

Abstract
The objective of this review is to systematically evaluate the short-term efficacy of mud therapy in the treatment of knee osteoarthritis (KOA).
Randomized controlled trials, in which treatment of KOA is mud therapy, were included by systematically searching the PubMed, Embase, and the Cochrane Library databases.
According to inclusion criteria and searching method, 11 articles, containing a total of 1106 patients, were included in the study. Our results showed significant differences in visual analog scale pain score and Western Ontario and McMaster Universities Osteoarthritis Index (pain, stiffness, function). In addition, the heterogeneity of study included is lower (I2 < 25%).
According to the results of this meta-analysis, mud therapy can effectively alleviate the pain and improve joint function for KOA.
Keywords: efficacy, knee osteoarthritis, meta-analysis, mud therapy, short-term
1. Introduction
Knee osteoarthritis (KOA), known as musculoskeletal diseases with degradation of the articular cartilage and narrowing of the joint space, is common in middle-aged and elderly people aged over 50 years.[1,2] In general, pain, stiffness, and impaired function are the main clinical symptoms of KOA. It is known that obesity, age, occupation, and joint injury are high risk factors for KOA, but the exact pathogenesis of KOA remains unclear.[3] There are studies which have shown that proinflammatory cytokines such as IL-1β, IL-6, IL-8, and TNF-α were closely related to the occurrence and development of KOA.[4] The common treatments of KOA include pharmacotherapy, patient education, lifestyle modification, and joint-replacing procedures.[5]
Mud therapy, one of the conservative treatments of KOA, was used as approach to treat KOA many years ago in Europe.[6] Mud, a natural substances, consists of various amounts of organic and inorganic substances.[7] According to the report, the KOA patients experienced relief in joint pain after mud therapy.[8] The therapeutic effect of mud therapy has been ascribed mainly to thermal and systemic anti-inflammatory effect.[9,10] It plays an important role in treatment of KOA that an increase of cartilage turnover induced by thermal stress.[11] On the other hand, thermal stress could modify the expression of microRNA, which were up-regulated in OA.[12,13] New study showed mud therapy could relieve inflammatory reactions and have an immune-modulating effect,[14,15] in which levels of the proinflammatory cytokine IL-1β, TNF-α, IL-8, IL-6, and TGF-β decreased and anti-inflammatory IL-10 increased after mud therapy. In addition, mudbath, a combination of mud and mineral baths, had the advantage of low cost and convenience.[16–18]
Efficacy of mud therapy has been confirmed by a lot of researches, but still has some controversy. For example, since it is not clear which elements of mud are necessary and what is the appropriate concentration of these elements,[35] results of Evcik et al[28] and Gungen et al[23] showed efficacy of mud therapy was not significantly better than other therapies in alleviating pain. These inconsistent conclusions could affect clinical decision-making. This meta-analysis that included the latest randomized controlled trials (RCT) systematically evaluated the efficacy of mud therapy in treating KOA and provided evidence-based basis for clinical practice.
2. Materials and methods
2.1. Searching strategy
The meta-analysis was performed according to PRISMA guidelines.[19] This study does not need the approval of the ethics committee because it is based on literature research. Two investigators independently searched for three databases, PubMed, Embase, and the Cochrane Library, by using combination of MeSH terms and free words. There is no limit on the language and date of searching literature published before July 20, 2019. The English search terms included mud, pelotherapy, peloid therapy, knee osteoarthritis, etc.
2.2. Inclusion and exclusion criteria
Studies were included if satisfying the following criteria:
-
1.
Study was RCT.
-
2.
Patients were diagnosed with KOA.
-
3.
Clinical results included one of VAS and Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index in early stage.
-
4.
Experimental group must contain mud therapy and control group was not limited except mud therapy.
Relatively, studies will be excluded if they cannot meet the inclusion criteria.
2.3. Data extraction
All data were extracted independently by 2 investigators after reading and screening in detail. Data included the following: name of first author, year of publication, sample size, country, interventions of experimental groups and control groups, time out, outcome measures, age of patients, and BMI index. If different opinions arise, the third researcher will participate in the discussion and make decision.
2.4. Quality assessment
Methodological quality of RCT which were included were assessed by Cochrane risk of bias tool.[31] Assessment included 6 aspects: generation of random sequence, concealment allocation, application of blinding, integrity of outcome data, selective reporting, and other bias. According to assessment, the types of bias are divided into “high risk”, “unclear risk,” and “low risk.”
2.5. Statistical methods
Data which were combined in this meta-analysis were analyzed by using RevMan 5.3 software (Cochrane Collaboration, Oxford, UK). Homogeneity of studies was quantified by using the I-squared statistic (I2).[20] Author used fixed-effects model to generate the standardized mean difference (SMD) if there is not significant heterogeneity (I2 < 50%). On the contrary, when heterogeneity is significant (I2 > 50%), random effects was used.[21] Publication bias was evaluated by funnel plots graphically. It was considered with the absence of bias if funnel plots are symmetric.
3. Results
3.1. Literature selection
The process of literature screening is presented in Figure 1. According to required search terms, 2 investigators searched for 256 articles. Among 256 articles, 190 articles were excluded after looking through title and abstracts of articles. At last, 2 investigators read full text of the remaining 38 articles in detail, deciding to include 11 articles.
Figure 1.
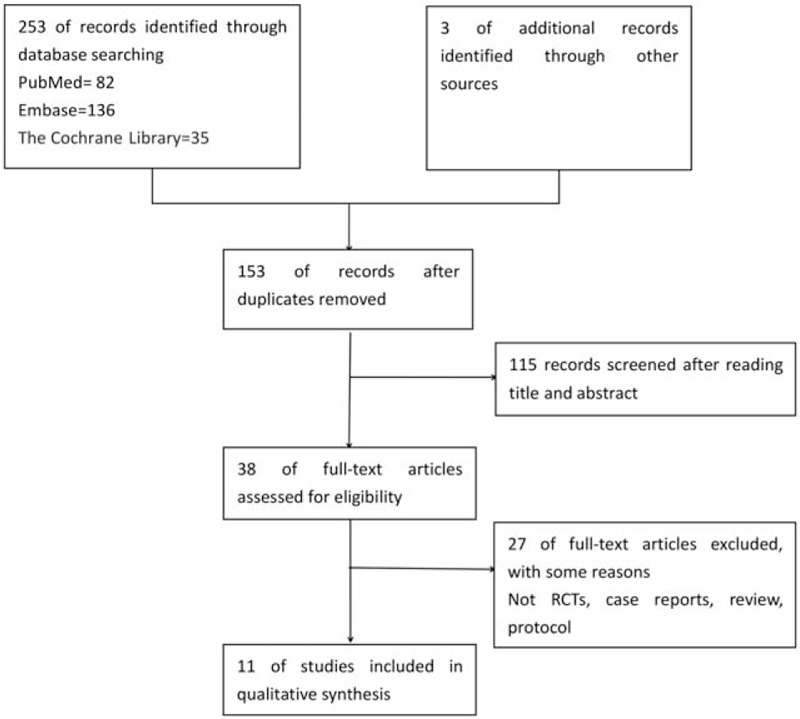
Flow diagram of included studies.
3.2. Literature characteristics
Characteristics of the 11 articles included are shown in Table 1. Among 11 articles included, there were 10 English articles[11,12,22–29] and 1 Spanish article,[30] in which 4 articles were from Italy, 3 articles were from Turkey, and the remaining 4 articles were from France, Hungary, Iran, and Spain.
Table 1.
Basic characteristics of the included studies.
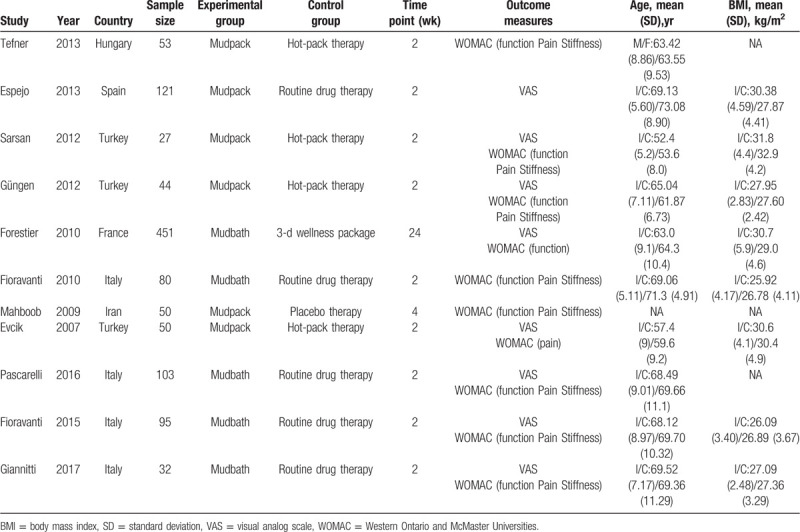
A total of 1106 patients were included, in which 565 were in the experimental group and 541 in the control group. The largest sample size was 451 and the smallest was 27. In the experimental group, intervention method of 6 groups[22,23,26,28–30] was mudpack therapy, and for remaining 5 groups[11,12,24,25,27] was mudbath therapy.
3.3. Quality assessment of literature
According to Cochrane risk of bias tool,[31] the assessment results are shown in Figure 2. The literature included were RCTs, in which 10 studies[8,9,22–27,29,30] described specific method of random, 2 studies[22,24] used allocation concealment, 2 studies[24,29] applied double blind methods, and 5 studies[22,24,26,28,30] reported absence of cases. It was not clear whether there was selective reporting in all. There were no statistically significant differences between the study groups in terms of baseline characteristic.
Figure 2.
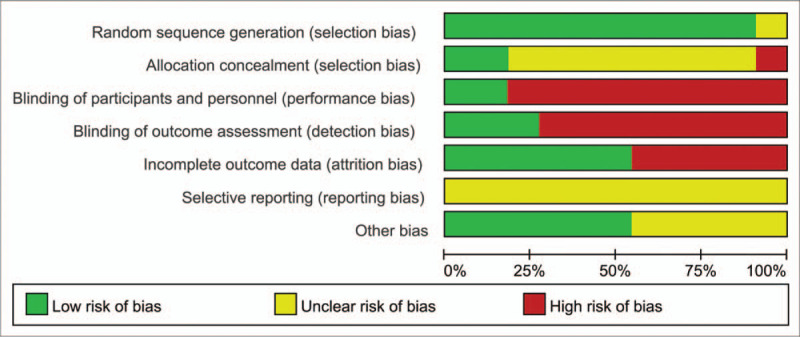
Risk of bias summary of included studies.
3.4. Meta-analysis
3.4.1. VAS pain score
Visual analog scale pain scores of 8 articles[11,12,22–24,27,28,30] were combined and analyzed to assess the short-term efficacy of mud therapy in alleviating pain. As shown in Figure 3, the result showed it was significantly different in characteristics of the experimental and control groups [SMD = –0.74, 95% CI (–1.08, –0.41), P < .0001], implying the use of mud therapy can effectively alleviate pain symptoms when compared with other intervention methods. On the other hand, (I2 = 15%, P = .31) presented heterogeneity of combined data was low.
Figure 3.
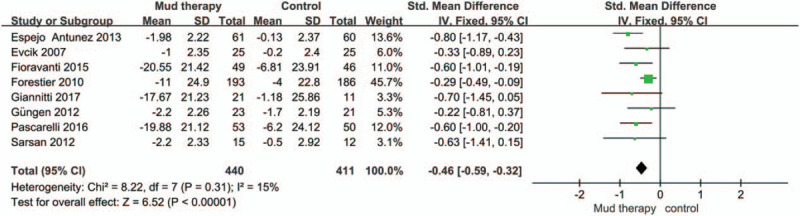
Forest plot of visual analog scale pain score. CI = confidence interval, SD = standard deviation.
3.4.2. WOMAC Osteoarthritis Index (pain, stiffness, function)
We combined and analyzed WOMAC Osteoarthritis Index[32] in this study. There are 10 articles which reported WOMAC Osteoarthritis Index, in which 9 articles[11,12,22,23,25–29] provided WOMAC pain index, 8 articles[11,12,22,23,25–27,29] WOMAC stiffness index, and 9 articles[11,12,22–27,29] WOMAC joint functions index. As shown in Figures 4–6, all statistical analysis applied fixed-effects model due to lower heterogeneity (I2 < 25%). It is shown in Figure 4 that patients in the experimental group had significantly lower WOMAC pain index [SMD = –0.53, 95% CI (–0.71, –0.36), P < .00001]. There was significant difference in characteristics of the experimental and control groups [SMD = –0.50, 95%CI (–0.68, –0.31), P < .00001] (Fig. 5). Similarly, patients who had mud therapy showed significantly lower WOMAC joint function index [SMD = –0.43, 95% CI (–0.57, –0.29), P < .00001] (Fig. 6).
Figure 4.
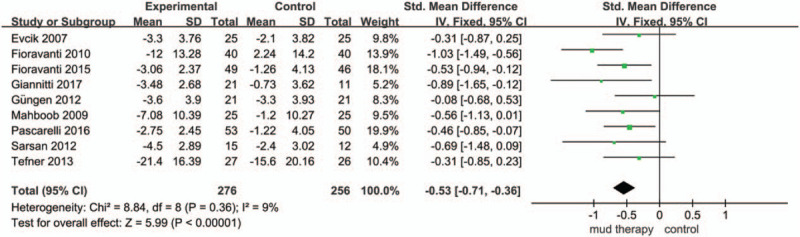
Forest plot of Western Ontario and McMaster Universities pain index. CI = confidence interval, SD = standard deviation, VAS = visual analog scale.
Figure 6.
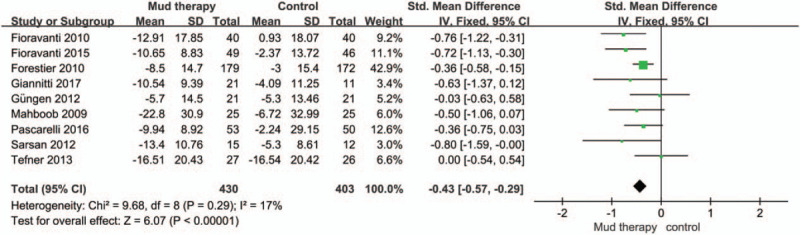
Forest plot of Western Ontario and McMaster Universities joint functions index. CI = confidence interval, SD = standard deviation.
Figure 5.
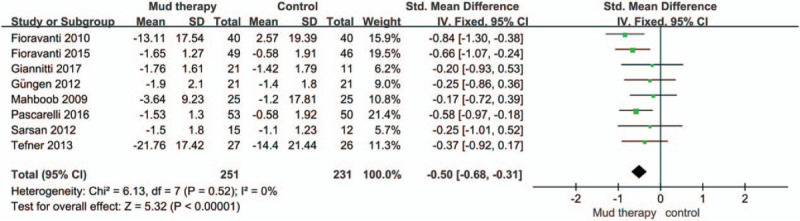
Forest plot of Western Ontario and McMaster Universities stiffness index. CI = confidence interval, SD = standard deviation.
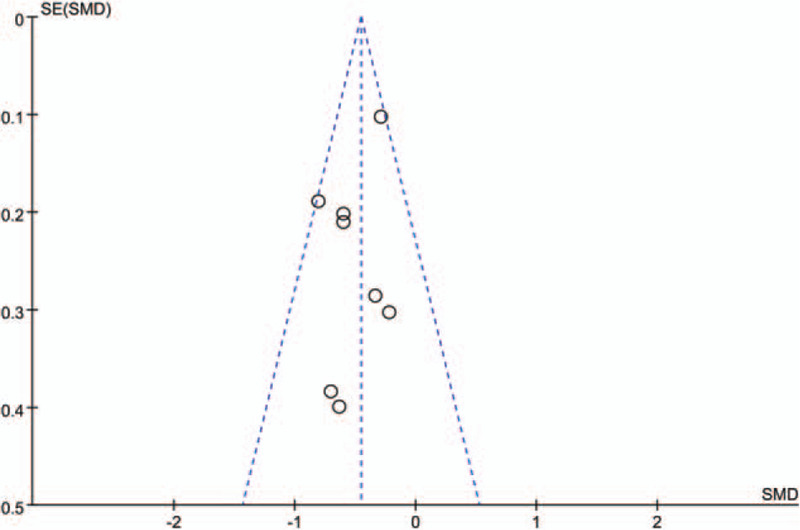
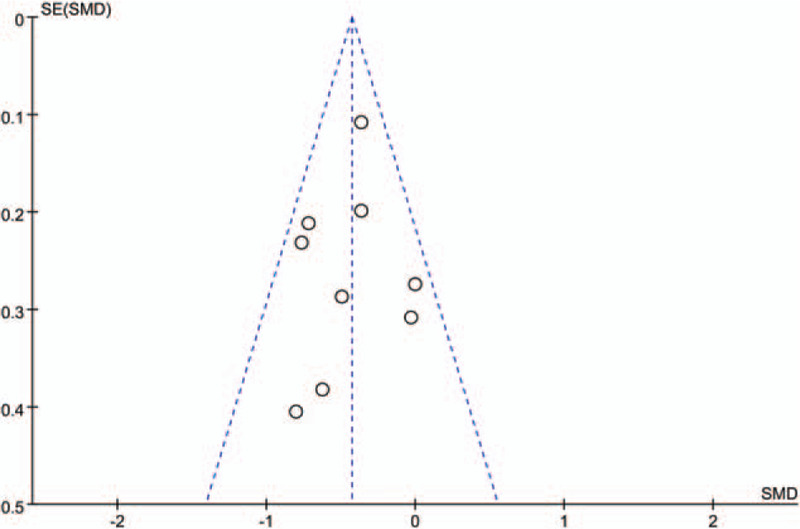
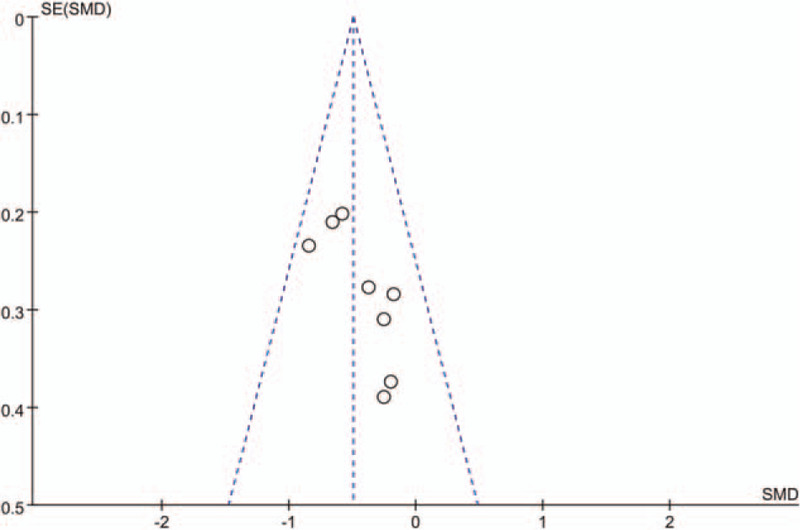
3.5. Publication bias
According to results of funnel plots (Figs. 7–10), studies may have certain publication bias because symmetry of funnel plots is unsatisfactory.
Figure 7.
Funnel plot of the visual analog scale pain score. SMD = standardized mean difference, SE = standard error.
Figure 10.
Funnel plot of Western Ontario and McMaster Universities joint functions index. SMD = standardized mean difference, SE = standard error.
Figure 8.
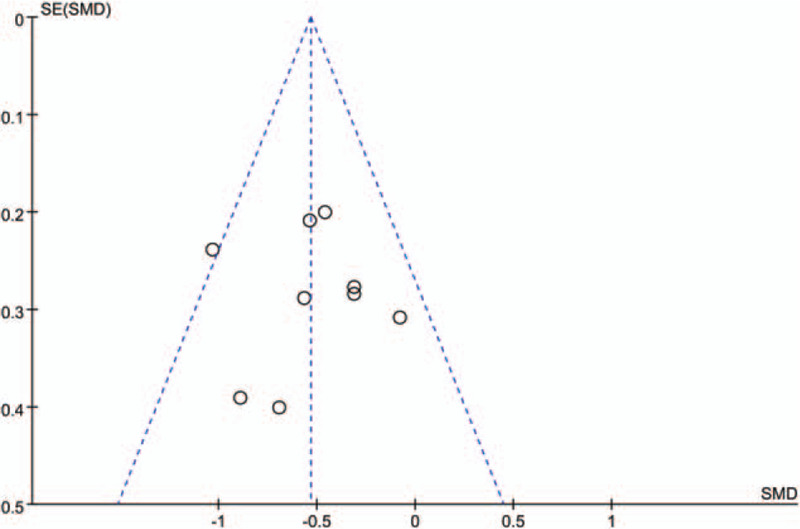
Funnel plot of Western Ontario and McMaster Universities pain index. SMD = standardized mean difference, SE = standard error.
Figure 9.
Funnel plot of Western Ontario and McMaster Universities stiffness index. SMD = standardized mean difference, SE = standard error.
4. Discussion
This meta-analysis, including 11 trials, systematically assessed the beneficial effects of mud therapy in treating KOA. According to result of our meta-analysis (Figs. 3 and 4), patients who received mud treatment significantly relieved pain compared with other treating methods. As shown in Figures 5 and 6, the application of mud therapy can significantly improve joint functions compared to the control group. On the other hand, heterogeneity of all studies was low.
At present, Liu et al[33] and Xiang, Wu, and Li [34] showed that it is possible to alleviate pain and improve function by the use of mud therapy, but their meta-analyses have some drawbacks. At first, the conclusion of study is unstable because of high heterogeneity of combined studies. In addition, Flusser et al[10] and Odabasi et al,[35] in which the experimental and control groups both have mud therapy, were unable to judge the difference between the mud therapy and other treatments.
Compared with previously published meta-analyses, this review has some advantages. First, this review includes more articles. Secondly, the outcome indicators of study are more comprehensive. Finally, the conclusions of study are stable due to low heterogeneity.
This review has limitations. First, according to result of quality assessment, there are biases in studies to influence experimental results. For example, some studies did not use allocation concealment, others did not blind methods because of specific characteristics of mud therapy, but the conclusion of studies was still credible due to low heterogeneity. Secondly, long-term efficacy of mud therapy in treatment of KOA is unclear because this meta-analysis only made an early observation. However, compared with observation of long-term efficacy, the observation of short-term efficacy can more truly reflect the efficacy of mud therapy because long-term efficacy may be influenced with other interfering factors. Hence, the observation of short-term efficacy is more in accord with the purpose of this study.
5. Conclusions
Based on existing evidence, the short-term efficacy of mud therapy was significant in relieving pain and improving joint functions for patients with KOA.
Author contributions
Conceptualization: Chengzhi Hou.
Data curation: Chengzhi Hou, Long Liang.
Formal analysis: Chengzhi Hou, Xuelei Chu.
Funding acquisition: Yong Zhao.
Methodology: Chengzhi Hou, Weikai Qin.
Resources: Chengzhi Hou, Yongyao Li.
Software: Long Liang.
Supervision: Yong Zhao.
Writing – original draft: Chengzhi Hou.
Writing – review & editing: Chengzhi Hou, Long Liang, Xuelei Chu, Yong Zhao.
Footnotes
Abbreviations: KOA = knee osteoarthritis, RCT = randomized controlled trial, VAS = visual analog scale, WOMAC = Western Ontario and McMaster Universities.
How to cite this article: Hou C, Liang L, Chu X, Qin W, Li Y, Zhao Y. The short-term efficacy of mud therapy for knee osteoarthritis: a meta-analysis. Medicine. 2020;99:17(e19761).
CH, LL, and XC contributed equally to this work and are the co-first authors.
This study was supported by grants from the Fundamental Research Funds for the Central public welfare research institutes (ZZ11-034) and National Natural Science Foundation of China (No. 81703845).
The author(s) of this work have nothing to disclose.
References
- [1].Thomas E, Peat G, Croft P. Defining and mapping the person with osteoarthritis for population studies and public health. Rheumatology (Oxford) 2014;53:338–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Goldring SR, Goldring MB. Clinical aspects, pathology and pathophysiology of osteoarthritis. J Musculoskelet Neuronal Interact 2006;6:376–8. [PubMed] [Google Scholar]
- [3].Blagojevic M, Jinks C, Jeffery A, et al. Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthr Cartil 2010;18:24–33. [DOI] [PubMed] [Google Scholar]
- [4].Mabey T, Honsawek S. Cytokines as biochemical markers for knee osteoarthritis. World J Orthop 2015;6:95–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Hussain SM, Neilly DW, Baliga S, et al. Knee osteoarthritis: a review of management options. Scot Med J 2016;61:7–16. [DOI] [PubMed] [Google Scholar]
- [6].Zhang W, Doherty M, Arden N, et al. EULAR evidence based recommendations for the management of hip osteoarthritis: report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis 2005;64:669–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Veniale F, Barberis E, Carcangiu G, et al. Formulation of muds for pelotherapy: effects of “maturation” by different mineral waters. App Clay Sci 2004;25:135–48. [Google Scholar]
- [8].Fraioli A, Mennuni G, Grassi M, et al. SPA treatments of diseases pertaining to internal medicine. Clin Ter 2010;161:e63–79. [PubMed] [Google Scholar]
- [9].Bellometti S, Cecchettin M, Galzigna L. Mud pack therapy in osteoarthrosis. Changes in serum levels of chondrocyte markers. Clin Chim Acta 1997;268:101–6. [DOI] [PubMed] [Google Scholar]
- [10].Flusser D, Abu-Shakra M, Friger M, et al. Therapy with mud compresses for knee osteoarthritis: comparison of natural mud preparations with mineral-depleted mud. J Clin Rheumatol 2002;8:197–203. [DOI] [PubMed] [Google Scholar]
- [11].Pascarelli NA, Cheleschi S, Bacaro G, et al. Effect of mud-bath therapy on serum biomarkers in patients with knee osteoarthritis: results from a randomized controlled trial. Isr Med Assoc J 2016;18:232–7. [PubMed] [Google Scholar]
- [12].Giannitti C, De Palma A, Pascarelli NA, et al. Can balneotherapy modify microRNA expression levels in osteoarthritis? A comparative study in patients with knee osteoarthritis. Int J Biometeorol 2017;61:2153–8. [DOI] [PubMed] [Google Scholar]
- [13].Cheleschi S, De Palma A, Tenti S, et al. Mud-bath therapy regulates the expression levels of microRNA in osteoarthritis. Epigenetic contribution to explain the mechanism of action of balneotherapy. Clin Exp Rheumatol 2018;36:75–6. [Google Scholar]
- [14].Dischereit G, Fetaj S, Goronzy JE, et al. Effects of serial mud baths in osteoarthritis on parameters of functional health and cytokines: a controlled, randomised, prospective trial. Aktuel Rheumatol 2017;2:129–36. [Google Scholar]
- [15].Ortega E, Galvez I, Hinchado MD, et al. Anti-inflammatory effect as a mechanism of effectiveness underlying the clinical benefits of pelotherapy in osteoarthritis patients: regulation of the altered inflammatory and stress feedback response. Int J Biometeorol 2017;61:1777–85. [DOI] [PubMed] [Google Scholar]
- [16].Fioravanti A, Ciani O, Tenti S, et al. Balneotherapy in knee osteoarthritis: a cost/effectiveness analysis alongside an Italian randomized controlled clinical trial. Clin Exp Rheumatol 2018;33:61–2. [Google Scholar]
- [17].Ciani O, Pascarelli NA, Giannitti C, et al. Mud-bath therapy in addition to usual care in bilateral knee osteoarthritis: an economic evaluation alongside a randomized controlled trial. Arthritis Care Res 2017;69:966–72. [DOI] [PubMed] [Google Scholar]
- [18].Fioravanti A, Bacaro G, Giannitti C, et al. One-year follow-up of mud-bath therapy in patients with bilateral knee osteoarthritis: a randomized, single-blind controlled trial. Int J Biometeorol 2015;59:1333–43. [DOI] [PubMed] [Google Scholar]
- [19].Alessandro L, Altman DG, Jennifer T, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Epidemiol Biostat Public Health 2009;6:e1–34. [DOI] [PubMed] [Google Scholar]
- [20].Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539–58. [DOI] [PubMed] [Google Scholar]
- [21].Dersimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177. [DOI] [PubMed] [Google Scholar]
- [22].Sarsan A, Akkaya N, Ozgen M, et al. Comparing the efficacy of mature mud pack and hot pack treatments for knee osteoarthritis. J Back Musculoskelet 2012;25:193–9. [DOI] [PubMed] [Google Scholar]
- [23].Gungen G, Ardic F, Findikoglu G, et al. The effect of mud pack therapy on serum YKL-40 and hsCRP levels in patients with knee osteoarthritis. Rheumatol Int 2012;32:1235–44. [DOI] [PubMed] [Google Scholar]
- [24].Forestier R, Desfour H, Tessier JM, et al. Spa therapy in the treatment of knee osteoarthritis: a large randomised multicentre trial. Ann Rheumatic Dis 2010;69:660–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Fioravanti A, Iacoponi F, Bellisai B, et al. Short- and long-term effects of spa therapy in knee osteoarthritis. Am J Phys Med Rehabil 2010;89:125–32. [DOI] [PubMed] [Google Scholar]
- [26].Mahboob N, Sousan K, Shirzad A, et al. The efficacy of a topical gel prepared using Lake Urmia mud in patients with knee osteoarthritis. J Altern Complement Med 2009;15:1239–42. [DOI] [PubMed] [Google Scholar]
- [27].Fioravanti A, Giannitti C, Cheleschi S, et al. Circulating levels of adiponectin, resistin, and visfatin after mud-bath therapy in patients with bilateral knee osteoarthritis. Int J Biometeorol 2015;59:1691–700. [DOI] [PubMed] [Google Scholar]
- [28].Evcik D, Kavuncu V, Yeter A, et al. The efficacy of balneotherapy and mud-pack therapy in patients with knee osteoarthritis. Joint Bone Spine 2007;74:60–5. [DOI] [PubMed] [Google Scholar]
- [29].Tefner IK, Gaal R, Koroknai A, et al. The effect of Neydharting mud-pack therapy on knee osteoarthritis: a randomized, controlled, double-blind follow-up pilot study. Rheumatol Int 2013;33:2569–76. [DOI] [PubMed] [Google Scholar]
- [30].Espejo Antunez L, Caro Puertolas B, Ibanez Burgos B, et al. Effects of mud therapy on perceived pain and quality of life related to health in patients with knee osteoarthritis. Reumatol Clin 2013;9:156–60. [DOI] [PubMed] [Google Scholar]
- [31].Furlan AD, Malmivaara A, Chou R, et al. 2015 updated method guideline for systematic reviews in the Cochrane back and neck group. Spine 2015;40:1660–73. [DOI] [PubMed] [Google Scholar]
- [32].Klassbo M, Larsson E, Mannevik E. Hip disability and osteoarthritis outcome score. an extension of the Western Ontario and McMaster Universities Osteoarthritis Index. Scand J Rheumatol 2003;32:46–51. [DOI] [PubMed] [Google Scholar]
- [33].Liu H, Zeng C, Gao SG, et al. The effect of mud therapy on pain relief in patients with knee osteoarthritis: a meta-analysis of randomized controlled trials. J Int Med Res 2013;41:1418–25. [DOI] [PubMed] [Google Scholar]
- [34].Xiang J, Wu D, Li J. Clinical efficacy of mudpack therapy in treating knee osteoarthritis: a meta-analysis of randomized controlled studies. Am J Phys Med Rehabil 2016;95:121–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Odabasi E, Turan M, Erdem H, et al. Does mud pack treatment have any chemical effect? A randomized controlled clinical study. J Altern Complement Med 2008;14:559–65. [DOI] [PubMed] [Google Scholar]