

Abstract
COVID‐19 is a pandemic that began in China in December 2019. World health organization (WHO) has expressed fears that Pakistan might emerge as the next epicenter of this pandemic. We hypothesize that at present the Pakistani masses are not prepared to face any threat of a looming epidemic. The main aim of this study was to evaluate the basic knowledge of educational and health care workers (HCWs) regarding COVID‐19, its control, and prevention. Knowledge about origin, symptoms, and spread of viral infection was assessed. In this cross‐sectional survey, a self‐designed questionnaire was distributed among 302 HCWs including physicians (10.9%), nurses (1.32%), lab staff (1.65%), and academic individuals including faculty and students (86.42%) of different organizations. Results were analyzed using the χ 2 test. Obtained results validate our null hypothesis that Pakistani masses are not well aware of the COVID‐19 and strategies for the prevention and control of infection. The study concluded that individuals belonging to the front‐line workers and high literacy groups are not prepared for the alarming situation in the country. Effectual implementation of infection control programs should be practiced, and it depends on awareness, training, and cooperation of individuals.
Keywords: awareness, coronavirus, COVID‐19, epidemic, Pakistan, preparedness
Highlights
Pakistan is facing a looming threat of COVID‐19 epidemic.
Strict measures need to be taken to avert the threat of COVID‐19.
Vigilant training sessions should be carried out for front‐line workers.
1. INTRODUCTION
COVID‐19 has been first reported as a cluster of pneumonia cases of unknown etiology from Wuhan, Hubei, Mainland China on 8th December 2019. 1 This novel coronavirus outbreak is believed to be originated from an animal source in individuals who visited the local seafood and animal market in Wuhan, after which community transmission led to the initial endemic turning into a pandemic. 2 , 3 Travel associated cases of COVID‐19 infection have been reported by different countries. 4 , 5 , 6 At present as the world health organization (WHO) has declared the COVID‐19 as a pandemic, Pakistan is facing a critical situation and strict measures need to be taken to avert the threat of a national health crisis. WHO has expressed its fears that Pakistan is facing a major COVID‐19 challenge. They mentioned that if effective measurements are not taken Pakistan might emerge as the next epicenter of this pandemic. 7 , 8 , 9 It is believed that insufficient consideration is given to the basic infection control protocols including hand washing and personal protective equipment use in the educational and health care institutes of the country. The Ministry of Health, Pakistan has declared new guidelines for infection control which are based on the WHO recommendations. 10 However, the implementation of the basic infection control protocols is possible only when people and employees are made aware of the introduced policies by giving them clear guidelines. Awareness level and compliance of the educational and healthcare workers play an important role in the effective and timely prevention and control of a public health crisis. 11 To formulate a healthy policy, the multi‐disciplinary teams including key front‐line workers should be a part of the policy planning to ensure that these policies function effectively. 12 Pakistan faces many specific challenges about infection control that must be met by devising national policies.
Our null hypothesis states that “Pakistani masses are not prepared to face a looming threat of a COVID‐19 epidemic.” The main aim of the present questionnaire‐based analysis was to check the awareness level among the employees at educational institutes and the health care workers (HCWs) in various organizations across Pakistan. Questionnaires were filled by diverse groups of faculty, students, HCWs (physicians, nurses and lab staff). These questionnaires addressed access to information, training, confidence in the ability of faculty and HCWs to implement the introduced policies at their workplaces and asses the main threats which could lead to a possible public health crisis. These forms also evaluated the level of preparedness that any institute had to deal with a COVID‐19 outbreak.
2. METHODS
2.1. Subjects
A total of 303 individuals were included in this study. These include students and faculty (261) and HCWs (41) of which 32 physicians, 4 nurses and 5 laboratory staff in public and private sector educational and health institutes across Pakistan filled a questionnaire.
2.2. Questionnaire
View of students, faculty and HCWs from educational and health institutes regarding the recent public health emergency of the pandemic COVID‐19 was collected by filling in a standardized questionnaire. Questionnaires were distributed using the quick mode of communications including Facebook, emails, and WhatsApp. Anonymous responses were recorded and no ethical approval was required for this survey. Feedback was taken based on their knowledge about COVID‐19, its spread, and prevention and control measures implemented at their organizations. The questionnaire contained 21 different questions on basic knowledge of the infection, personal attitudes, and common practices during infection outbreak, control programs and policies, training and orientation conducted to bring awareness on origin, a common mode of transmission, signs, and symptoms. The participants were asked to either choose from given options or write their own opinion. Please access the manuscript at: https://forms.gle/r2SmQa4BEsb3QnJQ6.
2.3. Statistical analysis
All the data were analyzed with computer software SPSS version 21. The χ 2 test was applied and P value .1 or less was considered significant. Level of significance was measured to evaluate the difference in proportion among different respondent groups (HCW and professionals from educational institutes).
3. RESULTS AND DISCUSSIONS
3.1. Characteristics of study group
In total 303 individuals including students and faculty (86.42%) and HCWs (13.56%) of which 10.59% physicians, 1.32% nurses and 1.65% laboratory staff in public and private sector educational and health institutes across Pakistan submitted their responses to the questionnaire. Figure 1 summarizes the characteristics of the study groups in terms of age, gender and organization (educational and health care). Out of these respondents, 50.99% were aged less than 25 years, 48.66% between 25 and 50 years, and 0.33% above 50 years comprising of 28.47% males and 71.52% females. A total of 12.58% of the respondents were from government hospitals, 7.61% were from private hospitals and 79.8% were from the educational institutes.
Figure 1.
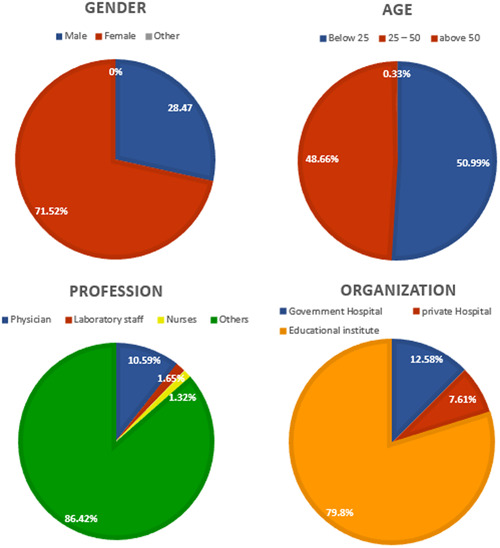
Visual representation of demographic characteristics of study group. A total of 28.74% (blue males and 71.52% (red) females participated in the study. A total of 50.99% of participants were below the age of 25 years, 48.66% were between ages 25 to 50 years and 0.33% belonged to the age group above 50 years. A total of 86.42% of participants belonged to the educational institutes, and 13.56% were health care workers. A total of 79.8% of respondents belonged to the educational institutes and 20.19% belonged to the health care workers (HCWs)
3.2. Profession‐based awareness
Responses to questions were compared among subjects from educational institutes, physicians, nurses, and lab staff. Response percentage in each group and their P values which were obtained using the χ 2 test are summarized in Table 1. The responses to questions regarding basic knowledge, that is name, origin, common signs and symptoms, sources of infection of COVID‐19 and awareness of any other pandemic viral infection in the past varied greatly.
Table 1.
Distribution of responses according to organization
| Number/percentage of group | ||||||
|---|---|---|---|---|---|---|
| Questions | Responses | All Organization (N = 302) | Educational institute (N = 241) | Government hospitals (N = 38) | Private hospitals (N = 23) | P value |
| 1 | Yes | 288/95.36 | 231/95.85 | 35/92.11 | 22/95.65 | .573 |
| No | 7/2.32 | 4/1.66 | 2//5.26 | 1/4.35 | ||
| Maybe | 7/2.32 | 6/2.49 | 1/2.63 | 0/0 | ||
| 2 | Yes | 249/82.45 | 199/82.57 | 31/81.58 | 19/82.61 | .872 |
| No | 27/8.94 | 20/8.3 | 4/10.53 | 3/13.04 | ||
| Maybe | 26/8.61 | 22/9.13 | 3/7.89 | 1/4.35 | ||
| 3 | Yes | 276/91.39 | 218/90.46 | 36/94.74 | 22/95.65 | .781 |
| No | 15/4.97 | 13/5.39 | 1/2.63 | 1/4.35 | ||
| Maybe | 11/3.64 | 10/4.15 | 1/2.63 | 0/0 | ||
| 4 | Yes | 31/10.26 | 29/12.03 | 2/5.26 | 0/0 | .049* |
| No | 131/43.38 | 99/41.08 | 16/42.11 | 16/69.57 | ||
| Maybe | 140/46.36 | 113/46.89 | 20/52.63 | 7/30.43 | ||
| 5 | Yes | 76/25.17 | 61/25.31 | 5/13.16 | 10/43.48 | .081* |
| No | 122/40.4 | 100/41.49 | 15/39.47 | 7/30.43 | ||
| Maybe | 104/34.44 | 80/33.2 | 18/47.37 | 6/26.09 | ||
| 6 | Yes | 104/34.44 | 83/34.44 | 10/26.32 | 11/47.83 | .395 |
| No | 123/40.73 | 101/41.91 | 16/42.11 | 6/26.09 | ||
| Maybe | 75/24.83 | 57/23.65 | 12/31.58 | 6/26.09 | ||
| 7 | Yes | 214/70.86 | 168/69.71 | 26/68.42 | 20/86.96 | .304 |
| No | 58/19.21 | 50/20.75 | 6/15.79 | 2/8.7 | ||
| Maybe | 30/9.93 | 23/9.54 | 6/15.79 | 1/4.35 | ||
| 8 | Yes | 223/73.84 | 181/75.1 | 27/71.05 | 15/65.22 | .587 |
| No | 12/3.97 | 8/3.32 | 3/7.89 | 1/4.35 | ||
| Maybe | 67/22.19 | 52/21.58 | 8/1.05 | 7/30.43 | ||
| 9 | Yes | 90/29.8 | 55/22.82 | 22/57.89 | 13/56.52 | .0001* |
| No | 158/52.32 | 136/56.43 | 13/34.21 | 9/39.13 | ||
| Maybe | 54/17.88 | 50/20.75 | 3/7.89 | 1/4.35 | ||
| 10 | Yes | 193/63.91 | 148/61.41 | 30/78.95 | 15/65.22 | .262 |
| No | 40/13.25 | 34/14.11 | 2/5.26 | 4/17.39 | ||
| Maybe | 69/22.85 | 59/24.48 | 6/15.79 | 4/17.39 | ||
| 11 | Yes | 115/38.08 | 82/34.02 | 21/55.26 | 12/52.17 | .046* |
| No | 171/56.62 | 114/47.3 | 17/44.74 | 10/43.48 | ||
| Maybe | 16/5.3 | 15/6.22 | 0/0 | 1/4.35 | ||
| 12 | Yes | 57/18.87 | 35/14.52 | 15/39.47 | 7/30.43 | .001* |
| No | 187/61.92 | 158/65.56 | 15/39.47 | 14/60.87 | ||
| Maybe | 58/19.21 | 48/19.92 | 8/21.05 | 2/8.7 | ||
| 13 | Yes | 78/25.83 | 56/23.24 | 13/34.21 | 9/39.13 | .208 |
| No | 122/40.4 | 98/40.66 | 14/36.84 | 10/43.48 | ||
| Maybe | 102/33.77 | 87/36.1 | 11/28.95 | 4/17.39 | ||
| 14 | Yes | 71/23.51 | 52/21.58 | 14/36.84 | 5/21.74 | .28 |
| No | 145/48.01 | 121/50.21 | 13/34.21 | 11/47.83 | ||
| Maybe | 86/28.48 | 68/28.22 | 11/28.95 | 7/30.43 | ||
| 15 | Yes | 171/56.62 | 134/55.6 | 23/60.53 | 14/60.87 | .564 |
| No | 41/13.58 | 32/13.28 | 4/10.53 | 5/21.74 | ||
| Maybe | 90/29.8 | 75/31.12 | 11/28.95 | 4/17.39 | ||
| 16 | Yes | 29/9.6 | 24/9.96 | 3/7.89 | 2/8.7 | .894 |
| No | 217/71.85 | 174/72.2 | 28/73.68 | 15/65.22 | ||
| Maybe | 56/18.54 | 43/17.84 | 7/18.42 | 6/26.09 | ||
Significant results P value < .1.
In response to a query regarding the name of the virus 95.36%, individuals responded that they were aware and 2.32% responded that they did not know the name of the virus. A P value of .85 suggests that results were insignificant and the variables (profession and awareness regarding the name of the virus were not related). The second question posed was regarding the origin of COVID‐19, 82.45% of respondents said that they were aware of its origin, while 8.94% said that they did not know its origin, 8.61% of respondents were not sure whether they knew or not the origin of COVID‐19. The highest uncertainty (50) about the origin of COVID‐19 was found among the nurses. Based on professional awareness it was seen that 93.75% of physicians, 25% nurses, 100% lab technicians, and 81.61% of staff/students from educational institutions were aware of the origin of COVID‐19. P value of .022 suggested the significant result that the variable (profession and awareness of the viral origin were related). The third question posed was ‘are you aware of the signs and symptoms of COVID‐19′? 91.3% of people said that they knew the signs and symptoms while 4.97% said that they were not aware of them while 3.64% said that maybe they were aware and maybe not. P value .257 suggests that variables (profession and awareness of signs and symptoms are not linked). The fourth query posed was “does having flu, fever, and cough means that you are infected.” Response reflected that 10.26% of people said yes, 43.38% said no and 46.36% reported maybe. A P value of .155 suggests that the profession and awareness of COVID‐19 symptoms are not linked. From our results, it is clear that most people have heard about the name and origin of COVID‐19 but people who think that they are aware of signs and symptoms are not aware of it. Physicians seemed to be most aware of the signs and symptoms of COVID‐19 indicating that awareness level is linked to the profession of an individual.
There were insignificant variations in response to the query concerning the acquisition of infection from an incoming parcel from china presented in a P value of .285. From the total respondents, 25.17% of people answered yes while 40.4% in no and 34.44% responded maybe. Concerning the acquisition of infection from pets (question 7) insignificant results were obtained (P value .285). A total of 34.44% of people are of the view that they can get it from pets while 40.73% think that it is not possible while 24.83% are uncertain about this query. These results indicate that people in Pakistan are uncertain of the viral acquisition routes and the majority will not follow the standard precautionary measures.
Significant data (P value .042) was obtained regarding knowledge about other pandemic viral infections of the past. A total of 70.86% of individuals knew of the past pandemic, 19.21% didn't know of any pandemic of the past while 9.93% were uncertain. Regarding information about how the viral transmission can be stopped in Pakistan, respondents were uncertain, and result obtained was not significant (P value .181). The 73.84% of respondents believed that viral transmission in Pakistan can be prevented, while 3.97% said that it cannot be prevented. In 22.19% respondent's uncertainty was observed. Pakistani people are well aware of the pandemics of the past but many people are uncertain that the looming threat of an upcoming COVID‐19 epidemic can be averted.
The responses to the questions related to the institute specific queries varied in terms of awareness. A P value of .0001 suggested significant results regarding the institutional infection control program query. 29.8% of the respondents were aware of an infection control program at their institute while 52.32% were unaware of any existing infection control program. A total of 17.88% of the respondents were uncertain. The HCWs were more aware of the infection control strategies at their institutes as compared to the academic respondents. Among the HCWs 59.38% of physicians, 75% nurses and 60% lab staff were aware of the existing institutional safety program while in the case of academic staff only 24.9% of respondents answered in affirmation. The query regarding the existence of an emerging infection task force was also significant (0.006). Only 18.87% of respondents were aware of an existing task force. Among HCWs 31.25% physicians, 25% nurses, 60% lab staff and 16.48% academic personnel were aware of an existing task force. The Pakistani masses are not prepared to encounter a potential COVID‐19 outbreak at their institute as many are unaware of the existence of any emergency response team.
The results regarding the infection control policies and guidelines of the country were insignificant (P value .811). A total of 63.91% of respondents said that they were aware of the countries policy concerning COVID‐19 pandemic while 13.25% were unaware and 22.85% were uncertain. Among HCWs highest uncertainty exist among the lab staff while physicians were least uncertain. When asked about any formal training of infection prevention and control the responses were insignificant (P value .237). Only 57.25% physicians, 50% nurses, 60% lab staff and 35.25% academic individuals had received any formal training of infection control. Almost half of the HCWs who participated in the survey have not undertaken any formal training to deal with a COVID‐19 case which shows that front‐line workers are not prepared.
Regarding the staff behavior in public health, emergency respondents were uncertain as depicted by P value .287. Only 25.83% of people said that their fellow staff is taking the necessary measures while 40.4% believe that it is not so, however, 33.77% were uncertain. A total of 46.88% of physicians believe that their fellow staff is not prompt, 50% of nurses and 40% of lab staff also believe the same. In the case of academic personnel, only 24.14% believe that their fellows are prompt and taking the necessary precautions. In general, individuals are not cautious enough to protect themselves and people around.
It was found from the results that both health care (48.01%) and academic professionals (49.43%) do not believe that their organization is prepared for an infection outbreak. While queries about the cure of the viral infection got positive responses both from HCWs including 62.5% physicians, 100% nurses and 55.56% from academic staff. A least positive response was obtained from lab staff (40%) for this query.
The overall response to the query about practicing the social distancing was satisfactory, 71.88% from physicians, 50% nurses, 60% lab staff, and 72.41% academic staff were of the view that going to public and their workplace is not safe.
For the query about sources of information regarding COVID‐19, the internet, and social media remained at the highest level while the newspaper is considered as the third source of information in all professions however most prominent trend was noticed in academic subjects (Figure 2).
Figure 2.
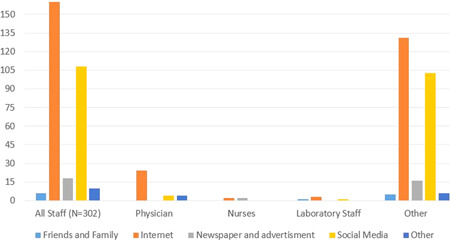
Bar chart for distribution of responses according to profession. This figure represents the various sources used by the people to gather knowledge about COVID‐19. Light blue bar represents friends and family, orange bar stands for internet sources, gray bar represents newspaper and advertisement, the yellow bar represents social media and dark blue bar stands for other sources of information
3.3. Organization based awareness
Organization wise distribution of the responses is shown in Table 2. Results are presented in terms of several respondents and percentages; the P value is also recorded for each response. The overall trend of the queries regarding name, origin and common signs and symptoms of COVID‐19 lies approximately in a similar range for all types of institutes. However, the least uncertainty was found in the participants of the private hospital. In the question about having cough and fever mean a person is infected, the least response in yes was recorded from the respondents of the private hospital (0/0) however the highest level of uncertainty was recorded for Government hospital subjects (52.63%). Queries about the catching of viral infections from parcels coming from china and pets, most people from all included organizations were of the view that they cannot get an infection from both these sources. Data represented in Table 3 about the previous pandemics, a high level of awareness was found in all organizations. A similar pattern of responses was noticed in a query about the spread of infection in Pakistan. It is clear from the data presented in Table 3 that most people think that viral spared can be stopped in Pakistan. In the same query people from educational institutes also showed their uncertain opinion. Queries about the infection control program in the particular institute, country's infection control policies and guidelines, training for infection, prevention, control and readiness of institutes for the emerging outbreak in the country got responses in No. When asked about the staff's attitude towards the outbreak, mix responses obtained majorly in No and Maybe while little answered in Yes. In the query about the preparation of the organization for the COVID‐19 outbreak, most people thought that their organization is not ready for a deadly outbreak of viral infection.
Table 2.
Gender‐based distribution of healthcare professionals and academic staff ( χ 2 = 9.818; P value = 0.02); age group distribution of healthcare by profession and organization type (profession χ 2 = 34.594 P value = .0001 organization χ 2 = 33.036; P value = .0001)
| Gender | ||||
|---|---|---|---|---|
| Male (N = 86) | Female (N = 216) | |||
| Profession | N [expected] [percentage of male] | N [expected] [percentage of male] | ||
| Physician | 16 [9.1] [18.60] | 16 [22.9] [7.41] | ||
| Nursing | 2 [1.1] [2.33] | 2 [2.9] [0.93] | ||
| Laboratory staff | 2 [1.4] [2.33] | 3 [3.6] [1.39] | ||
| Others | 66 [74.3] [76.7] | 195 [186.7] [90.3] | ||
| Age group | ||||
|---|---|---|---|---|
| Below 25 (N = 154) | 25‐50 (N = 147) | Above 50 (N = 1) | ||
| N [expected] [percentage] | N [expected] [percentage] | N [expected] [percentage] | ||
| Profession | ||||
| Physician | 4 [16.3] [2.59] | 25 [15.6] [17.0] | 1 [.1] [100] | |
| Nurses | 2 [2.0] [1.29] | 2 [1.9] [1.36] | 0 [0] [0] | |
| Laboratory staff | 0 [2.5] [0] | 5 [2.4] [3.40] | 0 [0] [0] | |
| Other | 148 [133.1] [96.1] | 113 [127.0] [76.87] | 0 [.9] [0] | |
| Organization | ||||
| Educational institutes | 141 [122.9] [91.5] | 100 [117.3] [68.02] | 0 [.8] [0] | |
| Government hospitals | 7 [19.4] [4.54] | 30 [18.5] [20.4] | 1 [.1] [100] | |
| Private hospitals | 6 [11.7] [11.2] | 17 [11.2] [11.56] | 0 [.1] [0] | |
Table 3.
Distribution of responses according to profession
| Number/percentage of group | |||||||
|---|---|---|---|---|---|---|---|
| Questions | Responses | All staff (N = 302) | Physician (N = 32) | Nurses (N = 4) | Laboratory staff (N = 5) | Other (N = 261) | P value |
| 1 | Yes | 288/95.36 | 32/100 | 3/75.0 | 5/100 | 248/95.02 | .85 |
| No | 7/2.32 | 0/0 | 1/25.0 | 0/0 | 6/2.3 | ||
| Maybe | 7/2.32 | 0/0 | 0/0 | 0/0 | 7/2.68 | ||
| 2 | Yes | 249/82.45 | 30/93.75 | 1/25.0 | 5/100 | 213/81.61 | .022* |
| No | 27/8.94 | 1/3.13 | 1/25.0 | 0/0 | 25/9.58 | ||
| Maybe | 26/8.61 | 1/3.13 | 2/50.0 | 0/0 | 23/8.81 | ||
| 3 | Yes | 276/8.61 | 32/100 | 4/100 | 4/80.0 | 236/90.42 | .257 |
| No | 15/4.97 | 0/0 | 0/0 | 0/0 | 15/5.75 | ||
| Maybe | 11/3.64 | 0/0 | 0/0 | 1/20.0 | 10/3.83 | ||
| 4 | Yes | 31/0.26 | 1/3.13 | 0/0 | 0/0 | 30/11.49 | .155 |
| No | 131/43.38 | 21/65.63 | 2/50.0 | 3/60.0 | 105/40.23 | ||
| Maybe | 140/46.36 | 10/31.25 | 2/50.0 | 2/40.0 | 126/48.28 | ||
| 5 | Yes | 76/25.17 | 7/21.88 | 1/25.0 | 1/20.0 | 67/25.67 | .285 |
| No | 122/40.4 | 18/56.25 | 0/0 | 2/40.0 | 102/39.08 | ||
| Maybe | 104/34.44 | 7/21.88 | 3/75.0 | 2/40.0 | 92/35.25 | ||
| 6 | Yes | 104/34.44 | 10/31.25 | 3/75.0 | 1/20.0 | 90/34.48 | .607 |
| No | 123/40.73 | 14/43.75 | 0/0 | 3/60.0 | 106/40.61 | ||
| Maybe | 75/24.83 | 8/20.0 | 1/25.0 | 1/20.0 | 65/24.9 | ||
| 7 | Yes | 214/70.86 | 27/84.38 | 2/50.0 | 5/100 | 214/81.99 | .042* |
| No | 58/19.21 | 4/12.5 | 0/0 | 0/0 | 58/22.22 | ||
| Maybe | 30/9.93 | 1/3.13 | 2/50.0 | 0/0 | 30/11.49 | ||
| 8 | Yes | 223/73.84 | 22/68.75 | 4/100 | 4/80.0 | 193/73.95 | .181 |
| No | 12/3.97 | 3/9.38 | 0/0 | 1/20.0 | 8/3.07 | ||
| Maybe | 67/22.19 | 7/21.88 | 0/0 | 0/0 | 60/22.99 | ||
| 9 | Yes | 90/29.8 | 19/59.38 | 3/75.0 | 3/60.0 | 65/24.9 | .0001* |
| No | 158/52.32 | 12/37.5 | 1/25.0 | 1/20.0 | 144/55.17 | ||
| Maybe | 54/17.88 | 1/3.13 | 0/0 | 1/20.0 | 52/19.92 | ||
| 10 | Yes | 193/63.91 | 23/71.88 | 2/50.0 | 3/60.0 | 165/63.22 | .811 |
| No | 40/13.25 | 4/12.5 | 1/25.0 | 0/0 | 35/3.41 | ||
| Maybe | 69/22.85 | 5/15.63 | 1/25.0 | 2/40.0 | 61/23.37 | ||
| 11 | Yes | 115/38.08 | 18/56.25 | 2/50.0 | 3/60.0 | 92/35.25 | .237 |
| No | 171/56.62 | 14/43.75 | 2/50.0 | 2/40.0 | 153/58.62 | ||
| Maybe | 16/5.3 | 0/0 | 0/0 | 0/0 | 16/6.13 | ||
| 12 | Yes | 57/18.87 | 10/31.25 | 1/25.0 | 3/60.0 | 43/16.48 | .006* |
| No | 187/61.92 | 20/62.5 | 1/25.0 | 0/0 | 166/63.6 | ||
| Maybe | 58/19.21 | 2/6.25 | 2/50.0 | 2/40.0 | 52/19.92 | ||
| 13 | Yes | 78/25.83 | 11/34.38 | 2/50.0 | 2/40.0 | 63/24.14 | .287 |
| No | 122/40.4 | 15/46.88 | 2/50.0 | 1/20.0 | 104/39.85 | ||
| Maybe | 102/33.77 | 6/18.75 | 0/0 | 2/40.0 | 94/36.02 | ||
| 14 | Yes | 71/23.51 | 7/21.88 | 1/25.0 | 3/60.0 | 60/22.99 | .33 |
| No | 145/48.01 | 15/46.88 | 1/25.0 | 0/0 | 129/49.43 | ||
| Maybe | 86/28.48 | 10/31.25 | 2/50.0 | 2/40.0 | 72/27.59 | ||
| 15 | Yes | 171/56.62 | 20/62.5 | 4/100 | 2/40.0 | 145/55.56 | .411 |
| No | 41/13.58 | 6/18.75 | 0/0 | 1/20.0 | 34/13.03 | ||
| Maybe | 90/29.8 | 6/18.75 | 0/0 | 2/40.0 | 82/31.42 | ||
| 16 | Yes | 29/9.6 | 3/9.38 | 0/0 | 0/0 | 26/9.96 | .573 |
| No | 217/71.85 | 23/71.88 | 2/50.0 | 3/60.0 | 189/72.41 | ||
| Maybe | 56/18.54 | 6/18.75 | 2/50.0 | 2/40.0 | 46/17.62 | ||
Significant results P value < .1.
When we look at the response of people about the latest update about COVID‐19, most people rely on getting information from the internet followed by social media (Figure 3).
Figure 3.
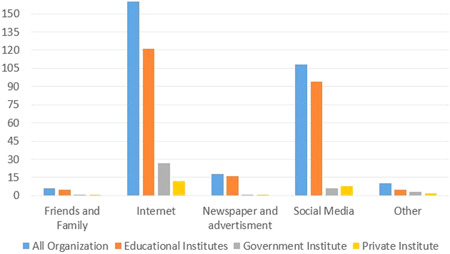
Bar chart for distribution of responses according to organization. This figure represents the various sources used by the people to gather knowledge about COVID‐19. Light blue bar represents all organizations, orange bar stands for educational institutes, gray bar represents government institute, the yellow bar represents private institute
3.4. Gender‐wise distribution of responses from HCWs and professionals from educational institutes
Male and female distribution across different professions was significantly varied ( χ 2 9.818; P value .001; Table 2). Physicians, nursing and laboratory staff were less likely to be male and female than expected, while the other was significantly more likely to be female and less likely to be male as compared to the expected. According to the profession, the distribution of responses to the questions was varied, so we checked whether gender has any impact on responses. However, both male and female response distribution is very much similar.
3.5. Age‐wise distribution of responses from different profession and organization type
According to the age group we also considered whether there might be a variation in an organization or profession type or question response. Distribution across different professions significantly varied according to different age groups (χ 2 34.594; P value .001; Table 2). It was observed that higher number of the physician than expected falling in 25 to 50 years’ group that were fewer in below 25‐year group, while the opposite is the case with other in which higher number of individual's fallings in both below 25 years and 25 to 50 years’ group (Table 2). Also, concerning the organization, there is a significant variation in the distribution of age groups ( χ 2 33.036; P value .001). It was mainly observed that in Government and private hospital participants were more likely falling in 25‐ to 50‐year group that is below 25 years were lesser than expected, whereas educational institute participants were more likely to be falling in below 25 years than expected as compared to the 25‐ to 50‐year group where the ratio of expected is higher than the observed.
The outcome of this questionnaire suggests that Pakistan faces a unique challenge related to public health, which majorly is the people's response towards COVID‐19 outbreak. Lack of infection prevention and control policies at organizations and hospitals have been observed under the recent challenge. Informative campaigns should be organized through social and digital media to make the citizens aware of this highly contagious infection. In all these cases, staff training, and strict implementation of rules and regulations, effective development of policies and specific guidelines relating to virus spread are required, and all organizations and hospitals need to ensure the proper implementation of the government policies.
To make the HCWs well prepared in Pakistan to find this COVID‐19 pandemic, a series of proper trainings are required. Public awareness programs shall be introduced to make the general public aware of their personal and restrict the community transmission of this virus. Data obtained highlighted the need to initiate capacity building activities towards COVID‐19 as an obligatory step to establish an effective surveillance system in Pakistan.
4. CONCLUSION
To avert the threat of an epidemic, it is significant that public knowledge, attitude, and behavior towards COVID‐19 response is prompt. However, the results of our study reveal that the masses of Pakistan are not aware of the gravity of the situation. Moreover, front‐line workers are not prepared to face the challenge. It is a matter of urgency that awareness at all levels is promoted.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
AUTHOR CONTRIBUTIONS
SK and MZ designed the study and compiled the manuscript, MK and KM performed the statistical analysis, NH compiled the statistical results, TH carried out the final formatting and manuscript proofread. All authors have read the manuscript and agree to the submission.
Khan S, Khan M, Maqsood K, Hussain T, Noor‐ul‐Huda, Zeeshan M. Is Pakistan prepared for the COVID‐19 epidemic? A questionnaire‐based survey. J Med Virol. 2020;92:824–832. 10.1002/jmv.25814
REFERENCES
- 1. Deng S‐Q, Peng H‐J. Characteristics of and public health responses to the Coronavirus disease 2019 outbreak in China. J Clin Med. 2020;9(2):575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Zu ZY, Jiang MD, Xu PP, et al. Coronavirus disease 2019 (COVID‐19): a perspective from China. Radiology. 2020:200490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Millán‐Oñate J, Rodriguez‐Morales AJ, Camacho‐Moreno G, Mendoza‐Ramírez H, Rodríguez‐Sabogal IA, Álvarez‐Moreno C. A new emerging zoonotic virus of concern: the 2019 novel Coronavirus (COVID‐19). Infectio. 2020;24:3. [Google Scholar]
- 4. Phelan AL, Katz R, Gostin LO. The novel coronavirus originating in Wuhan, China: challenges for global health governance. JAMA. 2020;323(8):709‐710. [DOI] [PubMed] [Google Scholar]
- 5. Anzai A, Kobayashi T, Linton NM, et al. Assessing the impact of reduced travel on exportation dynamics of novel coronavirus infection (COVID‐19). J Clin Med. 2020;9(2):601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Rocklöv J, Sjödin H, Wilder‐Smith A. COVID‐19 outbreak on the Diamond Princess cruise ship: estimating the epidemic potential and effectiveness of public health countermeasures. J Travel Med. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Dagia N. Pakistan Facing Major Covid‐19 Challenge. WHO; 2020. [Google Scholar]
- 8. 52 new coronavirus cases push Pakistan's tally to 237.
- 9. Xinhua . Number of COVID‐19 Cases in Pakistan surpasses 100; 2020.
- 10. Ministry of Health P . National Action Plan for Corona virus disease (COVID‐19) Pakistan; 2020.
- 11. Storr J, Twyman A, Zingg W, et al. Core components for effective infection prevention and control programmes: new WHO evidence‐based recommendations. Antimicrobial Resistance & Infection Control. 2017;6(1):6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Park Y‐S, Lee C, Kim KM, et al. The first case of the 2015 Korean Middle East respiratory syndrome outbreak. Epidemiol Health. 2015;37. [DOI] [PMC free article] [PubMed] [Google Scholar]