

Abstract
Background
People living in sub-Saharan Africa (SSA) are disproportionately exposed to trauma and may be at increased risk for posttraumatic stress disorder (PTSD). However, a dearth of population-level representative data from SSA is a barrier to assessing PTSD. This manuscript sought to calculate pooled PTSD prevalence estimates from nationally and regionally representative surveys in SSA.
Methods and findings
The search was conducted in PubMed, Embase, PsycINFO, and PTSDpubs and was last run between October 18, 2019, and November 11, 2019. We included studies that were published in peer-reviewed journals; used probabilistic sampling methods and systematic PTSD assessments; and included ≥ 450 participants who were current residents of an SSA country, at least 50% of whom were aged between 15 and 65 years. The primary outcomes were point prevalence estimates of PTSD across all studies, and then within subgroups. The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) (registration number CRD42016029441). Out of 2,825 unique articles reviewed, 25 studies including a total of 58,887 eligible participants (54% female) in 10 out of the 48 countries in SSA were identified. Most studies enrolled any adult aged 18 years or older. However, some studies only enrolled specific age brackets or persons as young as 15 years old. Six studies were national surveys, and 19 were regional.
There were 4 key findings in the meta-analysis: (1) the overall pooled prevalence of probable PTSD was 22% (95% CI 13%–32%), while the current prevalence—defined as 1 week to 1 month—was 25% (95% CI 16%–36%); (2) prevalence estimates were highly variable, ranging from 0% (95% CI 0%–0%) to 74% (95% CI 72%–76%); (3) conflict-unexposed regions had a pooled prevalence of probable PTSD of 8% (95% CI 3%–15%), while conflict-exposed regions had a pooled prevalence of probable PTSD of 30% (95% CI 21%–40%; p < 0.001); and (4) there was no significant difference in the pooled prevalence of PTSD for men and women. The primary limitations of our methodology are our exclusion of the following study types: those published in languages other than English, French, and Portuguese; smaller studies; those that focused on key populations; those that reported only on continuous measures of PTSD symptoms; and unpublished or non–peer-reviewed studies.
Conclusions
In this study, PTSD symptoms consistent with a probable diagnosis were found to be common in SSA, especially in regions exposed to armed conflict. However, these studies only represent data from 10 of the 48 SSA countries, and only 6 studies provided national-level data. Given the enormous heterogeneity expected across the continent, and also within countries and regions, this review cannot speak to rates of PTSD in any regions not included in this review. Thus, substantial gaps in our knowledge of PTSD prevalence in SSA remain. More research on population-level prevalence is needed to determine the burden of trauma symptoms and PTSD in SSA and to identify acceptable and feasible approaches to address this burden given limited mental healthcare resources.
Lauren Ng and co-workers investigate the prevalence of post-traumatic stress disorder in countries in sub-Saharan Africa.
Author summary
Why was this study done?
Repeated and prolonged exposure to violence, armed conflict, and mass-casualty events, combined with a lack of access to mental health treatment, may result in a substantial effect on the population burden of posttraumatic stress disorder (PTSD) in sub-Saharan Africa (SSA).
While many studies of PTSD have been conducted in SSA, most of these studies derived their estimates from nonrepresentative samples or specific populations.
Population-representative epidemiologic data are critical to understand the burden of PTSD in SSA and develop national and regional policies to address that burden.
What did the researchers do and find?
We conducted a systematic review and meta-analysis of the prevalence of PTSD from representative national and regional studies in SSA.
Pooled prevalence estimates were calculated across all studies, and then within subgroups including by sex, assessment time frame (i.e., 1 week, 1 month, 1 year), use of a screening or diagnostic measure, and whether populations were affected or not affected by mass-casualty war or armed conflict.
We identified 25 unique studies (N = 58,887) across 10 of the 48 SSA countries.
The pooled prevalence of probable PTSD across all studies was 22% (95% CI 13%–32%).
The pooled prevalence of probable PTSD in participants from war-exposed regions was 30% (95% CI 20%–40%), while the estimate from war-unexposed regions was 8% (95% CI 3%–15%; p = 0.01).
What do these findings mean?
These data suggest that PTSD symptoms and probable PTSD are common in SSA.
However, information was only found on 10 of the 48 SSA countries, and only 6 studies provided national-level data.
Only one study used a measure of PTSD symptoms whose reliability and validity had been assessed previously in the population of interest.
Our results suggest both that PTSD is a major public health problem in SSA and that large gaps in our knowledge of this problem remain.
Introduction
Mental and substance use disorders account for 23% of years lost to disability, making them the leading cause of disability worldwide [1]. Posttraumatic stress disorder (PTSD) is a large contributor to the global burden of disease and is estimated to affect almost 4% of the world’s population [2]. PTSD persists for over a year in 50% of all cases [2] and often leads to substantial declines in functioning and productivity [3]. National and regional data on prevalence are used to develop policies and action plans for addressing PTSD and other related disorders. Recently, much of the data on global and national estimates of PTSD has come from the World Health Organization’s World Mental Health (WMH) surveys of the cross-national prevalence of PTSD in 26 countries [2,4,5]. The WMH surveys collected representative population data across the world using structured diagnostic measures to assess PTSD, which allowed for the calculation of global population prevalence estimates of PTSD [2]. However, the WMH surveys only included one national survey and one regional survey from sub-Saharan Africa (SSA); in addition, the one national estimate was from South Africa, one of the few upper-middle–income countries in SSA [2]. The limited number of countries from SSA contributing data on PTSD in the WMH surveys is consistent with the lack of population mental health data from SSA generally [6,7].
People living in SSA may be disproportionately affected by individual and population-level trauma exposure. Indeed, research from the World Health Organization has found that the lifetime prevalence of road traffic deaths [8] and of reported intimate partner violence and/or nonpartner sexual violence are highest in the Africa region [9,10]. In addition, although other regions of the world experience more natural disasters, the great majority of countries most vulnerable to natural disasters are in SSA [11]. SSA has also been disproportionately affected by war and armed conflicts, many of which have been ongoing for years, if not decades [12]. In 2019, 20 countries in SSA were classified by the World Bank as hosting fragile and conflict-affected situations, which represents more than 50% of the fragile and conflict-affected countries globally [13]. Moreover, the legacy of violence, loss, and historical trauma inflicted on the people in SSA through colonization may contribute to high rates of posttraumatic stress [14].
Increased exposure to traumatic life experiences in SSA is compounded by very low rates of access to mental health treatment [15,16]. Of the 48 countries in SSA [17], 24 (50%) are low-income countries, 18 (37.5%) are lower-middle–income countries, and the remaining 6 (12.5%) are upper-middle–income countries [18]. It is estimated that the gap between those who need mental healthcare and those who receive it often exceeds 90% in low-income countries for most mental disorders [19–21]. It is estimated that 77% of people with PTSD in lower-middle–income countries have not received treatment [2]. Given that the majority of countries in Africa are low-income or lower-middle–income, it is likely that the vast majority of people with PTSD in SSA will never receive treatment and are at high risk for chronic symptoms. Repeated and prolonged exposure to violence, armed conflict, and mass-casualty events, combined with a lack of access to mental health treatment [15,16], may result in a substantially larger effect on the population burden of PTSD in SSA [22,23].
Aims
The goal of this meta-analysis was to synthesize the existing data on the population prevalence of PTSD in SSA. While many studies of PTSD have been conducted in SSA, most of these studies derived their estimates from nonrepresentative samples or specific populations such as refugees or internally displaced persons (IDPs) [24–30], patients [31–35], parents [36–40], or students [41–49]. While studies have summarized PTSD prevalence in conflict-affected populations, including those in SSA [50,51], PTSD occurs in response to a wide range of traumas (both interpersonal and non-interpersonal) that occur in non-conflict settings (e.g., car accidents, sexual assault). Population-representative epidemiologic data are critical to understand the burden of PTSD in SSA and develop national and regional policies to address that burden. To our knowledge, this is the first meta-analysis to summarize the data on population-based point prevalence of PTSD in SSA across all settings. The objectives of this paper were to (a) conduct a systematic review and meta-analysis of the prevalence of PTSD from representative national or regional studies and (b) explore the association between sex, population-level exposure to armed conflict, and pooled prevalence of PTSD.
Methods
Search strategy and selection criteria
Study inclusion criteria are as follows:
Participants were current residents of a country in SSA (e.g., citizens, permanent residents, IDPs, or refugees or immigrants who had resided in the country for at least 6 months).
In order to capture studies that focused primarily on adults, at least 50% of participants had to be between 15 and 65 years of age, which is defined as the “working age population” by the World Bank [52].
PTSD data were reported for at least 450 participants. We selected a priori a sample size cutoff to ensure that we would have enough power to detect prevalence estimates lower than 3.9%, which is the mean lifetime PTSD prevalence across the WMH surveys [2]. A minimum sample size requirement of 450 would allow us to identify prevalence as low as 3.3% with a precision of 1.65% within each study or region [53].
Studies used a systematic method of classifying participants as those with or without PTSD. Studies could be included if they used structured or semi-structured interviews—either administered by trained lay interviewers or clinicians—to provide a diagnosis or if they used a symptom checklist or diagnostic assessment and applied a cut-point to classify people as having PTSD or not having PTSD. In addition, we included studies that assessed cultural idioms of distress that were clearly related to symptoms developed in response to a stressful or traumatic event [54]. These are referred to as “post trauma reaction syndromes.” For the purposes of this paper, any participants who were either diagnosed with PTSD following an interview or who scored above a cut-point criterion set by the study authors were considered to have symptoms consistent with a diagnosis of PTSD.
Studies employed probabilistic procedures to obtain nationally or regionally representative samples. Representative samples that were limited to a specific sex were also included.
Articles were written in English, French, or Portuguese, which covers most of the scientific literature from SSA.
Studies were published in a peer-reviewed journal with no journal date restrictions.
If studies included a mixture of eligible and ineligible participants and data from the group meeting inclusion criteria could be disaggregated, the data that met inclusion criteria were included in the review.
The search strategy was developed and initially conducted in PubMed between February 22, 2016, and August 1, 2017. The search was expanded to 4 databases and rerun using PubMed, Embase, PsycINFO, and PTSDpubs between October 18, 2019, and November 11, 2019. Search terms were “[Name of SSA Country] AND PTSD (in any field).” The search was run for each country in SSA. Using Kenya as an example, PubMed automatically generates the following search when these terms are entered: (“Kenya” [medical subject heading (MeSH) Terms] OR “Kenya” [All Fields]) AND (“stress disorders, post-traumatic” [MeSH Terms] OR (“stress” [All Fields] AND “disorders” [All Fields] AND “post-traumatic” [All Fields]) OR “post-traumatic stress disorders” [All Fields] OR “ptsd” [All Fields]). The full texts of articles that appeared to meet inclusion criteria based on the abstract were downloaded, and references were reviewed to identify additional papers that might meet the eligibility criteria.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [55] (see Fig 1 for complete PRISMA flow diagram) process was followed to identify and include/exclude the papers in this review. Citations, abstracts, and full-text articles (when available) for all potentially eligible articles were downloaded and double coded by a team of 8 researchers to ensure they met criteria.
Fig 1. Study selection flow diagram.
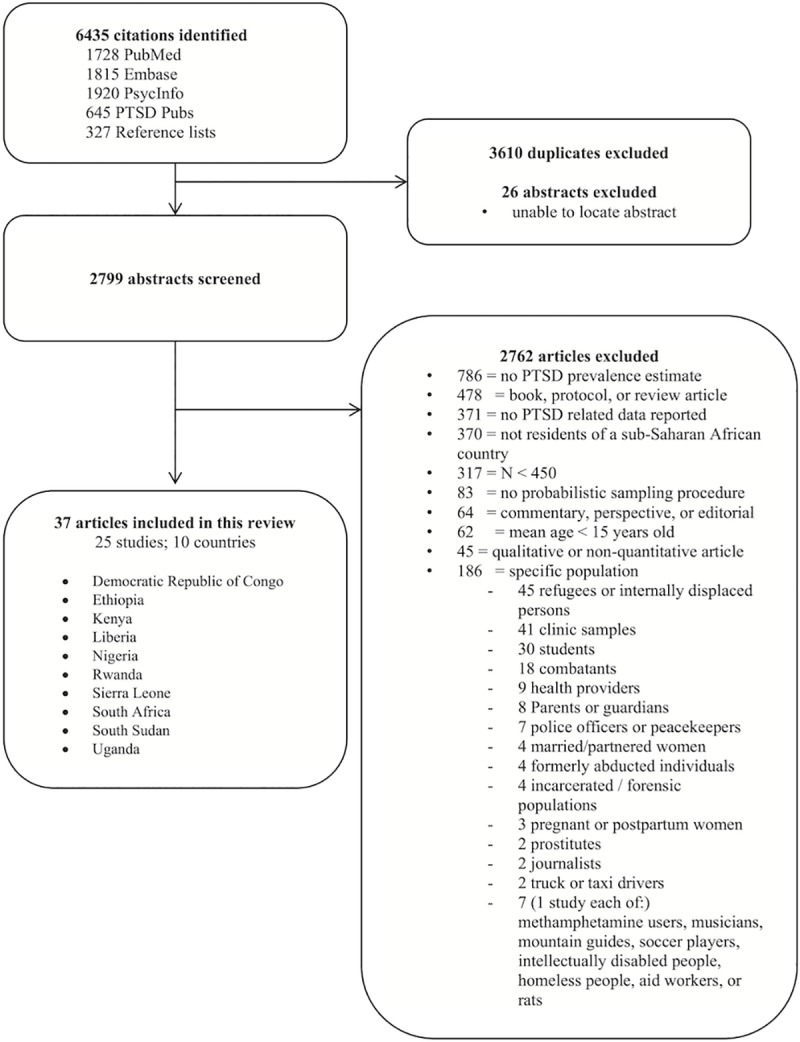
PTSD, posttraumatic stress disorder.
Articles were identified through the PubMed, Embase, PsycINFO, and PTSDpubs search and by reviewing references from the identified papers. Seven fields were then extracted from each paper and entered into a Google Docs spreadsheet: article title, year, first author, journal, search date, researcher conducting the search, and abstract. Duplicate entries were flagged and filtered out of the spreadsheet. To identify eligible studies from the remaining articles, the full text of each article was reviewed, and one coder entered information related to each inclusion and exclusion criteria into the database. A second coder independently reviewed each of the inclusion and exclusion criteria to assess concordance. Disagreements about study eligibility were reviewed and discussed by the research team, and final decisions were made by consensus.
The abstracts of non-English articles were reviewed by native speakers of the article language to determine eligibility, and if the abstract was deemed eligible, the full article was reviewed by the native speaker and also underwent targeted translation into English to enable accurate data extractions by a second coder. Studies that were not related to the eligibility criteria (e.g., a commentary or a study describing physical trauma instead of psychological trauma) were flagged and removed. For studies for which it was unclear whether they met eligibility criteria, the first author (L.C.N.) emailed the authors of the study to clarify.
Study quality was assessed using a standardized tool for observational studies [56]. Loney and colleagues (1998) was selected against a range of checklists and scales based on its applicability to prevalence studies, validation, reliability, and clear methodology for rating studies [57]. The tool contains 8 items, each with a possible score of 1, with a maximum total score of 8.
In implementing the quality assessment tool, we operationalized 4 of the questions on the Loney tool to best suit the purposes of this systematic review and meta-analysis:
On the first question (“Are the study design and sampling method appropriate for the research question?”), a full point was given if the study was a whole population or a random sample and the authors described the process in enough detail to support the statement from region down to the randomization of the individual selected to participate. Studies received a 0 if they were not the whole population or a random sample, or a half point if the study design was described as a “random sample”, but there was not enough evidence to confirm this.
On the fourth question (“Are objective, suitable, and standard criteria used for measurement of the health outcome?”), we defined this as “PTSD measurement tools which are consistent with accepted clinical/research criteria and validated in the population of interest.” If the battery was an acceptable clinical/research tool but had not been validated during the study or previously in the population of interest, it received a half point.
On the fifth question (“Is the health outcome measured in an unbiased fashion?”), we adapted this to make it more appropriate to our study framework. The original tool recommends blinding interviewers to the purpose of the study in some cases. We did not feel this was applicable in the context of prevalence studies of PTSD in SSA as most teams employed interviewers to conduct the batteries and trained them specifically on research methods in order to implement the study. Papers received a full point on this question if they described the assessors and described the training that they received to conduct the interviews and if internal reliability was calculated. If only one of these items was stated in the paper, the question was scored as a half point.
On the sixth question (“Is the response rate adequate? Are the refusers described?”), papers received a full point if the response rate was at least 70% and if the authors described any demographic details about the refusers. Studies scored a 0 if they did not meet the response rate threshold and did not describe the refusers, or a half point if they did one or the other. All other items on the Loney tool were scored as either 0 or 1 with no half points. The association between study quality and prevalence estimate was assessed using a meta-regression analysis.
This systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) on December 1, 2016, and updated on June 21, 2019 (registration number CRD42016029441; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=29441&VersionID=52136).
Data analysis
Data were extracted from eligible articles by author L.C.N., and all extractions were reviewed and confirmed by at least one other researcher. The primary outcomes of interest were the point prevalence estimates of PTSD. In addition, information on the number, age, and sex of participants; population-level trauma exposure; sampling procedures; and the language, translation, validity, and reliability of the PTSD assessment tools were also extracted.
Pooled prevalence estimates were calculated across all studies, and then within subgroups including by sex, assessment time frame (i.e., 1 week, 1 month, 1 year), use of a screening or diagnostic measure, and whether populations were affected or not affected by mass-casualty war or armed conflict. War or armed conflict was defined using the international humanitarian law definition, in which armed conflict occurs between organized armed groups, governmental or nongovernmental [58]. Pooled prevalences at the national and regional level were calculated to produce a heat map of available PTSD estimates in SSA (see Fig 2). Pooled estimates were calculated using the Stata version 14.2 [59] metaprop [60] command, which allows for the inclusion of all studies, including those with 0% or 100% prevalence proportions. Metaprop was run using (a) a random-effects model, which assumes that differences in prevalence estimates are not solely due to sampling error, (b) the exact confidence intervals, and (c) the Freeman-Tukey double arcsine transformation to normalize the prevalence estimates prior to pooling [60]. Q and I2 were calculated to assess heterogeneity across all studies and within and between subgroups [61]. Finally, a meta-regression with all a priori–defined subgroups in which significant differences in pooled prevalence were identified was run using the Stata metareg command [62].
Fig 2. PTSD in SSA: Pooled prevalence from countries with regionally or nationally representative data.
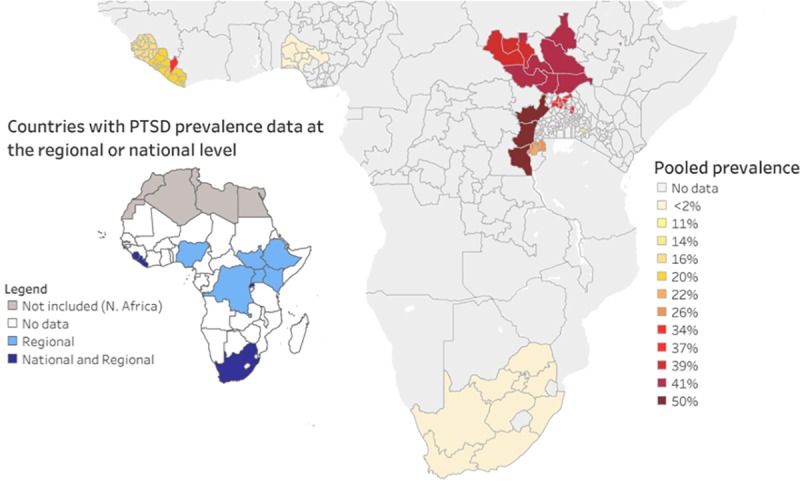
PTSD, posttraumatic stress disorder; SSA, sub-Saharan Africa.
Weighted prevalence estimates were used if they were reported; otherwise, raw numbers of participants with PTSD and total sample size were included as data. If raw numbers of participants with PTSD were not reported, they were calculated from summary data reported in the manuscripts. Prevalence estimates were calculated based on the total number of participants included in the studies regardless of whether or not they reported experiencing a traumatic event. In some cases, publications only reported conditional PTSD prevalence estimates (i.e., PTSD prevalence only among people who reported a traumatic event). In cases in which the manuscript only reported conditional prevalence, but the overall prevalence estimate could be calculated based on the other information provided in the manuscript, the overall prevalence estimate was calculated and was included in the meta-analysis. Study authors were contacted for clarification by L.C.N. in cases for which prevalence estimates were ambiguous.
Results
A total of 6,435 articles were identified through database and reference searches, of which 2,825 were unique articles (see Fig 1 for complete PRISMA flow diagram). After removing the duplicates and 26 abstracts that could not be located, 2,799 articles remained for full review. The coders disagreed on the eligibility of 4 articles: for 2 studies, the mean PTSD symptom scores were reported but not estimates of diagnostic prevalence [63,64], and 2 studies met all inclusion criteria except that they did not report PTSD scores [65,66]. After review by the first author and in discussion with the coders, consensus was reached on eligibility. Ultimately, 2,762 articles were excluded, leaving 37 that met eligibility. The 37 articles described 25 unique studies across 10 of the 48 SSA countries (see Table 1 and Fig 2).
Table 1. Identified studies.
| Country | Studies | Population-level trauma exposure | National or regional | Regional, specified | If regional, how/why region was selected | Year of data collection | Inclusion criteria | Response rate | N with PTSD data | PTSD measure and scoring | Time frame | PTSD prevalence (95% CI) | Women with PTSD data | PTSD %; sex difference | Age: M (years) (SD/CI); range | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DRC | Johnson et al., 2010 [124] | Violence and armed conflict for decades | Regional | Subregions of the North and South Kivu provinces and the Ituri district | High levels of violence during the war in Rwanda that crossed over the border into the DRC | Mar 2010 | Adults (18+) | 98.9% | 989 | PSS-I in Kiswahili; DSM-IV criteria Lay administered |
1 month | 50.1% (43.8%–56.3%) | 593 | 60.0% | Men: 44.4% (35.4%–53.4%) Women: 54.0% (46.6%–61.5%). p = 0.08 |
Mean = 40.1 (95% CI 38.2–42.0 years) |
| Ethiopia | Asnakew et al., 2019 [83] | Deadly garbage landfill landslide | Regional | Area of the Koshe landslide, Addis Ababa, Ethiopia, 2018 | Area experienced trauma due to landslide | May and June 2018 | Participants (15+ years old) | 98.2% | 830 | PCL-C in Amharic | 1 month | 37.3% (34.1% to 40.8%) | 491 | 59.2% | Men: 31.3% (26.4%–36.5%) Women: 41.5% (37.1%–46.0%) p = 0.003 |
Mean = 33 years (SD = 12) |
| Kenya | Jenkins et al., 2015 [125] | Election violence in August 2007 and 2013 | Regional | The Maseno area in Kisumu county, Nyanza Province in western Kenya | Endemic for malaria. In addition, Nyanza province experienced serious election violence in August 2007 | 6 months in 2013 | None reported | 96.4% | 1,146 | TSQ in English, Kiswahili, and Dholuo Cutoff of 6 Restricted to those who experienced trauma after age 16 |
1 week | 10.6% (8.8%–12.5%) | 545 | 47.6% | Men: 6.7% (4.8%–9.0%) Women: 14.9% (12.0%–18.1%) p < 0.001 |
<30 years = 281; 30–60 years = 448; >60 years = 171 |
| Liberia | Galea et al., 2010 [84] | Armed violence and conflict from 1989 to 2003 | Regional | Rural areas of Nimba County | History of civil conflict in Nimba County | Nov and Dec 2008 | Analyses restricted to those aged 19+ | 98.0% | 1,376 | HTQ in Liberian English Self-reported |
1 week | 48.3% (45.7%–50.9%) | 631 | 45.9% | Not reported | <35 y = 574 (41.7%); >35 = 802 (58.3%) |
| Johnson et al., 2008 [67] | National | N/A | N/A | May 2008 | Adults (18+), give accurate information about household | 98.2% | 1,661 | PSS-I in Liberian English; DSM-IV criteria Lay administered |
1 month | 44.0% (38.0%–49.0%) | 876 | 52.7% | Men: 46% (38%–54%) Women: 42% (38%–46%) p = 0.17 |
Mean = 41 (95% CI 40–42 years) | ||
| Vinck et al., 2013 [68] | National | N/A | N/A | Nov and Dec 2010 | Adults (18+) | 93.4% | 4,496 | PCL-C (language not reported) Cutoff of 44 Information on PCL-C assessors is not provided |
1 month | 12.6% (11.5%–13.9%) | 2,272 | 50.5% | Men: 6.3% (5.3%–7.4%) Women: 18.8% (17.2%–20.5%) p < 0.0001 |
Mean = 37.4 (SE = 0.26) | ||
| Nigeria | Gureje et al., 2006 [98] | None reported | Regional | Yoruba-speaking areas: Lagos, Ogun, Osun, Oyo, Ondo, Ekiti, Kogi, and Kwara | Not reported | Feb and Nov 2002 | Adults (18+), fluent in Yoruba | 79.9% | 4,984 | WMH Survey version of the CIDI in Yoruba Lay administered |
12 months | 0.0% (0.0%–0.0%) | 2,552 | 51.2% | Men: 0% (0%–0.2%) Women: 0% (0%–0.1%) p > 0.95 |
Mean = 35 (SE = 0.37) |
| Rwanda | Fodor et al., 2015 [96] | 1994 genocide that followed years of ethnic tensions and conflict | Regional | Ngoma commune in the Huye district in the South Province | Heavily affected by the genocide | Feb and Mar 2011 | Adults (18+) | 96% | 500 | PCL-C in Kinyarwanda Cutoff score of 44 Administered by trained native Rwandan college graduates in interview format |
1 month | 21.6% (18.1%–25.5%) | 349 | 75.0% | Not reported | Mean = 41.06 (14.9); 18–83 |
| Munyandamutsa et al., 2012 [70], Eytan et al., 2015 [69] | National | N/A | N/A | 3 months in 2008 | Ages 16+, Rwandan, fluent in Kinyarwanda, no mental impairment | Not reported | 962 | PTSD section of the MINI DSM-IV and ICD-10 criteria Clinician-administered |
1 month | 26.1% (23.2%–28.9%) | 567 | 58.9% | Men: 20.5% (16.6%–24.8%) Women: 30.0% (26.2%–33.9%) p = 0.001 |
Median = 33; range: 16–108 years | ||
| Pham et al., 2004 [126] | Regional | 4 communes: Ngoma (known as Butare town), Mabanza, Buyoga, and Mutura) | Diversity in region, level of urbanization, experience with the genocide, and relationship to the ICTR | Feb 2002 | Adults (18+) | 99% | 2,091 | PCL-C (language not reported); cutoff of 44 Self-reported |
1 month | 24.8% (23.0%–26.6%) | 1,074 | 51.4% | Men: 19.6% (17.2%–22.2%) Women: 29.7% (27.0%–32.5%) p < 0.001 |
Mean = 36.4 years; range 18–94 years | ||
| Rugema et al., 2015 [80] | Regional | Southern Province | Not reported | Dec 2011 to Jan 2012 | Aged 20–35 years, Rwandan | 99.8% | 913 | MINI in Kinyarwanda Clinician-administered |
1 month | 13.6% (11.4%–16.0%) | 477 | 52.0% | Men: 7.1% (4.8%–9.9%) Women: 19.5% (16.0%–23.3%) p < 0.001 |
20–24 = 275 (30.3%); 25–29 = 300 (33.0%); 30–35 = 333 (36.7%) | ||
| Sierra Leone | Betancourt et al., 2016 [97] | Civil war from 1991–2002 and EVD | Regional | Western area rural district and western area urban district | Diversity in ethnic composition and degrees of war exposure; was epicenter of EVD cases during the 2014–2015 outbreak | Jan to Apr 2015 | Adults (18+) | 98% | 1,008 | PSS-I adapted for use in Liberia in Krio Lay (trained research assistants) administered |
1 month | 6% (4%–7%) | 505 | 50.8% | Not reported | Mean = 34.2 years (95% CI 33.2–35.2) |
| Jalloh et al., 2018 [71] | Ebola | National | N/A | N/A | Jul 2015 | Head of household and another individual (aged between 15 years and 24 years) or a woman | 98% | 3,564 | IES-6 Administered by trained data collectors |
1 week | 16% (14.7%–17.1%) | 1,774 | 50% | Not reported | Median = 35 (SD = 15) | |
| South Africa | Herman et al., 2009 [75]; Williams et al., 2008 [127]; Atwoli et al., 2013 [72]; Atwoli et al., 2017 [73]; Koenen et al., 2017 [2]; Stein et al., 2008 [74]; Myer et al., 2009 [128]; Duckers et al., 2018 [129] | Apartheid until 1994. In the post-Apartheid era, high rates of nonpolitical violence and crime, child abuse, IPV, and HIV/AIDS and TB | National | N/A | N/A | Jan 2002 to June 2004 | Adult South Africans residing in households and hostels | 87.1% | 4,351 | CIDI version 3.0 in English, Afrikaans, Zulu, Xhosa, North Sotho, South Sotho, and Tswana; DSM-IV PTSD Lay administered |
12 months | 0.6% (0.4%–0.8%) | 2,619 | 60.2% | Men: 0.6% (0.3%–1.1%) Women: 0.6% (0.3%–1.0%) p = 0.92 |
Not reported |
| Machisa et al., 2017 [85] | Regional | Gauteng Province | Not reported | 2010 | Adult women | 79% | 501 |
HTQ in English, Zulu, Sotho, and Afrikaans Researcher administered Mean score ≥ 2.5 |
1 week | 11.6% (9%–14%) | 495 | 100.0% | Only women included | 18–29 = 30%; 30–44 = 36%; >45 = 33% | ||
| Peltzer and Pengpid, 2019 [77] | National | N/A | N/A | 2012 | Aged 15+ | 92.6% | 15,201 | 17-item DTS Information on assessors is not provided |
1 week | 2.1% (1.9%–2.3%) | 8,254 | 54.3% | Men: 2.0% (1.7%–2.4%) Women: 2.3% (2.0%–2.6%) p = 0.20 |
Mean = 36.8 (SD = 16.5) | ||
| Smit et al., 2006 [82] | Regional | Periurban settlement outside Cape Town, South Africa | High HIV prevalence | Not reported | Aged 15+ | 64.3% | 645 | HTQ in Xhosa and English; a cutoff score of 75 Self-reported |
1 week | 14.9% (12.2%–17.9%) | 357 | 55.3% | Men: 18.7% (14.0%–24.0%) Women: 13.7% (10.3%–17.7%) p = 0.10 |
Mean = 30.3 (11.9) | ||
| Topper et al., 2015 [81] | Regional | Eastern Cape Province, urban and semiurban areas of Nelson Mandela Bay and the semirural area of Kirkwood | Not reported | Not reported | Aged 18–40 years | 97.7% | 977 | MINI, version 6.0.0 in Xhosa, English, and Afrikaans; information on PCL-C assessors is not provided | 1 month | 10.8% (9.0%–13.0%) | 467 | 47.8% | Men: 11.6% (8.9%–14.7%) Women: 10.1% (7.5%–13.2%) p = 0.45 |
Not reported | ||
| South Sudan | Ayazi et al., 2012 [99]; Ayazi et al., 2014 [130] | Decades of ongoing civil war | Regional | The Greater Bahr el Ghazal region | Not reported | 2010 | Adults (18+) | 95% | 1,200 | HTQ with minor adaptations; Arabic with key terms in indigenous languages Cutoff of 2.0 Information on HTQ assessors is not provided |
2 weeks | 37.6% (34.8%–40.4%) | 506 | 44.0% | Men: 33.6% (30.0%–37.4%) Women: 42.1% (37.8%–46.5%) p = 0.003 |
18–25 = 308 (25.7%); 26–35 = 391 (32.6%); 36–50 = 395 (32.9%); >50 = 89 (7.4%) |
| Ng et al., 2017 [131] | Regional | 11 sites in 6 of South Sudan’s 10 states: (Central Equatoria, Jonglei, Upper Nile, Western Equatoria, Eastern Equatoria, and Lakes) and Abyei | Diverse in terms of ethnicity, socioeconomic status, livelihood, exposure to conflict, and security access | Dec 2014 to Apr 2015 | Adults (18+); South Sudanese | 99.5% | 1,520 | The HTQ-R in Classical Arabic, Juba Arabic, Dinka, Nuer, Shilluk, and Bari DSM-IV criteria Information on HTQ-R assessors is not provided |
1 week | 40.7% (38.2%–43.2%) | 773 | 50.9% | Men: 45.2% (41.6%–48.9%) Women: 36.2% (32.8%–39.7%) p < 0.001 |
Mean = 36.93 years (SD 13.90); range 18–86 | ||
| Roberts et al., 2009 [132] | Regional | Juba Town | High numbers of IDPs, returned IDPs and refugees | 20–30 Nov 2007 | Adults (18+) | 96.2% | 1,242 | Adapted version of the HTQ in Juba Arabic and Bari Mean PTSD scores ≥ 2.0 Trained lay administered |
1 week | 36.2% (33.2%–39.4%) | 630 | 50.7% | Men: 29.7% (25.4%–34.5%) Women: 42.5% (39.4%–45.7%) p < 0.01 |
Mean = 33 years | ||
| Uganda | Ertl et al., 2014 [79]; Neuner et al., 2012 [78] | Twenty-one years of war | Regional | Anaka, Awer, and Padibe Acholi regions | Varying degrees of war exposure and distance from the largest town, Gulu | Jul 2007 to Apr 2008 | Aged 12–25 | 99.9% | 1,113 | PDS in Luo Information on PDS assessors is not provided |
1 month | 15% (13%–17%) | 693 | 62.3% | Not reported | Not reported |
| Mugisha et al., 2015 [133]; Mugisha et al., 2015 [134]; Mugisha et al., 2016 [135] | Regional | Subcounties Lalogi and Koro (in Gulu district); Amuru and Atiak (in Amuru district); and Koch Goma and Alero (in Nwoya district) | Some of the most affected subdistricts by the 20-year civil war in northern Uganda that had a health center | 2 Jan 2013 to 2 June 2013 | Adults (18+), stayed in the area for more than 6 months, could fluently speak Luo | 100% | 2,361 | MINI in Luo Administered by trained psychiatric nurses |
1 month | 11.8% (10.5%–13.1%) | 1,475 | 62.5% | Men: 13.4% (11.2%–15.7%) Women: 10.9% (9.3%–12.5%) p = 0.002 |
18–24 = 555 (23.5%); 25–34 = 644 (27.3%); 35–44 = 490 (20.8%); 45–54 = 672 (28.5%) | ||
| Pham et al., 2009 [136] | Regional | 8 districts: Amuru, Gulu, Kitgum, Pader, Lira, Oyam, Amuria, and Soroti | Represent a variety of ethnic groups (Acholi, Iteso, and Langi) and exposure to the armed conflict | Mar to June 2007 | Adults (18+) | 64.5% | 2,867 | PCL-C in 3 local languages Cutoff score of 44 Non-clinician administered |
1 month | 54% (52%–56%) | 1,417 | 49.5% | Men: 40% (37.5%–42.6%) Women: 68.3% (65.8%–70.7%) p < 0.001 |
Mean = 35.4 years (SD = 14.35) | ||
| Vinck et al., 2007 [137] | Regional | Four districts: Gulu, Kitgum, Lira, and Soroti | Selected to represent a diversity of ethnic composition (Acholi, Langi, and Teso) and varying degrees of exposure to the war | Apr to May 2005 | Adults (18+) | 73% | 2,389 | PCL-C in Acholi, Lango, and Ateso Cutoff score of 44 Information on PCL-C assessors is not provided |
1 month | 74.3% (72.5%–76.0%) | 1,198 | 50.1% | Men: 64.7% (61.9%–67.4%) Women: 83.3% (81.6%–85.8%) p < 0.001 |
Mean = 37 years (SD = 13.8 years) | ||
Abbreviations: CI, confidence interval; CIDI, Composite International Diagnostic Interview [94]; DRC, Democratic Republic of Congo; DSM-IV, Diagnostic and Statistical Manual Version 4 [138]; DTS, Davidson Trauma Scale [89]; EVD, Ebola virus disease; HTQ, Harvard Trauma Questionnaire [86]; HTQ-R, Harvard Trauma Questionnaire-Revised; ICD-10, International Classification of Diseases, Tenth Revision [139]; ICTR, United Nations’ International Criminal Tribunal for Rwanda; IDP, internally displaced person; IES-6, Impact of Event Scale-6 [91]; IPV, intimate partner violence; MINI, Mini International Neuropsychiatric Interview [92]; N/A, Not applicable; PCL-C, PTSD Checklist-Civilian Version [87]; PDS, Posttraumatic Stress Diagnostic Scale [90]; PSS-I, PTSD Symptom Scale Interview [93]; PTSD, posttraumatic stress disorder; SE, standard error; TB, tuberculosis; TSQ, Trauma Screening Questionnaire [88]
Six of the studies were national surveys, including 2 from Liberia [67,68], 1 from Rwanda [69,70], 1 from Sierra Leone [71], and 2 from South Africa [2,72–77]. The other 19 studies were representative samples of a region within a country. Across the 25 studies, data were available from 58,887 participants, 54% of which were women (n = 31,672 of 58,795 participants with data on sex). Some studies did not include the raw number of participants by sex, and so the number of women was calculated based on the information available in the paper, such as the percentage of participants who were women. Most studies enrolled any adult (men and women aged 18 years or older). However, some studies only enrolled specific age brackets (e.g., any person aged 12 to 25 [78,79], 20 to 35 [80], and 18 to 40 years) [81]. In addition, 3 studies enrolled any person aged 15 or older [82,83], 1 study enrolled any person 16 and older [69,70], and 1 study enrolled any adult aged 18 or older but restricted analyses to those aged 19 and older [84]. In addition, 1 study only enrolled adult women [85]. There were no studies that only enrolled adult men.
Across the 25 studies, presence of PTSD was assessed using translated, and in some cases adapted, scales (see Table 1). Sixteen studies used self-reported screening instruments administered by trained lay researchers/data collectors, including the Harvard Trauma Questionnaire (HTQ) [86] (6 studies), PTSD Checklist-Civilian Version (PCL-C) [87] (6 studies), Trauma Screening Questionnaire (TSQ) [88] (1 study), the Davidson Trauma Scale (DTS) [89] (1 study), the Posttraumatic Stress Diagnostic Scale (PDS) [90] (1 study), and the Impact of Event Scale-6 (IES-6) [91] (1 study). The other 9 studies used structured or semi-structured interviews, including the Mini International Neuropsychiatric Interview (MINI) [92] (4 studies), the PTSD Symptom Scale Interview (PSS-I) [93] (3 studies), and the Composite International Diagnostic Interview (CIDI) [94] (2 studies). The PDS was the only scale with validated psychometrics in the population of interest [95]. The majority of studies (n = 14; 58.3%) reported on past-month prevalence. A minority of studies used a 1- or 2-week time frame for assessment (n = 9; 36%), and only 2 studies (8%) assessed 1-year prevalence (see Table 1).
Study quality
Overall, the methodology of the included studies had many strengths (see Table 2). Out of a maximum total of 8, quality scores ranged from 4 (50%) to 7 (87.5%) with an average score of 6.36 (79.5%) using Loney and colleagues (1998) [56]. Sampling methods and sample sizes were very strong. All but 2 of the 25 studies used random samples and described their sampling methods in detail. More than 70% of the studies used an unbiased sampling frame, such as census data, and sample sizes were large, ranging from 500 to 15,201 participants. Response rates were very high. One study did not report a response rate, and one had a response rate of only 64.3%, but for three-quarters of the studies response rates were >90%.
Table 2. Study quality indicators.
| Country | Studies | 1. Random sample or whole population | 2. Unbiased sampling frame (i.e., census data) | 3. Adequate sample size (>300 participants) | 4. Measures were the standarda | 5. Outcomes measured by unbiased assessorsb | 6. Adequate response rate (70%), refusers described | 7. Confidence intervals, subgroup analysis | 8. Study participants described | Total (max 8) | Percentage of 100% |
|---|---|---|---|---|---|---|---|---|---|---|---|
| DRC | Johnson et al., 2010 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% |
| Ethiopia | Asnakew et al., 2019 | 1 | 0 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 75.0% |
| Kenya | Jenkins et al., 2015 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% |
| Liberia | Galea et al., 2010 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% |
| Johnson et al., 2008 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% | |
| Vinck et al., 2013 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 7 | 87.5% | |
| Nigeria | Gureje et al., 2006 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% |
| Rwanda | Fodor et al., 2015 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% |
| Munyandamutsa et al., 2012 | 1 | 0 | 1 | 0.5 | 0.5 | 0 | 1 | 1 | 5 | 62.5% | |
| Pham et al., 2004 | 1 | 0 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 68.8% | |
| Rugema et al., 2015 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% | |
| Sierra Leone | Betancourt et al., 2016 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 7 | 87.5% |
| Jalloh et al., 2018 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 7 | 87.5% | |
| South Africa | Herman et al., 2009 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% |
| Machisa et al., 2017 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% | |
| Peltzer and Pengpid, 2019 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 7 | 87.5% | |
| Smit et al., 2006 | 0.5 | 0 | 1 | 0.5 | 0 | 0 | 1 | 1 | 4 | 50.0% | |
| Topper et al., 2015 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 6.5 | 81.3% | |
| South Sudan | Ayazi et al., 2012 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 7 | 87.5% |
| Ng et al., 2017 | 0 | 0 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 5 | 62.5% | |
| Roberts et al., 2009 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 7 | 87.5% | |
| Uganda | Ertl et al., 2014 | 1 | 0 | 1 | 1 | 1 | 0.5 | 1 | 1 | 6.5 | 81.3% |
| Mugisha et al., 2015 | 1 | 0 | 1 | 0.5 | 1 | 1 | 1 | 1 | 6.5 | 81.3% | |
| Pham et al., 2009 | 1 | 0.5 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6.5 | 81.3% | |
| Vinck et al., 2007 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 7 | 87.5% |
aPTSD measurement tools consistent with generally accepted clinical/research criteria and tool validated during study or in population previously?
bInterviewers and their training described; internal reliability calculated.
Abbreviations: DRC, Democratic Republic of Congo; PTSD, posttraumatic stress disorder
Every study used accepted clinical or research tools for measuring PTSD. While most articles acknowledged that the tools had been validated elsewhere, of note, only one study in the meta-analysis used a tool that had been validated during the study in question or in the same study population previously, Ertl and colleagues (2014) in Uganda [79]. The assessors and their training to implement the instruments were well-described (all but 2 studies provided details about the interviewers); however, reliability was inconsistently reported. Over half (n = 14) of the studies ran and stated Cronbach's alpha for internal reliability, while the remaining 11 did not report it.
Overall pooled prevalence of probable PTSD
Prevalence estimates had reporting time frames of 1 week to 1 year, and estimates were highly variable, ranging from 0% (95% CI 0%–0%) to 74% (95% CI 72%–76%), and heterogeneous (Q = 18,326.70, df = 24, p < 0.001, I2 = 99.87%). Overall, pooled prevalence across all studies was 22% (95% CI 13%–32%) (see Fig 2 and Fig 3). Pooled estimates were recalculated only including the 20 studies that achieved at least an 80% quality score. The pooled estimate from the high-quality studies was 20% (95% CI 11%–32%). There was no association between study quality and prevalence (b = −0.001 [95% CI −0.11 to 0.11], p = 0.98).
Fig 3. Overall prevalence estimates.

CI, confidence interval; ES, effect size (proportion).
Pooled prevalence by sex
Five studies [71,79,84,96,97] did not report prevalence estimates by sex, and so they were not included in the analysis of prevalence by sex. Herman and colleagues (2009) [75] and Gureje and colleagues (2006) [98] did not report prevalence by sex but did report that there was no significant difference by sex, and so the overall mean score was included as the score for both men and women. Machisa and colleagues (2017) [85] only sampled women, and so the data from this study were included in the pooled analysis for women but not men.
Of the 19 studies that reported data comparing the rates of PTSD in men and women, 12 reported a significant difference (see Table 1). Of the 12 studies that reported a significant difference in the prevalence of PTSD in men compared to women, 10 reported higher rates of PTSD in women, and 2 reported higher rates of PTSD in men. There were no significant differences in the pooled prevalence of PTSD by sex (test of heterogeneity between groups = 0.42, df = 1, p = 0.52). The pooled prevalence estimate for females was 25% (95% CI 14%–39%). The pooled prevalence estimate for males was 20% (95% CI 10%–31%) (see S1 Fig). Post hoc meta-regression indicated that the lack of a significant difference in probable PTSD prevalence by sex persisted when predictors included conflict exposure, reporting time frame, and assessment tool type (b = −0.08 [95% CI −0.19 to 0.04], p = 0.18).
Pooled prevalence by reporting time frame
The 2 WMH Survey studies [75,98] were the only ones to use a 1-year time frame. Because the study by Ayazi and colleagues [99] was the only study that utilized a 2-week time frame, it was grouped with those using a 1-week time frame when stratifying by assessment time frame, since this study used the HTQ [86], which has a 1-week–assessment time frame [86]. Across all studies, there were significant differences by assessment time frame (random heterogeneity test between subgroups = 79.61, df = 2, p < 0.001; see S2 Fig). However, this difference is explained by the 2 studies that assessed PTSD over a 1-year time frame. These 2 studies (Gureje and colleagues [98] and Herman and colleagues [75]) were part of the cross-national WMH Surveys [100] and were the only 2 studies to use the CIDI [94]. They each had pooled prevalence estimates of 0% (95% CI 0%–0%). In contrast, the pooled prevalence in the past week was 22% (95% CI 9%–38%), and the pooled prevalence in the past month was 27% (95% CI 16%–40%). There was no significant difference in the weekly versus monthly pooled prevalence (random heterogeneity test between subgroups = 0.28, df = 1, p ≤ 0.60). The overall pooled prevalence of probable current PTSD, defined as a period prevalence ranging from 1 week to 1 month, was 25% (95% CI 16%–36%).
Pooled prevalence by screener versus diagnostic assessment tool
There was not a significant difference in the prevalence estimates between studies that used screening instruments (27% [95% CI 15%–41%]) compared to those using diagnostic structured and semi-structured interviews (14% [95% CI 4%–29%]; random test for heterogeneity between subgroups = 1.76, df = 1, p = 0.18).
Pooled prevalence by exposure to war or armed conflict
There was a significant difference in pooled prevalence estimates between studies that were conducted in regions exposed to mass-casualty war or armed conflict at any point during the lifetime of the participants and those that were unexposed (random test for heterogeneity between subgroups = 13.64, df = 1, p = 0.01) (see Fig 4). The pooled prevalence estimate of studies from exposed regions was 30% (95% CI 20%–40%), while the estimate from unexposed regions was 8% (95% CI 3%–15%). Results of the adjusted R2 from a meta-regression indicated that conflict exposure accounted for 22.77% of the variance in the pooled prevalence estimates.
Fig 4. Prevalence estimates by exposure to mass-casualty war or armed conflict.

Random test of heterogeneity between subgroups: 13.64, df = 1, p < 0.001. CI, confidence interval; ES, effect size (proportion).
Discussion
The goal of this review was to provide a more complete picture of the population-based data on the current prevalence of PTSD in SSA than is available from any single study. We identified 25 studies assessing 58,887 individuals in the SSA region. There were 4 key findings in the meta-analysis: (1) The overall pooled prevalence across all studies, including 2 studies that calculated a 1-year prevalence estimate, was 22% (95% CI 13%–32%). The pooled prevalence of current symptoms (defined as duration of 1 week to 1 month) consistent with a probable diagnosis of PTSD in SSA was 25% (95% CI 16%–36%). (2) Prevalence estimates of current symptoms across the individual studies were highly variable, ranging from 2% (95% CI 2%–2%) to 74% (95% CI 72%–76%). (3) There was no significant difference in the pooled prevalence of PTSD for men and women, for reporting time frame, or for whether the study used a screening versus diagnostic instrument. (4) Prevalence estimates across regions differed substantially by population-level exposure to war or armed conflict. We discuss these findings in more detail subsequently.
The high 22% prevalence of probable PTSD found in this meta-analysis seems to be driven in large part by the 30% prevalence of probable PTSD found across the 17 studies that were conducted on populations exposed to war and armed conflict. The finding that populations experiencing war or armed conflict within the lifetime of the study participants have higher probable PTSD prevalence is consistent with expectations. Countries with higher rates of conflict have populations exposed to higher levels of trauma and thus more PTSD symptoms. However, the prevalence of PTSD of 30% found in this meta-analysis still exceeds the rates found in 3 other meta-analyses in populations exposed to war of 15% [50], 26% [101], and 24% [51]. Moreover, the 8% prevalence of PTSD in non–war-exposed populations exceeds the 4% rate of PTSD prevalence found in other population-based cross-national studies [2], suggesting that there was still a substantial population-level burden of PTSD symptoms in non–conflict-affected countries, a burden that has often been overlooked. Taken together, these data suggest that PTSD symptoms and probable PTSD are common in SSA. The higher prevalence of PTSD found in this meta-analysis may be partially explained by studies finding that people living in SSA may be disproportionately affected by individual and population-level trauma exposure [8,10–12,14,102] and that the vast majority of people in SSA have very low access to mental health treatment [15,16]. These factors may result in a larger effect on the population burden of PTSD in SSA [22,23].
There was no consistent pattern in the results for sex differences in PTSD prevalence. While 10 of the 19 studies that reported on sex differences in PTSD prevalence reported that women had higher rates of probable PTSD, 7 studies reported no sex difference, and 2 studies reported that men had higher rates of probable PTSD. However, there was no difference in the overall pooled prevalence by sex. These findings suggest that sex may frequently be a critical variable to consider when understanding PTSD prevalence but that its explanatory power may vary by population context.
Due to large variability in prevalence estimates, there was not a significant difference in prevalence estimates between studies that used screening instruments compared to those using diagnostic structured and semi-structured interviews. However, the mean ratio of the difference between studies using screening instruments (27% [95% CI 15%–41%]) and those using diagnostic structured and semi-structured interviews (14% [95% CI 4%–29%]) was in line with the results of a meta-regression of prevalence of PTSD in countries experiencing war and armed conflict that found that symptom scales produced prevalence estimates that were 1.5 to 2 times higher than diagnostic tools [50]. The authors of the meta-regression suggest that this discrepancy may occur because symptom scales do not assess clinical significance or functional impairment and may therefore overestimate the prevalence of PTSD [50]. While the lack of data on functional impairment in symptom scales is certainly problematic, studies have found a strong correlation between elevated distress on symptom scales and functional impairment [103–105]. Indeed, subthreshold PTSD is associated with high distress and impairment and increased risk of suicidality globally [106]. Given that only 1 study used an instrument for PTSD that had been validated in the population of interest, we are unable to conclude whether symptom scales or diagnostic instruments may be under- or overestimating PTSD.
Limitations
In producing pooled estimates, we encountered at least 4 limitations of the identified studies that limit our ability to make interpretations from our findings. First, only 1 study (Ertl et al., 2014 [78,79]) used a measure of PTSD symptoms whose reliability and validity had been assessed previously in the population of interest. PTSD symptoms are highly prevalent in the SSA countries where they have been studied. However, the lack of reliable and valid instruments used in the populations studied is a major limitation for both research and practice. In a 2018 review of qualitative studies examining post-trauma symptoms across cultural contexts, most study participants reported symptoms consistent with Western diagnostic criteria but also reported a number of symptoms not captured in those diagnostic classifications [107], supporting the need for local contextualization of measures. Measures that are not locally contextualized and valid may result in substantial under- or overreporting of trauma exposure and PTSD symptoms. For example, a study of Zulu-speaking participants in northeastern KwaZulu-Natal, South Africa found that the PTSD section of the Structured Clinical Interview for Diagnostic and Statistical Manual (DSM) Disorders, Axis I, Research Version (SCID-I RV) [108] undercounted participants who had been exposed to traumatic events by almost 20% compared to a Zulu Culture-Specific Trauma Experience Questionnaire [109]. Pragmatic and feasible approaches to cultural and contextual validation of measures of post-trauma symptoms in challenging settings have been described [110] and need to become more widely employed prior to undertaking population surveys. Rigorous epidemiological research to examine the predictive validity of PTSD constructs in diverse settings is also an important priority.
Second, although data were available from a relatively large number of participants, the studies only represent data from 10 of the 48 SSA countries, and only 6 studies provided national-level data. There is a complete absence of national or regional population-based data on PTSD from more than 80% of SSA countries, including those affected by ongoing fragile and conflict-affected situations, such as Central African Republic, Mali, and Somalia. Given the enormous heterogeneity expected not only across the continent but also within countries and regions, this review cannot speak to rates of PTSD in any of these other regions. Thus, substantial gaps in our knowledge of PTSD prevalence in the majority of SSA remain.
These disparities in PTSD prevalence data parallel the lack of mental health data and services broadly in SSA [1]. Despite the enormous burden that mental disorders are projected to pose in SSA by 2050, they remain a low priority in terms of policy initiatives and research funding [111]. Even with political will and support, many countries may have difficulty meeting identified mental health needs given limited resources and competing priorities. Indeed, although 72% of countries in the Africa region reported that they had a stand-alone mental health policy, only 27% had allocated resources towards implementing that plan [112].
Third, as noted previously, there was high heterogeneity in the prevalence estimates with an I2 of more than 99%. We were therefore unable to statistically assess the risk of publication bias in this meta-analysis because none of the publication bias methods provide accurate results with more than moderate levels of heterogeneity (i.e., I2 < 50%) [113]. We are therefore unable to provide insight into the level of publication bias that may be present in these results.
Finally, the goal of this review was to focus on adult PTSD, and we excluded studies that focused exclusively or primarily on participants who are younger than 15 years old, which is the youngest age that the World Bank considers part of the “working age population” and is the youngest age of majority in countries throughout the world. All of the identified studies had participants whose mean age was 18 years old or older. However, 5 studies [70,79,82,83] included individuals who were younger than 18 years old, and therefore some of the data come from adolescents. However, when these studies were removed from the analyses, the results were unchanged.
In addition, there are several limitations in the methodology of our review that should be noted. Our inclusion criteria required that studies have at least 450 participants, use a probabilistic sampling procedure, and report a quantitative estimate of PTSD. As a result, we excluded smaller studies, those that focused on key populations, and those that reported only continuous measures of PTSD symptoms. Our review does not, therefore, speak to subthreshold PTSD, PTSD in specific populations (e.g. refugees, people living with HIV, students, or combatants), or nuances in context that may impact PTSD presentation and prevalence, such as IDPs currently living in conflict zones compared to those living in safe environments.
Disparities between our pooled estimates and WMH surveys
The pooled prevalence of probable PTSD in this systematic review (computed from 1 week to 1 year prevalence rates) is extremely high compared to the prevalence reported by a 2017 summary of data from the WMH surveys. For example Karam and colleagues (2014) [4] reported a WMH 12-month survey prevalence of 1.1% ranging from 3.8% in Northern Ireland to a low of 0.2–0.3% in Beijing and Shanghai in the People’s Republic of China, 0.3% in Colombia, and 0.3% in Mexico [4]. Indeed, the current PTSD pooled prevalence found in this study far exceeds the 3.9% lifetime rate found in the WMH surveys [2]. There are at least 4 possible reasons for the disparity found between the pooled PTSD prevalence estimates identified in this meta-analysis and the prevalence estimates found in the WMH surveys. First, although our review reports data from only 10 countries, 6 of those countries have experienced war and armed conflict during the lifetime of the participants. Very few such countries are included in the WMH surveys, with Iraq and Lebanon being notable exceptions [4]. However, even in Iraq and Lebanon, the prevalence of PTSD diagnosis is very low compared with the estimates of prevalence observed in SSA. Second, many of the studies in our pooled estimate specifically focused on PTSD assessment as a primary aim of the study. The WMH survey, in contrast, aims to document the population burden of all mental and behavioral disorders globally without one particular focus. In addition, in most cases the survey is administered in 2 stages, and PTSD is only included in the second stage of the survey [114]. Third, there are specific assessment nuances of the CIDI [100] (WMH survey studies were the only ones that used the CIDI) that may have impacted PTSD symptom report. First, in this review, the CIDI was the only diagnostic interview that was lay administered. Another key issue with the CIDI, compared to other instruments used in most of the studies, is the skip out related to reporting trauma. That is, PTSD is only assessed in persons who reported a qualifying trauma. Thus, if a participant does not report a trauma, either because their trauma is not on the list queried or because the person chooses not to report such sensitive information, then these participants do not get assessed for PTSD [114]. As a result, PTSD symptoms may go undetected. This is particularly problematic when the trauma events have not been culturally and contextually validated [109]. There is some data to suggest that the results of trauma may be underreported in the WMH surveys. For example, the lifetime exposure of sexual violence in the South African WMH Survey found a prevalence rate of rape of 2%; however, other epidemiological surveys from South Africa have found lifetime rates of rape between 4.5% and 12% [115].
Fourth, there may be differences in the way that individuals from different countries, communities, and cultures respond to items, which may result in under- or overreporting of symptoms. The CIDI, like many highly structured interviews, applies an algorithm of combinations of types of symptoms following the Diagnostic and Statistical Manual version 4 (DSM-IV) [116] in order to produce a diagnosis. The algorithms, like the diagnostic criteria in DSM-IV, are derived predominantly from Western populations, which give weight to the core symptoms that are known to have salience in those settings but not necessarily in other settings. Concerns about the cross-cultural applicability of the CIDI have been reported in Nepal [117], Ethiopia [118], and American Indian Reservation populations [119]. Indeed, a study that used latent-class analysis to reexamine the depression results of the WMH surveys from the US, New Zealand, South Africa, and Nigeria found that participants in Nigeria and South Africa who endorsed the screening questions endorsed more severe depression symptoms than participants from the US and New Zealand who endorsed the screening questions [120]. When these differential patterns of responding were taken into account, the prevalence estimate for depression in Nigeria was highest (22%), whereas the results of the Nigeria WMH Survey found that it had the lowest rate of depression (3%). Studies are needed that examine the reliability and validity of the diagnostic criteria of PTSD as well as widely used assessments such as the CIDI in SSA populations.
Conclusions and directions for future study
Methodological limitations of the extant literature as described earlier lead us to conclude that our pooled estimate should be interpreted with caution. Given limited information on the reliability and validity of the assessment tools used and the lack of data available from most countries in the region, more work is needed before strong conclusions can be made about the population burden of PTSD in SSA. Furthermore, the identified studies provide little or no evidence regarding the proportion of the population requiring specific levels of intervention and therefore do little to inform service planning.
However, even given these limitations, our findings suggest that health systems in SSA need to improve the identification of and access to treatment for persons with PTSD. The percentage of individuals with PTSD seeking treatment is globally low and is most strikingly low in countries of low to lower-middle income and of upper-middle income [2]. Improving detection of trauma and PTSD in primary care may be an efficient strategy, given that globally, people with PTSD are more likely to seek care in general health settings than in specialty mental health clinics [2]. However, major efforts to scale up mental healthcare, such as the Programme for Improving Mental Health Care (PRIME) [121]—which is focused on improving mental healthcare in nonhumanitarian settings in several low- and middle- income countries through integration with maternal and primary care—have not, to date, included PTSD as a target disorder. This is likely, in part, due to a lack of data on the prevalence of PTSD and the burden it poses in these settings. Moreover, misconceptions about PTSD remain. For example, PTSD is more widely recognized as a problem for refugees, in high-conflict situations, and in humanitarian crises. PTSD is included in the Mental Health Gap Action Programme (mhGAP) Intervention Guide for humanitarian settings but not yet included in the primary mhGAP [122,123]. However, epidemiologic data suggest that, globally, sexual violence in the context of intimate partnerships is responsible for the largest burden of PTSD [5]. Thus, much foundational epidemiological work remains to be done to document the burden of PTSD in SSA. This work will be critical to inform policy, research, and treatment; above all, it will be critical to address issues of access to care and decrease the burden of PTSD in SSA.
Supporting information
(DOC)
Random test of herterogeneity between subgroups: 0.42, df = 1, p = 0.052. CI, confidence interval; ES, effect size (proportion)
(TIFF)
Random test of heterogeneity between subgroups: 79.61, df = 2, p < 0.001. CI, confidence interval; ES = efect size (proportion)
(TIFF)
Acknowledgments
The authors thank Emilie Wigdor, Supriya Misra, Kristen Nishimi, Fernando Martinez Gausch, and Yuhan Cheng for their incredible assistance with identifying and coding articles, Yuhan Cheng for helping to format this manuscript for publication, Zach Leber and Jonathan Drummey for their guidance on creating the prevalence heat map, and OpenStreetMap contributors (openstreetmap.org) for the underlying data used in the map.
Abbreviations
- CIDI
Composite International Diagnostic Interview
- DRC
Democratic Republic of Congo
- DSM-IV
Diagnostic and Statistical Manual version 4
- DTS
Davidson Trauma Scale
- EVD
Ebola virus disease
- HTQ
Harvard Trauma Questionnaire
- HTQ-R
Harvard Trauma Questionnaire-Revised
- ICTR
United Nations’ International Criminal Tribunal for Rwanda
- IDP
internally displaced person
- IES-6
Impact of Event Scale-6
- MeSH
medical subject heading
- mhGAP
Mental Health Gap Action Programme
- MINI
Mini International Neuropsychiatric Interview
- PCL-C
PTSD Checklist-Civilian Version
- PDS
Posttraumatic Stress Diagnostic Scale
- PRIME
Programme for Improving Mental Health Care
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROSPERO
International Prospective Register of Systematic Reviews
- PSS-I
PTSD Symptom Scale Interview
- PTSD
posttraumatic stress disorder
- SCID
Structured Clinical Interview for DSM Disorders, Axis I, Research Version
- SSA
sub-Saharan Africa
- TSQ
Trauma Screening Questionnaire
- WMH
World Mental Health
Data Availability
Due to the nature of the meta-analysis, all data are present in the paper and are therefore publicly available.
Funding Statement
This study was supported by the National Institute of Mental Health (L.N., #K23MH110601), by Cohen Veterans Bioscience (K.C.K), by the UK Department for International Development (DfID) (C.H., #201446) as part of the Programme for Improving Mental health carE (PRIME), by the National Institute of Health Research (NIHR) Global Health Research Unit on Health System Strengthening in Sub-Saharan Africa, King’s College London (C.H., GHRU 16/136/54), and by AMARI as part of the DELTAS Africa Initiative (C.H., DEL-15-01). The views expressed in this article do not necessarily reflect the UK Government’s official policies, those of the NHS, the NIHR, or the Department of Health and Social Care. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1.Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–86. Epub 2013/09/03. 10.1016/S0140-6736(13)61611-6 . [DOI] [PubMed] [Google Scholar]
- 2.Koenen KC, Ratanatharathorn A, Ng L, McLaughlin KA, Bromet EJ, Stein DJ, et al. Posttraumatic stress disorder in the World Mental Health Surveys. Psychological medicine. 2017;47(13):2260–74. Epub 2017/04/08. 10.1017/S0033291717000708 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kessler RC. Posttraumatic stress disorder: the burden to the individual and to society. J Clin Psychiatry. 2000;61 Suppl 5:4–12; discussion 3–4. Epub 2000/04/13. . [PubMed] [Google Scholar]
- 4.Karam EG, Friedman MJ, Hill ED, Kessler RC, McLaughlin KA, Petukhova M, et al. Cumulative traumas and risk thresholds: 12-month PTSD in the World Mental Health (WMH) surveys. Depression and anxiety. 2014;31(2):130–42. Epub 2013/08/29. 10.1002/da.22169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kessler RC, Aguilar-Gaxiola S, Alonso J, Benjet C, Bromet EJ, Cardoso G, et al. Trauma and PTSD in the WHO World Mental Health Surveys. Eur J Psychotraumatol. 2017;8(sup5):1353383 Epub 2017/10/28. 10.1080/20008198.2017.1353383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Baxter AJ, Patton G, Scott KM, Degenhardt L, Whiteford HA. Global epidemiology of mental disorders: what are we missing? PloS one. 2013;8(6):e65514 Epub 2013/07/05. 10.1371/journal.pone.0065514 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.World Health Organization. WHO | mhGAP Mental Health Gap Action Programme [Internet]. World Health Organization. 2008. [cited 2015 Dec 15]. Available from: http://www.who.int/mental_health/evidence/mhGAP/en/index.html. [Google Scholar]
- 9.World Health Organization. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non- partner sexual violence. Geneva: 2013.
- 10.Abrahams N, Devries K, Watts C, Pallitto C, Petzold M, Shamu S, et al. Worldwide prevalence of non-partner sexual violence: a systematic review. Lancet. 2014;383(9929):1648–54. Epub 2014/02/18. 10.1016/S0140-6736(13)62243-6 . [DOI] [PubMed] [Google Scholar]
- 11.Bundis Entwicklung Hilft. World Risk Report Analysis and prospects 2017. 2017.
- 12.Marc A. CONFLICT AND VIOLENCE IN THE 21ST CENTURY CURRENT TRENDS AS OBSERVED IN EMPIRICAL RESEARCH AND STATISTICS. World Bank Group.
- 13.The World Bank. Fragile and conflict affected situations: World Bank Group; 2019 [cited 2019 July 11]. Available from: https://data.worldbank.org/region/fragile-and-conflict-affected-situations.
- 14.Fanon F. Black Skin, White Masks. New York: Grove Press; 1952. [Google Scholar]
- 15.Saxena S, Thornicroft G, Knapp M, Whiteford H. Resources for mental health: scarcity, inequity, and inefficiency. Lancet. 2007;370(9590):878–89. Epub 2007/09/07. 10.1016/S0140-6736(07)61239-2 . [DOI] [PubMed] [Google Scholar]
- 16.World Health Organization. Mental health atlas. Geneva: WHO Press; 2014. [Google Scholar]
- 17.The World Bank. Sub-Saharan Africa: World Bank Group; 2017 [cited 2018 Jan 22]. Available from: https://data.worldbank.org/region/sub-saharan-africa.
- 18.The World Bank. World Bank Country and Lending Groups: The World Bank Group; 2019 [cited 2019 July 11]. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
- 19.Kebede D, Alem A, Deyassa N, Shibre T, Negash A, Beyero T. Socio-demographic correlates of depressive disorder in Butajira, rural Ethiopia. Cent Afr J Med. 2003;49(7–8):78–83. Epub 2004/06/25. . [PubMed] [Google Scholar]
- 20.Wang PS, Aguilar-Gaxiola S, Alonso J, Angermeyer MC, Borges G, Bromet EJ, et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet. 2007;370(9590):841–50. Epub 2007/09/11. 10.1016/S0140-6736(07)61414-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Eaton J, McCay L, Semrau M, Chatterjee S, Baingana F, Araya R, et al. Scale up of services for mental health in low-income and middle-income countries. Lancet. 2011;378(9802):1592–603. Epub 2011/10/20. 10.1016/S0140-6736(11)60891-X . [DOI] [PubMed] [Google Scholar]
- 22.Charlson FJ, Flaxman A, Ferrari AJ, Vos T, Steel Z, Whiteford HA. Post-traumatic stress disorder and major depression in conflict-affected populations: an epidemiological model and predictor analysis. Global Mental Health. 2016;3:e4 10.1017/gmh.2015.26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bromet EJ, Atwoli L, Kawakami N, Navarro-Mateu F, Piotrowski P, King AJ, et al. Post-traumatic stress disorder associated with natural and human-made disasters in the World Mental Health Surveys. Psychological medicine. 2017;47(2):227–41. Epub 2016/08/31. 10.1017/S0033291716002026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rasmussen A, Nguyen L, Wilkinson J, Vundla S, Raghavan S, Miller KE, et al. Rates and impact of trauma and current stressors among Darfuri refugees in Eastern Chad. The American journal of orthopsychiatry. 2010;80(2):227–36. Epub 2010/06/18. 10.1111/j.1939-0025.2010.01026.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Mels C, Derluyn I, Broekaert E, Rosseel Y. The psychological impact of forced displacement and related risk factors on Eastern Congolese adolescents affected by war. Journal of child psychology and psychiatry, and allied disciplines. 2010;51(10):1096–104. Epub 2010/03/30. 10.1111/j.1469-7610.2010.02241.x . [DOI] [PubMed] [Google Scholar]
- 26.de Jong JT, Komproe IH, Van Ommeren M, El Masri M, Araya M, Khaled N, et al. Lifetime events and posttraumatic stress disorder in 4 postconflict settings. JAMA: the journal of the American Medical Association. 2001;286(5):555–62. Epub 2001/08/14. 10.1001/jama.286.5.555 . [DOI] [PubMed] [Google Scholar]
- 27.Salah TT, Abdelrahman A, Lien L, Eide AH, Martinez P, Hauff E. The mental health of internally displaced persons: an epidemiological study of adults in two settlements in Central Sudan. The International journal of social psychiatry. 2013;59(8):782–8. Epub 2012/09/18. 10.1177/0020764012456810 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Karunakara UK, Neuner F, Schauer M, Singh K, Hill K, Elbert T, et al. Traumatic events and symptoms of post-traumatic stress disorder amongst Sudanese nationals, refugees and Ugandans in the West Nile. Afr Health Sci. 2004;4(2):83–93. Epub 2004/10/13. [PMC free article] [PubMed] [Google Scholar]
- 29.Onyut LP, Neuner F, Ertl V, Schauer E, Odenwald M, Elbert T. Trauma, poverty and mental health among Somali and Rwandese refugees living in an African refugee settlement—an epidemiological study. Conflict and health. 2009;3:6 Epub 2009/05/28. 10.1186/1752-1505-3-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Roberts B, Ocaka KF, Browne J, Oyok T, Sondorp E. Factors associated with post-traumatic stress disorder and depression amongst internally displaced persons in northern Uganda. BMC psychiatry. 2008;8:38 Epub 2008/05/21. 10.1186/1471-244X-8-38 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ndetei DM, Khasakhala L, Maru H, Pizzo M, Mutiso V, Ongecha-Owuor FA, et al. Clinical epidemiology in patients admitted at Mathari Psychiatric Hospital, Nairobi, Kenya. Social psychiatry and psychiatric epidemiology. 2008;43(9):736–42. Epub 2008/05/10. 10.1007/s00127-008-0360-y . [DOI] [PubMed] [Google Scholar]
- 32.Mahenge B, Likindikoki S, Stockl H, Mbwambo J. Intimate partner violence during pregnancy and associated mental health symptoms among pregnant women in Tanzania: a cross-sectional study. Bjog. 2013;120(8):940–6. Epub 2013/03/08. 10.1111/1471-0528.12185 . [DOI] [PubMed] [Google Scholar]
- 33.Whetten K, Shirey K, Pence BW, Yao J, Thielman N, Whetten R, et al. Trauma history and depression predict incomplete adherence to antiretroviral therapies in a low income country. PloS one. 2013;8(10):e74771 Epub 2013/10/15. 10.1371/journal.pone.0074771 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kinyanda E, Hoskins S, Nakku J, Nawaz S, Patel V. The prevalence and characteristics of suicidality in HIV/AIDS as seen in an African population in Entebbe district, Uganda. BMC psychiatry. 2012;12:63 Epub 2012/06/21. 10.1186/1471-244X-12-63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Peltzer K, Naidoo P, Matseke G, Louw J, McHunu G, Tutshana B. Prevalence of post-traumatic stress symptoms and associated factors in tuberculosis (TB), TB retreatment and/or TB-HIV co-infected primary public health-care patients in three districts in South Africa. Psychology, health & medicine. 2013;18(4):387–97. Epub 2012/10/16. 10.1080/13548506.2012.726364 . [DOI] [PubMed] [Google Scholar]
- 36.El-Sayed AM, Hadley C, Tessema F, Tegegn A, Cowan JA Jr., Galea S. Back and neck pain and psychopathology in rural sub-Saharan Africa: evidence from the Gilgel Gibe Growth and Development Study, Ethiopia. Spine (Phila Pa 1976). 2010;35(6):684–9. Epub 2010/02/09. 10.1097/BRS.0b013e3181b4926e [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Adewuya AO, Ologun YA, Ibigbami OS. Post-traumatic stress disorder after childbirth in Nigerian women: prevalence and risk factors. BJOG. 2006;113(3):284–8. Epub 2006/02/21. 10.1111/j.1471-0528.2006.00861.x . [DOI] [PubMed] [Google Scholar]
- 38.Chhagan MK, Mellins CA, Kauchali S, Craib MH, Taylor M, Kvalsvig JD, et al. Mental health disorders among caregivers of preschool children in the Asenze study in KwaZulu-Natal, South Africa. Maternal and child health journal. 2014;18(1):191–9. Epub 2013/03/08. 10.1007/s10995-013-1254-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kuo C, Operario D. Health of adults caring for orphaned children in an HIV-endemic community in South Africa. AIDS care. 2011;23(9):1128–35. Epub 2011/04/12. 10.1080/09540121.2011.554527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ertl V, Saile R, Neuner F, Catani C. Drinking to ease the burden: a cross-sectional study on trauma, alcohol abuse and psychopathology in a post-conflict context. BMC psychiatry. 2016;16:202 Epub 2016/06/28. 10.1186/s12888-016-0905-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Verelst A, De Schryver M, Broekaert E, Derluyn I. Mental health of victims of sexual violence in eastern Congo: associations with daily stressors, stigma, and labeling. BMC women's health. 2014;14:106 Epub 2014/09/10. 10.1186/1472-6874-14-106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Mels C, Derluyn I, Broekaert E, Rosseel Y. Screening for traumatic exposure and posttraumatic stress symptoms in adolescents in the war-affected eastern Democratic Republic of Congo. Archives of pediatrics & adolescent medicine. 2009;163(6):525–30. Epub 2009/06/03. 10.1001/archpediatrics.2009.56 . [DOI] [PubMed] [Google Scholar]
- 43.Othieno CJ, Okoth R, Peltzer K, Pengpid S, Malla LO. Traumatic experiences, posttraumatic stress symptoms, depression, and health-risk behavior in relation to injury among University of Nairobi students in Kenya. Int J Psychiatry Med. 2015;50(3):299–316. Epub 2015/11/13. 10.1177/0091217415610310 . [DOI] [PubMed] [Google Scholar]
- 44.Oladeji BD, Morakinyo JJ, Gureje O. Traumatic events and post-traumatic stress symptoms among adolescents in Ibadan. African journal of medicine and medical sciences. 2011;40(1):23–31. Epub 2011/08/13. . [PubMed] [Google Scholar]
- 45.Neugebauer R, Fisher PW, Turner JB, Yamabe S, Sarsfield JA, Stehling-Ariza T. Post-traumatic stress reactions among Rwandan children and adolescents in the early aftermath of genocide. International journal of epidemiology. 2009;38(4):1033–45. 10.1093/ije/dyn375 . [DOI] [PubMed] [Google Scholar]
- 46.Saile R, Ertl V, Neuner F, Catani C. Does war contribute to family violence against children? Findings from a two-generational multi-informant study in Northern Uganda. Child abuse & neglect. 2014;38(1):135–46. Epub 2013/11/19. 10.1016/j.chiabu.2013.10.007 . [DOI] [PubMed] [Google Scholar]
- 47.Okello J, Nakimuli-Mpungu E, Musisi S, Broekaert E, Derluyn I. War-related trauma exposure and multiple risk behaviors among school-going adolescents in Northern Uganda: the mediating role of depression symptoms. Journal of affective disorders. 2013;151(2):715–21. Epub 2013/09/10. 10.1016/j.jad.2013.07.030 . [DOI] [PubMed] [Google Scholar]
- 48.O'Donnell DA, Roberts WC, Schwab-Stone ME. Community violence exposure and post-traumatic stress reactions among Gambian youth: the moderating role of positive school climate. Social psychiatry and psychiatric epidemiology. 2011;46(1):59–67. 10.1007/s00127-009-0162-x . [DOI] [PubMed] [Google Scholar]
- 49.Seedat S, Nyamai C, Njenga F, Vythilingum B, Stein DJ. Trauma exposure and post-traumatic stress symptoms in urban African schools. Survey in CapeTown and Nairobi. The British journal of psychiatry: the journal of mental science. 2004;184:169–75. Epub 2004/02/03. 10.1192/bjp.184.2.169 . [DOI] [PubMed] [Google Scholar]
- 50.Charlson F, van Ommeren M, Flaxman A, Cornett J, Whiteford H, Saxena S. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. Lancet. 2019;394(10194):240–8. Epub 2019/06/16. 10.1016/S0140-6736(19)30934-1 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Hoppen TH, Morina N. The prevalence of PTSD and major depression in the global population of adult war survivors: a meta-analytically informed estimate in absolute numbers. Eur J Psychotraumatol. 2019;10(1):1578637 Epub 2019/03/06. 10.1080/20008198.2019.1578637 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.OECD (2020). Working age population (indicator). [cited 27 Apr 2020]. 10.1787/d339918b-en [DOI]
- 53.Naing L, Winn T, Rusli B. Practical issues in calculating the sample size for prevalence studies. Archives of orofacial Sciences. 2006;1:9–14. [Google Scholar]
- 54.Kohrt BA, Rasmussen A, Kaiser BN, Haroz EE, Maharjan SM, Mutamba BB, et al. Cultural concepts of distress and psychiatric disorders: literature review and research recommendations for global mental health epidemiology. International journal of epidemiology. 2014;43(2):365–406. Epub 2013/12/25. 10.1093/ije/dyt227 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Moher D, Liberati A, Tetzlaff A, Altman DG, PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009;6(7):e1000097 10.1371/journal.pmed.1000097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Loney PL, Chambers LW, Bennett KJ, Roberts JG, Stratford PW. Critical appraisal of the health research literature: prevalence or incidence of a health problem. Chronic diseases in Canada. 1998;19(4):170–6. Epub 1999/02/24. . [PubMed] [Google Scholar]
- 57.Shamliyan T, Kane RL, Dickinson S. A systematic review of tools used to assess the quality of observational studies that examine incidence or prevalence and risk factors for diseases. Journal of clinical epidemiology. 2010;63(10):1061–70. Epub 2010/08/24. 10.1016/j.jclinepi.2010.04.014 . [DOI] [PubMed] [Google Scholar]
- 58.International Committee of the Red Cross (ICRC). How is the Term "Armed Conflict" Defined in International Humanitarian Law? March 2008. [cited 27 Apr 2020]. Available from: https://www.icrc.org/en/doc/assets/files/other/opinion-paper-armed-conflict.pdf.
- 59.StataCorp. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP.; 2015.
- 60.Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Archives of public health = Archives belges de sante publique. 2014;72(1):39 Epub 2014/01/01. 10.1186/2049-3258-72-39 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ: British Medical Journal. 2003;327(7414):557–60. 10.1136/bmj.327.7414.557 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Harbord RM, Higgins JPT. Meta-regression in Stata. Stata Journal. 2008;8(4):493–519. [Google Scholar]
- 63.Pence BW, Shirey K, Whetten K, Agala B, Itemba D, Adams J, et al. Prevalence of psychological trauma and association with current health and functioning in a sample of HIV-infected and HIV-uninfected Tanzanian adults. PloS one. 2012;7(5):e36304 Epub 2012/05/19. 10.1371/journal.pone.0036304 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Kohli A, Perrin N, Mpanano RM, Case J, Murhula CM, Binkurhorhwa AK, et al. Social interaction in the aftermath of conflict-related trauma experiences among women in Walungu Territory, Democratic Republic of Congo. Global public health. 2015;10(1):55–70. Epub 2014/11/05. 10.1080/17441692.2014.972426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Ayazi T, Lien L, Eide AH, Jenkins R, Albino RA, Hauff E. Disability associated with exposure to traumatic events: results from a cross-sectional community survey in South Sudan. BMC public health. 2013;13:469 Epub 2013/05/16. 10.1186/1471-2458-13-469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Jenkins R, Njenga F, Okonji M, Kigamwa P, Baraza M, Ayuyo J, et al. Psychotic symptoms in Kenya—prevalence, risk factors, and relationship with common mental disorders. Int J Environ Res Public Health. 2012;9(5):1748–56. Epub 2012/07/04. 10.3390/ijerph9051748 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Johnson K, Asher J, Rosborough S, Raja A, Panjabi R, Beadling C, et al. Association of combatant status and sexual violence with health and mental health outcomes in postconflict Liberia. JAMA: the journal of the American Medical Association. 2008;300(6):676–90. 10.1001/jama.300.6.676 . [DOI] [PubMed] [Google Scholar]
- 68.Vinck P, Pham PN. Association of exposure to intimate-partner physical violence and potentially traumatic war-related events with mental health in Liberia. Social science & medicine. 2013;77:41–9. Epub 2012/12/12. 10.1016/j.socscimed.2012.10.026 . [DOI] [PubMed] [Google Scholar]
- 69.Eytan A, Munyandamutsa N, Nkubamugisha PM, Gex-Fabry M. Long-term mental health outcome in post-conflict settings: Similarities and differences between Kosovo and Rwanda. The International journal of social psychiatry. 2015;61(4):363–72. Epub 2014/08/26. 10.1177/0020764014547062 . [DOI] [PubMed] [Google Scholar]
- 70.Munyandamutsa N, Nkubamugisha PM, Gex-Fabry M, Eytan A. Mental and physical health in Rwanda 14 years after the genocide. Social psychiatry and psychiatric epidemiology. 2012;47(11):1753–61. 10.1007/s00127-012-0494-9 [DOI] [PubMed] [Google Scholar]
- 71.Jalloh MF, Li W, Bunnell RE, Ethier KA, O’Leary A, Hageman KM, et al. Impact of Ebola experiences and risk perceptions on mental health in Sierra Leone, July 2015. BMJ global health. 2018;3(2):e000471 Epub 2018/04/03. 10.1136/bmjgh-2017-000471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Atwoli L, Stein DJ, Williams DR, McLaughlin KA, Petukhova M, Kessler RC, et al. Trauma and posttraumatic stress disorder in South Africa: analysis from the South African Stress and Health Study. BMC psychiatry. 2013;13:182 Epub 2013/07/04. 10.1186/1471-244X-13-182 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Atwoli L, Stein DJ, King A, Petukhova M, Aguilar-Gaxiola S, Alonso J, et al. Posttraumatic stress disorder associated with unexpected death of a loved one: Cross-national findings from the world mental health surveys. Depression and anxiety. 2017;34(4):315–26. Epub 2016/12/07. 10.1002/da.22579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Stein DJ, Seedat S, Herman A, Moomal H, Heeringa SG, Kessler RC, et al. Lifetime prevalence of psychiatric disorders in South Africa. The British journal of psychiatry: the journal of mental science. 2008;192(2):112–7. Epub 2008/02/05. 10.1192/bjp.bp.106.029280 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Herman AA, Stein DJ, Seedat S, Heeringa SG, Moomal H, Williams DR. The South African Stress and Health (SASH) study: 12-month and lifetime prevalence of common mental disorders. South African medical journal = Suid-Afrikaanse tydskrif vir geneeskunde. 2009;99(5 Pt 2):339–44. Epub 2009/07/11. [PMC free article] [PubMed] [Google Scholar]
- 76.Williams DR, Gonzalez HM, Williams S, Mohammed SA, Moomal H, Stein DJ. Perceived discrimination, race and health in South Africa. Social science & medicine. 2008;67(3):441–52. 10.1016/j.socscimed.2008.03.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Peltzer K, Pengpid S. High physical activity is associated with post-traumatic stress disorder among individuals aged 15 years and older in South Africa. The South African journal of psychiatry: SAJP: the journal of the Society of Psychiatrists of South Africa. 2019;25:1329 Epub 2019/11/21. 10.4102/sajpsychiatry.v25i0.1329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Neuner F, Pfeiffer A, Schauer-Kaiser E, Odenwald M, Elbert T, Ertl V. Haunted by ghosts: prevalence, predictors and outcomes of spirit possession experiences among former child soldiers and war-affected civilians in Northern Uganda. Social science & medicine. 2012;75(3):548–54. Epub 2012/05/15. 10.1016/j.socscimed.2012.03.028 . [DOI] [PubMed] [Google Scholar]
- 79.Ertl V, Pfeiffer A, Schauer-Kaiser E, Elbert T, Neuner F. The challenge of living on: psychopathology and its mediating influence on the readjustment of former child soldiers. PloS one. 2014;9(7):e102786 Epub 2014/07/24. 10.1371/journal.pone.0102786 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Rugema L, Mogren I, Ntaganira J, Krantz G. Traumatic episodes and mental health effects in young men and women in Rwanda, 17 years after the genocide. BMJ open. 2015;5(6):e006778 Epub 2015/06/26. 10.1136/bmjopen-2014-006778 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Topper K, van Rooyen K, Grobler C, van Rooyen D, Andersson LM. Posttraumatic Stress Disorder and Barriers to Care in Eastern Cape Province, South Africa. Journal of traumatic stress. 2015;28(4):375–9. Epub 2015/08/14. 10.1002/jts.22032 . [DOI] [PubMed] [Google Scholar]
- 82.Smit J, Myer L, Middelkoop K, Seedat S, Wood R, Bekker LG, et al. Mental health and sexual risk behaviours in a South African township: a community-based cross-sectional study. Public health. 2006;120(6):534–42. Epub 2006/05/11. 10.1016/j.puhe.2006.01.009 . [DOI] [PubMed] [Google Scholar]
- 83.Asnakew S, Shumet S, Ginbare W, Legas G, Haile K. Prevalence of post-traumatic stress disorder and associated factors among Koshe landslide survivors, Addis Ababa, Ethiopia: a community-based, cross-sectional study. BMJ open. 2019;9(6):e028550 10.1136/bmjopen-2018-028550 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Galea S, Rockers PC, Saydee G, Macauley R, Varpilah ST, Kruk ME. Persistent psychopathology in the wake of civil war: long-term posttraumatic stress disorder in Nimba County, Liberia. American journal of public health. 2010;100(9):1745–51. Epub 2010/07/17. 10.2105/AJPH.2009.179697 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Machisa MT, Christofides N, Jewkes R. Mental ill health in structural pathways to women’s experiences of intimate partner violence. PloS one. 2017;12(4):e0175240 Epub 2017/04/07. 10.1371/journal.pone.0175240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Mollica R, Caspi-Yavin Y, Lavelle J. The Harvard Trauma Questionnaire (HTQ) manual: Cambodian, Laotian, and Vietnamese Versions. Torture Quarterly Journal on Rehabilitation of Torture Victims and Prevention of Torture. 1996;(Supplement 1):19–42. [Google Scholar]
- 87.Weathers F, Litz B, Herman D, Huska J, Keane T. The PTSD checklist-civilian version (PCL-C). Boston, MA: National Center for PTSD; 1994. [Google Scholar]
- 88.Brewin CR, Rose S, Andrews B, Green J, Tata P, McEvedy C, et al. Brief screening instrument for post-traumatic stress disorder. The British journal of psychiatry: the journal of mental science. 2002;181:158–62. Epub 2002/08/02. 10.1017/s0007125000161896 . [DOI] [PubMed] [Google Scholar]
- 89.Davidson JR, Book SW, Colket JT, Tupler LA, Roth S, David D, et al. Assessment of a new self-rating scale for post-traumatic stress disorder. Psychological medicine. 1997;27(1):153–60. Epub 1997/01/01. 10.1017/s0033291796004229 . [DOI] [PubMed] [Google Scholar]
- 90.Foa EB, Cashman L, Jaycox LH, Perry K. The validation of a self-report measure of posttraumatic stress disorder: The Posttraumatic Diagnostic Scale. Psychological assessment. 1997;9(4):445–51. 10.1037/1040-3590.9.4.445. [DOI] [Google Scholar]
- 91.Thoresen S, Tambs K, Hussain A, Heir T, Johansen VA, Bisson JI. Brief measure of posttraumatic stress reactions: impact of Event Scale-6. Social psychiatry and psychiatric epidemiology. 2010;45(3):405–12. Epub 2009/05/30. 10.1007/s00127-009-0073-x . [DOI] [PubMed] [Google Scholar]
- 92.Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59 Suppl 20:22–33;quiz 4–57. Epub 1999/01/09. . [PubMed] [Google Scholar]
- 93.Foa EB, Riggs DS, Dancu CV, Rothbaum BO. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. 1993. 1994-15951-001. [Google Scholar]
- 94.Robins LN, Wing J, Wittchen HU, Helzer JE, Babor TF, Burke J, et al. The Composite International Diagnostic Interview. An epidemiologic Instrument suitable for use in conjunction with different diagnostic systems and in different cultures. Archives of general psychiatry. 1988;45(12):1069–77. Epub 1988/12/01. 10.1001/archpsyc.1988.01800360017003 . [DOI] [PubMed] [Google Scholar]
- 95.Ertl V, Pfeiffer A, Saile R, Schauer E, Elbert T, Neuner F. Validation of a mental health assessment in an African conflict population. Psychological assessment. 2010;22(2):318–24. Epub 2010/06/10. 10.1037/a0018810 . [DOI] [PubMed] [Google Scholar]
- 96.Fodor KE, Pozen J, Ntaganira J, Sezibera V, Neugebauer R. The factor structure of posttraumatic stress disorder symptoms among Rwandans exposed to the 1994 genocide: A confirmatory factor analytic study using the PCL-C. J Anxiety Disord. 2015;32:8–16. Epub 2015/04/04. 10.1016/j.janxdis.2015.03.001 . [DOI] [PubMed] [Google Scholar]
- 97.Betancourt TS, Brennan RT, Vinck P, VanderWeele TJ, Spencer-Walters D, Jeong J, et al. Associations between Mental Health and Ebola-Related Health Behaviors: A Regionally Representative Cross-sectional Survey in Post-conflict Sierra Leone. PloS medicine. 2016;13(8):e1002073 Epub 2016/08/10. 10.1371/journal.pmed.1002073 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Gureje O, Lasebikan VO, Kola L, Makanjuola VA. Lifetime and 12-month prevalence of mental disorders in the Nigerian Survey of Mental Health and Well-Being. The British journal of psychiatry: the journal of mental science. 2006;188:465–71. Epub 2006/05/02. 10.1192/bjp.188.5.465 . [DOI] [PubMed] [Google Scholar]
- 99.Ayazi T, Lien L, Eide AH, Ruom MM, Hauff E. What are the risk factors for the comorbidity of posttraumatic stress disorder and depression in a war-affected population? A cross-sectional community study in South Sudan. BMC psychiatry. 2012;12:175 Epub 2012/10/23. 10.1186/1471-244X-12-175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Kessler RC, Ustun TB. The World Mental Health (WMH) Survey Initiative Version of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). Int J Methods Psychiatr Res. 2004;13(2):93–121. Epub 2004/08/07. 10.1002/mpr.168 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Morina N, Stam K, Pollet TV, Priebe S. Prevalence of depression and posttraumatic stress disorder in adult civilian survivors of war who stay in war-afflicted regions. A systematic review and meta-analysis of epidemiological studies. Journal of affective disorders. 2018;239:328–38. Epub 2018/07/22. 10.1016/j.jad.2018.07.027 . [DOI] [PubMed] [Google Scholar]
- 102.World Health Organization. mhGAP in Ethiopia: Proof of Concept. 2013. [cited 27 Apr 2020]. Available from: https://www.who.int/mental_health/mhgap/mhgap_ethiopia_proof_of_concept_2013.pdf.
- 103.Bolton P, Wilk CM, Ndogoni L. Assessment of depression prevalence in rural Uganda using symptom and function criteria. Social psychiatry and psychiatric epidemiology. 2004;39(6):442–7. Epub 2004/06/19. 10.1007/s00127-004-0763-3 . [DOI] [PubMed] [Google Scholar]
- 104.Bolton P, Neugebauer R, Ndogoni L. Prevalence of depression in rural Rwanda based on symptom and functional criteria. The Journal of nervous and mental disease. 2002;190(9):631–7. Epub 2002/10/03. 10.1097/00005053-200209000-00009 . [DOI] [PubMed] [Google Scholar]
- 105.Mollica RF, McInnes K, Sarajlic N, Lavelle J, Sarajlic I, Massagli MP. Disability associated with psychiatric comorbidity and health status in Bosnian refugees living in Croatia. JAMA: the journal of the American Medical Association. 1999;282(5):433–9. Epub 1999/08/12. 10.1001/jama.282.5.433 . [DOI] [PubMed] [Google Scholar]
- 106.McLaughlin KA, Koenen KC, Friedman MJ, Ruscio AM, Karam EG, Shahly V, et al. Subthreshold posttraumatic stress disorder in the world health organization world mental health surveys. Biological psychiatry. 2015;77(4):375–84. Epub 2014/05/21. 10.1016/j.biopsych.2014.03.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Michalopoulos LM, Meinhart M, Yung J, Barton SM, Wang X, Chakrabarti U, et al. Global Posttrauma Symptoms: A Systematic Review of Qualitative Literature. Trauma, violence & abuse. 2018:1524838018772293 Epub 2018/04/28. 10.1177/1524838018772293 . [DOI] [PubMed] [Google Scholar]
- 108.First M, B., Spitzer R, L., Gibbon M, Williams Janet BW. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Non-patient Edition (SCID-I/NP). New York, NY: New York State Psychiatric Institute, 2002. [Google Scholar]
- 109.Madigoe T, Burns J, Zhang M, Subramaney U. Towards a culturally appropriate trauma assessment in a South African Zulu community. Psychol Trauma. 2017;9(3):274–81. Epub 2017/05/02. 10.1037/tra0000231 . [DOI] [PubMed] [Google Scholar]
- 110.Haroz EE, Bass JK, Lee C, Murray LK, Robinson C, Bolton P. Adaptation and testing of psychosocial assessment instruments for cross-cultural use: an example from the Thailand Burma border. BMC psychology. 2014;2(1):31 Epub 2015/02/17. 10.1186/s40359-014-0031-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Hyman SE. The Unconscionable Gap Between What We Know and What We Do. Science Translational Medicine. 2014;6(253):253cm9 10.1126/scitranslmed.3010312 [DOI] [PubMed] [Google Scholar]
- 112.Mental health atlas 2017. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO.
- 113.van Aert RCM, Wicherts JM, van Assen MALM. Publication bias examined in meta-analyses from psychology and medicine: A meta-meta-analysis. PloS one. 2019;14(4):e0215052–e. 10.1371/journal.pone.0215052 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.The World Health Organization. Download the WHO WMH-CIDI Instruments 2017 [cited 2019 March 7]. Available from: https://www.hcp.med.harvard.edu/wmhcidi/download-the-who-wmh-cidi-instruments/.
- 115.Jewkes R, Abrahams N. The epidemiology of rape and sexual coercion in South Africa: an overview. Social science & medicine. 2002;55(7):1231–44. Epub 2002/10/09. 10.1016/s0277-9536(01)00242-8 . [DOI] [PubMed] [Google Scholar]
- 116.American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-IV). 4th ed. Washington DC: American Psychiatric Association; 2000. [Google Scholar]
- 117.van Ommeren M, Sharma B, Makaju R, Thapa S, de Jong J. Limited Cultural Validity of the Composite International Diagnostic Interview’s Probe Flow Chart. Transcult Psychiatry. 2000;37(1):119–29. 10.1177/136346150003700107. [DOI] [Google Scholar]
- 118.Gelaye B, Williams MA, Lemma S, Deyessa N, Bahretibeb Y, Shibre T, et al. Diagnostic validity of the composite international diagnostic interview (CIDI) depression module in an East African population. Int J Psychiatry Med. 2013;46(4):387–405. Epub 2013/01/01. 10.2190/PM.46.4.e [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Beals J, Manson SM, Whitesell NR, Mitchell CM, Novins DK, Simpson S, et al. Prevalence of major depressive episode in two American Indian reservation populations: unexpected findings with a structured interview. The American journal of psychiatry. 2005;162(9):1713–22. Epub 2005/09/02. 10.1176/appi.ajp.162.9.1713 . [DOI] [PubMed] [Google Scholar]
- 120.Scorza P, Masyn K, Salomon JA, Betancourt TS. The impact of measurement differences on cross-country depression prevalence estimates: A latent transition analysis. PloS one. 2018;13(6):e0198429 Epub 2018/06/08. 10.1371/journal.pone.0198429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Lund C, Tomlinson M, De Silva M, Fekadu A, Shidhaye R, Jordans M, et al. PRIME: a programme to reduce the treatment gap for mental disorders in five low- and middle-income countries. PLoS medicine. 2012;9(12):e1001359 Epub 2013/01/10. 10.1371/journal.pmed.1001359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.World Health Organization. mhGAP intervention guide for mental, neurological and substance use disorders in non-specialized health settings: Mental Health Gap Action Programme (mhGAP). Geneva: World Health Organization; 2010. [PubMed] [Google Scholar]
- 123.World Health Organization and United Nations High Commissioner for Refugees. mhGAP Humanitarian Intervention Guide (mhGAP-HIG): clinical management of mental, neurological and substance use conditions in humanitarian emergencies (Version 1.0). Geneva: 2015.
- 124.Johnson K, Scott J, Rughita B, Kisielewski M, Asher J, Ong R, et al. Association of sexual violence and human rights violations with physical and mental health in territories of the Eastern Democratic Republic of the Congo. JAMA: the journal of the American Medical Association. 2010;304(5):553–62. 10.1001/jama.2010.1086 . [DOI] [PubMed] [Google Scholar]
- 125.Jenkins R, Othieno C, Omollo R, Ongeri L, Sifuna P, Mboroki JK, et al. Probable Post Traumatic Stress Disorder in Kenya and Its Associated Risk Factors: A Cross-Sectional Household Survey. Int J Environ Res Public Health. 2015;12(10):13494–509. Epub 2015/10/31. 10.3390/ijerph121013494 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Pham PN, Weinstein HM, Longman T. Trauma and PTSD symptoms in Rwanda: implications for attitudes toward justice and reconciliation. JAMA: the journal of the American Medical Association. 2004;292(5):602–12. 10.1001/jama.292.5.602 . [DOI] [PubMed] [Google Scholar]
- 127.Williams DR, Herman A, Stein DJ, Heeringa SG, Jackson PB, Moomal H, et al. Twelve-month mental disorders in South Africa: prevalence, service use and demographic correlates in the population-based South African Stress and Health Study. Psychological medicine. 2008;38(2):211–20. Epub 2007/10/02. 10.1017/S0033291707001420 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Myer L, Stein DJ, Grimsrud AT, Herman A, Seedat S, Moomal H, et al. DSM-IV-defined common mental disorders: association with HIV testing, HIV-related fears, perceived risk and preventive behaviours among South African adults. South African medical journal = Suid-Afrikaanse tydskrif vir geneeskunde. 2009;99(5 Pt 2):396–402. . [PMC free article] [PubMed] [Google Scholar]
- 129.Dückers MLA, Alisic E, Brewin CR. A vulnerability paradox in the cross-national prevalence of post-traumatic stress disorder. British Journal of Psychiatry. 2018;209(4):300–5. Epub 01/02. 10.1192/bjp.bp.115.176628 [DOI] [PubMed] [Google Scholar]
- 130.Ayazi T, Lien L, Eide A, Swartz L, Hauff E. Association between exposure to traumatic events and anxiety disorders in a post-conflict setting: a cross-sectional community study in South Sudan. BMC psychiatry. 2014;14:6 Epub 2014/01/15. 10.1186/1471-244X-14-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Ng LC, Lopez B, Pritchard M, Deng D. Posttraumatic stress disorder, trauma, and reconciliation in South Sudan. Social psychiatry and psychiatric epidemiology. 2017;52(6):705–14. Epub 2017/04/13. 10.1007/s00127-017-1376-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Roberts B, Damundu EY, Lomoro O, Sondorp E. Post-conflict mental health needs: a cross-sectional survey of trauma, depression and associated factors in Juba, Southern Sudan. BMC psychiatry. 2009;9:7 Epub 2009/03/06. 10.1186/1471-244X-9-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Mugisha J, Muyinda H, Wandiembe P, Kinyanda E. Prevalence and factors associated with Posttraumatic Stress Disorder seven years after the conflict in three districts in northern Uganda (The Wayo-Nero Study). BMC psychiatry. 2015;15:170 Epub 2015/07/25. 10.1186/s12888-015-0551-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Mugisha J, Muyinda H, Malamba S, Kinyanda E. Major depressive disorder seven years after the conflict in northern Uganda: burden, risk factors and impact on outcomes (The Wayo-Nero Study). BMC psychiatry. 2015;15:48 Epub 2015/04/17. 10.1186/s12888-015-0423-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Mugisha J, Muyinda H, Kagee A, Wandiembe P, Mpugu SK, Vancampfort D, et al. Prevalence of suicidal ideation and attempt: associations with psychiatric disorders and HIV/AIDS in post-conflict Northern Uganda. Afr Health Sci. 2016;16(4):1027–35. Epub 2017/05/10. 10.4314/ahs.v16i4.20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Pham PN, Vinck P, Stover E. Returning home: forced conscription, reintegration, and mental health status of former abductees of the Lord's Resistance Army in northern Uganda. BMC psychiatry. 2009;9:23 Epub 2009/05/19. 10.1186/1471-244X-9-23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Vinck P, Pham PN, Stover E, Weinstein HM. Exposure to war crimes and implications for peace building in northern Uganda. JAMA: the journal of the American Medical Association. 2007;298(5):543–54. 10.1001/jama.298.5.543 . [DOI] [PubMed] [Google Scholar]
- 138.American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM). Washington, DC: American Psychiatric Association; 1994. [Google Scholar]
- 139.World Health Organization. ICD-10: international statistical classification of diseases and related health problems: tenth revision. 2nd ed: World Health Organization; 2004. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOC)
Random test of herterogeneity between subgroups: 0.42, df = 1, p = 0.052. CI, confidence interval; ES, effect size (proportion)
(TIFF)
Random test of heterogeneity between subgroups: 79.61, df = 2, p < 0.001. CI, confidence interval; ES = efect size (proportion)
(TIFF)
Data Availability Statement
Due to the nature of the meta-analysis, all data are present in the paper and are therefore publicly available.