 | 58.1 | 1215 | 48.7 | 47.5 |
| Overweight | 548 | 45.7 | 46.1 | 348 | 26.9 | 27.1 | 896 | 35.9 | 37.0 |
| Obese | 171 | 14.3 | 15.4 | 164 | 12.7 | 11.9 | 335 | 13.4 | 13.7 |
| Missing | 4 | 0.3 | – | 4 | 0.3 | – | 8 | 0.3 | – |
| Smoking status | |||||||||
| Daily | 349 | 29.1 | 31.3 | 268 | 20.7 | 23.2 | 617 | 24.7 | 27.4 |
| Occasionally | 106 | 8.8 | 8.2 | 96 | 7.4 | 7.6 | 202 | 8.1 | 7.9 |
| Former | 323 | 26.9 | 26.9 | 354 | 27.3 | 25.8 | 677 | 27.1 | 26.3 |
| Never | 420 | 35.0 | 33.7 | 576 | 44.4 | 43.4 | 996 | 39.9 | 38.3 |
| Missing | 1 | 0.1 | – | 2 | 0.2 | – | 3 | 0.1 | – |
| Alcohol consumption | |||||||||
| Low | 180 | 15.0 | 16.7 | 151 | 11.7 | 12.3 | 331 | 13.3 | 14.6 |
| Moderate | 760 | 63.4 | 64.3 | 821 | 63.3 | 64.8 | 1581 | 63.4 | 64.6 |
| High | 245 | 20.4 | 19.0 | 314 | 24.2 | 22.9 | 559 | 22.4 | 20.9 |
| Missing | 14 | 1.2 | – | 10 | 0.8 | – | 24 | 1.0 | – |
| Socioeconomic status | |||||||||
| Low | 151 | 12.6 | 14.7 | 113 | 8.7 | 9.6 | 264 | 10.6 | 12.3 |
| Medium | 702 | 58.5 | 61.4 | 800 | 61.7 | 63.5 | 1502 | 60.2 | 62.4 |
| High | 346 | 28.9 | 23.9 | 382 | 29.5 | 26.8 | 728 | 29.2 | 25.3 |
| Missing | 0 | 0 | – | 1 | 0.1 | – | 1 | 0.0 | – |
Values shown are frequencies in percentages.
*Percentage of the sample (unweighted).
†Weighted percentage (weighting factors were used to adjust the distribution of the sample to match the German population for sex, age, education and region).
LTPA, leisure time physical activity; OPA, occupational physical activity; , maximal oxygen consumption.
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient-relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Outcome variable
Cardiorespiratory fitness was measured using a standardised, submaximal cycle ergometer test (Ergosana Sana Bike 350/450 (Ergosana, Germany), heart rate monitor (Polar, Finland), blood pressure cuffs (Ergosana, Germany), a heart rate transmitter (Oregon Scientific, USA) and a notebook with ergometer software (Dr Schmidt GmbH, Germany)). Test methodology, protocol and exclusion criteria have been described elsewhere.19 20 DEGS1 participants were included in the ergometer test if they were aged 18–64 years, gave informed consent and were test qualified based on a modified German version of the Physical Activity Readiness Questionnaire (PAR-Q).21 22 If any PAR-Q contraindications were reported, the participant was seen by a physician, who decided whether they should be enrolled into the exercise test. Cardiorespiratory fitness was assessed using the test protocol recommended by WHO.23 Beginning at 25 W, the workload was increased by 25 W every 2 min until 85% of the estimated age-specific maximal heart rate was exceeded, a maximum level of 350 W was achieved or the study staff terminated the test. Heart rate was monitored continuously throughout the test. The formula 208–0.7×Age was used to calculate the age-predicted maximum heart rate.24 To derive physical work capacity at HRmax (PWC100%), the measured heart rate (beats/min) during the incremental phase was regressed against corresponding workload in watts for each participant. Assuming a linear relationship between heart rate and workload, PWC100% was obtained by extrapolation using the individual regression equation PWC100%=intercept + HRmax ×slope.25 PWC100% was converted to using a metabolic equation provided by the American College of Sports Medicine: 3.5 mL/min/kg+12.24 × (PWC100%) / (body weight).26 Estimated was categorised into low (sex-specific quintiles 1–2) and intermediate to high (quintiles 3–5).
Exposure variable
Occupational physical activity: a physical work demands index
To assess occupational physical activity, we used an indirect method and computed specific job exposure matrices to distinguish participants’ occupation by level of physical demand. These matrices are an established methodological tool to allow inclusion of specific occupational exposure in analyses, drawing on studies that assess information about job titles. They are constructed using available secondary data to determine exposure profiles for each occupation. These profiles are matched to primary data using standardised job classifications. In our case, such matrices were constructed using data from a large-scale representative study on working conditions of 20 000 employees in Germany,27 28 which was part of the European Working Conditions Survey regularly conducted in member states of the European Union. The overall job index and specific indexes have been described and applied elsewhere.29–31 In this study, we used a specific subindex of perceived physical work demands. To construct the index, we used data on the frequency of lifting and carrying heavy loads (men≥20 kg, women≥10 kg). The item was assessed with a frequency scale with four answer categories: ‘often’, ‘sometimes’, ‘rarely’ and ‘never’.27 28 The physical demand index was assigned to the occupations based on hierarchic multilevel analyses adjusted for sex, age, job experience and part time employment. In contrast to the use of occupation-specific means, this procedure allows adjustment for other variables besides the specific occupation that could also influence the level of demand (eg, the sex ratio or the level of part-time employment). The levels for the multilevel estimation were defined by the 2-digit, 3-digit and 4-digit codes of the International Classification of Occupations of 1988 (ISCO-88) classification. These matrices were then classified into deciles. Occupations with the lowest level of physical work demands had a value of 1 (first decile), and those with the highest level had a value of 10 (tenth decile). Using the ISCO-88, the matrices were matched to DEGS1. To create a combined physical activity variable, this index was then dichotomised into low (index values 1–6) and high occupational physical activity (index values 7–10). A list of the most frequent occupations in DEGS1 by occupational physical activity level for men and women is shown in online supplementary table S1.
bmjopen-2019-034610supp001.pdf (173.4KB, pdf)
Leisure time physical activity: physical exercise
Leisure time physical activity was assessed by asking participants ‘How often do you engage in physical exercise?’32 Leisure time physical activity usually refers to all physical activity in freely disposable time, but sport and exercise are the main elements33 so were used in this study. Responses were on a five-point scale of ‘no physical exercise’, ‘less than 1 hour a week’ and ‘regularly 1–2 hours a week’, ‘regularly up to 4 hours’ and ‘regularly more than 4 hours’, and were categorised into three groups: no physical exercise, <2 hours/week and ≥2 hours/week.
Combined occupational and leisure time physical activity
To analyse the combined relationship of occupational and leisure time physical activity on cardiorespiratory fitness, we generated a combined variable by grouping no, <2 hours, and ≥2 hours leisure time physical activity with each of low and high occupational physical activity, giving six possible categories.
Covariates
Relevant covariates were selected from the literature.34 35 Age was categorised into five groups: 18–24 years, 25–34 years, 35–44 years, 45–54 years and 55–64 years. Smoking was grouped into daily, occasionally, former and never. Alcohol intake was estimated by multiplying the calculated quantity of each alcoholic beverage, assessed by a food frequency questionnaire, with standard ethanol content (beer: 4.8%; wine: 11%, spirits: 33%) and classified into low (quintile 1), medium (quintile 2–4) and high (quintile 5) alcohol consumption using sex-specific quintiles. Body mass index and waist circumference have been shown to be independently related to cardiorespiratory fitness,34 35 so we included both parameters as covariates. Body height and weight were measured by standardised procedures using portable electronic scales (SECA, Germany) and stadiometer (Holtain, UK). Body mass index (kg/m2) was categorised using WHO guidelines.36 Waist circumference was measured at the smallest site between the lowest rib and the superior border of the iliac crest with flexible, non-stretchable measurement tape (Sibner Hegner, Switzerland) and categorised as ‘normal’, ‘increased’ and ‘strongly increased’ using international guidelines.37 Socioeconomic status was determined using a composite additive index, based on information about participants’ education, occupational position and net equivalent income.38
Statistical analyses
Leisure time and occupational physical activity were cross tabulated to show the association of the domain-specific activity levels. Prevalence and 95% CIs of low were calculated by occupational and leisure time physical activity and covariates. Multivariable logistic regression models were computed to estimate the associations between domain-specific physical activity (exposure) and low (outcome). In a first step, the main effects of occupational and leisure time physical activity were investigated; in a second step, the combined activity variable was used. In both steps, we fitted an age-adjusted model and one adjusting for age, body mass index, waist circumference, smoking, alcohol intake and socioeconomic status. Finally, we computed predicted margins39 from the fully adjusted logistic regression model investigating the combined physical activity variable to plot adjusted prevalence of low by domain-specific physical activity. All analyses were performed separately for men and women to identify sex-specific physical activity patterns associated with cardiorespiratory fitness and to detect potential effect modification by sex. Analyses were performed with Stata V.15.1 (Stata Corp.). To enhance the external validity of the results, weighting factors were used to adjust for distribution of the sample by sex, age, education and region, to match the German population. Stata’s survey procedures were applied to account for the clustered sampling design.
Results
Occupational and leisure time physical activity levels
Prevalence of high occupational physical activity was 40.3% among men and 33.0% among women (table 1). In total, 24.9% of men and 24.7% of women engaged in no leisure time physical activity, 39.8% and 49.9% in less than 2 hours per week, and 35.3% and 25.3% in 2 hours or more per week. Leisure time physical activity did not vary with occupational physical activity level among men, but women with high occupational physical activity were less likely to engage in 2 hours or more leisure time physical activity per week than women with low occupational physical activity (table 2).
Table 2.
Association of leisure time and occupational physical activity among male and female German Health Interview and Examination Survey for Adults participants
| Low OPA | High OPA | |||
| % | (95% CI) | % | (95% CI) | |
| Men | ||||
| No LTPA | 24.0 | (20.1 to 28.3) | 26.2 | (21.4 to 31.5) |
| <2 hours LTPA | 39.4 | (35.2 to 43.7) | 40.4 | (34.9 to 46.2) |
| ≥2 hours LTPA | 36.6 | (32.7 to 40.7) | 33.4 | (27.7 to 39.7) |
| Women | ||||
| No LTPA | 21.6 | (17.9 to 25.9) | 31.1 | (25.6 to 37.3) |
| <2 hours LTPA | 49.6 | (44.8 to 54.3) | 50.6 | (44.9 to 56.4) |
| ≥2 hours LTPA | 28.8 | (25.1 to 32.8) | 18.2 | (14.4 to 22.9) |
Values shown are frequencies in percentages with 95% CIs.
LTPA, leisure time physical activity; OPA, occupational physical activity.
Low
Overall, the prevalence of estimated low was 41.2% (95% CI 37.6 to 44.8) for men and 40.5% for women (95% CI 37.1 to 44.0). Table 3 shows the prevalence of low by domain-specific physical activity and sociodemographic, health behaviour and anthropometric variables. Binary analyses showed that men and women with higher leisure time activity levels had substantially lower prevalence of low . There were no relevant differences in low by occupational physical activity among men, but women with high occupational physical activity had a higher prevalence of low than women with low occupational physical activity.
Table 3.
Prevalence and 95% CIs of low estimated by domain-specific physical activity, health behavioural, anthropometric and sociodemographic characteristics among male and female German Health Interview and Examination Survey for Adults participants
| Men | Women | |||
| % | (95% CI) | % | (95% CI) | |
| Total | 41.2 | (37.6 to 44.8) | 40.5 | (37.1 to 44.0) |
| LTPA | ||||
| No | 63.2 | (56.4 to 69.4) | 56.1 | (49.1 to 62.9) |
| <2 hours | 42.2 | (36.5 to 48.0) | 41.2 | (36.6 to 45.9) |
| ≥2 hours | 24.7 | (19.8 to 30.5) | 24.1 | (19.0 to 30.1) |
| OPA | ||||
| Low | 41.5 | (36.8 to 46.4) | 37.2 | (33.0 to 41.6) |
| High | 40.8 | (35.0 to 46.8) | 47.4 | (41.5 to 53.4) |
| OPA/LTPA | ||||
| No LTPA, low OPA | 68.5 | (59.2 to 76.4) | 48.0 | (39.7 to 56.3) |
| No LTPA, high OPA | 56.0 | (44.9 to 66.5) | 67.7 | (56.7 to 77.0) |
| <2 hours LTPA, low OPA | 42.6 | (35.8 to 49.7) | 39.3 | (33.5 to 45.5) |
| <2 hours LTPA, high OPA | 41.6 | (32.3 to 51.5) | 44.9 | (37.5 to 52.5) |
| ≥2 hours LTPA, low OPA | 22.8 | (17.1 to 29.6) | 25.4 | (19.0 to 33.0) |
| ≥2 hours LTPA, high OPA | 28.0 | (19.1 to 39.0) | 19.9 | (11.6 to 32.1) |
| Age | ||||
| 18–24 Years | 28.0 | (19.9 to 37.7) | 25.8 | (17.9 to 35.7) |
| 25–34 Years | 36.0 | (28.9 to 43.8) | 29.2 | (23.3 to 35.9) |
| 35–44 Years | 41.9 | (34.9 to 49.2) | 36.1 | (30.3 to 42.3) |
| 45–54 Years | 47.2 | (40.9 to 53.7) | 48.5 | (42.1 to 55.1) |
| 55–64 Years | 51.9 | (42.3 to 61.4) | 68.7 | (60.2 to 76.1) |
| Waist circumference | ||||
| Normal | 27.1 | (23.2 to 31.4) | 26.9 | (23.0 to 31.1) |
| Increased | 54.6 | (46.2 to 62.8) | 46.4 | (38.5 to 54.6) |
| Strongly increased | 74.2 | (66.7 to 80.4) | 72.5 | (66.3 to 77.9) |
| Body mass index | ||||
| Underweight | 19.8 | (3.3 to 64.1) | 18.9 | (7.7 to 39.4) |
| Normal weight | 21.7 | (16.9 to 27.4) | 27.1 | (23.4 to 31.2) |
| Overweight | 47.5 | (42.3 to 52.8) | 53.7 | (46.4 to 60.8) |
| Obese | 71.1 | (62.4 to 78.4) | 83.1 | (75.3 to 88.8) |
| Smoking status | ||||
| Daily | 40.7 | (34.9 to 46.8) | 38.8 | (31.6 to 46.7) |
| Occasionally | 31.7 | (22.3 to 42.9) | 33.5 | (22.9 to 46.0) |
| Former | 49.6 | (42.3 to 56.9) | 46.7 | (40.0 to 53.6) |
| Never | 37.5 | (31.4 to 44.0) | 39.0 | (34.0 to 44.3) |
| Alcohol consumption | ||||
| Low | 45.7 | (38.0 to 53.7) | 50.2 | (40.8 to 59.5) |
| Moderate | 39.1 | (34.9 to 43.6) | 41.1 | (36.6 to 45.8) |
| High | 43.4 | (35.1 to 52.2) | 33.2 | (26.7 to 40.5) |
| Socioeconomic status | ||||
| Low | 39.9 | (30.7 to 49.8) | 56.3 | (45.8 to 66.3) |
| Medium | 43.3 | (38.7 to 48.1) | 43.4 | (39.3 to 47.5) |
| High | 36.8 | (30.8 to 43.2) | 28.2 | (22.4 to 34.9) |
LTPA, leisure time physical activity; OPA, occupational physical activity; , maximal oxygen consumption.
Multivariable analyses (table 4) showed that women in jobs with high levels of occupational physical activity were more likely to have a low estimated when adjusting only for age (OR 1.71; 95% CI 1.23 to 2.36). This association disappeared when controlling for leisure time physical activity and other covariates (OR 1.06; 95% CI 0.75 to 1.49). Neither model showed any association between low and occupational physical activity for men (OR 1.05; 95% CI 0.75 to 1.46 and OR 0.95; 95% CI 0.64 to 1.42).
Table 4.
Domain-specific physical activity and low estimated among male and female German Health Interview and Examination Survey for Adults participants
| Men | Women | |||||||
| OR* | (95 % CI) | OR† | (95 % CI) | OR* | (95 % CI) | OR† | (95 % CI) | |
| Main effects model | ||||||||
| OPA | ||||||||
| Low OPA | (Ref.) | (Ref.) | (Ref.) | (Ref.) | ||||
| High OPA | 1.05 | (0.75 to 1.46) | 0.95 | (0.64 to 1.42) | 1.71 | (1.23 to 2.36) | 1.06 | (0.75 to 1.49) |
| LTPA | ||||||||
| No LTPA | 4.97 | (3.47 to 7.13) | 4.46 | (2.89 to 6.89) | 4.96 | (3.26 to 7.54) | 4.65 | (2.90 to 7.45) |
| <2 hours LTPA | 2.17 | (1.48 to 3.19) | 2.04 | (1.32 to 3.15) | 2.49 | (1.72 to 3.62) | 2.13 | (1.44 to 3.14) |
| ≥2 hours LTPA | (Ref.) | (Ref.) | (Ref.) | (Ref.) | ||||
| OPA/LTPA model | ||||||||
| No LTPA, low OPA | 4.92 | (2.56 to 9.46) | 4.45 | (2.14 to 9.23) | 4.37 | (2.02 to 9.47) | 6.54 | (2.98 to 14.3) |
| No LTPA, high OPA | 2.86 | (1.47 to 5.58) | 2.34 | (1.08 to 5.07) | 11.1 | (5.15 to 24.1) | 10.5 | (4.39 to 24.9) |
| <2 hours LTPA, low OPA | 1.69 | (0.94 to 3.06) | 1.54 | (0.77 to 3.06) | 2.84 | (1.39 to 5.78) | 3.52 | (1.75 to 7.09) |
| <2 hours LTPA, high OPA | 1.70 | (0.91 to 3.17) | 1.54 | (0.75 to 3.16) | 4.01 | (1.90 to 8.49) | 3.69 | (1.80 to 7.60) |
| ≥2 hours LTPA, low OPA | 0.67 | (0.35 to 1.27) | 0.64 | (0.32 to 1.27) | 1.37 | (0.64 to 2.92) | 1.93 | (0.90 to 4.13) |
| ≥2 hours LTPA, high OPA | (Ref.) | (Ref.) | (Ref.) | (Ref.) | ||||
| n | 1199 | 1181 | 1296 | 1277 | ||||
Different adjustment criteria were used in multivariable logistic regression analyses.
*Adjusted for age.
†Adjusted for age, waist circumference, body mass index, smoking status, alcohol consumption and socioeconomic status index.
LTPA, leisure time physical activity; OPA, occupational physical activity; , maximal oxygen consumption.
Men and women who did no or less than 2 hours leisure time physical activity per week were more likely to have a low than participants who did 2 hours or more. The effect size did not change considerably when adjusting for occupational physical activity and other controls.
Multivariable analyses of the combined physical activity variable (fully adjusted model) showed that less-active men were more likely to have a low with ORs of 4.45 (95% CI 2.14 to 9.23) for no leisure time/low occupational physical activity, 2.34 (95% CI 1.08 to 5.07) for no leisure time/high occupational physical activity, 1.54 (95% CI 0.77 to 3.06) for <2 hours leisure time/low occupational physical activity, 1.54 (95% CI 0.75 to 3.16) for <2 hour leisure time/high occupational physical activity and 0.64 (95% CI 0.32 to 1.27) for ≥2 hours leisure time/low occupational physical activity compared with men with ≥2 hours leisure time/high occupational physical activity. The corresponding ORs for women were 6.54 (95% CI 2.98 to 14.3), 10.5 (95% CI 4.39 to 24.9), 3.52 (95% CI 1.75 to 7.09), 3.69 (95% CI 1.80 to 7.60) and 1.93 (95% CI 0.90 to 4.13), indicating women were most likely to have a low fitness if they worked in physically demanding jobs and did not engage in leisure time physical activity.
Based on the final model with the combined variable, we plotted predicted probabilities of having a low to show these different patterns for men and women (figure 2).
Figure 2.

Figure 2Predicted probabilities (with 95% CIs) of low by domain-specific physical activity among men and women who participated in the nationwide German Health Interview and Examination Survey for Adults. Adjusted for age, waist circumference, body mass index, smoking status, alcohol consumption and socioeconomic status index. LTPA, leisure time physical activity; OPA, occupational physical activity.
Discussion
Summary of results
This cross-sectional study showed a strong association between low leisure time physical activity and low estimated , but not between occupational physical activity and . The association between domain-specific physical activity and low also varied by sex. After adjustment for potential confounding, women working in physically demanding occupations who did not participate in leisure time physical activity had the highest likelihood of having a low . However, the men with the highest risk of low were those who did not engage in leisure time physical activity and were not working in physically demanding occupations.
Comparison with other studies
The strong association between leisure time physical activity and cardiorespiratory fitness has been shown in numerous studies.34 However, evidence of the association between occupational physical activity and cardiorespiratory fitness is inconclusive. Historically, occupational physical activity has been seen as a way to improve health in behavioural medicine, but as a potential health hazard in occupational medicine.6 40 Recent studies agree that occupational physical activity does not lead to increased cardiorespiratory fitness.41–44 A Swiss study among adults reported no association between the amount of objectively assessed steps during work-time and , and a lower among participants doing manual work than those doing sedentary work (according to reported job title), while controlling for leisure time physical activity and various other covariates.41 A cross-regional study in Germany also found higher levels of among participants with high levels of leisure time physical activity, but was lower among participants with higher levels of occupational physical activity (assessed by questionnaire).43 A study among the Danish working population observed that self-reported work and leisure sitting time had different associations with : there was a strong negative association between sitting leisure time and , but no similar association with sitting time at work.45 However, a study among male workers in Japan found higher levels of among those with self-reported high occupational physical activity than low46 and a study from Finland found a positive association between cardiorespiratory fitness and self-reported occupational physical activity even after adjustment for leisure time physical activity among young men.47
Occupational physical activity has been linked to negative health outcomes: in a meta-analysis, Li et al6 found evidence that it might increase the risk of cardiovascular disease, although leisure time physical activity considerably reduced the risk. Another meta-analysis found that men with high occupational physical activity had an increased risk of preliminary mortality, but women did not.7 In particular, the combination of high occupational physical activity with low cardiorespiratory fitness seems to be associated with a higher risk of adverse cardiovascular outcomes.48 49
Potential mechanisms
Regular aerobic exercise induces biological changes, such as increased stroke volume and decreased venous oxygen content, both of which lead to increased individual cardiorespiratory fitness.10 To increase , exercise should ideally be performed with sufficient intensity at ≥50% of the maximal aerobic capacity for untrained individuals.10 Cardiorespiratory fitness is determined by the cardiac output and arteriovenous oxygen difference, so it can be enhanced by an increase in stroke volume, oxygen difference or both.10 Leisure time physical activity, especially sport, is usually relatively short duration but high intensity, and provides sufficient recovery time between occasions. This is important, because this type of activity can achieve a training effect of the myocardium. This reduces the heart rate, the heart muscle remains longer in diastole and the stroke volume increases.50 In contrast, physical activity without recovery leads to prolonged elevation of heart rate and blood pressure.51 This can result in erosion of the endothelium, which can provoke atherosclerosis.52 This prolonged activity is typically observed in occupational physical activity, where workers also have limited control of work speed and duration.9 50 Sufficient recovery is therefore not possible, because individuals are unable to decide for themselves how to perform their work, and when to pause. Assuming average occupational physical activity as a constant, monotonous but low intensity activity, it has also been proposed that its intensity might be too low to increase individual fitness.9 However, this might not hold true for all occupations. Studies among blue-collar workers found that directly assessed intensity of physical activity was higher during work than leisure time,53 especially among those with low fitness levels.54
Differences between men and women
The results suggest that the association between domain-specific physical activity and cardiorespiratory fitness is different for men and women. High occupational physical activity was associated with lower fitness among women doing low levels of leisure time physical activity. Online supplementary table S1 shows that men in physically demanding occupations mainly worked in manual and technical professions (eg, electricians, plumbers and mechanics), and women in physically demanding jobs worked mainly in the service sector (eg, nursing/care, catering and cleaning). These service jobs are particularly affected by limited work control and higher job strain, which may be a possible explanation for these sex-specific patterns. For example, healthcare workers in Germany reported very high levels of job demands compared with the average level for all occupations, and also had low decision-making autonomy.55 56 This is particularly concerning because high-strain jobs can lead to lower leisure time physical activity57 and high occupational stress in combination with low cardiorespiratory fitness considerably increases the cardiovascular risk.58 These potential physiological mechanisms hold especially true for the most common high activity demand professions for women. For example, cleaners often work continuously for long periods, but at insufficient intensity to increase fitness, and this is coupled with a high relative workload.13
Recommendations for further research and practical implications
To take into account the observed sex differences, it is recommended that future studies should investigate men and women separately. It is generally assumed that high levels of leisure time physical activity increase individual cardiorespiratory fitness and are also beneficial for general health. However, some studies have found that a moderate-to-high level of leisure time physical activity was associated with adverse health outcomes among those exposed to high occupational physical activity levels.59 60 Thus, the inter-relationships between occupational and leisure time physical activity remain unclear and further research is needed to explain these potentially contradictory results. Furthermore, much of the research on this topic is based on self-reported physical activity with high heterogeneity among the instruments used. Future studies should investigate the domain-specific effects of physical activities using objective measures.61
When recommending higher levels of leisure time physical activities, it is important to consider the embedded and dependent relationship of the different domains of physical activity. Occupational and leisure time activity are not the only areas of physical activity. Transportation and domestic activities are also relevant. This is important because both these domains can also be described as non-discretionary time62 with limited individual autonomy. Second, physical activity in all these domains depends on structures at the societal, environmental and individual level.63 Individuals face obstacles in engaging in more leisure time physical activity, such as cultural temporal structures (eg, public transport timetables) or individual responsibilities (eg, parenthood). Thus, measures and policies to create an activity-friendly environment are needed, rather than blaming individuals for lack of exercise.1 Finally, we recommend that policy-makers and public health experts involved in the development of physical activity recommendations consider specifying these recommendations by level of occupational physical activity, because recent guidelines do not make this distinction.
Strengths and limitations
A major strength of this study is its use of a large population-based nationally representative sample of the non-institutionalised, resident adult working population. This allows the findings to be generalised. Significant efforts were made to reduce potential sources of bias in DEGS1,64 65 but our study still needs to be interpreted in the context of some limitations. First, the study’s cross-sectional design does not permit any causal inferences to be drawn about the observed relationship between physical activity patterns and cardiorespiratory fitness. It is well known that regular physical activity can increase cardiorespiratory fitness, but reversed causality cannot be ruled out: for example, individuals who have inherited a lower cardiorespiratory fitness may tend to be less active.66 We therefore cannot conclude that a higher cardiorespiratory fitness can be traced to higher leisure time physical activity levels. Second, due to the use of the PAR-Q screening questionnaire, our sample consists of a relatively healthy study-population. This implies the exclusion of most study participants using cardiorespiratory-related medication. However, it is possible that the use of other medications (eg, psychotropic or antidiabetic drugs) may act as a source of bias. The use of a relatively healthy study population may also have hampered the generalisability of our results. The results might also be affected by the so-called healthy worker effect, a specific form of selection bias where more healthy individuals are more likely to work in physically demanding occupations. Third, as in most large-scale epidemiological studies,10 34 was estimated using a submaximal ergometer test in a highly standardised and quality-assured procedure19 and not directly assessed by breath gas analysis. Fourth, self-reports on physical activity levels are prone to recall and social desirability bias.67 68 We cannot exclude the possibility that the level of physical activity was over-reported or under-reported. This is also true for most of the studies cited. Leisure time physical activity was assessed based on information about the duration per week, but not intensity, although intensity may have an additional impact on cardiorespiratory fitness.10 In the case of occupational physical activity, self-reports are restricted to specific task, such as lifting of heavy loads. In contrast, objectively measured activity levels usually include general activities at work. This is particularly important, because this type of task influences cardiorespiratory fitness in a different way from general activities. Fifth, occupational physical activity was assessed indirectly via job exposure matrices. These were based on a very large sample and the use of hierarchical linear regression models, controlling for age, sex, working hours and job experience, reduced the likelihood of confounding. However, they are generally not able to account for variability of exposure within jobs.69 If the prevalence of high physical demands within occupations varied widely, this could have led to biased results on observed occupational physical activity levels, which would reduce the magnitude of the observed associations.
Conclusions
This study showed a strong association between patterns of physical activity during leisure time and work and cardiorespiratory fitness among men and women in the working population in Germany. For example, women doing little or no leisure time physical activity were likely to have low cardiorespiratory fitness, especially if they worked in physically demanding jobs. These findings therefore contribute to the increasing body of evidence about different domain-specific effects of physical activity on health outcomes. They also emphasise the importance of considering different domains of physical activity in future studies. Current guidelines do not distinguish between work and leisure time physical activity, and it may be helpful to specify leisure time physical activity recommendations by occupational physical activity levels. Further research is needed to understand the pathways through which different domains of physical activity lead to divergent health effects and to confirm these findings with objective measures of physical activity.
Supplementary Material
Acknowledgments
The authors thank Melissa Leffler for editing a draft of this manuscript.
Footnotes
Contributors: GBMM and JDF were involved in the design and conduct of DEGS1, JDF in particular for the ergometer testing. JZ, LEK and JDF conceptualised the current study. JZ, MD and LEK conducted the analysis. JZ drafted the manuscript. GBMM, JDF and TK contributed to the analysis plan and interpretation of the results. MD, GBMM, JDF and TK critically revised it. All authors contributed to the interpretation of findings, reviewed, edited and approved the final manuscript.
Funding: The study was financed by the Robert Koch Institute which is a federal institute within the portfolio of the German Federal Ministry of Health.
Competing interests: None declared.
Patient consent for publication: Not required.
Ethics approval: DEGS1 was approved by the Federal and State Commissioners for Data Protection and by the Charité—Universitätsmedizin Berlin ethic committee (no EA2/047/08).
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data are available upon reasonable request. A dataset of DEGS1 is available via Public Use File (https://www.rki.de/EN/Content/Health_Monitoring/Public_Use_Files/application/application_node.html (accessed 23 September 2019)).
References
- 1.World Health Organization Global action plan on physical activity 2018–2030: more active people for a healthier world. Geneva: WHO, 2018. [Google Scholar]
- 2.World Health Organization Global action plan for the prevention and control of noncommunicable diseases 2013–2020. Geneva: WHO, 2013. [Google Scholar]
- 3.World Health Organization Global recommendations on physical activity for health. Geneva: WHO, 2010. http://www.who.int/dietphysicalactivity/global-PA-recs-2010.pdf [PubMed] [Google Scholar]
- 4.Ng SW, Popkin BM. Time use and physical activity: a shift away from movement across the globe. Obes Rev 2012;13:659–80. 10.1111/j.1467-789X.2011.00982.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Samitz G, Egger M, Zwahlen M. Domains of physical activity and all-cause mortality: systematic review and dose-response meta-analysis of cohort studies. Int J Epidemiol 2011;40:1382–400. 10.1093/ije/dyr112 [DOI] [PubMed] [Google Scholar]
- 6.Li J, Loerbroks A, Angerer P. Physical activity and risk of cardiovascular disease: what does the new epidemiological evidence show? Curr Opin Cardiol 2013;28:575–83. 10.1097/HCO.0b013e328364289c [DOI] [PubMed] [Google Scholar]
- 7.Coenen P, Huysmans MA, Holtermann A, et al. Do highly physically active workers die early? A systematic review with meta-analysis of data from 193 696 participants. Br J Sports Med 2018;52:1320–6. 10.1136/bjsports-2017-098540 [DOI] [PubMed] [Google Scholar]
- 8.Holtermann A, Hansen JV, Burr H, et al. The health paradox of occupational and leisure-time physical activity. Br J Sports Med 2012;46:291–5. 10.1136/bjsm.2010.079582 [DOI] [PubMed] [Google Scholar]
- 9.Holtermann A, Krause N, van der Beek AJ, et al. The physical activity paradox: six reasons why occupational physical activity (opa) does not confer the cardiovascular health benefits that leisure time physical activity does. Br J Sports Med 2018;52:149–50. 10.1136/bjsports-2017-097965 [DOI] [PubMed] [Google Scholar]
- 10.Ross R, Blair SN, Arena R, et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American heart association. Circulation 2016;134:e653–99. 10.1161/CIR.0000000000000461 [DOI] [PubMed] [Google Scholar]
- 11.Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA 2009;301:2024–35. 10.1001/jama.2009.681 [DOI] [PubMed] [Google Scholar]
- 12.Coenen P. Preventing disease by integrating physical activity in clinical practice: what works for whom? Heart 2018;104:1140–1. 10.1136/heartjnl-2017-312891 [DOI] [PubMed] [Google Scholar]
- 13.Korshøj M, Krustrup P, Jespersen T, et al. A 24-h assessment of physical activity and cardio-respiratory fitness among female Hospital cleaners: a pilot study. Ergonomics 2013;56:935–43. 10.1080/00140139.2013.782427 [DOI] [PubMed] [Google Scholar]
- 14.Finger JD, Tylleskär T, Lampert T, et al. Physical activity patterns and socioeconomic position: the German National health interview and examination survey 1998 (GNHIES98). BMC Public Health 2012;12:1079. 10.1186/1471-2458-12-1079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hobler D, Pfahl S, Spitznagel J, et al. WSI GenderDatenPortal [horizontal segregation of the labor market] 2020., 2017. Available: https://www.boeckler.de/121336.htm# [Accessed 10 Jan 2020].
- 16.Hands B, Parker H, et al. Male and female differences in health benefits derived from physical activity: implications for exercise prescription. J Womens Health Issues Care 2016;5 10.4172/2325-9795.1000238 [DOI] [Google Scholar]
- 17.Kurth B-M. The RKI health monitoring - What it contains and how it can be used [Das RKI-Gesundheitsmonitoring - Was es enthält und wie es genutzt werden kann]. Public Health Forum 2012;20:4.e1–4.e3. [Google Scholar]
- 18.Scheidt-Nave C, Kamtsiuris P, Gößwald A, et al. German health interview and examination survey for adults (DEGS) - design, objectives and implementation of the first data collection wave. BMC Public Health 2012;12:730. 10.1186/1471-2458-12-730 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Finger JD, Gößwald A, Härtel S, et al. Measurement of cardiorespiratory fitness in the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013;56:885–93. 10.1007/s00103-013-1694-5 [DOI] [PubMed] [Google Scholar]
- 20.Finger JD, Krug S, Gößwald A, et al. Cardiorespiratory fitness among adults in Germany: results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013;56:772–8. 10.1007/s00103-013-1672-y [DOI] [PubMed] [Google Scholar]
- 21.Deutsche Gesellschaft für Sportmedizin und Prävention (DGSP) PAR-Q-Fragebogen (German version), 2007. [Google Scholar]
- 22.Canadian Society for Exercise Physiology Physical Activity Readiness Questionnaire - PAR-Q (revised 2002). Ottawa: Health Canada, 2002. [Google Scholar]
- 23.Andersen KL, Shephard R, Denolin H, et al. Fundamentals of exercise testing, 1971. Available: https://apps.who.int/iris/handle/10665/40145 [Accessed 15 Feb 2019].
- 24.Tanaka H, Monahan KD, Seals DR. Age-predicted maximal heart rate revisited. J Am Coll Cardiol 2001;37:153–6. 10.1016/S0735-1097(00)01054-8 [DOI] [PubMed] [Google Scholar]
- 25.Gore CJ, Booth ML, Bauman A, et al. Utility of pwc75% as an estimate of aerobic power in epidemiological and population-based studies. Med Sci Sports Exerc 1999;31:348–51. 10.1097/00005768-199902000-00020 [DOI] [PubMed] [Google Scholar]
- 26.American College of Sports Medicine ACSM's guidelines for exercise testing and prescription. 280 5th Edition Baltimore: Williams & Wilkins, 1995. [DOI] [PubMed] [Google Scholar]
- 27.Kroll LE. Konstruktion und Validierung eines allgemeinen Index für die Arbeitsbelastung in beruflichen Tätigkeiten anhand von ISCO-88 und KldB-92 [Construction and validation of a general index for job demands in occupations based on ISCO-88 and KldB-92]. Methoden — Daten — Analysen 2011;5:63–90. [Google Scholar]
- 28.Rohrbach-Schmidt D, Hall A. BIBB/BAuA employment survey 2012. Bonn, Germany: BIBB-FDZ Data and Methodological Reports Federal Institute for Vocational Education and Training, 2013. [Google Scholar]
- 29.Kroh M, Neiss H, Kroll L, et al. Menschen mit hohem Einkommen leben länger [High-income people live longer]. DIW-Wochenbericht 2012;79:3–15. [Google Scholar]
- 30.Santi I, Kroll LE, Dietz A, et al. To what degree is the association between educational inequality and laryngeal cancer explained by smoking, alcohol consumption, and occupational exposure? Scand J Work Environ Health 2014;40:315–22. 10.5271/sjweh.3403 [DOI] [PubMed] [Google Scholar]
- 31.Santi I, Kroll LE, Dietz A, et al. Occupation and educational inequalities in laryngeal cancer: the use of a job index. BMC Public Health 2013;13:1080. 10.1186/1471-2458-13-1080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Krug S, Jordan S, Mensink GBM, et al. Physical activity: results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013;56:765–1. 10.1007/s00103-012-1661-6 [DOI] [PubMed] [Google Scholar]
- 33.Steinbach D, Graf C. Leisure time physical activity and sedentariness : Kirch W, Encyclopedia of public health. Dordrecht: Springer, 2008: 849–51. [Google Scholar]
- 34.Zeiher J, Ombrellaro KJ, Perumal N, et al. Correlates and determinants of cardiorespiratory fitness in adults: a systematic review. Sports Med Open 2019;5:39. 10.1186/s40798-019-0211-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Zeiher J, Manz K, Kuntz B, et al. Individual and interpersonal correlates of cardiorespiratory fitness in adults - Findings from the German Health Interview and Examination Survey. Sci Rep 2020;10:445. 10.1038/s41598-019-56698-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.World Health Organization Bmi classification, 2019. Available: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html [Accessed 20 Feb 2019].
- 37.World Health Organization Obesity: preventing and managing the global epidemic. Geneva: World Health Organization, 2000. [PubMed] [Google Scholar]
- 38.Lampert T, Kroll L, Müters S, et al. Measurement of socioeconomic status in the German health interview and examination survey for adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013;56:1–5. [DOI] [PubMed] [Google Scholar]
- 39.Graubard BI, Korn EL. Predictive margins with survey data. Biometrics 1999;55:652–9. 10.1111/j.0006-341X.1999.00652.x [DOI] [PubMed] [Google Scholar]
- 40.Morris JN, Heady JA, Raffle PA, et al. Coronary heart-disease and physical activity of work. Lancet 1953;262:1111–20. 10.1016/S0140-6736(53)91495-0 [DOI] [PubMed] [Google Scholar]
- 41.Mundwiler J, Schüpbach U, Dieterle T, et al. Association of occupational and leisure-time physical activity with aerobic capacity in a working population. PLoS One 2017;12:e0168683. 10.1371/journal.pone.0168683 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ruzic L, Heimer S, Misigoj-Durakovic M, et al. Increased occupational physical activity does not improve physical fitness. Occup Environ Med 2003;60:983–5. 10.1136/oem.60.12.983 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Bahls M, Groß S, Baumeister SE, et al. Association of domain-specific physical activity and cardiorespiratory fitness with all-cause and cause-specific mortality in two population-based cohort studies. Sci Rep 2018;8:16066. 10.1038/s41598-018-34468-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lakka TA, Laaksonen DE, Lakka H-M, et al. Sedentary lifestyle, poor cardiorespiratory fitness, and the metabolic syndrome. Med Sci Sports Exerc 2003;35:1279–86. 10.1249/01.MSS.0000079076.74931.9A [DOI] [PubMed] [Google Scholar]
- 45.Saidj M, Jørgensen T, Jacobsen RK, et al. Differential cross-sectional associations of work- and leisure-time sitting, with cardiorespiratory and muscular fitness among working adults. Scand J Work Environ Health 2014;40:531–8. 10.5271/sjweh.3443 [DOI] [PubMed] [Google Scholar]
- 46.Nagaya T, Kondo Y, Shibata T. Effects of sedentary work on physical fitness and serum cholesterol profile in middle-aged male workers. Int Arch Occup Environ Health 2001;74:366–70. 10.1007/PL00007954 [DOI] [PubMed] [Google Scholar]
- 47.Tammelin T, Näyhä S, Rintamäki H, et al. Occupational physical activity is related to physical fitness in young workers. Med Sci Sports Exerc 2002;34:158–65. 10.1097/00005768-200201000-00024 [DOI] [PubMed] [Google Scholar]
- 48.Holtermann A, Mortensen OS, Burr H, et al. Physical work demands and physical fitness in low social classes--30-year ischemic heart disease and all-cause mortality in the Copenhagen Male Study. J Occup Environ Med 2011;53:1221–7. 10.1097/JOM.0b013e318233865f [DOI] [PubMed] [Google Scholar]
- 49.Holtermann A, Mortensen OS, Burr H, et al. Physical demands at work, physical fitness, and 30-year ischaemic heart disease and all-cause mortality in the Copenhagen male study. Scand J Work Environ Health 2010;36:357–65. 10.5271/sjweh.2913 [DOI] [PubMed] [Google Scholar]
- 50.Krause N. Physical activity and cardiovascular mortality--disentangling the roles of work, fitness, and leisure. Scand J Work Environ Health 2010;36:349–55. 10.5271/sjweh.3077 [DOI] [PubMed] [Google Scholar]
- 51.Hall C, Heck JE, Sandler DP, et al. Occupational and leisure-time physical activity differentially predict 6-year incidence of stroke and transient ischemic attack in women. Scand J Work Environ Health 2019;45:267–79. 10.5271/sjweh.3787 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Khera A, Mitchell JH, Levine BD. Preventive cardiology: The effects of exercise In: Willerson JT, Cohn JN, Wellens HJJ, et al., eds Cardiovascular medicine: Springer, 2007: 2631–48. [Google Scholar]
- 53.Gram B, Westgate K, Karstad K, et al. Occupational and leisure-time physical activity and workload among construction workers - a randomized control study. Int J Occup Environ Health 2016;22:36–44. 10.1080/10773525.2016.1142724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Coenen P, Korshøj M, Hallman DM, et al. Differences in heart rate reserve of similar physical activities during work and in leisure time - A study among Danish blue-collar workers. Physiol Behav 2018;186:45–51. 10.1016/j.physbeh.2018.01.011 [DOI] [PubMed] [Google Scholar]
- 55.Schmucker R. Arbeitsbedingungen in Pflegeberufen [Working conditions in nursing care] : Jacobs K, Kuhlmey A, Greß S, et al., Pflege-Report 2019: Mehr Personal in der Langzeitpflege - aber woher. Berlin, Heidelberg: Springer, 2019: 49–60. [Google Scholar]
- 56.Theobald H, Szebehely M, Preuß M. Arbeitsbedingungen in der Altenpflege [Working conditions in geriatric care]. Berlin: Sigma, 2013. [Google Scholar]
- 57.Fransson EI, Heikkilä K, Nyberg ST, et al. Job strain as a risk factor for leisure-time physical inactivity: an individual-participant meta-analysis of up to 170,000 men and women: the IPD-Work Consortium. Am J Epidemiol 2012;176:1078–89. 10.1093/aje/kws336 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Schilling R, Colledge F, Ludyga S, et al. Does cardiorespiratory fitness moderate the association between occupational stress, cardiovascular risk, and mental health in police officers? Int J Environ Res Public Health 2019;16:E2349. 10.3390/ijerph16132349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Clays E, De Bacquer D, Janssens H, et al. The association between leisure time physical activity and coronary heart disease among men with different physical work demands: a prospective cohort study. Eur J Epidemiol 2013;28:241–7. 10.1007/s10654-013-9764-4 [DOI] [PubMed] [Google Scholar]
- 60.Korshøj M, Lidegaard M, Skotte JH, et al. Does aerobic exercise improve or impair cardiorespiratory fitness and health among cleaners? a cluster randomized controlled trial. Scand J Work Environ Health 2015;41:140–52. 10.5271/sjweh.3475 [DOI] [PubMed] [Google Scholar]
- 61.Ketels M, De Bacquer D, Geens T, et al. Assessing physiological response mechanisms and the role of psychosocial job resources in the physical activity health paradox: study protocol for the Flemish employees' physical activity (FepA) study. BMC Public Health 2019;19:765. 10.1186/s12889-019-6950-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.van Tienoven TP, Deyaert J, Harms T, et al. Active work, passive leisure? associations between occupational and non-occupational physical activity on weekdays. Soc Sci Res 2018;76:1–11. 10.1016/j.ssresearch.2018.08.012 [DOI] [PubMed] [Google Scholar]
- 63.Bauman AE, Reis RS, Sallis JF, et al. Correlates of physical activity: why are some people physically active and others not? Lancet 2012;380:258–71. 10.1016/S0140-6736(12)60735-1 [DOI] [PubMed] [Google Scholar]
- 64.Gößwald A, Lange M, Dölle R, et al. The first wave of the German health interview and examination survey for adults (DEGS1). recruitment of participants, fieldwork, and quality assurance. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013;56:1–8. [DOI] [PubMed] [Google Scholar]
- 65.Kamtsiuris P, Lange M, Hoffmann R, et al. The first wave of the German health interview and examination survey for adults (DEGS1). sampling design, response, weighting, and representativeness. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013;56:1–10. [DOI] [PubMed] [Google Scholar]
- 66.Després J-P. Physical activity, sedentary behaviours, and cardiovascular health: when will cardiorespiratory fitness become a vital sign? Can J Cardiol 2016;32:505–13. 10.1016/j.cjca.2015.12.006 [DOI] [PubMed] [Google Scholar]
- 67.Prince SA, Adamo KB, Hamel ME, et al. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int J Behav Nutr Phys Act 2008;5:56. 10.1186/1479-5868-5-56 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Brenner PS, DeLamater J, Lies DJ. Lies, damned lies, and survey Self-Reports? identity as a cause of measurement bias. Soc Psychol Q 2016;79:333–54. 10.1177/0190272516628298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Tielemans E, Heederik D, Burdorf A, et al. Assessment of occupational exposures in a general population: comparison of different methods. Occup Environ Med 1999;56:145–51. 10.1136/oem.56.3.145 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2019-034610supp001.pdf (173.4KB, pdf)