

Abstract
Active surveillance for zoonotic respiratory viruses is essential to inform the development of appropriate interventions and outbreak responses. Here we target individuals with a high frequency of animal exposure in Vietnam. Three‐year community‐based surveillance was conducted in Vietnam during 2013‐2016. We enrolled a total of 581 individuals (animal‐raising farmers, slaughterers, animal‐health workers, and rat traders), and utilized reverse transcription‐polymerase chain reaction to detect 15 common respiratory viruses in pooled nasal‐throat swabs collected at baseline or acute respiratory disease episodes. A respiratory virus was detected in 7.9% (58 of 732) of baseline samples, and 17.7% (136 of 770) of disease episode samples (P < .001), with enteroviruses (EVs), rhinoviruses and influenza A virus being the predominant viruses detected. There were temporal and spatial fluctuations in the frequencies of the detected viruses over the study period, for example, EVs and influenza A viruses were more often detected during rainy seasons. We reported the detection of common respiratory viruses in individuals with a high frequency of animal exposure in Vietnam, an emerging infectious disease hotspot. The results show the value of baseline/control sampling in delineating the causative relationships and have revealed important insights into the ecological aspects of EVs, rhinoviruses and influenza A and their contributions to the burden posed by respiratory infections in Vietnam.
Keywords: asymptomatic, cohort study, viral etiology, respiratory disease, Vietnam, zoonoses
Highlights
We reported the detection of common respiratory viruses in individuals with a high frequency of animal exposure in Vietnam, an emerging infectious disease hotspot. The results show the value of baseline/control sampling in delineating the causative relationships and have revealed important insights into the ecological aspects of EVs, rhinoviruses and influenza A and their contributions to the burden posed by respiratory infections in Vietnam.
1. INTRODUCTION
Annually, acute respiratory tract infections are responsible for more than 3 million deaths worldwide.1 In Vietnam, a developing country in Southeast Asia, mortality attributed to acute respiratory infections accounted for half of that attributed to the other infectious diseases combined in 2016.1
Viruses are regarded as the most common causes of acute respiratory diseases, and some emerging respiratory diseases as the Middle East respiratory syndrome (MERS) and severe acute respiratory syndrome (SARS), both related to coronaviruses (CoVs), are listed in the WHO's List of Blueprint priority diseases2 because of their pandemic potential. While the reported patterns of the etiological agents vary between geographic locations and age groups, generally, respiratory syncytial virus (RSV)‐A, RSVB, influenza A virus, influenza B virus, adenovirus (ADV), enterovirus (EVs); human metapneumovirus (MPV), human rhinovirus (HRV), parainfluenza virus (PIV)1‐4, human CoV (including subtypes OC43 and NL63), human bocavirus (BoV) and parechovirus (PEV) are the most common viruses detected in respiratory samples worldwide.3, 4, 5, 6, 7, 8, 9 Of these, influenza A virus, influenza B virus, and CoV have been reported as the most common viruses detected in people over 5 years old,10, 11, 12, 13 while RSV and PIVs have been regarded as the leading causes of respiratory infections in children under 5 years old in South East Asia.3, 14, 15
Zoonotic infections are of global concern, and approximately 60% of known infectious diseases in humans are of zoonotic origin.16 In addition, Southeast Asia, including Vietnam, is one of the hotspots of emerging infectious diseases. Indeed, many of the recent respiratory outbreaks are linked with zoonotic viruses as SARS‐CoV,17 avian influenza A virus H5N1,18 pandemic influenza A virus subtype H1N1,19 and more recently MERS‐CoV,20 with the majority being first reported in Asia. Collectively, active surveillance for (novel) zoonotic viruses in this vulnerable part of the world is of both medical and public health significance. As such, for the detection of novel zoonotic viruses in humans and animals, during 2012‐2015 the Vietnam Initiative on Zoonotic InfectiONS (VIZIONS) project, consisting of the various hospital‐ and community‐based studies, was conducted across Vietnam.21, 22 Herein, we focus our analysis on a community‐based study, which was designed to capture the cross‐species transmission events of zoonotic viruses among individuals with a high risk of zoonotic infections in southern and highland Vietnam. In this study, our aim was to describe the frequency of common respiratory viruses in clinical samples collected from these individuals, later called cohort members, at baseline and when a respiratory disease episode was reported during the study period.
2. METHODS
2.1. Study design and inclusion criteria
This study was a part of the High‐Risk Sentinel Cohort (HRSC) study which was a community‐based component of the VIZIONS project.21 The HRSC study was first commenced in June 2013 in Dong Thap and then in February 2014 in Dak Lak. These are provinces located in southern and highland of Vietnam, respectively, representing two different geographic areas in Vietnam.
Animal‐raising farmers, animal health workers, and slaughterers were eligible to be enrolled in the study since these are common occupations in rural Vietnam with frequent occupational exposure to animals. Rat traders in Dong Thap were additionally recruited due to the commonality of this occupation in this locality. The animal‐raising farmers accounted for about two‐third of the population with occupational exposure to animals in these study provinces.
On the basis of the animal farm census, letters were sent out to invite potential participants to attend an introductory meeting. The consent forms were then obtained from those who were willing to join the HRSC study. For each farmer household, up to four members having the highest frequency of working with animals were recruited. The slaughterers were recruited from all local central abattoirs or slaughter points. The animal‐health workers and rat traders were selected by convenience. Consequently, a total of 581 individuals (median age in year, 38; range, 2‐89), including 415 (71.4%) animal‐raising farmers, 100 (11.7%) slaughterers, 61 (10.5%) animal‐health workers, and 5 (1.8%) rat‐traders, were recruited. Each cohort members were followed up annually for up 3 years since recruitment.
2.2. Data collection
Annually, to establish the baseline data (ie, no disease episode reported), the cohort members were interviewed, and clinical specimens, including rectal, pooled nasal, and throat swabs and blood were also collected from each interviewee. These baseline data were collected from all cohort members, except for the farmers, for which only one person mostly working with animals per household was interviewed and sampled.
During the study period, whenever getting illness (diarrhea and respiratory infection) defined as any signs/symptoms of respiratory tract infections (eg, sneezing, coughing or sore throat), plus fever (≥38°C), the cohort members informed the local study teams. Within 48 hours, the site study doctors made a visit to the participant houses and collected information about animal exposures, associated symptoms, and medication. In addition, clinical specimens, including blood, and (when relevant) rectal‐ or pooled nasal and throat swabs were collected. All the specimens were stored at −80°C until analysis. Here, we focused on respiratory episodes. As such, only pooled nasal‐throat swabs of each individual were analyzed.
2.3. Respiratory virus detections by real‐time polymerase chain reaction analysis
To detect common respiratory viruses in pooled nasal and throat swabs, we first isolated total nucleic acid (NA) from patient samples using MagNA Pure 96 platform (Roche Diagnostics, Mannheim, Germany), following the manufacturer's instructions. The NA output was then eluted in 50 µL of elution buffer and immediately screened for respiratory viruses using multiplex real‐time polymerase chain reaction (RT‐PCR) assays.
The RT‐PCR assays used in the present study were derived from previous publications,23, 24, 25, 26 which captured 15 common respiratory viruses and a wide range of their subtypes, including RSVA, RSVB; influenza A virus, influenza B virus, ADV; EVs; MPV; HRV; PIV‐1, PIV‐2, PIV‐3, PIV4; CoV subtype OC43 and NL63; BoV and PEV.23, 24, 25 Influenza A virus‐positive samples were further tested for (zoonotic) subtypes, including H3, H1N1pdm09, H1, and avian/H5 25, 26 (primer and probe sequences are listed in Table S2). All the RT‐PCR reactions were carried in a LightCycler 480 Instrument II (96‐wells) (Roche Molecular Systems, Inc).
2.4. Data analysis
The data were analyzed by STATA software, version 12.0.27 The pairwise comparisons of categorical variables were calculated by Pearson's χ 2 test (or Fisher exact test when the sample size was less than five in any of the cells of a contingency table) or two‐sample t test with equal variances. The errors of multiple comparisons were corrected by the Bonferroni method.28 P ≤ .05 was considered the significance. EpiTools29 were used to calculate 95% confidence intervals for the odds ratio. The rat traders (n = 5) were excluded from these tests because of an insufficient sample size.
2.5. Ethics
The HRSC study was approved by the Oxford Tropical Research Ethics Committee (OxTREC) in the United Kingdom, and by the Ethics Committees of Dong Thap Hospital, Dak Lak Hospital, the sub‐Departments of Animal Health in Dong Thap and Dak Lak, and the Hospital of Tropical Diseases in Ho Chi Minh City in Vietnam. Written informed consent was obtained from each study participant.
3. RESULTS
3.1. Collection of respiratory swabs and reports of disease episodes
The detailed characteristics of the cohort members are briefly summarized in Table 1. Approximately half (51.1%; 297 of 581) of the study population was annually interviewed during 2013‐2015, corresponding to a total of 829 interviews conducted (291, 273, and 265 interviews in 2013, 2014, and 2015, respectively) (Table 1). Consequently, 732 pooled nasal‐throat swabs were collected at these annual interviews for respiratory virus detection. Herein, these samples were considered as baseline samples.
Table 1.
Baseline characteristics
| All | Dak Lak | Dong Thap | P value a | |
|---|---|---|---|---|
| Occupation | N = 581 | N = 299 | N = 282 | .012 |
| Farmers, n (%) | 415 (71) | 201 (67) | 214 (76) | .021 |
| Animal‐health workers, n (%) | 61 (10) | 31 (10) | 30 (11) | .915 |
| Slaughterers, n (%) | 100 (17) | 67 (22) | 33 (12) | .001 |
| Rat traders, n (%) | 5 (1) | 0 | 5 (2) | |
| Median age (range), y | 38 (2‐89) | 39 (2‐89) | 38 (4‐76) | .995 b |
| Age groups | ||||
| ≤15, n (%) | 59 (10) | 24 (8) | 35 (12) | .080 |
| ≥16, n (%) | 522 (90) | 275 (92) | 247 (88) | |
| Sex ratio (male/female) | 1.2 (322/259) | 1.1 (157/142) | 1.4 (165/117) | .146 |
| No. of cohort members interviewed annually for baseline c | N = 297 | N = 162 | N = 135 | |
| 1st year, n (%) | 291 (98) | 162 (100) | 129 (96) | .042 |
| 2nd year, n (%) | 273 (92) | 150 (93) | 123 (91) | .114 |
| 3rd year, n (%) | 265 (89) | 147 (91) | 118 (87) | .077 |
| No. of cohort members reporting respiratory illness | N = 386 | N = 219 | N = 167 | |
| 1st year, n (%) | 227 (59) | 154 (70) | 73 (44) | <.001 |
| 2nd year, n (%) | 193 (50) | 109 (50) | 84 (50) | .088 |
| 3rd year, n (%) | 151 (39) | 67 (31) | 84 (50) | .043 |
| No. of reported respiratory episodes d | N = 812 | N = 394 | N = 418 | |
| 1st year, n (%) | 317 (39) | 183 (46) | 134 (32) | .017 |
| 2nd year, n (%) | 317 (39) | 129 (33) | 188 (45) | .001 |
| 3rd year, n (%) | 178 (22) | 82 (21) | 96 (23) | .758 |
P value (Pearson's χ 2 or Fisher exact test) of the difference between Dak Lak and Dong Thap.
t Test.
At these follow‐up time points, a respiratory sample was collected from each individual.
A total of 770 samples were collected and included in polymerase chain reaction analysis, with 314, 281, and 175 samples in first, second, and third years, respectively.
Over the 3‐year period, 66.4% (386 of 581) of the cohort members reported having respiratory infections, corresponding to a total of 812 respiratory episodes (Table 1), or an average of 2.1 episodes per reporting individual, and 1.4 (812/581) episodes per individual among all cohort members. The slaughterers (225/100) were more likely to have respiratory diseases than the animal‐health workers (92/61) and the farmers (491/415) (P < .003). In total, of the 812 reported respiratory episodes, 770 pooled nasal‐throat swabs were collected for respiratory virus detection.
3.2. Frequency of respiratory viruses detected at baseline and the disease episodes
Evidence of a respiratory virus by RT‐PCR analysis was documented in 7.9% (58 of 732) of samples collected at the baseline, and 17.7% (136 of 770) of samples collected when a respiratory disease episode was reported (P < .001) (Table 2). In addition, mixed infections were recorded in 2 (0.3%) and 7 (0.9%) samples collected at baseline and disease episodes, respectively (Table 2).
Table 2.
Number (percentage) of cohort members with detected viruses from tested pooled nasal and throat swabs
| Whole study | 1st year | 2nd year | 3rd year | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline (N = 732) | Disease episode (N = 770) | P value | OR (95% CI) | Baseline (N = 290) | Disease episode (N = 314) | P value | OR (95% CI) | Baseline (N = 240) | Disease episode (N = 281) | P value | OR (95% CI) | Baseline (N = 202) | Disease episode (N = 175) | P value | OR (95% CI) | |
| EVs | 29 (4.0) | 67 (8.7) | <.001 | 2.3 (1.5‐3.6) | 2 (0.7) | 12 (3.8) | .013 | 5.7 (1.3‐26) | 10 (4.2) | 40 (14.2) | <.001 | 3.8 (1.8‐7.8) | 17 (8.4) | 15 (8.6) | .96 | 1 (0.5‐2.1) |
| HRV | 5 (0.7) | 32 (4.2) | <.001 | 6.3 (2.4‐16) | 2 (0.7) | 21 (6.7) | <.001 | 10.3 (2.4‐44) | 1 (0.4) | 9 (3.2) | .024 | 7.9 (1‐63) | 2 (1.0) | 2 (1.1) | 1 | 1.2 (0.2‐8.3) |
| Influenza A virus | 14 (1.9) | 18 (2.3) | .568 | 1.2 (0.6‐2.5) | 4 (1.4) | 4 (1.3) | 1 | 1 (0.2‐3.7) | 6 (2.5) | 11 (3.9) | .365 | 1.6 (0.6‐4.4) | 4 (2.0) | 3 (1.7) | 1 | 0.8 (0.2‐3.9) |
| H3 | 3 (21.4) | 12 (66.7) | .016 | 7.3 (1.5‐36) | 0 | 1 (0.3) | 1 | NA | 0 | 10 (3.6) | .002 | NA | 3 (1.5) | 1 (0.6) | .63 | 0.4 (0‐3.7) |
| H1‐seasonal | 0 | 0 | NA | NA | 0 | 0 | NA | NA | 0 | 0 | NA | NA | 0 | 0 | NA | NA |
| H1‐pan09 | 0 | 0 | NA | NA | 0 | 0 | NA | NA | 0 | 0 | NA | NA | 0 | 0 | NA | NA |
| H5 | 0 | 0 | NA | NA | 0 | 0 | NA | NA | 0 | 0 | NA | NA | 0 | 0 | NA | NA |
| ADV | 1 (0.1) | 9 (1.2) | .021 | 8.6 (1.1‐68) | 1 (0.3) | 4 (1.3) | .375 | 3.7 (0.4‐33) | 0 | 2 (0.7) | .502 | 4.3 (0.2‐90) | 0 | 3 (1.7) | .1 | 8.2 (0.4‐160) |
| CoV a | 8 (1.1) | 7 (0.9) | .72 | 0.8 (0.3‐2.3) | 1 (0.3) | 4 (1.3) | .375 | 3.7 (0.4‐33) | 6 (2.5) | 3 (1.1) | .314 | 3.2 (1.3‐8) | 1 (0.5) | 0 | 1 | NA |
| RSVA | 0 | 3 (0.4) | .25 | NA | 0 | 3 (1.0) | .250 | NA | 0 | 0 | NA | NA | 0 | 0 | NA | NA |
| MPV | 0 | 2 (0.3) | .5 | NA | 0 | 1 (0.3) | 1 | NA | 0 | 1 (0.4) | 1 | NA | 0 | 0 | NA | NA |
| RSVB | 1 (0.1) | 2 (0.3) | 1 | 1.9 (0.2‐21) | 1 (0.3) | 0 | 1 | 0.3 (0‐7.5) | 0 | 2 (0.7) | .502 | NA | 0 | 0 | NA | NA |
| Influenza B virus | 0 | 2 (0.3) | 0.5 | NA | 0 | 0 | NA | NA | 0 | 0 | NA | NA | 0 | 2 (1.1) | .22 | NA |
| PIV4 | 0 | 1 (0.1) | 1 | NA | 0 | 0 | NA | NA | 0 | 1 (0.4) | 1 | NA | 0 | 0 | NA | NA |
| BoV | 2 (0.3) | 1 (0.1) | .615 | 0.5 (0‐5.3) | 1 (0.3) | 0 | .48 | NA | 0 | 1 (0.4) | 1 | NA | 1 (0.5) | 0 | 1 | NA |
| (+) ≥1 virus | 58 (7.9) | 136 (17.7) | <.001 | 2.5 (1.8‐3.5) | 12 (4.1) | 45 (14.3) | <.001 | 3.9 (2‐7.5) | 22 (9.2) | 67 (23.8) | <.001 | 3.1 (1.8‐5.2) | 24 (12) | 24 (13.7) | .64 | 1.2 (0.6‐2.1) |
| (+) ≥2 viruses b | 2 (0.3) | 7 (0.9) | .18 | 3.3 (0.7‐16) | 0 | 2 (0.6) | .5 | 4.6 (0.2‐97) | 1 (0.4) | 4 (1.4) | .38 | 3.4 (0.4‐31) | 1 (0.5) | 1 (0.6) | 1 | 1.2 (0‐18.6) |
Note: The OR was the disease episodes vs baseline. P values were calculated by Pearson's χ 2 or Fisher exact test.
Abbreviations: ADV, adenovirus; BoV, bocavirus; CI, confidence interval; CoV, coronavirus; EV, enterovirus; HRV, human rhinovirus; OR, odds ratio; PEV, parechovirus; PIV, parainfluenza virus; RSV, respiratory syncytial virus.
Subtype OC43 and NL63.
Including one EVs‐BoV and one influenza A virus‐CoV in the baseline, and one AdV‐influenza B virus, one BoV‐influenza A virus, two EVs‐influenza A virus, one EVs‐RSVB, one EVs‐HRV and one EVs‐AdV‐CoV in the disease episodes PIV‐1, ‐2, ‐3, and PEV were not detected in all samples.
Of the detected viruses, EVs, HRV and influenza A virus were the most common viruses detected in samples collected at both baseline and disease episodes, followed by ADV and CoV (Table 2). There were significant differences in the frequencies of EVs, HRV and ADV detected in the two groups; 29 of 732 (4%) at baseline vs 67 of 770 (8.7%) at disease episodes (P < .001) for EVs, 5 of 732 (0.7%) vs 32 of 770 (4.2% (P < .001) for HRV, and 1 of 732 (0.1%) vs 9 of 770 (1.2%; (P = .021) for ADV (Table 2). In addition, of the influenza A virus RT‐PCR positive cases, subtype H3 was detected at a higher frequency at disease episodes than at baseline, 66.7% (12 of 15) vs 21.4% (3 of 14), P = .016. Remaining influenza A virus‐positive cases were RT‐PCR negative for specific RT‐PCR for the other tested subtypes (H1N1pdm09, H1N1, and H5) (Table 2).
3.3. Clinical signs/symptoms of cohort members in acute respiratory diseases with the detected viruses
For the altogether 770 reported respiratory episodes, cough and sneezing were the most common symptoms recorded, present in 76% (585 of 770) and 74.7% (575 of 770) of cases, respectively, followed by sore throat (65.3%; 503 of 770), headache (51.4%; 396 of 770), body aches (41.8%; 322 of 770), and dyspnea (7.4%; 57 of 770) (Table 3). In addition, gastrointestinal symptoms were recorded in 7.3% (56 of 770), but watery diarrhea was more often recorded in cohort members without a virus detected than in those with a positive finding, 52 of 634 (8.2%) vs 4 of 136 (2.9%), P = .029 (Table 3).
Table 3.
Number (and percentage) for demographics and clinical characteristics of cohort members reporting respiratory episodes
| Tested samples (N = 770) | Positive samples (N = 136) | Negative samples (N = 634) | P value | OR (95% CI) | EVs (N = 67) | HRV (N = 32) | Influenza A virus (N = 18) | ADV (N = 9) | CoV a (N = 7) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Age ≤ 15 | 60 (7.8) | 15 (11) | 45 (7.1) | .121 | 1.6 (0.9‐3) | 8 (11.9) | 3 (9.4) | 2 (11.1) | 2 (22.2) | 2 (28.6) |
| Fever | 770 (100) | 136 (100) | 634 (100) | NA | NA | 67 (100) | 32 (100) | 18 (100) | 9 (100) | 7 (100) |
| Cough | 585 (76.0) | 102 (75.0) | 483 (76.2) | .770 | 0.9 (0.6‐1.4) | 49 (73) | 23 (72) | 15 (83) | 8 (89) | 6 (86) |
| Sneezing | 575 (74.7) | 105 (77.2) | 470 (74.1) | .455 | 1.2 (0.8‐1.8) | 50 (75) | 25 (78) | 15 (83) | 6 (67) | 7 (100) |
| Sore throat | 503 (65.3) | 90 (66.2) | 413 (65.1) | .818 | 1.1 (0.7‐1.6) | 46 (69) | 16 (50) | 15 (83) | 4 (44) | 5 (71) |
| Dyspnea | 57 (7.4) | 8 (5.9) | 49 (7.7) | .456 | 0.8 (0.3‐1.6) | 4 (6) | 2 (6) | 0 | 0 | 0 |
| Headache | 396 (51.4) | 70 (51.5) | 326 (51.4) | .991 | 1 (0.7‐1.5) | 30 (45) | 20 (63) | 11 (61) | 3 (33) | 3 (43) |
| Body aches | 322 (41.8) | 48 (35.2) | 274 (43.2) | .089 | 0.7 (0.5‐1.1) | 21 (31) | 11 (34) | 9 (33) | 0 | 2 (29) |
| Watery diarrhea | 56 (7.3) | 4 (2.9) | 52 (8.2) | .029 | 0.3 (0.1‐1) | 2 (3) | 2 (6) | 0 | 0 | 0 |
| Nausea | 55 (7.1) | 8 (5.9) | 47 (7.4) | .529 | 0.8 (0.4‐1.7) | 3 (4) | 1 (3) | 2 (11) | 1 (11) | 1 (14) |
| Antibiotic use b , c | 199 (25.8) | 37 (27.2) | 162 (25.6) | .689 | 1.1 (0.7‐1.7) | 18 (26.9) | 5 (15.6) | 4 (22.2) | 1 (11.1) | 2 (28.6) |
Note: Four patients have no data on gender and age. P values were calculated by Pearson's χ 2 or Fisher exact test. The difference in each viral infection inducing each clinical symptom was not significant (P > .05). The OR was the disease “positive samples” vs “negative samples”.
Abbreviations: ADV, adenovirus; CI, confidence interval; CoV, coronavirus; EV, enterovirus; HRV, human rhinovirus; OR, odds ratio.
Subtype OC43 and NL63.
The antibiotic use of the patients from the first symptoms to the incidence interview/sampling.
Antibiotic types used Cephalosporin, Amoxicillin, Clarithromycin, Ampicillin, Augmentin, Azithromycin, Chloramphenicol, Ciprofloxacin, Erythromycin, Ofloxacin, Spiramycin.
Of the virus‐positive cases, watery diarrhea was only recorded in those positive for EVs and HRV, whilst sore throat was predominantly recorded in those positive for influenza A virus. Otherwise, there were considerable similarities in age and clinical presentations of cohort‐member groups who were positive for different viruses (Table 3).
3.4. The frequency of respiratory viruses detected by provinces
To assess the differences in the frequencies of respiratory viruses under investigation between Dong Thap and Dak Lak, which represent the two distinct geographic localities in Vietnam, we stratified the data for these two individual provinces (Table 4). Subsequently, EVs, HRV and influenza A virus remained the leading viruses detected in the tested samples from these provinces, while the detection rates of EVs and HRV in disease episode samples collected in Dong Thap were significantly higher than that in Dak Lak (11.1% [42 of 379] vs 6.4% [25 of 391]; P = .021, and 6.1% [23 of 379] vs 2.3% [9 of 391], P = .009, respectively). In Dong Thap, EVs and HRV were significantly more often detected in samples collected at disease episode than at baseline; P < .001 for both EVs and HRV. In Dak Lak, no significant differences were found (Table 4).
Table 4.
Number (percentage) of cohort members with different detected viruses at baseline and disease episodes in Dak Lak and Dong Thap
| Dak Lak | Dong Thap | Baseline (Dak Lak vs Dong Thap) | Disease episodes (Dak Lak vs Dong Thap) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline (N = 434) | Disease episode (N = 391) | P value | OR (95% CI) a | Baseline (N = 298) | Disease episode (N = 379) | P value | OR (95% CI) a | P value | OR (95% CI) b | P value | OR (95% CI) b | |
| EVs | 18 (4.1) | 25 (6.4) | .147 | 1.6 (0.9‐2.9) | 11 (3.7) | 42 (11.1) | <.001 | 3.3 (1.6‐6.4) | 0.756 | 1.1 (0.5‐2.4) | .021 | 0.6 (0.3‐0.9) |
| HRV | 4 (0.9) | 9 (2.3) | .112 | 2.5 (0.8‐8.3) | 1 (0.3) | 23 (6.1) | <.001 | 19 (2.6‐143) | 0.653 | 2.8 (0.3‐25) | .009 | 0.4 (0.2‐0.8) |
| Influenza A virus | 6 (1.4) | 9 (2.3) | .324 | 1.7 (0.6‐4.8) | 8 (2.7) | 9 (2.4) | .798 | 0.9 (0.3‐2.3) | 0.206 | 0.5 (0.2‐1.5) | .947 | 1 (0.4‐2.5) |
| H3 | 0 | 4 (44.4) | .103 | NA | 3 (37.5) | 8 (88.9) | .050 | 13.3 (1.1‐166) | 0.067 | 0.1 (0‐1.9) | .256 | 0.5 (0.1‐1.6) |
| H1‐seasonal | 0 | 0 | NA | NA | 0 | 0 | NA | NA | NA | NA | NA | NA |
| H1‐pan09 | 0 | 0 | NA | NA | 0 | 0 | NA | NA | NA | NA | NA | NA |
| H5 | 0 | 0 | NA | NA | 0 | 0 | NA | NA | NA | NA | NA | NA |
| ADV | 1 (0.2) | 5 (1.3) | .107 | 5.6 (0.7‐48) | 0 | 4 (1.1) | .135 | NA | 1 | 2.1 (0.1‐50) | 1 | 1.2 (0.3‐4.6) |
| CoV c | 4 (0.9) | 3 (0.8) | 1 | 0.8 (0.2‐3.7) | 4 (1.3) | 4 (1.1) | .736 | 0.8 (0.2‐3.2) | 0.722 | 0.7 (0.2‐2.8) | .721 | 0.7 (0.2‐3.3) |
| RSVA | 0 | 0 | NA | NA | 0 | 3 (0.8) | .26 | NA | NA | NA | .119 | 0.1 (0‐2.7) |
| MPV | 0 | 0 | NA | NA | 0 | 2 (0.5) | .506 | NA | NA | NA | .242 | 0.2 (0‐4) |
| RSVB | 1 (0.2) | 0 | 1 | NA | 0 | 2 (0.5) | .506 | NA | 1 | 2.1 (0.1‐50) | .242 | 0.2 (0‐4) |
| Influenza B virus | 0 | 0 | NA | NA | 0 | 2 (0.5) | .506 | NA | NA | NA | .242 | 0.2 (0‐4) |
| PIV4 | 0 | 0 | NA | NA | 0 | 1 (0.3) | 1 | NA | NA | NA | .492 | 0.3 (0‐8) |
| BoV | 1 (0.2) | 0 | 1 | NA | 1 (0.3) | 1 (0.3) | 1 | 0.8 (0.1‐12) | 1 | 0.7 (0‐11) | .492 | 0.3 (0‐8) |
| (+) ≥1 virus | 33 (7.6) | 48 (12.3) | .024 | 1.7 (1.1‐2.7) | 25 (8.4) | 88 (23.2) | <.001 | 3.3 (2.1‐5.3) | 0.699 | 0.9 (0.5‐1.5) | <.001 | 0.5 (0.3‐0.7) |
| (+) ≥2 viruses d | 2 (0.5) | 2 (0.5) | .917 | 1.1 (0.2‐7.9) | 0 | 5 (1.3) | .071 | NA | 0.517 | 3.4 (0.2‐72) | .28 | 0.4 (0.1‐2) |
Note: Other viral pathogens were not showed as they were detected in less than 10 samples. P values were calculated by Pearson's χ 2 or Fisher exact test
Abbreviations: ADV, adenovirus; CI, confidence interval; CoV, coronavirus; EV, enterovirus; HRV, human rhinovirus; OR, odds ratio.
The OR was the disease episodes vs. baseline.
The OR was Dak Lak and Dong Thap.
Subtype OC43 and NL63.
Including one EVs‐BoV and one influenza A virus‐CoV in the baseline, and one AdV‐influenza B virus, one BoV‐influenza A virus, two EVs‐influenza A virus, one EVs‐RSVB, one EVs‐HRV, and one EVs‐AdV‐CoV in the disease episodes.
3.5. Temporal and seasonal differences in the frequency of detection of respiratory viruses
There were some fluctuations in the detection of the most common viruses (especially EVs and HRV; Table 2) over the study period. Of particular note was the significant increase in the frequency of EVs from baseline to disease episodes in the first 2 years (from 0.7% at baseline to 3.8% at disease episodes in the first year, and from 4.2% to 14.2% in the second year, respectively) (Table 2). In year 3, the detection of EVs remained high but was comparable in samples collected at baseline (8.4%, 17 of 202) and disease episodes (8.6%, 15 of 175) (Table 2). In contrast to EVs, there was a downward trend of HRV detection over time, while the frequency of influenza A virus was relatively stable over the 3‐year period (Table 2).
In terms of seasonality, overall, there were some clear trends in the seasonality of the most common viruses (especially EVs and influenza A virus, Figure 1). More specifically, EVs and influenza A virus were significantly more often found in rainy season (May‐October) than in dry season (November‐April); the detection rates were 12.2% (43 of 353) vs 5.8% (24 of 417) (P = .002) for EVs, and 3.7% (13 of 353) vs 1.2% (5 of 417), P = .023 for influenza A virus, respectively. In contrast to EVs and influenza A virus, ADV was more often found in the dry season than in the rainy season (1.9%, 8 of 417 vs 0.3%, 1 of 353, P = .044) (Figure 1).
Figure 1.
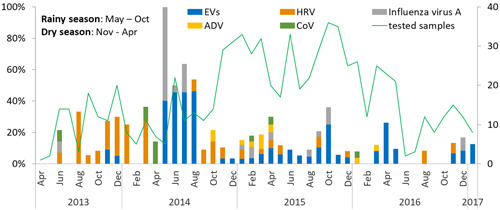
The seasonal distribution of symptomatic EVs‐, HRV‐, influenza A virus‐, ADV‐, and CoV (subtype OC43 and NL63)‐infected cases detected by RT‐PCR assay. The bars show the proportion of the viruses detected among total samples tested (the line chart) each month. EVs and influenza A virus were more likely detected in the rainy season than in the dry season (P = .002 and P = .023, respectively), while the ADV detections were more frequent in the dry season as compared with the rainy one (P = .044). There was no significant difference in the detections of HRV and CoV (subtype OC43 and NL63) between dry and rainy seasons (P = .333 and .227, respectively). ADV, adenovirus; CoV, coronavirus; EV, enterovirus; HRV, human rhinovirus; RT‐PCR, real‐time polymerase chain reaction
3.6. Animal exposure
Overall, the cohort members were exposed to a wide range of animals, including 11 types of exotic animals and 11 types of domestic animals, within ≤1 month prior to the disease episode (n = 770) (Table S1). There was no difference in the patterns of animal exposure among cohort members who were positive for the predominant viruses (EVs, HRV, and influenza A virus). The numbers of the remaining viruses were insufficient to informatively assess their associations with age, seasonality, clinical presentation, and animal exposure.
4. DISCUSSION
Here we describe the frequency of common human viruses causing acute respiratory infections in people with high exposure to animals in Dong Thap (Southern) and Dak Lak (Highland) provinces. We showed that EVs, HRV and influenza A virus were the predominant viruses detected in respiratory samples of the cohort members in both localities and that their detection rates were significantly higher in respiratory samples collected at respiratory disease episodes than in those collected at baseline. In addition, the results have also revealed important insights into the ecological characteristics of these predominant viruses. More specifically, our analysis shows that EVs and influenza A virus were more often found in the rainy season (from May to October), and there were fluctuations in the detection of EVs and HRV over time, while influenza A virus activity was relatively stable over the study period, suggesting that these viruses may have interacted with the immune landscape of the study population.
Although viral detection in upper respiratory samples like pooled nasal and throat swabs may merely reflect the carriage of such viruses in these body cavities, a higher detection frequency in samples collected at disease episodes than at baseline suggests an association between the detected viruses and the reported respiratory episodes. As such, the high frequency of EVs and HRV detected in samples collected at disease episodes in the present study further expand our knowledge about the clinical burden posed by viruses of the genus Enterovirus in Vietnam. Indeed, an outbreak of enterovirus associated diseases like hand foot and mouth disease (HFMD) have been frequently reported in Vietnam and Asia since 1997.30, 31 Likewise, enteroviruses have been reported to be one of the leading causes of central nervous system infections and respiratory illness in Vietnam.5, 32, 33 In addition, in line with the observed cyclical epidemic patterns of HFMD in Vietnam and Asia,30, 31 for which the underlying mechanism remains unknown, the fluctuations in the detection EVs and HRV over the study period and between Dong Thap and Dak Lak suggest an interplay between the pathogens and the proportion of susceptible individuals in respective provinces.
The higher detection of influenza A virus subtype H3 in samples collected at the disease episodes than in those collected at baseline points to the association between subtype H3 with respiratory illness in Vietnam. In contrast to the prevalence of influenza A virus subtype H3, the result showing an overall comparable prevalence of influenza A virus in both sample groups suggests that there is a high level of asymptomatic infection of influenza A virus in the general population, in agreement with previous reports.34, 35 The difference in sensitivities between RT‐PCR assays used may explain our failure to identify the specific influenza A virus subtypes in the remaining pan‐influenza A virus RT‐PCR positive samples.
The low prevalence or absence of respiratory viruses like PIVs, PEV, RSVA, and RSVB in the present study may be attributed to the age structure of the present cohort. Indeed, while, these viral species are well‐established agents of (respiratory) infections in children, and to some extent in elderly people (eg, in case of PIVs),3, 10, 14, 15, 36, 37, 38 over 92% of the respiratory disease episodes reported in this study were among cohort members aging ≥16 years. In terms of seasonal distribution of the predominant viruses as EVs, influenza A virus, HRV and ADV, our report supports previous findings.39, 40, 41, 42, 43
Our overall RT‐PCR yield of 17.7% of viral agents in respiratory samples of the cohort members with the majority age from 16 years or above is in agreement with the diagnostic yields of previous studies.44, 45, 46, 47, 48, 49 The results suggest that it is probably because adults have acquired substantial immunity during their life, leading to the rapid clearance of the infecting viruses from their respiratory tract, thereby shortening the duration of viral shedding.
Our study has some limitations. First, no human subjects without animal exposure were recruited as controls. Therefore, we were unable to assess the effect (if any) of animal exposure on the frequency of the respiratory disease incidence, as well as the observed viral patterns. Second, despite a holistic effort, nonviral agents as bacterial pathogens were not tested. Third, a slight decrease in sensitivity of the multiplex RT‐PCR platforms used in the present study as compared with that of the corresponding monoplex RT‐PCRs have previously been reported,23 which may in part explain the absence of respiratory viruses in some of the tested samples. Collectively, future studies should explore if unbiased pan‐pathogen assays, namely metagenomic next‐generation sequencing‐based approach could improve the etiological detection in patients presenting with respiratory infection; the usefulness of this approach has already been shown for other diseases worldwide, especially in low‐ and middle‐income countries like Vietnam.50
5. CONCLUSION
We reported the detection of common respiratory viruses in individuals with a high frequency of animal exposure in two distinct geographic regions in Vietnam, representing one of the broad‐range, prospective and controlled screenings for viral etiologies of respiratory illnesses in people with unique animal contacts in a setting where zoonotic emerging infections are likely to occur. The results show the value of baseline/control sampling in analyzing causative relationships and have revealed important insights into the ecological aspects of EVs, HRV and influenza A and their contributions to the burden posed by respiratory infections in Vietnam.
THE VIZIONS CONSORTIUM MEMBERS
The VIZIONS Consortium members (alphabetical order by surname) from the Oxford University Clinical Research Unit are Bach Tuan Kiet, Stephen Baker, Alessandra Berto, Maciej F. Boni, Juliet E. Bryant, Bui Duc Phu, James I. Campbell, Juan Carrique‐Mas, Dang Manh Hung, Dang Thao Huong, Dang Tram Oanh, Jeremy N. Day, Dinh Van Tan, H. Rogier van Doorn, Duong An Han, Jeremy J. Farrar, Hau Thi Thu Trang, Ho Dang Trung Nghia, Hoang Bao Long, Hoang Van Duong, Huynh Thi Kim Thu, Lam Chi Cuong, Le Manh Hung, Le Thanh Phuong, Le Thi Phuc, Le Thi Phuong, Le Xuan Luat, Luu Thi Thu Ha, Ly Van Chuong, Mai Thi Phuoc Loan, Behzad Nadjm, Ngo Thanh Bao, Ngo Thi Hoa, Ngo Tri Tue, Nguyen Canh Tu, Nguyen Dac Thuan, Nguyen Dong, Nguyen Khac Chuyen, Nguyen Ngoc An, Nguyen Ngoc Vinh, Nguyen Quoc Hung, Nguyen Thanh Dung, Nguyen Thanh Minh, Nguyen Thi Binh, Nguyen Thi Hong Tham, Nguyen Thi Hong Tien, Nguyen Thi Kim Chuc, Nguyen Thi Le Ngoc, Nguyen Thi Lien Ha, Nguyen Thi Nam Lien, Nguyen Thi Ngoc Diep, Nguyen Thi Nhung, Nguyen Thi Song Chau, Nguyen Thi Yen Chi, Nguyen Thieu Trinh, Nguyen Thu Van, Nguyen Van Cuong, Nguyen Van Hung, Nguyen Van Kinh, Nguyen Van Minh Hoang, Nguyen Van My, Nguyen Van Thang, Nguyen Van Thanh, Nguyen Van Vinh Chau, Nguyen Van Xang, Pham Ha My, Pham Hong Anh, Pham Thi Minh Khoa, Pham Thi Thanh Tam, Pham Van Lao, Pham Van Minh, Phan Van Be Bay, Maia A. Rabaa, Motiur Rahman, Corinne Thompson, Guy Thwaites, Ta Thi Dieu Ngan, Tran Do Hoang Nhu, Tran Hoang Minh Chau, Tran Khanh Toan, Tran My Phuc, Tran Thi Kim Hong, Tran Thi Ngoc Dung, Tran Thi Thanh Thanh, Tran Thi Thuy Minh, Tran Thua Nguyen, Tran Tinh Hien, Trinh Quang Tri, Vo Be Hien, Vo Nhut Tai, Vo Quoc Cuong, Voong Vinh Phat, Vu Thi Lan Huong, Vu Thi Ty Hang, and Heiman Wertheim; from the Center for Immunity, Infection, and Evolution, University Of Edinburgh: Carlijn Bogaardt, Margo Chase‐Topping, Al Ivens, Lu Lu, Dung Nyugen, Andrew Rambaut, Peter Simmonds, and Mark Woolhouse; from The Wellcome Trust Sanger Institute, Hinxton, United Kingdom: Matthew Cotten, Bas B. Oude Munnink, Paul Kellam, and My Vu Tra Phan; from the Laboratory of Experimental Virology, Department of Medical Microbiology, Center for Infection and Immunity Amsterdam (CINIMA), Academic Medical Center of the University of Amsterdam, Amsterdam, the Netherlands: Martin Deijs, Lia van der Hoek, Maarten F. Jebbink, and Seyed Mohammad Jazaeri Farsani; and from Metabiota, CA: Karen Saylors and Nathan Wolfe.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
Supporting information
Supporting information
ACKNOWLEDGMENTS
We deeply acknowledge all the cohort members, and the VIZIONS Consortium members listed below for their participation and contributions in the study. This study was funded by the Wellcome Trust of Great Britain (106680/B/14/Z, 204904/Z/16/Z, and WT/093724).
Nguyen TTK, Ngo TT, Tran MP, et al. Respiratory viruses in individuals with a high frequency of animal exposure in southern and highland Vietnam. J Med Virol. 2020;92:971–981. 10.1002/jmv.25640
Contributor Information
Tu Thi Kha Nguyen, Email: tuntk@oucru.org.
Tan Le Van, Email: tanlv@oucru.org.
REFERENCES
- 1. World Health Organization . Disease burden and mortality estimates: cause‐specific mortality, 2000–2016. http://www.who.int/healthinfo/global_burden_disease/estimates/en/. Published 2017. Accessed July 1, 2019.
- 2. World Health Organization . List of Blueprint priority diseases. https://www.who.int/blueprint/priority‐diseases/en/. Accessed July 1, 2019.
- 3. Do LAH, Bryant JE, Tran AT, et al. Respiratory syncytial virus and other viral infections among children under two years old in southern Vietnam 2009‐2010: clinical characteristics and disease severity. PLoS One. 2016;11(8):1‐16. 10.1371/journal.pone.0160606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Tran DN, Trinh QD, Pham NTK, et al. Clinical and epidemiological characteristics of acute respiratory virus infections in Vietnamese children. Epidemiol Infect. 2016;144(3):527‐536. 10.1017/S095026881500134X [DOI] [PubMed] [Google Scholar]
- 5. Do AHL, van Doorn HR, Nghiem MN, et al. Viral etiologies of acute respiratory infections among hospitalized Vietnamese children in Ho Chi Minh City, 2004‐2008. PLoS One. 2011;6(3):2004‐2008. 10.1371/journal.pone.0018176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Yoshida LM, Suzuki M, Yamamoto T, et al. Viral pathogens associated with acute respiratory infections in Central Vietnamese children. Pediatr Infect Dis J. 2010;29(1):75‐77. [DOI] [PubMed] [Google Scholar]
- 7. Alroy KA, Do TT, Tran PD, et al. Expanding severe acute respiratory infection (SARI) surveillance beyond influenza: the process and data from 1 year of implementation in Vietnam. Influenza Other Respir Viruses. 2018;12(5):632‐642. 10.1111/irv.12571 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Nguyen HKL, Nguyen SV, Nguyen AP, et al. Surveillance of severe acute respiratory infection (SARI) for hospitalized patients in Northern Vietnam, 2011–2014. Jpn J Infect Dis. 2017;70:522‐527. 10.7883/yoken.JJID.2016.463 [DOI] [PubMed] [Google Scholar]
- 9. Thi Ty Hang V, Thi Han Ny N, My Phuc T, et al. Evaluation of the Luminex xTAG Respiratory Viral Panel FAST v2 assay for detection of multiple respiratory viral pathogens in nasal and throat swabs in Vietnam. Wellcome Open Res. 2017;2:80. 10.12688/wellcomeopenres.12429.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Todd S, Huong NTC, Thanh NTL, et al. Primary care influenza‐like illness surveillance in Ho Chi Minh City, Vietnam 2013‐2015. Influenza Other Respir Viruses. 2018;12(5):623‐631. 10.1111/irv.12574 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Seah SGK, Lim EAS, Kok‐Yong S, et al. Viral agents responsible for febrile respiratory illnesses among military recruits training in tropical Singapore. J Clin Virol. 2010;47(3):289‐292. 10.1016/j.jcv.2009.12.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Andrews D, Chetty Y, Cooper BS, et al. Multiplex PCR point of care testing versus routine, laboratory‐based testing in the treatment of adults with respiratory tract infections: a quasi‐randomized study assessing the impact on the length of stay and antimicrobial use. BMC Infect Dis. 2017;17(1):1‐11. 10.1186/s12879-017-2784-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Jiang L, Lee VJM, Cui L, et al. Detection of viral respiratory pathogens in mild and severe acute respiratory infections in Singapore. Sci Rep. 2017;7:42963. 10.1038/srep42963 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Yoshida LM, Suzuki M, Nguyen HA, et al. Respiratory syncytial virus: co‐infection and paediatric lower respiratory tract infections. Eur Respir J. 2013;42(2):461‐469. 10.1183/09031936.00101812461 [DOI] [PubMed] [Google Scholar]
- 15. Yoshihara K, Le MN, Okamoto M, et al. Association of RSV‐A ON1 genotype with increased pediatric acute lower respiratory tract infection in Vietnam. Sci Rep. 2016;6:27856. 10.1038/srep27856 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. World Health Organization . Zoonoses ‐ Fact sheet. http://www.wpro.who.int/vietnam/topics/zoonoses/fa. Published 2019. Accessed August 19, 2019.
- 17. Horby PW, Pfeiffer D, Oshitani H. Prospects for emerging infections in East and Southeast Asia 10 years after severe acute respiratory syndrome. Emerg Infect Dis. 2013;19(6):853‐860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Pappaioanou M. Highly pathogenic H5N1 avian influenza virus: cause of the next pandemic? Comp Immunol Microbiol Infect Dis. 2009;32(4):287‐300. 10.1016/j.cimid.2008.01.003 [DOI] [PubMed] [Google Scholar]
- 19. Fineberg HV. Pandemic preparedness and response—lessons from the H1N1 influenza of 2009. N Engl J Med. 2014;370(14):1335‐1342. 10.1056/NEJMra1208802 [DOI] [PubMed] [Google Scholar]
- 20. Omrania AS, Shalhoub S. Middle East respiratory syndrome coronavirus (MERS‐CoV): what lessons can we learn? J Hosp Infect. 2015;91(3):188‐196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Carrique‐Mas JJ, Tue NT, Bryant JE, et al. The baseline characteristics and interim analyses of the high‐risk sentinel cohort of the Vietnam Initiative on Zoonotic InfectiONS (VIZIONS). Sci Rep. 2015;5:17965. 10.1038/srep17965 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Rabaa MA, Tue NT, Phuc TM, et al. The Vietnam Initiative on Zoonotic Infections (VIZIONS): a strategic approach to studying emerging zoonotic infectious diseases. Ecohealth. 2015;12(4):726‐735. 10.1007/s10393-015-1061-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Jansen RR, Schinkel J, Koekkoek S, et al. Development and evaluation of a four‐tube real‐time multiplex PCR assay covering fourteen respiratory viruses, and comparison to its corresponding single target counterparts. J Clin Virol. 2011;51(3):179‐185. 10.1016/j.jcv.2011.04.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Do LA, van Doorn HR, Bryant JE, et al. A sensitive real‐time PCR for detection and subgrouping of the human respiratory syncytial virus. J Virol Methods. 2012;179(1):250‐255. 10.1016/j.jviromet.2011.11.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. The US Centers for Disease Control . CDC Realtime RTPCR (RRTPCR) Protocol for Detection and Characterization of Influenza (Version 2007). 2007.
- 26. The US Centers for Disease Control . CDC Protocol of Realtime RT‐PCR for Swine Influenza A(H1N1).
- 27. StataCorp LLC. Stata 12 ‐ Data Analysis and Statistical Software. Available at: https://www.stata.com/
- 28. Armstrong RA. When to use the Bonferroni correction. Ophthalmic Physiol Opt. 2014;34:502‐508. 10.1111/opo.12131 [DOI] [PubMed] [Google Scholar]
- 29.Sergeant ESG. Epitools epidemiological calculators. Ausvet Pty Ltd. 2019. Available at http://epitools.ausvet.com.au
- 30. Sabanathan S, Tan le V, Thwaites L, Wills B, Qui PT, Rogier van Doorn H. Enterovirus 71 related severe hand, foot and mouth disease outbreaks in South‐East Asia: current situation and ongoing challenges. J Epidemiol Community Health. 2014;68(6):500‐502. 10.1136/jech-2014-203836 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Nhan LNT, Hong NTT, Nhu LNT, et al. Severe enterovirus A71 associated hand, foot and mouth disease, Vietnam, 2018: preliminary report of an impending outbreak. Euro Surveill. 2018;23(46):1‐5. 10.2807/1560-7917.ES.2018.23.46.1800590 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Ho Dang Trung N, Le Thi Phuong T, Wolbers M, et al. Aetiologies of central nervous system infection in Viet Nam: a prospective provincial hospital‐based descriptive surveillance study. PLoS One. 2012;7(5):e37825. 10.1371/journal.pone.0037825 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Tan LV, Qui PT, Ha DQ, et al. Viral etiology of encephalitis in children in Southern Vietnam: results of a one‐year prospective descriptive study. PLoS Negl Trop Dis. 2010;4(10):e854. 10.1371/journal.pntd.0000854 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Riaz N, Wolden SL, Gelblum DY, Eric J. The fraction of influenza virus infections that are asymptomatic: a systematic review and meta‐analysis. 2016;118(24):6072‐6078. 10.1002/cncr.27633.Percutaneous
- 35. Furuya‐Kanamori L, Cox M, Milinovich GJ, Soares Magalhaes RJ, Mackay IM, Yakob L. Heterogeneous and dynamic prevalence of asymptomatic influenza virus infections. Emerg Infect Dis. 2016;22(6):1052‐1056. 10.3201/eid2206.151080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Wertheim HFL, Nadjm B, Thomas S, et al. Viral and atypical bacterial aetiologies of infection in hospitalised patients admitted with clinical suspicion of influenza in Thailand, Vietnam and Indonesia. Influenza Other Respir Viruses. 2015;9(6):315‐322. 10.1111/irv.12326 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.National Foundation for Infectious Diseases. Respiratory syncytial virus in older adults: a hidden annual epidemic, A Report by the National Foundation for Infectious Diseases. 2016.
- 38. Fieldhouse JK, Toh TH, Lim WH, et al. Surveillance for respiratory syncytial virus and parainfluenza virus among patients hospitalized with pneumonia in Sarawak, Malaysia. PLoS One. 2018;13:e0202147. 10.1371/journal.pone.0202147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Anders KL, Nguyen HL, Nguyen NM, et al. Epidemiology and virology of acute respiratory infections during the first year of life: A birth cohort study in Vietnam. Pediatr Infect Dis J. 2015;34(4):361‐370. 10.1097/INF.0000000000000643 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Horm SV, Mardy S, Rith S, et al. Epidemiological and virological characteristics of influenza viruses circulating in Cambodia from 2009 to 2011. PLoS One. 2014;9(10):e110713. 10.1371/journal.pone.0110713 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Chittaganpitch M, Waicharoen S, Yingyong T, et al. Viral etiologies of influenza‐like illness and severe acute respiratory infections in Thailand. Influenza Other Respir Viruses. 2018;12(4):482‐489. 10.1111/irv.12554 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Foong Ng K, Kee Tan K, Hong Ng B, Nair P, Ying Gan W. Epidemiology of adenovirus respiratory infections among hospitalized children in Seremban, Malaysia. Trans R Soc Trop Med Hyg. 2015;109(7):433‐439. 10.1093/trstmh/trv042 [DOI] [PubMed] [Google Scholar]
- 43. World Health Organization . Seasonal influenza. https://www.who.int/ith/diseases/influenza_seasonal/en/. Accessed July 1, 2019.
- 44. Prasetyo AA, Desyardi MN, Tanamas J, et al. Respiratory viruses and torque teno virus in adults with acute respiratory infections. Intervirology. 2015;58(1):57‐68. 10.1159/000369211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Vong S, Guillard B, Borand L, et al. Acute lower respiratory infections in ≥5‐year‐old hospitalized patients in Cambodia, a low‐income tropical country: clinical characteristics and pathogenic etiology. BMC Infect Dis. 2013;13:97. 10.1186/1471-2334-13-97 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Furuse Y, Suzuki A, Kishi M, et al. Detection of novel respiratory viruses from influenza‐like illness in the Philippines. J Med Virol. 2010;82(6):1071‐1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Hong CY, Lin RT, Tan ES, et al. Acute respiratory symptoms in adults in general practice. Fam Pract. 2004;21(3):317‐323. 10.1093/fampra/cmh319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Buecher C, Mardy S, Wang W, et al. Use of a multiplex PCR/RT‐PCR approach to assess the viral causes of influenza‐like illnesses in Cambodia during three consecutive dry seasons. J Med Virol. 2010;82:1762‐1772. 10.1002/jmv.21891 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Arnott A, Vong S, Mardy S, et al. A study of the genetic variability of human respiratory syncytial virus (HRSV) in Cambodia reveals the existence of a new HRSV group B genotype. J Clin Microbiol. 2011;49(10):3504‐3513. 10.1128/JCM.01131-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Anh NT, Thu T, Truc N, Thanh T, Lau C. Viruses in Vietnamese patients presenting with community‐acquired sepsis of unknown cause. J Clin Microbiol. 2019;57(9):1‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information