

Abstract
Pain is a significant burden among different communities, but little is known regarding the epidemiology of pain, particularly with respect to socioeconomic status (SES).
The aim of the study was to estimate the prevalence of body pain and to identify risk factors of pain in middle-aged and older Chinese.
The data were extracted from the 2008 Chinese Suboptimal Health Study that consisted of 18,316 Chinese subjects aged 18 to 65 years. Information on SES including occupation and education levels and body pain were collected. A Likert scale was used to evaluate reported body pain. We used the multiple logistic regression model to examine the association between SES and body pain.
Overall, 65.34% reported body pain (male: 60.93%; female: 69.73%). After adjustments based on sex, age, education, area of residence, marital status, smoking, drinking and health status, the results showed that students (odds ratio [OR] = 1.51; 95% confidence interval [CI]: 1.32–1.74) and professionals (OR = 1.22; 95% CI: 1.08–1.37) had significant high risk for body pain, compared with civil servants and farmers (OR = 0.64; 95% CI: 0.55–0.75) who significantly lower risk of body pain. The study demonstrates there is a significant negative association between education and reported body pain.
The results indicated an association between SES and body pain within the Chinese community. Body pain varied among different Chinese occupation-related population and people with higher education level are less like to have body pain.
Keywords: socioeconomic status, pain, China
1. Introduction
Body pain has resulted in a significant public health burden,[1] and affects nearly 1/3 adults worldwide.[2] In China, the prevalence of pain among the general population from Chongqing city community is 42.2%.[3] Among Chinese teachers, the prevalence of neck/shoulder pain and low back pain was 48.7% and 45.6%, respectively,[4] while the prevalence of back pain was 38.4% among farmers from north China.[5]
Several studies report the associations between socioeconomic status (SES) and diseases could be varied and even reversed in developed and developing countries.[6,7] The studies of body pain from nonwestern countries is limited, and Jackson et al conducted a systematic review on the prevalence of chronic pain, and identified 122 publications in 28 low-income and middle-income countries.[8] This review did reveal an association between socioeconomic inequalities and body pain.[9] Yet, most studies that address the relationship between SES and body pain are from western countries. Low SES has been shown to be associated with high prevalence of body pain, especially low back pain,[10] and SES plays an important role in occupational class disparities for persistent or recurrent body pain.[11] People in the highest socioeconomic categories tend to have less body pain than those in lower socioeconomic categories.[1] The characteristics and effects of pain can be explained by socioeconomic factors such as years of education and occupational history.[12] Race and ethnicity could modify the relationship between SES and body pain according to previous studies verified among the different race/ethnic groups,[1,12,13] but Janevic et al found that prevalence differences of body pain associated with education, race/ethnicity, and age as not significant.[14]
In general, occupation, education, and income are the 3 most important indicators within the literature that are examined in relation to SES. Definitions of income may include wages, salaries, profits, or rent. In China, it is relatively easy to obtain records of people's wages/salaries; however, wages/salaries are only a part of many Chinese incomes. Income is also a highly sensitive topic in China and people are reluctant to disclose their income levels in surveys. As a result, occupation and education are used in this study to approximate SES.[15]
There are many published studies on this subject, and many other studies findings have found similar results. For example, studies from the United States, Singapore, and Germany found that that low SES in adults was associated with chronic pain.[1–3] Also, a recent review indicated that disparities based on SES affect pain development and management.[4] To the best of our knowledge, there is no study that addresses the SES–pain relationship among people in China. Because more than 40 years ago, there was almost no SES difference in China because everyone had a similar income and all the occupations were considered “equal.” Individuals were identified by “classes” based on background of family origin, which is another set of classification. Only after “open and reform,” did the SES classification begin to form in China. Few studies address the effect of SES on health in China. It is unclear whether socioeconomic factors have a specific influence among Chinese population and as a result, our studies aim to investigate this potential relationship. We conducted a national sample study to determine whether there is an association between SES and body pain among Chinese communities. To clarify the association of SES with body pain, while taking into account other risk factors, we examined the associations in a large, national study in a nonwestern setting. We tested the following hypothesis: body pain varies among different SES categories within the Chinese population.
2. Methods
The sampling method of the survey is reported in elsewhere,[16] but briefly, the China Sub-optimal Health Survey (CSHS) was created in 2008 to understand the changing health status of China based on a nationally representative sample of the population. The CSHS selected individuals from 6 provinces to represent the 1.4 billion individuals in the nation's population. A multistage, random cluster sampling design was used to select study subjects. All 31 provinces or municipalities were divided into 6 administrative regions (Northeast, North, East, Central South, Southwest, and Northwest). The regions of Jilin, Beijing, Jiangsu, Hubei, Sichuan, and Gansu were randomly selected to represent those 6 administrative regions. Each of the above randomly selected regions was then divided into multiple urban and suburban regions. From this, 1 to 2 urban regions and 1 to 2 suburban regions were randomly selected to represent both the urban and suburban population. Within those selected regions, residents including local college students, government staff, business and farm workers, and other nonaffiliated residents were clustered and randomly selected as the sample groups.
The participants were required to fill the questionnaire by themselves, after the explanation of questionnaires. All the questionnaires were returned to the interviewer in person. Finally, 19,665 participants were selected to participate in the study, of which 18,631 responded and filled out questionnaires (for a response rate of 94.7%).
The Chinese adults aged between 18 and 65 years were included in this study. We excluded individuals who had reported mental illnesses that could potentially affect feeling of pain; and patients with cancer, rheumatology pain, and other related diseases. After exclusion criteria were applied, 18,284 participants were included in the final analysis.
2.1. Ethics statement
This study was approved by the Institutional Review Board at Peking Union Medical College and followed the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants.
2.2. Data collection
All individuals in each randomly selected cluster unit were asked to complete a self-administered questionnaire. The data on demographic and personal characteristics were collected, including gender, age, marital status, education, smoking, drinking, and health information (medical history, illness, and diseases that occurred during the last 12 months). Information on occupation was based on categories set forth by the Chinese labor law.
2.3. Body pain
Body pain was assessed by the following questions inserted into a self-reported questionnaire:
“In the last month, have you had a body pain?” (Body pain)
In the question respondents were asked to use a Likert scale for their responses (1 = no, 2 = mild, 3 = moderate, 4 = severe, and 5 = extreme). This classification was utilized as it was consistent with a previous study examining lower back pain.[17]
2.4. Statistic method
Statistical analyses were carried out with Windows Statistical Software Package Version 9.0 (SAS Institute, Cary, NC). Occupations were analyzed as a categorical variable and education level was categorized into 3 groups: literate or primary school, high school, and college or above. Body pain was categorized into 2 groups: no body pain (respondent selecting “1”) and having body pain (respondents selecting “2”and above), which were investigated as binary outcome variables. This cut-off point has been validated by previous studies.[18,19]
Chi-squared tests were used to compare participants’ characteristics with and without body pain. Logistic regression models were applied to estimate the odds ratio (OR) and 95% confidence interval [CI] of pain by occupation and education, adjusted for potential confounders. Logistic regression models were applied to estimate the OR and 95% CIs of pain by occupation and education, adjusted for potential confounders. Potential confounders considered were sex, age, occupation/education, area of residence, marital status, smoking, drinking, and health status (as categorized in Table 1). A significance level of 0.05 is required to allow the variable to enter the model. Health status was assessed based on self-reports of chronic illness including hypertension, diabetes, coronary heart disease, hyperlipidemia, and hepatitis.
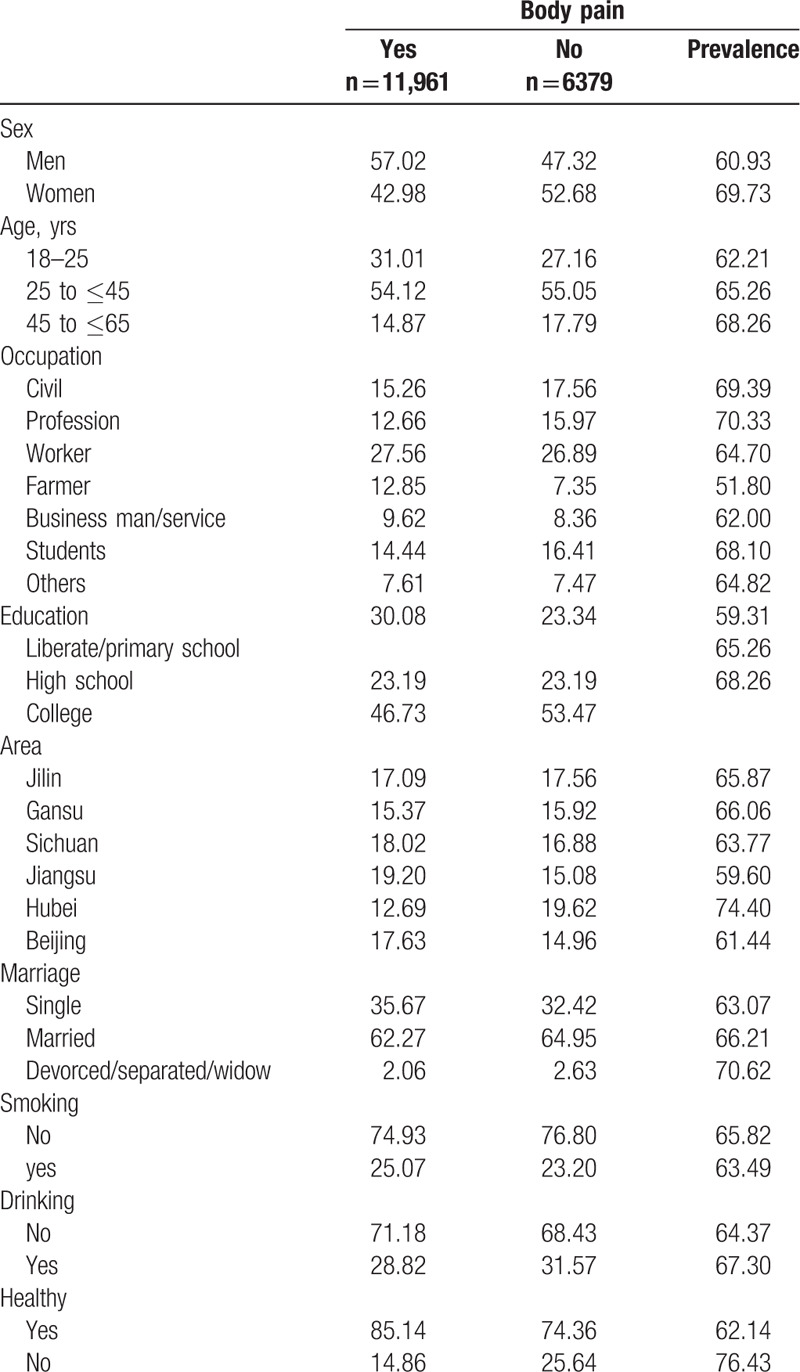
Table 1.
Participant characteristics (column %) and frequencies (row %) among the people with and without body pain.
Participants reporting having any of the above chronic diseases were labeled as “unhealthy.” Two sets of potential confounders were used in the adjusted models. Model 1 adjusted for sex and age, while model 2 additionally adjusted for education, area of residence, marital status, smoking, drinking, and health status. All potential confounders are summarized in Table 1, and all the tests were 2-sided and significance level was set at 0.05.
3. Results
The study included a total of 18,340 Chinese adults from 6 provinces with a mean age of 33.1 years (standard deviation = 10.6). Among the participants, 50.69% were males and 49.31% were females. Overall in the total sample 65.34% of respondents reported body pain (male: 60.93%; female: 69.73%).
The prevalence of body pain was varied based on occupation and education level. For the various occupations, 69.39% of civil servants, 70.33% professional workers, 64.70% of blue-collar workers, 51.80% of farmers, and 62.00% of business workers, 68.1% of students, and 64.82% of other individuals reported pain. Regarding educational attainment, 59.31% of primary education or less, 65.26% of high school, and 68.26% of college reported having pain.
3.1. Association between occupation and pain
Table 2 illustrates the results of both the simple and multiple logistic regression models used to analyze the effects of different occupations on the association of body pain. The OR adjusted for age and sex of body pain is 0.88 (95% CI: 0.80–0.97) for blue collar workers, 0.51 (95% CI: 0.45–0.57) for farmers, 0.83 (95% CI: 0.73–0.94) for businessmen, and 1.35 (95% CI: 1.18–1.54) for students, compared with civil servants. Additional adjustments based on education, area of residence, marital status, smoking, drinking, and health status in model 2 did not attenuate the effect of occupation for farmer (OR = 0.64; 95% CI: 0.55–0.75), and students (OR = 1.51; 95% CI: 1.32–1.74), but there was an attenuation of the effect of occupation for worker (OR = 1.00; 95% CI: 0.90–1.08), and businessmen (OR = 1.02; 95% CI: 0.89–1.17). In model 2, the adjusted OR for body pain is 1.22 (95% CI: 1.08–1.37) for professional compared with civil servants.
Table 2.
Multiple logistic regression models and the associations between occupation and pain.

3.2. Association between education and pain
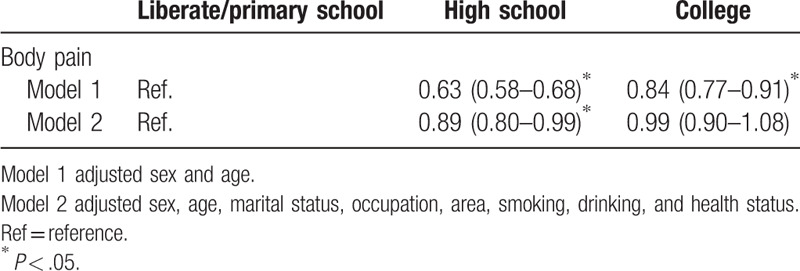
Table 3 highlights the results of the simple and multiple logistic regression models used to understand the effects of different education levels on the association of pain. The OR for body pain was 0.63 (95% CI: 0.58–0.68) for high school, and 0.84 (95% CI: 0.77–0.91) for college, compared to that of liberate or primary school. Additional adjustments based on education, area of residence, marital status, smoking, drinking, and health status in model 2 did not attenuate the association among high school (OR = 0.89; 95% CI: 0.80–0.99), but there was attenuation of this association found among college (OR = 0.99; 95% CI: 0.90–1.08).
Table 3.
Multiple logistic regression models and the associations between education and pain.
4. Discussion
The results demonstrate that professional workers had a higher prevalence of body pain, compared to farmers and individuals in other occupations.
Results from the multiple logistic regression analysis, showed that professional workers and students had a significantly higher risk for body pain, while farmers had a significantly lower risk compared with individuals in other occupations. Educational level was significant, and negatively associated with body pain.
Our results are in line with previous studies that found low SES associated with a high rate of body pain.[20] In general, highly educated individuals in this study had significantly more favorable health outcomes compared to those with less education.[21] However, Riskowski using the National Health and Nutrition Examination Survey, reported that the people with high SES are more likely to have body pain.[1] Of note, farmers in our study had significantly lower risk of body pain compared to other occupations.
One possible explanation of the variation of body pain is the occupation of participants (1 important component of the SES). Chu et al reported that 68% of pain patients had a history of injury occurrence at work[22] and other studies reported that occupation is associated with low back pain.[23,24] Jin et al conducted a cross-section study in China and found that garment workers had a higher annual prevalence of low back pain (74%) compared to teachers (40%), and had a prevalence ratio of 1.9 (95% CI = 1.4–2.4). These results could be explained by the nature of work within this occupational category, especially among persons doing work in fixed and sedentary postures that would likely impact the back area compared to other body parts/regions.
Another potential mechanism is that SES is associated with pain tolerance and tolerance interval. Miljković et al investigated the association of experimentally induced pain threshold and tolerance within different SES categories. A significant association between experimentally induced pain tolerance and tolerance interval with material status was shown, suggesting that poor people indeed do hurt more with respect to pain compared to those in the higher wealth categories.[25] In their study, education was strongly correlated with pain in the correlation analysis, but the use of multivariate analytic methods yielded nonsignificant results and suggested that only material status was associated with pain tolerance and tolerance interval.
Body pain is self-reported, and there are individual differences in sensitivities and tolerance levels for body pain. Until now, we do not have an objective measurement of body pain to validate the self-reported nature body pain. In general, this study found that farmers have a higher threshold of pain compared to nonfarmers. Also, compared with white collar workers, farmers had a lower prevalence of neck, or shoulder pain due to work environments, but they could at times have a higher prevalence of low back pain.
Further, lower levels of educational attainment and income levels are associated with a chronic pain diagnosis.[26] Jöud et al conducted a study on 3730 people in Sweden during 2010 to 2012 and reported that low (OR = 1.69; 95% CI: 1.50–1.91) or moderate education (OR = 1.43; 95% CI: 1.30–1.57), and low (OR = 1.40; 95% CI: 1.25–1.57) or moderate income (OR = 1.24; 95% CI: 1.10–1.38) was associated with a chronic pain diagnosis. Additionally, lack of efficient and effective pain management results in high levels of chronic pain recurrence.[22]
The SES was also associated with pain management, and educational levels and family income have been shown to be significantly associated with treatment for low back pain.[27] Chen et al found that the higher education levels, especially, bachelor degrees (β6: −0.96; 95% CI: −1.69 to −0.22) and postgraduate (β6: −2.10; 95% CI: −3.39 to −0.81) degrees were associated with lower probability of choosing a treatment option for pain among patients with low back pain.[27] Of note, Chen et al's study was conducted among patients with pain who visit a traditional Chinese medicine center with the aim of being treated with acupuncture or low frequency infrared treatment.
Our results are not in lined with some previous studies finding that there was a negative association between SES and pain. However, recently Fliesser et al found that job position was the best single predictor of CLBP intensity,[28] followed by a multidimensional index. Education and income had no significant association with intensity. Regarding education level, people with higher education level tend to have higher income jobs, which often lead to better medical care benefits. Also, people with high education level tend to have greater access to health resources, which could be helpful to find methods to relieve body pain.
The mechanisms of SES and body pain could partly explain by the educational inequalities impacting health via health literacy.[29] Ikeda et al pointed out in their study on low back pain that low SES is more likely to be a psychosocial stressor rather caused purely by material poverty.[30] Of note, psychosocial factors play an important role in body pain and their significance should not be ignored when considering interventions.[31] Lastly, people with lower SES more likely to face barriers in accessing medical care compared to those in wealthier SES categories.[32]
The strengths of this study include the large sample size and the adjustments for other important confounders (sex, etc). However, our study has several limitations. Pain data were self-reported, which can be less than accurate if impacted by reporting and recall biases. This could underestimate the association because people in the lower SES category are less likely to report their body pain. Furthermore, there are no validated tools for assessing self-reported pain, which impacts the validity of such reported pain categories. Future studies with pain scales are suggested to limit this bias. In addition, data on depression[33] and pain killers, which could be potential confounders, were not available but could play an important role not currently accounted for. Also, adverse life events and psychologic distress could also mediate the association between the SES and body pain, which if reported and collected could affect the results.[34] Finally, the association between sleep and pain is complex and often interrelated. As a result, there is often a reciprocal relationship among the 2, making it difficult to tease the 2 apart. For example, pain can disrupt sleep and poor sleep can exacerbate pain intensity. Due to the complexity of the relationship between pain and sleep, our current study data could not accurately assess this interrelationship.
Body pain is a challenge in the medicine, and there is a demonstrated relationship between pain and the current opioid crisis. Our research indicted there was an association between SES and body pain, which might demonstrate a need for special considerations in policies around how providers address pain management. Understanding this could help policy maker identify high-risk population more susceptible to body pain and target prevention accordingly.
In conclusion, our results indicated an association between SES and body pain within the Chinese community. Body pain varied among different Chinese occupation-related population and people with higher education level are less like to have body pain. Further investigations of the variables that impact pain are suggested to identify other factors that affect pain in future studies.
Acknowledgment
The authors thank all the participants for their co-operation in the data collection.
Author contributions
Conceptualization: Tong Yu, Tan Xu, Wenjie Sun.
Data curation: Yan Jiang, Jian Li.
Formal analysis: Yan Jiang, Jian Li.
Methodology: Tong Yu, Tan Xu, Wenjie Sun.
Writing – original draft: Tong Yu, Zhen Wei, Daihe Yang, Wenjie Sun.
Writing – review & editing: Zhen Wei, Daihe Yang, Jingnan Han, Michelle Gamber.
Correction
The article was originally published with an incorrect degree listed for Dr. Michelle Gamber. Dr. Gamber's degree has been corrected from PhD to DrPH, MA.
Footnotes
Abbreviations: CI = confidence interval, OR = odds ratio, SES = socioeconomic status.
How to cite this article: Yu T, Wei Z, Xu T, Gamber M, Han J, Jiang Y, Li J, Yang D, Sun W. The association between the socioeconomic status and body pain: a nationwide survey. Medicine. 2020;99:12(e19454).
ZW was considered as cofirst author.
This study was supported by Humanities and Social Sciences Foundation of the Anhui Higher Education Institutions of China (no: SK2019A0211).
The authors have no conflicts of interest to disclose.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Riskowski JL. Associations of socioeconomic position and pain prevalence in the United States: findings from the national health and nutrition examination survey. Pain Med 2014;15:1508–21. [DOI] [PubMed] [Google Scholar]
- [2].Elzahaf RA, Tashani OA, Unsworth BA, et al. The prevalence of chronic pain with an analysis of countries with a human development index less than 0.9: a systematic review without meta-analysis. Curr Med Res Opin 2012;28:1221–9. [DOI] [PubMed] [Google Scholar]
- [3].Jackson T, Chen H, Iezzi T, et al. Prevalence and correlates of chronic pain in a random population study of adults in Chongqing, China. Clin J Pain 2014;30:346–52. [DOI] [PubMed] [Google Scholar]
- [4].Yue P, Liu F, Li L. Neck/shoulder pain and low back pain among school teachers in china, prevalence and risk factors. BMC Public Health 2012;12:789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Liu X, Wang L, Stallones L, et al. Back pain among farmers in a northern area of China. Spine (Phila Pa 1976) 2012;37:508–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Xu Z, Yu D, Yin X, et al. Socioeconomic status is associated with global diabetes prevalence. Oncotarget 2017;8:44434–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].McLaren L. Socioeconomic status and obesity. Epidemiol Rev 2007;29:29–48. [DOI] [PubMed] [Google Scholar]
- [8].Jackson T, Thomas S, Stabile V, et al. Prevalence of chronic pain in low-income and middle-income countries: a systematic review and meta-analysis. Lancet 2015;385: Suppl 2: S10. [DOI] [PubMed] [Google Scholar]
- [9].Poleshuck EL, Green CR. Socioeconomic disadvantage and pain. Pain 2008;136:235–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Latza U, Kohlmann T, Deck R, et al. Influence of occupational factors on the relation between socioeconomic status and self-reported back pain in a population-based sample of German adults with back pain. Spine 2000;25:1390–7. [DOI] [PubMed] [Google Scholar]
- [11].Plouvier S, Leclerc A, Chastang JF, et al. Socioeconomic position and low-back pain--the role of biomechanical strains and psychosocial work factors in the GAZEL cohort. Scand J Work Environ Health 2009;35:429–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Stanaway FF, Blyth FM, Cumming RG, et al. Back pain in older male Italian-born immigrants in Australia: the importance of socioeconomic factors. Eur J Pain 2011;15:70–6. [DOI] [PubMed] [Google Scholar]
- [13].Green CR, Hart-Johnson T. The association between race and neighborhood socioeconomic status in younger black and white adults with chronic pain. J Pain 2012;13:176–86. [DOI] [PubMed] [Google Scholar]
- [14].Janevic MR, McLaughlin SJ, Heapy AA, et al. Racial and socioeconomic disparities in disabling chronic pain: findings from the health and retirement study. J Pain 2017;18:1459–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Yu T, Jiang Y, Gamber M, et al. Socioeconomic status and self-rated health in China: findings from a cross-sectional study. Medicine 2019;98:e14904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Sun W, Yu Y, Yuan J, et al. Sleep duration and quality among different occupations--China national study. PLoS One 2015;10:e0117700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Stewart Williams J, Ng N, Peltzer K, et al. Risk factors and disability associated with low back pain in older adults in low- and middle-income countries. Results from the WHO Study on global AGEing and adult health (SAGE). PLoS One 2015;10:e0127880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Yu T, Ma J, Jiang Y, et al. Assessing pain among Chinese elderly-Chinese health and retirement longitudinal study. Iran J Public Health 2018;47:553–60. [PMC free article] [PubMed] [Google Scholar]
- [19].Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs 2005;14:798–804. [DOI] [PubMed] [Google Scholar]
- [20].Bonathan C, Hearn L, Williams AC. Socioeconomic status and the course and consequences of chronic pain. Pain Manag 2013;3:159–62. [DOI] [PubMed] [Google Scholar]
- [21].Wyshak G. Health disparities paradoxes: depression and chronic back pain in college alumnae and U.S. women, 39-49. Scand J Public Health 2013;41:230–2. [DOI] [PubMed] [Google Scholar]
- [22].Chu MC, Law RK, Cheung LC, et al. Pain management programme for Chinese patients: a 10-year outcome review. Hong Kong Med J 2015;21:304–9. [DOI] [PubMed] [Google Scholar]
- [23].Jin K, Sorock GS, Courtney TK. Prevalence of low back pain in three occupational groups in Shanghai, People's Republic of China. J Safety Res 2004;35:23–8. [DOI] [PubMed] [Google Scholar]
- [24].Stranjalis G, Tsamandouraki K, Sakas DE, et al. Low back pain in a representative sample of Greek population: analysis according to personal and socioeconomic characteristics. Spine 2004;29:1355–60. [DOI] [PubMed] [Google Scholar]
- [25].Miljković A, Stipcic A, Bras M, et al. Is experimentally induced pain associated with socioeconomic status? Do poor people hurt more? Med Sci Monit 2014;20:1232–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Jöud A, Petersson IF, Jordan KP, et al. Socioeconomic status and the risk for being diagnosed with spondyloarthritis and chronic pain: a nested case-control study. Rheumatol Int 2014;34:1291–8. [DOI] [PubMed] [Google Scholar]
- [27].Chen LC, Cheng LJ, Zhang Y, et al. Acupuncture or low frequency infrared treatment for low back pain in Chinese patients: a discrete choice experiment. PLoS One 2015;10:e0126912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Fliesser M, De Witt Huberts J, Wippert PM. Education, job position, income or multidimensional indices? Associations between different socioeconomic status indicators and chronic low back pain in a German sample: a longitudinal field study. BMJ Open 2018;8:e020207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].van der Heide I, Wang J, Droomers M, et al. The relationship between health, education, and health literacy: results from the Dutch Adult Literacy and Life Skills Survey. J Health Commun 2013;18: Suppl 1: 172–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Ikeda T, Sugiyama K, Aida J, et al. Socioeconomic inequalities in low back pain among older people: the JAGES cross-sectional study. Int J Equity Health 2019;18:15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Sharma S, Pathak A, Jha J, et al. Socioeconomic factors, psychological factors, and function in adults with chronic musculoskeletal pain from rural Nepal. J Pain Res 2018;11:2385–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Elstad JI. Income inequality and foregone medical care in Europe during The Great Recession: multilevel analyses of EU-SILC surveys 2008-2013. Int J Equity Health 2016;15:101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Chen X, Cheng HG, Huang Y, et al. Depression symptoms and chronic pain in the community population in Beijing, China. Psychiatry Res 2012;200:313–7. [DOI] [PubMed] [Google Scholar]
- [34].Macfarlane GJ, Norrie G, Atherton K, et al. The influence of socioeconomic status on the reporting of regional and widespread musculoskeletal pain: results from the 1958 British Birth Cohort Study. Ann Rheum Dis 2009;68:1591–5. [DOI] [PubMed] [Google Scholar]