

Abstract
Objectives
To evaluate skin barrier and hydration effects of a new rebalancing moisture treatment (TRMT) and to assess efficacy and tolerability in subjects with photodamaged skin.
Methods
In an epidermal skin model, tissues (n = 5/group) were topically treated with 25 µL of TRMT, 25 µL of a market‐leading moisturizer (MLM), or untreated for 60 minutes. Hydration was measured at 0, 15, and 30 minutes. Tissues were harvested for gene expression analysis of markers associated with skin barrier and hydration: Claudin (CLD), Aquaporin (AQP), Hyaluronic Acid Syntheses (HAS), and Hyaluronidase (HYAL). A clinical study evaluated twice‐daily application of TRMT, assessing changes in fine lines/wrinkles, brightness, texture, erythema, and tolerability from baseline through week 8. Hydration was measured using electrical impedance.
Results
TRMT and MLM demonstrated significant increases in hydration vs untreated tissue at each timepoint (P < .005), with greater hydration effects observed for TRMT vs MLM. TRMT‐treated tissues demonstrated greater expression of CLD, AQP, and HA, and reduced expression of HYAL vs untreated and MLM‐treated tissues. Twice‐daily application of TRMT demonstrated significant improvements at 2 weeks in fine lines/wrinkles (P < .001), brightness (P < .0001), texture (P < .0004), and hydration (P < .004). At 8 weeks, statistically significant improvements were achieved in all categories.
Conclusion
In an epidermal skin model, TRMT demonstrated significant increases in hydration, greater hydration effects, and expression of key markers associated with skin barrier and hydration vs a MLM. Twice‐daily application of TRMT was well tolerated and resulted in early, significant improvements in hydration and visible improvements in skin brightness, texture, fine lines/wrinkles, and erythema at 8 weeks.
Keywords: cosmeceutical, hydration, moisturizing, photoaging of the skin, skin barrier
1. INTRODUCTION
Youthful skin is characterized by its turgor, resilience, and pliability, in large part owing to its high water content. Skin aging is a complex biological process that includes both intrinsic and extrinsic factors. Natural skin aging is associated with a significant reduction in the capacity of skin to retain water, as well as decreased sebum production (particularly in women).1, 2, 3, 4 In addition to intrinsic changes, extrinsic factors, including exposure to ultraviolet (UV) radiation, smog, and cigarette smoke, also cause loss of skin hydration and impairments to barrier function.4, 5 Together, these changes lead to dry skin and contribute to other aging‐related manifestations, including fine lines and wrinkles, and dull and uneven skin tone and texture.
Skin is the first layer of defense against external insults to the body and is instrumental in protecting the body from harmful substances such as bacteria.1 Healthy, hydrated skin constantly renews itself to maintain the barrier's protective function.6 However, excessive environmental exposure can compromise and overwhelm the innate ability of the skin barrier to maintain and repair itself. Compared with adequately hydrated skin, dry or compromised skin, owing to aging or excessive environmental exposure, is characterized by a thicker stratum corneum and a weaker barrier.7, 8 This manifests as xerosis and an increased vulnerability to infection, irritation, and allergens, as well as other consequences associated with environmental insults, including malignancies and skin diseases.9, 10 Skin requires adequate hydration levels to maintain epidermal barrier integrity and normal functional activities.6
Optimal water content is essential in maintaining a healthy barrier as well as other health‐related and cosmetic benefits to skin.11 Three critical elements in supporting skin hydration include the maintenance of natural moisturizing factors (NMF), the skin's natural lipid bilayer, and hyaluronic acid (HA). These elements work together to facilitate and maintain moisturization of the epidermis and underlying skin structures to ensure a healthy barrier.
Natural moisturizing factors are comprised of a group of highly efficient humectants that attract and bind water from the atmosphere and are essential to water retention in the stratum corneum. Filaggrin, a large protein localized in the corneocyte layer in the stratum corneum, is converted to NMF in the more superficial layers of the stratum corneum.12 Proteolysis of filaggrin is dependent on water activity within the corneocytes as well as external relative humidity and can only occur within a narrow range of water activity within corneocytes.12 Of note, exposure to UV radiation has been shown to impair the natural degradation of filaggrin into NMF.12
Components of NMF include amino acids and derivatives of amino acids, such as pyrrolidone carboxylic acid (PCA), lactic acid, and urea. Lactic acid stimulates synthesis of ceramides and improves and prevents symptoms associated with xerosis; urea stimulates expression of enzymes involved in the synthesis of ceramides and aquaporins (AQPs). Often referred to as “water pores” or “water channels”, AQPs are transmembrane proteins that transport and distribute water (as well as glycerol and urea) throughout the epidermis.13, 14 Sufficient levels of NMF maintain adequate hydration of the stratum corneum, skin plasticity, and optimize barrier function. Suboptimal levels of NMF can manifest clinically as dry skin with scaling, flaking, and cracking, and have been associated with conditions such as atopic dermatitis and psoriasis.7, 8, 12
Primary intercellular barrier lipids, including cholesterol, essential fatty acids (EFAs), and ceramides, work together to form a barrier to prevent transepidermal water loss (TEWL). Barrier lipids help maintain skin's natural collagen, elastin, and proteins by minimizing TEWL, increasing hydration, and reinforcing the protective barrier. TEWL impairs the normal desquamation process, leading to dry flaky skin. All three barrier lipids are needed for proper maturation and natural skin desquamation in the stratum corneum.14 Notably, atopic dermatitis is characterized by a reduction in all three key barrier lipids.15 Corneocytes, where filaggrin originates, are embedded in the barrier lipids of the stratum corneum and have a primary role in supporting barrier function.16 Essential fatty acids are primarily composed of polyunsaturated fatty acids such as linoleic acid, which is the most abundant type of polyunsaturated fatty acid.
A third critical component involved in skin moisturization is hyaluronan or hyaluronic acid (HA). HA is a glycosaminoglycan (GAG) and predominant element of the extracellular matrix; the synthesis of epidermal HA is greatly influenced by the dermis. Hydration of the skin depends on HA's unique capacity to bind and retain water molecules in the dermis and epidermis. In addition to its rapid turnover rate in the skin (~24 hours), both intrinsic and extrinsic factors contribute to a marked reduction of epidermal HA, making it one of the most dramatic changes observed in senescent skin.17 HA synthase (HAS) is an enzyme that facilitates HA synthesis; hyaluronidase is an enzyme that degrades HA. Skin moisturization is optimized by agents that maximize HAS and minimize HYAL.
A compromised skin barrier requires supplemental support that promotes synthesis of HA and inhibits its breakdown, as well as maintains sufficient levels of NMF and lipids to keep skin moisturized and hydrated. Moisturizers are an essential component of a skin‐care regimen.18 Ideally, they mimic the skin's own natural moisturizing systems19 and help to rebalance skin by supporting barrier function and enhancing hydration. Using advanced chemistry, a unique moisturizing treatment cream (TRMT) has been developed to address the three critical elements to natural skin moisturization. The ingredients in TRMT were specifically selected to bolster adequate stratum corneum hydration by supporting NMF, enhance barrier function by maximizing lipid content of the skin, and replenish HA by supporting its synthesis and reducing its degradation (Table 1).
Table 1.
TRMT key ingredients
| Key ingredient | Skin benefits | |
|---|---|---|
| Natural moisturizing factors (NMF) | Urea complex | Increases skin's resiliency and provides intense moisturization |
| Sodium PCA | Enhances skin moisture, smoothness, feelings of elasticity | |
| Salicornia herbacea extract | Supports “water channels” | |
| Carnosine | Biomimetic peptide, targets glycation, supports promotion of NMF | |
| Sodium lactate | Helps retain water in the skin | |
| Barrier function | Cholesterol | Lipid, enhances barrier function |
| Ceramides 1 and 3 | Supports hydration, reinforces skin's barrier | |
| Linoleic and linolenic acids | EFAs, support skin's barrier (Omega‐6, Omega‐3) | |
| Carnitine | Naturally occurring amino acid, restores and hydrates skin | |
| Squalene | Naturally occurs in skin, supports moisture retention | |
| Hyaluronic acid | Aminopropyl ascorbyl phosphate | Reduces HA degradation, increases skin smoothness |
| Sodium lactate | Promotes HA, keeps skin soft, supple | |
| Sodium hyaluronate | Helps provide skin with high moisture retention, free‐radical protection | |
| Support | Glycerin | Provides hydration to skin |
| Caffeine | Enhances hydration | |
| Jojoba esters | Provides hydration, supports skin's barrier |
As part of a research program evaluating the efficacy of TRMT, we first investigated the effect of TRMT on hydration and analyzed, via gene expression, key markers associated with skin barrier function and hydration utilizing a reconstructed human epidermal skin model. In a second study, we examined the clinical efficacy and tolerability of TRMT over 8 weeks in healthy subjects with moderate to severe photodamaged skin.
2. EVALUATING SKIN HYDRATION AND BARRIER EFFECTS UTILIZING AN EPIDERMAL SKIN MODEL
2.1. Objective
To evaluate TRMT and a market‐leading moisturizer, via gene expression analysis, for effects on hydration and key epidermal barrier markers in a human epidermal skin model.
2.2. Materials and methods
This study utilized highly differentiated, human epidermal skin tissues (EpiDermFT™; MatTek Corp.) comprised of normal, human‐derived epidermal keratinocytes. This model contains organized and proliferative basal cells, spinous and granular layers, as well as cornified epidermal layers that are both mitotically and metabolically active. Tissues were equilibrated in 2.5 mL of EFT‐400‐MM media for 1 hour at 37°C/5%CO2. Media was replaced, and tissues were incubated at 37°C/5%CO2 for 18 + 3 hours. On Day 1, tissues were equilibrated to room temperature for 90 minutes, after which basal electrical impedance of the tissues was measured using a Nova Meter (NOVA™ DPM 9003BT; NOVA Technology Corp.). Tissues were divided into three different groups of tissues (N = 5, each): untreated (negative control; NC), TRMT, and a market‐leading moisturizer (MLM).
2.2.1. Hydration evaluation
Tissues were topically treated for 60 minutes with 25 µL of the two test formulations; the third group of tissues remained untreated. Residual test formulations were removed from tissue surfaces with a sterile swab. Immediately 0, 15, and 30 minutes following removal, epidermal hydration was evaluated using a Nova Meter. Media was replaced and tissues were re‐dosed with test formulations and incubated at 37°C/5%CO2 for 24 ± 2 hours.
2.2.2. Biomarker evaluation
On Day 2, tissues were harvested for gene expression analysis (N = 3, each). Tissues were then fixed in 8 mL of 10% formalin for 24 ± 3 hours for histological processing and H&E staining. Key biomarkers were analyzed using real‐time quantitative polymerase chain reaction (RT qPCR), a standard laboratory technique in which copies of genes are generated over a short period of time to allow for more accurate or robust measurement. cDNA was synthesized using total RNA with Qiagen reagents; total RNA was isolated using RNAqueous kit (Ambion; Thermo Fisher Scientific) following the manufacturer's procedure. Expression of the following biomarkers was evaluated: Aquaporin (AQP; proteins that transport water, glycerol, and urea across cell membranes), Claudin (CLD; a component of tight junction proteins that regulates permeability of the stratum corneum), Hyaluronic Acid Synthase (HAS; an enzyme responsible for HA synthesis), and Hyaluronidase (HYAL; an enzyme that degrades HA).
2.3. Results
2.3.1. Epidermal hydration
After 60 minutes of treatment, tissues treated with TRMT exhibited higher hydration potential than a MLM immediately following removal of product (456 vs 302 DPM Units, respectively). Additionally, TRMT‐treated tissues retained hydration for a longer duration of time (at 15 and 30 minutes) where hydration effects were greater than that of an MLM.
Tissues treated with TRMT demonstrated statistically significant increases in hydration vs NC at 0, 15, and 30 minutes following application (P < .005) (Figure 1). Tissues treated with TRMT demonstrated up to 2x greater hydration effects compared with tissues treated with MLM.
Figure 1.
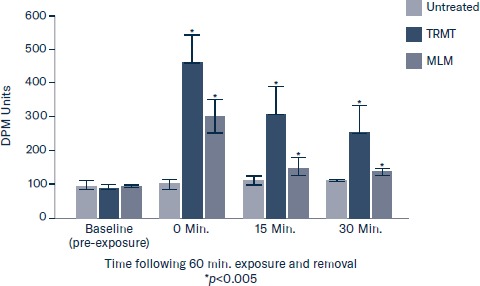
Epidermal hydration in tissues following 60 min of exposure
2.3.2. Expression of biomarkers
mRNA expression of epidermal barrier biomarkers was analyzed 24 hours after treatment with TRMT and a MLM. TRMT‐treated tissues demonstrated greater expression of key biomarkers vs NC and MLM, with greater expression of CLD, AQP, and HAS. TRMT also substantially reduced expression of HYAL compared with the MLM (Figure 2A‐D).
Figure 2.

Expression of epidermal barrier biomarkers in tissues: A, claudin (CLD); B, aquaporin (AQP), C, hyaluronic acid synthase (HAS), and D, hyaluronidase (HYAL)
3. EFFICACY AND TOLERABILITY IN PHOTODAMAGED SKIN
3.1. Study objectives
This open‐label, dual‐center study evaluated efficacy and tolerability in subjects with moderate to severe photodamaged skin following twice‐daily application of TRMT over 8 weeks across two dermatology research centers.
3.2. Study design and methods
This study evaluated improvements from baseline in the appearance of fine lines/wrinkles, erythema, skin brightness, skin texture, and pore size at 2, 4, and 8 weeks based on a 6‐point grading scale (0 = none, 1 = minimal, 2 = mild, 3 = moderate, 4 = moderately severe, and 5 = severe) using expert‐graded digital photographic assessment (Canfield VISIA® CR). Subjects were instructed to apply TRMT to clean skin twice daily, AM and PM, for 8 weeks. In addition, changes in global improvement were evaluated at weeks 2, 4, and 8 using a 5‐point scale (0 = no improvement, 1 = minimal Improvement, 2 = mild Improvement, 3 = Mmderate Improvement, and 4 = marked Improvement).
Changes in skin hydration were evaluated from baseline at weeks 2, 4, and 8 using noninvasive, bioinstrumentation (NOVA™ DPM 9003BT; NOVA Technology Corp.). Prior to imaging and skin hydration measurements, subjects were required to cleanse their face and acclimate to the treatment room for at least 30 minutes. Measurements were obtained by placing the probe with low pressure in a vertical manner against the surface of the cheek; three consecutive readings were obtained from the same location. Increases in post‐treatment readings from baseline indicate a hydrating effect resulting from increased skin moisture content, whereas decreases indicate a drying effect.
Subjects completed self‐assessment questionnaires at weeks 2, 4, and 8. Adverse events (AEs) were captured throughout the study period.
3.2.1. Study subjects
Eligible subjects included healthy men and women between the ages of 35 and 65 years with moderate to severe photodamage, Fitzpatrick Skin Types (FST) II‐V, and no known medical conditions that could interfere with study participation. Subjects agreed to use only sponsor‐supplied skin‐care products and minimize sun exposure. Subjects were excluded from study participation if they had any disorder which may have interfered with accurate evaluation (such as, but not limited to, any active inflammatory skin condition, severe acne vulgaris, acne conglobata, acne fulminans, facial seborrheic dermatitis, diabetes, chronic kidney or liver disease, autoimmune disease, or anyone undergoing cancer treatment, taking systemic steroid medication, or an immunosuppressive agent); were pregnant or breastfeeding; had concurrent use of topical or oral medication that could interfere with evaluation; and/or concurrent or recent use of any skin‐care product(s) (cosmetic, prescription, and nonprescription) or procedure(s) within the past 2 months, which may interfere with evaluation. Subjects were also excluded if they were unable or unwilling to comply with the study protocol, including refraining from sunbathing. In order to minimize the potential influence of additional ingredients found in some moisturizers, such as peptides, growth factors, retinol, or AHAs, on baseline measurements, subjects routinely using any hydration cream(s) or moisturizer(s) at baseline underwent a brief 1‐week washout period. There was no washout period regarding use of sunscreen. Throughout the study, subjects were instructed to apply a broad‐spectrum sunscreen (SPF46) in the morning 30 minutes prior to being outdoors, reapply as needed, and to utilize a basic daily cleanser prior to application of the study product.
This study was conducted in accordance with all applicable guidelines for the protection of human subjects for research as outlined in 21 CFR 50, the accepted standards for Good Clinical Practice (GCP), and approved by Advarra IRB (Columbia, MD).
3.2.2. Statistical methods
Mean (LS) improvement and mean (LS) percent improvement from baseline to each timepoint for category was analyzed using a t test. The significance of improvement over time was analyzed using a mixed effects model.
3.3. Results
Forty subjects with an average age of 57 years were enrolled in this study; 39 completed the study (one subject withdrew). The majority of subjects were female (1 male subject), FST III, and had moderate photodamage.
Expert assessments demonstrated significant mean percent improvements from baseline in the appearance of fine lines/wrinkles (15%; P < .0001), erythema (32%; P = .0009), skin brightness (144%; P < .0001), and skin texture (23%; P < .0001) following twice‐daily use after 8 weeks (Figure 3A‐C). Visible improvements in fine lines/wrinkles and skin texture were demonstrated as early as week 2, as well as a 54% increase in skin brightness from baseline (P < .0001). Statistically significant differences were observed in all categories by week 4, with continued, progressive improvements from baseline achieved in all categories by week 8. Nova Meter measurements demonstrated an 11% increase in hydration at 2 weeks (P < .004), 36% increase at 4 weeks (P < .0001), and 25% increase at 8 weeks (P = .0002) (Figure 4). Global improvement was statistically significant at all timepoints (P < .0001).
Figure 3.

A, Demonstrated improvements from baseline through week 8. B, Unretouched digital photography on clean face at Baseline and at week 8. C, Unretouched digital photography on clean face at Baseline and at week 8. * indicates statistical significance of P < .04 to P < .0001
Figure 4.
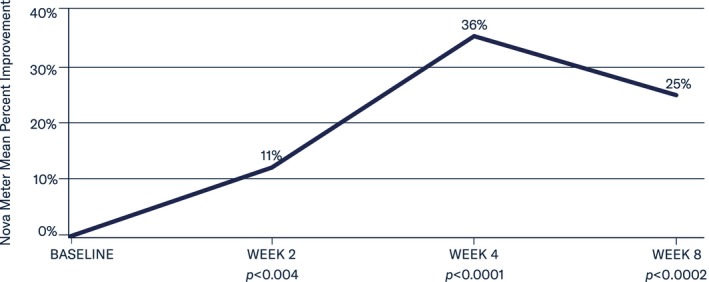
Demonstrated improvements in hydration from baseline through week 8
After 8 weeks, nearly all subjects reported that TRMT made their skin feel moisturized (97%), smoother (92%), softer (95%), less dry, and less rough (90%, each), and did not make their skin feel greasy (97%). Subjects reported that TRMT worked well with their makeup, and nearly all reported it absorbed easily. Prior to using TRMT, only 7% of subjects described their skin tone as bright, this increased to 48% at 4 weeks and 51% after 8 weeks of use. Similarly, the percentage of subjects who described their skin texture as smooth and soft doubled from 20% at study outset to 40% at 4 weeks and 54% at 8 weeks.
Adverse events deemed possibly related to study product included perioral break‐out (n = 2) and one subject who reported experiencing rash/hives at 4 weeks leading to study discontinuation.
4. DISCUSSION
Healthy, hydrated skin constantly renews itself and is able to maintain its protective barrier despite environmental insults and age‐related changes.6, 9 Sufficient hydration is essential for maintaining the skin's barrier11 and is dependent upon optimal levels of hyaluronic acid, NMF, and lipids to keep the barrier moisturized and hydrated. Clinical consequences of insufficient hydration include dry skin, manifestations of aging, and increased vulnerability to environmental factors.9
Moisturizers are a key component of every skin‐care regimen.18 Ideal moisturizers mimic the skin's own natural moisturizing systems, and address primary goals including repairing and restoring the barrier and barrier function, and increasing hydration or water content on the skin.19 There are many types of moisturizers, and not all are designed to or capable of mitigating xerosis.14 While occlusive agents coat the skin with friction‐reducing substances like silicones to increase skin smoothness, their benefits are temporary.14, 15, 18, 19 More than just coating the surface of skin, effective moisturizers are capable of improving skin barrier homeostasis and function. Additionally, ideal moisturizers are appropriate for use in sensitive and compromised skin, quickly absorbed, and long‐lasting.13, 14, 20, 21
The moisture treatment cream highlighted in these studies was designed to address three critical components essential to natural skin moisturization. This unique approach bolsters skin's innate mechanism for restoring and maintaining proper moisturization by supporting the modulation of hyaluronic acid, natural moisturizing factors and external barrier lipids for optimal functioning of the skin barrier.
Results from in vitro and in vivo studies performed support TRMT's effect on skin hydration and barrier function, as well as its effectiveness in enhancing hydration and visibly improving photodamaged skin in healthy subjects. Using a reconstructed human epidermal skin model, tissues treated with TRMT demonstrated statistically significant increases in hydration at all timepoints vs untreated control and demonstrated up to two times greater hydration compared with a market‐leading moisturizer. Tissues treated with TRMT demonstrated greater expression of CLD, AQP, and HAS vs a MLM. CLDs are proteins that are the most important components of tight junctions and thus play an important role in enhancing barrier function by regulating the flow of water through the epidermis.22 AQPs function as molecular water channel proteins that transport and distribute water, glycerol, and urea throughout the epidermis.13, 14 Hyaluronic acid is comparable to a skin hydration reservoir—attracting and maintaining moisture. Increased expression of HAS and decreased expression of HYAL, as was observed in tissues treated with TRMT, facilitates hyaluronan synthesis and increased water retention in the skin.
The physiologic benefits of TRMT demonstrated through gene expression analysis in the epidermal skin model translated to clinically significant improvements in the appearance of photodamaged skin after 8 weeks of twice‐daily application. TRMT use led to significant improvements in the appearance of fine lines/wrinkles, erythema, skin brightness, and skin texture, as well as significant improvements in skin hydration based on objective biometric measurements over 8 weeks. Despite extreme changes in temperatures during the winter months on the east coast, subjects continued to experience significant increases in hydration through week 8. TRMT was well tolerated and nearly all subjects reported that TRMT made their skin feel moisturized, smoother, and softer, and was cosmetically elegant—nongreasy and worked well with makeup.
Limitations of this study include conducting additional research in a larger population for a longer duration, as this would be beneficial in understanding the long‐term benefits of TRMT. Additionally, although it is routine to include washout periods when evaluating a new treatment in an effort to minimize the number of variables potentially attributed to treatment effects, subjects who regularly used moisturizers may have presented with drier skin at the baseline timepoint due to the 1‐week washout period. Finally, in this study each subject served as their own control in measuring changes from baseline over an 8‐week period. Additional studies may include the use of a separate control group.
5. CONCLUSIONS
Together, these studies demonstrate the physiologic and clinical benefits of a new rebalancing moisture treatment cream. In an epidermal skin model, TRMT increased hydration and expression of key markers associated with enhanced barrier function. These effects were greater than a market‐leading moisturizer. Clinical manifestations of these effects led to significant increases in hydration and visible improvements in subjects with photodamaged skin as early as two weeks after treatment initiation, with continued progressive improvements through 8 weeks.
CONFLICT OF INTEREST
Dr McDaniel served as an investigator to skinbetter science. Dr Jeffrey Dover served as an investigator to skinbetter science. Dr Mitch Wortzman and Ms Diane Nelson are employees of skinbetter science.
ACKNOWLEDGMENTS
We would like to thank Lynne Kolton Schneider, PhD, for her editorial assistance on this manuscript.
McDaniel DH, Dover JS, Wortzman M, Nelson DB. In vitro and in vivo evaluation of a moisture treatment cream containing three critical elements of natural skin moisturization. J Cosmet Dermatol. 2020;19:1121–1128. 10.1111/jocd.13359
Funding information
This study was funded by skinbetter science, LLC.
REFERENCES
- 1. Luebberding S, Krueger N, Kerscher M. Age‐related changes in skin barrier function – quantitative evaluation of 150 female subjects. Int J Cosmet Sci. 2013;35(2):183‐190. [DOI] [PubMed] [Google Scholar]
- 2. Leubberding S, Krueger N, Kerscher M. Skin physiology in men and women: in vivo evaluation of 300 people including TEWL, SC hydration, sebum content and skin surface pH. Int J Cosmet Sci. 2013;35(5):477‐483. [DOI] [PubMed] [Google Scholar]
- 3. Narurkar VA, Fabi SG, Bucay VW, et al. Rejuvenating hydrator: restoring epidermal hyaluronic acid homeostasis with instant benefits. J Drugs Dermatol. 2016;15(1 Suppl 2):s24‐s37. [PubMed] [Google Scholar]
- 4. Parrish AR. The impact of aging on epithelial barriers. Tissue Barriers. 2017;5(4):e1343172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. McDaniel D, Farris P, Valacchi G. Atmospheric skin aging – contributors and inhibitors. J Cosmet Dermatol. 2018;17:124‐137. [DOI] [PubMed] [Google Scholar]
- 6. Kim H, Kim JT, Barua S, et al. Seeking better topical delivery technologies of moisturizing agents for enhanced skin moisturization. Expert Opin Drug Deliv. 2018;15(1):17‐31. [DOI] [PubMed] [Google Scholar]
- 7. Feng L, Chandar P, Lu N, Vincent C, Bajor J, McGuiness H. Characteristic differences in barrier and hygroscopic properties between normal and cosmetic dry skin. II. Depth profile of natural moisturizing factor and cohesivity. Int J Cosmet Sci. 2014;36(3):231‐238. [DOI] [PubMed] [Google Scholar]
- 8. Lu N, Chandar P, Tempesta D, Vincent C, Bajor J, McGuiness H. Characteristic differences in barrier and hygroscopic properties between normal and cosmetic dry skin. I. Enhanced barrier analysis with sequential tape‐stripping. Int J Cosmet Sci. 2014;36(2):167‐174. [DOI] [PubMed] [Google Scholar]
- 9. Engebretsen KA, Kezic S, Riethmüller C, et al. Changes in filaggrin degradation products and corneocyte surface texture by season. Br J Dermatol. 2018;178(5):1143‐1150. [DOI] [PubMed] [Google Scholar]
- 10. Schwartz J, Friedman AJ. Exogenous factors in skin barrier repair. J Drugs Dermatol. 2016;15(11):1289‐1294. [PubMed] [Google Scholar]
- 11. Arezki NR, Williams AC, Cobb AJ, Brown MB. Design, synthesis and characterization of linear unnatural amino acids for skin moisturization. Int J Cosmetic Sci. 2017;39:72‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Fowler J. Understanding the role of natural moisturizing factor in skin hydration. Practical Dermatol. 2012. https://practicaldermatology.com/articles/2012-jul/understanding-the-role-of-natural-moisturizing-factor-in-skin-hydration?c4src=issue:feed [Google Scholar]
- 13. Bonté F. Skin moisturization mechanisms: new data. Ann Pharm Fr. 2011;69(3):135‐141. [DOI] [PubMed] [Google Scholar]
- 14. Draelos ZD. Modern moisturizer myths, misconceptions, and truths. Cutis. 2013;91(6):308‐314. [PubMed] [Google Scholar]
- 15. Elias PM, Sugarman J. Does moisturizing the skin equate with barrier repair therapy? Ann Allergy Asthma Immunol. 2018;121(6):653‐656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Sahle FF, Gebre‐Mariam T, Dobner B, Wohlrab J, Neubert RH. Skin diseases associated with the depletion of stratum corneum lipids and stratum corneum lipid substitution therapy. Skin Pharmacol Physiol. 2015;28(1):42‐55. [DOI] [PubMed] [Google Scholar]
- 17. Papakonstantinou E, Roth M, Karakiulakis G. Hyaluronic acid: a key molecule in skin aging. Dermato‐endocrinology. 2012;4(3):253‐258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Cosmeceuticals DZD. What's real, what's not. Dermatol Clin. 2019;37(1):107‐115. [DOI] [PubMed] [Google Scholar]
- 19. Spada F, Barnes TM, Greive KA. Skin hydration is significantly increased by a cream formulated to mimic the skin's own natural moisturizing systems. Clin Cosmet Investig Dermatol. 2018;11:491‐497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Brandner JM. Pores in the epidermis: aquaporins and tight junctions. Int J Cosmetic Sci. 2007;29:413‐422. [DOI] [PubMed] [Google Scholar]
- 21. Lodén M. Treatments improving skin barrier function. Curr Probl Dermatol. 2016;49:112‐122. [DOI] [PubMed] [Google Scholar]
- 22. Zorn‐Kruppa M, Vidal‐y‐Sy S, Houdek P, et al. Tight junction barriers in human hair follicles‐ role of claudin‐1. Sci Rep. 2018;8(1):12800. [DOI] [PMC free article] [PubMed] [Google Scholar]