

Abstract
Objectives:
The aim of this study was to determine the antibiotic resistance profile, clonal relation and efficacy of antibiotic combinations in nosocomial multidrug resistant (MDR) Acinetobacter baumannii.
Materials and Methods:
Antibiotic susceptibilities of 84 MDR A. baumannii against tigecycline (TGC), colistin (CL), amikacin (AK), ciprofloxacin (CIP), meropenem (MR), moxifloxacin (MXF), rifampicin (RF) were determined by microdilution method. Clonal relationship was investigated by genotyping using AP-PCR and antibiotyping. Interactions of antibiotic combinations were tested against clonally unrelated strains by the checkerboard (CB) method. The efficacy of the best combinations was also assesed on a selected isolate by the time-kill (TK) method.
Results:
CIP, RF, MXF, MR, AK resistance was found as 90.47%; 47.62%; 22.62%; 58.33%; 50% respectively; however; CL and TGC were not ascertained. The isolates were distinguished as 25 different antibiotypes and 15 varied molecular patterns. The best synergistic effect was detected in combinations of CL with RF (100%) and MR (100%), in combinations of TGC with RF (53%) against clonally unrelated 15 MDR A. baumannii isolates by the CB method. While CL-RF and CL-MR showed synergy by TK method like CB, on the other hand TGC-RF indicated additive interactions by TK.
Conclusion:
In this study, both synergy tests showed that CL in combination with RF would be a good option in MDR A. baumannii.
Keywords: Acinetobacter, AP-PCR, checkerboard, time-kill, tigecycline, colistin
INTRODUCTION
Acinetobacter baumannii is an opportunistic pathogen and causes hospital acquired infections such as bacteremia, septicemia, and ventilator associated pneumonia.1,2,3 Before the 1970s, A. baumannii was susceptible to most traditional antibiotics such as broad spectrum beta-lactams, cephalosporins and tetracyclines. In recent years Acinetobacter related infections have been eradicated with difficulty in general by using single antimicrobial agent because of the ability of the bacteria to develop resistance. Especially multidrug resistant (MDR) A. baumannii has been continuously reported as nosocomial pathogen which causes significant morbidity and mortality in critically ill patients.4,5
Carbapenems are considered the drugs of choice for the treatment of serious infections caused by MDR A. baumannii. However carbapenem-resistant A. baumannii has been reported worldwide.6 As a result of this increasing carbapenem resistance, alternative antibiotic classes have become part of treatment.1 Of these alternative classes, polymyxin and tigecycline (TGC) remain the most active treatments in vitro against MDR A. baumannii but resistance against these antibiotics is also reported.4,6,7,8 Combination therapy is often used in the treatment of MDR A. baumannii infections to prevent the emergence of resistance and obtain a synergistic effect.1,3,8
The aim of this study was to determine the antimicrobial resistance profile, clonal relation and efficacy of antimicrobial combinations on nosocomial MDR A. baumannii.
EXPERIMENTAL
Microorganisms
Identifications and antibiotic susceptibilities of Acinetobacter spp. isolates were elicited by Phoenix TM 100 (BD, United States) at the Clinical Microbiology Laboratory of İzmir Katip Çelebi University Atatürk Training and Research Hospital, between 2009-2010, and 84 MDR Acinetobacter spp. isolates were selected for the study. Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as control strains.
Determination of minimum inhibitory concentrations and antibiotypes
Minimum inhibitory concentrations (MICs) of TGC (Pfizer, İstanbul, Turkey), colistin (CL) (Sigma-Aldrich, USA), amikacin (AK) (Eczacıbaşı, İstanbul, Turkey), ciprofloxacin (CIP) (Koçak, İstanbul, Turkey), meropenem (MR) (Astra Zeneca, İstanbul, Turkey), moxifloxacin (MXF) (Bayer, İstanbul, Turkey) and rifampicin (RF) (Koçak, İstanbul, Turkey) antibiotics against the isolates were indicated by broth microdilution method according to “Clinical and Laboratory Standards Institute (CLSI)”.9 Because, CLSI has not suggested available breakpoints, the United States Food and Drug Administration (2005) susceptibility breakpoints for TGC, and the recommendations of Principe et al.7 for MXF and RF were utilized. By considering MIC values, the isolates were classified into different antibiotype groups.
Molecular typing
Epidemiologic relations were investigated genetically with M13 universal primers by Arbitrarily-primed polymerase chain reaction (AP-PCR).10,11 To obtain crude DNA extracts, freshly cultured bacterial colony suspensions in sterile distilled water were heated for 10 min at 95°C, cooled on ice, and centrifuged at 12.000 g. For totally 50 µL volume PCR mix, 2 mM primers, 200 µM dNTP’s together with 1 U of Taq polymerase (Fermentas) were used. M13 primers [5’-GTA AAA CGA CGG CCA GTG AA-3’ (forward amplification primer) and 5’-GGA AAC AGC TAT GAC CAT GA-3’ (reverse amplification primer)] were purchased from Fermentas. The PCR conditions were as follows: 2 cycles of 94°C for 5 min, 40°C for 5 min, 72°C for 5 min followed by 40 cycles of 94°C for 1 min, 40°C for 1 min, and 72°C for 2 min. PCR end products were examined by a ultraviolet transilluminator after electrophoresis for 60 min on 1.5 percent (wt/vol) agarose gels. The genotypes were interpreted according to the band patterns of DNA marker.
Efficacy of the antibiotic combinations
Chequerboard (CB) method: Activity of TGC and CL combination, and combinations of these antibiotics individually with AK, CIP, MR, MXF, RF against clonally unrelated 15 MDR A. baumannii isolates were tested. In vitro interactions by fractional inhibitory concentration index (FICI) of each agent was calculated as a ratio of MIC when used in combination and MIC when used alone. For each antibiotic, seven concentrations (8X MIC, 4X MIC, 2X MIC, MIC, MIC/2, MIC/4 ve MIC/8) were investigated. FICI were interpreted as synergistic, indifference, additivity and antagonism. FICI was interpreted as follows: synergy FICI≤0.5, additivity/indifference 0.5<FICI≤4 and antagonism FICI>4.0.7,12
Time-kill (TK) method: Effective combinations found by the CB method were also approved by TK method against one of the test isolates. TK studies were performed in flasks containing Mueller Hinton Broth (Merck, Darmstadt, Germany) at 37°C. Samples were removed at 0th, 6th, and 24th h of incubation from the test and growth-control cultures and appropriately diluted and inoculated onto Mueller-Hinton Agar (Merck, Darmstadt, Germany) plates. After incubation at 37°C for 24-48 h, bacterial colonies were counted. All TK studies were performed twice. Synergy or antagonism was defined as an increase or decrease of at least 100-fold compared to the effect of the most active agent singly and an increase of 100 times less than additive interaction.12
RESULTS
While 25 different antibiotypes were observed according to antibiotic resistance profiles of 84 MDR Acinetobacter spp. isolates, 15 different patterns were distinguished by AP-PCR with M13 primers. Thirty six (43%) isolates showed similar genetic pattern and 22 of these isolates were found in the same resistance pattern according to antibiotype groups and the band patterns of 50 bp DNA marker (Table 1) (Figure 1).
Table 1. The distribution of A. baumannii isolates according to antibiotypes and genotypes.
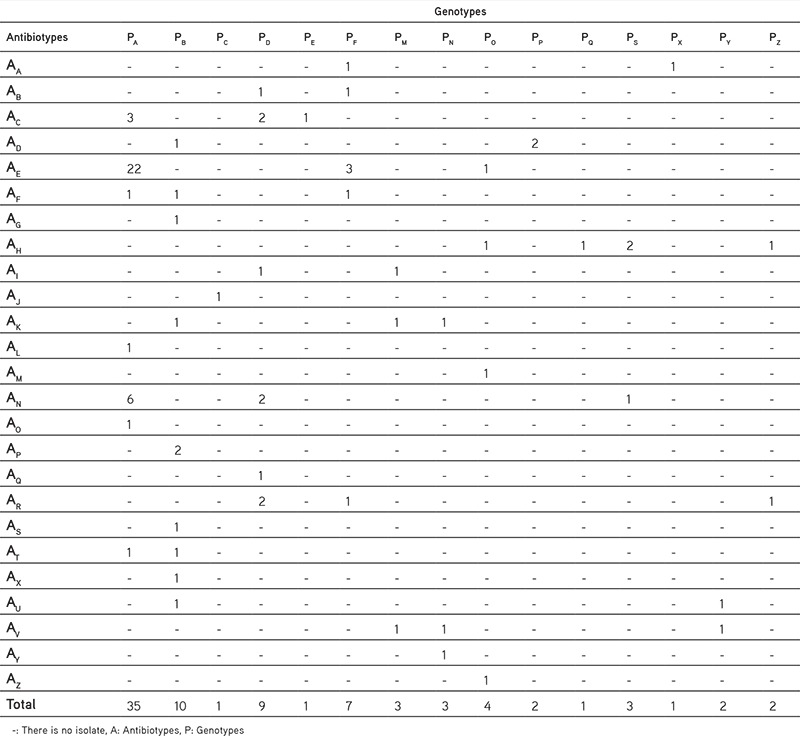
Figure 1.
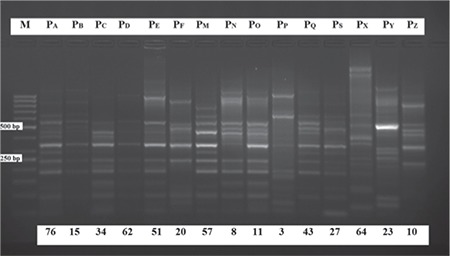
Genotypes of A. baumannii isolates to 15 different band patterns obtained by arbitrarily primed-polymerase chain reaction with M-13 primers
M: 50 bp DNA marker
Resistance rates in 84 MDR Acinetobacter spp. isolates against CIP, RF, MXF, MR, AK were found as 90.47%; 47.62%; 22.62%; 58.33%; 50% respectively. CL and TGC resistance were not found.
CL in combination with MR and RF demonstrated higher levels of synergy than the other antibiotics according to the CB method. As shown in Table 2, the best synergistic effect was detected in the CL combinations for CL-RF (100%), CL-MR (100%), in the TGC combinations for TGC-RF (53%) combinations. The lowest synergy was seen in the CL combinations for CL-AK (47%) and seen in the TGC combinations for TGC-CIP (20%). Generally, the combinations with TGC demonstrated a higher rate of additive interaction in compared with the CL combinations. Antagonistic interaction was observed between TGC-CL (20%), TGC-AK (6%), TGC-MXF (6%) and CL-CIP (6%) (Table 2).
Table 2. In vitro effects of antibiotic combinations against 15 A. baumannii isolates according to the checkerboard method.

TGC-RF combination (0.015-2 µg/mL) indicated synergy according to the CB method, but it indicated additive interactions by the TK method. Besides, CL-RF (0.06-0.25 µg/mL) and CL-MR (0.03-0.12 µg/mL) combinations showed a synergistic effect when considering both CB and TK methods. TGC-CL combination (0.03-0.5 µg/mL) was found as additive according to the CB method, but that combination demonstrated synergistic effect at 3th and 6th hours and an additive effect at 24 h as to the TK method. The synergistic effect of CL-RF (0.06-0.25 µg/mL) combination by the TK method was demonstrated in the Figure 2.
Figure 2.
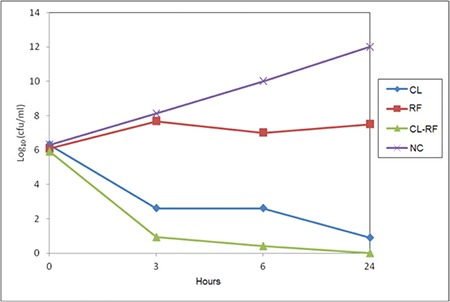
The synergistic effect of CL-RF (0.06-0.25 μg/mL) combination against A. baumannii in 3., 6. and 24. hours by time-kill method
CL: Colistin, RF: Rifampicin, NC: Negative growth control without antibiotics
DISCUSSION
Antibiotic susceptibility testing and molecular typing are necessary for the monitoring and treatment of infections caused by Acinetobacter species that become resistant against many antibiotics easily through more than one mechanism. AP-PCR is a quite common PCR-based genotyping method currently because it is easily applicable, is easily distinguishable and provides quick results. It is reported in some studies that the use of M13 universal primers in the AP-PCR generates more distinct band patterns, gives good results and has quite good distinguishing ability is quite good.13,14 In this study 15 different band patterns were detected according to AP-PCR method by using M13 universal primers. Almost 8-15 bands were obtained after the gel electrophoresis of the PCR products. The number of the bands was found sufficient to determine clonally associated strains. To see the reproducibility of the results, the trials were triplicated. Similar to recent studies,10,15 our results showed intense clonal spread of resistant A. baumannii strains in the intensive care units (80%), particularly. The isolates in the same or close antibiotic resistance patterns were often observed in the same clonal group according to molecular classification with AP-PCR. It was considered that isolation dates and locations in the hospital of A. baumannii isolates resulted in different molecular clones.
The most important issue in the Acinetobacter infections is the development of resistance against many kinds of antibiotics including primarily preferred carbapenems, CL and sulbactam.16 Due to the difficulties in the treatment of hospital-acquired infections, broad spectrum antibiotics are commonly chosen. Thus, causative strains become resistant easily. Consequently, new treatment alternatives have been required. TGC, a promising semisynthetic tetracycline, is considered as first choice of the new drugs for the therapy of carbapenem-resistant A. baumannii infections. This broad-spectrum antibiotic is shown to be highly effective against MDR Acinetobacter spp. isolates.16,17,18,19 However, several studies have currently reported decreased susceptibility to TGC. Certain in vivo and in vitro researches also highlighted developed resistance to sub-MIC concentrations of TGC. CL is shown as the only effective antibiotic against MDR A. baumannii in many countries that have not used TGC yet. In recent years, CL again has become a current issue for the treatment of infections caused by Acinetobacter species resistant to all antibiotics except CL. However, there are some major disadvantages of CL when used alone, because of its pharmacokinetic properties, side effects and fast, easy improvement of resistance. Thus, combined use of antibiotics is recommended to prevent the development of resistance and increase the success in the treatment of MDR A. baumannii infections since.7,19,20
Recent studies in Turkey found that imipenem-netilmicin,21 RF-ampicillin/sulbactam,22 CL-TGC,23 CL-vancomycin3 in combination showed synergistic interaction, and they were considered as strong choices in the treatment of infections caused by MDR A. baumannii.
In this study, the interactions of TGC and CL combinations with different antibiotics; AK, CIP, MR, MXF, RF and each other were investigated by CB and TK methods. The best synergistic effect was detected in the CL combinations by CB method, for CL-RF (100%), CL-MR (100%), and in the TGC combinations for TGC-RF (53%). Besides, synergy between TGC and CL was found as 46%.
We also compared the results of CB and TK methods for one of the tested strains. Synergy was determined for the combinations CL with RF and MR by both CB and TK methods. While TGC-RF combination showed synergy by CB, additive interaction was shown by TK method. Percin et al.3 (2014) investigated CL-vancomycin combinations because of good efficacy by TK as well as CB method, and found consistency of both the results.
Interaction of levofloxacin and CIP alone and their combinations with ceftazidime, cefepime, imipenem, piperacillin/tazobactam AK was investigated in a synergy study conducted in 2005, where 5 Acinetobacter spp. were evaluated. The highest synergy was seen in beta-lactam-fluoroquinolone and fluoroquinolone-AK combinations.24 While in a study conducted in 2011, Tan et al.8 detected rate of synergy by CB method between polymyxin B-RF and TGC-RF as 19%, those between polymyxin B-TGC was 12%. The same rates obtained by TK methods were 56%, 19% and 44% respectively. When all studied strains were evaluated, the observed synergy rate was 40% by TK method and 17% by the checkerboard method. According to these results, researchers have noted that the best observed in vitro synergy rate by TK method was between polymyxin B-RF combination. In a study conducted with 31 MDR and polymyxin B-sensitive A. baumannii isolates, Lim et al.25 reported that the best level of bactericidal activity at 24th hour is in polymyxin B-RF combination (42%), whereas the TGC-RF combination shows very low levels by TK method. In a study conducted by using TK method, initially antagonism was observed in TGC-polymyxin B combination, then variable action was seen where as no interaction was determined when other antibiotics were combined with TGC.26 In 2013 Lee et al.4 investigated by TK method the interaction of CL-RF combination for the first time by changing CL concentrations within in vitro pharmacodynamic and pharmacokinetic model in aim to achieve clinical concentrations. They observed that this combination prevents the expression of CL resistant subpopulations in CL- susceptible and -resistant MDR A. baumannii. In a study conducted in 2012, it was emphasized that the use of inappropriate antibiotic combination increases CL resistance.27
Principe et al.7 for the first time reported that they have noticed the synergy between TGC and CL by TK method in one A. baumannii isolate. In two studies conducted by CB method in TGC-CL combination28 and in TGC-sulbactam, TGC-CL combinations29 a synergistic effect was observed.
With regard to the assessment of the interaction of the combination used in our study, only one of the 15 strains tested by CB method has also been evaluated by TK method and similar results were obtained with both methods in this strain.
In 2015 a meta-analysis evaluated several studies. It was noted that CL showed in vitro synergy and bactericidal activity with many antibiotics against MDR A. baumannii strains, especially RF and carbapenem combinations suppressed CL resistance and synergy was observed at over 50% in CL-resistant strains. Synergy rates according to TK method were higher than CB and E-test methods. However, researchers underlined that in vivo studies to support in vitro studies are insufficient, because some factors like host immune response, bacterial virulence, infection site and antibiotics concentration can alter the effect of the combination of antibiotics. Thus it was declared that there is a need for randomized clinical trials to support the in vitro studies.5,6,30
CONCLUSION
Today, various methods have been developed for investigation of antibiotic combinations; but there is not a standard approach yet. In this study, both synergy tests showed that CL in combination with RF would be a good option in the treatment of MDR A. baumannii infections. Although both methods pose some difficulties such as high work-load, the length of time involved and working with the lowest concentration of antibiotic, they are useful when the reliable results are considered. However, those in vitro studies should be supported by in vivo studies to determine effective new combinations.
Acknowledgments
This study was supported as an Ege University Scientific Research Project (10ECZ023). The authors would like to thank to Prof. Zeki Topçu for helping in molecular part of the study.
Footnotes
Conflict of Interest: No conflict of interest was declared by the authors.
References
- 1.Hagihara M, Housman ST, Nicolau DP, Kuti JL. In vitro pharmacodynamics of polymyxin B and tigecycline alone and in combination against carbapenem-resistant Acinetobacter baumannii. Antimicrob Agents Chemother. 2014;58:874–879. doi: 10.1128/AAC.01624-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.O’Hara JA, Ambe LA, Casella LG, Townsend BM, Pelletler ML, Ernst RK. Activities of vancomycin-containing regimens against colistin-resistant Acinetobacter baumannii clinical strains. Antimicrob Agents Chemother. 2013;57:2103–2108. doi: 10.1128/AAC.02501-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Percin D, Akyol S, Kalın G. In vitro synergism of combinations of colistin with selected antibiotics against colistin-resistant Acinetobacter baumannii. GMS Hyg Infect Control. 2014;9:Doc14. doi: 10.3205/dgkh000234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lee HJ, Bergen PJ, Bulitta JB, Tsuji B, Forrest A, Nation RL, Li J. Synergistic activity of colistin and rifampin combination against multidrug-resistant Acinetobacter baumannii in an in vitro pharmacokinetic/pharmacodynamic model. Antimicrob Agents Chemother. 2013;57:3738–3745. doi: 10.1128/AAC.00703-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ni W, Shao X, Di X, Cui J, Wang R, Lui Y. In vitro synergy of polymyxins with other antibiotics for Acinetobacter baumannii: A systematic review and meta-analysis. Int J Antimicrob Agents. 2015;45:8–18. doi: 10.1016/j.ijantimicag.2014.10.002. [DOI] [PubMed] [Google Scholar]
- 6.Al-Shaer M, Nazer LH, Kherallah M. Rifampicin as adjunct to colistin therapy in the treatment of multidrug-resistant Acinetobacter baumannii. Ann Pharmacother. 2014;48:766–771. doi: 10.1177/1060028014528306. [DOI] [PubMed] [Google Scholar]
- 7.Principe L, D’Arezzo S, Capone A, Petrosillo N, Visca P. In vitro activity of tigecycline in combination with various antimicrobials against multidrug resistant Acinetobacter baumannii. Ann Clin Microbiol Antimicrob. 2009;8:18. doi: 10.1186/1476-0711-8-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tan TY, Lim TP, Lee WHL, Sasikala S, Hsu LY, Kwa AL. In vitro antibiotic synergy in extensively drug-resistant Acinetobacter baumannii: the effect of testing by time-kill, checkerboard, and E test methods. Antimicrob Agents Chemother. 2011;55:436–438. doi: 10.1128/AAC.00850-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.No authors listed. Clinical and Laboratory Standards Institute. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically .Approved Standard, 7th ed. CLSI document M7-A7, Wayne, PA, USA. 2006;p:1–17. [Google Scholar]
- 10.Prashanth K, Badrinath S. Epidemiological investigation of nosocomial Acinetobacter infections using arbitrarily primed PCR & pulse field gel electrophoresis. Indian J Med Res. 2005;122:408–418. [PubMed] [Google Scholar]
- 11.Ayan M, Durmaz R, Aktaş E, Durmaz B. Bacteriological, clinical and epidemiological characteristics of hospital-acquired Acinetobacter baumannii infection in a teaching hospital. J Hosp Infect. 2003;54:39–45. doi: 10.1016/s0195-6701(03)00076-8. [DOI] [PubMed] [Google Scholar]
- 12.Pillai SK, Mollering RC, Eliopoulos GM. Antimicrobial combinations, in Antibiotics in Laboratory Medicine, Ed: V. Lorian, pp. 365-440, Williams and Wilkins, New York. 2005. [Google Scholar]
- 13.Schreckenberger PC, Daneshvar MI, Weyant RS. Acinetobacter, Achromobacter, Chryseobacterium, Moraxella, and other nonfermentative gram-negative rods, in: Manuel of Clinical Microbiology, Eds: P. R. Murray, E.J. Baron, M.A. Pfaller, M.L. Landry, J.H. Jorgensen, p. 770, ASM Press, Washington DC. 2007. [Google Scholar]
- 14.Vila J, Marcos MA, Jimenez De Anta MT. A comparative study of different PCR-based DNA fingerprinting techniques for typing of the Acinetobacter calcoaceticus-A. baumannii complex. J Med Microbiol. 1996;44:482–489. doi: 10.1099/00222615-44-6-482. [DOI] [PubMed] [Google Scholar]
- 15.Ranjbar R, Sadeghifard N, Ahmadi A. Antimicrobial susceptibility and AP-PCR typing of Acinetobacter spp. strains. Iranian J Pub Health. 2007;36:50–56. [Google Scholar]
- 16.Zer Y, Özgür Akın FE, Namıduru M. Acinetobacter baumannii suşlarında tigesiklin etkinliğinin araştırılması. Infeks Derg. 2007;21:193–196. [Google Scholar]
- 17.Kuşcu F, Öztürk DB, Tütüncü EE, Uslu M, Gürbüz Y, Gülen G, Şencan İ. Çoğul antibiyotik dirençli Acinetobacter baumannii izolatlarında tigesiklin duyarlılık oranlarının E-Test yöntemiyle araştırılması. KLİMİK Derg. 2009;22:48–51. [Google Scholar]
- 18.Navon-Venezia S, Leavitt A, Carmeli Y. High tigecyline resistance in multidrug-resistant Acinetobacter baumannii. J Antimicrob Chemother. 2007;59:772–774. doi: 10.1093/jac/dkm018. [DOI] [PubMed] [Google Scholar]
- 19.Özdemir M, Erayman İ, Gündem NS, Baykan M, Baysal B. Hastane infeksiyonu etkeni Acinetobacter suşlarının çeşitli antibiyotiklere duyarlılıklarının araştırılması. ANKEM Derg. 2009;23:127–132. [Google Scholar]
- 20.Li J, Nation RL, Turnidge JD, Milne RW, Coulthard K, Rayner CR, Paterson D. Colistin: the re-emerging antibiotic for multidrug-resistant gramnegative bacterial infections. Lancet Infect Dis. 2006;6:589–601. doi: 10.1016/S1473-3099(06)70580-1. [DOI] [PubMed] [Google Scholar]
- 21.Gazi H, Tünger Ö, Vural Ş, Özbakkaloğlu B, Sürücüoğlu S. Çeşitli antibiyotik kombinasyonlarının çoğul dirençli Acinetobacter baumannii suşlarına in vitro etkileri. Türk Mikrobiyol Cem Derg. 2007;37:11–1. [Google Scholar]
- 22.Cetin ES, Tekeli A, Ozseven AG, Us E, Cicioglu Aridogan B. Determination of in vitro activities of polymyxin b and rifampin in combination with ampicillin/sulbactam or cefoperazone/sulbactam against multidrugresistant Acinetobacter baumannii by the E-test and checkerboard methods. Jpn J Infect Dis. 2013;66:463–468. doi: 10.7883/yoken.66.463. [DOI] [PubMed] [Google Scholar]
- 23.Karaoglan I, Zer Y, Bosnak VK, Mete AO, Namıduru M. In vitro synergistic activity of colistin with tigecycline or b-lactam antibiotic/b-lactamase inhibitör combinations against carbapenem-resistant Acinetobacter baumannii. J Int Med Res. 2013;41:1830–1837. doi: 10.1177/0300060513496172. [DOI] [PubMed] [Google Scholar]
- 24.Drago L, De Vecchi E, Nicola L, Tocalli L, Gismondo MR. In vitro selection of resistance in Pseudomonas aeruginosa and Acinetobacter spp. by levofloxacin and ciprofloxacin alone and in combination with betalactams and amikacin. J Antimicrob Chemother. 2005;56:353–359. doi: 10.1093/jac/dki204. [DOI] [PubMed] [Google Scholar]
- 25.Lim TP, Tan TY, Lee W, Sasikala S, Tan TT, Hsu LY, Kwa AL. In vitro activity polymyxin B, rifampisin, tigecycline alone and in combination against carbapenem resistant Acinetobacter baumannii in Singapore. PLoS One. 2011;6:e18485. doi: 10.1371/journal.pone.0018485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Scheetz MH, Qi C, Warren JR, Postelnick MJ, Zembower T, Obias A, Noskin GA. In vitro activities of various antimicrobials alone and in combination with tigecycline against carbapenem-intermediate or resistant Acinetobacter baumannii. Antimicrob Agents Chemother. 2007;51:1621–1626. doi: 10.1128/AAC.01099-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Vidaillac C, Benichou L, Duvala RE. In vitro synergy of colistin combinations against colistin-resistant Acinetobacter baumannii, Pseudomonas aeruginosa, and Klebsiella pneumoniae isolates. Antimicrob Agents Chemother. 2012;56:4856–4861. doi: 10.1128/AAC.05996-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dong X, Chen F, Zhang Y, Liu H, Liu Y, Ma L. In vitro activities of rifampin, colistin, sulbactam and tigecycline tested alone and in combination against extensively drug-resistant Acinetobacter baumannii. J Antibiot (Tokyo). 2014;67:677–680. doi: 10.1038/ja.2014.99. [DOI] [PubMed] [Google Scholar]
- 29.Ni W, Cui J, Liang B, Cai Y, Bai N, Cai X, Wang R. In vitro effects of tigecycline in combination with colistin (polymyxin E) and sulbactam against multidrug-resistant Acinetobacter baumannii. J Antibiot (Tokyo). 2013;66:705–708. doi: 10.1038/ja.2013.84. [DOI] [PubMed] [Google Scholar]
- 30.Claeys KC, Fiorvento AD, Rybak MJ. Review of novel combinations of colistin and lipopeptide or glycopeptide antibiotics for the treatment of multidrug-resistant Acinetobacter baumannii. Infect Dis Ther. 2014;3:69–81. doi: 10.1007/s40121-014-0051-9. [DOI] [PMC free article] [PubMed] [Google Scholar]