

Abstract
Objective:
In a randomized trial for women with alcohol use disorders (AUD), the efficacy of Female-Specific Cognitive Behavioral Therapy (FS-CBT) was compared to Gender-Neutral CBT (GN-CBT; Epstein et al., 2018). The current study examined whether putative mechanisms of change differed between treatment conditions, using a novel statistical approach. Both treatments were hypothesized to work by increasing use of alcohol-related coping skills (coping) and confidence to abstain from drinking (confidence), but FS-CBT additionally targeted female-salient mechanisms: anxiety, depression, sociotropy (i.e., over-investment in others’ opinion of oneself), autonomy, and social networks supportive of abstinence.
Method:
Ninety-nine women with AUD (55 in GN-CBT, 44 in FS-CBT) completed self-report assessments at baseline and 0, 6, and 12 months post-treatment. Multilevel vector autoregression estimation was used to analyze associations between putative mechanisms of change, and network models of those associations were generated using network analysis.
Results:
Across conditions, higher confidence and coping were directly associated with less drinking; autonomy was directly and indirectly associated with drinking. Additionally, network analysis indicated that while variation in depression was associated with change in other variables specifically for GN-CBT, sociotropy was associated with change specifically in FS-CBT.
Conclusions:
Women receiving CBT-AUD changed their drinking through increased confidence to abstain and greater use of coping skills. Autonomy played a central role in behavior change across treatment conditions. Participants receiving treatment tailored to women also changed through decreases in sociotropy and increases in social support for abstinence. For women who received standard CBT, changes in depression were important to clinical improvement.
Keywords: Women, Alcohol, Mechanisms of Change, Cognitive-Behavioral Therapy
Around the start of 21st century, alcohol treatment research began focusing on empirically testing mechanisms by which psychotherapy may evoke behavior change (Kazdin & Nock, 2003). Although many treatments are effective for treating alcohol use disorder (AUD), an understanding of how these treatments have their effect would substantially advance the field (Longabaugh et al., 2005). With regard to cognitive behavioral therapy (CBT) for AUD, theory and existing research on the topic strongly suggest that improved alcohol-related coping skills and increased self-efficacy or confidence to maintain abstinence mediate post-treatment drinking outcomes (Longabaugh et al, 2005; Magill, Kiluk, McCrady, Tonigan, & Longabaugh, 2015; McCrady, 2017). However, full understanding of mechanisms of change in CBT for AUD has not yet been elucidated (Magill, Kiluk, McCrady, Tonigan, & Longabaugh, 2015). Further, it is not known if specific types of treatments lead to outcomes via unique as well as common mechanisms of change.
Mechanisms of Change among Women with AUD
In the current study, we examined data from a randomized clinical trial (RCT) for women with AUD. The RCT compared Female-Specific Cognitive Behavioral Therapy (FS-CBT) to Gender-Neutral CBT (GN-CBT) (Epstein et al., 2018). The study used a “pure comparison design” (Sobell, Sobell, & Agrawal, 2009), such that both GN- and FS-CBT targeted core CBT for AUD components, while FS-CBT additionally targeted female-salient issues. Specifically, both treatments were hypothesized to work by improving confidence to remain abstinent and increasing patients’ use of alcohol-related coping skills. FS-CBT additionally targeted evidence-based, female-salient issues including increased autonomy and increased social networks supportive of abstinence, as well as decreased anxiety, depression, and sociotropy. Sociotropy refers to over-concern with others’ opinion of oneself and dependence on positive feedback from others as a primary source of gratification (Bieling, Beck, & Brown, 2000). Women with AUD have been found to experience higher rates of co-occurring mood and anxiety disorders (Rosenthal, 2013), to drink in response to different triggers (Abulseoud et al., 2013) and situations (Zweig, McCrady, & Epstein, 2009) compared to men, suggesting that these factors may be important therapeutic targets within this population.
Primary results of the RCT (Epstein et al., 2018) found no significant treatment condition effect on engagement, with women in both treatment conditions having high engagement and reporting high treatment satisfaction. Drinking outcomes improved similarly across conditions, and there were not any significant treatment condition differences in change among most non-drinking mechanisms of change variables, including coping, confidence to abstain, sociotropy, autonomy, depression, or anxiety. In the year post-treatment, women in FS-CBT, but not GN-CBT, increased the number of abstainers in their social network. Since female-specific variables (i.e., autonomy, sociotropy, depression, anxiety, and social support) were targeted directly in FS-CBT but not in GN-CBT, and since both treatment conditions targeted coping skills and confidence to avoid drinking, we were able to examine if the common mechanisms of change behaved as hypothesized, and if the hypothesized female-specific mechanisms of change were impactful specifically in the FS-CBT condition. In other words, based on the design of our parent study, we were able to examine if women in two different treatments, GN-CBT and FS-CBT - which had some shared and some divergent components - attained the same results (i.e., positive drinking outcomes) but via two different pathways - that is, via change in different mechanisms - based on treatment condition. The current study sought to build on the main RCT findings by using a different statistical approach to more closely examine putative mechanisms of change.
A Novel Statistical Approach to Exploring Mechanisms of Change
Statistical approaches have been limited in their ability to examine the interactional and reciprocal effects of multiple mechanisms within a model (Constantini et al., 2015). Many analyses to examine mechanisms of change, such as mediation models, posit a linear causal chain (e.g., treatment condition→ increased coping skills→ decreased frequency of alcohol use) and do not necessarily model alternative causal hypotheses or allow for interactions among multiple mechanisms (Constantini et al., 2015). This approach – imposing a constrained structural model typically used in mediation analyses and in path models more generally – prohibits the examination of interactive and reciprocal effects among multiple mechanisms within a treatment (Constantini et al., 2015). One meta-analysis on mechanisms of change in depression treatment helps illustrate this problem: although 80% of studies that tested mediation included more than one mediator (Lemmens et al., 2016), the interrelationships and interactions among these multiple mediators were often unaccounted for, with only “a small number” looking at relative importance of each mediator (assessed by comparing effect sizes or regression coefficients of the different mediators; Lemmens et al., 2016). Testing mechanisms of change hypotheses using restricted, linear causal chain analyses in these ways introduces a number of risks. Advanced statistical approaches are rapidly addressing this issue and allowing researchers to model mediational effects with increasing sophistication (e.g., multiple mediation, latent growth curve mediation, latent difference score mediation), but all statistical approaches have limitations. Using varied statistical approaches is an important step in identifying mechanisms of change (Nock, 2007).
Network Analysis.
Network Analysis is a broad term for a family of statistical approaches that examines the connections among variables in a network (Afzali et al., 2017), and may be useful in highlighting potential causal pathways when applied to longitudinal data (Epskamp, Waldorp, Mõttus, & Borsboom, 2018), such as that from RCTs. In the current study, analyses were used that combine multi-level modeling, which models time in flexible ways, with network analysis, which examines the connections between variables or “nodes” (as they are referred to in network analysis; Epskamp, Waldorp, Mõttus, & Borsboom, 2018). In network analysis, a network of nodes can be visually modeled to illustrate associations among all combinations of variables. The main outcome measure in the current study is centrality of nodes. Centrality is estimated for each node, or each variable of interest within the network (e.g., confidence, depression, anxiety), and reflects the relative importance or influence that node holds within the network of several nodes. High node centrality is an important indicator of a larger change process and are indicative of variables that may be important therapeutic targets. Centrality can be measured in several ways (see Method section), and those several measures are examined to provide information about which nodes are most influential or important in that network. In the present analyses, we modeled eight nodes, or variables, which reflect putative mechanisms of change in GN-CBT and FS-CBT (including a node reflecting frequency of drinking). A highly central node is a variable that, when it varies, has broad effects on the rest of the nodes in the network and thus reflects a larger process of change; specifically, it reflects a variable that is not only associated with significant change in drinking (i.e., a potential mechanism of behavior change for AUD treatment in the present study), but is also associated with all the measured nodes in the network. For example, depression as a highly central node within a network would suggest that variation in depression is associated with change in the other variables – drinking, anxiety, self-confidence, coping skills, etc. Pathways within the network (also referred to as “edges”) may be examined to understand which nodes are most closely associated with one another; for example, if depression were a highly central node, the network may show that it is specifically associated with drinking and/or anxiety, demonstrated by a solid edge in the network model. We can also examine specific associations, such as those between each node and the drinking node (given that drinking is our primary behavior of interest in AUD treatment). It is important to note, however, that these analyses allow all variables, or nodes, to covary, which can lead to confounding and suppression effects (MacKinnon, Krull, & Lockwood, 2000). These effects can cause, for instance, a counter-intuitive direct association between two variables in a network model. Therefore, results speak less to directionality and causality of effects between nodes (as in traditional mediation analyses); rather, highly central nodes are reflective of the relative “importance” of certain variables that are responsible for significant change within the network.
Multilevel Vector Autoregression (mlVAR) Estimation.
These analyses allow us to examine associations between nodes, as described above, while also modeling time in a flexible way. This is important because change is a process (DiClemente, 2007), and although certain variables may be important in predicting concurrent changes in drinking, other variables may be important in predicting time-lagged change; additionally, some variables may be important across all time points – for example, confidence to abstain from alcohol may be predictive of alcohol use generally, regardless of how time is modeled. These analyses allow us to examine network structure (i.e., associations between nodes) across or within single assessment points by generating three networks, each of which treats time differently. Specifically, using repeated measures data, temporal networks examine the association between a node at one time point (t) and all nodes at the next time point (t+1) (Constantini et al., 2015). Contemporaneous networks provide information about associations between nodes concurrently (within a single time point), and between-subjects networks provide information about random effects, estimating a network between stationary means of different participants.
Importantly, these analyses allow us to identify multiple potential mechanisms of change, which may act in parallel or have interactive and/or reciprocal effects. This is an added benefit of this approach over multiple mediator models. For example, two mechanisms of change in CBT for AUD are patient’s increased ability to cope with high-risk situations that potentiate drinking, and improved confidence to avoid drinking (Magill, Kiluk, McCrady, Tonigan, & Longabaugh, 2015). However, the extent to which confidence is a product of other mechanisms, such as improved coping skills or decreases in drinking, is unclear (Kadden & Litt, 2011; Hallgren, Epstein, & McCrady, 2019); in other words, increased confidence may represent a marker or signal of change rather than act as a mechanism of change itself (DiClemente, 2007). By modeling networks based on the covariation among relevant mechanisms (e.g., confidence, coping, depression, anxiety, drinking), multilevel vector autoregression estimation allows us to explore multiple pathways to behavior change, identifying direct and indirect pathways between variables - while controlling for the presence and variation of all other variables in the model and reciprocal effects between variables. To achieve this benefit of controlling for several other putative mechanisms of change (and their interactions), as mentioned above, we sacrifice specificity about directionality of associations between specific nodes, focusing instead on the importance of certain variables in terms of how each variable affects change among other variables in the network (Epskamp, Waldorp, Mõttus, & Borsboom, 2018).
Study Aims
The current study examines networks of mechanisms of change among women in two types of CBT for AUD (FS-CBT and GN-CBT), with FS-CBT targeting possible female-specific mechanisms. We hypothesized that the putative mechanisms of change shared by GN-CBT and FS-CBT (improved coping skills, confidence to remain abstinence) would be central (or influential) nodes within the networks modeled for both treatment conditions. We also hypothesized that “female specific” mechanisms (i.e., autonomy, sociotropy, depression, anxiety, social network supportive of abstinence) explicitly targeted in FS-CBT but not in GN-CBT would be central nodes specifically in the FS-CBT network, and not in the GN-CBT network.
Methods and Materials
Study Design
The parent RCT was a two-arm choice study (McCrady, Epstein, Cook, Jensen, & Ladd, 2011) in which women with AUD were given the option of choosing a couple (McCrady, Epstein, Hallgren, Cook, & Jensen, 2016) or individual therapy arm (Epstein et al., 2018), then randomized into one of two conditions within the chosen arm. Women included in the current analyses were from the individual therapy arm, in which they were randomized to receive the Female-Specific (n=44) or Gender-Neutral (n=55) CBT for AUD. Study procedures were approved by the University IRB and conducted in accordance with established ethical guidelines.
Participants
Participants were recruited into the study via a variety of strategies including media articles, advertisements, and community outreach. Inclusion criteria were: (a) woman, aged 18 or older; (b) in a committed heterosexual relationship (married, separated, cohabiting at least 6 months, or in a committed dating relationship for at least 1 year) to accommodate the choice design; (c) consumed alcohol in the 30 days prior to telephone screen; (d) met DSM–IV (American Psychiatric Association, 2000) criteria for alcohol abuse or dependence. Exclusion criteria were: (a) physiologically dependent on drugs other than marijuana or nicotine, (b) psychotic symptoms in past 6 months, and/or (c) gross cognitive impairment. See Table 1 for demographic information and baseline characteristics (see Epstein et al., 2018 for additional sample details).
Table 1.
Participant baseline demographic, drinking, and psychological conditions
| Full Sample (N = 99) | GN-CBT (N = 55) | FS-CBT (N = 44) | ||||
|---|---|---|---|---|---|---|
| M/N | (SD)/% | M/N | (SD)/% | M/N | (SD)/% | |
| Age | 47.88 | (8.85) | 48.24 | (8.45) | 47.43 | (9.41) |
| Education | 15.09 | (2.50) | 15.22 | (2.57) | 14.93 | (2.42) |
| Household Income (thousands) | 96.62 | (60.44) | 97.97 | (46.16) | 94.91 | (75.20) |
| Employed | 53 | 53.54% | 28 | 50.91% | 25 | 56.82% |
| White, Non-Hispanic | 91 | 91.92% | 52 | 94.55% | 39 | 88.64% |
| Mean N of Alcohol Abuse & Dependence Symptoms (of 11) | 8.48 | (1.82) | 8.60 | (1.78) | 8.34 | (1.88) |
| Percent Drinking Days | 70.99 | (28.77) | 69.51 | (29.61) | 72.83 | (27.91) |
| Percent Heavy Drinking Days1 | 53.18 | (34.14) | 55.07 | (33.47) | 50.81 | (35.20) |
| Drinks Per Drinking Day | 6.83 | (3.94) | 7.07 | (4.28) | 6.52 | (3.49) |
| >1 Current Axis-I Disorder | 45 | 45.45% | 29 | 52.73% | 16 | 36.36% |
| Current MDD2 or Dysthymia | 34 | 34.34% | 24 | 43.64% | 10 | 22.73% |
| ≥1 Current anxiety disorder | 33 | 33.33% | 19 | 34.54% | 14 | 31.82% |
Note: GN-CBT = Gender-neutral cognitive-behavioral therapy. FS-CBT = Female-specific cognitive-behavioral therapy. No significant differences were noted between FS-CBT and GN-CBT on independent samples t test or Fisher’s exact test.
Defined for women as ≥4 standard drinks within a day
MDD is Major Depressive Disorder
Procedures
Participants completed a telephone and in-person clinical screen at the University’s Center of Alcohol Studies to establish eligibility, during which they completed self-report questionnaires and semi-structured clinical interviews. After establishing clinical eligibility, women returned for the baseline research assessment at which they signed consent and completed a number of self-report and interview questionnaires. Participants were paid $50 for baseline assessment completion. Urn randomization (Stout, Wirtz, Carbonari, & DelBoca, 1994) was used to balance levels of depression (Beck Depression Inventory score <14 vs. ≥14), personal drinking goal (abstinent or non-abstinent drinking goal), and partner drinking status (recovering, abstinent, or light drinker vs. moderate/heavy drinker). Participants completed follow-up assessments at 0, 6, and 12 months post-treatment. Assessment data from these four time points (baseline, 0, 6, and 12 months post-treatment) comprised the data for the current analyses.
Study Treatments
Both treatments were manual-guided, outpatient, individual modality 12-session CBT protocols with a goal of abstinence from alcohol. Sessions in both conditions were 60 minutes except session one, which was 90 minutes.
Gender-Neutral CBT for AUD
(GN-CBT; Epstein & McCrady, 2009) included core CBT, motivational enhancement therapy (MET) and relapse prevention (RP) treatment components (e.g., identifying alcohol-related triggers, behavior chains, decisional matrix). Two putative mechanisms of change were targeted in both this treatment condition and in FS-CBT: use of alcohol-related coping skills (referred to as coping) and confidence or self-efficacy to abstain from alcohol (referred to as confidence).
Female-Specific CBT for AUD
(FS-CBT; Epstein et al., 2018) included the same core CBT, MET, and RP components described above; however, all language, examples, vignettes, worksheets, and illustrations were female-specific. Additionally, the FS-CBT protocol integrated interventions that target issues shown to be associated with women’s alcohol use, and thus are putative mechanisms of change for women with AUD. These targeted topics (including developing a social support network that supports abstinence; coping with comorbid depression and anxiety; increasing autonomy and decreasing sociotropy) were also covered in the twelve sessions.
Follow-up.
Women were assessed 0, 6, and 12 months after treatment. The initial follow-up assessment (0 months) was delayed to the end of treatment (up to 16 weeks after baseline) for women who were still in treatment beyond the scheduled 12 weeks. 0-, 6- and 12-month follow-up rates were 91%, 85%, and 80%, respectively.
Measures
Abbreviations for each mechanism/node used in the network models (seen in Figure 1) are presented in bold below, where relevant.
Figure 1.
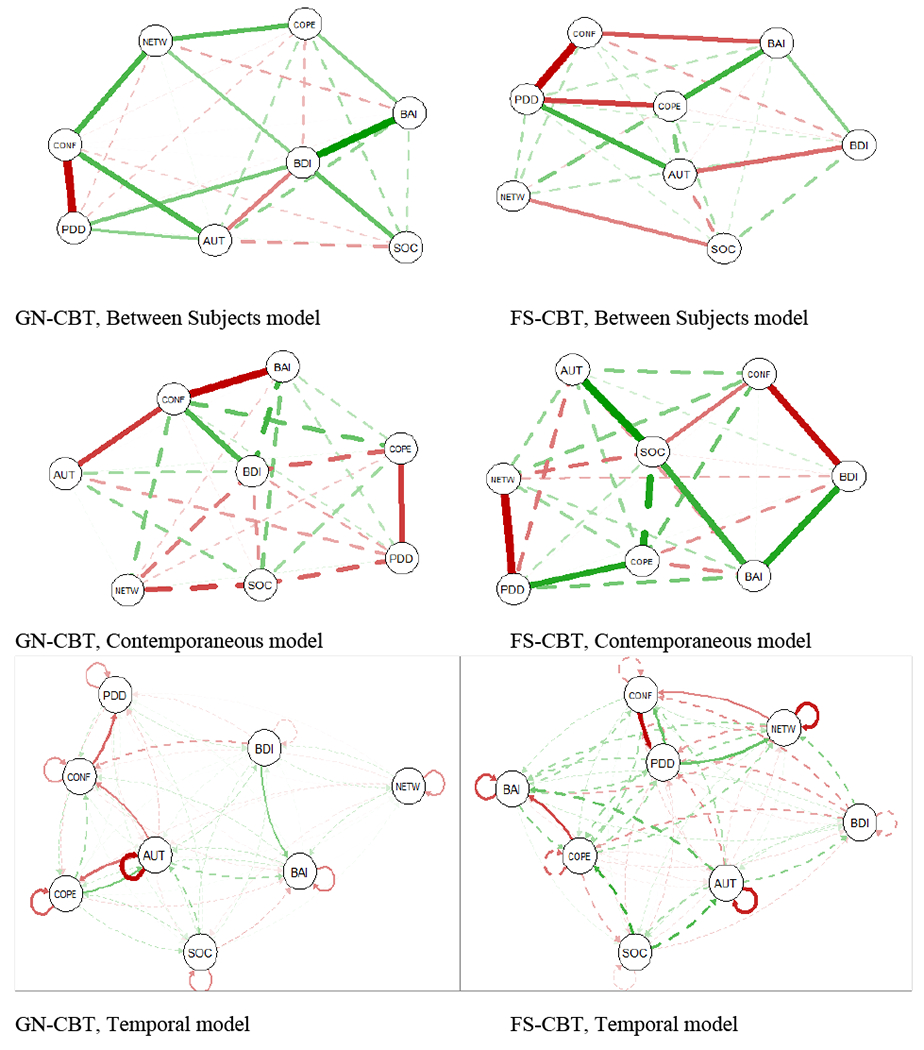
Variable networks, by model type
PDD = Percent Days Drinking (in 3 months prior to assessment); CONF=confidence to abstain; AUT=autonomy; COPE=use of alcohol-related coping skills; SOC=sociotropy; BAI=Beck Anxiety Inventory; BDI=Beck Depression Inventory; NETW=size of social network who is supportive of abstinence. Green = positive coefficients, Red = negative coefficients. See Methods for details. Data from all four assessment periods inform the development of these networks. If an association is significant at multiple assessment periods (or multiple combinations of assessment periods, in the temporal models), then the edge, or line, between two nodes is thicker.
Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-IV, First et al., 2002).
The SCID-IV is a semi-structured interview to assess current and lifetime Axis I disorders (including AUD) using DSM-IV (APA, 2000) criteria.
Coping Behaviors Inventory (CBI; Litman, Stapleton, Oppenheim, & Peleg, 1983; coping/COPE).
The CBI is a 36-item self-report questionnaire to measure frequency of use of various behaviors to cope with alcohol-related thoughts, situations, and cravings on a scale from 0 (“I have never tried this”) to 3 (“I have usually tried this”). The total score of the CBI was used, which ranged from 0 to 108. The Cronbach’s alpha coefficient for the current sample was .93.
Situational Confidence Questionnaire (SCQ-8; Breslin, Sobell, Sobell, & Agrawal, 2000; confidence/CONF).
The SCQ is an 8-item self-report measure of confidence, or self-efficacy, in one’s ability to not drink alcohol in eight separate situations. Each item is rated on a scale from 0% (not at all confident) to 100% (totally confident). For this study, the total score was used, which is the participant’s average rating across all items.
Beck Depression Inventory-II (Beck, Steer, & Garbin, 1988; depression/BDI) and Beck Anxiety Inventory (Beck, Epstein, Brown, & Steer, 1988; anxiety/BAI).
The BDI-II and BAI are 21-item measures that assess the severity of depression (last two weeks) or anxiety symptoms (last week), respectively. For both measures, each item is rated on a scale from 0 (non-presence of symptom) to 3 (worst severity of symptom) and total scores range from 0-63. Cronbach alphas in the current sample were 0.91 for BDI-II and 0.94 for BAI.
Sociotropy-Autonomy Scale (SAS; Bieling, Beck & Brown, 2000; sociotropy/SOC and autonomy/AUT).
The SAS is a 27-item self-report measure of two subscales, sociotropy and autonomy. All items are rated on a 0-5 Likert scale and reflect the extent to which the participant agrees with each statement. The sociotropy scale reflects an individual’s concern with others’ opinion of her and is described as, “the person’s investment in positive interchange with others” and, “dependence on social feedback for gratification and support” (Bieling et al., 2000, p. 763). Autonomy is defined as “the person’s investment in preserving and increasing his(her) independence, mobility, and personal rights” (Bieling et al., 2000, p. 763).
Important People Interview (IPI, Longabaugh, Wirtz, Zweben, & Stout, 1998; social network supportive of abstinence /NETW).
The IPI is a structured interview used to assess the extent of drinking and response to abstinence within a person’s social network. Although several variables can be calculated from the IPI, the current study used the percent of each participant’s network that the patient identified as being accepting/encouraging of her abstinence.
Timeline Follow-Back (TLFB; Sobell & Sobell, 1996; percentage of days drinking/PDD).
The TLFB uses a calendar and other memory aids to determine an individual’s drinking over a specified time. At baseline, participants were interviewed about their drinking on each of the 90 days prior to last drink before baseline; the TLFB also was administered at the three post-treatment research assessments. The TLFB has excellent reliability (Sobell & Sobell, 1978) and validity for alcohol use (Sobell, Maisto, Sobell & Copper, 1980). TLFB data were used to calculate percentage of days drinking (PDD).
Daily Drinking Log (DDL).
Women were asked to keep daily records of drinking during the twelve-session treatment period, from which within-treatment PDD was calculated. Data from the TLFB at the first post-treatment assessment were used in lieu of missing DDL data for the within treatment period. Previous studies of the DDL have revealed correlations of .90 or greater between patient and partner reports of number of drinking days per month (McCrady, Epstein & Hirsch, 1999).
Data Analytic Plan
Network Analysis.
Network analysis is an approach used to formulate a model containing “nodes” (i.e., variables, or symptoms and behaviors such as depression, anxiety, PDD), along with “edges” (i.e., relations between variables; Constantini et al., 2015). Demonstrating covariation between nodes, network models show the extent to which the variation of one variable (or node) stimulates or inhibits the presence and variation of all other variables (Constantini et al., 2015; Afzali et al., 2017). In this study, we conducted network analyses using data from the four study time points (baseline, 0-, 6- and 12-month post-treatment; Haslbeck & Waldorp, 2018). As described in the introduction, applying multilevel modeling techniques to network analysis, described below, provided three networks that show associations between putative mechanisms of change while also allowing for examination of the effects of time (Epskamp et al., 2018).
Multilevel Vector Autoregression Estimation.
Analyses were conducted using R statistical software, version 3.4.1, with software packages mlVAR and graphicalVAR (Epskamp et al., 2018). Two-Step Multilevel Vector Autoregression Analysis (mlVAR) was used to examine the associations between nodes within each of the two treatment conditions (Epskamp et al., 2018). mlVAR estimates three networks, each one treating time differently. For a hypothetical example, although a person’s confidence to abstain may be very closely associated with her drinking on any given day, it may be less closely associated with her drinking six months later. These three models (between-subjects, contemporaneous, and temporal) help make such distinctions.
These models are estimated as such: To estimate temporal networks (demonstrating lag-1 models of associations between nodes), sequential univariate multilevel regression of the nodes is performed onto lagged versions [i.e., node/variable at time point t is regressed to a lagged (t-1) version of that node]. This is conducted using within-person centered variables as predictors at the within-subject level and sample means of all other variables as predictors at the between-subject level. Temporal effects were modeled as fixed, with only the intercept as random. In the second step, between-subject networks are estimated from the covariance structure of stationary means (i.e., collapsed over time, within one assessment time point, demonstrating networks at the between-person level). The variance-covariance matrix of the residuals from the first step is then used to model contemporaneous effects (i.e., the statistically causal relationships within one time, or assessment, point). Contemporaneous networks reflect associations or effects that are happening more quickly than effects in the temporal model (the latter reflects change across the course of four-to-six months in the current RCT). Both between-subject and contemporaneous networks reflect associations between nodes at any one time point (collapsing across all 4 assessment time points). For example, increased depression at any one assessment time point may be associated with increased drinking at that same assessment time point. If there is an association between drinking and depression at every time point – baseline, post-treatment, and at each follow-up assessment – the edge (reflecting a regression coefficient) between those two nodes would be significant in the between-subjects network model.
For contemporaneous and between-subject networks, a significant edge may reflect that (a) node A statistically predicts node B, (b) node B statistically predicts node A, or (c) nodes A and B statistically predict each other. Temporal networks reflect directionality, therefore significant edges may be interpreted as potentially causal pathways (Epskamp et al., 2018). However, this is an exploratory approach and not all requirements for establishing causality are met, given that variables were not directly or independently manipulated. Although these analyses do establish temporal precedence, the potential for missing confounding variables to explain network associations remains an un-met assumption and general limitation to most longitudinal mechanism studies. Thus, it is important to emphasize that these relationships are only potential causal pathways.
Interpreting Results - Measures of Centrality.
Centrality measures operationalize the importance of a node or variable (i.e., the extent to which variation in one node influences variation in other nodes). This study used four indices of centrality, which were calculated for each of the eight nodes/putative mechanisms of change. These four indices of centrality are generated for each node, within each of the three types of networks (between, contemporaneous, and temporal), as time can affect which nodes are more or less central. The four indices of centrality reported in this study are: (a) degree (the number of connections, or significant bridges, incident to the node of interest), (2) strength (the sum of weights of connections in weighted networks; each “edge” has a parameter estimate which provides a weight as these analyses are regression-based), (c) closeness centrality (the proximal association between nodes – nodes high in closeness centrality are tightly clustered with other nodes, while low closeness nodes are structurally further, or less closely associated, with other nodes in the network), (d) betweenness centrality (if a node high in betweenness centrality is removed, the distances among other nodes will generally increase; Costantini et al., 2015). There may be conditions in which certain nodes become more or less central, or important, to change within that network of variables. In our study, we hypothesized that node centrality will differ based on treatment condition – i.e., different nodes, or putative mechanisms of change, would be central in FS-CBT and GN-CBT.
In addition to examining centrality parameters, we also identified variables that were directly associated with PDD within each model, given that these women were in treatment for AUD and our interest is in mechanisms of change for alcohol use. While we must analyze the exact directionality of these associations between particular nodes and PDD carefully, due to suppressor and confounder effects described above (Epskamp, Waldorp, Mõttus, & Borsboom, 2018; MacKinnon, Krull, & Lockwood, 2000), the network results indicate which nodes are directly related to drinking while adjusting for variation in all other nodes. For instance, there may be a positive partial correlation between use of alcohol-related coping skills and drinking in a given network. This is unlikely to represent a true positive association and is likely due to the inclusion of multiple nodes in the network that are allowed to co-vary; however, the strength of that association is the focus of these analyses and results. Thus, nodes that show centrality to the network are the variables (or putative mechanisms of change) that are indicative of the overall change process among women receiving either GN- or FS-CBT for AUD, and nodes that are directly related to PDD are those that have direct effects on drinking.
Results
See Table 1 for participant demographics and Table 2 for correlations between network nodes in FS-CBT and GN-CBT.
Table 2.
Correlations between variables, collapsed across time points
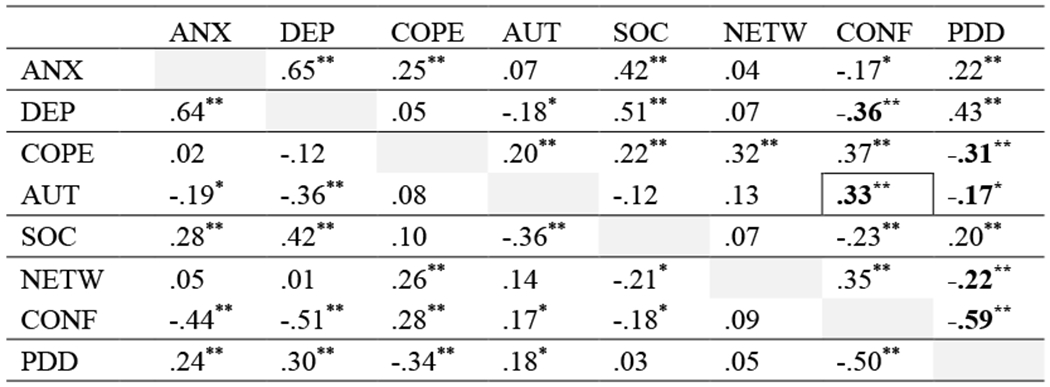 |
p<.01 ;
p<.05
Values below diagonal are correlations among women in FS-CBT condition, values above the diagonal are correlations among women in GN-CBT; Bolded values reflect negative direct correlations which are positive in the network, Bolded and boxed values reflect positive direct correlations which are negative in the network
Preliminary Analyses
A node was coded to reflect the presence of missing data, for each participant at each assessment time point. Then, networks with and without the missing data node modeled were compared to ensure that missing data did not affect outcomes. Specifically, a node or variable reflecting whether a participant had missing data (yes/no) was entered into analyses. Running analyses with that node entered allowed us to examine whether excluding missing data affected the results. These comparisons were completed with data at baseline and during the follow-up period using between-subject networks. In addition to having similar network structures, the networks were the same regarding centrality measures of degree, closeness, and betweenness, regardless of whether missing data were or were not modeled. Therefore, we excluded data from time points in which there were missing data.
Additionally, to test whether the network models were consistent at each time point, we conducted cross-sectional analyses. Specifically, between-subject networks for each time point were created and centrality parameters were estimated, by treatment condition, for each of the 4 time points. The results of these cross-sectional analyses showed that the nodes with the highest centrality parameters had consistent high centrality across time points in FS-CBT, and especially GN-CBT. This demonstrates consistency across time points (e.g., in cross-sectional networks, depression and confidence were consistently central in GN-CBT, while autonomy and sociotropy are consistently central in FS-CBT). Further, there was no specific trend in the data across time points (e.g., there was no consistent change in centrality associated with time). This consistency was also reflected in networks that accounted for spacing between assessments. There were four months between the first and second assessments, and six months between the remaining assessments. Networks including the first assessment (as reported here) and networks using the last three assessments only showed consistent results.
Between-Subject Networks in GN-CBT and FS-CBT
Examining between-subject networks within each treatment condition provides information about the centrality, or relative influence, of each node overall, and the nodes associated with aggregate level of drinking across all time points. (See Figure 1, top row, for networks, and Figure 2a for graphed centrality parameters).
Figure 2.
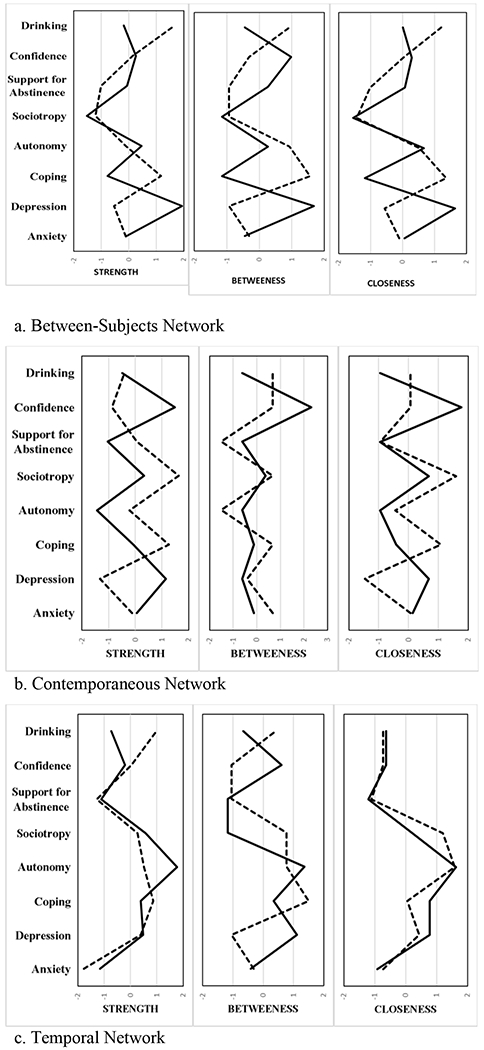
Centrality parameters across treatment conditions
Notes: Solid line = GN-CBT, Dashed line = FS-CBT. Parameter values are standardized z-scores for clear comparison; higher z-score reflects higher centrality.
GN-CBT.
Depression showed the greatest level of betweenness, closeness, and strength, indicating that depression had the strongest and greatest number of connections to other nodes in the network (Figure 2a). Thus, it was the most central (or influential) node in the GN-CBT network, collapsing across all time points. Additionally, its closeness-centrality indicates that depression was most likely to be affected by changes in other nodes. Depression also had the highest betweenness centrality, indicating that if it were removed the distances among other nodes would increase. Thus, long-term changes (increases or decreases) in depression played an important mediating role between other variables – including drinking – in the model. This mediating role of depression can be seen in Figure 1 (top row).
The GN-CBT network showed that confidence (partial r = −.59), autonomy (partial r = .26), and depression (partial r = .31) were directly associated with drinking (conditional on other variables in the network), across participants and time. While the negative association between confidence and PDD and positive association of depression with drinking are consistent with direct associations, the positive association of autonomy with drinking is contrary to direct associations. However, the network model suggests that higher autonomy was both directly associated with higher PDD and indirectly associated with lower PDD due to partial mediation effects of lower depression and higher confidence, which associated with autonomy and PDD across time.
FS-CBT.
PDD and use of coping skills were the most central nodes in the FS-CBT between-subjects model (Figure 2a). PDD and coping were the most closeness-central nodes (suggesting that they were most quickly affected by changes in the other nodes) and had the strongest and most significant edges with other variables in the network. As in GN-CBT, autonomy (partial r = .43) and confidence (partial r = −.59) were directly associated with PDD. Unlike in GN-CBT, coping (partial r = −.44) was also directly associated with PDD. While the negative associations of confidence and coping with PDD are consistent with hypotheses and direct associations, the positive association between autonomy and PDD was inconsistent with hypotheses but consistent with direct correlations. As in GN-CBT, autonomy was negatively associated with depression.
In sum, when examining between-subject networks, GN-CBT and FS-CBT showed similar associations, with confidence and autonomy being associated with women’s drinking in both groups. However, the nodes that were most central overall differed between conditions. Among women in GN-CBT, variation in their depression broadly impacted the other variables in the network (with direct effects on drinking, anxiety, sociotropy, and autonomy). Among women in FS-CBT, variation in their use of alcohol-related coping skills and the amount they were drinking broadly impacted other variables in the model (with direct effects on confidence, anxiety, and autonomy)
Contemporaneous Models in GN-CBT and FS-CBT
Contemporaneous network models represent whether two variables are statistically associated within the same time point, after controlling for all other variables in the network model. Thus, contemporaneous models suggest what nodes are concurrently associated with drinking. If an association is significant at all four assessment time points, the line in the contemporaneous network model will be thicker than if, for instance, the association is only significant at one assessment time point (Figure 1, middle row, Figure 2b).
GN-CBT.
For GN-CBT, confidence was the most central node, with regard to degree, centrality, betweenness, and strength (Figure 2b). As in the GN-CBT between-subjects model, depression was a central node in terms of strength.
In these GN-CBT contemporaneous networks, use of alcohol-related coping skills was the only node directly related to drinking (PDD) (partial r = −.18). In other words, at any given time point, the extent to which women in GN-CBT reported using alcohol-related coping skills was most closely and negatively related (after conditioning on all other variables in the model) to drinking in the three months prior to that measurement period.
FS-CBT.
Among women who received FS-CBT, coping and sociotropy were the most central nodes on strength and closeness measures (Figure 2b), having greatest effect on all the other nodes in the network.
As in GN-CBT, FS-CBT participants’ use of coping skills was directly associated with drinking in the prior three months (partial r= .18). Unlike GN-CBT, the size of social network supportive of sobriety was concurrently, negatively affecting drinking (partial r= −.27).
In sum, contemporaneous network models, which reflect the concurrent associations between nodes, show that GN- and FS-CBT have different central nodes. While confidence to abstain and depression were most central in the GN-CBT condition, use of coping skills and sociotropy were most central in FS-CBT. Focusing on drinking, there were the similar results across conditions, with use of coping skills most directly associated with drinking, but with participants’ social network supportive of sobriety also associated with drinking in FS-CBT. Contemporaneous models demonstrated some unexpected direct associations between variables and drinking, potentially due to PDD reflecting drinking in the 3 months prior to assessment and the multiple, concurrent effects of multiple variables on drinking.
Temporal Models in GN-CBT and FS-CBT
Temporal models show associations between network nodes across time points, including time-lagged changes in drinking. Temporal models also show whether nodes have auto-regressive effects, reflecting whether a focal node at time point A is predictive of itself at time point B. Significant auto-regressive effects indicate stability in a node over time, with positive effects reflecting stability over time and negative effects reflecting more change in a node. As in contemporaneous models, a thicker edge reflects that two nodes were associated across multiple time points (e.g., baseline node A predicted post-treatment node B, post-treatment node A also predicted 6-month post-treatment node B at 6.).
GN-CBT.
The temporal network among women who completed GN-CBT showed that most nodes were negatively auto-regressive over time among women in GN-CBT (Figure 1, bottom row). The one node that this was not true for was depression, which had a non-significant auto-regressive effect from time A to time B (e.g., a participant’s depression post-treatment was not positively or negatively predictive of depression 6 months post-treatment). Autonomy and depression were the most central nodes in GN-CBT temporal networks, suggesting these variables were most influential on variables at subsequent time points (Figure 2c).
Confidence was the only variable directly predicting PDD (B= −.32, p=.000), and it also mediated the effect of autonomy on PDD (Figure 1, bottom row). Specifically, higher confidence was associated with less drinking at the next time point.
FS-CBT.
Among women in FS-CBT, unlike GN-CBT, only three (autonomy, anxiety, and size of supportive network) of the eight nodes were significantly (negatively) auto-regressive, reflecting negative associations between time points(Figure 1, bottom row).
Use of coping skills, autonomy, and sociotropy were the most central variables within FS-CBT. Both confidence to abstain (B= −.44, p =.00) and size of social network supportive of abstinence (B= .25, p =.03) were significant predictors of drinking for FS-CBT. Specifically, higher confidence was associated with less drinking at the next point. Higher PDD was associated with larger social networks supportive of abstinence at the next time point. While the former finding is consistent with theory and past research, the latter is less intuitive. While this finding may be related to spurious effects, as described above, it may also be that higher PDD at time point A may prompt or motivate participants to change their social networks by time point B. This is supported by the finding that the significant association was due to the effect of PDD at time A on social network at time B, but not vice-versa.
In summary, autonomy was a consistently central node across treatment condition in temporal models. Confidence to abstain was the only node in both treatment conditions that was directly related to PDD in these temporal models.
Summary of Results
To summarize comparisons between treatment conditions (also, see Tables 2 and 3): One node – depression – was found to be an important variable specifically in GN-CBT (as indexed by centrality parameters and identifying nodes directly associated with drinking). Two different nodes – sociotropy and size of social network supportive of abstinence – were found to be important variables specifically in FS-CBT. Three nodes were found to be important variables in both GN- and FS-CBT – confidence to abstain from alcohol, use of alcohol-related coping skills, and autonomy.
Table 3.
Results summary table
| Network Type | Gender Neutral CBT | Female Specific CBT | ||
|---|---|---|---|---|
| Most Central Nodes | Directly Related to PDD+ (partial r) | Most Central Nodes | Directly Related to PDD+ (partial r) | |
|
Between-Subjects (participants’ deviation from the sample mean in these variables/nodes affects other network nodes, collapsed across time) |
Depression | Confidence (−.59**) Autonomy (.26*) Depression (.31*) |
Coping PDD |
Confidence (−.59**) Coping (−.44**) Autonomy (.43**) |
|
Contemporaneous (nodes relate to each other within each time/assessment point) |
Confidence Depression |
Coping (−.18*) | Coping Sociotropy |
Coping (.18**) Supportive Network (−.27*) |
|
Temporal (nodes at time point A relate to nodes at time point B) |
Autonomy Depression |
Confidence (CONF→PDD= −.32**) |
Coping Autonomy Sociotropy |
Confidence (PDD → CONF = .26* CONF → PDD = −.44**) Supportive Network (PDD→NETW = .25*) |
p<.05,
p<.01;
These are nodes that were directly related to percent days’ drinking (PDD) over the three months prior to each measurement time point.
Note: Bolded nodes are mechanisms specifically targeted in FS-CBT, non-bolded nodes are mechanisms targeted in both treatment conditions. Confidence= confidence to abstain from alcohol; Coping=use of alcohol-related coping skills; PDD=percent days drinking in 3 months prior to assessment; Supportive Network=size of social network that is supportive of patient’s abstinence from alcohol.
When attending to network model type, regardless of treatment condition, notable results can be summarized as follows: Autonomy, confidence to abstain, and coping skills were associated with drinking across all time points (between-subject models). Use of alcohol-related coping skills was most predictive of a woman’s concurrent drinking (contemporaneous models). Similarly, autonomy and confidence to abstain were most associated with time-lagged changes in drinking (temporal models).
Discussion
This study used a novel approach to examine how two treatments led to change in alcohol use and other relevant therapeutic targets among women with AUD. These analyses focused on examining mechanisms of behavior change among women receiving treatment for AUD, including apriori-established variables that were hypothesized to improve during treatment and contribute to decreased alcohol. Additionally, the statistical approach allowed for the examination of the contributions of individual mechanisms, while simultaneously accounting for the variation in several other relevant mechanisms. Although results of the parent RCT analyses showed similar, positive outcomes in the two treatment conditions – female-specific (FS-) and gender-neutral CBT for AUD (GN-CBT) – the current analyses showed that there were both similarities and some distinctions in the mechanisms of change in the treatments that have important implications for research on mechanisms of change, particularly among women with AUD. Therefore, the results extend AUD literature on mechanisms of change generally, and particularly extends our understanding of mechanisms of change among treatment-engaged women.
One node –depression – was found to be an important variable specifically in GN-CBT. This was unanticipated, given that FS-CBT directly targeted depression while GN-CBT did not, however it is consistent with past research showing that depression is an important factor in women’s recovery (Greenfield et al., 2007). One potential explanation is that because depression was not directly targeted in GN-CBT, it varied more within women in GN-CBT or was not neutralized during treatment since it was not directly addressed, and therefore affected variation in the other network nodes, including drinking, in a way that was more controlled among women in FS-CBT. This was reflected in the sample variances for GN- and FS-CBT, with the variance in GN-CBT being more than twice that of FS-CBT. Two female-specific nodes – sociotropy and social network supportive of abstinence – were central variables specifically in FS-CBT. This is consistent with the focus on these mechanisms in FS-CBT (but not GN-CBT), which explicitly addressed the importance of decreasing sociotropy and having supportive social networks, and teaching participants in that group strategies for developing such networks.
Three nodes were found to be important variables in both GN- and FS-CBT – confidence to abstain from alcohol, use of alcohol-related coping skills, and autonomy. Use of coping skills and confidence were both targeted in both GN- and FS-CBT, and thus their centrality is consistent with hypotheses. It is important to note that this study demonstrates the importance of these mechanisms of change in AUD treatment while controlling for the presence of several other mechanisms of change – including depression, anxiety, social network support for abstinence, sociotropy, and autonomy. Additionally, examining the network models suggests that use of coping skills and confidence to abstain are important mechanisms that influence not only drinking, but also other related and important constructs such as anxiety, depression, and autonomy. The emergence of autonomy as a node that was directly associated with drinking in both treatment conditions, aggregated across time and after conditioning on all the other variables in the network, is notable and a novel finding.
Autonomy is not generally targeted in psychotherapy for AUD, yet this study demonstrates broad effects that changes in a woman’s autonomy during treatment can have, as reflected by the centrality of this node within the temporal networks for both GN- and FS-CBT. Autonomy was targeted directly only in FS-CBT, but in the temporal GN-CBT model autonomy was shown to statistically predict both women’s coping and confidence to abstain at the next study time point. It is possible that participant’s autonomy is an important mechanism, potentially via its effects on confidence to abstain and increase her use of coping skills – which then, as illustrated in the current study and extensive past research, are closely associated with decreased alcohol use. Given the inclusion of multiple mechanisms of change in these networks, the exact effect of autonomy on drinking and the other variables cannot be determined, however these results suggest autonomy as a potential important mechanism of change in women treatment receiving AUD treatment.
Limitations
Both a benefit and complication of allowing multiple variables to interact is that there are some contradictory associations. These are highlighted in Table 2. For example, although autonomy was a very central node in the GN-CBT between-subjects network, the positive direction of its association to drinking is contradictory. However, in GN-CBT bivariate correlations, autonomy and drinking were negatively associated (Table 2), becoming positively associated only when looking at partial correlations (Table 3). Given that autonomy had a strong positive association with confidence, which then was negatively associated with drinking, the positive association between autonomy and drinking may be due to a suppressor effect, which can occur when bivariate correlations change significantly and/or switch directionality when conditioned on the other variables in the models (e.g., as a partial correlation) (Simpson, 1951). The central nodes identified in this study deserve further study to more clearly understand the nature of their association with drinking and recovery from AUD.
An additional limitation is the predominance of White, Non-Hispanic participants in the sample (92%); therefore, the results may not generalize to other racial or ethnic groups. This is particularly true given that the effects of variation in some of the variables – for example, autonomy and sociotropy – may differ between cultures. This is an important area in need of continued research.
Future Directions & Conclusions
In addition to the centrality of confidence to abstain and use of alcohol-related coping skills, autonomy was central in a number of the models across treatment conditions. Although autonomy, and its counterpart sociotropy, have been linked to other compulsive behaviors such as bulimia (Hayaki, Friedman, Whisman, Delinsky, & Brownell., 2003) and smoking (Westmaas, Ferrence, & Wild, 2006), as well as depression, anxiety, and self-consciousness (McBride, Bacchiochi, & Bagby, 2005) among women, it has not been focused on among women with AUD. Additionally, the centrality of a social network supportive of abstinence in the FS-CBT networks reflects the importance of this variable in the recovery of women with AUD (and has been shown in previous research to be associated with recovery from substance misuse more generally, Magill, Kiluk, McCrady, Tonigan, & Longabaugh, 2015). Autonomy and social support network may be important avenues for exploration, especially in providing treatment for women with AUD. Although the current study has demonstrated their relevance to women specifically, it would be beneficial to assess them in mixed-gender samples to further examine the gender specificity of these processes.
If confidence to abstain and use of alcohol-related coping skills are mechanisms of change in CBT for AUD, a relevant question would be how to increase these among women. While coping skills can be directly taught, confidence to abstain is not easily “taught” in treatment. Results from the current study suggest that increased autonomy and social networks supportive of abstinence may not only impact drinking directly but may also increase women’s use of coping skills and confidence. Increasing autonomy and supportive social network are tangible mechanisms that can be targeted in treatment, which can lead to increased confidence, coping, and, subsequently, likelihood of abstinence.
Use of multilevel vector autoregression estimation and network analysis represents a novel approach to exploring mechanisms of change in AUD treatment. An important contribution of this approach is that it does not impose pre-specified models onto the data or assume the existence of latent variables that underlie and drive participant change and progress. Rather, this approach allows the data to describe how changes occur. Using a multilevel modeling approach to network analysis also is consistent with the idea of behavior change as a process, acknowledging the important effect of time. Continued work on and research using these methods with RCT data may advance our knowledge of mechanisms of behavior change and understanding of how our therapies confer their beneficial effects.
Public Health Significance:
This study examined the mechanisms that lead to behavior change among women receiving female-specific and gender-neutral cognitive behavioral therapy for alcohol use disorder (AUD), using a novel statistical approach. Results support and extend previous research findings by: (a) demonstrating that increasing a woman’s self-confidence to avoid drinking and increasing her use of alcohol-related coping skills is central to change in AUD treatment, (b) demonstrating the importance of personal autonomy as an additional mechanism of change in treating women’s AUD, and (d) showing that the two treatment conditions led to improvements via both overlapping and divergent mechanisms.
Acknowledgments
Funding information: This project was supported by NIAAA grant R01AA007070. Authors report no conflicts of interest. Preliminary results of these analyses were presented as a poster at the annual conference of the Research Society on Alcoholism in June 2018.
Appendix 1: Masked Narrative Description
The data reported in this manuscript have been previously published. Findings from the data collection have been reported in separate manuscripts. MS 1 (published) reports on the main outcomes of the study, comparing FS-CBT to GN-CBT in terms of primary and secondary outcomes, as described in the introduction of this manuscript. MS 2 (published) focuses on abstinence plans that were developed in the first session of treatment, and examines which plans were associated with drinking outcomes. MS 3 (published) focuses on sudden gains during treatment, focusing on percent days drinking, urge intensity, and urge frequency. MS 4 (published) focuses on the internal and external motivation among the participants to engage in treatment. MS 5 (published) examined women’s preferences for individual versus couple-based treatment for AUD. MS 6 (published) examined differences in treatment outcome based on age, using data from this study and a second, related clinical trial. MS 7 (published) examined sudden gains in drinking related to sessions treating anxiety and depression, using data from this study and a second, related clinical trial. MS 8 (published) focused on co-occurring anxiety disorders among the sample and whether diagnosis was associated with drinking outcomes.
References
- Abulseoud OA, Karpyak VM, Schneekloth T, Hall-Flavin DK, Loukianova LL, Geske JR, … & Frye MA (2013). A retrospective study of gender differences in depressive symptoms and risk of relapse in patients with alcohol dependence. The American Journal on Addictions, 22(5), 437–442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Afzali MH, Sunderland M, Teesson M, Carragher N, Mills K, & Slade T (2017). A network approach to the symptom-level association between alcohol use disorder and posttraumatic stress disorder. Social Psychiatry and Psychiatric Epidemiology, 52(3), 329–339. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders (4th ed., Text Revision). Washington, DC: APA. [Google Scholar]
- Borsboom D, & Cramer AOJ (2013). Network analysis: An integrative approach to the structure of psychopathology. Annual Review of Clinical Psychology, 9, 91–121. [DOI] [PubMed] [Google Scholar]
- Beck AT, Epstein N, Brown G, & Steer RA (1988). An inventory for measuring clinical anxiety: Psychometric properties. Journal of Consulting and Clinical Psychology, 56(6), 893–89. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, & Garbin MG (1988). Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review, 8(1), 77–100. [Google Scholar]
- Bieling PJ, Beck AT, & Brown GK (2000). The Sociotropy-Autonomy Scale: Structure and implications. Cognitive Therapy and Research, 24, 763–780. [Google Scholar]
- Breslin FC, Sobell LC, Sobell MB, & Agrawal S (2000). A comparison of a brief and long version of the Situational Confidence Questionnaire. Behaviour Research and Therapy, 38(12), 1211–1220. [DOI] [PubMed] [Google Scholar]
- Constantini G, Epskamp S, Borsboom D, Perugini M, Mõttus R, Waldorp LJ, & Cramer AOJ (2015). State of the aRt personality research: A tutorial on network analysis of personality data in R. Journal of Research in Personality, 54, 13–29. [Google Scholar]
- DiClemente CC (2007). Mechanisms, determinants and processes of change in the modification of drinking behavior. Alcoholism: Clinical and Experimental Research, 31(s3). [DOI] [PubMed] [Google Scholar]
- Epskamp S, Waldorp LJ, Mõttus R, & Borsboom D (2018). The Gaussian Graphical Model in cross-sectional and time-series data. Multivariate Behavioral Research, 1–28. [DOI] [PubMed] [Google Scholar]
- Epstein EE, & McCrady BS (2009). Treatments that work: Individual cognitive behavioral therapy for alcohol use problems. Therapist manual. New York: Oxford University Press. [Google Scholar]
- Epstein EE & Menges D (2013). Women and addiction In: McCrady BS & Epstein EE (Eds). Addictions: A comprehensive guidebook (2nd ed., pp. 788–818). NY: Oxford U. Press. [Google Scholar]
- Epstein EE, McCrady BS, Hallgren KA, Cook S, Jensen NK, & Hildebrandt T (2018). A randomized trial of female-specific cognitive behavior therapy for alcohol dependent women. Psychology of Addictive Behaviors, 32(1), 1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- First MB, Spitzer RL, Gibbon M, & Williams JBW (2002). Structured Clinical Interview for the DSM-IV-TR Axis I Disorders, Research Version, Patient Edition (SCID-I/P), New York: Biometrics Research, New York State Psychiatric Institute. [Google Scholar]
- Greenfield SF, Brooks AJ, Gordon SM, Green CA, Kropp F, McHugh RK, … & Miele GM (2007). Substance abuse treatment entry, retention, and outcome in women: A review of the literature. Drug and Alcohol Dependence, 86(1), 1–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hallgren KA, Epstein EE, & McCrady BS (2019, in press). Changes in hypothesized mechanisms of change before and after initiating abstinence in cognitive-behavioral therapy for women with alcohol use disorder. Behavior Therapy. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haslbeck JM, & Waldorp LJ (2018). How well do network models predict observations? On the importance of predictability in network models. Behavior Research Methods, 50(2), 853–861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayaki J, Friedman MA, Whisman MA, Delinsky SS, & Brownell KD (2003). Sociotropy and bulimic symptoms in clinical and nonclinical samples. International Journal of Eating Disorders, 34, 172–176. [DOI] [PubMed] [Google Scholar]
- Kadden RM, & Litt MD (2011). The role of self-efficacy in the treatment of substance use disorders. Addictive Behaviors, 36(12), 1120–1126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kazdin AE, & Nock MK (2003). Delineating mechanisms of change in child and adolescent therapy: Methodological issues and research recommendations. Journal of Child Psychology and Psychiatry, 44(8), 1116–1129. [DOI] [PubMed] [Google Scholar]
- Lemmens LH, Müller VN, Arntz A, & Huibers MJ (2016). Mechanisms of change in psychotherapy for depression: An empirical update and evaluation of research aimed at identifying psychological mediators. Clinical Psychology Review, 50, 95–107. [DOI] [PubMed] [Google Scholar]
- Litman GK, Stapleton J, Oppenheim AN, & Peleg BM (1983). An instrument for measuring coping behaviours in hospitalized alcoholics: Implications for relapse prevention treatment. Addiction, 78(3), 269–276. [DOI] [PubMed] [Google Scholar]
- Longabaugh R, Wirtz PW, Zweben A, & Stout RL (1998). Network support for drinking, Alcoholics Anonymous and long-term matching effects. Addiction, 93, 1313–1333. [DOI] [PubMed] [Google Scholar]
- Longabaugh R, Donovan DM, Karno MP, McCrady BS, Morgenstern J, & Tonigan JS (2005). Active ingredients: How and why evidence-based alcohol behavioral treatment interventions work. Alcoholism: Clinical and Experimental Research, 29(2), 235–247. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP, Krull JL, & Lockwood CM (2000). Equivalence of the mediation, confounding, and suppression effects. Prevention Science, 1(4), 173–185). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Magill M, Kiluk BD, McCrady BS, Tonigan JS, & Longabaugh R (2015). Active ingredients of treatment and client mechanisms of change in behavioral treatments for Alcohol Use Disorders: Progress 10 years later. Alcoholism: Clinical and Experimental Research, 39(10), 1852–1862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McBride C, Bacchiochi JR, & Bagby RM (2005). Gender differences in the manifestation of sociotropy and autonomy personality traits. Personality and Individual Differences, 38, 129–136. [Google Scholar]
- McCrady BS, Epstein EE, & Hirsch L (1999). Maintaining change after conjoint behavioral alcohol treatment for men: Outcomes at six months. Addiction, 94, 1381–1396. [DOI] [PubMed] [Google Scholar]
- McCrady BS, Epstein EE, Cook S, Jensen NK, & Ladd BO (2011). What do women want? Alcohol treatment choices, treatment entry and retention. Psychology of Addictive Behaviors, 25(3), 521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrady BS, Epstein EE, Hallgren KA, Cook S, & Jensen NK (2016). Women with alcohol dependence: A randomized trial of couple versus individual plus couple therapy. Psychology of Addictive Behaviors, 30(3), 287–299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrady BS (2017). Alcohol use disorders: Treatment and mechanisms of change In McKay D, Abramowitz JS, & Storch EA (Ed.), Treatments for Psychological Problems and Syndromes. NY: Wiley Press. [Google Scholar]
- Nock MK (2007). Conceptual and design essentials for evaluating mechanisms of change. Alcoholism: Clinical and Experimental Research, 31(S3), 4S–12S. [DOI] [PubMed] [Google Scholar]
- Rosenthal RN (2013). Treatment of persons with substance use disorder and co-occurring other mental disorders McCrady BS & Epstein EE (Eds.). Addictions: A Comprehensive Guidebook. NY: Oxford University Press, 659–707. [Google Scholar]
- Simpson EH (1951). The interpretation of interaction in contingency tables. Journal of the Royal Statistical Society B, 13, 238–241. [Google Scholar]
- Sobell LC, & Sobell MB (1978). Validity of self-reports in three populations of alcoholics. Journal of Consulting and Clinical Psychology, 46, 901–907. [DOI] [PubMed] [Google Scholar]
- Sobell LC, Maisto SA, Sobell MB, & Cooper AM (1980). Reliability of alcohol abusers’ self-reports of drinking behavior. Behavior Research and Therapy, 17, 157–160. [DOI] [PubMed] [Google Scholar]
- Sobell LC. & Sobell MB. (1996). Timeline followback user’s guide: a calendar method for assessing alcohol and drug use. Toronto, Ontario, Canada: Addiction Research Foundation. [Google Scholar]
- Sobell LC, Sobell MB, & Agrawal S (2009). Randomized controlled trial of a Cognitive-Behavioral Motivational Intervention in a group versus individual format for substance use disorders. Psychology of Addictive Behaviors, 23(4), 672–283. [DOI] [PubMed] [Google Scholar]
- Stout RL, Wirtz PW, Carbonari JP, & Del Boca FK (1994). Ensuring balanced distribution of prognostic factors in treatment outcome research. Journal of Studies on Alcohol, supplement, (12), 70–75. [DOI] [PubMed] [Google Scholar]
- Westmaas JL, Ferrence R, & Wild TC (2006). Autonomy (vs. sociotropy) and depressive symptoms in quitting smoking: Evidence for trait-congruence and the role of gender. Addictive Behaviors, 31, 1744–1760. [DOI] [PubMed] [Google Scholar]
- Zweig RD, McCrady BS, & Epstein EE (2009). Investigation of the psychometric properties of the Drinking Patterns Questionnaire. Addictive Disorders & Their Treatment, 8(1), 39–51. [Google Scholar]