

Abstract
Objectives:
There has been advocacy for legalization of abusable substances, but systematic data on societal beliefs regarding such legalization are limited. People who use substances may have unique beliefs about legalization, and this study assessed whether they would be in favor of drug legalization/decriminalization. It was hypothesized that those who use particular drugs (especially marijuana) would support its legalization/decriminalization, but that this would not be the case across all classes (especially opioids and stimulants).
Methods:
A nationwide sample of 506 adults were surveyed online to assess demographic characteristics, substance misuse, and beliefs regarding drug legalization/decriminalization. Legalization/decriminalization beliefs for specific drugs were assessed on an 11-point scale (0=strongly disagree; 10=strongly agree).
Results:
For persons with opioid misuse (15.4%), when asked about their agreement with: “heroin should be legalized,” the mean score was 4.6 (SEE= 0.4; neutral). For persons with stimulant misuse (12.1%), when asked about their agreement with: “cocaine should be legalized,” the score was 4.2(0.5). However, for persons with marijuana misuse (34.0%), when asked about their agreement with: “medical marijuana should be legalized” the score was 8.2 (0.3; indicating agreement), and for “recreational marijuana” the score was also 8.2(0.3).
Conclusions:
These results suggest that persons who used marijuana strongly support the legalization of both recreational and medical marijuana, whereas persons who primarily have opioid or stimulant misuse have less strongly held beliefs about legalization of substances within those respective categories. By including those who misuse drugs, these data assist in framing discussions of drug legalization and have the potential to inform drug policy considerations.
Keywords: drug legalization, drug decriminalization, medical marijuana, opioid misuse, stimulant misuse
1.0. Introduction
Substance use is a major concern in both the United States (US) and abroad, with important consequences related not only to morbidity and mortality, but legal and economic concerns as well. In 2010, the Global Burden of Diseases, Injuries, and Risk Factors Study found that mental illness was the leading cause of years living with disability worldwide, with illicit substance use disorders (SUDs) and alcohol use disorders (AUDs) accounting for 11% and 10% of disability-adjusted life years within that category, respectively (Whiteford et al., 2013). The 2016 National Survey on Drug Use and Health (NSDUH) estimates that 7.8% of adults in the US had a SUD during that year (Center for Behavioral Health Statistics and Quality, 2017).
While much drug use remains illegal, there are growing efforts to legalize and/or decriminalize certain drug classes (such as marijuana and heroin), despite international drug treaties prohibiting the non-medical use of marijuana, cocaine, amphetamines, and heroin (Hall, 2017). This is related, in part, to evidence that drugs such as marijuana or heroin, which had been previously categorized as having no medicinal value, may have potential medical benefit. These efforts are also premised upon the experiences of countries like Portugal, which decriminalized all illicit drugs in 2001 and reported subsequent decreases in drug-related societal problems, as well as support for legalizing drugs like marijuana for non-medical use in countries such as Canada and Uruguay (Room, 2014; Goncalves et al., 2015; Cox, 2018). Several European countries and Canada have now endorsed the use of medicinal injectable and oral heroin (diacetylmorphine or diamorphine) as an effective medication for heroin use disorder among persons who are not otherwise responding to treatments (Ayanga et al., 2016).
The US is beginning to demonstrate varied support for drug legalization and decriminalization. For instance, although not formally supported by the US federal government, eight states and the District of Columbia have legalized recreational marijuana, and twenty-nine states have legalized medicinal marijuana. However, systematic data on the opinions of Americans regarding the legalization/decriminalization of marijuana are lacking, and attitudes regarding the legalization/decriminalization of other substances are even sparser. Data show that the public’s opinions about marijuana seem to have changed over time (Carliner et al., 2017), with 12% of the public supporting legalization in 1969 (based on survey data), compared with 61% per an online poll conducted in 2017 (Geiger, 2018). Another recent online poll of registered US voters found that a modest majority (68%) was in support of legalization of marijuana for medical purposes, with 52% supporting its legalization for recreational purposes. However, this sample was vastly opposed to the legalization and decriminalization of other drugs (including cocaine, heroin, and methamphetamine), for both medical and recreational purposes (Lopez, 2016).
Opinions about drug legalization/decriminalization can differ based on whether a person has a personal history of substance use and as a function of demographic and ideological characteristics (such a religious or political preference); these associations have only been evaluated in a few studies. The first such study was conducted in 2002 among 188 out-of-treatment persons who used substances, and persons who did not use substances, from low income, high drug-use sections of a US urban setting (Houston, TX), and reported that persons who used substances (marijuana, heroin, cocaine, or methamphetamine) were more likely to support the legalization of marijuana (68% in favor) than persons who did not use substances (33%), while each group showed little support for the legalization of heroin (12% vs. 8%) or cocaine (14% vs. 8%, respectively; Trevino and Richard, 2002). More recently, an online poll reported that Americans identifying as Democrats were more likely to be in favor of marijuana legalization (69%) than Republicans (43%). Also, white mainline Protestants were more in favor of marijuana legalization (64%) than white evangelical Protestants (38%) or Catholics (52%), while those who were not affiliated with any religion showed the highest support (78%; Geiger, 2018).
These polls have various limitations, and have not focused upon the attitudes and beliefs of people who use drugs. This population may have unique beliefs about legalization and/or decriminalization of a drug - either their drug of choice, or illicit drugs more broadly. The direct experience of using a drug might predispose a person to support more ready availability of that drug or, conversely, might make a person more cautious about decreasing barriers to its use. Survey data have demonstrated that opinions on drug legalization/decriminalization can differ based on the person’s belief system, such as varying as a function of political or religious affiliation. Persons who are generally more conservative may not be in favor of legalizing or decriminalizing substances. Surprisingly, there is little information on attitudes regarding legalization/decriminalization of drugs that systematically evaluates these domains. This study aimed to address this gap by surveying both persons who used substances and persons who did not use substances about their opinions regarding legalization and decriminalization of drugs, and to also evaluate whether differences in these attitudes were associated with different religious and political affiliations, or the lack thereof, as a secondary outcome. It was hypothesized that individuals who use marijuana would support the legalization and decriminalization of that drug, but that this would not be the case for heroin or cocaine among persons who used opioids or stimulants, respectively.
2.0. Methods
2.1. Participants
The sample was recruited online between July and November 2017. Participants (N=506) were registered as “workers” on the Amazon Mechanical Turk (AMT) platform (Paolacci et al., 2010; Bartneck et al., 2015), which is an online forum where workers can anonymously complete tasks (such as surveys) assigned by “requestors” for a wage. Workers receive requestor approval ratings based on the quality of their work and completion time, which serves as an index of credibility and reliability (Peer et al., 2014). To take the present survey, workers had to have an average requestor approval rating of 90% (as a quality control measure) and be located in the US. A short screening survey was given to ensure that participants were at least 18 years old, and it included other demographic questions, such as sex and race, to distract from the subject of the survey. The screening survey also limited the number of persons per category of primary substance used (including no use) using quotas, with a goal of obtaining at least 60 people in each primary substance category. A total of 2,672 persons attempted the screening survey, and 545 persons completed the primary survey. Those who were not eligible to continue on to the primary survey received $0.10 for completing the screening survey. After providing consent by agreeing to participate in the survey, those who answered questions in the primary survey received a bonus of two dollars, for a total of $2.10. The following quality control questions were included: 1) “Have you taken this survey before?” and 2) “Is there any reason for which we should not use your responses? For instance, you weren’t paying attention, you did not answer honestly, you had major computer issues, etc.” Those who answered “yes” to either of these questions were not included. The survey was hosted on Qualtrics (Provo, UT). The Johns Hopkins University Institutional Review Board approved the use of AMT for this survey research.
2.2. Measures
Demographic and Drug Use Characteristics:
Primary survey questions included demographic information such as education level, employment status, and income, as well as characteristics related to religious and political affiliations and whether the participant or someone close to them had ever experienced legal consequences related to substance use (Table 1). Participants were asked whether they identified with a particular religion and to choose which major political party they identified with most among a list of the most common options; the options “none” and “other” were also provided. Additionally, participants were provided a list of substances and asked which they had used in the past year (including a write-in “other” option); for each substance they reported using, they were then asked to characterize use based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) SUD criteria (American Psychiatric Association, 2013). Answering “yes” to two or more symptoms was operationalized as meeting criteria for a SUD for that substance. Participants who indicated using more than one substance in the past year were asked to identify which substance they would consider their primary substance; this was the basis upon which they were categorized for the remainder of the survey analyses.
Table 1.
Participant demographic data (N=506)1
| Primary Substance Used | |||||||
|---|---|---|---|---|---|---|---|
| Opioids (N=78) | Stimulants (N=61) | Marijuana (N=172) | Alcohol (N=118) | None (N=77) | Total (N=506) | ||
| Age | Mean (SD), years | 33.6(10.5)a | 31.4 (8.2)a | 31.6 (8.2)a | 34.6 (10.5)ab | 38.2 (12.6)b | 33.6(10.1) |
| Sex | % Male | 41 | 47.5 | 55.8 | 55.1 | 59.7 | 53 |
| Marital Status | % Never Married | 46.2 | 41.0 | 43.6 | 45.8 | 51.9 | 45.5 |
| Race* | % Minority | 25.6ab | 27.9a | 32.6a | 22.9ab | 14.3b | 25.9 |
| Employment Status | % Employed Full Time | 64.1 | 70.5 | 61 | 62.7 | 54.5 | 62.1 |
| Highest Education Level Achieved* | % Associate’s degree or above | 48.7a | 65.6bc | 64.0b | 61.9ab | 49.4ac | 59.1 |
| Yearly Household Income Level* | % $45,000 or less | 61.5ad | 36.1b | 52.3acd | 40.7bc | 61.0d | 50.4 |
| Do you identify with a particular religion?* | % Yes | 30.8ab | 36.1a | 21.5b | 37.3a | 37.7a | 30.8 |
| Political Affiliation* | % Democratic Party | 50.0ab | 52.5ab | 60.5ac | 44.1b | 42.9b | 51.4 |
| Are you registered to vote? | % Yes | 84.6 | 90.2 | 90.1 | 92.4 | 83.1 | 88.7 |
| Have you or someone close to you experienced a legal consequence related to substance use?* | % Yes | 35.9a | 39.3a | 43.0a | 36.4a | 19.5b | 36.4 |
Asterisks indicate those variables for which the overall F or x2 statistic was significant at p<0.05. Differences among groups were compared using a Chi-square test, with pairwise comparisons, or a one-way ANOVA with Tukey’s post hoc tests for pairwise comparisons. Categories within a row that do not share a common superscript were significantly different (p< 0.05).
Decriminalization and Legalization Questions:
Participants were provided with definitions of legalization and decriminalization, and were then asked to rate their level of agreement with statements about legalization and decriminalization of heroin, cocaine, medical marijuana, and recreational marijuana on an 11-point scale with 0 representing “strongly disagree,” and 10 representing “strongly agree.” Some statements were worded in support of legalization/decriminalization of the substance while others were worded against legalization/decriminalization, to ensure participants were maintaining attention. Responses to the latter were reverse coded for consistency in reporting.
2.3. Statistical analyses
Participants were categorized into groups based on their self-reported primary substance used in the past year, with heroin and prescription painkiller misuse (taking pills other than how they were prescribed) collapsed into the “opioids” group; cocaine, methamphetamines, prescription stimulant misuse, or other stimulant use collapsed into the “stimulants” group; marijuana products, including synthetics, making up the “marijuana” group; any alcohol use included in the “alcohol” group; and no substance use in the “none” group. The degree to which demographic characteristics were associated with ratings for decriminalization/legalization was also assessed. Some demographic characteristics with multiple subgroups were dichotomized given limited numbers in some subgroups, including marital status (never married vs. ever married), race (minority vs. Caucasian), employment status (employed full time vs. other), education level (associates degree vs. less education), household income (less than or equal to $45,000 vs. more than $45,000) and political affiliation (Democrat vs. other).
Opinions on drug legalization and decriminalization as a function of primary substance used served as the primary analyses, while all others were secondary analyses. Categorical data, including demographics and SUD categorization were analyzed with chi-square analyses. Continuous data, such as age and drug legalization/decriminalization ratings, were analyzed with ANOVA or ANCOVA as appropriate. ANCOVAs controlled for those demographic variables that were significantly different among groups and showed a significant relationship with the outcome measure (see Table 2). Between-group planned comparisons of drug legalization/decriminalization ratings were compared between the primary substance categories, and then as a function of the group for whom the rating was deemed most relevant (e.g., ratings for heroin among persons who primarily used opioids, for cocaine among persons who primarily used stimulants, and for medical/recreational marijuana among persons who primarily used marijuana). Analyses used Type III sums of squares and planned comparisons among the primary substance use groups, and Pearson’s correlations to evaluate the relationship between legalization/decriminalization ratings. The primary outcome variables (legalization and decriminalization ratings) were not normally distributed. For the analyses in which we needed to control for certain demographic variables, ANCOVA were used as the main analyses, based on support for analyzing Likert data with parametric statistics (Lubke and Muthén, 2004; De Winter and Dodou, 2010). The analyses by primary substance were significant when analyzed with Kruskal-Wallis tests, indicating that parametric and nonparametric statistics are approximately equivalent for these data. There were minor exceptions among the secondary analyses, but not the primary analyses. All analyses were performed in SPSS version 24.0. Statistical tests were considered significant at the p < 0.05 level.
Table 2.
Level of agreement with statements as a function of primary substance used1
| Heroin should be legalized | Heroin should be decriminalized | Cocaine should be legalized | Cocaine should be decriminalized* | Medical marijuana should be legalized* | Medical marijuana should be decriminalized* | Recreational marijuana should be legalized* | Recreational marijuana should be decriminalized* | |
|---|---|---|---|---|---|---|---|---|
| Primary Substance Used | Mean(SEE) | Mean(SEE) | Mean(SEE) | Mean(SEE) | Mean(SEE) | Mean(SEE) | Mean(SEE) | Mean(SEE) |
| Opioids | 4.6(0.4) | 3.1(0.4) | 4.0(0.4) | 3.2(0.4)a,b | 7.3(0.4)a,b | 8.0(0.3)a,b | 6.7(0.4)a,b | 7.2(0.4)a,c |
| Stimulants | 3.3(0.5) | 2.7(0.4) | 4.2(0.5) | 3.5(0.4)a,b | 7.5(0.5)a,b | 8.4(0.3)b | 7.8(0.4)b,c | 7.4(0.4)a,b |
| Marijuana | 4.1(0.3) | 3.6(0.3) | 4.4(0.3) | 4.4(0.3)b | 8.2(0.3)b | 9.2(0.2)b | 8.2(0.3)c | 8.4(0.2)b |
| Alcohol | 3.4(0.4) | 2.6(0.3) | 3.2(0.3) | 2.8(0.3)a | 7.2(0.3)a,b | 8.9(0.2)b | 7.4(0.3)b,c | 7.9(0.3)a,b |
| None | 3.4(0.4) | 2.4(0.4) | 3.4(0.4) | 2.8(0.4)a | 6.0(0.4)a | 7.1(0.3)a | 5.9(0.4)a | 5.9(0.4)c |
Scales ranged from 0–10, with 0 being strongly disagree and 10 being strongly agree. Asterisks indicate those variables for which the overall F statistic was significant at p<0.05. Differences among the adjusted means for all groups were compared using an ANCOVA and Fisher’s LSD procedure was used to conduct pairwise comparisons for variables with a significant group effect. Each analysis controlled for having a religious affiliation, while age served as a covariate for cocaine legalization and recreational marijuana decriminalization analyses, heroin and cocaine legalization analyses controlled for income, and analyses involving legalization of medical and recreational marijuana, and decriminalization of recreational marijuana controlled for political affiliation. Categories within a column that do not share a common superscript were significantly different (p< 0.05). SEE= Standard error of the estimate
3.0. Results
3.1. Participant characteristics
A total of 506 participants completed the survey (Table 1). Over the time of enrollment, the screening process targeted participants to ensure there were at least 60 subjects for each primary substance category. The final population had a mean age of 33.6 years old and was 53.0% male, 45.5% single (never married), and 25.9% racial minority (i.e., not Caucasian). Sixty-two percent of participants were employed full-time, 59.1% had at least an Associate’s degree, and 50.4% had a yearly household income of $45,000 or less. Among the total population, 36.4% of persons had experienced a legal consequence related to substance use among themselves or someone close to them. This was significantly more common among persons who used opioids (35.9%), stimulants (39.3%), marijuana (43.0%), or alcohol (36.4%), compared to those without substance use (19.5%). Participants were located in 43 states and the District of Columbia. For those persons who self-reported a primary substance used in the past year (N=429; 84.8%), a substantial proportion within each substance category reported symptoms meeting criteria for a SUD, including OUD (33/78; 42.3% of persons with opioid misuse), stimulant use disorder (25/61; 41.0%), marijuana use disorder (35/172; 20.3%), and AUD (39/118; 33.1%).
3.2. Preference for drug legalization and decriminalization of specific drug categories (Table 2)
3.2.1. Heroin
Overall, participants were not in favor of legalizing heroin (mean 3.8/10 for the total sample). However, persons whose primary substance was an opioid tended to have higher ratings (reflecting more positive attitudes) towards legalizing heroin (4.6/10) than persons who were classified as having primarily stimulant (3.3/10) or alcohol (3.4/10) use, as well as persons with no past-year substance use (3.4/10). The ratings of those with primary opioid misuse were similar to the ratings of persons with primary marijuana misuse with respect to attitudes towards heroin legalization (4.2/10). Ratings among all groups for decriminalization of heroin were even lower (total mean 2.9/10) indicating general lack of support. Persons who primarily misused opioids rated heroin decriminalization at 3.1 on average, which was not significantly different from other groups.
3.2.2. Cocaine
Similarly, the total sample of 506 persons was not in favor of cocaine legalization (3.8/10) or decriminalization (3.3/10). Persons with stimulant misuse rated cocaine legalization (4.2/10) and decriminalization (3.5/10) in a comparably low manner. Those who primarily used marijuana rated their agreement with cocaine decriminalization significantly higher (4.4/10), compared to those with primary alcohol use (2.8/10) and those with no use (2.8/10).
3.2.3. Marijuana
The total group of 506 participants was generally more in favor of the legalization and decriminalization of both medical (means for legalization = 7.2/10 and for decriminalization = 8.3/10) and recreational marijuana (legalization = 7.2/10 and decriminalization = 7.4/10), compared to legalization or decriminalization of heroin and cocaine. When examining the specific substance use groups, persons without any past-year substance use had lower ratings regarding legalization and decriminalization of marijuana, compared to other primary substance use groups. Conversely, persons with primary marijuana use had higher ratings for marijuana legalization (medical and recreational both = 8.2/10) and decriminalization (medical = 9.2/10 and recreational = 8.4/10).
3.3. Ratings as a function of primary substance used
This study hypothesized that respondents who identified a particular substance as their primary substance of use over the past year might be more inclined to see that substance legalized and/or decriminalized (particularly for marijuana). Results demonstrated that participants categorized as having primary opioid or stimulant misuse rated legalization and decriminalization of heroin and cocaine, respectively, at significantly lower values (indicating less endorsement) when compared to how those with primary marijuana use rated legalization and decriminalization of both medical and recreational marijuana (see corresponding cells of Table 2).
3.4. Religious characteristics
Whether persons identified with a particular religion or not proved to be an important variable among demographic characteristics, as well as legalization/decriminalization ratings (with religion serving as a covariate for those analyses). Thirty percent of participants identified with a religion. A significantly lower proportion of persons who used marijuana (21.5%) identified with a religion, compared to those who primarily used alcohol (37.3%), stimulants (36.1%), or no substances (37.7%). Similarly, those who identified with a religion were significantly less likely to report primary marijuana use (23.7%) than those who did not (38.6%). However, those persons who identified with a religion and used substances were significantly more likely to endorse 2 or more criteria on the DSM-5 SUD checklist (37.8%) than those who used substances but did not identify with a particular religion (27.8%).
There were statistically significant, though weak, negative correlations between identifying with a religion, and all drug legalization/decriminalization ratings (see Supplemental Table 1). Participants with a self-reported religious affiliation had significantly lower mean legalization/decriminalization ratings compared to those without any religious affiliation (Figure 1a).
Figure 1.
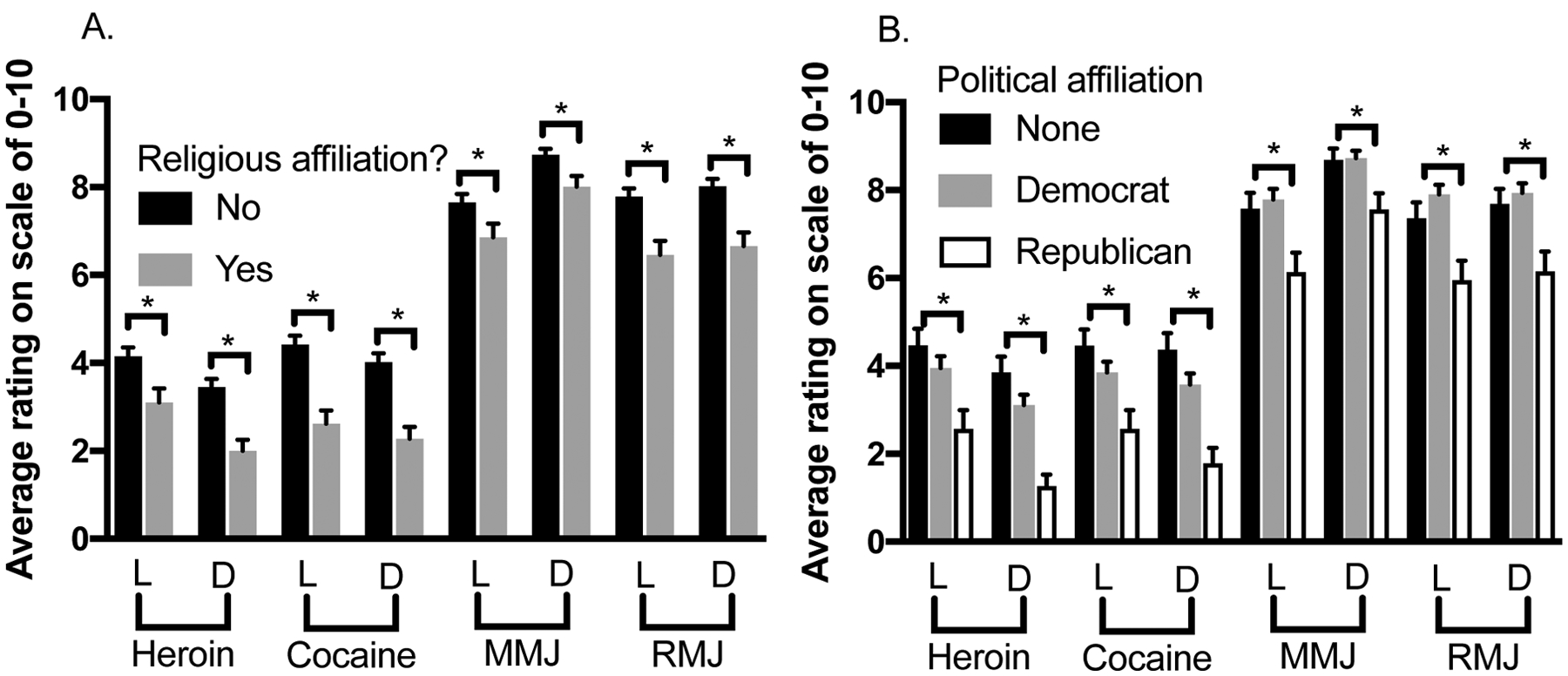
Mean drug legalization/decriminalization ratings as a function of (a) religious or (b) political affiliation1
1Scales rated from 0–10, with 0 being strongly disagree and 10 being strongly agree. Unadjusted mean differences between groups were assessed with one-way ANOVA, with Tukey’s post hoc comparisons among political groups. Asterisks indicate p < 0.05 (b). Error bars indicate standard error of the mean (SEM). Asterisks indicate p < 0.05 when comparing persons who identify as republicans to those who identify as Democrats or have no political affiliation. Abbreviations: L- legalization, D- decriminalization, MMJ- medical marijuana, RMJ- recreational marijuana
3.5. Political characteristics
Political party affiliation (or the lack thereof) was also a significant factor among the demographic makeup of this population, their substance use, and opinions on drug legalization/decriminalization (making it a covariate for these analyses). The majority of persons surveyed (88.7%) were registered to vote. Fifty-one percent of participants identified with the Democratic Party, and the proportion of persons who used marijuana and identified as Democrats (60.5%) was significantly higher than those who primarily used alcohol (44.1%) or no substances (42.9%). Those who identified as Democrats were significantly more likely to use marijuana (40%) compared to non-Democrats (27.6%). Among those persons whose primary substance was alcohol, Democrats were significantly less likely to have an alcohol use disorder (12.7%) compared to non-Democrats (19.1%). Persons who identified as Republicans had significantly lower legalization/decriminalization ratings for each substance compared to those who identified as Democrats and those without any political affiliation (see Figure 1b).
3.6. Ratings as a function of having a DSM-5 SUD vs. no SUD within primary drug categories
It is also possible that people with a more severe pattern of use (i.e., a SUD) would be more supportive of legalizing and/or decriminalizing the substance they use. However, there were no differences in ratings for legalization and decriminalization for any substance when comparing persons who use a substance but did not fulfill the DSM-5 SUD criteria, with those within that substance category who did meet the DSM-5 SUD criteria (data not shown).
3.7. Correlation of medical marijuana ratings to ratings of other substances
The use of medical marijuana is becoming more acceptable across the US, and it is possible that people who support the legalization/decriminalization of medical marijuana may also be open to supporting the legalization/decriminalization of other substances. We found a significant, though at times weak, positive correlation between how much participants agreed that medical marijuana should be decriminalized with ratings on heroin decriminalization (r=0.13, p=0.003), cocaine decriminalization (r= 0.15, p=0.001), recreational marijuana legalization (r=0.37, p=0.000) and recreational marijuana decriminalization (r=0.39, p=0.000). There was a significant, positive correlation between how participants rated medical marijuana legalization, and decriminalization of cocaine (r=0.09, p=0.038), legalization of recreational marijuana (r=0.43, p=0.000) and decriminalization of recreational marijuana (r=0.28, p=0.000).
4.0. Discussion
The current study provides new insights into opinions regarding the legalization and decriminalization of heroin, cocaine and marijuana. This study is unique in examining attitudes as a function of past year drug use, and hypothesized that persons who used substances would have differing drug legalization/decriminalization ratings for their self-reported primary substance, especially when comparing persons who primarily used marijuana to those who primarily used opioids and stimulants. Our hypothesis was supported by these findings, as persons who primarily used marijuana rated both the legalization and decriminalization of this drug favorably, but persons who primarily used opioids and simulants rated their support for both the legalization and decriminalization of heroin and cocaine relatively low, respectively. We found that overall most respondents were in favor of the legalization and decriminalization of marijuana (both medical and recreational), but not heroin and cocaine. These findings are consistent with the limited data that is currently known about opinions on marijuana legalization and decriminalization (Lopez, 2016; Carliner et al., 2017; Geiger, 2018) as well as, heroin and cocaine (Trevino and Richard, 2002; Geiger, 2018), though this is the first hypothesis-driven study of its kind since recent changes in marijuana laws have been made. Of note, while the concepts of legalization and decriminalization are fundamentally different, and were asked about separately in our survey, we found that they tended to track together (i.e. for each drug the mean ratings were either low, or below five, as in the case of heroin and cocaine, or above 5, as in the case of both recreational and medical marijuana). Thus, we will discuss the attitudes about both together.
These findings are particularly important because persons who misuse legal or illicit substances often have had interactions with the legal system, which may influence their attitudes and beliefs. Over a third of our participants had experienced legal consequences related to substance use themselves or through someone close to them. Data from the 2002–2008 NSDUH survey provides corroborating evidence of this relationship between drug use and legal consequences by showing that among those who had past year illicit drug dependence or abuse, 18% and 36% had been arrested once or more than once that year, respectively. Within the subsample of NSDUH respondents reporting past year alcohol dependence or abuse, these values increased to 38% and 52%, respectively (Lattimore et al., 2014). The estimated prevalence of SUDs among incarcerated persons, while largely varied across studies, is substantial within both female (30–60%) and male (10–48%) prisoners (Gerstein and Harwood, 1990; Mason et al., 1997; Lo and Stephens, 2000; Fazel et al., 2006). The high prevalence and comorbidity with SUDs indicates that legal issues are a significant factor in the current climate of substance use in the US.
The majority of our participants were not in favor of legalizing nor decriminalizing heroin and cocaine, even if they or someone they knew had suffered legal consequences related to substance use, or if they themselves met criteria for a SUD. These findings suggest that this population would not support policy changes related to heroin and cocaine legalization/decriminalization, which may reflect their own experiences, making them more cautious about increasing availability of these drugs. This sample was generally supportive of legalization and decriminalization of both medical and recreational marijuana. However, persons without any substance use in the last 12 months had significantly lower ratings than other groups, and were mainly neutral about marijuana legalization/decriminalization. The exception was that persons with no primary substance use had a higher rating on decriminalization of medical marijuana (mean 7.1/10) compared with their other ratings, perhaps because this was the most conservative marijuana option given. Interestingly, there was a positive relationship between agreement with decriminalizing medical marijuana, and decriminalizing heroin, cocaine, and recreational marijuana among our total population, suggesting an openness to minimizing criminal consequences associated with medical marijuana tracked with openness to the same for other drugs.
Understanding attitudes and associated characteristics towards drug legalization and decriminalization is important, especially in the currently changing social landscape, as several states in the US have passed laws legalizing and/or decriminalizing marijuana. For example, a study involving persons who voted on the initiative to legalize marijuana in Washington state reported that once marijuana stores began to open, persons who previously voted against the initiative were more likely to change their vote, if given the chance, compared to those who had voted in support of it (Subbaraman and Kerr, 2016). Given the current changing environment, it is timely to determine whether persons continue to support legalization/decriminalization of marijuana and, more broadly, whether they would support legalization/decriminalization of other illicit drugs. Additionally, with other countries conducting research on heroin as a treatment for OUD (Ayanga et al., 2016), it is important to consider how this may be perceived in the US and whether attitudes vary as a function of demographic and/or ideological beliefs.
There are several limitations to this work. The use of an online survey through AMT involves some selection bias, and resulted in a population which, while diverse, is not completely representative of the US population as a whole though it is demographically consistent with other studies involving AMT workers (Chandler and Shapiro, 2016). Additional studies conducted within a representative sample of the US population would be helpful to determine the impact of demographic characteristics, as well as legal status of marijuana in the state of residence, on perceptions of drug decriminalization/legalization. The fact that self-reported substance use was not verified, and was from an anonymous population, is another limitation, in addition to the fact that all persons who used opioids or stimulants were grouped together, due to small numbers, instead of being able to assess those who used heroin and cocaine, specifically. We were also unable to look at how the use of multiple substances (especially those with primary use of alcohol, a legal substance, in addition to illegal substances) affected attitudes toward drug legalization/decriminalization.
This study appears to be the first to systematically study opinions of persons from across the US who use substances, and those who do not, about the legalization and decriminalization of multiple substances, and results have relevance for current and future policies. Legalization/decriminalization of marijuana was supported, but not in the case of other drugs, despite changes in apparent attitudes in other countries. As more information is learned about potential health benefits of certain substances that may drive policy changes in favor of their legalization/decriminalization, it is critical that persons who are directly affected by any policy changes (i.e. those who use substances) be included in these discussions to provide their unique perspectives. Studies among persons in SUD treatment, or those with varying SUD severity, are also warranted, as they may prove even more insightful to inform policies on legalization/decriminalization and the use of currently illicit drugs as treatment for SUDs. It is also important to monitor and track the evolution in changes in attitudes and beliefs over time. These nuances may impact public health messaging and the ability to target certain groups.
Supplementary Material
Conflict of interest and Source of Funding:
This work was supported by internal funding from the Johns Hopkins University School of Medicine. No conflicts declared.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Arlington, VA: American Psychiatric Pub; 2013. [Google Scholar]
- Ayanga D, Shorter D, Kosten TR. Update on pharmacotherapy for treatment of opioid use disorder. Expert Opin Pharmacother 2016;17: 2307–2318. [DOI] [PubMed] [Google Scholar]
- Bartneck C, Duense A, Moltchanova E, Zawieska K. Comparing the similarity of responses received from studies in Amazon’s Mechanical Turk to studies conducted online and with direct recruitment. PloS one 2015;10: e0121595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carliner H, Brown QL, Sarvet AL, Hasin DS. Cannabis use, attitudes, and legal status in the US: A review. Prev Med 2017;104:13–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Center for Behavioral Health Statistics and Quality. Results from the 2016 National Survey on Drug Use and Health: Detailed tables; 2017. Retrieved from https://www.samhsa.gov/data/. Accessed May 22, 2018.
- Chandler J, Shapiro D. Conducting clinical research using crowdsourced convenience samples. Annual Review of Clinical Psychology 2016;12:53–81. [DOI] [PubMed] [Google Scholar]
- Cox C The Canadian Cannabis Act legalizes and regulates recreational cannabis use in 2018. Health Policy 2018;122:205–209. [DOI] [PubMed] [Google Scholar]
- De Winter JC, Dodou D. Five-point Likert items: t test versus Mann-Whitney-Wilcoxon. Practical Assessment, Research & Evaluation 2010;15:1–12. [Google Scholar]
- Fazel S, Bains P, Doll H. Substance abuse and dependence in prisoners: a systematic review. Addiction 2006;101:181–191. [DOI] [PubMed] [Google Scholar]
- Geiger A About six-in-ten Americans support marijuana legalization. 2018. Retrieved from http://www.pewresearch.org/fact-tank/2018/01/05/americans-support-marijuana-legalization/. Accessed May 22, 2018.
- Gerstein DR, Harwood HJ. Treating drug problems: A study of the evolution, effectiveness, and financing of public and private drug treatment systems (Vol. 1). Washington, DC: Institute of Medicine, 1990. [PubMed] [Google Scholar]
- Goncalves R, Lourenco A, Silva SN. A social cost perspective in the wake of the Portuguese strategy for the fight against drugs. Int J Drug Policy 2015;26:199–209. [DOI] [PubMed] [Google Scholar]
- Hall W The future of the international drug control system and national drug prohibitions. Addiction 2017;113(7):1210–1223. [DOI] [PubMed] [Google Scholar]
- Lattimore PK, Steffey DM, Gfroerer J, et al. Arrestee substance use: comparison of estimates from the national survey on drug use and health and the arrestee drug abuse monitoring program. Rockville (MD): Substance Abuse and Mental Health Services Administration; 2014. [PubMed] [Google Scholar]
- Lo CC, Stephens RC. Drugs and prisoners: Treatment needs on entering prison. The American journal of drug and alcohol abuse 2000;26: 229–245. [DOI] [PubMed] [Google Scholar]
- Lopez G Poll: The only drug Americans want to legalize is marijuana. 2016. Retrieved from https://www.vox.com/2016/3/15/11224500/marijuana-legalization-war-on-drugs-pol. Accessed May 22, 2018.
- Lubke GH, Muthén BO. Applying multigroup confirmatory factor models for continuous outcomes to Likert scale data complicates meaningful group comparisons. Structural equation modeling 2004;11:514–534. [Google Scholar]
- Mason D, Birmingham L, Grubin D. Substance use in remand prisoners: a consecutive case study. BMJ 1997;315:18–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paolacci G, Chandler J, Ipeirotis PG. Running experiments on Amazon Mechanical Turk. Judgment and Decision Making 2010;5(5):411–419. [Google Scholar]
- Peer E, Vosgerau J, Acquisti A. Reputation as a sufficient condition for data quality on Amazon Mechanical Turk. Behavior research methods 2014; 46:1023–1031. [DOI] [PubMed] [Google Scholar]
- Room R Legalizing a market for cannabis for pleasure: Colorado, Washington, Uruguay and beyond. Addiction 2014;109;345–351. [DOI] [PubMed] [Google Scholar]
- Subbaraman MS, Kerr WC. Marijuana policy opinions in Washington state since legalization: would voters vote the same way? Contemporary drug problems 2016;43:369–380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trevino RA, Richard AJ. Attitudes towards drug legalization among drug users. Am J Drug Alcohol Abuse 2002;28:91–108. [DOI] [PubMed] [Google Scholar]
- Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. The Lancet 2013;382:1575–1586. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.