

Abstract
Background
gp91phox, the catalytic core of NADPH oxidase (NOX) and biomarker of NOX activation, has been recently recognized as a parameter of systemic oxidative stress in several studies. Subclinical hypothyroidism (SH) is characteristic of elevated level of serum thyroid stimulating hormone (TSH) and is frequently accompanied with cholesterolemia. In this study, the levels of serum soluble gp91phox were measured to assess the oxidative stress in patients with SH. And the relationship among gp91phox, low-density lipoprotein-C (LDL-C), and TSH was also investigated.
Methods
A total of 51 subjects were enrolled and categorized into four groups: the healthy controls subjects (n = 13), controls with high level of LDL-C alone (n = 12), SH with normal level of LDL-C (n = 11), and SH with high level of LDL-C (n = 15). The related clinical and laboratory data were collected for statistical analysis. All the patients were newly diagnosed and did not take any medication. The information of lipid profile and thyroid function was extracted, and the concentrations of gp91phox were obtained with ELISA.
Results
The levels of serum soluble gp91phox evidently increased in the patients with SH with a high level of LDL-C (81.52 ± 37.00 ug/mL) as compared to the healthy controls (54.98 ± 1.83ug/mL, p < 0.001), controls with high level of LDL-C (61.21 ± 4.48 ug/mL, p=0.038) and SH with a normal level of LDL-C (62.82 ± 11.67ug/mL, p=0.027). Additionally, the levels of gp91phox showed a significant positive correlation with both the levels of LDL-C (r = 0.595, p < 0.001) and TSH (r = 0.346, p=0.013) by the Spearman correlation analyses. The correlation remained significant even when the effect of another factor was controlled (TSH: when the effect of LDL-C was controlled, r = 0.453, p=0.001; LDL-C: when the effect of TSH was controlled, r = 0.291, p=0.040). The main effect analysis showed an independent main effect of either LDL-C (p = 0.041) or TSH (p=0.022) on gp91phox without interaction (p=0.299).
Conclusions
Our work demonstrated that the levels of gp91phox, a novel biomarker for measuring the oxidative stress, were significantly elevated in the patients with SH. And LDL-C and TSH were both independent predictors of gp91phox. Abbreviations. BMI : Body mass index; TC : Total cholesterol; LDL-C : Low-density lipoprotein cholesterol; HDL-C : High-density lipoprotein cholesterol; TG : Triglyceride; FBG : Fasting blood glucose; FT3 : Free triiodothyronine; FT4 : Free thyroxine; TSH: Thyroid stimulating hormone; SBP : Systolic blood pressure; DBP : Diastolic blood pressure; SD : Standard deviation; LSD: Least significant difference.
1. Introduction
Subclinical hypothyroidism (SH) is referred to as the condition where the levels of serum thyroid stimulating hormone (TSH) are elevated and the concentrations of thyroid hormones are within the reference ranges. SH occurs in 3% to 15% of general population in the whole world, and the prevalence increased markedly in adult females [1–3]. A growing number of studies have suggested that there is an increased risk of cardiovascular diseases in patients with SH [4, 5]. Those well-documented concomitant cardiovascular risk factors in SH include hypercholesterolemia, insulin resistance, impaired endothelial function, and inflammation [6–8].
Oxidative stress, an imbalance in the equilibrium favoring the increased production of free radicals and diminished antioxidants, has been demonstrated to be elevated in SH [9]. However, the results are still scarce and somewhat controversial [10–14]. It has been correlated with a wide range of biological and pathological conditions [15], especially in the cardiovascular system [16]. NADPH oxidase (NOX), one of the most important oxidases responsible for ROS formation in the cardiovascular system, plays a pivotal role in the initiation and progression of atherosclerotic diseases [17, 18]. gp91phox, the catalytic core of NOX and marker of NOX activation, has been recognized as a parameter of systemic oxidative stress in an array of recent studies [19, 20]. However, relevant reports are still missing on the concentrations of serum soluble gp91phox in SH.
The increased intensity of oxidative stress in SH has been associated with the elevated concentrations of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) [21]. And several research groups have advocated that TSH could directly influence the oxidative stress in SH [22]. Thus, the extent of hyperthyrotropinemia in SH might be applied as an indicator not only of the severity of hypothyroidism but also of the extent of the associated lipid peroxidation [23]. Despite these findings, the relationship of oxidative stress with TSH and lipid profiles in SH has yet to be clarified to date.
Given the high prevalence of SH in the general population and undetermined correlation of oxidative stress with hyperthyrotropinemia and hyperlipidemia, we aimed to explore in this study the levels of gp91phox as well as the effects of LDL-C and TSH on gp91phox in patients with SH.
2. Materials and Methods
2.1. Study Design and Subjects
A total of 51 subjects were recruited from the Health Management Center of Shandong Provincial Hospital. All patients were newly diagnosed. To avoid the confounding effects on the oxidative stress, those subjects were excluded based on the criteria as follows: (1) with any sign of acute infection; (2) with chronic infections including chronic gastroenteritis, nephritis, bronchitis, nephritic syndrome, or autoimmune hepatitis; (3) having a history of hypertension, diabetes mellitus, coronary heart disease, malignant cancers, or cardiac/renal/hepatic/thyroid dysfunction; (4) administrated with drugs such as lipid-lowering drugs, antioxidant vitamin supplements, or hormone replacement therapy; (5) smoker, alcoholics, long-time tea drinking, and having recent heavy physical. The study was approved by the Ethics Committee of Shandong Provincial Hospital. Written informed consent was obtained from each subject prior to their enrollment to the study.
As the level of LDL-C, which is a well-known risk factor for atherosclerosis, is increased in SH, the patients with SH were further divided into two subgroups by the levels of LDL-C. In summary, these subjects were categorized into four groups: healthy control subjects (n = 13), newly control subjects with high level of LDL-C (n = 12), newly diagnosed SH with normal level of LDL-C (n = 11), and newly diagnosed SH with high level of LDL-C (n = 15). The definition of SH was an elevated TSH (>4.2 mIU/L) with normal levels of free thyroxine (FT4) (12–22 pmol/ml) and free triiodothyronine (FT3) (3.1–6.8 pmol/ml). The concentration of LDL-C higher than 3.36 mmol/L was defined as the high level, and the value of 0.5–3.36 mmol/L was regarded as the normal level.
2.2. Anthropometric Measurements
Body weight (kg) and height (cm) were measured without shoes and/or hats. The BMI was calculated as the weight (kg) divided by the height (m) squared. The blood pressure of their right arm was measured three times with a desk-model sphygmomanometer. The systolic blood pressure (SBP) and diastolic blood pressure (DBP) were both determined by the mean value of three measurements.
2.3. Sample Collection
After overnight fasting, venous blood samples were drawn and centrifuged for 20 min at 3000 rpm. The aliquots of serum samples were separated and stored at −80°C (Thermo Fischer Scientific, USA) for further analysis.
2.4. Thyroid Profiles
Thyroid profiles were assessed by measuring the levels of serum TSH, FT3, and FT4 using the chemiluminescent immunometric assay (Elecsys 2010, Roche, Basel, Switzerland). All of the intra-assay and interassay coefficients of variation were less than 5%. The reference ranges for FT3, FT4, and TSH were 3.1–6.8 pmol/ml, 12–22 pmol/ml, and 0.27–4.2 mIU/L, respectively. All the experiments were performed at the clinical laboratory of Provincial Hospital.
2.5. Lipid Profiles and FBG
Concentrations of serum fasting blood glucose (FBG), total cholesterol (TC), LDL-C, HDL-C, and triglycerides (TG) were measured using standard enzymatic methods by automated spectrophotometry on the Olympus AU5400 system (Olympus Corporation, Tokyo, Japan). The intra-assay and interassay coefficients of variation were less than 5% and 10%, respectively. The reference ranges for FBG, TC, LDL-C, HDL-C, and TG were 3.9–6.3 mmol/L, 3.6–6.2 mmol/L, 0.5–3.36 mmol/L, 0.8–1.5 mmol/L, and 0.4–1.8 mmol/L, respectively. All the above parameters were obtained from the clinical laboratory of Provincial Hospital affiliated to Shandong University.
2.6. Assay for Oxidative Stress Parameter gp91phox
The levels of serum soluble gp91phox were determined by the commercially available ELISA kits (Blue Gene Biotech, China) according to the manufacturer's instructions. 100 μL of sample was added into the antibody-coated well, and then, 50μL of conjugated solution was added into each well. After mixture and subsequent incubation for 60 minutes at 37°C, the samples were washed 5 times with washing buffer. 50 μL of enzyme substrates A and B was then added before the reaction was stopped with 50 μL of stop solution. The absorbance was read at 450 nm using a microplate reader immediately (Multiscan MS). The values were expressed in the form of ng/mL. The intra-assay and interassay coefficients of variation were 5.6% and 7.9%, respectively.
2.7. Statistical Analysis
The continuous variables were shown by the mean ± standard deviation (SD). The normal distribution was assessed by the Kolmogorov–Smirnov test. For analyzing those continuous variables, the comparisons among the four groups were examined with the parametric one-way ANOVA test followed by a least significant difference (LSD) post hoc test when the normal distribution was conformed. Otherwise, the nonparametric one-way ANOVA Kruskal–Wallis test along with pairwise comparison was applied if a skewed distribution was met. For categorical variables, a chi-squared or Fisher's exact test was selected. The correlations between the variables and gp91phox were assessed by the Spearman and partial correlation analysis. The main effect analysis and interactive analysis were performed with a univariate general linear regression analysis. All the statistical analyses were performed using the SPSS software version 17 (SPSS Inc, Chicago, IL, USA) for Windows. A two-sided p valve less than 0.05 was considered statistically significant.
3. Results
3.1. Clinical Characteristics of the Subjects
As shown in Table 1, demographic characteristics of gender, age, and BMI were matched among the four groups. The detailed information of lipid profiles (LDL-C, HDL-C, TC, and TG), FBG, and thyroid profiles (FT3, FT4, and TSH) of the four groups is also listed in Table 1. A Spearman correlation analysis revealed that the levels of TSH were positively correlated with those of LDL-C (r = 0.249, p=0.040) and TC (r = 0.262, p=0.033) in the whole population of 51 subjects (Figure 1).
Table 1.
Clinical characteristics of four groups in the study.
| Healthy controls | Controls with high LDL | SH with normal LDL | SH with high LDL | p1∗ | p2# | |
|---|---|---|---|---|---|---|
| n = 13 | n = 12 | n = 11 | n = 15 | |||
| Gender (F/M) | 10/3 | 9/3 | 9/2 | 11/3 | 0.978 | - |
| Age (years) | 50.38 ± 3.52 | 50.33 ± 4.12 | 54.09 ± 6.88 | 51.60 ± 7.60 | 0.202 | 0.423 |
| BMI (kg/m2) | 22.9 ± 2.21 | 23.15 ± 2.48 | 24.48 ± 2.62 | 24.44 ± 2.31 | 0.343 | 0.172 |
| TC (mmol/L) | 4.56 ± 0.37 | 5.41 ± 0.39 | 5.54 ± 0.53 | 6.31 ± 1.00 | <0.001 | <0.001 |
| LDL-C (mmol/L) | 2.27 ± 0.53 | 3.65 ± 0.30 | 2.86 ± 0.28 | 4.02 ± 0.61 | N/A | N/A |
| HDL-C (mmol/L) | 1.35 ± 0.13 | 1.19 ± 0.13 | 1.18 ± 0.16 | 1.45 ± 0.34 | 0.021 | 0.782 |
| TG (mmol/L) | 1.05 ± 0.34 | 1.16 ± 0.36 | 1.15 ± 0.34 | 1.40 ± 0.34 | 0.144 | 0.020 |
| FBG (mmol/L) | 5.08 ± 0.41 | 4.97 ± 0.65 | 5.50 ± 0.73 | 6.58 ± 2.18 | 0.008 | 0.169 |
| FT3 (pmol/L) | 5.20 ± 0.62 | 5.47 ± 0.36 | 4.93 ± 0.71 | 4.73 ± 0.28 | 0.002 | 0.028 |
| FT4 (pmol/L) | 16.41 ± 1.58 | 17.76 ± 1.65 | 15.36 ± 1.85 | 15.59 ± 2.04 | 0.013 | 0.397 |
| TSH (mIU/L) | 2.22 ± 0.92 | 2.19 ± 0.85 | 6.62 ± 1.98 | 7.17 ± 2.58 | N/A | N/A |
∗, nonparametric one-way Kruskal–Wallis for all the four groups; #, healthy controls vs. SH with high LDL. BMI : body mass index; TC : total cholesterol; LDL-C : low-density lipoprotein cholesterol; HDL-C : high-density lipoprotein cholesterol; TG : triglyceride; FBG : fasting blood glucose; FT3 : free triiodothyronine; FT4 : free thyroxine; TSH: thyroid stimulating hormone.
Figure 1.
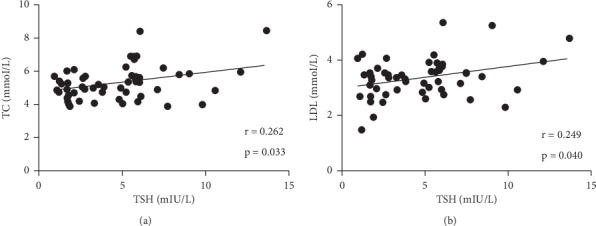
Spearman correlation analysis of TSH with (a) TC and (b) LDL-C. Spearman correlation analysis revealed that the levels of TSH were positively correlated with those of LDL-C (r = 0.249, p=0.040) and TC (r = 0.262, p=0.033) in the whole population of 51 subjects. TC : total cholesterol; LDL-C : low-density lipoprotein cholesterol; TSH : thyroid stimulating hormone.
3.2. gp91phox Levels among the Four Groups
The levels of serum soluble gp91phox evidently increased in the patients with SH with high level of LDL-C as compared to the healthy controls (81.52 ± 37.00ug/mL vs. 54.98 ± 1.83ug/mL, p < 0.001), controls with high level of LDL-C (81.52 ± 37.00ug/mL vs. 61.21 ± 4.48ug/mL, p=0.038), and SH with normal level of LDL-C (81.52 ± 37.00ug/mL vs. 62.82 ± 11.67ug/mL, p=0.027), indicating that the level of LDL-C or TSH might exert an effect on that of gp91phox. There was also a significant difference between the healthy controls and controls with high level of LDL-C (54.98 ± 1.83ug/mL vs. 61.21 ± 4.48ug/mL, p=0.002) and between the healthy controls and SH with normal level of LDL-C (54.98 ± 1.83ug/mL vs. 62.82 ± 11.67ug/mL, p=0.030). However, the levels of gp91phox were comparable between the controls with high level of LDL-C and SH with normal level of LDL-C (61.21 ± 4.48ug/mL vs. 62.82 ± 11.67ug/mL, p=0.392) (Figure 2).
Figure 2.
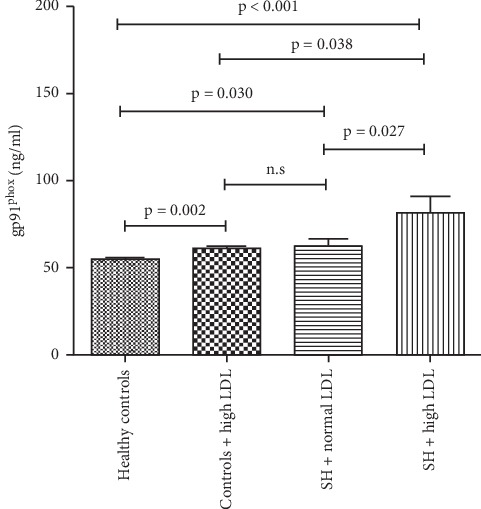
Levels of serum soluble gp91phox of four groups in the study. The levels of serum soluble gp91phox of four groups were compared, respectively. ns, not significant. LDL-C : low-density lipoprotein cholesterol; TH : subclinical hypothyroidism.
3.3. Correlation Analyses of gp91phox with TSH and LDL-C
The levels of gp91phox showed a significant correlation with both the levels of LDL-C (r = 0.595, p < 0.001) and TSH (r = 0.346, p=0.013), shown by the Spearman correlation analyses (Tables 2 and 3, Figure 3). Further partial correlation analyses showed that the correlations remained significant with the levels of TSH (when the effect of LDL-C was controlled, r = 0.453, p=0.001) and LDL-C (when the effect of TSH was controlled, r = 0.291, p=0.040) even when the effect of another factor was controlled (Table 3).
Table 2.
Spearman correlation of different variables with gp91phox.
| Variables | r | p |
|---|---|---|
| Age (years) | −0.120 | 0.400 |
| BMI (kg/m2) | 0.27 | 0.314 |
| HDL (mmol/L) | −0.004 | 0.978 |
| LDL (mmol/L) | 0.595 | <0.001 |
| TC (mmol/L) | 0.547 | <0.001 |
| FT3 (pmol/L) | −0.105 | 0.465 |
| FT4 (pmol/L) | 0.026 | 0.854 |
| TSH (mIU/L) | 0.346 | 0.013 |
| TG (mmol/L) | 0.173 | 0.225 |
| FBG (mmol/L) | 0.156 | 0.274 |
BMI : body mass index; TC : total cholesterol; LDL-C : low-density lipoprotein cholesterol; HDL-C : high-density lipoprotein cholesterol; TG : triglyceride; FBG : fasting blood glucose; FT3 : free triiodothyronine; FT4 : free thyroxine; TSH: thyroid stimulating hormone.
Table 3.
Correlation analyses between gp91phox with TSH and LDL-C.
| Correlation coefficient | Controlling factor | p | |
|---|---|---|---|
| TSH | 0.494 | — | <0.001 |
| TSH | 0.453 | LDL-C | 0.001 |
| LDL-C | 0.359 | — | 0.010 |
| LDL-C | 0.291 | TSH | 0.040 |
Spearman correlation coefficients and partial correlation coefficients of TSH and LDL-C with gp91phox were calculated. BMI : body mass index; TC : total cholesterol; LDL-C : low-density lipoprotein cholesterol; HDL-C : high-density lipoprotein cholesterol; TG : triglyceride; FBG : fasting blood glucose; FT3 : free triiodothyronine; FT4 : free thyroxine; TSH: thyroid stimulating hormone.
Figure 3.
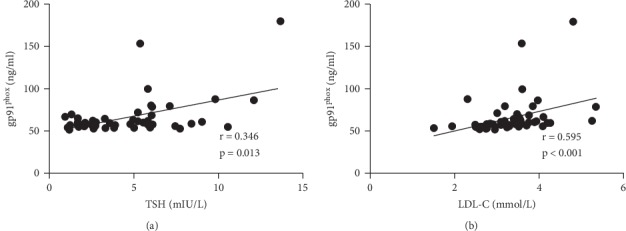
Spearman correlation of TSH and LDL-C with gp91phox. LDL-C : low-density lipoprotein cholesterol; TSH: thyroid stimulating hormone.
The main effect analysis by using a univariate general linear regression model also showed an independent main effect of either the levels of LDL-C (p=0.041) or TSH (p=0.022) on the levels of gp91phox. Besides, the interactive analysis demonstrated no interaction between the levels of LDL-C and TSH (p=0.299) in terms of the levels of gp91phox, suggesting that LDL-C and TSH were both independent predictors of gp91phox.
4. Discussion
Our study first demonstrated the elevated levels of gp91phox in SH and it advocated that SH is tightly correlated with the increased oxidative stress and risk of atherosclerosis [4, 11]. NOX family is a group of key enzymes of the innate immune system in various cell lines [24–26]. Several NOX homologs, namely, NOX1, NOX3, NOX4, and NOX5, which are relevant to the production of oxidant species, have been recently detected in the cardiovascular system [27]. One experimental study using blood cells demonstrated that 90% of serum soluble gp91phox was derived from the platelets, neutrophils, and monocytes [20]. Besides, NOX-derived superoxide anions are an effective scavenger of NO and could mediate LDL-C oxidation in atherosclerosis [25, 26, 28]. And monocytes/macrophages and platelets in the vascular walls are also one of the most significant sources of these anions. In this study, our results might shed light on a novel predictive biomarker as well as therapeutic target for measuring the oxidative stress in SH.
The influence of SH on the lipid metabolism is another debated issue. Consistent with several previous studies, our results showed the increased levels of TC and LDL-C in SH [2, 29, 30]. Similarly, our study pointed towards a positive correlation between the levels of TSH and TC and LDL-C [7, 31, 32]. One recent research also indicated a potential mechanism for hypercholesterolemia involving a direct action of TSH on the liver [33].
Accumulating evidence supported an enhanced intensity of oxidative stress in hypercholesterolemia. Several experimental and clinical studies have also shown that hypercholesterolemia is associated with the enhanced production of ROS in the endothelial cells and platelets [28, 34]. Pignatelli et al. demonstrated that the levels of gp91phox were significantly higher in the subjects with hypercholesterolemia [20]. In our study, an increased level of gp91phox was noted in the patients with SH and high level of LDL-C. And we further observed a positive correlation of the levels of LDL-C and gp91phox by the Spearman correlation analysis and partial correlation analysis, as well as an independent predictive role of LDL-C in the levels of gp91phox, by the main effect analysis and interactive analysis.
The excess TSH per se might also account for the increase in oxidative processes in SH. It is widely accepted that the endothelial dysfunction is an early step in the development of atherosclerosis and is associated with an increased risk of cardiovascular events [35]. The endothelium-dependent vasodilation impairment is characterized by the decreased nitric oxide (NO) availability and, frequently, by the increased oxidative stress [36, 37]. Recent studies have validated that TSH is able to induce IL-6 and TNF-α secretion in vitro [38, 39], which might be involved in the modulation of vascular function by increasing NO metabolites in vivo [40]. It suggests a possible link between TSH and inflammation and oxidative stress. In a recent study, the enhanced inflammation and oxidative stress have been demonstrated in the patients with differentiated thyroid carcinoma treated with high concentrations of recombinant human TSH [22]. Our study showed that the level of TSH was another independent predictive indicator of the changes in the levels of gp91phox, and it also significantly and positively correlated with the levels of gp91phox. This indicates that both hyperthyrotropinemia and dyslipidemia might indeed play an independent role in the elevation of oxidative stress level in SH. In summary, the measurement of serum gp91phox could be applied as a useful and promising biomarker and predictor to evaluate the levels of oxidative stress as well as the clinical prognosis in patients with SH.
Several limitations existed which should be paid to interpret the results in this study. First, the observational study design inevitably introduced a source of potential bias. Second, this cross-sectional study mainly reported descriptive data and does not allow to evaluate the causal relationships between the gp91phox increase and thyroid function evolution. Third, the simple sizes of the whole cohort and each subgroup were relatively small and it was a single-center study. Fourth, the level of gp91phox might be affected by other potential confounding variables.
5. Conclusions
In conclusion, our study showed an increase in the levels of gp91phox, a novel biomarker for evaluating the oxidative stress, in patients with SH. And the levels of LDL-C and TSH might both possess independent effects on the levels of gp91phox. Future multicenter prospective studies with larger cohorts are warranted to evaluate those results.
Acknowledgments
This work was supported by the Natural Science Foundation of Shandong Province (ZR2019MH025 and ZR2018BH002), National Natural Science Foundation of China (81800255), Jinan Science and Technology Development Plan (201704105), and Shandong key Research and Development plan (2017GSF18120).
Data Availability
All data generated or analyzed during this study were included in this article.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
Authors' Contributions
Xiaochun Ma and Furong Wang contributed equally to the work.
References
- 1.Biondi B., Cooper D. S. The clinical significance of subclinical thyroid dysfunction. Endocrine Reviews. 2008;29(1):76–131. doi: 10.1210/er.2006-0043. [DOI] [PubMed] [Google Scholar]
- 2.Canaris G. J., Manowitz N. R., Mayor G., Ridgway E. C. The Colorado thyroid disease prevalence study. Archives of Internal Medicine. 2000;160(4):p. 526. doi: 10.1001/archinte.160.4.526. [DOI] [PubMed] [Google Scholar]
- 3.Peeters R. P. Subclinical hypothyroidism. New England Journal of Medicine. 2017;376(26):2556–2565. doi: 10.1056/nejmcp1611144. [DOI] [PubMed] [Google Scholar]
- 4.Blum M. R., Gencer B., Adam L., et al. Impact of thyroid hormone therapy on atherosclerosis in the elderly with subclinical hypothyroidism: a randomized trial. The Journal of Clinical Endocrinology & Metabolism. 2018 Aug 1;103(8):2988–2997. doi: 10.1210/jc.2018-00279. [DOI] [PubMed] [Google Scholar]
- 5.Yang C., Lu M., Chen W., et al. Thyrotropin aggravates atherosclerosis by promoting macrophage inflammation in plaques. Journal of Experimental Medicine. 2019;216(5):1182–1198. doi: 10.1084/jem.20181473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Danese M. D., Ladenson P. W., Meinert C. L., Powe N. R. Effect of thyroxine therapy on serum lipoproteins in patients with mild thyroid failure: a quantitative review of the literature. The Journal of Clinical Endocrinology & Metabolism. 2000;85(9):2993–3001. doi: 10.1210/jcem.85.9.6841. [DOI] [PubMed] [Google Scholar]
- 7.Taddei S., Caraccio N., Virdis A., et al. Impaired endothelium-dependent vasodilatation in subclinical hypothyroidism: beneficial effect of levothyroxine therapy. The Journal of Clinical Endocrinology & Metabolism. 2003;88(8):3731–3737. doi: 10.1210/jc.2003-030039. [DOI] [PubMed] [Google Scholar]
- 8.Taddei S., Caraccio N., Virdis A., et al. Low-grade systemic inflammation causes endothelial dysfunction in patients with hashimoto’s thyroiditis. The Journal of Clinical Endocrinology & Metabolism. 2006;91(12):5076–5082. doi: 10.1210/jc.2006-1075. [DOI] [PubMed] [Google Scholar]
- 9.Marfella R., Ferraraccio F., Rizzo M. R., et al. Innate immune activity in plaque of patients with untreated and l-thyroxine-treated subclinical hypothyroidism. The Journal of Clinical Endocrinology & Metabolism. 2011;96(4):1015–1020. doi: 10.1210/jc.2010-1382. [DOI] [PubMed] [Google Scholar]
- 10.Öztürk Ü, Vural P., Özderya A., Karadağ B., Doğru-Abbasoğlu S., Uysal M. Oxidative stress parameters in serum and low density lipoproteins of hashimoto’s thyroiditis patients with subclinical and overt hypothyroidism. International Immunopharmacology. 2012;14(4):349–352. doi: 10.1016/j.intimp.2012.08.010. [DOI] [PubMed] [Google Scholar]
- 11.Cebeci E., Alibaz-Oner F., Usta M., Yurdakul S., Erguney M. Evaluation of oxidative stress, the activities of paraoxonase and arylesterase in patients with subclinical hypothyroidism. Journal of Investigative Medicine. 2012;60(1):23–28. doi: 10.2310/jim.0b013e31823581dd. [DOI] [PubMed] [Google Scholar]
- 12.Baser H., Can U., Baser S., Yerlikaya F. H., Aslan U., Hidayetoglu B. T. Assesment of oxidative status and its association with thyroid autoantibodies in patients with euthyroid autoimmune thyroiditis. Endocrine. 2015 Apr;48(3):916–923. doi: 10.1007/s12020-014-0399-3. [DOI] [PubMed] [Google Scholar]
- 13.Ruggeri R. M., Vicchio T. M., Cristani M., et al. Oxidative stress and advanced glycation end products in hashimoto’s thyroiditis. Thyroid. 2016;26(4):504–511. doi: 10.1089/thy.2015.0592. [DOI] [PubMed] [Google Scholar]
- 14.Ates I., Yilmaz F. M., Altay M., Yilmaz N., Berker D., Güler S. The relationship between oxidative stress and autoimmunity in Hashimoto’s thyroiditis. European Journal of Endocrinology. 2015;173(6):791–799. doi: 10.1530/eje-15-0617. [DOI] [PubMed] [Google Scholar]
- 15.Dursun B., Dursun E., Capraz I., Ozben T., Apaydin A., Suleymanlar G. Are uremia, diabetes, and atherosclerosis linked with impaired antioxidant mechanisms? Journal of Investigative Medicine. 2008;56(2):545–552. doi: 10.2310/jim.0b013e3181641ce3. [DOI] [PubMed] [Google Scholar]
- 16.Finkel T., Holbrook N. J. Oxidants, oxidative stress and the biology of ageing. Nature. 2000;408(6809):239–247. doi: 10.1038/35041687. [DOI] [PubMed] [Google Scholar]
- 17.Sedeek M., Hébert R. L., Kennedy C. R., Burns K. D., Touyz R. M. Molecular mechanisms of hypertension: role of nox family nadph oxidases. Current Opinion in Nephrology and Hypertension. 2009;18(2):122–127. doi: 10.1097/mnh.0b013e32832923c3. [DOI] [PubMed] [Google Scholar]
- 18.Pejenaute Á, Cortés A., Marqués J, et al. NADPH oxidase overactivity underlies telomere shortening in human atherosclerosis. International Journal of Molecular Sciences. 2020;21(4) doi: 10.3390/ijms21041434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cangemi R., Celestini A., Calvieri C., et al. Different behaviour of nox2 activation in patients with paroxysmal/persistent or permanent atrial fibrillation. Heart. 2012;98(14):1063–1066. doi: 10.1136/heartjnl-2012-301952. [DOI] [PubMed] [Google Scholar]
- 20.Pignatelli P., Carnevale R., Cangemi R., et al. Atorvastatin inhibits gp91 phox circulating levels in patients with hypercholesterolemia. Arteriosclerosis, Thrombosis, and Vascular Biology. 2010;30(2):360–367. doi: 10.1161/atvbaha.109.198622. [DOI] [PubMed] [Google Scholar]
- 21.Santi A., Duarte M. M. M. F., de Menezes C. C., Loro V. L. Association of lipids with oxidative stress biomarkers in subclinical hypothyroidism. International Journal of Endocrinology. 2012;2012:p. 7. doi: 10.1155/2012/856359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dardano A., Ghiadoni L., Plantinga Y., et al. Recombinant human thyrotropin reduces endothelium-dependent vasodilation in patients monitored for differentiated thyroid carcinoma. The Journal of Clinical Endocrinology & Metabolism. 2006;91(10):4175–4178. doi: 10.1210/jc.2006-0440. [DOI] [PubMed] [Google Scholar]
- 23.Haribabu A., Reddy V. S., Pallavi C., et al. Evaluation of protein oxidation and its association with lipid peroxidation and thyrotropin levels in overt and subclinical hypothyroidism. Endocrine. 2013 Aug;44(1):152–157. doi: 10.1007/s12020-012-9849-y. [DOI] [PubMed] [Google Scholar]
- 24.Yousefian M., Shakour N., Hosseinzadeh H., Hayes A. W., Hadizadeh F., Karimi G. The natural phenolic compounds as modulators of NADPH oxidases in hypertension. Phytomedicine. 2019;55:200–213. doi: 10.1016/j.phymed.2018.08.002. [DOI] [PubMed] [Google Scholar]
- 25.Sonkar V. K., Kumar R., Jensen M., et al. Nox2 NADPH oxidase is dispensable for platelet activation or arterial thrombosis in mice. Blood Advances. 2019;3(8):1272–1284. doi: 10.1182/bloodadvances.2018025569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sarna L. K., Wu N., Hwang S.-Y., Siow Y. L. Berberine inhibits NADPH oxidase mediated superoxide anion production in macrophagesThis article is one of a selection of papers published in a Special Issue on Oxidative Stress in Health and Disease. Canadian Journal of Physiology and Pharmacology. 2010;88(3):369–378. doi: 10.1139/y09-136. [DOI] [PubMed] [Google Scholar]
- 27.O F., Basili S., Nigro C., Pignatelli P. Role of nadph oxidase in atherosclerosis. Future Cardiology. 2009;5(1):83–92. doi: 10.2217/14796678.5.1.83. [DOI] [PubMed] [Google Scholar]
- 28.Pignatelli P., Sanguigni V., Lenti L., et al. Oxidative stress-mediated platelet CD40 ligand upregulation in patients with hypercholesterolemia: effect of atorvastatin. Journal of Thrombosis and Haemostasis. 2007;5(6):1170–1178. doi: 10.1111/j.1538-7836.2007.02533.x. [DOI] [PubMed] [Google Scholar]
- 29.Saric M. S., Jurasic M.-J., Sovic S., Kranjcec B., Glivetic T., Demarin V. Dyslipidemia in subclinical hypothyroidism requires assessment of small dense low density lipoprotein cholesterol (sdLDL-C) Romanian Journal of Internal Medicine. 2017;55(3):159–166. doi: 10.1515/rjim-2017-0015. [DOI] [PubMed] [Google Scholar]
- 30.Alamdari S., Amouzegar A., Tohidi M, et al. Hypothyroidism and lipid levels in a community based study (TTS) Int J Endocrinol Metab. 2015;14(1) doi: 10.5812/ijem.22827.e22827 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lee W.-Y., Suh J.-Y., Rhee E.-J., Park J.-S., Sung K.-C., Kim S.-W. Plasma CRP, apolipoprotein A-1, apolipoprotein B and Lp(a) levels according to thyroid function status. Archives of Medical Research. 2004;35(6):540–545. doi: 10.1016/j.arcmed.2004.08.003. [DOI] [PubMed] [Google Scholar]
- 32.Iqbal A., Jorde R., Figenschau Y. Serum lipid levels in relation to serum thyroid-stimulating hormone and the effect of thyroxine treatment on serum lipid levels in subjects with subclinical hypothyroidism: the tromso study. Journal of Internal Medicine. 2006;260(1):53–61. doi: 10.1111/j.1365-2796.2006.01652.x. [DOI] [PubMed] [Google Scholar]
- 33.Tian L., Song Y., Xing M., et al. A novel role for thyroid-stimulating hormone: up-regulation of hepatic 3-hydroxy-3-methyl-glutaryl-coenzyme a reductase expression through the cyclic adenosine monophosphate/protein kinase A/cyclic adenosine monophosphate-responsive element binding protei. Hepatology. 2010;52(4):1401–1409. doi: 10.1002/hep.23800. [DOI] [PubMed] [Google Scholar]
- 34.Rueckschloss U., Galle J., Holtz J., Zerkowski H.-R., Morawietz H. Induction of NAD(P)H oxidase by oxidized low-density lipoprotein in human endothelial cells. Circulation. 2001;104(15):1767–1772. doi: 10.1161/hc4001.097056. [DOI] [PubMed] [Google Scholar]
- 35.Heitzer T., Schlinzig T., Krohn K., Meinertz T., Münzel T. Endothelial dysfunction, oxidative stress, and risk of cardiovascular events in patients with coronary artery disease. Circulation. 2001;104(22):2673–2678. doi: 10.1161/hc4601.099485. [DOI] [PubMed] [Google Scholar]
- 36.Godo S., Shimokawa H. Endothelial functions. Arteriosclerosis, Thrombosis, and Vascular Biology. 2017;37(9):e108–e114. doi: 10.1161/atvbaha.117.309813. [DOI] [PubMed] [Google Scholar]
- 37.Maruhashi T., Kihara Y., Higashi Y. Assessment of endothelium-independent vasodilation. Journal of Hypertension. 2018;36(7):1460–1467. doi: 10.1097/hjh.0000000000001750. [DOI] [PubMed] [Google Scholar]
- 38.Antunes T. T., Gagnon A., Bell A., Sorisky A. Thyroid-stimulating hormone stimulates interleukin-6 release from 3T3-L1 adipocytes through a cAMP-protein kinase A pathway. Obesity Research. 2005;13(12):2066–2071. doi: 10.1038/oby.2005.256. [DOI] [PubMed] [Google Scholar]
- 39.Wang H.-C., Dragoo J., Zhou Q., Klein J. R. An intrinsic thyrotropin-mediated pathway of TNF-α production by bone marrow cells. Blood. 2003;101(1):119–123. doi: 10.1182/blood-2002-02-0544. [DOI] [PubMed] [Google Scholar]
- 40.Giusti M., Valenti S., Guazzini B., et al. Circulating nitric oxide is modulated by recombinant human tsh administration during monitoring of thyroid cancer remnant. Journal of Endocrinological Investigation. 2003;26(12):1192–1197. doi: 10.1007/bf03349156. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data generated or analyzed during this study were included in this article.