

Summary
Background
Hepatitis C infection (HCV) can have a harmful effect on the health of people and can impose relevant healthcare costs. The World Health Organization has identified the elimination of Hepatitis C by 2030 as an important goal for all countries. This study aimed to identify the HCV-related policies in Iran.
Methods
A qualitative approach was used for this study. Data was collected through a comprehensive search of documents and interviews with different stakeholders related to the HCV program. Data was analyzed and validated using content analysis based on the policy triangle framework.
Results
Our findings highlighted that certain social and cultural issues related to stigma can impact on awareness-raising processes. It is also necessary to consider HCV directly in the context of government policies. All relevant stakeholders should be included. Continued talks and interactions need to be made between them for the active participation of all actors.
Conclusion
The findings of this study can provide useful information for improving, supporting and developing policy processes. Healthcare providers should address all aspects of the disease by 2030 in order to achieve the goal of HCV elimination. Evidence-based planning, support for up-to-date policies and resource mobilization are needed to achieve this ambitious goal.
Keywords: Hepatitis C virus, Policy analysis, Ethical features, Stigma, Policy triangle framework
Introduction
Viral hepatitis is a major public health challenge worldwide [1]. Hepatitis C infection (HCV), a blood-borne viral hepatitis, can have a harmful effect on the health of people and can impose relevant healthcare costs [2, 3]. In 2017, the World Health Organization (WHO) has estimated that, globally, around 71 million people have been infected with chronic HCV infection [4] and about 399,000 people have developed liver cirrhosis and hepatocellular carcinoma [4].
The WHO has identified the elimination of this infection by 2030 as a major and important objective. As such, all countries are required to reduce new infections by 90% and related deaths by 60% within 2030 [5]. To achieve such an ambitious goal, effective policies should be used to prevent and treat HCV [6]. In recent years, valuable advances have been made regarding epidemiological evidence, diagnosis and treatment of HCV by using direct antiviral agents (DAAs). The use of antiviral drugs has, indeed, increased the rate of recovery in patients by up to 90% [7, 8]. This has changed management perspectives: many countries have put HCV infection as a health priority [9-11].
Health policy-making is a complex process that examines the different dimensions of decisions, plans, role of various stakeholders and actions needed to be taken in order to achieve a health-care goal [12]. Policy analysis as a practice in the health sector is increasing in low- and middle-income countries. Paying attention to the nature of policies, how they are created, implemented, and affect health, and how agenda setting is developed is of crucial importance [13]. A better understanding of processes underlying healthcare and the acknowledgement of their impact on health issues can lead to an effective design and policy-making [14].
Due to the specific nature of the health sector, policy analysis requires more attention and sensitivity because it has a direct impact on the health of the community [13]. In Iran, the prevalence of HCV infection is relatively low according to epidemiological studies [15], especially when compared to settings such as the Middle East and North Arica (MENA) countries, like Pakistan and Egypt, even though in the last years the scenario is changing. According to a recent meta-analysis, the prevalence of HCV in the general population is estimated to be 0.6% [16]. In a further meta-analysis conducted in blood donors in 2013, HCV prevalence is estimated to be 0.5% [17]. In high-risk groups, the estimated prevalence of HCV is 32.3% and can increase up to 43.1% among injection drug users (IDUs) [18]. In meta-analyses in prisoners, street children and thalassemia patients, the prevalence of HCV has been found to be, respectively, 28%, 2.4% and 19% [19-21]. In Iran, the number of injecting drug users is increasing and this is reflected by the parallel increase in HCV infection rate: this is considerably changing the HCV epidemiology in the country [15].
Health systems around the world have implemented various strategies and programs for preventing, screening and treating HCV and achieving the WHO goal [22]. Understanding these policies is important in any country or community, and healthcare policy-makers can make better decisions about implementing HCV elimination programs by knowing more about the factors involved in the transmission and spread of the infection [23]. Many people believe that due to the seriousness of HCV for public health, prevention and control plans by the government, organizations and stakeholders at the highest levels should be considered.
In Iran, the Ministry of Health and Medical Education (MoHME) has launched various programs – the last in 2017 – in order to eliminate new cases of infection in three major areas: prevention, screening and treatment [24]. The educational programs are aimed at raising public awareness by providing appropriate information related to HCV prevention [25]. Currently HCV screening is carried out passively in Iran. Across the country, good laboratories and facilities work to diagnose the disease [26]. In 2014, it has been estimated that there are about 18,6500 HCV patients in Iran [27]. By providing DAAs to infected patients, the National Health System aims to reach Sustainable Development Goals (SDGs) goals, and to eliminate the disease by 2030 [27].
The MoHME, in line with the upfront documentation of long-term national development and the fulfilment of the country’s international obligations, understands the necessity and importance to prevent and control the disease. The MoHME has, therefore, planned to adopt a comprehensive and systematic approach as well as to implement effective strategies to eliminate the disease together with the establishment of a national hepatitis committee.
This study aimed to examine the HCV-related processes, programs, strategies, and documents in Iran, with the aim that identifying these policies can improve the existing gaps between the present and the desired situation.
Methods
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
This study received ethical approval from the School of Health Management, Iran University of Medical Sciences (IR.SUMS.REC.1396.9423557001).
RESEARCH TEAM AND REFLEXIVITY
Two authors (MB and HAG) conducted the first (documents collection and review) and second (interviews) steps of the present investigation. The research team involved has experience in conducting qualitative studies. For a better coordination, before the study was completed, a meeting was held and the research methodology process was discussed. Training events were also organized in order to better get in touch with the participants. Prior to conducting interviews, questions were sent to five experts on HCV for the pilot, and their comments and feedbacks were used to modify the questionnaire, if deemed necessary.
STUDY DESIGN
A qualitative policy analysis approach was used for this study. Data were collected through a broad and comprehensive search of documents and interviews with different stakeholders related to the HCV program (Figure 1).
DOCUMENTS COLLECTION AND REVIEW
The first step was to review policy documents related to HCV. To find documents, first the MoHME website was searched. After finding documents in the MoHME website, a list of relevant stakeholders including ministries, national and international organizations, companies and non-governmental organizations (NGOs) was prepared. The websites of the Parliament (Majlis) and the Expediency Discernment Council (EDC) were also searched. In Iran, for macro policies, the leader has a very important role in determining policies, and, as such, the documents communicated by him were also examined. The WHO website containing reports, policies and programs was also mined. In addition, international scholarly databases such as PubMed/MEDLINE, Scopus, ISI/Web of Science (WoS) and Embase, and the national databases including MagIran and SID were extensively searched for finding relevant policies-related documents.
INTERVIEWS
This step was based on the “Consolidated criteria for reporting qualitative research” (COREQ) checklist[28], a 32-item checklist for properly conducting qualitative research interviews and focus groups. These items regard three major domains; namely (i) research team and reflexivity, (ii) study design and (iii) data analysis and reporting.
The number of people contacted for the interviews was 26, of which 21 answered. They were contacted by telephone and email before the interview, and they were given a description of the goals and reasons for doing the study. For optimal use of interview time, the questionnaire was sent to them prior to the interview.
The second step comprised of interviews with diverse groups of respondents (n = 21), including policy-makers, academics involved in health policy, hepatitis specialists, senior researchers, senior clinicians, representatives of pharmaceutical companies, health directors working in the field of primary health care (PHC), NGOs, blood bank managers, nurses, laboratory managers and journalists. The key informants were identified with assistance from documents collection and review and the research unit at the MoHME. During the interview, snowballing sampling was used: the interviewees were asked to introduce other people who had experience or vision in HCV to participate in the study. Face-to-face interviews were conducted at workplace, clinics, or where the participants felt comfortable. To create a friendly and confident relationship – during the interview – only the participants and researchers were present. All the interviews were conducted following the proper methodology: no interview needed to be repeated. Researchers recorded and took written notes of each interview.
DATA COLLECTION
This study was conducted between September 2017 and July 2018. After the search and collection of relevant documents, a form was prepared and the title, content and year of publication of HCV-related policies and documents were extracted. Semi-structured, face-to-face interviews with participants of length varying between 45 and 60 minutes were performed and were digitally recorded with their permission. Open-ended questions were used. Interviews continued until data saturation was reached. After sixteen interviews no new data emerged and therefore the material was considered saturated.
ANALYTICAL FRAMEWORK
The policy triangle framework is a useful model for analyzing topics in the health sector. This model includes four components related to policy issues, such as context, content, actors and process. This model can provide a very important framework for understanding health sector-related issues for policy- and decision-makers. This model can be used retrospectively or prospectively [29].
Questions related to prevention, screening and treatment were asked. More in detail, the questions were the following:
Please describe the social, cultural, political, international and economic dimensions of HCV disease in Iran.
What is the structure of HCV-related policy in Iran since its inception concerning the prevention, screening and treatment? Which goals are being pursued in the country regarding the control and management of hepatitis C?
How do you see the policy process in the country? How are policies being developed, implemented and evaluated?
How and why are these policies taken into account? Why are these policies considered as one of the main priorities for health policy in the country?
Which organizations, institutions or individuals have a great impact on the hepatitis C policy process in Iran?
Are there other points of view regarding the state of policies and plans for hepatitis C in the country?
DATA ANALYSIS
The policy triangle model was used as a framework for extraction and analysis of identified policy documents [29]. After the recorded interviews, two authors transcribed them verbatim.
Data related to each phase of the HCV disease – including: prevention, screening and treatment – and the four components (context, content, actors and process) of the study framework were extracted from the interviews. Any disagreements between authors were resolved by discussion [30]. Data were analyzed and validated using content analysis. To validate the data, prolonged engagement and proper interaction with participants, and careful data revision helped to increase the credibility of the data. Also, methodological triangulation and diversity of sampling increased the credibility of the data and led to confirmability. Concerning verifiability, this was guaranteed by two academic members, with assistance of the researchers, by thorough and careful review of the text of the interviews, the codes, and the themes of the framework until agreement was reached. The transcription of interviews, the use of external checks and re-reading of all data ensured the overall reliability of the process. After being provided with the codes, a number of participants gave confirmation feedbacks.
Results
Overall, 21 different experts in the field and stakeholders related to the HCV program in Iran were interviewed. The mean age of participants was 39 ± 11.3 years. Among them, 17 were male and 4 females.
CONTEXT
In Iran, the general public has a negative attitude towards HCV. They think the disease is fatal and affects people who do not observe ethical issues. People believe that patients should be quarantined to prevent the transmission and spread of disease. Many people do not know enough about the ways and strategies to prevent it, and they consider it a terrible disease, like HIV.
“When colleagues or people understand that I suffer from HCV, their behaviours change. They think that I have committed an immoral act and stay away from me. People do not feel good about me and they are not even willing to interact with me”.
To increase awareness among people, educational activities are carried out at various levels of the health sector. Most of these activities take place especially in PHC, informing and raising awareness about HCV, but are generally poor and badly organized. Most HCV research activities have also been carried out by research centres of the Ministry of Health whereas less attention has been paid to socio-cultural and economic dimensions.
“Perhaps due to cultural problems associated with attitudes towards HCV in the Iranian society, schools, universities, and centres that do not have the task of informing about various health-related issues important for the community are less likely to inform about the disease”.
Most health services in Iran are based on a public sector model. PHC is completely free, and in addition to state-sponsored subsidies, health insurance also covers a portion of the health-care generated costs. Medical universities affiliated with the Ministry of Health and Social welfare hospitals provide healthcare related to HCV patients. All PHC activities are provided in the public sector. Many of these hospitals have good laboratories to detect HCV.
“Diagnostic capacities in Iran have grown dramatically in recent years, and therefore there is no problem in diagnosing HCV patients. On the one hand, the government should have a lot of financial support for managing these patients. On the other hand, in my opinion, if all the costs of these patients would be free, patients would be more interested in the treatment and this could prevent further outbreaks of the disease”.
Screening and active case finding play an important role in preventing the transmission of disease. The introduction of the family physician in some villages in Iran in 1997, the community-based training, the referral of suspect case, the early detection and treatment demonstrated to be effective strategies to prevent and control HCV.
However, these strategies have not been implemented all over the country and therefore their advantages are not nationwide.
“One of the benefits of a family doctor is the timely screening of people suspected of HCV. If the family doctor in Iran was fully implemented, this could prevent and screen many illness cases in Iran”.
Diagnosis and treatment of HCV patients are important, especially if defined and provided through a multi-professional evaluation. Hepatitis network – that includes gastroenterologists, specialists in infectious disease and general practitioners – implemented locally, in order to avoid patient transfer to the capital which implies paying for travel and accommodation, should be considered. Despite this, some service providers are not willing to cooperate in treating HCV patients for various reasons.
“Unfortunately, some doctors in Iran do not believe that HCV patients can be treated and, therefore, are unwilling to collaborate in providing services”.
Pharmaceutical companies have recently begun to produce HCV drugs and insurers have sponsored domestic medications and put them on the list of medications they support. Of course, in some cases, people who tend to use foreign drugs should pay some of the cost of the treatment. The main concern is about people who do not have insurance coverage and must have out-of-pocket payments.
“In all countries, drug companies are providing medicines and meeting with the needs of patients. In recent years, some companies have imported drugs due to lack of manufacturing technology. This has caused problems for patients, and insurers did not have the desire to support and cover for the cost of these drugs, but with the pursuit of authorities in Iran, some companies have begun to produce drugs locally, which significantly reduced costs”.
Neighbourhood with Pakistan or other countries with high HCV rates and Afghanistan as the largest drug producer in the world have led to the highest transit of narcotics from Iran. This has resulted into an increase in the number of injecting drug users in recent years. Cupping and tattooing are also rising as factors contributing to the spread of HCV infection.
“HCV disease, like many diseases, depends on several national and international variables. The prevalence of HCV in neighbouring countries is a dangerous alarm for the Iranian health sector. The high security level in Iran has caused many immigrants to decide to live in this country, and so we have to think in terms of various communicable diseases, including HCV, for properly screening them”.
One of the weaknesses in the health sector in Iran is the lack of a framework to prioritize the main problems in this area. It seems that if Iranian had a proper information system, it could have a better prioritization of illnesses and this would help administrators in planning. Local and regional data on HCV, especially in high-risk groups, are not available in many Iranian provinces. Hence, planning for these groups is difficult without proper evidence.
“Despite the many problems that HCV can have for any country, Iran has still major weaknesses in the information gathering system for these patients. Researcher, in view of the role of information in planning for disease control, should conduct research in the general population and at-risk groups in different provinces”.
Like many countries that have committed to the SDGs to eliminate HCV by 2030, health policy- and decision-makers are aware both of the importance and of the problems that this disease can cause to Iran, and therefore they are trying to implement effective policies to achieve this international goal.
“Iran has been struggling to achieve international goals in recent years. In terms of the Millennium Development Goals (MDGs), Iran has been able to improve its health indicators and achieve its goals. So, policy- and decision-makers are trying to reach the goals of the SDGs, which makes it possible to eliminate HCV”.
There are limited financial resources in the health sector in all countries. In Iran, in recent years, there has been limited funding available for educational programs, activities and treatment for HCV patients, but, after the implementation of the Health Development Plan, funds were provided by the Ministry of Health. The plan made the processes associated with these patients more prominent and the government paid a large part of the cost of treatment.
“Many health ministry staff members say that for health-related problems, more spending and new financial resources are needed. In the last decades, health has been considered as a very important priority. We should take this opportunity and use the new financial resources for health challenges like HCV”.
The health sector, however, faces a shortage of human resources. There are shortages of nurses in many hospitals. In some provinces there is a shortage of specialized physicians. Given the attitudes of some providers about infectious diseases and the hardships they should undergo during HCV treatment processes; they expect to receive better payments. Low salaries for nurses, failure to enforce tariffs for services for them, low tariffs for internal and external medical practitioners, delay in reimbursement by insurers are some of the problems that healthcare providers have to face.
“Iran’s health system faces a serious shortage of human resources concerning all professional groups (from general practitioners to specialists and nurses and other allied health workers). The high volume of work for many employees has made them tired. This shortage reduces the quality of services provided and is also a threat to HCV. If we pay more for HCV service providers, we can improve the quality of services to patients”.
The private sector has currently no role to play in the provision of healthcare to these patients, but in the future it could participate together with the government in providing management and treatment options to HCV patients.
“To reduce the volume of work in the public sector, some services can be provided by the private sector. Of course, in order to reduce costs for patients, the government has a lot to do for HCV together with the private sector”.
CONTENT
A national survey would be required to determine the current state of HCV in Iran at the country level. This type of study can be of great help to policy- and decision-makers.
“There is no information on HCV based on a large study. If we can do this with the help of researchers, we can have a better and more realistic plan”.
In many years, governments have mandated many organizations to work on prevention, diagnosis and treatment for all people in the community, and they have accepted such responsibility.
“In recent years, health policy- and decision-makers have been working to make HCV a top priority. The efforts that have been made to diagnose, treat and educate have somewhat contributed to counteract and mitigate the burden of disease. However, for instance, the higher risk of HCV in co-infected people, such as those with HIV, has not yet been mentioned directly in important national documents. Once explicitly mentioned, more funds may be available to control the spread of infections”.
“One of the strengths associated with HCV is the existence of national and international collaborations for Iran. There is a good relationship between Iranian and international researchers. Iranian physicians are well-known for their studies on HCV”.
Studies show that the content of the laws and the plans developed by policy- and decision-makers in Iran increases the access to healthcare for patients. HCV screening and treatment is also a favourite target of policy-makers. They are trying to approve upstream legislation to support these patients.
Documents and policies indicate that Iran’s health sector is seeking to fulfil its international obligations. In particular, Iran is trying to achieve the 2030 target. The Health Ministry has been working to achieve this goal, in accordance with the WHO framework, in its four areas.
The Iranian Blood Transfusion Organization has been asked to screen all donated blood for HCV. This has provided access to healthy blood products.
Considering that the number of HCV patients in Iran is increasing, screening for at-risk groups should be considered as an optimal strategy, including for example, HCV test before imprisonment, but this has not been yet fully implemented.
“Many people need blood to continue living. It is very good that today there is no problem in getting healthy blood. It costs a lot, but people are no longer concerned”.
The health sector plans to reduce HCV-related deaths by 65% and to curb new HCV cases by 90% by 2030.
“In the action plan, the main goal of the health sector in relation to HCV is to achieve the goals of the SDGs and, in accordance with the WHO guidelines, it aims to be consistent with global goals and targets”.
For a better treatment and management of HCV patients, the health department has provided physicians with advice on delivering optimal services and improving patient recovery, as well as with national and international guidelines. Of course, valid and up-to-date global references can also be used.
ACTORS
The most important actor who has the greatest impact on HCV policies in Iran is the MoHME. The ministry carries out extensive activities to support policies aimed at controlling the disease, including planning, funding, medical, educational and screening activities.
Several organizations in Iran have the responsibility to focus on activities such as screening, providing social, cultural, and financial support for patients and people at risk. However, there seems to be a kind of lack of effective collaboration between them. Moreover, some organizations are responsible for social protection of addicts, but little is done for a variety of reasons, such as lack of financial resources. In the meantime, screening in prisons has still to be fully implemented.
“It is not good that the entire workload related to HCV is up to the Ministry of Health. If at least some funding was provided by a number of organizations, this would help the Ministry of Health focus on patient care. If the dialogue between the Ministry of Health and other organizations is combined with practical action, we could see more success in reaching the SDGs”.
NGOs and media associations do not currently play a major role in raising awareness about HCV society whereas members of the religious section in Iran have a good place among people, but it seems that there is no good cooperation between policy- and decision-makers and religious people due to the negative attitudes towards HCV in society and the lack of proper use of emerging information and communication technologies (ICTs).
“Many people use the information services of NGOs in Iran. In addition, with the recent development of virtual networks and ICTs, these important facilities and infrastructures seem to have an enormous potential for education, which is still underused. These groups and networks can be used to change the attitudes of people towards the disease”.
The role of international organizations in coping with financial issues related to HCV in Iran is currently minor, even though this is changing in the last years. For instance, the WHO has been able to influence health policies by providing its own reports on HCV. Accordingly, the Iranian Ministry of Health has developed its plans and programs for the disease control and management in accordance with the framework of the WHO and other relevant international organizations.
One of the important actors in blood screening and blood supply for those in need is the Iran Blood Transfusion Organization. After 76 years, the organization has been required to screen all donated blood. Therefore, Iran has currently no problem in providing healthy blood.
“Undoubtedly, the policy of healthy blood in Iran has been very successful. Thanks to the efforts of the blood transfusion organization, in addition to screening services, provision of healthy blood for the needs of at-risk groups is very desirable. Perhaps the free provision of these services has led many people to use them with great satisfaction”.
Pharmaceutical companies have been able to play an important role in the treatment process and in reducing the costs by producing locally HCV drugs. This has resulted in a decrease in the economic-financial burden that the Ministry of Health had previously to cope with. The private sector has currently little to do with investing in the drug sector and providing diagnostic services, even if in the future there is room for its engagement and involvement.
Finally, the Iran’s Hepatitis Network has a huge impact on the implementation of the program as a government group (identifying, recording patients’ information, and treating them).
“The Iran’s Hepatitis Network has done a very good job in the process of controlling and managing HCV. If not, most of the patients would be unaware of their status. They do a lot of educational and therapeutic activities”.
PROCESS
A key step in the HCV policy-making process in Iran has been the formation of a national hepatitis committee, in which key people were researchers, health policy- and decision-makers. The main tasks of the committee are policy-making and planning, management, monitoring and evaluation, training and guidance of activities related to HCV control programs. The committee has been created by the Ministry of Health. At the same time, various meetings with other organizations related to HCV programs have taken place and almost good decisions have been made to counteract the spread of HCV. In order to attract the cooperation and participation of all ministries, organizations and stakeholders in maintaining and promoting the health of Iranian communities, the Council has helped create more cohesive programs through the formation of networks and the presence of many important members actively involved and engaged in HCV programs.
“The Hepatitis Country Committee in Iran has played a very important role in controlling hepatitis. People who are present in this committee have a high, reputed scientific and political status. The presence of these people is a great opportunity to implement large-scale programs to eliminate or at least control HCV”.
The most important source of funding for health sector programs in Iran is provided by the Parliament based on a proposal from the government. Like many countries, many lobbyists are trying to use funds in other sectors, but the most important point is that most members of Parliament (MPs) are paying particular, increasing attention to health and related programs. The Ministry of Health is in charge of meeting with the needs of the health sector and interacts with the government and parliament.
“In recent years, the Ministry of Health has implemented several good plans and Iranian policy- and decision-makers have opened new perspectives by providing better services and addressing community health problems. Effective conversations and interactions between the Ministry of Health and policy- and decision-makers have been conducted to get their comments and feedbacks on how to effectively run the programs”.
Most HCV-related policies are top-down. There is a great deal of work and activities to carry out related to healthcare in the health sector, and as a result of the problems with the treatment of HCV patients, there are some processes that are prolonged. Some organizations do not fulfil their duties and all the expectations from the Ministry of Health are confronting this important challenge. All relevant stakeholders should be more actively engaged in HCV-related policies and plans.
“One of the main challenges in Iran’s health system is its doctor-centeredness. Many physicians manage many departments. The treatment perspective is dominant. If some members of the staff who perform executive activities are used in the training, some policies and programs would be more realistic to run. Many services offered should be presented as long-term processes and objectives”.
With the arrival of the President Rouhani, the establishment of his government and the launch of a broad health promotion plan, the availability of new financial resources, the need of controlling the increase in injectable drug users and the obligations of SDGs for Iran have been considered as a good opportunity for HCV-related policies to be put into action and to be implemented.
“The Health Transformation Plan has many good strengths. With regard to new activities that can be used to provide services to marginalized settings and those who do not have a proper financial situation, prevention and control programs can be further implemented”.
The role of service providers in PHC and nurses in the provision of services should be given more attention.
Moreover, the lack of proper implementation of the referral system is one of the weaknesses of the health sector. Unfortunately, despite the role of PHC, patients are only aware of their illnesses in hospitals and do not use PHC services to monitor the treatment. If PHC collaborated more extensively, it would be easier for patients to have more adequate time and space.
“The potential of the PHC network for HCV is not fully exploited. A large number of Iranian communities, especially those living in villages, would be interested in using these services. There must be a simple and up-to-date program for them”.
Finally, there is no specific mechanism for evaluating HCV policies in the country. The evaluations are mostly individual, personal, cross-sectional rather than longitudinal, limited, with short-term organizational goals, and there is no specific structure and system for it. The related organizations have carried out independent monitoring activities, which are largely interrupted, inadequate and non-conclusive.
“In recent years, evaluation has not been carried out on programs for the training, screening and treatment of HCV. The weaknesses and strengths of these programs are not clear. The Ministry of Health must have an appropriate evaluation system in cooperation with other independent organizations”.
Discussion
The present study comprehensively addressed HCV-related policies and programs in Iran. The findings of this study emphasized the impact and complexity of various factors for policy making. Policy analysis has shown that for the development and implementation of a health program, some barriers that prevent it from being properly implemented should be identified and properly removed. Therefore, in order to investigate the health sector’s challenges, we must correctly identify the problems and consider the various options for solving them and consider the different issues at the implementation stage [31].
Using a policy model, this study examined the various dimensions of HCV in Iran. More in detail, in the context of HCV, one of the major barriers that policy- and decision-makers in Iran have been unable to properly defeat is illness-related stigma. This has caused many people not to be educated enough concerning HCV and be afraid of individuals infected [32]. The lack of trust in information and the lack of mass media use has led to a lack of public awareness in Iran [33]. Policy- and decision-makers have had a lot of problems in raising social awareness of diseases such as HCV and HIV [34]. One of the major challenges associated with HCV control is the lack of awareness among the general population and health workers. Supporting educational programs by government and relevant organizations is of paramount importance [35]. The Ministry of Health can exploit national TV to raise awareness about HCV. In recent years, people have become more aware of HIV through the use of television, radio, social media, and people who have a great impact on the general public’s perception of HIV (the so-called advocacy). Policy- and decision-makers can make use of the experience gained in this area to change people’s awareness and attitudes towards HCV in Iran.
HCV can have devastating effects on the economies of the countries, and therefore adequate funds for controlling this disease, in addition to those for preventing the transmission of the disease, would counteract the loss of funds imposed by the disease [36]. In recent years, funding for treating patients has been a major concern for the Ministry of Health, who has been working to provide good support for people who are not able to pay for the treatment.
Regarding the content of existing HCV-related policies in Iran, there is no specific reference to HCV in macro policies. There are many programs and activities in the form of guidelines issued by the Ministry of Health, although organizations and health departments are not directly instructed. In this regard, the National Committee on Hepatitis in Iran has been working to guide physicians, staff and other organizations.
Considering that Afghanistan as the neighbouring country of Iran is the largest producer of narcotics and given the high volume of immigration, Afghanistan’s health policy- and decision-makers need to be involved in controlling HCV refugees. Unfortunately, despite the fact that many people from Afghanistan migrate to Iran annually, international organizations do not actually donate funds to Iran to improve their health [37]. Therefore, the Ministry of Health needs international financial resources for the screening and treatment of Afghan refugee patients [38].
The findings of this study showed that the major problems with the HCV programs is how policies have been designed (most of them are top-down) and the lack of use of comments and feedbacks from relevant stakeholders. When decision- and policy-makers do not use the views of individuals who run the executive process of a policy, it seems to be difficult to achieve the desired goals [39]. Furthermore, existing evidence suggests that physicians and other relevant stakeholders should be involved in the HCV policy-making processes.
In addition to specialized hospitals and clinics, the PHC health services network plays an important role in providing educational, health and therapeutic services. The potential of this network has not been fully exploited for the purpose of patients, so doctors working in this network have still much to offer to patients with HCV [40].
Other points to be noted are that the policies that have been taken to control HCV are at a national level and have not or little responded to local priorities, especially in areas with high-risk factors for transmitting and spreading the disease [41].
Because of the high level of healthcare bureaucracy, policies aimed at controlling HCV should be quickly implemented. In some cases, such as insurance services and subsidies for patients, the government must notify the organizations to enforce them, but, in other cases, it seems that the length of approval and implementation is too long, and hence the effectiveness of these policies is less than that expected [42].
Despite the existence of national data on vulnerable groups, there are still not many local data. In addition, many policies that are introduced on the basis of these data encounter many problems and issues during the implementation phase. In order to properly implement policies, they should be presented clearly and without any ambiguity. One of the important reasons for this lack of proper implementation is the weakness during the step of knowledge translation and the lack of effective communication between policy-, decision-makers and researchers [43].
Many stakeholders are involved in the process of controlling HCV in Iran. One of the challenges is the lack of appropriate interactions between the actors and the various organizations. Due to the fact that the national documents do not refer directly to HCV, the tasks of the organizations are not exactly defined. Of course, there are activities for each of them, but many organizations consider the Ministry of Health as the main actor and responsible for the plans; practically, activities that are relevant to the cultural, social and economic structures of society and patients are not properly implemented. For example, many injecting drug users are faced with plenty of economic problems that should be addressed. On the other hand, many stakeholders only consider the treatment of patients and have forgotten other issues such as education, culture, and protection of high-risk groups.
There is no doubt that the most important and powerful actor in charge of the HCV control program in Iran is the Ministry of Health, but the Ministry alone cannot do all the activities. Other organizations must fulfil their obligations. This commitment is in the fields of education, screening and treatment [44]. Health policy- and decision-makers need broad support to implement their HCV control policies [45].
As in many countries in the world, people using injecting drugs are the most important sources of HCV transmission in Iran [46], as well as prisoners [19]. Evidence suggests that screening and treatment activities among these people should be seriously addressed by policy- and decision-makers to prevent HCV [47], implementing strategies such as needle and syringe programs (NSPs) and opioid substitution therapy (OST) [48, 49]. In recent years, the Ministry of Health has set up centres to provide services to reduce harm and prevent the transmission of communicable diseases such as HIV and HCV [50].
These policies can be effective in reducing HCV transmission in Iran, but despite the positive attitude of prison staff towards implementing these policies, some officials and managers have little commitment and motivation [51] and many people who inject drugs (PWID) do not use the services of the centres.
Moreover, the evaluation of services provided in the HCV program has not yet been taken seriously by policy- and decision-makers [52]. The Ministry of Health and other organizations should implement the evaluation of HCV-related programs.
Our study has some strengths: it is one of the first studies, if not the first, focusing on HCV-related policies in the WHO Eastern Mediterranean Regional Office (EMRO) region, which is a geographical area with a high HCV incidence. Regarding the triangle policy framework, various aspects of HCV were studied. To increase the credibility and reliability of the data, after evaluating the results, a group of experts was involved and consulted in the various steps of the research.
On the other hand, our study has some limitations. Some people were not willing to be interviewed. As such, the sample recruited may be not representative of all the stakeholders involved in HCV-related policies.
Conclusions
The findings of this study, based on the policy triangle framework as a model of policy analysis, showed that various factors can affect HCV policy in Iran. Certain cultural problems caused by stigma can impact on awareness-raising processes. It is also necessary to consider HCV directly in the context of governmental policies. All relevant stakeholders, including the private sector, should be involved. The findings of this study can provide good information for improving, supporting and developing policy processes in Iran. Evidence-based planning, epidemiological surveys conducted in Iranian provinces characterized by HCV prevalence rates, support for up-to-date policies and resource mobilization are needed to achieve the ambitious goal of HCV elimination by 2030.
Figures and tables
Fig. 1.
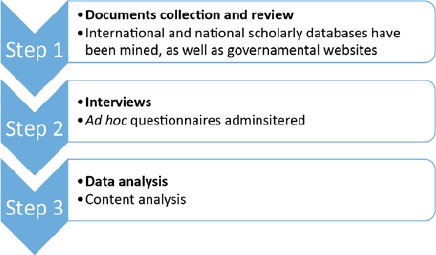
Flowchart adopted in the present investigation.
Acknowledgements
Funding sources: this study was supported by the Iran University of Medical Sciences, Iran (No: IUMS/SHMIS_1396/9423557001).
Footnotes
Conflict of interest statement
The authors declare no conflict of interest.
Authors’ contributions
MB and NLB conceived the study, MB, NLB and MM drafted the manuscript, SA, HAG and MM revised the manuscript. MB, SA, MM and NLB performed a search of the literature. All authors critically revised the manuscript. All authors have read and approved the latest version of the manuscript.
References
- [1].Papatheodoridis G, Hatzakis A. Public health issues of hepatitis C virus infection. Best Pract Res Clin Gastroenterol 2012;26:371-80. https://doi.org/10.1016/j.bpg.2012.09.012 10.1016/j.bpg.2012.09.012 [DOI] [PubMed] [Google Scholar]
- [2].Razavi H, Elkhoury AC, Elbasha E, Estes C, Pasini K, Poynard T, Kumar R. Chronic hepatitis C virus (HCV) disease burden and cost in the United States. Hepatology 2013;57:2164-70. https://doi.org/10.1002/hep.26218 10.1002/hep.26218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Stanaway JD, Flaxman AD, Naghavi M, Fitzmaurice C, Vos T, Abubakar I, Abu-Raddad Lj, Assadi R, Bhala N, Cowie B, Forouzanfour MH, Greger J, Hanafiah KM, Jacobsen KH, James SL, MacLachlan J, Malekzadeh R, Martin NK, Mokdad AA, Mokdad AH, Murray CJL, Plass D, Rana S, Rein DB, Richardus JH, Sanabria J, Saylan M, Shahraz S, So S, Valssov VV, Weiderpass E, Wiersma ST, Younis M, Yu M, Yu C, El Sayed Zaki M, Cooke GS. The global burden of viral hepatitis from 1990 to 2013: findings from the global burden of disease study 2013. Lancet 2016;388:1081-8. https://doi.org/10.1016/S0140-6736(16)30579-7 10.1016/S0140-6736(16)30579-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].WHO. Global hepatitis report, 2017. Available at: http://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/. (Accessed on 30 August 2018).
- [5].WHO. Combating hepatitis B and C to reach elimination by 2030 2016. Available from: http://www.who.int/hepatitis/publications/hep-elimination-by-2030-brief/en/. (Accessed on 30 August 2018).
- [6].Tachi K. Hepatitis C virus infection in Ghana: time for action is now. Ghana Med J 2018;52:1-2. https://doi.org/10.4314/gmj.v52i1.1 10.4314/gmj.v52i1.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Ara AK, Paul JP. New direct-acting antiviral therapies for treatment of chronic hepatitis C virus infection. Gastroenterol Hepatol (N Y) 2015;11:458-66. [PMC free article] [PubMed] [Google Scholar]
- [8].Schietroma I, Scheri GC, Pinacchio C, Statzu M, Petruzziello A, Vullo V. Hepatitis C virus and hepatocellular carcinoma: pathogenetic mechanisms and impact of direct-acting antivirals. Open Virol J 2018;12:16-25. https://doi.org/10.2174/1874357901812010016 10.2174/1874357901812010016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Burki T. Elimination on the agenda for hepatitis C. Lancet Infect Dis 2014;14:452-3. https://doi.org/10.1016/s1473-3099(14)70704-2 10.1016/s1473-3099(14)70704-2 [DOI] [PubMed] [Google Scholar]
- [10].El-Akel W, El-Sayed MH, El Kassas M, El-Serafy M, Khairy M, Elsaeed K, Kabil K, Hassany M, Shawky A, Yosry A, Shaker MK, ELShazly Y, Waked I, Esmat G, Doss W. National treatment programme of hepatitis C in Egypt: Hepatitis C virus model of care. J Viral Hepat 2017;24:262-7. https://doi.org/10.1111/jvh.12668 10.1111/jvh.12668 [DOI] [PubMed] [Google Scholar]
- [11].Nasrullah M, Sergeenko D, Gamkrelidze A, Averhoff F. HCV elimination - lessons learned from a small Eurasian country, Georgia. Nat Rev Gastroenterol Hepatol 2017;14:447-8. https://doi.org/10.1038/nrgastro.2017.100 10.1038/nrgastro.2017.100 [DOI] [PubMed] [Google Scholar]
- [12].Maddalena V. Evidence-based decision-making 8: health policy, a primer for researchers. Methods Mol Biol 2015;1281:501-17. https://doi.org/10.1007/978-1-4939-2428-8_30 10.1007/978-1-4939-2428-8_30 [DOI] [PubMed] [Google Scholar]
- [13].Gilson L, Raphaely N. The terrain of health policy analysis in low and middle income countries: a review of published literature 1994-2007. Health Policy Plan 2008;23:294-307. https://doi.org/10.1093/heapol/czn019 10.1093/heapol/czn019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Green A, Gerein N, Mirzoev T, Bird P, Pearson S, Anh le V, Martineau T, Mukhopadhyay M, Qian X, Ramani KV, Soors W. Health policy processes in maternal health: a comparison of Vietnam, India and China. Health Policy 2011;100:167-73. [DOI] [PubMed] [Google Scholar]
- [15].Taherkhani R, Farshadpour F. Epidemiology of hepatitis C virus in Iran. World J Gastroenterol 2015;21:10790-810. https://doi.org/10.3748/wjg.v21.i38.10790 10.3748/wjg.v21.i38.10790 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Mirminachi B, Mohammadi Z, Merat S, Neishabouri A, Sharifi A H, Alavian SH, Poustchi H, Malekzadeh R. Update on the prevalence of hepatitis C virus infection among Iranian general population: a systematic review and meta-analysis. Hepat Mon 2017;17:e42291. [Google Scholar]
- [17].Khodabandehloo M, Roshani D, Sayehmiri K. Prevalence and trend of hepatitis C virus infection among blood donors in Iran: A systematic review and meta-analysis. J Res Med Sci 2013;18:674-82. [PMC free article] [PubMed] [Google Scholar]
- [18].Nematollahi S, Ayubi E, Almasi-Hashiani A, Mansori K, Moradi Y, Veisani Y, Jenabi E, Gholamaliei B, Khazeei S. Prevalence of hepatitis C virus infection among high-risk groups in Iran: a systematic review and meta-analysis. Public Health 2018;161:90-8. https://doi.org/10.1016/j.puhe.2018.04.011 10.1016/j.puhe.2018.04.011 [DOI] [PubMed] [Google Scholar]
- [19].Behzadifar M, Gorji HA, Rezapour A, Bragazzi NL. Prevalence of hepatitis C virus infection among prisoners in Iran: a systematic review and meta-analysis. Harm Reduct J 2018;15:24 https://doi.org/10.1186/s12954-018-0231-0 10.1186/s12954-018-0231-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Behzadifar M, Gorji HA, Rezapour A, Bragazzi NL. Prevalence of hepatitis C virus among street children in Iran. Infect Dis Poverty 2018;7:88 https://doi.org/10.1186/s40249-018-0469-5 10.1186/s40249-018-0469-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Behzadifar M, Gorji HA, Bragazzi NL. The prevalence of hepatitis C virus infection in thalassemia patients in Iran from 2000 to 2017: a systematic review and meta-analysis. Arch Virol 2018;163:1131-40. https://doi.org/10.1007/s00705-018-3767-0 10.1007/s00705-018-3767-0 [DOI] [PubMed] [Google Scholar]
- [22].Hutin Y, Low-Beer D, Bergeri I, Hess S, Garcia-Calleja JM, Hayashi C, et al. Viral hepatitis strategic information to achieve elimination by 2030: key elements for HIV program managers. JMIR Public Health Surveill 2017;3(4):e91 https://doi.org/10.2196/publichealth.7370 10.2196/publichealth.7370 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Dore GJ, Hajarizadeh B. Elimination of hepatitis C virus in Australia: laying the foundation. Infect Dis Clin North Am 2018;32:269-79. https://doi.org/10.1016/j.idc.2018.02.006 10.1016/j.idc.2018.02.006 [DOI] [PubMed] [Google Scholar]
- [24].Alavian S M, Sharafi H. Update on Recommendations for the clinical management of hepatitis C in Iran 2017. Hepat Mon 2017;17:e63956 https://doi.org/10.5812/hepatmon.guideline 10.5812/hepatmon.guideline [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Hesamizadeh K, Sharafi H, Rezaee-Zavareh MS, Behnava B, Alavian SM. Next steps toward eradication of hepatitis C in the era of direct acting antivirals. Hepat Mon 2016;16:e37089 https://doi.org/10.5812/hepatmon.37089 10.5812/hepatmon.37089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Alavian SM, Hajarizadeh B, Bagheri Lankarani K, Sharafi H, Ebrahimi Daryani N, Merat S, Mohraz M, Mardani M, Fattahi MR, Poustchi H, Nikbin M, Nabavi M, Adibi P, Ziaee M, Behnava B, Rezaee-Zavareh MS, Colombo M, Massoumi H, Bizri AR, Eghtesad B, Amiri M, Namvar A, Hesamizadeh K, Malejzadeh R. Recommendations for the clinical management of hepatitis C in Iran: a consensus-based national guideline. Hepat Mon 2016;16:e40959 https://doi.org/10.5812/hepatmon.guideline 10.5812/hepatmon.guideline [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Hajarizadeh B, Razavi-Shearer D, Merat S, Alavian SM, Malekzadeh R, Razavi H. Liver disease burden of hepatitis C virus infection in Iran and the potential impact of various treatment strategies on the disease burden. Hepat Mon 2016;16:e37234 https://doi.org/10.5812/hepatmon.37234 10.5812/hepatmon.37234 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007;19:349-57. https://doi.org/10.1093/intqhc/mzm042 10.1093/intqhc/mzm042 [DOI] [PubMed] [Google Scholar]
- [29].Walt G, Gilson L. Reforming the health sector in developing countries: the central role of policy analysis. Health Policy Plan 1994;9:353-70. https://doi.org/10.1093/heapol/9.4.353 10.1093/heapol/9.4.353 [DOI] [PubMed] [Google Scholar]
- [30].Morse JM. Critical analysis of strategies for determining rigor in qualitative inquiry. Qual Health Res 2015;25:1212-22. https://doi.org/10.1177/1049732315588501 10.1177/1049732315588501 [DOI] [PubMed] [Google Scholar]
- [31].Lavis JN, Røttingen JA, Bosch-Capblanch X, Atun R, El-Jardali F, Gilson L, Lewin S, Oliver S, Ongolo-Zogo P, Haines A. Guidance for evidence-informed policies about health systems: linking guidance development to policy development. PLoS Med 2012;9:e1001186 https://doi.org/10.1371/journal.pmed.1001186 10.1371/journal.pmed.1001186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Treloar C, Rance J, Backmund M. Understanding barriers to hepatitis C virus care and stigmatization from a social perspective. Clin Infect Dis 2013;57(Suppl 2):S51-5. https://doi.org/10.1093/cid/cit263 10.1093/cid/cit263 [DOI] [PubMed] [Google Scholar]
- [33].Karimi-Sari H, Bayatpoor ME, Aftabi Khotbesara M, Ebrahimi MS, Sattari Z, Sattari P, Saberi Shakib N, Taheri H, Abdolrahim Poor Heravi S, Dinizadeh M, Vahed P, Shirsavar K, Hosseini H, Rashvand S, Jalaei D, Azarafraz M, Naderi M, Pourzakaria M, Firoozbakht M, Khosravi MH, Alavian SM. Knowledge, attitude, and practice of Iranian health sciences students regarding hepatitis B and C virus infections: a national survey. Am J Infect Control 2017;45:e135-e41. [DOI] [PubMed] [Google Scholar]
- [34].Khodayari-Zarnaq R, Ravaghi H, Mohammad Mosaddeghrad A, Sedaghat A, Mohraz M. HIV/AIDS policy agenda setting in Iran. Med J Islam Repub Iran 2016;30:392. [PMC free article] [PubMed] [Google Scholar]
- [35].WHO. Prevention and control of viral hepatitis infection: framework for global action 2012. [Available at: http://www.who.int/hiv/pub/hepatitis/Framework/en/. (Accessed on 27 September 2018).
- [36].Wittenborn J, Brady J, Dougherty M, Rein D. Potential epidemiologic, economic, and budgetary impacts of current rates of hepatitis C treatment in medicare and non-medicare populations. Hepatol Commun 2017;1:99-109. https://doi.org/10.1002/hep4.1031 10.1002/hep4.1031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Hosseini Divkolaye NS, Burkle FM., Jr The enduring health challenges of Afghan immigrants and refugees in Iran: a systematic review. PLoS Curr 2017;9:ecurrents.dis.449b4c549951e359363a90a7f4cf8fc4 https://doi.org/10.1371/currents.dis.449b4c549951e359363a90a7f4cf8fc4 10.1371/currents.dis.449b4c549951e359363a90a7f4cf8fc4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Sharma S, Carballo M, Feld JJ, Janssen HL. Immigration and viral hepatitis. J Hepatol 2015;63515-22. https://doi.org/10.1016/j.jhep.2015.04.026 10.1016/j.jhep.2015.04.026 [DOI] [PubMed] [Google Scholar]
- [39].Mukamel DB, Haeder SF, Weimer DL. Top-down and bottom-up approaches to health care quality: the impacts of regulation and report cards. Annu Rev Public Health 2014;35:477-9. https://doi.org/10.1146/annurev-publhealth-082313-115826 10.1146/annurev-publhealth-082313-115826 [DOI] [PubMed] [Google Scholar]
- [40].Behzadifar M, Gorji HA, Rezapour A, Bragazzi NL, Alavian SM. The role of the primary healthcare network in Iran in hepatitis C virus elimination by 2030. J Virus Erad 2018;4:186-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Duffell EF, Hedrich D, Mardh O, Mozalevskis A. Towards elimination of hepatitis B and C in European union and European economic area countries: monitoring the world health organization’s global health sector strategy core indicators and scaling up key interventions. Euro Surveill 2017;22:30476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].El-Jardali F, Lavis JN, Ataya N, Jamal D, Ammar W, Raouf S. Use of health systems evidence by policymakers in eastern Mediterranean countries: views, practices, and contextual influences. BMC Health Serv Res 2012;12:200 https://doi.org/10.1186/1472-6963-12-200 10.1186/1472-6963-12-200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Nedjat S, Gholami J, Yazdizadeh B, Nedjat S, Maleki K, Majdzadeh R. Research’s practice and barriers of knowledge translation in Iran. Iran J Public Health 2014;43:968-80. [PMC free article] [PubMed] [Google Scholar]
- [44].Walt G, Shiffman J, Schneider H, Murray SF, Brugha R, Gilson L. ‘Doing’ health policy analysis: methodological and conceptual reflections and challenges. Health Policy Plan 2008;23:308-17. https://doi.org/10.1093/heapol/czn024 10.1093/heapol/czn024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Miri-Bonjar M, Khorram A, Ansari-Moghaddam A. The necessity of enhanced harm reduction programs to prevent blood-borne infections amongst injection drug users. Health Scope 2016;5:e32754. [Google Scholar]
- [46].Sharhani A, Mehrabi Y, Noroozi A, Nasirian M, Higgs P, Hajebi A, Hamzeh B, Khademi N, Noroozi M, Shakiba E, Etemad K. Hepatitis C virus seroprevalence and associated risk factors among male drug injectors in Kermanshah, Iran. Hepat Mon 2017;17:e58739. [Google Scholar]
- [47].Bielen R, Stumo SR, Halford R, Werling K, Reic T, Stöver H, Robaeys G, Lazarus JV. Harm reduction and viral hepatitis C in European prisons: a cross-sectional survey of 25 countries. Harm Reduct J 2018;15:25 https://doi.org/10.1186/s12954-018-0230-1 10.1186/s12954-018-0230-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [48].Iversen J, Wand H, Topp L, Kaldor J, Maher L. Reduction in HCV incidence among injection drug users attending needle and syringe programs in Australia: a linkage study. Am J Public Health 2013;103:1436-44. https://doi.org/10.2105/AJPH.2012.301206 10.2105/AJPH.2012.301206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [49].Hedrich D, Alves P, Farrell M, Stöver H, Møller L, Mayet S. The effectiveness of opioid maintenance treatment in prison settings: a systematic review. Addiction 2012;107:501-17. https://doi.org/10.1111/j.1360-0443.2011.03676.x 10.1111/j.1360-0443.2011.03676.x [DOI] [PubMed] [Google Scholar]
- [50].Hajarizadeh B. Generic direct acting antiviral treatment: the first step towards elimination of hepatitis C in Iran. Hepat Mon 2017;17:e45788. [Google Scholar]
- [51].Farnia M, Shahbazi M, Moradi G, Alizadeh S, Ebrahi B, Kandi Kalle M. Evaluation of Harm reduction Programs in prisons from the attitude and viewpoint of Iranian prison staff. SJSPH 2013;11:29-44. [Google Scholar]
- [52].McDonnell A, Wilson R, Goodacre S. Evaluating and implementing new services. BMJ 2006;332:109-12. https://doi.org/10.1136/bmj.332.7533.109 10.1136/bmj.332.7533.109 [DOI] [PMC free article] [PubMed] [Google Scholar]