

Abstract
Objective:
This study evaluates the motivational processes between employee occupational safety and health climates and behaviors using the Theory of Self-Determination in a sample of diverse small businesses.
Methods:
We used cross-sectional data to assess whether employee safety/health intrinsic, identified, and external motives mediate the relationship between safety/health climate and behavior.
Results:
All three types of motivation mediated the relationship between safety and health climates and behaviors.
Conclusions:
Small businesses seeking to engage employees in Total Worker Health efforts should build strong safety and health climates because of their influence on employees’ motivation to participate in health promoting and health protective programs.
Keywords: health climate, safety climate, safety motivation, health motivation, Total Worker Health
INTRODUCTION
Developing strong positive safety and health climates, broadly defined as employees’ perceptions of their organization’s value for and commitment to their safety and health, are fundamental to Total Worker Health® (TWH) (1). TWH is defined as “policies, programs, and practices that integrate protection from work-related safety and health hazards with promotion of injury and illness prevention efforts to advance worker well-being” (2). For these policies, programs, and practices to be effective, employees must perceive that they are supported and rewarded in their daily work activities; in other words, there must be strong safety and health climates. With a strong climate, employee motivation to actively participate in TWH policies, programs, and practices should be high (3).
Safety and health climates
In 1975, Schneider argued that organizational climate research was unfocused and needed to evaluate “a climate for something” (4). In other words, organizational climate constructs should reflect employees’ perceptions about specific strategic priorities of the organization. Over 40 years later, Schneider (5) reflected that organizational climate researchers have heeded this call. Researchers have evaluated several different organizational climate constructs (e.g., climate for justice, service, innovation, trust), with safety climate being the most heavily studied climate construct in occupational health research.
Since Zohar’s (6) initial investigation of safety climate, hundreds of studies, summarized in multiple meta-analyses, have supported the basic idea that a stronger positive safety climate is associated with higher levels of safety performance, as well as reductions in other accident and injury outcomes (3, 7, 8). Although researchers have proposed a wide array of safety climate definitions, measurement models, and relationships with other variables, there is relative lack of consensus on the nature of safety climate (9) with past studies having investigated many potential dimensions of safety climate. However, management commitment to safety has been the most ubiquitous aspect of safety climate and is regarded as the core feature of safety climate (10). Thus, safety climate reflects employees’ perceptions of their organization’s commitment to workplace safety programs and their beliefs about how much their organization values having a safe workplace. These perceptions develop over time as employees observe what safety practices are rewarded and supported by the company.
Schneider (5) also noted a need for organizational climate researchers to begin to understand multiple organizational climates in tandem. Within a TWH framework, health climate would be considered to be a second important climate to consider along with safety climate and how they are related to each other and to motivation and behavior. Following Zweber et al.’s (11) definition, we define health climate to be employee perceptions of active support from management for the physical and psychological well-being of employees. Although health climate research can be traced at least back to the 1990s (12, 13), relatively few studies have investigated health climate and still fewer have investigated both health and safety climates together. Zweber and colleagues (11) argued that health and safety climates are conceptually distinct as each may be viewed and prioritized differently by organizations. Safety climate reflects policies, procedures, and practices to comply with governmental and company rules with the aim of preventing work-related injury, illness, and fatality whereas health climate reflects policies, procedures, and practices to promote employees’ personal health and well-being. Mearns and colleagues (14) found that, although safety and health climates were moderately correlated (r = .50), only safety climate was associated with higher employee commitment and better safety compliance in multivariate analyses with both climate measures in the model. Zweber et al. (11) also found safety and health climates were moderately correlated (r = .66) but only health climate predicted job stress and overall health when both climates were analyzed together. Finally, using factor analysis, Sawhney and colleagues (15) found that health and safety climates are correlated (r = .55) but are empirically distinct. This literature suggests that safety and health climates are related but distinct concepts with differential patterns of relationships with outcomes. However, there is considerable variability between studies in the climate measures used and in the health- and safety-focused outcomes of interest, warranting further investigation of the relationships between safety climate and health climate.
Safety/Health Motivation
Efforts to understand the impact of safety/health climate need to be informed by an understanding of the psychological mechanisms that connect climate perceptions to employee outcomes. The safety literature has arrived at some level of consensus about the important role of motivation in the climate-behavior relationship. In a series of studies, Neal and Griffin (16–18) demonstrated that safety motivation partly explained the relationship between safety climate and safety performance – a relationship subsequently confirmed by meta-analytic path analyses (3). To our knowledge, the relationships among health climate, motivation, and behavior has not received attention in prior research. However, we propose that the same underlying model may explain the relationship between health climate, health motivation, and health behavior.
Although the importance of motivation in the climate-performance relationship is well accepted, an understudied question in the climate literature concerns what specific motivational processes influence employees’ safe behavior. Most safety motivation measures capture employees’ “total” motivation with questions that generally focus on how important safety is to the employee (19). Although such measures fit the general model of motivation as a mediator of the climate-behavior relationship, they do not reflect current developments in motivational theory which acknowledge that employees have multiple potential motives for workplace behavior, including both health- and safety-related behavior.
Self Determination Theory (SDT) makes a critical distinction between autonomous and controlled motivation (20, 21). Autonomous motivation reflects people’s voluntary engagement in activities that they can choose willingly (i.e., they are self-determined) and typically that they find interesting, satisfying, or pleasurable. The most autonomous form of motivation is intrinsic motivation, which reflects employees’ inherent interest in or satisfaction with safety/health. Controlled motivation reflects motivation to engage in activities based on contingencies that guide the individual’s behavior. The most controlled form of motivation is extrinsic regulation, often referred to as extrinsic motivation, which reflects the desire to perform a behavior because of contingent rewards or punishments. Extrinsic regulation is arguably the most consistent with Zohar’s model of safety climate which focuses on employees expected outcomes of behaving safely (22). Employees who perceive a stronger positive health/safety climate are more likely to believe that healthy/safe behavior is desired and even rewarded by their organization.
SDT proposes three additional types of external motives that reflect comparatively more internalized regulation: introjected, identified, and integrated, each of which refers to people performing behavior because the behavior reflects some internalized attitude, value, or regulatory structure (20). In this study, we focus on identified regulation which involves the belief that “a safe work environment is important and accept that performing safety [and health] activities are necessary to achieve that goal” (23).
Although SDT is perhaps one of the most heavily-cited models of work motivation, past peer reviewed literature examining the relationship between the components of SDT and workplace safety outcomes is sparse. Burstyn et al. (24) found that autonomy supportive safety inspectors obtained higher compliance rates, but they did not measure other aspects of the SDT model. Mariani et al. (19) found support for a SDT-based measure that distinguished the five types of safety motivations in confirmatory factor analyses, but did not link the different motivational measures to safety outcomes. Scott et al. (23) developed another safety motivation measure based on SDT and found both confirmatory factor analytic support for the distinctiveness of the dimensions and differential relationships of the dimensions with safety compliance and participation behaviors. Interestingly, in their study, extrinsic safety motivation did not predict either safety compliance or participation, rather, more autonomous types of motives did. This highlights the need to study other forms of safety motivation. Scott et al. (23) note that this finding is consistent with past SDT literature showing that more autonomous forms of motivation tend to be better predictors of behavior. Finally, to our knowledge, no research has applied SDT to understand the consequences of health climate.
Hypotheses
Our study builds on this prior literature in several ways. First, even though past literature supports the relationship between safety climate and safety motivation, no studies that we are aware of directly test the relationship between safety/health climates and the multiple safety/health motives described by SDT. Second, we partially replicate Scott et al.’s (23) findings by testing the link between three forms of safety motivation (extrinsic, identified, and intrinsic) and safety participation behaviors. This is potentially important in helping to explain the mechanisms that link safety climate to safety performance and other outcomes. Whereas extrinsic motivation may account for the effects of safety/health climate (22), other motives may be more important (23). So, further evidence is clearly needed to inform which motives account for safety behavior. Third, we extend past literature by examining relationships between health climate, health motivation and health participation (i.e., in wellness programs).
Finally, very little safety climate research and no known health climate research has examined the small business setting. Small businesses often lack the resources to manage safety and health issues in the same manner as larger organizations (25). Thus, it is not clear whether safety/health climate research in larger organizations can be generalized to the unique context of small businesses – an issue that is especially important for designing interventions to serve the needs of the small business community.
Hypothesis 1: Employees who report more positive perceptions of safety climate will report higher levels of external (H1a), intrinsic (H1b), and identified (H1c) safety motivation.
Hypothesis 2: Employees who report more positive perceptions of health climate will report higher levels of external (H2a), intrinsic (H2b), and identified (H2c) health motivation.
Hypothesis 3: Employees who report higher levels of external (H3a), intrinsic (H3b), and identified (H3c) safety motivation will report greater safety participation.
Hypothesis 4: Employees who report higher levels of external (H4a), intrinsic (H4b), and identified (H4c) health motivation will report greater safety participation.
Hypothesis 5: The relationship between safety climate and safety participation will be mediated by external (H5a), intrinsic (H5b), and identified (H5c) safety motivation.
Hypothesis 6: The relationship between health climate and health participation will be mediated by external (H6a), intrinsic (H6b) and identified (H6c) health motivation.
Method
Sample
The sample of workers in the present study is a part of the Small+Safe+Well (SSWell) study conducted by the Center for Health, Work & Environment (CHWE), a National Institute for Occupational Safety and Health (NIOSH) Center of Excellence for Total Worker Health® (TWH) (1). The SSWell study examined how small organizations support their employees’ workplace safety, health and well-being and how employees perceive their organization’s safety and health climates. SSWell aims to assess TWH workplace practices and climate, and ultimately assess impact of interventions on employees’ health, safety, and well-being. As part of the SSWell study, each business completes an annual business-level assessment of their health and safety policies and programs. Their employees are invited to take an annual health and safety culture survey. For this study, we used employee survey data collected from April 2017 to May 2018. This study was approved by the Colorado Multiple Institutional Review Board.
There were a total of 1,052 individual employee survey respondents representing 36 participating organizations. About half of the individuals worked in the service industry (53%, N = 558) with the clear majority in the urban regions of Colorado (89%, N = 939). The median business size in this study was 139 (Range: 4 to 430). Respondents were on average 40 years old (SD: 13 years), college educated (63%) non-Hispanic white (79%), women (64%). Most were full-time employees (84%) with 42% having supervisory duties. A full summary of participating businesses and employees can be found in Table 1. Table 1 also shows business-level demographic information, industry, and region, obtained from the Health Links Healthy Workplace Assessment™ that each business completed as part of the SSWell study (25).
Table 1.
Demographic information, N=1052
| Mean | SD | N | % | |
|---|---|---|---|---|
| Organizational Level | ||||
| Industry | ||||
| Construction | 140 | 13.31 | ||
| Manufacturing | 35 | 3.33 | ||
| Public administration | 54 | 5.13 | ||
| Retail and wholesale trade | 140 | 13.31 | ||
| Services | 558 | 53.04 | ||
| Transportation | 125 | 11.88 | ||
| Region | ||||
| Urban | 939 | 89.26 | ||
| Rural | 113 | 10.74 | ||
| Number of employees | 175 | 131.66 | ||
| Employee Level | ||||
| Age | 40.30 | 13.37 | ||
| Gender | ||||
| Male | 320 | 35.83 | ||
| Female | 571 | 63.94 | ||
| Other | 2 | 0.22 | ||
| Race | ||||
| White | 833 | 79.18 | ||
| Black or African American | 23 | 2.19 | ||
| Asian | 20 | 1.90 | ||
| Native American or Alaskan Native | 16 | 1.52 | ||
| Native Hawaiian or Other Pacific Islander | 7 | .67 | ||
| Ethnicity | ||||
| Hispanic or Latino or Spanish Origin | 96 | 10.80 | ||
| Not Hispanic or Latino or Spanish Origin | 793 | 89.20 | ||
| Education | ||||
| Did not complete high school | 8 | 1.02 | ||
| High school diploma or GED | 72 | 9.18 | ||
| Some college or 2-year degree | 207 | 26.40 | ||
| 4-year college degree | 338 | 43.11 | ||
| Graduate or professional degree | 159 | 20.28 | ||
| Household Income | ||||
| Below $20,000 | 45 | 5.80 | ||
| $20,001 – $30,000 | 50 | 6.44 | ||
| $30,001 – $40,000 | 71 | 9.15 | ||
| $40,001 – $50,000 | 72 | 9.28 | ||
| $50,001 – $60,000 | 63 | 8.12 | ||
| $60,001 – $70,000 | 55 | 7.09 | ||
| $70,001 – $80,000 | 63 | 8.12 | ||
| $80,001 – $90,000 | 62 | 7.99 | ||
| $90,001 – $100,000 | 58 | 7.47 | ||
| More than $100,000 | 237 | 30.54 | ||
| Job Level | ||||
| Supervisor | 373 | 41.73 | ||
| Non-supervisor | 521 | 58.27 | ||
| Job Tenure | 5.18 | 6.86 | ||
| Type of Work | ||||
| Full-time | 750 | 84.27 | ||
| Part-time | 140 | 15.73 | ||
| Work hours | 38.90 | 13.23 | ||
| Salary paid | 460 | 51.74 | ||
| Hourly paid | 429 | 48.26 | ||
| Contractor or consultant | 39 | 4.38 | ||
| Shift work | 146 | 16.44 |
Measures
Employee Health and Safety Culture Survey.
The SSWell research team administers an annual employee health and safety culture survey to employees of all participating organizations using the REDCap electronic data capture tool (26). One organization requested a paper survey; those data were later entered into the REDCap database manually. Employees who completed the survey were offered the opportunity to put their email addresses into a raffle to win one of fifteen $100 gift cards via a separate online database. No identifying information was collected in the survey, and the employer was blinded to the individual level responses.
The employee health and safety culture survey is a comprehensive survey used to understand employees’ perceptions of their organizational environment regarding safety and health. Demographic information is also collected in the survey. For this study, we drew from climate, motivation, and behavior constructs measured in the employee survey.
Safety and Health Climates.
For safety climate, we asked employees six questions about their organization’s value of, and commitment to, safety. Each question was on a five-point scale from strongly disagree to strongly agree. Lee et al. (27) developed this safety climate measure based on the work of Zohar and Luria (28). We adapted the measure to our study by changing the preface of each question to “My organization…” instead of “Top management…” An example item is, “My organization reacts quickly to solve the problem when told about safety concerns.”
Similarly, we also asked employees about their organization’s health climate, each on a five-point Likert scale from strongly disagree to strongly agree (4 items). We used the organizational health climate factor from Zweber et al. (11). An example item is, “When management learns that something about our work or the workplace is having a bad effect on employee health or well-being, then something is done about it.”
Safety and Health Motivations.
We asked each employee about their motivations towards workplace safety and worksite wellness. Conchie et al. (29) developed a safety motivation measure based on Guay’s (30) situational motivation scale: intrinsic – “interesting”, identified – “good for me”, and extrinsic – “required to do it”. We used this safety motivation measure to evaluate intrinsic safety motivation (e.g., “I think worksite wellness is interesting,” 3 items), identified regulation safety motivation (e.g., “I’m doing it for my own good,” 3 items), and external regulation safety motivation (e.g., “I’m supposed to do it,” 3 items). These questions were prefaced with “Safety means preventing you from being injured or made ill on the job. I engage in workplace safety because…” We also created a corresponding worksite wellness motivation measure to evaluate intrinsic health motivation (3 items), identified regulation health motivation (3 items), and external regulation health motivation (3 items). These questions were prefaced with “Worksite wellness refers to policies and programs that help promote your physical and mental health. I engage in worksite wellness because…” All questions were rated on a five-point scale from strongly disagree to strongly agree.
Safety and Health Participatory Behaviors.
We used Griffin and Neal’s (16) three-item safety participatory behavior scale. These questions were prefaced with “Safety means preventing you from being injured or made ill on the job.” An example question is, “I promote the safety program within the organization.” We also created a corresponding three-item health participatory behavior measure. These questions were prefaced with “Worksite wellness refers to policies and programs that help promote your physical and mental health.” An example question is, “I voluntarily carry out tasks or activities that help to improve the worksite wellness program.” All questions were rated on a five-point scale from strongly disagree to strongly agree.
Covariates
We included additional covariates from both the health and safety culture survey and the Health Links Healthy Workplace Assessment. From the culture survey, we included job tenure (i.e., number of years with current company) and whether they were in a management role. From the Health Links Healthy Workplace Assessment, we included a categorical variable for industry and a continuous variable for business size (i.e., number of employees).
Statistical analysis
Prior to testing our hypotheses, we conducted a series of confirmatory factor analyses investigating the empirical distinctiveness of our measures. We used Stata version 14.2 (College Station, TX) for these analyses and compared our expected ten-factor structure (i.e., safety climate, health climate, 3 factors each for the safety and health motivations, safety participatory behaviors, and health participatory behaviors) against a series of more parsimonious models. These alternative models included a one-factor model where all items are represented by one construct, a two-factor model where all safety items are represented by one construct and all health items represented by one construct, a three-factor model where climate, motivation, and behavior constructs each have their own factor, and, finally, a six-factor model including safety climate, health climate, safety motivation, health motivation, safety participatory behaviors, and health participatory behaviors.
Support for the ten-factor model would show that participants distinguish both the multiple types of climate, the multiple motivational, and multiple behavior constructs. We used the following goodness of fit indices to identify the model that best fit the data: root-mean-squared error of approximation (RMSEA) (<0.08 indicates adequate fit), comparative fit index (CFI) (>0.90 indicates adequate fit), standardized root mean square residual (SRMR) (<0.08 indicates adequate fit), chi-square test, and chi-square difference test between the hypothesized eight factor model and the four nested models (31, 32).
We assessed each of our hypotheses by using the PROCESS SPSS macro developed by Hayes (33). The macro is an ordinary least squares regression path analysis tool that can be used to estimate direct and indirect effects of mediation models using a 5000-sample bootstrapping technique. The macro estimates the path from climate to motivation (a), path from motivation to participatory behaviors (b), the direct effect of climate on participatory behaviors (c’), the total indirect effect of climate on participatory behaviors through motivation (ab), and the total effect of climate on participatory behaviors (c) (see Figure 1). In total, we estimated six mediation models using the macro. All models controlled for tenure, whether they were a management role, business size, and industry.
Figure 1.
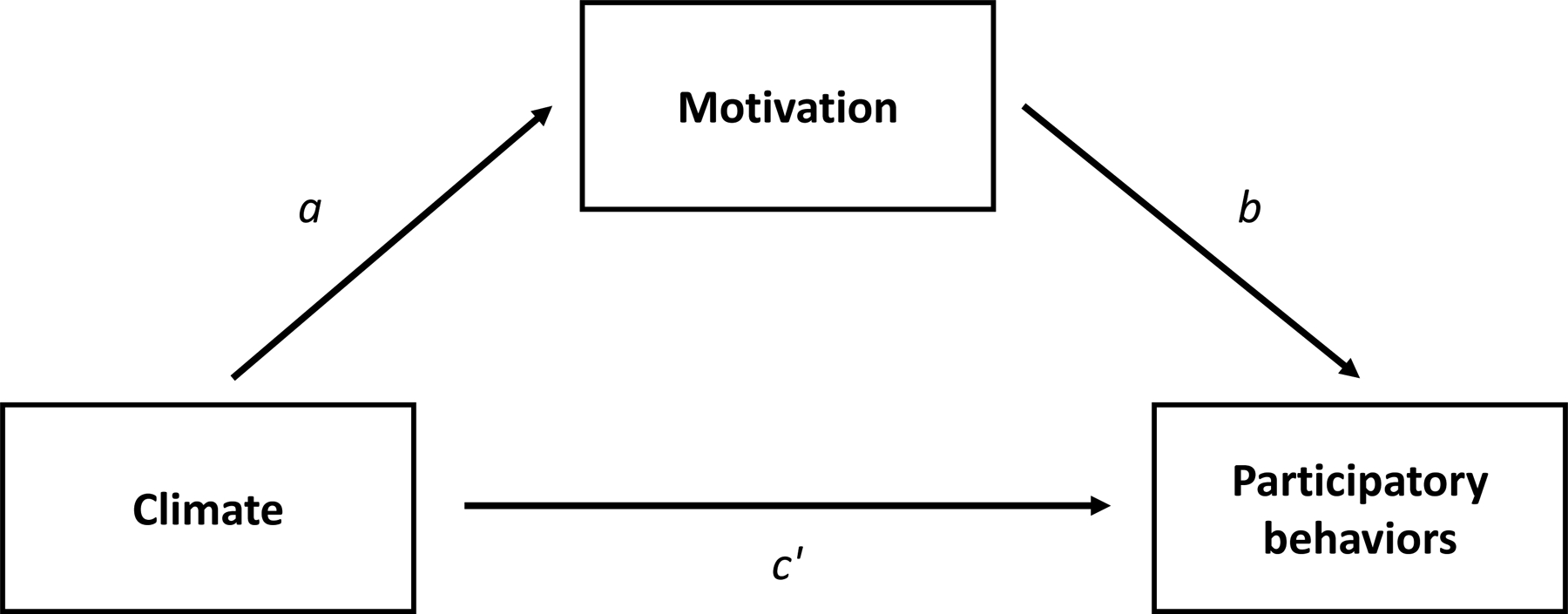
Representation of the simple mediation model tested to demonstrate the relationship between climate and participatory behaviors through motivation. Note the total effect (c) = c’ + ab.
Results
Confirmatory factor analysis
Our confirmatory factor analysis demonstrated that there are ten conceptually distinct factors related to safety and health climates, motivations, and behaviors (see Table 2). All of the fit indices indicated adequate support for our hypothesized model as the results of the alternative models yielded poorer fit to the data based on a chi-square difference test comparing alternative models to our hypothesized model (p < .01). The standardized loadings of each indicator to its hypothesized construct ranged from 0.66 to 0.94: safety climate ≥ 0.75, health climate ≥ 0.72, safety motivation – intrinsic ≥ 0.67, safety motivation – identified ≥ 0.66, safety motivation – external ≥ 0.71, health motivation – intrinsic ≥ 0.76, health motivation – identified ≥ 0.74, health motivation – extrinsic ≥ 0.79, safety participatory behavior ≥ 0.78, and health participatory behavior ≥ 0.88.
Table 2.
Confirmatory factor analysis – goodness of fit indices
| Model | χ2 | Df | χ2diff | Dfdiff | CFI | SRMR | RMSEA |
|---|---|---|---|---|---|---|---|
| #1 Alternative 1 Factor | 12349 | 594 | 10526 | 45* | 0.40 | 0.14 | 0.17 |
| #2 Alternative 2 Factors | 10764 | 599 | 8941 | 50* | 0.45 | 0.16 | 0.16 |
| #3 Alternative 3 Factors | 7361 | 557 | 5538 | 8* | 0.64 | 0.11 | 0.13 |
| #4 Alternative 6 Factors | 4269 | 545 | 2446 | 4* | 0.81 | 0.09 | 0.10 |
| Hypothesized 10 Factors | 1823 | 549 | - | - | 0.94 | 0.04 | 0.06 |
CFI: Comparative fit index, SRMR: Standardized root mean square residual, RMSEA: Root mean square error of approximation. Alternative 1 factor model: All items are represented by one construct. Alternative 2 factor model: All safety items are represented by one construct and all health items represented by one construct. Alternative 3 factor model: Climate, motivation, and behavior constructs. Alternative 6 factor model: safety climate, health climate, safety motivation, health motivation, safety participatory behaviors, health participatory behaviors.
p < 0.01
Descriptive statistics, correlations, and Cronbach’s alphas (α) for all scales are reported in Table 3. All reliability estimates exceeded 0.80 and all correlations were significant in the expected direction. Consistent with our expectations, safety climate was positively correlated with all three kinds of safety motivation (all r’s 0.25–0.27) and safety participatory behaviors (r = 0.44). Similarly, health climate was positively correlated with all three kinds of health motivation (all r’s 0.24–0.32) and health participatory behaviors (r = 0.42). Safety climate and health climate were moderately, positively correlated (r = 0.64). Finally, the correlations among the different types of motives were small to moderate, aside from the relatively large correlation between identified and intrinsic health motivation (r = 0.81). These findings support the distinctiveness of the safety and health motives we investigated.
Table 3.
Means, standard deviations, reliabilities, and correlations of safety and health climates, motivations, and participatory behaviors
| Mean | SD | Safety Climate | Health Climate | Safety Intrinsic Motivation | Safety identified regulation motivation | Safety external motivation | Health Intrinsic Motivation | Health Identified Regulation Motivation | Health External Motivation | Safety participatory behavior | Health participatory behavior | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Safety Climate | 3.84 | .83 | (.93) | .64 | .27 | .27 | .25 | .28 | .26 | .19 | .44 | .34 |
| Health Climate | 3.91 | .83 | (.89) | .28 | .23 | .18 | .31 | .32 | .25 | .40 | .42 | |
| Safety Intrinsic Motivation | 3.78 | .70 | (.82) | .62 | .34 | .54 | .45 | .28 | .53 | .33 | ||
| Safety Identified Regulation Motivation | 4.34 | .59 | (.83) | .48 | .42 | .54 | .25 | .44 | .22 | |||
| Safety External Motivation | 3.95 | .77 | (.82) | .25 | .31 | .56 | .32 | .15 | ||||
| Health Intrinsic Motivation | 4.03 | .70 | (.89) | .81 | .23 | .29 | .50 | |||||
| Health Identified Regulation Motivation | 4.26 | .64 | (.87) | .28 | .28 | .44 | ||||||
| Health External Motivation | 3.47 | .96 | (.90) | .29 | .27 | |||||||
| Safety Participatory Behavior | 3.93 | .78 | (.81) | .50 | ||||||||
| Health Participatory Behavior | 3.54 | .88 | (.93) |
Note. Reliabilities (Cronbach alpha) are along the diagonal. Correlations between measures are above the diagonal. All correlations have a p-value of <0.01.
Mediation model results for safety
Table 4 presents the results of the mediation analyses for safety. Consistent with hypothesis 1, we observed that safety climate was related to all three types of safety motivation (intrinsic: β = 0.23, 95% CI = 0.17, 0.28, identified: β = 0.19, 95% CI = 0.14, 0.24, extrinsic: β = 0.24, 95% CI = 0.18, 0.30). Additionally, we observed that each type of safety motivation was related to safety participation behaviors, which supports hypothesis 3 (intrinsic: β = 0.50, 95% CI = 0.43, 0.56, identified: β = 0.46, 95% CI = 0.38, 0.53, extrinsic: β = 0.23, 95% CI = 0.17, 0.29). Finally, the indirect effects of safety climate on safety participation behaviors through the three types of safety motivation were all significant - intrinsic: β = 0.11, 95% CI = 0.08, 0.15, identified: β = 0.09, 95% CI = 0.06, 0.12, and extrinsic: β = 0.05, 95% CI = 0.03, 0.08. This supports hypothesis 5, which stated that safety climate and safety participation would be mediated by all three types of motives.
Table 4.
Results of mediation analysis demonstrating safety climate’s (independent variable) relationship to safety participation behaviors (outcome) via three types of safety motivation (mediators)
| Estimate | SE | [95% CI] | |
|---|---|---|---|
| Mediator: Internal safety motivation | |||
| Mediator | |||
| Safety climate (a path) | 0.23 | 0.03 | [0.17, 0.28] |
| Outcome | |||
| Mediator to outcome (b path) | 0.50 | 0.03 | [0.43, 0.56] |
| Total effect of safety climate on outcome (c path) | 0.42 | 0.03 | [0.36, 0.48] |
| Direct effect safety climate on outcome (c’ path) | 0.31 | 0.03 | [0.25, 0.36] |
| Total indirect effect of safety climate on outcome through mediator (ab path) | 0.11 | 0.02 | [0.08, 0.15] |
| Mediator: Identified safety motivation | |||
| Mediator | |||
| Safety climate (a path) | 0.19 | 0.03 | [0.14, 0.24] |
| Outcome | |||
| Mediator to outcome (b path) | 0.46 | 0.04 | [0.38, 0.53] |
| Total effect of safety climate on outcome (c path) | 0.42 | 0.03 | [0.36, 0.48] |
| Direct effect safety climate on outcome (c’ path) | 0.33 | 0.03 | [0.28, 0.39] |
| Total indirect effect of safety climate on outcome through mediator (ab path) | 0.09 | 0.01 | [0.06, 0.12] |
| Mediator: External safety motivation | |||
| Mediator | |||
| Safety climate (a path) | 0.24 | 0.03 | [0.18, 0.30] |
| Outcome | |||
| Mediator to outcome (b path) | 0.23 | 0.03 | [0.17, 0.29] |
| Total effect of safety climate on outcome (c path) | 0.42 | 0.03 | [0.36, 0.48] |
| Direct effect safety climate on outcome (c’ path) | 0.36 | 0.03 | [0.30, 0.42] |
| Total indirect effect of safety climate on outcome through mediator (ab path) | 0.05 | 0.01 | [0.03, 0.08] |
Note. All models are controlled for tenure, management role, industry, and business size. SE = Standard error. CI = Confidence interval.
p<0.0001
Mediation model results for health
Table 5 presents the results of the mediation analyses for health. Consistent with hypothesis 2, we observed that health climate was related to all three types of health motivation (intrinsic: β = 0.25, 95% CI = 0.19, 0.30, identified: β = 0.24, 95% CI = 0.19, 0.29, extrinsic: β = 0.29, 95% CI = 0.21, 0.37). Additionally, we observed that each type of health motivation was related to health participation behaviors, which supports hypothesis 4 (intrinsic: β = 0.50, 95% CI = 0.43, 0.58, identified: β = 0.46, 95% CI = 0.37, 0.54, extrinsic: β = 0.17, 95% CI = 0.11, 0.22). Finally, the indirect effects of health climate on health participation behaviors through the three types of health motivation were all significant - intrinsic: β = 0.13, 95% CI = 0.10, 0.17, identified: β = 0.11, 95% CI = 0.08, 0.15, and extrinsic: β = 0.05, 95% CI = 0.03, 0.07. This supports hypothesis 6, which stated that health climate and health participation would be mediated by all three types of motives.
Table 5.
Results of mediation analysis demonstrating health climate’s (independent variable) relationship to health participation behaviors (outcome) via three types of health motivation (mediators)
| Estimate | SE | [95% CI] | |
|---|---|---|---|
| Mediator: Internal health motivation | |||
| Mediator | |||
| Health climate (a path) | 0.25 | 0.03 | [0.19, 0.30] |
| Outcome | |||
| Mediator to outcome (b path) | 0.50 | 0.04 | [0.43, 0.58] |
| Total effect of health climate on outcome (c path) | 0.45 | 0.03 | [0.38, 0.51] |
| Direct effect health climate on outcome (c’ path) | 0.32 | 0.03 | [0.25, 0.38] |
| Total indirect effect of health climate on outcome through mediator (ab path) | 0.13 | 0.02 | [0.10, 0.17] |
| Mediator: Identified health motivation | |||
| Mediator | |||
| Health climate (a path) | 0.24 | 0.03 | [0.19, 0.29] |
| Outcome | |||
| Mediator to outcome (b path) | 0.46 | 0.04 | [0.37, 0.54] |
| Total effect of health climate on outcome (c path) | 0.45 | 0.03 | [0.38, 0.51] |
| Direct effect health climate on outcome (c’ path) | 0.34 | 0.03 | [0.27, 0.40] |
| Total indirect effect of health climate on outcome through mediator (ab path) | 0.11 | 0.02 | [0.08, 0.15] |
| Mediator: External health motivation | |||
| Mediator | |||
| Health climate (a path) | 0.29 | 0.04 | [0.21, 0.37] |
| Outcome | |||
| Mediator to outcome (b path) | 0.17 | 0.03 | [0.11, 0.22] |
| Total effect of health climate on outcome (c path) | 0.45 | 0.03 | [0.38, 0.51] |
| Direct effect health climate on outcome (c’ path) | 0.40 | 0.03 | [0.33, 0.47] |
| Total indirect effect of health climate on outcome through mediator (ab path) | 0.05 | 0.01 | [0.03, 0.07] |
Note. All models are controlled for tenure, management role, industry, and business size. SE = Standard error. CI = Confidence interval. All p-values are less than 0.0001.
Discussion
With the field of Total Worker Health gaining momentum (34), it is important to consider how businesses’ adoption of health promotion and health protection practices influence workforce health, safety, and well-being. An important call for research has been specifically made to understand worker engagement and empowerment in TWH as well as to understand how a TWH strategy may affect employee health, safety, and well-being (35–37). This is especially important in small businesses since they often receive less attention from the research community and often lack the resources to implement TWH intervention efforts (38). This study responded to that call by examining the influence of both safety climate and health climate on safety and health participatory behaviors as well as the mediating role of multiple types of motives in those relationships among small businesses. Our findings showed that each form of climate was related to the corresponding participatory behavior and that all three forms of motivation mediated that relationship. We discuss each of these findings in turn along with further implications for research and practice.
Contributions
An understudied but growing area of interest related to TWH programs concerns how multiple types of climate relate to various behavioral outcomes. Our findings make a few contributions to this literature. First, we extended a large body of research linking safety climate to safety outcomes, in this case, self-reported safety participation. Although many studies have examined safety climate – safety behavior relationships (16–18), very few studies have examined this relationship in the setting of small businesses. Our findings support the idea that the safety climate – motivation – participation relationship studied in past literature generalizes to the small business setting, providing small business leaders with an evidence base from which to consider safety interventions.
Second, organizations of all sizes experience challenges with engaging employees in health promotion efforts. Although health climate should influence employees’ efforts at engaging in healthy behaviors, very little literature has investigated this issue and the results to date, have been mixed (11, 14, 15). Our study contributes to this literature by showing that, specifically in the small business context, organizations with more favorable climates promoting employee health also tend to have employees who are more likely to engage in healthy behaviors. Importantly, our confirmatory factor analysis findings show that even though safety and health climates are moderately related (r = .64), they can be empirically distinguished. This finding reinforces the value of studying health climate in addition to safety climate.
Third, we applied SDT to describe three distinct forms of safety/health motives: intrinsic, identified, and extrinsic. Each of these forms of motivation was associated both with the corresponding form of health/safety climate and the corresponding health/safety participation outcome. In the safety climate literature, while many studies have examined the role of safety motivation in predicting outcomes, most of that literature has not distinguished among specific kinds of motivational processes (23). Our confirmatory factor analyses supported the proposition that each of the three motives we investigated are empirically distinct from one another. In fact, with the exception of the fairly large relationship between intrinsic and identified motivation (r = .64 for safety and .81 for health) most of the relationships among the motives were small to moderate, indicating that employees can have multiple distinct forms of motivation for working safely and for engaging in health-promoting behaviors. This is an important theoretical contribution to the occupational safety and health literature both because it supports the assertion that SDT helps explain why employees might differ in their motives to be safer or healthier.
The SDT motive findings also provide an important extension to climate literature. Zohar’s (22) theorizing emphasizes the idea that the motivational effects of safety climate are through behavior-outcome contingencies – the idea that employees engage in safety behavior because of an expectation of positive outcomes of their behavior. SDT suggests a more nuanced view that there are a variety of distinct motivational processes that influence safety behavior, including the receipt of external rewards (extrinsic), the inherent pleasure of working safety (intrinsic), and the sense that safety is personally important (identified). Moreover, our study is the first to our knowledge to apply this conceptual distinction to health motivation specifically in climate-related research. Thus, for both safety and health, our findings suggest the need for future theorizing to incorporate a “multiple motives framework” to understand safe and healthy behavior at work.
Future Research
In terms of future research, we offer a couple of suggestions. First, we studied safety participation but not compliance behavior, which is another important aspect of safety behavior that could potentially have differential relationships with the various motives. We focused on participatory behaviors because their discretionary nature makes them especially relevant to the study of different types of employee motives. Future research should consider whether the same motives predict compliance-related outcomes. These may pertain more to the more compliance-based safety behaviors than to health, but as organizations increase their efforts to incentivize employees to be healthier, such as through wellness programs that link the costs of insurance to employees’ health status, the multiple motives framework may be especially important.
Second, it is important to note that we did not investigate the full range of motivations described by STD. For example, SDT describes introjected motivation as employees’ desire to perform a task out of a desire to meet their own self-worth or avoid shame. Thus, employees might engage in safe behavior out of a desire to avoid the sense of guilt that might come with behaving unsafely rather than out of a genuine value for safety. Similarly, SDT describes integration as motivation that comes from an activity being congruent with the individual’s values and belief systems. Employees with integrated motives might engage in health behavior out of a sense that being healthy is a strong part of their identity. Given that these and the three forms of SDT motives we did study all would be expected to predict the same outcomes, future research should investigate the extent to which each motive incrementally contributes to safety and health-related outcomes as well as whether they all serve as mediators of the climate-outcome relationship. It also might be useful to examine whether the different motives interact in the prediction of safety/health outcomes. For example, the effects of rewards/extrinsic safety motivation on participation might be even stronger for those who believe that safety is important. Alternately, the effects of safety rewards might only be present for those who value safety. Similarly, regarding health motivation, extrinsic rewards to encourage healthy behavior might only be effective for those who have internalized values about the importance of health.
Although not the focus of our hypotheses, we noted that the corresponding climate-outcome relationships (e.g., safety climate with safety participation) were similar in magnitude as the non-corresponding climate-outcome relationships (e.g., safety climate with health participation). This suggests the importance of future research investigating “cross-over” type effects such as safety climate predicting health outcomes. For example, safety and health climates might interact in their prediction of some outcomes, such that the relationships are strongest when both forms of climate are strong and positive. Similarly, it may be the case that the relationship between the climate measures themselves and the non-corresponding climate-outcome relationships are explained by a general sense that the organization cares about its employees. Thus, effects associated with specific climate constructs may in part represent effects of employees’ perceived organizational support - general perceptions about the extent to which their organization cares about their well-being (39).
Practical implications
Based on this study, we would make the following recommendations to small business owners who seek to create TWH programs with high employee engagement. First, employers must assess their company’s commitment to safety and health by asking for their employees’ perspective. Based on the literature, small businesses can work to improve these perceptions by building leadership capacity amongst company decision makers. These key leaders must facilitate the vision, role modeling, resource allocation, etc. to can motivate and guide businesses as they implement safety and health strategies (1, 40). Second, in addition to using extrinsic rewards/incentives to encourage employee participation, employers should incorporate participatory practices when developing and implementing ways to promote safety and health (37). Participatory interventions in which groups of employees are given a sense of ownership and encouraged to actively engage in the process of finding ways to promote safety and health will increase employee safety/health motives to participate in these initiatives (20, 21).
Strengths & Limitations
There are a few potential limitations to our work. First, our research relied on cross-sectional data. Thus, we cannot make causal claims about the relationships observed in the study. The various safety/health motives may differentially relate to climate or to safety/health outcomes over time.
Second, both a potential strength and weakness of our study is that we sampled from a broad array of employers. This is a strength in the sense that it enhances the generalizability of our findings to our target population of small businesses. However, it is also the case that businesses differ in the extent to which they have safety and health concerns, and therefore potentially differ in the relevance of safety/health participation or in the influence of climate and motivation on such behaviors. We addressed this to a degree by controlling for management role, business size, and industry in our analyses.
Third, given the practical constraints of our research, we relied on a short version of the climate measures. This was necessary so that survey length did not discourage small business leaders or their employees from participating. But, it does raise the question of whether the brief measures were missing important content. We assessed the “core” dimension captured in most climate research – organizational commitment to and value of safety/health. However, climate studies use a wide array of different climate dimensions, including, for example, distinctions between top management and front line supervisors, “generic” climate assessments versus those tailored to a particular occupation/industry, and additional dimensions such as the presence of appropriate training and coworker support for safety (9). Thus, while our climate measure effectively captured the central issues in safety/health climate assessment, we were not able to assess the value of these additional considerations in climate measurement.
Finally, our research relied on self-reported assessments. This raises potential concerns about whether common method biases influenced the relationships among several of our measures of interest. Common method variance is a frequently mentioned concern in organizational research, although many authors conclude that its potential biasing effects on studies may be overstated (41). Although climate research heavily relies on self-reported data gathered from standardized questionnaires, it may be valuable to consider other measurement strategies such as qualitative approaches or ratings of climate from other constituencies such as supervisors or customers/clients.
Conclusion
Organizational climate research provides an important opportunity for developing empirically supported recommendations to guide Total Worker Health interventions. Such efforts are especially important in small businesses where occupational health in general and Total Worker Health in particular, have received limited attention. Safety and health climates are two important types of strategic climates that can inform these efforts. Our findings show that both of these climates are associated with three types of motives – intrinsic, identified, and extrinsic – that influence safety/health-related behavior. This finding builds on a small literature investigating multiple motives for employee safety and health. Future efforts should be undertaken to develop a more comprehensive understanding of how and why safety and health climates influence safety and health behavior.
Acknowledgments
This publication was supported by the following grants K01OH011726 and U19 OH 011227 and funded by the Centers for Disease Control and Prevention/National Institute for Occupational Safety and Health. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
Footnotes
COI: none declared
References
- 1.Schwatka N, Tenney L, Dally M, et al. Small business Total Worker Health: A conceptual and methodological approach to facilitating organizational change. Occupational Health Science. 2018;2:25–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tamers S, Chosewood L, Childress A, Hudson H, Nigam J, Chang C. Total Worker Health 2014–2018: The Novel Approach to Worker Safety, Health, and Well-Being Evolves. Int J Environ Res Public Health. 2019;16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Christian MS, Bradley JC, Wallace JC, Burke MJ. Workplace safety: a meta-analysis of the roles of person and situation factors. Journal of Applied Psychology. 2009;94:1103–1127. [DOI] [PubMed] [Google Scholar]
- 4.Schneider B Organizational climates: An essay. Personnel Psychology. 1975;28:447–479. [Google Scholar]
- 5.Schneider B, Gonzalez-Roma V, Ostroff C, West M. Organizational climate and culture: Reflections on the history of the constructs in the Journal of Applied Psychology. J Appl Psychol. 2017;102:468–482. [DOI] [PubMed] [Google Scholar]
- 6.Zohar D Safety climate in industrial organizations: Theoretical and applied implications. Journal of Applied Psychology. 1980;65:96–102. [PubMed] [Google Scholar]
- 7.Clarke S An integrative model of safety climate: Linking psychological climate and work attitudes to individual safety outcomes using meta-analysis. Journal of Occupational and Organizational Psychology. 2010;83:553–578. [Google Scholar]
- 8.Nahrgang JD, Morgeson FP, Hofmann DA. Safety at work: A meta-analytic investigation of the link between job demands, job resources, burnout, engagement, and safety outcomes. Journal of Applied Psychology. 2011;96:71–94. [DOI] [PubMed] [Google Scholar]
- 9.Tetrick L, Sinclair R, Sawhney G, Chen T. We’ve got (safety) issues: Current methods and potential future direcetions in safety climate research. Human Resource Management Review. in press. [Google Scholar]
- 10.Hofmann DA, Burke MJ, Zohar D. 100 years of occupational safety research: From basic protections and work analysis to a multilevel view of workplace safety and risk. J Appl Psychol. 2017;102:375–388. [DOI] [PubMed] [Google Scholar]
- 11.Zweber ZM, Henning RA, Magley VJ. A practical scale for Multi-Faceted Organizational Health Climate Assessment. Journal of Occupational Health Psychology. 2016;21:250–259. [DOI] [PubMed] [Google Scholar]
- 12.Basen-Engquist K, Hudmon KS, Tripp M, Chamberlain R. Worksite Health and Safety Climate: Scale Development and Effects of a Health Promotion Intervention. Preventative Medicine. 1998;27:111–119. [DOI] [PubMed] [Google Scholar]
- 13.Ribisl KM, Reischl TM. Measuring the climate for health at organizations. Development of the worksite health climate scales. Journal of Occupational Medicine. 1993;35:812–824. [DOI] [PubMed] [Google Scholar]
- 14.Mearns K, Hope L, Ford MT, Tetrick LE. Investment in workforce health: Exploring the implications for workforce safety climate and commitment. Accident Analysis & Prevention. 2010;42:1445–1454. [DOI] [PubMed] [Google Scholar]
- 15.Sawhney G, Sinclair RR, Cox AR, Munc AH, Sliter MT. One Climate or Many: Examining the Structural Distinctiveness of Safety, Health, and Stress Prevention Climate Measures. J Occup Environ Med. 2018;60:1015–1025. [DOI] [PubMed] [Google Scholar]
- 16.Griffin M, Neal A. Perceptions of safety at work: a framework for linking safety climate to safety performance, knowledge, and motivation. Journal of Occupational Health Psychology. 2000;1:347–358. [DOI] [PubMed] [Google Scholar]
- 17.Neal A, Griffin MA. A study of the lagged relationships among safety climate, safety motivation, safety behavior, and accidents at the individual and group levels. Journal of Applied Psychology. 2006;91:946–953. [DOI] [PubMed] [Google Scholar]
- 18.Neal A, Griffin MA, Hart PM. The impact of organizational climate on safety and individual behaviour. Safety Science. 2000;34:99–109. [Google Scholar]
- 19.Mariani MG, Solda BL, Curcuruto M. Employee Safety Motivation: perspectives and measures on the basis of the Self-Determination theory. Med Lav. 2015;106:333–341. [PubMed] [Google Scholar]
- 20.Gagne M, Deci E. Self-determination theory and work motivation. J Organiz Behav. 2005;26:331–362. [Google Scholar]
- 21.Deci EL, Olafsen AH, Ryan RM. Self-Determination Theory in Work Organizations: The State of a Science. Annu Rev Organ Psych. 2017;4:19–43. [Google Scholar]
- 22.Zohar D Thirty years of safety climate research: Reflections and future directions. Accident Analysis and Prevention. 2010;42:1517–1522. [DOI] [PubMed] [Google Scholar]
- 23.Scott N, Fleming M, Kelloway E. Understanding why employees behave safely from a self-determination theory perspective In: Gagne M, ed. Oxford library of psychology The Oxford handbook of work engagement, motivation, and self-determination theory. New York, NY: Oxford University Press; 2014:276–294. [Google Scholar]
- 24.Burstyn I, Jonasi L, Wild C. Obtaining compliance with occupational health and safety regulations: a multilevel study using self-determination theory. International Journal of Environmental Health Research. 2010;20:271–287. [DOI] [PubMed] [Google Scholar]
- 25.Tenney L, Fan W, Dally M, et al. Health LinksTM assessment of Total Worker Health practices as indicators of organizational behavior in small business. Journal of Occupational & Environmental Medicine. 2019;61:623–634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics. 2009;42:377–381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lee J, Huang Y-H, Robertson MM, Murphy LA, Garabet A, Chang W-R. External validity of a generic safety climate scale for lone workers across different industries and companies. Accident Analysis & Prevention. 2014;63:138–145. [DOI] [PubMed] [Google Scholar]
- 28.Zohar D, Luria G. A multilevel model of safety climate: Cross-level relationships between organization and group-level climates. Journal of Applied Psychology. 2005;90:616–628. [DOI] [PubMed] [Google Scholar]
- 29.Conchie SM. Transformational leadership, intrinsic motivation, and trust: A moderated-mediated model of workplace safety. Journal of Occupational Health Psychology. 2013;18:198–210. [DOI] [PubMed] [Google Scholar]
- 30.Guay F, Vallerand RJ, Blanchard C. On the Assessment of Situational Intrinsic and Extrinsic Motivation: The Situational Motivation Scale (SIMS). Motivation and Emotion. 2001;24:175–213. [Google Scholar]
- 31.Brown TA. Confirmatory factor analysis for applied research. New York: The Guildford Press; 2006. [Google Scholar]
- 32.Hu L, Bentler P. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- 33.Hayes AF. Introduction to mediation, moderation, and conditional process analysis : a regression-based approach. New York: Guilford Press; 2018. [Google Scholar]
- 34.Hudson H, Nigam J, Sauter S, Chosewood L, Schill A, Howard J, eds. Total worker health. Washington, DC: American Psychological Association; 2019. [Google Scholar]
- 35.Lax MB. The Perils of Integrating Wellness and Safety and Health and the Possibility of a Worker-Oriented Alternative. NEW SOLUTIONS: A Journal of Environmental and Occupational Health Policy. 2016;26:11–39. [DOI] [PubMed] [Google Scholar]
- 36.Feltner C, Peterson K, Weber RP, et al. The effectiveness of Total Worker Health interventions: A systematic review for a National Institutes of Health Pathways to Prevention Workshop. Annals of Internal Medicine. 2016;165:262–269. [DOI] [PubMed] [Google Scholar]
- 37.Punnett L, Warren N, Henning R, Nobrega S, Cherniack M, CPH-NEW Research Team. Participatory ergonomics as a model for integrated programs to prevent chronic disease. Journal of Occupational and Environmental Medicine. 2013;55:S19–24. [DOI] [PubMed] [Google Scholar]
- 38.Tenney L, Newman L. Total Worker Health approaches in small to medium-sized enterprises In: Hudson H, Nigam J, Sauter S, Chosewood L, Schill A, Howard J, eds. Total Worker Health: American Psychological Association; 2019. [Google Scholar]
- 39.Eisenberger R, Huntinton R, Hutchinson SR, Sowa D. Percieved organizational support. Journal of Applied Psychology. 1986;71:500–507. [Google Scholar]
- 40.Shore E, Schwatka N, Dally M, Brown C, Tenney L, Newman L. Small business employees perceptions of leadership are associated with safety and health climates and their own behaviors. Journal of Environmental and Occupational Medicine. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Spector PE. Method variance in organizational research - Truth or urban legend? Organizational Research Methods. 2006;9:221–232. [Google Scholar]