

Abstract
Herein, we report that nosocomial infection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may be mitigated by using surgical masks and closed looped ventilation for both non-critical and critical patients. These preventive measures resulted in no viral contamination of surfaces in negative pressure environments.
Keywords: SARS-CoV-2, COVID-19, Environmental sampling, RT-PCR
Introduction
In early 2020, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spread from China to the rest of the world, with most countries reporting nosocomial infections by the end of March.1, 2, 3 Recently, a study conducted in Singapore has explored the mode of transmission and extent of environmental contamination in ambulatory patients.4 A concurrent study revealed that turbulent gas clouds around critical patients intubated with mechanical ventilators increased the risk of viral transmission.5 While SARS-CoV-2 can be detected on stainless steel or plastic for at least 2–3 days after initial contamination,6 the actual viral load on surfaces in negative-pressure intensive care units (ICU) remains unknown. In this study, we examine viral contamination by SARS-CoV-2 positive patients on surfaces in the ICU and an ordinary ward for 9 days.
Methods
The local surfaces around three patients were tested for viral contamination. Patient 1 was an 85-year-old male patient with critically severe SARS-CoV-2 pneumonia exhibiting respiratory failure and requiring mechanical ventilation. Patient 2, a 68-year-old male, and Patient 3, a 60-year-old female, both presented simple SARS-CoV-2 bronchopneumonia. All three patients were admitted to a negative-pressure isolation room in either a medical ICU (Patient 1) or an ordinary ward with 12 air exchanges per hour (patients 2 and 3). The negative-pressure differences for the ward area to buffer area and clean corridor to buffer area were −14 to −15 Pa and −8 to −9 Pa, respectively. The ward temperature was 23.2–23.9 °C and the relative humidity was 58.3–59.7%. For Patient 1, a heat and moisture exchange (HME) filter (VH-3110 FHME, Great Group Medical CO., LTD., Taiwan) was installed between the tubing loop from the patient to the ventilator to prevent the virus entering the device. A closed suction device (T20005 PAHSCO, Pacific Hospital Supply CO., LTD., Taiwan) was also connected for sputum suction and to prevent viral transmission. A nebulizer device was omitted from this study to limit aerosolized contamination. For the two non-critical patients, surgical masks were redressed daily. All areas were cleaned daily with a 1:10 dilution of 5% sodium hypochlorite, except the floor where a dilution ratio of 1:100 was used.
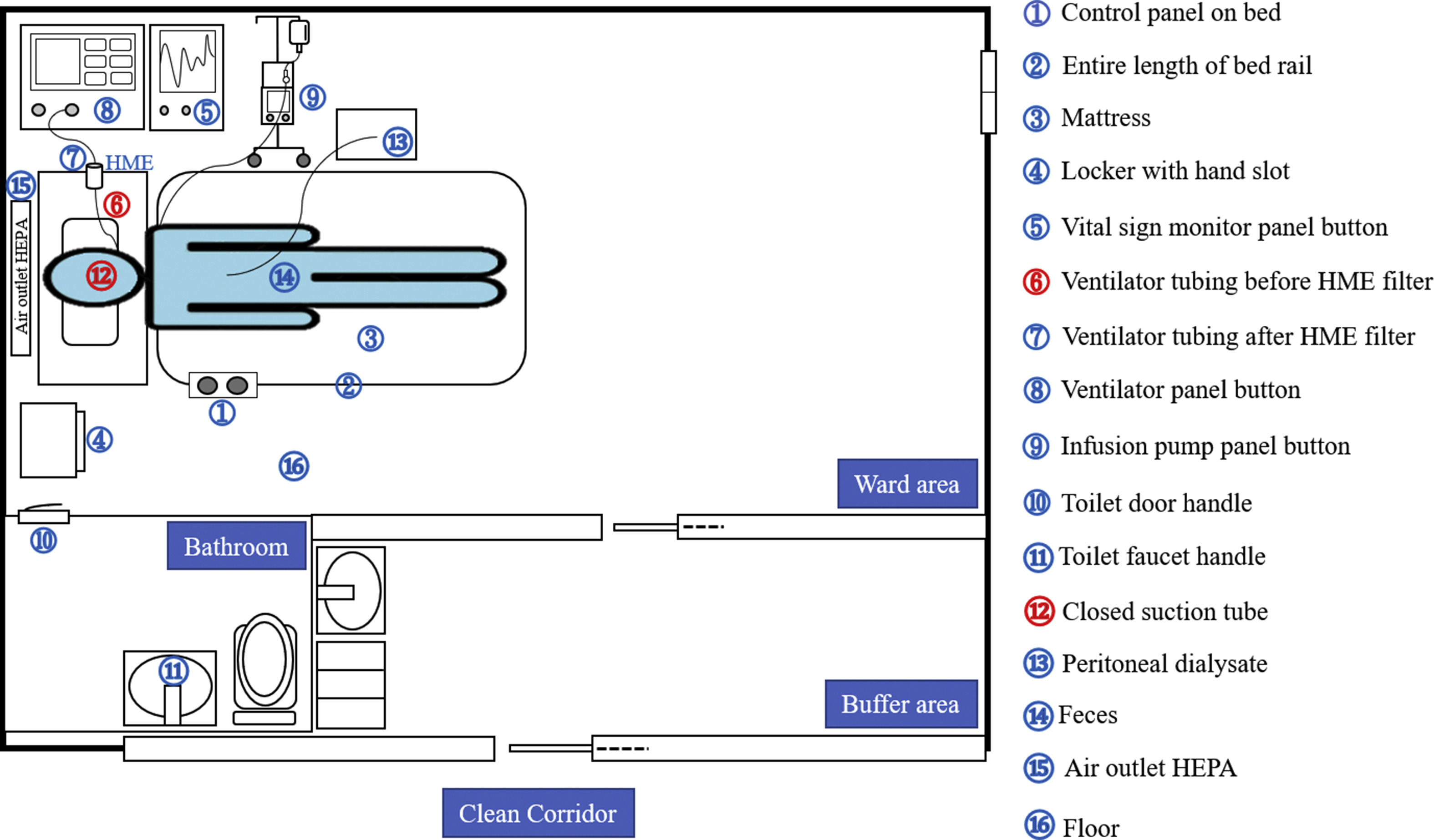
For Patient 1 in the ICU, environmental samples were collected from 16 sites (Figure S1) before routine cleaning on the same dates as throat swabs, peritoneal dialysate, and anal swabs were collected (March 9, 12, and 18, 2020). Sterile throat swabs (LIBO Specimen Collection and Transport Swabs, LIBO Medical Products Inc., Taiwan) were used for all environmental sampling and were transported in a Viral Transport Medium (CMP®, Taiwan). For the non-critical patients, environmental and clinical samples were collected from the 15 relative sites before routine cleaning on the same dates as positive throat swabs (April 2, 6, and 8, 2020). The percentage of positive results was verified through triplicate sampling at each site.
All samples were analyzed for SARS-CoV-2 using reverse transcriptase-polymerase chain reaction (RT-PCR) detection.7 Specific RT-PCR targeting of RNA-dependent RNA polymerase (RdRP), E, and N genes were used to detect the presence of SARS-CoV-2. The number of cycles required for the fluorescent signal to cross the threshold in RT-PCR (cycle threshold, Ct, values) determines the viral load with lower Ct values corresponding to higher viral loads. Samples were sent to a biosafety level 2 (BSL-2) laboratory with a built-in negative-pressure room for immediate storage at −20 °C prior to RT-PCR testing, which was conducted within three days of sampling. For the RdRP gene, a 20 μl-reaction was performed with 5 μl of template RNA and 15 μl of the PCR reaction master mix, as suggested by LightMix® Modular SARS-CoV-2 (COVID19) RdRP, and samples were detected on a Roche z480 (Roche Molecular Systems, Inc., California, US). Thermal cycling was performed at 55 °C for reverse transcription followed by initial denaturation at 95 °C for 5 min then 45 cycles of amplification at 95 °C for 5 s, 60 °C for 15 s, and 72 °C for 15 s, followed by cooling at 40 °C for 30 s. The positive findings were defined as the least significant Ct of the E and RdRP genes.
Results
Positive throat swabs for SARS-CoV-2 were obtained on three separate dates for all three patients. The corresponding environmental and clinical sample data are shown in Table 1 and Figure S1. For Patient 1, the throat swab exhibited positive RT-PCR E gene Ct values of 26.73, 28.85, and 29.86 on March 9, 12, and 18, 2020, respectively. Before routine cleaning, all environmental samples of the ICU were negative except for “Ventilator tubing before HME filter,” which was strongly positive, with an E gene Ct value of 30.41 on March 9, 2020 and 31.79 on March 12, 2020. Similarly, all clinical data exhibited negative RT-PCR results except for the closed suction tube specimen, which had Ct values of 29.52, 30.64, and 33.07 on March 9, 12, and 18, 2020, respectively.
Table 1.
RT-PCR results of environmental sampling and patient specimens.
| Sites | Patient 1 | Sites | Patient 2 | Patient 3 |
|---|---|---|---|---|
| Environmental sitesa | Positive ratec | Environmental sitesd | Positive ratec | Positive ratec |
| 1.Control panel on bed | 0/3 | 1.Control panel on bed | 0/3 | 0/3 |
| 2.Entire length of bed rail | 0/3 | 2. Entire length of bed rail | 0/3 | 0/3 |
| 3.Mattress | 0/3 | 3. Mattress | 0/3 | 0/3 |
| 4.Locker with hand slot | 0/3 | 4. Locker with hand slot | 0/3 | 0/3 |
| 5.Vital sign monitor panel button | 0/3 | 5. Light switch | 0/3 | 0/3 |
| 6.Ventilator tubing before HME filter | 2/3 | 6. Pillowcase | 0/3 | 0/3 |
| 7.Ventilator tubing after HME filter | 0/3 | 7. Curtain | 0/3 | 0/3 |
| 8.Ventilator panel button | 0/3 | 8. Kettle handle | 0/3 | 0/3 |
| 9.Infusion pump panel button | 0/3 | 9. Infusion stand | 0/3 | 0/3 |
| 10.Toilet door handle | 0/3 | 10. Toilet door handle | 0/3 | 0/3 |
| 11.Toilet faucet handle | 0/3 | 11. Toilet faucet handle | 0/3 | 0/3 |
| 15.Air outlet HEPA | 0/3 | 15. Air outlet HEPA | 0/3 | 0/3 |
| 16.Floor | 0/3 | 16. Floor | 0/3 | 0/3 |
| Clinical datab | Clinical datab | |||
| 12.Closed suction tube | 3/3 | 12. Surgical Mask | 2/3 | 2/3 |
| 13.Peritoneal dialysate | 0/3 | 13.Gargling fluid | 0/3 | 0/3 |
| 14.Anal swab | 0/3 |
Abbreviations: RT-PCR, reverse transcriptase-polymerase chain reaction; HME, heat and moisture exchange; HEPA, high-efficiency particulate absorption.
Environmental samples were collected around the patient where contamination may have been induced by the medical team.
Clinical data specimens were collected from potential virus transmission routes near the patient.
Calculated number of positive results out of three examinations on separate dates.
Environmental samples were collected around the patient where contamination may have been induced by patients themselves.
The throat swabs from Patient 2 exhibited positive RT-PCR results with E gene Ct values of 23.46, 28.97, and 27.77 on April 2, 6, and 8, 2020, respectively. The E gene Ct values of 26.83, 28.37, and 29.31 on April 2, 6, and 8, 2020, respectively, were detected for non-critical Patient 3. In the same situation, before routine cleaning, all environmental samples of the ordinary wards were negative except for “surgical mask,” which was weakly positive, with Ct values of 33.62, 36.24 on April 2, 2020 and 34.82, 37.35 on April 6, 2020.
Discussion
Viral load was undetectable with a daily routine cleaning using standard sodium hypochlorite, regardless if it was the ICU or an ordinary ward. These results contrast with those of Ong et al.,4 which might be explained by two critical differences in testing. First, the patient in the ICU was bed-ridden; thus, he was unable to contaminate the ward environment. The virus present in the patient's phlegm was contained by the closed suction tube and the HME filter with closed-loop ventilation.8 The negative anal swab and peritoneal fluid also indicated no possibility of contamination from the toilet.
Similarly, the surgical masks worn by patients 2 and 3 at all times, except when eating, contained the virus. Secondly, the medical team treating all three patients wore personal protective equipment when entering the negative-pressure ward, as well as two to three sets of gloves.9 , 10 The outermost gloves were changed or washed with 75% alcohol after performing the upper airway procedure or touching any secretions from the patients. We concluded that well documented environmental cleaning and the upper airway protection device successfully contained the viral spread. These findings suggest that upper airway containments, such as masks and filters on ventilators, can prevent nosocomial infection of medical personnel with SARS-CoV-2.
Funding/support
The study was supported by a grant from the Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (TCRD-TPE-109-16). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
The authors would like to acknowledge Miaw-Chi Peng, MSc, who performed the environmental sampling in the COVID-19 negative-pressure ICU and ordinary ward. We also acknowledge Hui-Ching Hang, MSc, who conducted nucleic acid extraction and RT-PCR detection of SARS-CoV-2. Both work at the Department of Pathology and Laboratory Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei, Taiwan.
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.jmii.2020.05.002.
Appendix A. Supplementary data
The following is the Supplementary data to this article:
Room layout of the negative-pressure ward in the medical intensive care unit. Numbered labels correspond to environmental sampling sites listed in Table 1. Red circles indicate samples with positive results, and blue circles indicate samples with negative results.
{kind=link}
References
- 1.Wu Z., McGoogan J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. J Am Med Assoc. 2020;323:1239–1242. doi: 10.1001/jama.2020.2648. [DOI] [PubMed] [Google Scholar]
- 2.Lee C.-Y., Wang P.-S., Huang Y.-D., Lin Y.-C., Hsu Y.-N., Chen S.-C. Evacuation of quarantine-qualified nationals from Wuhan for COVID-19 outbreak – Taiwan experience. J Microbiol Immunol Infect. 2020;53(3):392–393. doi: 10.1016/j.jmii.2020.03.023. S1684-1182(20)30083-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lau H., Khosrawipour V., Kocbach P., Mikolajczyk A., Ichii H., Zacharski M. The association between international and domestic air traffic and the coronavirus (COVID-19) outbreak. J Microbiol Immunol Infect. 2020;53(3):467–472. doi: 10.1016/j.jmii.2020.03.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ong S.W.X., Tan Y.K., Chia P.Y., Lee T.H., Ng O.T., Wong M.S.Y. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. J Am Med Assoc. 2020;323:1610–1612. doi: 10.1001/jama.2020.3227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bourouiba L. Turbulent gas clouds and respiratory pathogen emissions: potential implications for reducing transmission of COVID-19. J Am Med Assoc. 2020;323:1837–1838. doi: 10.1001/jama.2020.4756. [DOI] [PubMed] [Google Scholar]
- 6.van Doremalen N., Bushmaker T., Morris D.H., Holbrook M.G., Gamble A., Williamson B.N. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020;382:1564–1567. doi: 10.1056/NEJMc2004973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Corman V.M., Landt O., Kaiser M., Molenkamp R., Meijer A., Chu D.K.W. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020;25:2000045. doi: 10.2807/1560-7917.ES.2020.25.3.2000045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Liu Y., Li J., Feng Y. Critical care response to a hospital outbreak of the 2019-nCoV infection in Shenzhen, China. Crit Care. 2020;24:56. doi: 10.1186/s13054-020-2786-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chen F.-M., Feng M.-C., Chen T.-C., Hsieh M.-H., Kuo S.-H., Chang H.-L. Big data integration and analytics to prevent a potential hospital outbreak of COVID-19 in Taiwan. J Microbiol Immunol Infect. 2020 doi: 10.1016/j.jmii.2020.04.010. S1684-1182(20)30104-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Huang H.-T., Chen T.-C., Liu T.-Y., Chiu C.-F., Hsieh W.-C., Yang C.-J. How to prevent outbreak of a hospital-affiliated dementia day-care facility in the pandemic COVID-19 infection in Taiwan. J Microbiol Immunol Infect. 2020 doi: 10.1016/j.jmii.2020.04.007. S1684-1182(20)30101-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Room layout of the negative-pressure ward in the medical intensive care unit. Numbered labels correspond to environmental sampling sites listed in Table 1. Red circles indicate samples with positive results, and blue circles indicate samples with negative results.