

Abstract
This study was conducted with the aim of determining pain acceptance levels in patients with chronic pain attending an algology outpatients’ department.
The research was conducted as a descriptive and cross-sectional study. The population of the study consisted of 97 patients with chronic pain who attended the Algology Outpatients’ Department of the Health Implementation and Research Center of Bursa Uludağ University. A Patient Description Form and a Chronic Pain Acceptance Questionnaire (CPAQ) were used to collect research data.
The participants’ mean sub-score for accomplishing activities by patients with chronic pain was found to be 31.10 ± 11.84, their mean sub-score for pain willingness was 36.65 ± 10.37, and their mean score for the total scale was 67.76 ± 18.30. A statistically significant difference was found between the participants’ total score means and their sub-score means according to their education level and frequency of experiencing pain (P < .05), but no statistically significant difference was found according to such factors as age, profession, marital status, or medications used (P > .05).
It was found that female sex was generally exposed to chronic pain, and factors such as age, marital status, and drug treatment did not differ in the rate of acceptance of chronic pain, and the rate of acceptance of pain in workers was higher, those with lower education level were lower. There is a need that new studies with larger sample groups regarding the factors affecting the acceptance of chronic pain.
Keywords: activity engagement, chronic pain, pain willingness
1. Introduction
The word “pain” originates from the word “poena” which means punishment in Latin.[1] Pain is a universal experience and the humanity has been trying to explain it for centuries. The most valid definition of the pain concept was made by the International Association for the Study of Pain (IASP). According to this definition, pain is “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”[2]
Pain should be classified in order to examine it and determine its source and appropriate treatment. In medical classifications, pain is classified according to its etiology, duration, location, and neurophysiological mechanisms.[3] According to duration, pain is classified as acute, chronic, and recurrent pain. Acute pain emerges with tissue damage and disappears after healing. Chronic pain, on the other hand, maintains longer than expected or continues after recovery. Chronic pain is a weakening medical condition that affects 12% to 30% of the population and that has been continuing for at least 3 months (6 months according to some sources).[4–6] Chronic pain is a disease that affects behaviors and lifestyles.[3] Symptoms such as anger, desperation, hopelessness, fatalism, pessimism, difficulty in adaptation, social withdrawal, mental confusion, fatigue, constant anxiety, lack of future planning, loss of ideals, and decrease in interests and activities can be seen in patients with chronic pain.[7] Therefore, chronic pain affects the quality of life negatively and may appear with depressive symptoms and significant deficiencies.[4,8,9]
Another concept that varies among individuals is pain acceptance. Chronic pain acceptance reduces unsuccessful interventions to prevent or control pain; instead, it facilitates participation in valued activities and focusing on personal goals. In recent studies, it has been found that the acceptance of chronic pain is more effective in the prevention of pain-related depression, disability, anxiety, and on the physical and occupational functioning of the patient compared with the measures to cope with pain.[10,11] In other words, it is increasingly evidenced that the behavioral aspect of pain acceptance is associated with therapeutic changes.[12] Pain should be evaluated in a multidisciplinary manner by the health care team due to many personal and institutional reasons. Nurses, irreplaceable members of the health care team, should be able to evaluate pain acceptance in order to provide patient comfort.[13]
Pain acceptance can be evaluated by using scales. The evaluation of the acceptance of chronic pain will shape the approach of the health care team, especially nurses, on coping with pain and allow the understanding of individual differences in coping with pain. Pain is a complex, multifaceted condition since it is affected by different physical, emotional, psychological, and social factors.[14] Based on these reasons, this study was conducted to determine the rate of pain acceptance in patients with chronic pain who applied to the algology outpatient clinic.
2. Materials and methods
The study was conducted as a descriptive and cross-sectional study. As a result of the pilot study, according to the 27% inverse correlation between the frequency of pain and the total score of the pain scale, the sample size calculated for 0.05 significance level and 80% power was determined as 91 patients.The universe of the study consisted of 97 patients who had chronic pain (for at least 3 months) for any reason and who applied to the Algology Outpatient Clinic of Bursa Uludağ University Health Application and Research Center (September 2018–January 2019). The simple random sampling method was used and patients who accepted to participate constituted the sample of the study. The “Patient Identification Form” and the “Chronic Pain Acceptance Questionnaire” (CPAQ) were used to collect the research data.
2.1. Patient identification form
This form was prepared by the researchers and included the questions regarding the descriptive characteristics of the patients such as age, sex, occupation, educational status, marital status, clinical diagnosis, cause, duration, frequency of pain, and medications used.
2.2. Chronic pain acceptance questionnaire
The questionnaire was developed from the “Acceptance and Action” questionnaire which is a pain acceptance and experiential avoidance questionnaire developed by Geiser.[15] The initial version of the CPAQ had consisted of 34 items. Of these items, 24 had been used to calculate the total score. In the following studies, the content and factor structures were developed and the form that consisted of 20 items and 2 subscales was accepted as the most appropriate version.[3] The Turkish validity and reliability study of the Chronic Pain Acceptance Questionnaire was conducted by Akmaz et al[3] in 2015. The Likert type questionnaire consists of 20 items and is scored between 0 and 6 (0: never true, 1: very rarely true, 2: seldom true, 3: sometimes true, 4: often true, 5: almost always true, 6: always true). The first subscale, “Activity engagement,” consists of 11 items (items 1, 2, 3, 5, 6, 8, 9, 10, 12, 15, and 19) and evaluates how much the individual can take part in the daily activities in the presence of pain. The second subscale, “Pain willingness,” consists of 9 items (items 4, 7, 11, 13, 14, 16, 17, 18, and 20), and evaluates at which level pain can be tolerated without any attempt to avoid or control it. In the study, the Cronbach alpha value of the questionnaire was found to be 0.848.
The permission of the author who performed the Turkish adaptation study of the questionnaire was taken. Necessary legal permission was obtained from the Clinical Research Ethics Committee of the university where the study was carried out (Decision no: 2018–15/19). Moreover, informed consent was taken from the patients who accepted to participate in the study and who met the research criteria. Scale permission was obtained from the researcher who conducted the Turkish Reliability and Validity Study. Subsequently, questionnaire forms were collected face-to-face at an appropriate time in the outpatient clinic (The data were not collected at the time of treatment, rest, etc. sessions of the patients). The duration of the application of the questionnaire lasted approximately 10 to 15 minutes for each patient.
2.3. Analysis of data
Statistical analysis of the research data was performed with the statistics package IBM SPSS 22.0 (SPSS Inc., Chicago, IL). Numerical data was examined by the Kolmogorov Smirnov test for whether it showed normal distribution. Distributions of descriptive information on patients obtained as a result of the study were given as means and standard deviations. Because the research data showed normal distribution, the Independent Sample t test and the one-way Analysis of variance test were used in the analysis of the data. The level of statistical significance was determined as P < .05.
2.4. Inclusion criteria
-
1.
Being over 18 years old.
-
2.
Not having a psychiatric diagnosis.
-
3.
Not being and not receiving psychiatric medication.
-
4.
Having been suffering from chronic pain for at least 3 months.
-
5.
Providing volunteer participation to the research.
3. Results
Of the patients with chronic pain who were included in the study, 64.9% were women and 35.1% were men and the mean age was 52.9 ± 14.88 years. The majority were in the age ranges between 31–50 (39.2%) and 51–70 (40.2%) years. Of the patients, 39.2% were housewives, 80.4% were married, 51.5% were primary and or secondary school graduates. The mean subscale score of the patients was 31.10 ± 11.84 for the activity engagement subscale and 36.65 ± 10.37 for pain willingness subscale. The mean total score of the questionnaire was calculated as 67.76 ± 18.30 (Table 1).
Table 1.
Comparison of total and subscale scores of patients from “Chronic Pain Acceptance Questionnaire” according to their descriptive characteristics.
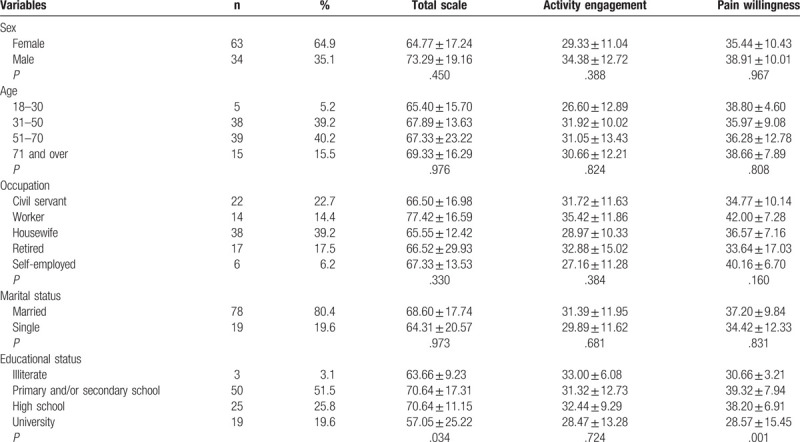
The activity engagement and pain willingness subscale scores and the total CPAQ score were found to be higher in men compared with women, in married ones compared with singles, and in those who worked as a worker compared with those in other occupational groups; however, there was no statistically significant difference (Table 1, P > .05). Participants who were at the age of 71 years and over were found to have a higher activity engagement subscale score and total CPAQ score; however, there was no statistically significant difference found between the groups (Table 1, P > .05).
When the mean scale scores of the participants were evaluated according to their educational status, it was found that those who were “primary and/or secondary school” and “high school” graduates had a higher mean total score, that those who were “illiterate” had a higher activity engagement subscale score, and that those who were “primary and/or secondary school” graduates had a higher pain willingness subscale score compared with other groups. Those who were university graduates had the lowest total CPAQ score and subscale scores. As a result of the statistical analysis, there was a statistically significant difference found between the mean total CPAQ score and the mean pain willingness subscale score in terms of the educational status of the patients (P < .05) (Table 1).
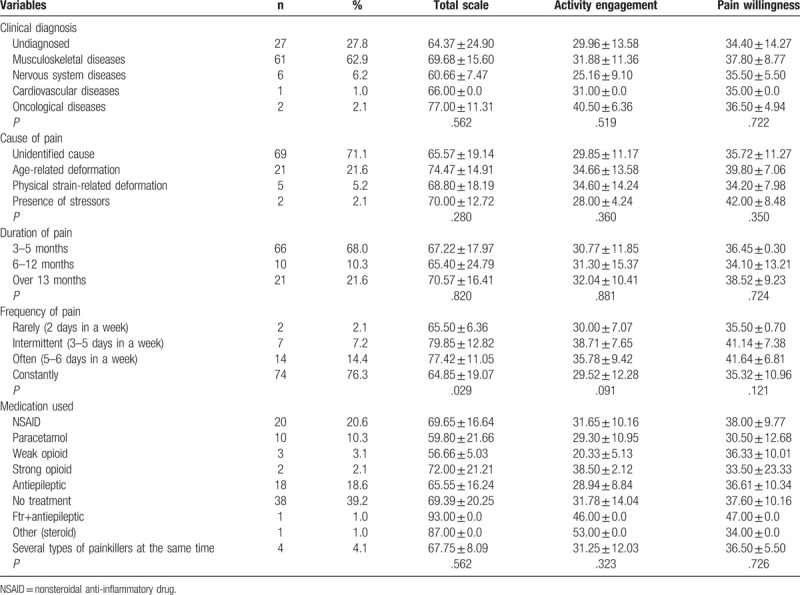
When the findings related to the health/disease status of the patients were examined, it was found that 62.9% of the patients had musculoskeletal diseases, that 71.1% had pain due to unidentified cause. 68% of the patients stated that they had pain for 3 to 5 months, 76.3% stated that they had pain constantly, and 39.2% stated that they did not receive medication (Table 2). When the findings related to the health/disease status of the patients and their total CPAQ scores and subscale scores were compared, the participants with oncological diseases were found to have the highest mean total score and activity engagement and pain willingness subscale scores. On the other hand, those with nervous system diseases had the lowest scores. However, there was no statistically significant difference found in the mean scores between the groups (P > .05). When the mean scale scores were examined according to the causes of pain, those who had age-related deformation had the highest mean scores and those who had pain due to the unidentified cause had the lowest mean scores. According to the duration of pain, those who had pain for over 13 months were found to have the highest mean scores. However, as a result of statistical analysis, there was no statistically significant difference found in the mean scores between the groups (P > .05). When the patients were evaluated according to the frequency of pain, those who had intermittent pain were found to have significantly higher mean total CPAQ score compared with those who had constant pain (P < .05) (Table 2).
Table 2.
Comparison of the health/disease findings of patients and their total and subscale scores from “Chronic Pain Acceptance Questionnaire (CPAQ).”.
4. Discussion
Chronic pain is a health problem that is frequently encountered in clinical practice and that increases rapidly.[16,17] Moreover, chronic pain is a common inhibitory disease that does not fully respond to current medical treatments.[14,18] Epidemiological studies on pain examine how much of the population complains of pain and the relationship between pain and variables such as age, sex, race, and social differences.[19] In this study, it was aimed to determine the rate of pain acceptance in patients with chronic pain and affecting variables.
Since pain is a subjective and individual finding, symptoms may vary from person to person.[20] For example; women have a higher prevalence of chronic pain than men.[14,21] When pain-related variables were examined, it was determined that 64.9% of the participants were women. In the study conducted by Wijnhoven et al,[14] similar results were obtained. The fact that the majority of the subjects that constituted the group of chronic pain patients were women suggests that women are more sensitive to pain. When the results were examined according to age, there was no statistically significant difference found between the mean age of the patients and the total CPAQ score and subscale scores. In the study conducted by Akmaz (2018) with patients with chronic pain, there was no significant difference found between the age, sex, and educational status of the patients and the mean total CPAQ score and subscale scores.[3] It was seen that this result supports our study.
In our study, those who were university graduates had the lowest total score and subscale scores and those who were primary, secondary, and high school graduates had the highest scores. Individuals who have a low educational level usually work in jobs that require severe physical conditions. In our study, the total score and subscale scores of the individuals who worked as a worker were found to be higher than the patients in other groups. This suggests that individuals who have a low educational level and who work as a worker may highly tolerate pain due to reasons such as lack of time or economic insufficiency, etc.
Chronic pain remains a major challenge for patients and healthcare workers due to their limited treatment and uncertain etiology.[22] At the same time, their widespread effects are costly for the community and they use up to 5 times more drugs than the general population.[14,23] Especially, pharmacological approaches take an important place in the treatment of chronic pain.[24] Despite current therapeutic approaches, the strongest drugs, including analgesic and opioid drugs, have been found to reduce pain by only 30% to 40%.[18] This is mostly due to the fact that chronic pain is accompanied with significant disability and depressive symptoms because of its negative effect on the quality of life.[4] According to the results of our research, it was determined that 20.6% of the patients used NSAID and that 39.2% did not receive any medication. When the studies in the literature were examined, it was found that 43.8% of the patients used NSAIDs and that 18% did not use analgesic drugs.[3] Drugs used in our study are similar to those in the literature.
The reason for the combined treatment and the variety of medications used in patients with chronic pain is that chronic pain is diagnosed on one or more body regions. When the literature was examined, in the study conducted by Ayvat et al,[23] it was found that patients experienced headache with the highest rate of 12.4%.[19] However, in the study conducted by Akmaz (2018), it was determined that chronic pain was experienced due to lumbar disc hernia with the highest rate of 41.8%.[3] When the distribution of pain regions and clinical diagnoses of the patients who participated in our research were examined, it was found that most of the patients had musculoskeletal pain (62.9%). However, it was seen that the participants who had a nervous system disease had the lowest total CPAQ score and mean activity engagement subscale score. The lowest rate of pain acceptance in the patients with nervous system pain was estimated to be due to the fact that the use of only analgesics was not sufficient for the management of such pain.
In addition, although 27.8% of the patients had chronic pain, they did not have a diagnosed disease. Other patients had chronic diseases that were unlikely to heal. Our results showed that the “Pain Acceptance Rate” of undiagnosed patients were lower than those diagnosed. In other words, the fact that the cause of the pain was not known had a negative effect on pain acceptance. In order to eliminate the prejudices experienced by many chronic pain patients, health professionals should accept that the pain is “real.” This is still an important approach in the treatment of chronic pain.[1] In other words, the tolerance to pain may increase if health professionals approach pain seriously and accept it.[25] Acceptance of pain means that a person engages to take valuable actions despite the pain.[26] Among the individuals who participated in this study, those who had pain due to “unidentified cause” and who had undiagnosed pain were found to have the lowest total CPAQ score and mean activity engagement subscale score. In the study conducted by Wang et al,[25] it was found that pain acceptance increased pain tolerance and endurance. These results suggest that prejudices experienced by patients may also affect the rate of pain acceptance in pain with an unidentified cause.
The frequency and duration of pain should be examined in the diagnosis of pain. In addition to the determination of the course of pain from the beginning to the present, the daily course of pain should also be recorded.[27] Because the course and duration of pain can trigger pain attacks in the patient and prolong pain-related deficits.[28] In our research, the lowest pain acceptance score was found to belong to those who experienced pain for 6 to 12 months. However, there was no statistically significant difference determined between the duration of pain and the total CPAQ score and subscale scores. On the other hand, when the patients were examined according to the periodic evaluation of pain, it was determined that those who suffered from constant pain had the lowest total CPAQ score and subscale scores; however, the difference was not significant. This suggests that the prolongation of pain recurrence may reduce pain tolerance in patients.
4.1. Limitations of research
-
1.
Since our study was conducted in a single center, it is not possible for the results to represent all patients with chronic pain.
-
2.
In our data collection instruments, a scale that objectively determines the degree of pain was not used. The duration of the pain rather than the degree of pain (chronic pain), frequency, and causes are focused.
-
3.
Scale items are based on the statements of the patients only.
5. Conclusion
Chronic pain negatively affects the quality of life of individuals and prevents efficiency in daily activities. Our study results show that women encounter chronic pain more frequently. On the other hand, it was determined that factors such as age, marital status, and drug treatment do not make a difference in the rate of pain acceptance and subscales. However, patients with low educational status were determined to have a lower rate of pain acceptance and that those who worked as a worker had a higher rate of pain acceptance. Furthermore, it was concluded that more frequent pain periods and recurrent pain obstruct to tolerate and accept pain. It is thought that conducting new researches with larger sample groups for determining the factors affecting chronic pain acceptance may contribute to understanding the current situation.
Author contributions
Conceptualization: Hava Gökdere Çinar, Dilek Yilmaz, Esra Akin.
Data curation: Hava Gökdere Çinar, Dilek Yilmaz.
Investigation: Hava Çinar.
Methodology: Dilek Yilmaz.
Project administration: Hava Gökdere Çinar.
Supervision: Hava Gökdere Çinar, Dilek Yilmaz, Esra Akin.
Writing – Original Draft: Hava Gökdere Çinar.
Writing – Review &Editing: Hava Gökdere Çinar, Dilek Yilmaz, Esra Akin.
Hava Gökdere Çinar orcid: 0000-0002-5792-5958.
Footnotes
Abbreviations: CPAQ = chronic pain acceptance questionnaire, NSAID = nonsteroidal anti-inflammatory drug.
How to cite this article: Çinar HG, Yilmaz D, Akin E. Pain acceptance levels of patients with chronic pain. Medicine. 2020;99:17(e19851).
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors have no conflicts of interest to disclose.
References
- [1].Bendelow G. Chronic pain patients and the biomedical model of pain. Virtual Mentor 2013;15:455–9. [DOI] [PubMed] [Google Scholar]
- [2].Aydin D, Sahiner NC, Çiftci EK. Comparison of the effectiveness of three different methods in decreasing pain during venipuncture in children: ball squeezing, balloon inflating and distraction cards. J Clin Nurs 2016;25:2328–35. [DOI] [PubMed] [Google Scholar]
- [3].Akmaz HE, Uyar M, Yildirim YK, et al. Validity and reliability of the Turkish chronic pain acceptance questionnaire. Balkan Med J 2018;35:238–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Carvalho SA, Gillanders D, Palmeira L, et al. Mindfulness, selfcompassion, and depressive symptoms in chronic pain: the role of pain acceptance. J Clin Psychol 2018;74:2094–106. [DOI] [PubMed] [Google Scholar]
- [5].Çeliker R. Kronik ağri sendromlari. Türk Fiz Tip Rehab Derg 2005;51:14–8. [Google Scholar]
- [6].Jeong S, Cho S. Acceptance and patient functioning in chronic pain: the mediating role of physical activity. Qual Life Res 2017;26:903–11. [DOI] [PubMed] [Google Scholar]
- [7].Karadakovan A. Eti Aslan F. Dâhili ve Cerrahi Hastaliklarda Bakim. 2. Baski Nobel Tip Kitabevi. Adana 2011;140–70. [Google Scholar]
- [8].Breivik H, Eisenberg E, O’Brien T. The individual and societal burden of chronic pain in Europe: the case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health 2013;13:1229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Gatchel RJ, Okifuji A. Evidence-based scientific data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain 2006;7:779–93. [DOI] [PubMed] [Google Scholar]
- [10].Singh MK, Patel J, Gallagher RM. Chronic pain syndrome. Phys Med Rehabil 2005. [Google Scholar]
- [11].Henriksson J, Wasara E, Rönnlund M. Effects of eight-week-web-based mindfulness training on pain intensity, pain acceptance, and life satisfaction in individuals with chronic pain. Psychol Rep 2016;119:586–607. [DOI] [PubMed] [Google Scholar]
- [12].Holmner EP, Stålnacke B-M, Enthoven P, et al. “The acceptance” of living with chronic pain – an ongoing Process: a qualitative study of patient experiences of multimodal rehabilitation in primary care. J Rehabil Med 2018;50:73–9. [DOI] [PubMed] [Google Scholar]
- [13].Abd El-Gawad SM, Elsayed LA. Effect of interactive distraction versus cutaneous stimulation for venipuncture pain relief in school age children. J Nurs Educ Pract 2015;5:32–40. [Google Scholar]
- [14].Wijnhoven HA, de Vet HC, Picavet HS. Prevalence of musculoskeletal disorders is systematically higher in women than in men. Clin J Pain 2006;22:717–24. [DOI] [PubMed] [Google Scholar]
- [15].McCracken LM, Eccleston C. Coping or acceptance: what to do about chronic pain? Pain 2003;105:197–204. [DOI] [PubMed] [Google Scholar]
- [16].McCracken LM, Vowles KE, Ecclestton C. Acceptance of chronic pain: component analysis and a revised assessment method. Pain 2004;107:159–66. [DOI] [PubMed] [Google Scholar]
- [17].Jensen MP, Smith AE, Alschuler KN, et al. The role of pain acceptance on function in individuals with disabilities: a longitudinal study. Pain 2016;157:247–54. [DOI] [PubMed] [Google Scholar]
- [18].Çöçelli P, Bacaksiz BD, Ovayolu N. Ağri tedavisinde hemşirenin rolü. Gaziantep Tip Dergisi 2008;14:53–8. [Google Scholar]
- [19].University of Nevada-Reno, Geiser DS. A Comparision of Acceptance-Focused and Control-Focused Psychological Treatments in a Chronic Pain Treatment Center. 1992;Unpublished doctoral dissertation. [Google Scholar]
- [20].Tütüncü R, Günay H. Chronic pain, psychological factors and depression. Dicle Med J 2011;38:257–62. [Google Scholar]
- [21].Kuru T, Yeldan İ, Zengin A, et al. The prevalence of pain and different pain treatments in adults. Ağri 2011;23:22–7. [DOI] [PubMed] [Google Scholar]
- [22].Chiesa A, Serretti A. Mindfulness-based interventions for chronic pain: a systematic review of the evidence. J Alternat Complement Med 2011;17:83–93. [DOI] [PubMed] [Google Scholar]
- [23].Ayvat PÜ, Aydin ON, Oğurlu M. Sociodemographic properties and pain prevalence of patients applying to the Algology Department polyclinic of Adnan Menderes University Medical Faculty. Ağri 2011;23:28–39. [DOI] [PubMed] [Google Scholar]
- [24].Kelle İ. Ağri tedavisinde alternatif ilaçlar. Dicle Tip Dergisi 2006;33:192–200. [Google Scholar]
- [25].Wang Y, Qi Z, Hofmann SG, et al. Effect of acceptance versus attention on pain tolerance: dissecting two components of mindfulness. Mindfulness (N Y) 2019;10:1352–9. [PMC free article] [PubMed] [Google Scholar]
- [26].McCracken LM. Learning to live with the pain: acceptance of pain predicts adjustment in persons with chronic pain. Pain 1998;74:21–7. [DOI] [PubMed] [Google Scholar]
- [27].Önal A. Algoloji. 2004;İstanbul: Nobel Tip Kitabevleri, 21–31. [Google Scholar]
- [28]. Twycross A, Dowden S, Stinson J. çocuklarda ağri yönetimi. (Çev. Edit: Bayat M., Avci, Ö.) Nobel Akademik Yayincilik, Ankara; 2018: 180–190. [Google Scholar]